Infection, nosocomial infection,SIRS MODS for 3rd year MBBS student
38
Infection, Nosocomial infection, SIRS, MODS DR. MD. SHERAJUL ISLAM FCPS (SURGERY) CONSULTANT(SURGERY) PABNA MEDICAL COLLEGE HOSPITAL
Transcript of Infection, nosocomial infection,SIRS MODS for 3rd year MBBS student

Infection, Nosocomial infection, SIRS, MODS
DR. MD. SHERAJUL ISLAMFCPS (SURGERY)
CONSULTANT(SURGERY)PABNA MEDICAL COLLEGE HOSPITAL

Micro-organisms are normally prevented from causing infection in tissues by intact epithelial surfaces. These are broken down in trauma and by surgery.
Protective mechanism can be divided into:•Mechanical barriers•Chemical: low gastric pH• Humoral: antibodies, complement and opsonins•Cellular: phagocytic cells, macrophages
polymorphonuclear cells and killer lymphocytes

Infection Invasion of microorganisms their multiplication and creation of
adverse host response by breakdown of local and systemic host defenses.
Causes of reduced host resistance to infection
1. Metabolic2. Disseminated disease3. Iatrogenic

Metabolic: i) Malnutrition (including obesity) ii) Diabetes iii) Uraemia iv) Jaundice
Disseminated disease: i) Cancer ii) Acquired immunodeficiency syndrome (AIDS)
Iatrogenic: i) Radiotherapy ii) Chemotherapy iii) Steroids

Classification of sources of infection
■ Primary: acquired from a community or endogenous source
■ Secondary or exogenous (HAI): acquired from the operating theatre or the ward or from contamination at or after surgery

Surgical Infections
A surgical infection is an Infection that is unlikely to respond to nonsurgical treatment or occurs in an operated site.
.

Examples of 1st group appendicitis , empyema, gas gangrene, and most abscess.
Examples of 2nd group Wound infections or SSIs

Surgical Site Infection (SSI)
Surgical site infection (SSI) is infection at the site of an operation either at the site of incision or in the organ or body cavity that are manipulated during operation.


Classification
1. Incisional SSI
2. Organ / Space SSI

Classification1. Incisional SSI i) Superficial incisional
SSI: only the skin or subcutaneous tissue of the incision
ii) Deep incisional SSI : deep tissues (i.e.
fascial and muscle layers)
2. Organ / Space SSI : involving any part of the
anatomy(i.e.organ/space), other than the incision, opened or manipulated during the surgical procedure

Wound infection
The infection of a wound can be defined as the invasion of organisms through tissues following a breakdown of local and systemic host defences, leading to cellulitis, lymphangitis, abscess and bacteraemia

A major SSI or major wound infection is defined as a wound that either discharges significant quantities of pus spontaneously or needs a secondary procedure to drain it.
The patient may have systemic signs such as tachycardia, pyrexia and a raised white count or delay in return home

Minor wound infections may discharge pus or infected serous fluid but should not be associated with excessive discomfort, systemic signs or delay in return home

Factors that determine whether a wound will becomeinfected or not
1. Host response2. Virulence and inoculum of infective agent3. Vascularity and health of tissue being
invaded (local ischaemia as well as systemic shock)
4. Presence of dead or foreign tissue5. Presence of antibiotics during the ‘decisive
period’

Risk factors for increased risk of wound infection
1. Malnutrition i) obesity ii) weight loss
2. Metabolic disease i) Diabetes ii) Uraemia iii) Jaundice
3.Immunosuppression i) Cancer ii) AIDS iii) Steroids iv) Chemotherapy
v) Radiotherapy4. Colonisation and
translocation in the gastrointestinal tract

Risk factors for increased risk of wound infection(Cont’)
5. Poor perfusion i) Systemic shock ii) Local ischaemia6. Foreign body /material7.Poor surgical technique 8. i) Dead space ii) Haematoma

Nosocomial infection
•Acquired infection originating in a patient while in a hospital or other health care facility is known as nosocomial infection. Also known as health care-associated infection (HAI) or Hospital Acquired Infection (HAI).

Nosocomial infection (Cont’)
There are four main groups: •Respiratory infections (including ventilator-associated pneumonia) •Urinary tract infections (mostly related to urinary catheters) •Bacteraemia (mostly related to indwelling vascular catheters) •SSIs

Nosocomial infection (cont’)
Source of infection1. Hospital personnel2. Operation theatre & ward A) Exogenous source
3. Patient ----------- B) Endogenous source

Prevention of Nosocomial infection
A) Reducing the sources of pathogens: B) Restricting the transmission: C) Protection of susceptible patients by
isolation in a side room

A) Reducing the sources of pathogens:
1. Detection of carriers, their isolation and treatment.2. Hospital staff those who are suffering from skin
disease/sore throat/diarrhoea/dysentery should be kept away from work until completely cured.
3. Barrier nursing4. Task nursinng

B) Restricting the transmission:
1. Hand washing 2. Adoption of effective aseptic techniques3. Adoption of proper sterilization and
disinfection procedures4. Droplet infection control by use of face
masks, spacing, prevention of overcrowding ,ensuring ventilation etc.
5. Dust control

C) Protection of susceptible patients by isolation in a side room

More common in:
•Diabetics•Immunosuppressed pt•Patient on steroid therapy•Patient on life supporting machine•Instrumentation•Pt on artificial prosthesis

Organisms:
•Hospital acquired wound infection: S. Aureus is the commonest
Others-Pseudomonas, Klebsiella, E. coli, Proteus.
•Hospital acquired respiratory tract infection: S. Pneumoniae, Haemophilus, Herpes, Varicella, Aspergillus, Pneumocystis carini
•Hospital acquired urinary tract infection: Klebsiella is the commonest

Management:
•Antibiotics.•Isolation•Blood, urine, pus for C/S•Blood transfusion, Plasma or albumin therapy•Ventilator support

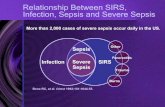
SIRS:
•Systemic inflammatory response syndrome is the body’s systemic response to infection or inflammation characterized by any two of :• Hyperthermia (> 38°C) or hypothermia (< 36°C)• Tachycardia (> 90/ min, no β-blockers) or tachypnoea (> 20/
min)•White cell count > 12 x 109 or < 4 x 109

Cause:
• Infection• Multiple trauma• Burn• Pancreatitis

Pathogenesis:
• Primary insult ( infection, trauma or surgery, burn,pancreatitis)
• Compounding insult• Hypoxia• Hypovolumia• Nosocomial infection• Bacterial and endotoxin leakage from GIT• Malnutrition• Hyperthermia• Hyperglycaemia

SIRS
• Increased cytokine production• Failure to localize cytokines• Abnormal NO production • Contact, coagulation and complement activation• Abnormal arachidonic acid metabolism• Neutrophil sequestration and degranulation• Free radical production

Sepsis
• Sepsis is defined as the systemic manifestation of SIRS, with a documented infection

Severe sepsis or sepsis syndrome
• is sepsis with evidence of one or more organ failures• [Respiratory (acute respiratory distress syndrome), • Cardiovascular (septic shock follows compromise of cardiac function and fall in
peripheral vascular resistance),• Renal (usually acute tubular necrosis),• Hepatic, • blood coagulation systems or central nervous system]

MODS :
• Multiple organ dysfunction syndrome is defined as tissue damage in organs distal to the origin of original injury, is the clinical manifestation of systemic inflammatory response syndrome.

Pathogenesis:
• Primary insult • Compounding insult
• SIRS • MODS

MODS
• cellular dysoxia (i.e. dysfunctional mitochodria)• microvascular occlusion or shunting• tissue hypoxia• cellular dysfunction and or death .

Management:
• Primary insult --------------------- unavoidable• Compounding insult ------------------- preventable or treatable.• SIRS --------------------------------------- manageable• MODS is fatal

Multiple system organ failure (MSOF)
• Multiple system organ failure (MSOF) is the end-stage of uncontrolled MODS.