Infection Prevention and Control Annual Report 1 April ...
29
Infection Prevention and Control Annual Report 1 st April 2013 - 31 st March 2014 Produced by: The Director of Infection Prevention and Control Written by: Lead Nurse Infection Prevention & Control Reviewing the period: April 2013 - March 2014 Approved by Infection Control Committee: July 2014 Received by Trust Board: July 2014
Transcript of Infection Prevention and Control Annual Report 1 April ...

Infection Prevention and Control Annual Report
1st
April 2013 - 31st
March 2014
Produced by: The Director of Infection Prevention and Control
Written by:
Lead Nurse Infection Prevention & Control
Reviewing the period: April 2013 - March 2014 Approved by Infection Control Committee: July 2014 Received by Trust Board: July 2014

- 2 –
Annual Report – Infection Prevention and Control April 2013-March 2014
Table of Contents
Section:
Page:
1 Introduction
4
2 Infection Control Roles and Governance Structures Within the Trust 2.1 Corporate Responsibility 2.2 Infection Prevention and Control team and Members 2.3 Infection Control Committee 2.4 Internal Reporting Arrangements 2.5 Reports to the Executive Team and Trust Board 2.6 Risk Register
4 4 4 5 5 6 6
3 Infection Control Resources Within the Trust 6
4 Infection Control in 2014/15: The Local Picture 4.1 Aseptic Non Touch Technique 4.2 Infection Prevention and Control Strategy
6 6 7
5 Mandatory Surveillance During 2014/15 5.1 Mandatory reporting 5.1.1 Meticillin Resistant Staphylococcus aureus (MRSA) 5.1.2 Meticillin Sensitive Staphylococcus aureus (MSSA) 5.1.3 Surveillance of Clostridium difficile toxins 5.1.4 Escherichia coli bacteraemia 5.1.5 Surveillance Glycopeptide Resistant Enterococcal (GRE) bacteraemia 5.2 Other Resistant Bacteria 5.3 Surgical Site Infection 5.3.1 Orthopaedic 5.3.2 Caesarean Section
7 7 8 9
10 10 11 11 12 12 13
6 The Infection Control Team: Other Core Activity During 2014/15 6.1 Education and Training 6.2 Supporting and Working with Infection Control Link Staff 6.3 Implementation of the European Directive on Safer Sharps 6.4 Audit and Monitoring 6.5 Working with the Patients and Public 6.6 Working to Ensure Optimum Hospital Hygiene 6.6.1 Cleaning and Catering Services 6.7 Sterile Services 6.8 Redesigning Environments and New Builds 6.8.1 Endoscopy
14 14 15 15 15 16 16 16 18 18 19
7 Infection Control Policy and Procedures Within the Trust
19
8 Outbreaks and Incidents at the Trust in 2014/15 8.1 Pandemic Influenza 8.2 Gastroenteritis / Norovirus 8.3 Needlestick incidents and Prevention of Needlestick injuries 8.4 Legionella and Water Quality Monitoring
19 19 19 20 20
9 Management of Antibiotics Prescribing at the Trust in 2014/15
22
10 Safety and Quality in Infection Control: Statutory Duties 10.1 Care Quality Commission
23 23
- 3 –
Annual Report – Infection Prevention and Control April 2013-March 2014
11 Measures of Infection Prevention and Control: Shaping Practice to Improve Performance
24
12 Looking Forward to 2014/15 24
13 Conclusion
25
14 Acronyms
26
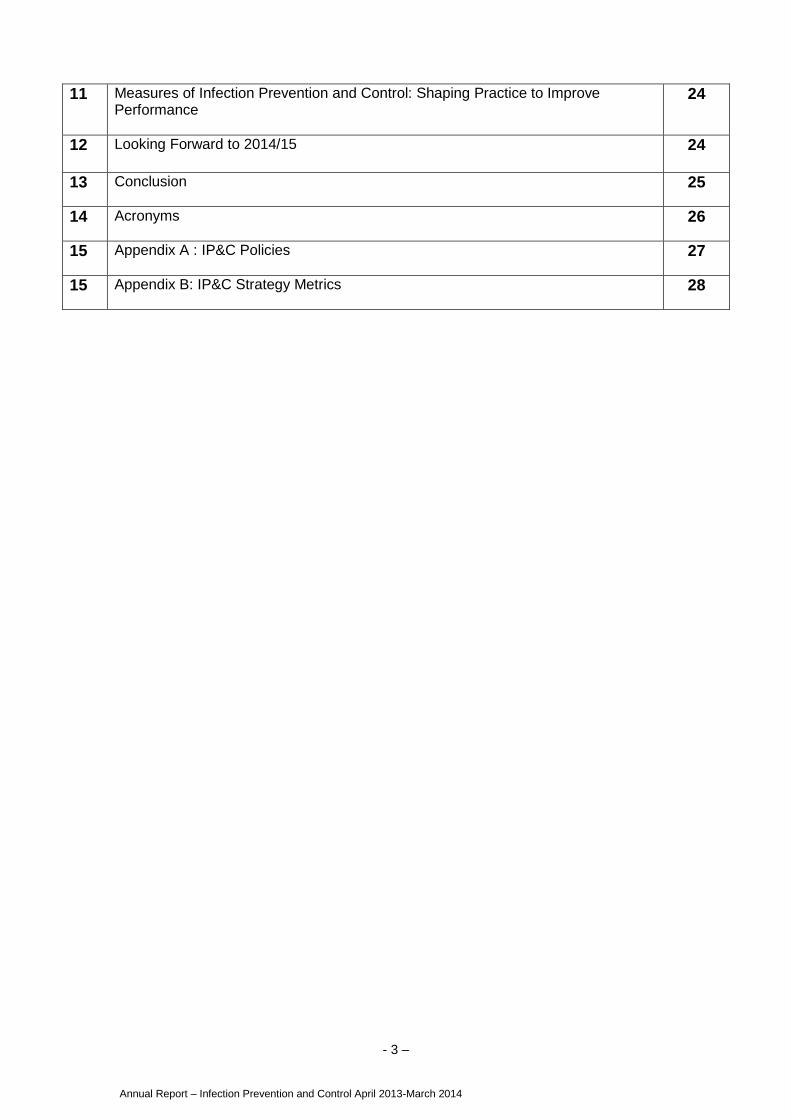
15 Appendix A : IP&C Policies
27
15 Appendix B: IP&C Strategy Metrics
28

- 4 –
Annual Report – Infection Prevention and Control April 2013-March 2014
1 Introduction to the Report
This is the annual report from the Director of Infection Prevention and Control (DIPC)
providing information on infection prevention and control activity across the
organisation. The purpose of this report is to provide detail to our patients, public,
staff, Trust Board, Commissioners and Monitor on the infection control agenda for the
previous year.
This report covers the period from 1st April 2013-31st March 2014 and provides
performance against national targets for:
Meticillin Resistant Staphylococcus Aureus (MRSA) bacteraemia figures,
Clostridium difficile Toxin (CDT) rates,
Healthcare associated infections
Other key activities and audit for the year.
Infection prevention and control remains a key patient safety and quality focus for the
organisation. This year was the first year NHS England set all MRSA bloodstream
infections targets as nil, as they continue to pursue a zero tolerance approach to
Health Care Associated Infections (HCAI). A zero target for MRSA, coupled with a
significant reduction in the Clostridium difficile threshold, proved very challenging for
the Trust at a time when there is greater scrutiny and challenge for reducing HCAI.
Whilst the Trust did not achieve the MRSA bloodstream infection target, performance
was sustained with only 1 case reported. Key achievements for 2013/14 include:
.
Clostridium difficile infections were reduced by 48% reporting only 12 cases
from a threshold of 14
No ward closures due to confirmed/suspected Norovirus through the winter
period, an achievement never seen before.
2.1 Corporate Responsibility
The Hillingdon Hospitals NHS Foundation Trust maintains a full compliment of staff
for infection prevention and control as required under the Health and Social Care Act.
The Director Infection Prevention and Control (DIPC) is both an Executive member of
the board and also the Director of Nursing and Patient Experience.
The Trust has two Consultant Microbiologists, one of whom holds the position of
infection control doctor and they continue to provide specialist advice and
microbiology support on a 24hour basis. The specialist nursing team and
antimicrobial pharmacist are available during office hours Monday to Friday.
2.2 Infection Prevention and Control (IPC) Team and Members
In May 2013 the Trust appointed a new Director of Nursing and Patient Experience
and as a result a new DIPC. Whilst this new appointment did not affect the specialist
nursing team, it did bring to the organisation an experienced DIPC and returned the
2 Infection Control Roles and Governance Structures Within the Trust

- 5 –
Annual Report – Infection Prevention and Control April 2013-March 2014
team to full strength with the return of the Deputy DIPC and Deputy Director of
Nursing.
Infection control team members consist of:
2.3 The Infection Control Committee
The Infection Control Committee (ICC) report an overview of the infection control
agenda and progress throughout the year to the Quality and Risk Committee (QRC).
ICC is a key forum for the development and performance management of the
infection control agenda across the organisation. The Committee meets bi monthly
and is chaired by the DIPC with key representation from across the organisation.
Membership includes the ICT, a number of senior management and senior nurses,
the Occupational Health Department, clinical governance staff, Pharmacy, Estates
and Facilities staff and external bodies such as the local Public Health England
(PHE) Health Protection Unit and Hillingdon Community Health (HCH).
A change in the NHS and consequently the community with the establishment of
Clinical Commissioning Groups (CCGs) has seen the Infection Control Committee for
HCH no longer exist. Whilst the Infection Control Nurses from HCH attend the Trusts
ICC it is challenging to collaboratively drive forward the IP&C agenda across the
health economy when there is no current ICC in the CCG.
2.4 Internal Reporting Arrangements
New to 2013/14 is a Patient Safety and Quality Report submitted quarterly. This
report includes key information on the Trusts quality and safety priorities reflecting
the new Clinical Quality Strategy. Infection control includes performance against
National objectives as well as progress on local trust initiatives and has been well
received across the organisation.
Infection Prevention and Control (IP&C) is also discussed monthly via divisional
dashboards at the Divisional Reviews with the Executive Team. These divisional
dashboards include HCAI data, overall IP&C performance and compliance to
antimicrobial prescribing.

- 6 –
Annual Report – Infection Prevention and Control April 2013-March 2014
2.5 Reports to the Executive Team and Trust Board
The Infection Control Team provide a range of measures to The Board monthly
which include cleaning scores, infection control audit results, compliance to restricted
antimicrobial prescribing, MRSA screening and other initiatives. IP&C performance is
also commented on in the monthly performance report so that direct feedback on
post infection reviews or root cause analysis is provided to the board and any
necessary actions.
2.6 Risk Register
The Trust includes the risk of HCAI on the corporate risk register. The risk is updated
and reviewed every 2 months at ICC, in order to reflect current priorities and
activities; and is presented to QRC for discussion and scrutiny.
The ICT continues to have a budget that is predominately staff pay. The team does
however continue to work closely with the procurement department to ensure the
trust purchases quality products, that are fit for purpose and deliver value for money.
In 2013 the ICT developed a business case to upgrade the current IT system ICNet
to the newer version NG. As part of this process the ICT bid in round one of the
Nursing Technology Fund (2013/14) to support this initiative. Whilst this was not
successful the organisation is planning to bid in the second round in the Spring 2014.
Some of the key activities over the past 12 months are outlined below:
4.1 Aseptic Non Touch Technique (ANTT)
ANTT is now an established technique across the Trust and remains key in reducing
intravenous (IV) related blood stream infections. Annual reassessments are
undertaken in each division, supported by the ICT. Across the organisation ANTT
was above 95% by the end of the year. The performance by division is demonstrated
in the chart below:
85%
90%
95%
100%
Medicine Surgery W&C CSS
91%
98%99%
100%
Divisional ANTT 2014 Competencies
Medicine
Surgery
W&C
CSS
3 Infection Control Resources Within the Trust
4 Infection Control in 2014/15: The Local Picture

- 7 –
Annual Report – Infection Prevention and Control April 2013-March 2014
4.2 Infection Prevention and Control Strategy
In the third and final year of the IP&C strategy the Trust successfully achieved a
number of measures (refer Appendix B) Those not achieved fully have been included
in the annual HCAI action plan and will form the basis of the new trust IP&C 3 year
strategy, these included:
C section surveillance
Further improvement in Antimicrobial prescribing and stewardship
5 The Infection Control Team: Mandatory Surveillance During 2013/14
5.1 Mandatory Reporting
The Trust reports the following mandatory HCAI statistics to both the Trust Board and
Public Health England (PHE) on a monthly basis.
Meticillin Resistant Staphylococcus aureus (MRSA) bacteraemia
Clostridium difficile infection
Meticillin Sensitive Staphylococcus aureus (MSSA) bacteraemia
Escherichia coli (E coli) bacteraemia
The Trust follows guidance for HCAI associated deaths. Where MRSA or C.diff is
included as a part 1A, 1B or 1C on a death certificate it is entered onto the Strategic
Executive Information System (STEIS).
Inclusion criteria in this data set are any incidents of C diff on the same ward if two or
more cases were reported in one week or three in a month. A Root Cause Analysis
(RCA) is undertaken on such cases and they are presented to ICC for monitoring and
scrutiny of any arising actions. In 2013/14 there were 3 cases reported under this
guidance as detailed below:
Reason for STEIS report Number of cases
MRSA on death certificate 2
C diff on death certificate 1
Two cases C diff on 1 ward in a week 0
Included in the above data is an MRSA case which was attributed to the CCG and
died shortly after admission and the MRSA case which was attributed to the
organisation sadly died. All of the above cases had root cause analysis (RCAs)
- 8 –
Annual Report – Infection Prevention and Control April 2013-March 2014
5.1.1 Meticillin Resistant Staphylococcus aureus (MRSA)
With the new NHS landscape and emergence of CCGs also came a change to the
MRSA bloodstream infection objectives and methods of attributing cases to
organisations.
Any Trust reporting a positive MRSA blood stream infection will be expected to
complete a Post Infection Review (PIR). The organisation for leading the case is
responsible for completing a PIR within 1 week of the date of assignment (acute
providers will be assigned the PIR for samples taken after the 1st two days of
admission and the CCG for those admitted septic.) The outcome of the PIR should
establish the organisation to which the bacteraemia should be finally assigned. The
final assignment will identify the organisation best placed to ensure that any lessons
learned are acted upon. It was envisioned that with this new system there would be
greater partnership working across the health economy.
The variety of MRSA objectives was abolished for 2013/14 with a zero tolerance
approach to MRSA bloodstream infections, therefore all organisations has a target of
zero for the year.
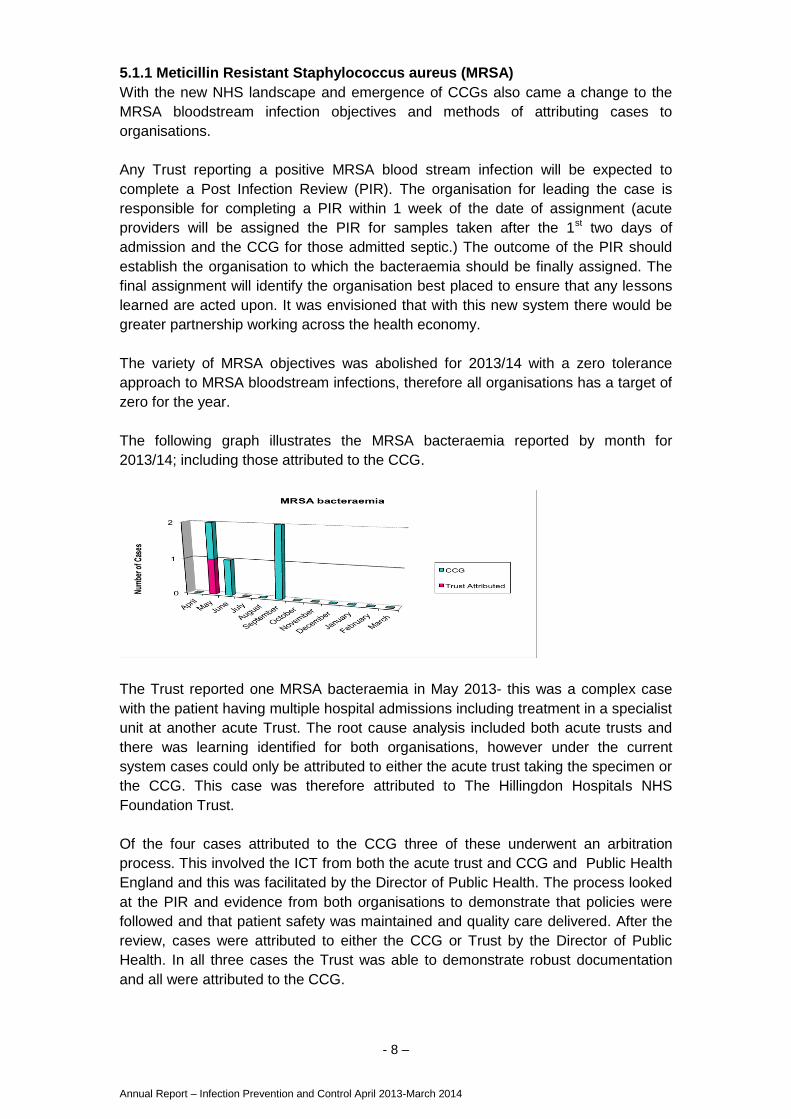
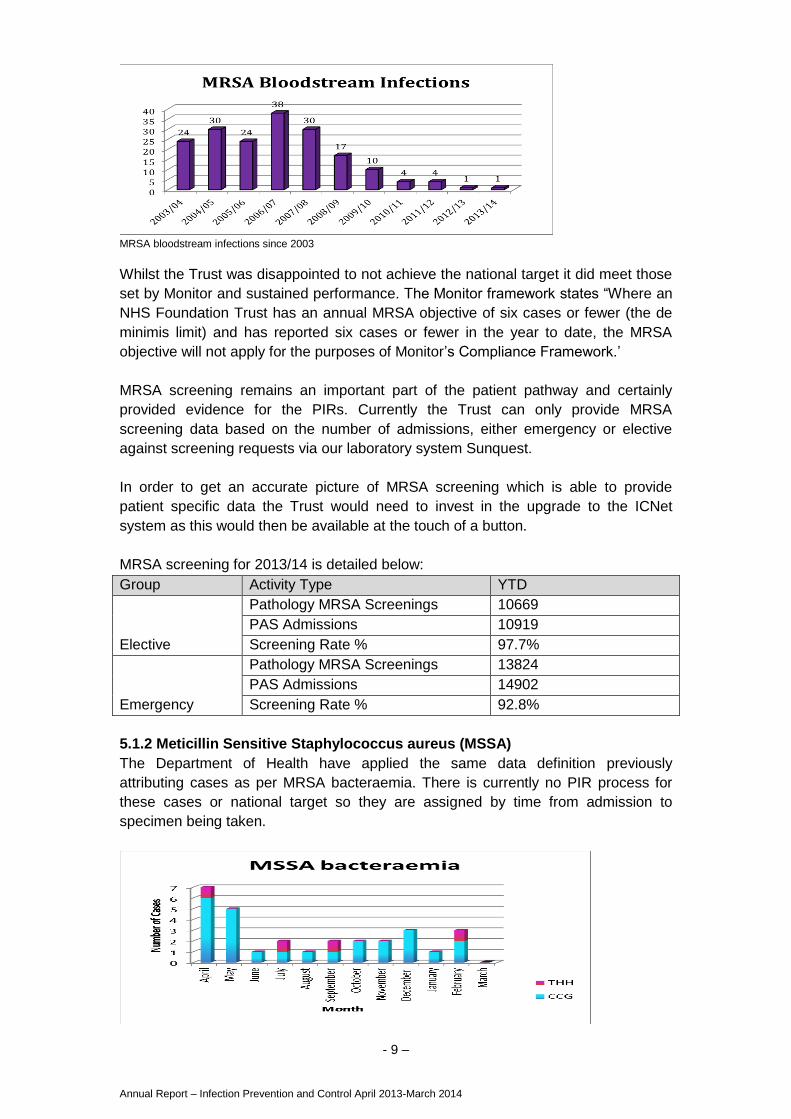
The following graph illustrates the MRSA bacteraemia reported by month for
2013/14; including those attributed to the CCG.
The Trust reported one MRSA bacteraemia in May 2013- this was a complex case
with the patient having multiple hospital admissions including treatment in a specialist
unit at another acute Trust. The root cause analysis included both acute trusts and
there was learning identified for both organisations, however under the current
system cases could only be attributed to either the acute trust taking the specimen or
the CCG. This case was therefore attributed to The Hillingdon Hospitals NHS
Foundation Trust.
Of the four cases attributed to the CCG three of these underwent an arbitration
process. This involved the ICT from both the acute trust and CCG and Public Health
England and this was facilitated by the Director of Public Health. The process looked
at the PIR and evidence from both organisations to demonstrate that policies were
followed and that patient safety was maintained and quality care delivered. After the
review, cases were attributed to either the CCG or Trust by the Director of Public
Health. In all three cases the Trust was able to demonstrate robust documentation
and all were attributed to the CCG.
- 9 –
Annual Report – Infection Prevention and Control April 2013-March 2014
MRSA bloodstream infections since 2003
Whilst the Trust was disappointed to not achieve the national target it did meet those
set by Monitor and sustained performance. The Monitor framework states “Where an
NHS Foundation Trust has an annual MRSA objective of six cases or fewer (the de
minimis limit) and has reported six cases or fewer in the year to date, the MRSA
objective will not apply for the purposes of Monitor’s Compliance Framework.’
MRSA screening remains an important part of the patient pathway and certainly
provided evidence for the PIRs. Currently the Trust can only provide MRSA
screening data based on the number of admissions, either emergency or elective
against screening requests via our laboratory system Sunquest.
In order to get an accurate picture of MRSA screening which is able to provide
patient specific data the Trust would need to invest in the upgrade to the ICNet
system as this would then be available at the touch of a button.
MRSA screening for 2013/14 is detailed below:
Group Activity Type YTD
Elective
Pathology MRSA Screenings 10669
PAS Admissions 10919
Screening Rate % 97.7%
Emergency
Pathology MRSA Screenings 13824
PAS Admissions 14902
Screening Rate % 92.8%
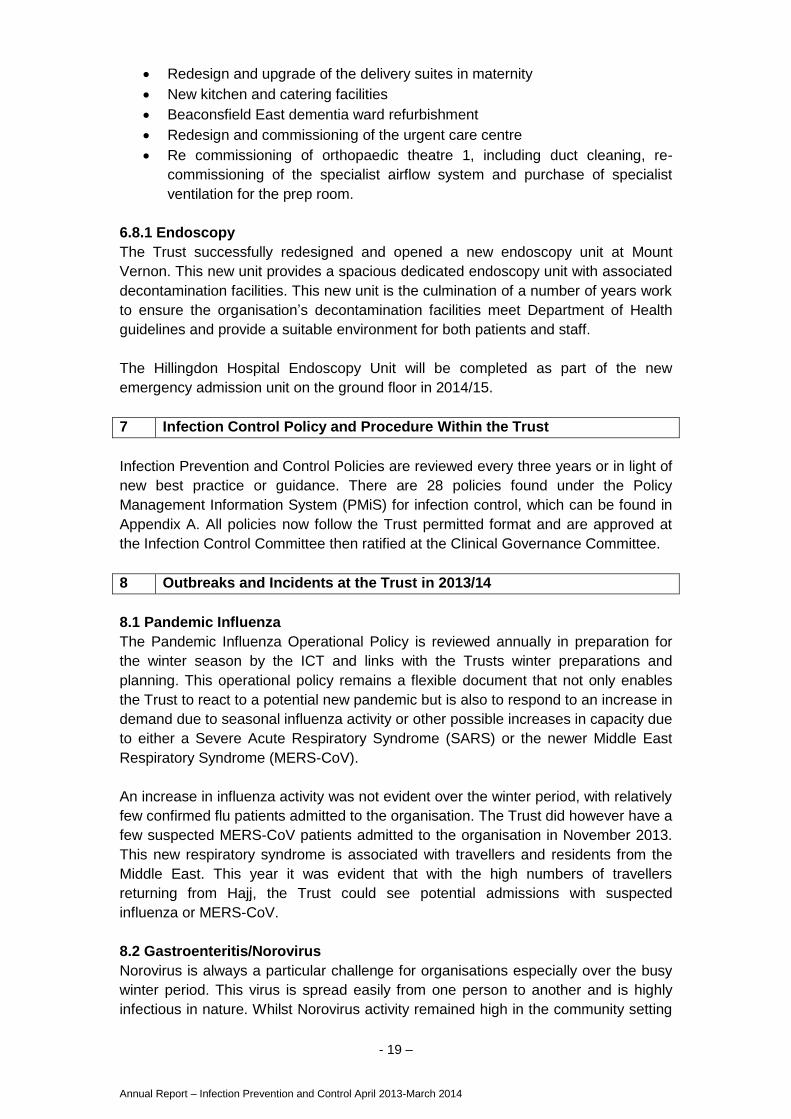
5.1.2 Meticillin Sensitive Staphylococcus aureus (MSSA)
The Department of Health have applied the same data definition previously
attributing cases as per MRSA bacteraemia. There is currently no PIR process for
these cases or national target so they are assigned by time from admission to
specimen being taken.

- 10 –
Annual Report – Infection Prevention and Control April 2013-March 2014
5.1.3 Surveillance of Clostridium difficile toxins
The annual objective for C. difficile was significantly reduced from the previous year’s
number to just 14. This was a significant challenge for the organisation having
finished 3 years with between 23-25 cases. A case attributed to the acute
organisation is defined as a case where the sample was taken on the fourth day or
later of an admission to that trust (where the day of admission is day one).
Following the previous year’s root cause analysis the Trust was aware that a
proportion of the positive cases were associated with inappropriate sampling. In
order to improve clinical practice and provide more accurate information for teams on
bowel management the ICT developed a new Bristol stool chart with the
multidisciplinary team. This was successfully passed through the clinical records
committee and is now used in clinical practice.
2013/14 demonstrated a significant reduction on previous year’s numbers reporting
12 cases which was a 48% reduction. This met both national and monitor targets for
the year.
C diff cases for 2013/14
The chart below details the number of cases per month
5.1.4 Escherichia coli (E coli) bacteraemia
E. coli is a species of bacteria commonly found in the intestines of humans and
animals. There are many different types of E. coli, and while some live in the intestine
quite harmlessly, others may cause disease.

- 11 –
Annual Report – Infection Prevention and Control April 2013-March 2014
There is no objective or target associated with this bacteramia and it is not included
in London performance data. However E coli bacteraemia contribute to a high
number of blood stream infections and the significant effect on both the patient and
burden on the health economy should not be underestimanted. In total there were
149 E coli blood stream infections for 2013/14 with the siginifcant number of patients
admitted with septicaemia.
By using the same data definitions as MRSA and MSSA attributed cases, the Trust
has reported the following cases as represented in the following graph.
5.1.5 Surveillance of Glycopeptide Resistant Enterococcal (GRE) Bacteraemia
GRE are resistant to glycopeptides (antibiotics such as vancomycin) and have been
nationally reported since 2003. During 2013/14 the Trust reported no cases, with the
last reported case being in 2010. Although the incidence remains low the ICT will
continue to monitor and report cases.
5.2 Other Resistant Bacteria
Carbapenemase-producing Enterobacteriaeae The Trust has received both a letter from Public Health England and a Patient Safety
Alert in relation to carbapenemase-producing Enterobacteriaceae and other
carbapenem-resistant organisms.
Enterobacteriaceae are a large family of bacteria that usually live harmlessly in the
gut of all humans and animals, but, in the wrong place, can cause serious infections.
Worldwide, a small but increasing number of strains of enterobacteriaceae have
become resistant to carbapenem antibiotics, which have been defined by WHO as
critically important antibiotics. Increasing trends in sporadic infections, clusters and
outbreaks of carbapenemase-producing Enterobacteriaceae (CPE) have been
observed in a number of NHS trusts in England. There is a high risk of this problem
becoming more widespread unless early and decisive action is taken by Trusts as
these bacteria represent a significant challenge in terms of prevention, treatment and
control.
In the UK, we have a window of opportunity to prevent widespread problems caused
by these organisms. Whilst we are seeing increasing numbers of carbapenemase-
producing Enterobacteriaceae, we have not yet reached the escalated situation seen
in other countries.
New guidance on the management and detection of these resistant organisms has
been produced and the Infection Prevention and Control Team are reviewing current

- 12 –
Annual Report – Infection Prevention and Control April 2013-March 2014
policies and practice to ensure we meet these new recommendations. Crucial to
these new guidelines is the ability to isolate a higher number of patients within the
organisation. This is clearly a challenge for all trusts as isolation facilities are at a
premium, and often risk based. If we are to fully implement the new guidance then in
2014 the ICT with the Trust will have to review the isolation facilities across the
organisation and provide recommendations on how isolation facilities can be both
improved and increased in number.
5.3 Surgical Site Infection
5.3.1 Orthopaedic
Surveillance of orthopaedic surgical site infection (SSI) is undertaken for both total
hip replacements and repair of fractured neck of femur only. Whilst this meets our
mandatory requirements for SSI the Trust would ideally like to extend this
surveillance over additional surgical techniques.
In the July - September 2013 submission period for total hip replacements and neck
of femur the Trust saw an unusual peak in the number of surgical site infections. For
this quarter the combined rates were 2% for hip replacement and 4.4% for repair
neck of femur, with National data for hip replacement at 1.2% and neck of femur
1.7%. This resulted in the Trust being identified as an outlier by PHE, as we are
outside national rates. In actual cases this represented four infections for neck of
femur in one data collection period which triggered the orthopaedic and infection
control team to review the cases.
The increased incidence of cases was discussed at the divisional audit day and ICC
in both January and March. Whilst initial investigation did not identify any immediate
themes such as the same surgeon a more detailed case review was undertaken by
the orthopaedic team. The Trust held a meeting with the wider multidisciplinary team
focusing on surgical site infection, the report on the cases and to identify any further
actions. In order to monitor the effectiveness of any change in practice the meeting
agreed to currently take forward work on:
Culture and behaviour within the theatre environment (including wearing of
scrubs outside theatre areas)
Maintenance of Normothermia- including pre, intra and post operative
rewarming
Skin decolonisation / washes prior to surgery
Dressing changes on non orthopaedic specialist wards.
Since 2013 the Trust has been reviewing the operating theatre environment and has
a planned programme of works which includes re-commissioning of the theatres.
Work on one orthopaedic theatre has been completed and the second orthopaedic
theatre has planned maintenance in May 2014, with the remaining theatres to follow.
Water testing for Pseudomonas aeruginosa was commenced in October 2013, as
this is national guidance for critical care areas where patients are either
immunocompromised or whose defences may have been breached ie: surgery. This
will be undertaken as per guidance every 6 months. The Trust did identify taps which
were positive and remedial work with re-testing was undertaken.

- 13 –
Annual Report – Infection Prevention and Control April 2013-March 2014
It should be noted that we did not report any SSIs in neck of femur for the following
two periods of surveillance but the increase in cases for July-September has clearly
affected the combined 4 month data.
There is only a small number of total hip replacements carried out at the Hillingdon
site. The majority of cases, as they are elective are undertaken at Mount Vernon
however patients with a Body Mass Index (BMI) over 40, ASA* 3 or 4 or require ITU
admission are done at the Hillingdon site. The one reported case for July-September
was very complex with a number of co-morbidities and high risk factors. PHE have
responded to a recent communication from the Trust that they would note that only
high risk cases are done at the Hillingdon site.
(*The ASA score is a subjective assessment of a patient's overall health that is
based on five classes (I to 5). 1 is patient has severe systemic disease that is not
incapacitating to 5 Patient has incapacitating disease that is a constant threat to life.)
The Trust is taking seriously this increased incidence and in collaboration with the
Infection Control Team, there is a current business case to upgrade ICNet to the NG
version and include the SSI module. This upgrade would enable real time monitoring
and greater ownership by the clinicians involved. Our strategy, risk register and HCAI
action plan all identify the need to expand SSI surveillance and for surgeons to have
the ability to analyse and own their own data in order to understand patient outcomes
and drive safer, quality care. Work on reducing surgical site infection is a priority for
2014/15.
Surgical site infections are estimated to account for 15 per cent of all hospital-
acquired infections and affect around 5 per cent of all patients undergoing a surgical
procedure. (PHE 2012) Monitoring of surgical site infections is complicated; while
many occur during hospitalisation, the majority manifest only after discharge, a
phenomenon that has increased as hospitals have sought to reduce the length of
inpatient stays. In these instances, the infection is often managed in primary care and
is only recognised by the host institution if the patient is readmitted and these cases
are typically not captured in monitoring/surveillance studies due to the manual nature
limiting scope of surveillance.
SSI data for 2013/14 is reflected in the table below
Trust
Site
Procedure Number of
cases
Number of
cases with SSI
% SSI National data
MVH Total hip
replacement
236 1 0.4% 1.2%
THH Neck of femur
fracture
169 5 3% 1.7%
THH Total hip
replacement
91 3 3.3% 1.2%
5.3.2 Caesarean section
Recent studies have shown that C-section infection could be as high as 9.6%
nationally in recent studies. The ICT have been working closely with the women and
children’s division in order to establish a C-section surveillance system as currently

- 14 –
Annual Report – Infection Prevention and Control April 2013-March 2014
the Trust does not have robust knowledge of current infection rates. With birth rates
increasing and patient choice we need to be able to monitor rates in order to drive
reductions, therefore encouraging more patients to choose the organisation.
A data collection sheet has been agreed with the division but there remain
challenges around receipt of completed data. A recent change in something as
simple as the colour of the data collection form has seen a significant increase in the
number of returns to the ICT office. In quarter 1 of 2014 it is anticipated that the Trust
will have some robust data to analyse.
6 The Infection Control Team: Other Core Activity during 2013/14
The ICT remains focussed on patient safety, reductions in HCAI and that no person
is harmed by a preventable infection. The team appreciate the focus and
commitment from the members of staff across the organisation, including the Trust
Board in ensuring they deliver safe quality care in a clean and suitable environment.
6.1 Education and Training
The ICT continue to deliver IP&C training to all members of staff across the
organisation; this training varies from regular formal sessions to individual bespoke
delivery at a ward or department level.
2013 saw a completely new approach for statutory and mandatory training across the
organisation. Instrumental to these changes was the move to ensure that the
organisation followed the ‘core skills training framework’ outcomes for subject
matters and included in this were refresher periods. The ICT had undertaken a risk
based approach in previous years, establishing 3 levels of training. This new system
has clinical and non-clinical staff only with refresher periods moving from every 2-3
years for clinical staff to annual and for non- clinical staff from once to every 3 years.
The ICT worked closely with the STaM training advisory group as subject matter
experts (SME) in IP&C. Concern was raised by the ICT at the time that current
training, which was over 80% across the organisation, would drop significantly and
measures would need to be in place to deliver extra-ordinary sessions.
The Trust announced in January the new move for STaM training with details of the
new fresher periods. An ‘amnesty’ period from February to March was announced
with a significant amount of additional sessions provided by SMEs. Linked to this
transition was the movement of the current reporting for STaM to a new system as
well as linking training records to ESR. Up to January 2014 the Trust was over 80%
compliant in all levels of IP&C training. Data for January and February was not
reported due to the ‘amnesty’, additional staff trained during this period is detailed
below:
Training Number of Staff attended
Non-clinical 76
Clinical 236

- 15 –
Annual Report – Infection Prevention and Control April 2013-March 2014
6.2 Supporting and Working with Infection Control Link Staff
Link nurses from wards and departments have a pivotal role as the member of the
team in order to drive forward the IP&C agenda. Each clinical area has a named link
nurse and in some departments and wards there are two members of staff who
support each other in this role.
The ICT held one link nurse study day in 2013 with representation from a number of
specialist staff. A key item on this agenda was work around waste management. The
Trust had just introduced new waste streams and it was essential that staff were
clear on the use of the new offensive and alternative waste streams including new
hard burn bins.
6.3 Implementation of the European Directive on Safer Sharps
July 2013 saw the introduction of new safety engineered devices and a week of
raised awareness on sharps, reporting and reducing risk. Educational stands were
held in both the main entrance and staff canteen, where representatives from the
new companies demonstrated their new products and were supported by the ICT,
Health and Safety Team and Occupational Health.
The new products had a staged roll out supervised by the procurement team and
supported with ward/departmental training by the company representatives. The
introduction of the new devices went smoothly as these products had been trialled in
key clinical areas prior to final approval.
Further work continued throughout the rest of the year with attention on risk
assessments for those devices where safety engineered products are not availanble
or practical.
6.4 Audit & Monitoring
The Trust and ICT currently use the Meridian (Optimum) system to support audit and
monitoring across the organisation. This system which is principally used for patient
experience data, is also used for some IP&C audits but cannot be used for all
measures due to limitations in the system.
Currently the system is used for hand hygiene, VIP, Bare Below Elbows by the ward
staff and for linen and isolation by the ICT. The Meridian system is due for contract
review at the end of the year and the ICT is working closely with the audit department
to ensure that the system is suitable for all of its users and provides appropriate data
and reports for the organisation.
The current audits & monitoring for IP&C in 2013/14 are detailed below:
Compliance with Hand Hygiene policy (monthly)
Compliance with Bare Below Elbows policy (monthly)
Compliance with Isolation policy (annually)
Compliance with Restricted Antibiotic Prescribing policy (quarterly)
Compliance with Linen policy (annually)
High Impact Intervention 1 Central Venous Catheter care (monthly)
High Impact intervention 2 Peripheral Line Care (monthly)
High Impact Intervention 4 Preventing Surgical site infection (bi annually)

- 16 –
Annual Report – Infection Prevention and Control April 2013-March 2014
High Impact Intervention 5 Ventilator Care (monthly)
High Impact Intervention 6 Urinary catheter care (monthly)
High Impact Intervention 7 Clostridium difficile care bundle (monthly)
High Impact Intervention 8 Cleaning and decontamination of clinical
equipment (bi-weekly)
6.5 Working with the Patients and Public
The Fighting Infection Together (FIT) is a public group that was established a number
of years ago. This longstanding group is one of a kind with people passionate about
infection prevention and the Trust as a whole. They provide a valuable interface, with
a critical eye between the public, staff and the ICT.
In addition to the support on infection control stands, producing and reading IP&C
leaflets and general awareness raising, they provided significant support in the Trusts
new hand hygiene products. In November 2013 after trials of new products the ICT
with the FIT group and procurement department approved the move from our
previous supply to our new supply Deb-cutan. This new product provided both a
foam sanitiser and soap that was gentle to hands as well as outstanding product
support with posters and our new ‘bus stop’ signs. The new hand hygiene signage is
clear, concise and eye catching with sanitiser signs in red throughout the
organisation.
New sanitiser signs in the main entrance 2013:
6.6 Working to Ensure Optimum Hospital Hygiene The Trust has undertaken a significant investment in order to ensure that we provide
a clean, safe, suitable environment for our patients, staff, visitors and the
organisation.
6.6.1 Cleaning & Catering services PLACE The new PLACE process has replaced the long standing PEAT (Patient Environment
Access Team) process in 2013. It has been introduced to both revitalise the
assessment of the patient environment process but also, more importantly, to ensure
that there is a greater focus on patient involvement in the process.
PLACE covers broadly the same areas as PEAT – namely privacy and dignity,
wellbeing, food, cleanliness and general maintenance of buildings and facilities. It
focuses entirely on the care environment and does not stray into clinical care

- 17 –
Annual Report – Infection Prevention and Control April 2013-March 2014
provision or staff behaviours. It extends only to areas accessible to patients and the
public (for example, wards, departments and common areas) and does not include
staff areas, operating theatres, main kitchens or laboratories.
In the past, all NHS providers have undertaken PEAT inspections and in the same
way, PLACE will continue to provide an invaluable resource in assessing the care
environment. This will directly support the provision of a high quality service to
patients.
The key feature of PLACE is the central role of patients in carrying out the
assessments. At least 50 per cent of the team must be patients, and local
Healthwatch must be offered the opportunity to be involved. Recruiting and training
patient assessors is carried out locally and there is criteria outlining who is eligible
and who is not available to become a patient assessor.
The PLACE assessments took place at Hillingdon and Mount Vernon in April 2013
and involved patient and staff assessors including representatives from Facilities,
Infection Control, Nursing and Estates. The four days of assessments covered
wards, Minor Injuries Unit, Accident and Emergency, outpatients, internal pubic areas
and grounds and buildings and generated almost 400 pages of assessment score
sheets. The assessment scores covered the key areas of hygiene and cleanliness;
condition, maintenance and appearance; privacy, dignity and wellbeing; and food and
hydration.
The results were published nationally in September 2013 with the Trust disappointed
to be below national average for cleanliness; privacy, dignity and wellbeing; and
condition and appearance at the Hillingdon site. Mount Vernon was above the
national average in all of the key domains. On the plus side the Trust’s food and
hydration scores were above the national average. In 2013 the results were used to
develop an Improvement Plan, which focused on the recurrent themes across the
organisation that led to possible failure to meet the required standard or a ‘qualified
pass’. This has resulted in a considerable amount of work that led to reception
changes, new signage, new patient and waiting area chairs, new patient wheelchairs,
an increased focus on cleanliness and hygiene and maintenance improvements.
Domain/Score Hillingdon % Score
Mount Vernon % Score
HH/MVH % Combined Score
National Average % Score
Cleanliness 86.67 98.48 87.66 95.74
Privacy, dignity & wellbeing
74.22 90.68 75.60 88.87
Condition, appearance and maintenance
75.54 90.12 76.76 88.75
Food & Hydration
86.18 92.04 86.67 84.98

- 18 –
Annual Report – Infection Prevention and Control April 2013-March 2014
Cleaning & Catering In August 2013 all cleaning and housekeeping rosters were reviewed and changed to
ensure that they better met the size and infection control risk of an area, the work
taking place there and the throughput. This led to many clinical areas receiving
increased cleaning inputs and achieved savings through better productivity and
utilisation of staff. The team engaged an external cleaning consultant to work with the
team on cleaning processes, equipment and training. Working with infection control
and nursing, for example, the cleaning team changed the processes and structure for
cleaning outpatient areas to improve the standards. There were considerable
catering service developments for both patient dining and retail services during the
year with a new patient and retail kitchen being installed and new patient menus
being introduced as well as a new HACCP manual developed to underpin food
handling and safety.
An internal audit was undertaken by TIAA to determine whether management had
implemented adequate and effective operational and management controls over the
Catering and Cleaning function.
The audit included focus on:
Policy and procedures to ensure the Trust’s catering and cleaning services
meet all applicable regulations and standards for NHS catering and cleaning
services (Trust has identified standards and regulations for compliance;
policies and procedure are in place; training is provided; cleaning
arrangements are in place).
And that Trust’s catering and cleaning service complies with the requirements
of CQC related standards (arrangements/action plans in place to ensure
compliance).
Overall the audit provided substantial assurance against the objectives.
Linen The London procurement program with facilities led the work to tender the linen and
sterile theatre packs contract in 2013. The infection control team played a crucial role
in the tender assessment process participating in the tender assessment group to
review the quality of linen and cleaning processes. Unfortunately the process in late
2013 needed to be repeated, from a contractual point of view, and this will take place
in April and May 2014.
6.7 Sterile Services
The sterile services contract with IHSS continues to provide a good service to the
organisation and is closely monitored by the facilities team in partnership with clinical
services. Performance remains high on equipment turnaround times, which is
encouraging as 2013 saw a number of additional trusts utilising the company and it is
essential that standards are maintained.
6.8 Redesigning Environments and New Builds
The ICT continue to work closely with the project team to ensure that the new
designs and builds are fit for purpose, meet the Health Technical Guidance and
provide a safe, clean environment. The new plans for 2013 included:
- 19 –
Annual Report – Infection Prevention and Control April 2013-March 2014
Redesign and upgrade of the delivery suites in maternity
New kitchen and catering facilities
Beaconsfield East dementia ward refurbishment
Redesign and commissioning of the urgent care centre
Re commissioning of orthopaedic theatre 1, including duct cleaning, re-
commissioning of the specialist airflow system and purchase of specialist
ventilation for the prep room.
6.8.1 Endoscopy
The Trust successfully redesigned and opened a new endoscopy unit at Mount
Vernon. This new unit provides a spacious dedicated endoscopy unit with associated
decontamination facilities. This new unit is the culmination of a number of years work
to ensure the organisation’s decontamination facilities meet Department of Health
guidelines and provide a suitable environment for both patients and staff.
The Hillingdon Hospital Endoscopy Unit will be completed as part of the new
emergency admission unit on the ground floor in 2014/15.
7 Infection Control Policy and Procedure Within the Trust
Infection Prevention and Control Policies are reviewed every three years or in light of
new best practice or guidance. There are 28 policies found under the Policy
Management Information System (PMiS) for infection control, which can be found in
Appendix A. All policies now follow the Trust permitted format and are approved at
the Infection Control Committee then ratified at the Clinical Governance Committee.
8 Outbreaks and Incidents at the Trust in 2013/14
8.1 Pandemic Influenza
The Pandemic Influenza Operational Policy is reviewed annually in preparation for
the winter season by the ICT and links with the Trusts winter preparations and
planning. This operational policy remains a flexible document that not only enables
the Trust to react to a potential new pandemic but is also to respond to an increase in
demand due to seasonal influenza activity or other possible increases in capacity due
to either a Severe Acute Respiratory Syndrome (SARS) or the newer Middle East
Respiratory Syndrome (MERS-CoV).
An increase in influenza activity was not evident over the winter period, with relatively
few confirmed flu patients admitted to the organisation. The Trust did however have a
few suspected MERS-CoV patients admitted to the organisation in November 2013.
This new respiratory syndrome is associated with travellers and residents from the
Middle East. This year it was evident that with the high numbers of travellers
returning from Hajj, the Trust could see potential admissions with suspected
influenza or MERS-CoV.
8.2 Gastroenteritis/Norovirus
Norovirus is always a particular challenge for organisations especially over the busy
winter period. This virus is spread easily from one person to another and is highly
infectious in nature. Whilst Norovirus activity remained high in the community setting

- 20 –
Annual Report – Infection Prevention and Control April 2013-March 2014
and other organisations had wards closed for the first time in years the Trust did not
close one ward or bay over winter due to confirmed/suspected Norovirus.
Seasonal activity was lower in comparison to previous years as can be seen in the
following chart from PHE. However the Trust still admitted cases with diarrhoea and
vomiting and successfully managed them in side rooms without impact on the
organisation. Possible contributing factors to the success of this year’s management
were:
Recent change of Hand Hygiene product and awareness leading to greater
compliance
New pull up banners in the main entrances highlighting Norovirus
A&E undertook a risk assessment for inpatients to identify those patients
currently not symptomatic but had been in household/ contact with relative
with known diarrhoea and vomiting, these patients were isolated as a
precaution.
8.3 Needlestick Incidents and Prevention of Needlestick Injuries
Occupational Health received 76 reports of needle stick injury for 2013/14, which is
three more than the previous year. It was noted that there was a significant rise in
reported needlestick injuries in July with 16 cases, compared with the usual 4-8 per
month. This rise coincided with the month where the Trust had ‘sharps awareness
week’ and is possibly due to the promotion of reporting. Certainly towards the end of
the year injuries from intravenous cannulae has significantly dropped due to the
introduction of the safety engineered device.
8.4 Legionella & Water Quality Monitoring
Legionella bacteria, which cause legionellosis, is an uncommon form of pneumonia
and the majority of cases are reported as single (isolated) cases but outbreaks can
and have occurred. Our duties, as an organisation, are provided in the approved
‘Code of Practice and guidance Legionnaires' disease: The control of legionella
bacteria in water systems (L8)’. This contains practical guidance on how to manage
and control the risks in your system. Control and prevention of the disease is through
treatment of the source of the infection, i.e. by treating the contaminated water
systems, and good design and maintenance to prevent growth in the first place.
The Trust continues to take this responsibility very seriously and is aware of the risks
inherent in a multi building site with a number of older facilities. The Trust has a

- 21 –
Annual Report – Infection Prevention and Control April 2013-March 2014
Water Quality group which meets regularly throughout the year monitoring Trust
performance for both Legionella and Pseudomonas. In February 2014 the Trust
tested a number of outlets as part of re-commissioning of units back into general use
following work or upgrades. A number of these outlets had positive counts and as a
result were chlorinated and a revised system put in place to ensure that outlets under
construction are tested and flushed just prior to handover.
Testing for Pseudomonas aeruginosa
P. aeruginosa is a Gram-negative bacterium, commonly found in wet or moist
environments. It is commonly associated with disease in humans with the potential to
cause infections in almost any organ or tissue, especially in patients compromised by
underlying disease, age or immune deficiency or whose defences have been
breached (for example, via a surgical site, tracheostomy or indwelling medical device
such as a vascular catheter). In most cases, colonisation will precede infection.
Some colonised patients will remain well but can act as sources for colonisation and
infection of other patients. Its significance as a pathogen is exacerbated by its
resistance to antibiotics, virulence factors and its ability to adapt to a wide range of
environments.
Contaminated water in a hospital setting can transmit P. aeruginosa to patients
through the following ways:
direct contact with the water through: ingesting bathing contact with mucous membranes or surgical site, or through splashing from water outlets or basins (where the flow from
the outlet causes splashback from the surface);
inhalation of aerosols from respiratory equipment, devices that produce an aerosol or open suctioning of wound irrigations;
medical devices/equipment rinsed with contaminated water;
indirect contact via healthcare workers’ hands following washing hands in contaminated water, from surfaces contaminated with water or from contaminated equipment such as reusable wash-bowls.
The Trust has identified areas across the organisation for testing of P. aeruginosa
and include ITU, NNU, Bevan and Theatres. In September 2013 the theatre complex
at Hillingdon was tested for P. aeruginosa and some water outlets came back
positive. As per guidance these outlets are taken out of use, remedial work is
undertaken and then retesting of the water supply is undertaken. Only after a number
of tests can the outlet be placed back in use.
Unfortunately during routine testing for theatres one of the positive outlets was
incorrectly labelled. This led to an incident of concern being raised and investigated
by the Trust to ensure that patients and staff were protected. All testing was
undertaken as per guidance with retesting in order to ensure results of <1 cfu/100ml.
No patients in the two weeks following the incident isolated Pseudomonas species.
The direct cause of the incident was attributed to human error exacerbated by a
number of additional factors detailed in the report. In order to prevent a similar
incident occurring the report recommended a number of actions which were

- 22 –
Annual Report – Infection Prevention and Control April 2013-March 2014
contained in a Pseudomonas action plan, a new Standard Operating Procedure and
signage was put into effect immediately.
9 Management of Antibiotic Prescribing at the Trust in 2013/14
The scale of the threat of Anti-Microbial Resistance (AMR) and the case for action
was set out in the “Annual Report of the Chief Medical Officer” published in March
2013. The UK Five Year Antimicrobial Resistance Strategy 2013-2018 set out actions
to address the key challenges to AMR. The overarching goal of the strategy is to
slow the development and spread of AMR. It focuses activities around three strategic
aims; improve the knowledge and understanding of AMR, conserve and steward the
effectiveness of existing treatments, stimulate the development of new antibiotics,
diagnostics and novel therapies.
Antimicrobial prescribing & stewardship (APS) competencies have been developed
by The Advisory Committee on Antimicrobial Resistance and Healthcare Associated
Infection (ARHAI) and PHE; the goal is to improve the quality of antimicrobial
treatment and stewardship and so reduce the risk of inadequate, inappropriate and ill
effect of treatment. The aim is to improve the safety and quality of patient care, as
well as contributing significantly to the reduction in the emergence and spread of
antimicrobial resistance
This year the Trust Antimicrobial Stewardship Group (ASG) started looking at Datix
incidents related to antimicrobials, it continues to monitor spending on antimicrobials
as well as Defined Daily Dosing (DDD)/1000 bed day report on selected restricted
antibiotics. Ward pharmacists continue to report restricted antibiotic use to the
antibiotic pharmacist, these are all reviewed by both the antibiotic pharmacist and the
consultant microbiologists with the average number of reported prescriptions as
184/month
The annual surgical prophylaxis audit which was completed in February 2014,
showed that 78% of patients were given antibiotics as recommended in Surgical
Prophylaxis Guideline. When looking at the timing of administration, in 88% of cases
the correct surgical prophylaxis antibiotic was given at the correct time, this is an
improvement from the 2012 audit.
The ‘Start Smart then Focus’ guidance and its subsequent action plan continue to be
developed. The audit programme for antibiotic compliance has recently changed
from monthly to quarterly. The frequency has been changed in collaboration with the
clinical audit department and ensures that with the new quarterly data an action plan
from divisions will be required to address low compliance. A recent meeting with the
ADOs, NSMs and CDs strengthened the focus on antimicrobial prescribing with a
commitment from specialties to undertake their own audits using a Trust template.
This will provide data specific to the specialty in order to drive performance.
The Trust Continues to take part in the European Antimicrobial Awareness day on
18th November of each year

- 23 –
Annual Report – Infection Prevention and Control April 2013-March 2014
10 Safety and Quality In Infection Control: Statutory Duties & External Visits
The Trust has an established assurance framework for IP&C as the safety of patients
and staff, and quality care is a key consideration for all organisations. The Health and
Social Care Act 2008 clearly reflects our duties and provides a collection of systems,
processes and procedures in order to define the risks to achieve high quality care.
10.1 Care Quality Commission
The Trust was inspected by the CQC over a number of days from 4th-7th October
2013. For Cleanliness and Infection Control the regulated outcome stipulates that;
‘People should be cared for in a clean environment and protected from the risk of
infection.’
The outcome of the inspection was reported by the CQC as the following:
‘Whilst the trust had many positive infection control indicators and audits showed a
low level of infection, we found a number of instances where the risks of the spread
of infection were increased.
We have judged that this has a minor impact on people who use the service, and
have told the provider to take action.
The provider was not meeting this standard’
The Trust was disappointed with the decision by the CQC which was based on:
Isolation doors not shut on all occasions
The use of a cordless phone-on one of the wards
Lack of knowledge amongst clinical staff on curtain changes
Cleaning of equipment
Damaged flooring/ condition of the building
As a result the Infection Control Team revised the current audit programme within the
organisation following the inspection. A new quick question assessment (QQA) tool
was devised using elements from the inspection such as correct use of personal
protective equipment, isolation standards and inspection of equipment in the clinical
area. This was then assessed twice a month and findings reported at both divisional
and Board level. The Trust will continue to audit mattresses annually as well as
adhoc inspections by staff to ensure damaged items are replaced.
The Estates and Facilities team have a robust programme of audit for cleaning of the
Trust and the supervising staff have all been given details of areas in which to pay
particular attention ie: high level dusting.
There is an existing PLACE improvement group which includes any Estates issues
that require rectification eg: damage to floors, and this has already been identified
and a report produced. There are a number of financial implications for the
organisation in particular the maintenance of the Estate and repairs to the existing
floors. A full report with costing on such repairs has been produced since the
inspection.

- 24 –
Annual Report – Infection Prevention and Control April 2013-March 2014
The Trust recognises that whilst it is not following best practice for closing all doors
when isolating patients, this has to be balanced against the risk to the patient. It was
explained during the inspection that as the doors are solid in some parts of the
building, when we have a confused, critically ill or patient at risk of falls then doors
cannot be closed for patient safety reasons. The Trust have however taken the
comments into account and are investigating the possibility of replacing the doors in
order to enable staff to patients clearly.
During the inspection the frequency of curtain changing was identified as a risk as
staff did not know the frequency of changes. The Trust does however have a named
person responsible for all curtains, where records are kept and these were not
requested during the visit. Staff know that they can request change of curtains when
these are damaged or stained and therefore this is not considered a risk to people
who use this service.
The Trust considers that these minor points raised in the inspection did not pose a
risk to patients or visitors. Where the inspection identified torn or damaged items
these were already condemned or replaced. Equipment and the general ward
environment is regularly inspected to ensure it meets standards.
11 Measures of Infection Prevention and Control: Shaping Practice to
Improve Performance
The ICT regularly review and update audit and monitoring to reflect both current
practice and to highlight any areas for improvement. The IP&C measures have been
used to drive performance and sustain best practice. In order to gain maximum
impact and to challenge the divisions around performance the league table
presentation was again reviewed and updated for 2013/14.
Whilst the ICT does utilise the Meridian system this does not fully integrate all of the
current audits and is time consuming to complete at ward level. It is essential in 2014
that when the audit system is reviewed that it is able to adapt to the ever increasing
demands of the organisation and supports staff in their work.
12 Looking forward to 2014/15
As we come to the end of the year new objectives for 2014/15 are established. As
with this year NHS England remain focused on a zero tolerance of MRSA blood
stream infections and have set the same objective of zero. This remains a
substantially challenging target across the NHS as the MRSA bloodstream infections
we see today are now complex, multi-factoral events. New from April 2014 is that
NHS England regional teams will take on the role of arbitrating disputed MRSA
bacteraemia cases which was previously held by Local Authority based Directors of
Public Health.
NHS England and Public Health England have noted that the rate of improvement for
C diff has slowed over recent years. There are indications that for some
organisations at least, C diff levels may be approaching their irreducible minimum

- 25 –
Annual Report – Infection Prevention and Control April 2013-March 2014
level at which these infections will occur regardless of the quality care provided.
Experts have now advised that a more flexible approach is now needed to objectives.
The new changes are primarily focused on further encouraging organisations to look
at each case they identify in order to understand what lessons they are able to learn
in order to improve patient safety.
Trusts have been divided into three cohorts for the purpose of calculating median C
diff rates; these are:
Teaching acute trusts
Non teaching acute trusts
CCGs
Recommendations for 2014/15
1. Upgrade of ICNet to NG version to enable :
Extended surgery interface and surgical site surveillance module
Dedicated Surgical outcome reports to support surgical directorates with
accurate rate reports on infection, readmission and mortality
Provide accurate real-time performance data on surgical infection rates
Enable real time Device Management tool to ensure that infection prevention
team is supported with accurate denominator data and microbiology reports
on device associated infections such as Catheter Associated Urinary Tract
Infections (CA-UTI) and Central Line Associated Bacteraemia (CLABSI).
Provide accurate MRSA screening data at both patient and ward level in
order to drive performance
2. Review of Isolation Facilities
In line with current guidance on isolation for new emerging infections the
current siderooms will not provide the required facilities for both staff and
patients. A risk assessment of the isolation facilities should be undertaken in
order to assess how the organisation will meet the ever increasing demands
for sideroom facilities.
13 Conclusion
The Hillingdon Hospitals NHS Foundation Trust has infection prevention and control
at the heart of its agenda. There have been significant achievements over the past
year for the organisation balanced against some disappointing performance in
PLACE and the CQC inspections. It is important that in this ever changing face of the
NHS where we are faced with new targets, emerging infections and financial
challenges that we ensure patients still receive safe quality care across the
organisation.
As ever infection prevention and control is not just the remit of the infection control
team but it is everybody’s responsibility and we would like to take the opportunity to
thank staff, patients, public, governors and all our stakeholders for their continued
support with this important agenda.
- 26 –
Annual Report – Infection Prevention and Control April 2013-March 2014
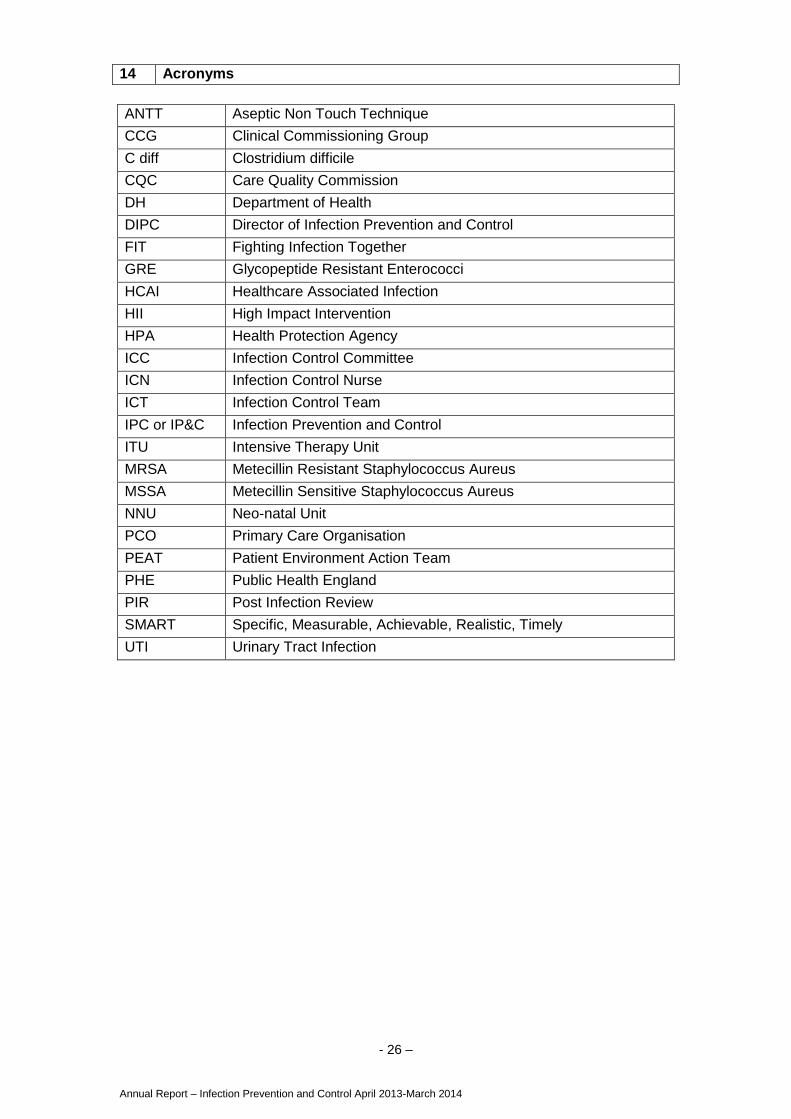
14 Acronyms
ANTT Aseptic Non Touch Technique
CCG Clinical Commissioning Group
C diff Clostridium difficile
CQC Care Quality Commission
DH Department of Health
DIPC Director of Infection Prevention and Control
FIT Fighting Infection Together
GRE Glycopeptide Resistant Enterococci
HCAI Healthcare Associated Infection
HII High Impact Intervention
HPA Health Protection Agency
ICC Infection Control Committee
ICN Infection Control Nurse
ICT Infection Control Team
IPC or IP&C Infection Prevention and Control
ITU Intensive Therapy Unit
MRSA Metecillin Resistant Staphylococcus Aureus
MSSA Metecillin Sensitive Staphylococcus Aureus
NNU Neo-natal Unit
PCO Primary Care Organisation
PEAT Patient Environment Action Team
PHE Public Health England
PIR Post Infection Review
SMART Specific, Measurable, Achievable, Realistic, Timely
UTI Urinary Tract Infection

- 27 –
Annual Report – Infection Prevention and Control April 2013-March 2014
15 Appendix A Infection Control Policies
Policy Number Policy
240 Animals & Pets In Hospital
188 Aseptic Technique Policy
178 Care & Management of Patients in Hospital with Diarrhoea Policy
183 Central Venous Catheter Insertion and Maintenance (CVC)
179 Clostridium Difficile (C diff) Associated Diarrhoea
169 Decontamination of Medical Devices
245 Employment Health Screening (including food handlers and drivers)
177 Hand Washing
244 Immunisation Policy (Occupational Health )
170 Isolation
185 Laundry Sorting
175 Meningitis including Meningococcal Septicaemia
174 MRSA Control (Methicillin-Resistant Staphylococcus)
167 Outbreak (Food Poisoning or Communicable Disease)
186 Re-use of Single Use Items Supplied for Single Use Only
165 Risks Associated with Infection Prevention and Control
166 Safe Handling & Removal of Infected Bodies
181 Scabies
172 Standard (Universal) Precautions
171 Surveillance
176 TB Prevention & Control
187 Transmissible Spongiform Encephalopathies (TSE) Creutzfeldt
Jacob Disease (CJD)
231 Urinary Catheter
189 Varicela Zoster Virus (Chickenpox/Shinges)
180 Viral Haemorrhagic Fever (VHF)- suspected cases of
173 Visual Infusion Phlebitis (VIP) Score

Strategy Priority Area and Strategy
Ref:
Action Plan Ref:
Priority Q1
Q2
Q3
Q4
Comments
6.1 Culture & leadership
Nos. 7&9
Receive and review Divisional HCAI action plans at ICC G G G G All divisions HCAI action plans presented bimonthly
Executive ward visits to include observation and discussion on IP&C measures G G G G Observation of care launched February 2013 which includes ward appearance
Sisters/Charge Nurses to enforce stricter IP&C measures – embed visitors’ charter, revised signage, enforce BBE/hand hygiene etc (recs from People in Partnership group work) – to be monitored through observation and discussion
A A A G Visitors’ charter implemented, new signage on for Hand Hygiene now Trust wide.
6.2 Accountabilities, responsibilities and organisational framework
Nos. 4,5&9
Discuss and endorse all RCA actions at executive level (trust attributed MRSA and CDI cases) and present actions to ICC
G G G G RCAs reviewed at ICC – itemised on agenda.
New Post Infection Review (PIR) process to be used across the organisation in line with Public Health England (PHE guidance. In case of arbitration cases DIPC and Lead ICN to attend
G G G G PIR process in place. 3 arbitration meetings attended to date all awarded to CCG
ToR refreshed 2012 for ICC and included more active medical representation A A A A Regular representative from Surgical division still pending
Antimicrobial Group to include revised membership, ensure robust annual action plan and bi-monthly reporting to ICC
A A G New member to ASG includes Lead Pharmacist. Reporting is an agenda item on ICC and papers now received
Each division to table one IP&C item at divisional governance forum per annum (e.g. antimicrobial stewardship)
A Dates to be confirmed and taken forward for 2014/15
6.3 Performance reporting
Nos. 3, 4, 5&8
Receive and review the HCAI assurance framework based on H&S Care Act at ICC every six months
G G HCAI Assurance Framework to ICC March.
Report key IP&C performance and compliance to ICC with exception reporting to QRC Committee
G G G G Robust reporting in place to ICC
Establish a surveillance system to enable performance reporting for SSI Caesarean section wounds
A A G SSI monitoring process agreed with W&C and date collection started March 2014
6.4 Accessible information
No. 11
Public website and staff Intranet information resources are to be reviewed and refreshed
G G G G FIT group reviewed current public information. LICN reviews staff Intranet monthly to ensure all aspects up to date.
Refresh posters in accordance with People in Partnership group work suggestions
A A G New posters for Hand Hygiene throughout Trust for hand hygiene. New Norovirus full pull up banners designed by FIT group in use.
6.5 Improving patient safety
No. 5, 13&14
Ensure that the review of IP&C policies is on track A A G Programme of review in place for all ICC policies and included in HCAI action plan.
Outbreak management procedures to be reviewed & amended based on learning from 2012/13 winter period
G G G G D&V protocol reviewed and approved September 2013. New banners in use and updated Norovirus leaflet reviewed and agreed by FIT group
Consider further and improved technology in relation to cleaning clinical areas post CDI/Norovirus etc
*G Further discussion with Estates and Facilities planned for Quarter 4 2013 after new in house cleaning contract embedded. New microfiber system purchased by Facilities to replace current system.

- 29 –
Annual Report – Infection Prevention and Control April 2013-March 2014
Comply with the new EU directive on sharp safety which includes introduction safety engineered devices
A A A A Sharp safety week in June. New Medical devices introduced July 2013. Further devices to be launched after trials
6.6 Surveillance & reporting
No.&10
Improve antimicrobial prescribing compliance to >95% A A A A Start Smart then Focus action plan in progress and clinical specialties undertaking own audits. Compliance still not consistently above 95% but discussion and engagement has significantly improved across the organisation.
ICT to validate local monitoring and performance to be published G G G G VIPS currently validated by ICT and urinary catheter audits. New QQA tool launched in November, adhoc validation.
Undertaken business case for ICNet upgrade to NG which includes SSI module and real time MRSA screening.
*G Business case complete. Not funded in 1st
round nursing technology fund and expression of interest submitted for 2
nd round funding
6.7 Risk assessment & audit
No. 12 Gain assurance that the replacement programme for hand wash basins is on schedule
* No budget for 2013/14 allocated to replace CHWB- £150K available for 2014/15 and audit planned April/May as major refurbs undertaken across organisation. Any new build/ refurb includes new CHWB
Risk assessments to be completed for sharp safety where new devices not available
A A
A A In progress, work only started in 2013 and will be ongoing process as new devices available.
Risk register for IP&C to be reviewed at ICC bimonthly and updated. G G G G Risk register updated bi monthly
6.8 Training & education
Nos. 1&3
Sustain compliance for IP&C training at > 80% A A G G Currently Trust overall performance 80% in all levels. New system to be launched Q3 across the organisation.
Deliver more robust ANTT programme and achieve compliance at >95% by March 2014
A A G New process resulted in annual assessment for 2013/14, staff required to have annual review to be completed by March 2014.
6.9 Partnership working
No. 6 Deliver annual joint IP&C awareness event with partners Due to change in PCT and new CCG there is currently no community ICC. Joint IP&C awareness event agreed for 2014.
FIT member engagement to agree IP&C patient information. To be included in new PLACE assessment process
G G G G FIT group reviewed IP&C leaflets Q2 and approved trial new hand hygiene products. FIT members included in PLACE assessments