
infection prevention and control in maternity care
14
ffl l a UNIVERSITY OF t:7 LIVERPOOL THINK SEPSIS, ACT FAST-M The urgent need to improve infection prevention and control in maternity care The intersection of WASH, IPC and AMR David Lissauer NIHR Professor of Global Maternal Health Malawi-Liverpool-Wellcome Trust, Blantyre, Malawi
Transcript of infection prevention and control in maternity care
ffll a UNIVERSITY OF
t:7 LIVERPOOL
THINK SEPSIS, ACT FAST-M
The urgent need to improve infection prevention and control in maternity care
The intersection of WASH, IPC and AMR
David Lissauer
NIHR Professor of Global Maternal Health Malawi-Liverpool-Wellcome Trust, Blantyre, Malawi

A positive and safe birth for all
Health workers in maternal and newborn care are committed to making childbirth a positive, life-affirming experience for women,
their babies and their birth partners



Water, sanitation and hygiene
Sanitation 35% facilities lack appropriate water 20% facilities lack toilets/latrines
(WHO,UNICEF 2015)
Hand Hygiene Challenges:
Infrastructure Staffing, crowding, time Compliance
But evidence of successful programs (WHO, 2015)

Water, sanitation and hygiene infrastructure
• Water, sanitation and hygiene (WASH) infrastructureis essential for effective infection prevention
• Factors to be assessed: • access to running or flowing water from a high-
quality source • sanitation services • toileting facilities, including menstrual hygiene
requirements in maternity areas • hand hygiene resources like soap and alcohol-
based handrub • safe health-care waste disposal facilities
• Tools such as WHO WASHFIT can help to assess and monitor WASH infrastructure
Source: Water and Sanitation for Health Facility Improvement Tool (WASH FIT). Geneva: World Health Organization; 2017 (https://apps.who.int/iris/handle/10665/25491.0).
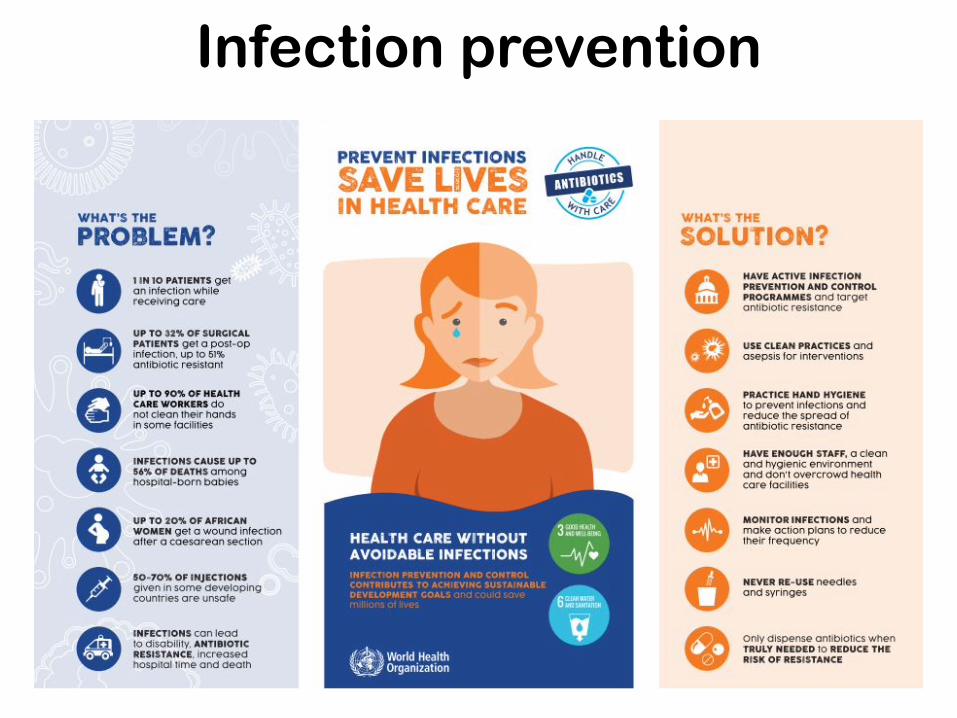
'S THE
PROBLEM?
0 0 Q 0 C,
-e
1 I N 10 PATIENTS ge an infectia while rece, ng core
UP TO S2% OF SURGICAL PATI ENTS get a past-op mlectio , up o 61 antibiotic resiSto nc
UP TO 90% OF HEALTH CARE WORKERS do no cleon t r hands in some acilities
I NFECTIONS CAUSE UP TO 56% OF DEATHS among llospJta l- t>orn babies
UP TO 20% OF AFRICAN WOMEN get o wound infection o tter a caesorean section
50-70% OF INJ IECTIONS given 1n some developing countries are unsafe
I NFECTIONS con lead to disobility, ANTIBIOTIC RESISTANCE, increased llosp11a1 time and death
HAVE ACTIVE INFECTION PREV£NTION AND CONTROL PROGRAMMES and arget antibiouc resistance
USE CLEAN PRACTICES and aseps1s for interventions
PRACTICE HAND HYGIENE to preven Infections o nd reduce the spread of antibio 1c resistance
HAVE ENOUCH STAFF, a clean and hygienic enviro ment and don·1 overcrowd lleaUh core f0<::IIU1es
MONITOR I NFECTIONS and make action pla ns to reduce th ir freq ency
NEVER RE- USE needles and syr inc;ies
Only dispense antibiotics wtien TRULY NEE.OED to REDUCE THE RISK OF RESISTANCE
Infection prevention
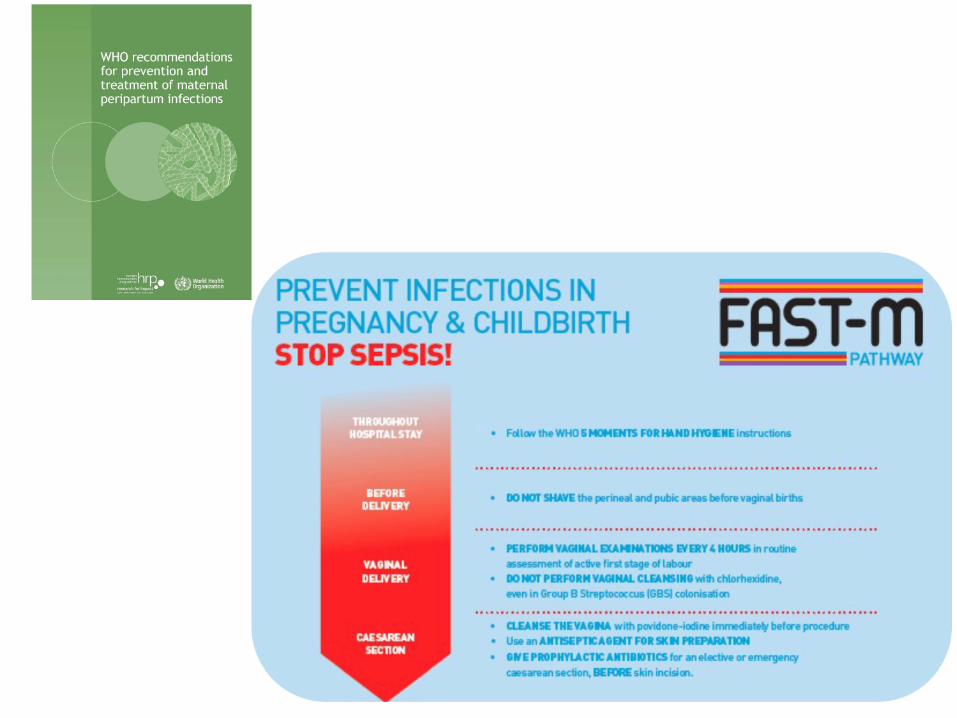
REVENT INFECT ONS I REGNANCY & CHILDBIRTH FAST-m
STOP SEPSIS! PATHWAY
• FollOft' th WHO MOMENTS FOR .-ND H't'GEN rGtructions
lilEFORE • DONCJT the rine I nd pubic ar s fore vagina\ births - DB.NERY
• PERFORM VAGINALEXAMINUIONS ERY 4 HOURS in rcutin V.UNAL se m ntof sta
DliUVERY • DO NOT PER NAL N nth chlorhexidine,
n In Group B Strep ococcus IGBSI coton ation
• CLEAN TH VA NA Ith povidone-4 i lmmedia b fore proc dure Cil~ • Use an AN PTICA EMT FOR N nn::t"JU'UlTION
SlCllON • fl P PHYlACTIC ANTIIUOTICS for n el r,.• or em rg ncy
s in incision.

GIVE ANTIBIOTIC PROPHYLAXIS CORRECTLY
1STTRIMESTER
2NDOR3RD TRl4E'STER
1ST,12ND STAG& OF LA80UR
3RDST.AGE OFLHIOUR
CAliSAREAN SliCTION
Abortion or Miscarriage Surgery IMVA/EVA('JO&CI
Premrm prelabour rupture of membranes IPPR0 MI
Uncomplicated second or third trimester
Premrm Labour w;tt, int.act amniotic membranes
Prelabour rupture of membranes IPROMI at or near term
Vaginal Group B Streptococcus (GBSI colonisation
Meconi um-stained amniotic fluid
Uncomplicated vaginal birth
Operative vaginal birth lforceps or vacuum-assisted delivery I
M nual removal of the placenta
3rd or 4th degree perineallears ltorn analsphincler, anus or rectum)
Electiw or emergency caesarean section (antibiotics should be giwn BEFORE skin incision!
UNITED AGAINST MATERNAL SEPSIS
YES NO
X
X
X
X
X
X
X
X
X
X
X
X
Antibiotic overuse and misuse are common in maternity

Avoiding overcrowding and adequate staffing
Facility overcrowding can:
• Increase the risk of HAIs, nosocomial outbreaks and the spread of antimicrobial resistance
• Lead to inadequate health-care worker staffing levels
To avoid overcrowding on admission and throughout the hospital stay, the facility should ensure:
• No more than one patient per bed
• Spacing of at least 1 metre between the edges of beds
• Overall occupancy that does not exceed the designed total bed capacity of the facility
• A referral system in case the facility reaches full capacity
WHO recommends adequate bed occupancy, avoiding overcrowding and adequate staffing as a core component of effective IPC programmes
Source: Guidelines on core components of infection prevention and control programmes at the national and acute health care facility level. Geneva: World Health Organization; 2016 (https://www.who.int/publications/i/item/9789241549929).

F?FFfTI~~~FAsgr-m 1
I 1 1 I I I I I I I I I I I I
1 11 11 1 1
I I I I I
I I I I I I I I I I I I I
I I I I I I I I I I I I I
I I I I I I I I I I I I I
, I I I I II II II 1111 I I I I I I I I I I I I I I
I I I I I I I I I I I I I I I I I I I I I I I I I
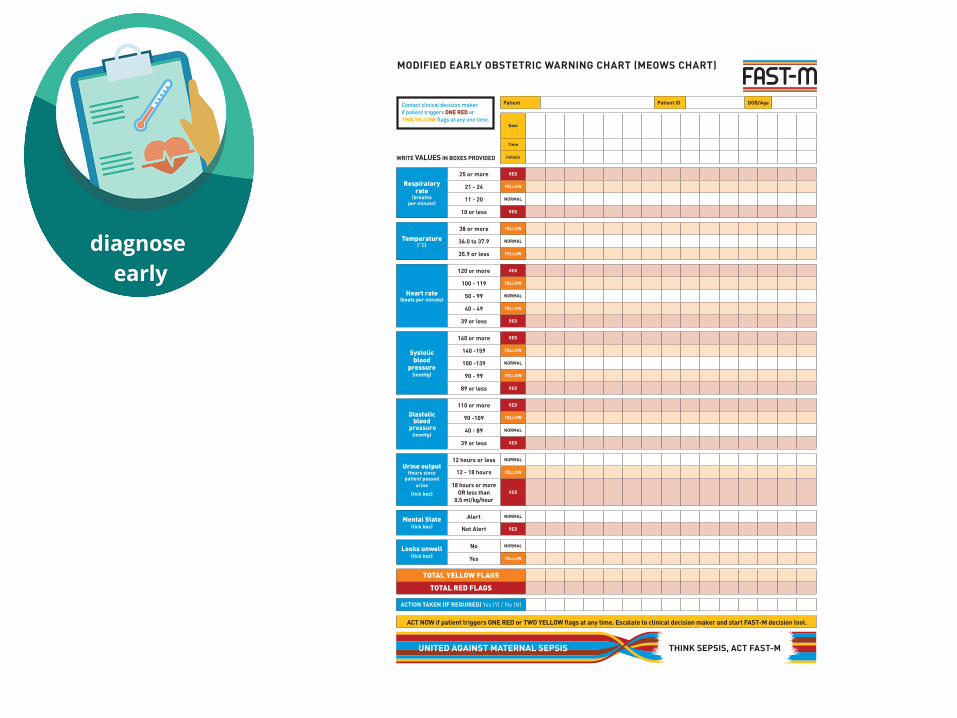
MODIFIED EARLY OBSTETRIC WARNING CHART (MEOWS CHART)
Date
Time
WRITE VALUES IN BOXES PROVIDED Initials
Respiratory rate
(breaths per minute)
25 or more RED
21 - 24 YELLOW
11 - 20 NORMAL
10 or less RED
Temperature (˚C)
38 or more YELLOW
36.0 to 37.9 NORMAL
35.9 or less YELLOW
Heart rate (beats per minute)
120 or more RED
100 - 119 YELLOW
50 - 99 NORMAL
40 - 49 YELLOW
39 or less RED
Systolic blood
pressure (mmHg)
160 or more RED
140 -159 YELLOW
100 -139 NORMAL
90 - 99 YELLOW
89 or less RED
Diastolic blood
pressure (mmHg)
110 or more RED
90 -109 YELLOW
40 - 89 NORMAL
39 or less RED
Urine output Hours since
patient passed urine
(tick box)
12 hours or less NORMAL
12 - 18 hours YELLOW
18 hours or more OR less than
0.5 ml/kg/hour RED
Mental State (tick box)
Alert NORMAL
Not Alert RED
Looks unwell (tick box)
No NORMAL
Yes YELLOW
TOTAL YELLOW FLAGS
TOTAL RED FLAGS
ACTION TAKEN (IF REQUIRED) Yes (Y) / No (N)
ACT NOW if patient triggers ONE RED or TWO YELLOW flags at any time. Escalate to clinical decision maker and start FAST-M decision tool.
Patient Patient ID DOB/AgeContact clinical decision maker if patient triggers ONE RED or TWO YELLOW flags at any one time.
UNITED AGAINST MATERNAL SEPSIS THINK SEPSIS, ACT FAST-M

TREAT SEPSIS
GIVE IV FLUIDS
GIVE IV ANTIBIOTICS
IDENTIFY &TREAT THE SOURCE OF INFECTION
CONSIDER TRANSFER TO SPECIALIZED CARE
MONITOR VITAL SIGNS OF THE MOTHER AND FETUS

TACKLING ANTIMICROBIAL
RESISTANCE: Supporting national
measures to address infection prevention
and control ancfwa er, sanitation and hygiene in
health care settings
World Health un·1cefttf'litOrganization ~
Antimicrobial resistance (AMR) presents asignificant threat to human health. World leaders have agreed that tackling AMR will require addressing both health and agriculture concerns with afocus on prevention. Improving infection prevention and control (IPC) and water, sanitation, and hygiene (WASH) is one of the five objectives in the World Health Organization's (WHO) AMR Global Action Plan. Nowhere is reducing infection more important than in health care facilities.Joint, immediate action to address IPC and WASH is essential.
3 lnaused burden ofexpensive, hanl-to-trut and llfe-thrHtenlng
Addressing these challenges will require accelerating joint efforts to improve WASH, IPC and AMR in health care settings.
reslstlnt Infections ==::::i lnaused use of antllllotlcs to trNt pmentallle InfectionsCempn11111sed
4 Deaease In patient confidence InIPCpractkes health are
lnaused reslstlnce


















