Health Expenditures, Longevity, and Growth by Dormont, Martins, Pelgrin, Suhrcke
Upload
tim-millerCategory
view
213download
0
LONGEVITY AND MEDICARE EXPENDITURES 215
Demography, Volume 38-Number 2, May 2001: 215–226 215
INCREASING LONGEVITY AND MEDICARE EXPENDITURES*
TIM MILLER
In official Medicare forecasts, the baby boom is a majorforce behind exploding program costs. The retirement of babyboomers during the next few decades will lead to very largeincreases in the number of Medicare enrollees. In addition, en-rollees are increasingly likely to live to advanced ages. OlderMedicare enrollees typically use more health care than youngerenrolles and are more expensive; therefore increasing longevityis viewed as causing an increase in Medicare costs.
To forecast the health costs of the Medicare population,one must predict both the number of enrollees and their healthstatus as reflected in average costs. Defining health status, notto mention predicting it, is a daunting task. One could definehealth status by indicators of disability or specific disease con-ditions. The Trustees, however, chose a simple demographicindicator, namely age. This parsimony is an important featureof their model, which is worth preserving. Age, however, doesnot adequately indicate the health status of an elderly popula-tion, and it is a poor basis for predicting the future.
In line with the arguments of Lubitz and Prihoba (1984),Fuchs (1984), and Lee (1994), I suggest an alternative de-mographic indicator of health status: time until death. Aver-age medical costs rise both with age and with time untildeath. In fact, the main reason why Medicare costs increasewith age is that older individuals as a group are closer todeath than younger individuals. From a cohort perspective,increases in longevity may be expected to lead to postpone-ment of these costs of the final decade and final year of life.From a period perspective, declines in age-specific mortalitymay be expected to lead to declines in age-specific costs be-cause declining mortality reduces the proportion of high-costusers (those near death).
In this paper I compare these two approaches to forecast-ing Medicare costs: one is based on a fixed age schedule ofcosts (similar to the Trustees’ current methodology), and theother on a fixed time-until-death schedule. These accountingmodels assume quite different views about the future healthstatus of the elderly. I report alternative projections of Medi-care expenditures and taxes. The time-until-death modelyields significantly lower cost forecasts than the Trustees’current methodology, especially in the face of more rapidgains in longevity such as those in the recent Census Bureauprojection. Yet the hypothetical cost savings from improvedhealth (declining death rates) is small relative to the size ofthe Medicare solvency problem caused by population aging.
FINANCING MEDICARE
The Medicare program reimburses Medicare enrollees forhealth care expenditures related mainly to hospital stays (the
Official Medicare projections forecast that the elderly popula-tion will be less healthy and more costly over the next century. Thisprediction stems from the use of age as an indicator of health sta-tus: increases in longevity are assumed to increase demand forhealth care as individuals survive to older and higher-use ages. Inthis paper I suggest an alternative approach, in which time untildeath replaces age as the demographic indicator of health status.Increases in longevity are assumed to postpone the higher Medicareuse and costs associated with the final decade of life. I contrast thetwo approaches, using mortality forecasts consistent with recentprojections from the U.S. Census Bureau and the Social SecurityAdministration. The time-until-death method yields significantlylower-cost forecasts. The hypothetical cost savings from improvedhealth are small, however, relative to the size of the Medicare sol-vency problem caused by population aging.
ver the next few decades, the United States will undergoa large demographic transformation introduced by the retire-ment of the baby boomers and the possibility of dramatic in-creases in their longevity. How will this affect the future ofMedicare, the federal government’s health insurance programfor the elderly?
The Medicare Trustees1 have the difficult task of as-sessing the finances of Medicare for the next few years anduntil 2075. Such long-run forecasting may seem a futile ex-ercise because we are uncertain about the number of Medi-care enrollees, their use of health care, the cost of such care,and the technologies that will be available near the end ofthis century. These kinds of modeling exercises, however,help us to distinguish between probable and improbablescenarios among an infinite number of imaginable futures.Modeling also forces us to examine our fundamental as-sumptions. In this paper I focus on one such assumption:the relationship between increases in longevity and futurehealth care costs.
O
*Tim Miller, Center for the Economics and Demography of Aging, Uni-versity of California at Berkeley, 2232 Piedmont Avenue, Berkeley, CA94720; E-mail: [email protected]. Research for this paper wasfunded by Grant R37-AG11761 from the NIA. An earlier version was pre-sented at the 1998 annual meetings of the Population Association ofAmerica, held in Chicago. Helpful suggestions were given by Ronald Lee,James Lubitz, reviewers at this journal, and participants at the PAA and atUC Berkeley’s Demography Brownbag Series. The model and data pre-sented here are available at http://www.demog.berkeley.edu/~tmiller.
1. The Health Care Financing Administration (HCFA) is the federalagency that administers Medicare. The Office of the Actuary in the HCFA,under the direction of the Board of Trustees, prepares Medicare’s annualforecasts. Throughout the paper I refer to methods and decisions as those ofthe Medicare Trustees, although actually they are those of the HCFA and theOffice of the Actuary.

216 DEMOGRAPHY, VOLUME 38-NUMBER 2, MAY 2001
Hospital Insurance or HI program) and physicians’ charges(the Supplementary Medical Insurance or SMI program). In1999, reimbursements totaled $213 billion or 12% of the fed-eral budget, making Medicare one of the largest federal gov-ernment programs. It is also one of the fastest-growing fed-eral programs, averaging 5% real annual growth over the lastdecade (U.S. Office of Management and the Budget 2000).The Trustees predict that by mid-century the Medicare pay-ments received by the elderly will be almost as great as theirSocial Security retirement benefits: the Medicare program isprojected to be 4.8% of the gross domestic product (GDP),and the Social Security retirement program (OASI) to be5.7% of the GDP (Board of Trustees, Federal Hospital Insur-ance Trust Fund 2000).
Because Medicare, like Social Security, is financed as apay-as-you-go system, it is convenient to construct periodmeasures of the annual finances. Let T represent aggregatetaxes collected and H represent aggregate expenditures. Wecan express these aggregates in terms of average earningsand health costs:
T = W × y × z,
where W is the working-age population, y is per capita earn-ings, and z is the Medicare tax rate. For ease of exposition, Iassume that all revenue derives from payroll taxes.2
H = E × h,
where E is the number of enrollees and h is the averageMedicare cost per enrollee.
We can solve for the Medicare tax rate by assuming thataggregate expenditures equal aggregate taxes:
z = [E / W] × [h / y].
We can use this simple formula to understand the broad out-lines of Medicare’s future financial difficulties. In 1999 therewas about one Medicare enrollee for every four workers, andannual expenditures per enrollee ($5,400) were about 18%of the average annual wage ($30,200). Thus, in a balancedsystem, Medicare taxes would stand at about 4.5% of payroll[0.045 = 0.25 × 0.18]. In 2075, Medicare taxes would be12.5%, nearly triple the 1999 level. This increase is duemainly to the effect of population aging: projections showabout one enrollee for every two workers in 2075, twice the1999 level. In addition, costs per enrollee are projected to beabout 24% of the average annual wage, 1.33 times the 1999level (Board of Trustees, Federal Hospital Insurance TrustFund 2000).
The rapid increase in health costs per enrollee is due topredicted increases in both the price and the use of medicaltechnology. During the initial 25 years of the Trustees’ projec-tion, the cost per unit of medical care is assumed to rise muchfaster than workers’ wages. Future cost containment policies
are assumed to rein in this growth. During the last 50 years ofthe Trustees’ projection, costs per unit of care are projected toincrease at the rate of productivity growth in the case of HI(Medicare reimbursement to hospitals), and at the rate of GDPgrowth in the case of SMI (Medicare reimbursement to physi-cians) (Board of Trustees, Federal Hospital Insurance TrustFund 2000; Board of Trustees, Supplementary Medical Insur-ance Trust Fund). Thus changes in demography are assumed tobe the only forces affecting Medicare costs beyond 25 years.
In addition to rising prices, the Trustees predict increas-ing Medicare HI use per enrollee. As noted earlier, the Trust-ees implicitly estimate the future health status of the Medi-care population on the basis of age. The aging of the Medi-care population leads to a predicted increase in Medicare use,at least in regard to HI. SMI does not appear to be forecaston the basis of age (White 1999). In addition, a growing pro-portion of Medicare users are enrolled in HMOs, for whichMedicare reimbursement is set in part by age.
HEALTH STATUS AS MEASURED BY TIME UNTILDEATH
As a basis for projecting costs, we must estimate how Medi-care expenditures vary by health status. Lubitz, Beebe, andBaker (1995) provide one set of estimates. The data aredrawn from the Continuous Medicare History Sample, whichcontains Medicare administrative data on a 5% randomsample of Medicare enrollees. From this sample they se-lected all persons 65 and older who died in 1989 or 1990.They excluded persons with end-stage renal disease, personsenrolled in HMOs, disabled persons under age 65, and per-sons not continuously covered by Medicare Hospital Insur-ance (HI) and Supplementary Medical Insurance (SMI).
The sample consists of 129,166 persons who died in1989 or 1990. For each person, the administrative data con-tain payment claims submitted to Medicare by physicians,hospitals, and other providers. The administrative records inthe sample date back only to 1974; therefore complete life-time cost histories are available only for those who died be-tween ages 65 and 81. For those who died at older ages, costdata for the earlier years are missing. As discussed below,however, Medicare costs are quite low for beneficiaries whoare many years away from death; therefore these missingdata are not vital for my estimation.
Lubitz et al. (1995) classified Medicare costs3 by twomeasures of health status: age and time until death. Table 1
2. In 1999, 57% of Medicare revenue was derived from payroll taxes.Other sources included general federal revenue (25%), premiums from en-rollees (8%), taxes on Social Security benefits (3%), and interest and othersources (7%) (Board of Trustees, Federal Hospital Insurance Trust Fund 2000;Board of Trustees, Supplementary Medical Insurance Trust Fund 2000).
3. The administrative records for beneficiaries report Medicare reim-bursements in current dollars for each year. Between 1974 and 1980, bothinflation and increases in the real volume of Medicare services led to largeincreases in Medicare spending. Therefore the retrospective cost historieswould show dramatic increases in costs in the final years of life. These couldbe attributed to period effects such as inflation and expansion of the Medi-care program. In an attempt to remove these effects, Lubitz et al. (1995)converted current dollar costs in year x to 1990 dollars, using the rate ofgrowth in per beneficiary Medicare costs between year x and 1990. In otherwords, an individual’s retrospective Medicare costs are measured in rela-tion to the average cost of beneficiaries in that year. These relative coststhen are converted to 1990 dollars by multiplying by the average cost ofbeneficiaries in 1990. Cost in 1990 dollars = cost in year x • (per capita costin 1990/per capita cost in year x).

LONGEVITY AND MEDICARE EXPENDITURES 217
and Riley (1993) provide empirical evidence that Medicarecosts of decedents relative to those of survivors remainedconstant over the period of their study (1976–1988). Garber,MaCurdy, and McClellan (1998), using Medicare data from1988–1995, find that relative spending on decedents did notchange over that period. They found shifts in the composi-tion of spending on decedents, however: declines in acutecare were offset by increases in hospice and home healthcare. These two studies are encouraging. Despite changesover the last two decades in medical technology, in the Medi-care program itself, and in the characteristics of Medicareenrollees (age and disability), time until death has remaineda consistent indicator of costs.
DELAY IN MORBIDITY
In its projection, the time-until-death model uses a fixedtime-until-death schedule of health costs. In this model I as-sume that increases in longevity will postpone the period ofhigh health costs and (by implication) of morbidity, whichhave characterized the final decade of life. This assumptionof delay in morbidity stands in contrast to the “compressionof morbidity” hypothesis proposed by Fries (1980, 1984).Considering the possibility of continued medical advancesin the face of a fixed life span, Fries proposed that “the pe-riod of infirmity may be compressed into a shorter periodtoward the end of life” (1984:354). A more pessimistic vi-sion holds that medical advances may be more successful inprolonging life than in postponing morbidity, leading to anexpansion of morbidity (Olshansky et al. 1991). The time-until-death model, with its assumption of a delay in morbid-ity, represents a middle path between potentially large costincreases due to an expansion of morbidity (implied by theTrustees’ model) and potentially large cost savings due to acompression of morbidity.
Research on trends in active or disability-free life ex-pectancy provides mixed evidence on the assumption of de-lay in morbidity. Crimmins, Saito, and Ingegneri (1997) ex-
presents my calculations of average Medicare costs for sev-eral illustrative ages by time until death. For example, wesee that annual Medicare costs for persons age 75 who werenine years away from death (that is, who would die at age84) were about $1,900. This amount does not vary much byage: costs are similar for persons age 85 who were also nineyears away from death (about $2,200). Costs rise in the finaldecade of life, however, and especially in the last years. Forpersons age 75 who were five years away from death, annualcosts were $3,000; for those in the final year of life, annualcosts were $13,500. Generally, Medicare costs were associ-ated very strongly with time until death and weakly with age.Using data on the age distribution of decedents in 1990, Ihave summarized the cost data by time until death in the fi-nal columns of Table 1.
The correlation between age and Medicare costs appearsto be explained largely by time until death. Therefore age isa poor measure of health status and cannot be used reliablyas a basis for forecasting. In the alternative forecasts Ipresent here, time until death is used as a measure of healthstatus; hence increases in longevity delay both death and thehigh costs associated with the final decade of life, especiallythe final years of life.
It is also evident from the first row of the table that thecosts of the final year of life seem to decline with age. Forexample, those dying at age 75 incurred costs of $13,500,while those dying at age 95 incurred costs of $7,000. De-clines in the costs of the final year of life at advanced agesmight be attributed either to age-based health care rationing(older patients treated less aggressively than younger pa-tients) or to frailty. Neither is likely to persist at current lev-els in the future. For this reason, a forecasting model usingboth age and time until death would be likely to understatefuture costs.
In the time-until-death model I use a fixed time-until-death schedule of health costs for projection. There is someevidence that this schedule has been stable over time. Lubitz
TABLE 1. ANNUAL MEDICARE COSTS PER ENROLLEE BY YEARS BEFORE DEATH
Age_________________________________________________________________________________________
Years Before Death 75 85 95 65+ 65+ (Relative Costs)
0 $13,500 $10,700 $7,000 $11,100 6.94
1 $8,600 $6,900 $4,900 $7,000 4.38
2 $5,100 $4,600 $3,700 $4,500 2.81
3 $4,200 $4,000 $3,200 $3,800 2.38
4 $3,400 $3,600 $3,300 $3,400 2.13
5 $3,000 $3,300 $3,000 $3,100 1.94
6 $3,000 $2,800 $2,800 $2,800 1.75
7 $2,400 $2,800 $2,500 $2,500 1.56
8 $2,400 $2,500 $2,400 $2,300 1.44
9 $1,900 $2,200 $2,100 $2,200 1.38
10 or More –– $1,700 $1,800 $1,600 1.00
Source: Author’s calculation based on data from Lubitz, Beebe, and Baker (1995).

218 DEMOGRAPHY, VOLUME 38-NUMBER 2, MAY 2001
offset by cost savings due to decline in disability. By con-trast, the time-until-death model links costs with mortalityrather than with disability; therefore costs can be postponedbut never eliminated.
Further research into multiple measures of health sta-tus, which include age, time until death, disability status,and specific disease conditions, is certainly warranted. A re-cent analysis by Cutler and Meara (1999) shows that dis-ability and time until death exert independent effects oncosts, and together explain most of the variation by age.Consideration of other population characteristics would leadto richer, more descriptive models, which also might lead tomore accurate forecasts of health costs. Yet there is consid-erable uncertainty in forecasting both the size and the healthcosts of numerous classification groups well into thetwenty-first century, when the disease frontier will haveshifted to numerous new diseases and new definitions ofdisabilities. In comparison, demographic indicators such asage and time until death are easily identifiable and can bepredicted reliably. In the sections that follow, I contrast twoforecast models: one uses a fixed age schedule of costs, im-plying an expansion of morbidity; the other uses a fixedtime-until-death schedule of costs, implying a delay in mor-bidity.
PROJECTIONS BASED ON COSTS BY AGE
Because a complete accounting of the Trustees’ forecastingmodel is not publicly available, I present a simple age model,
amined trends in the United States from 1970 to 1990. Mor-bidity expanded in the 1970s: the expected number of yearsdisabled after age 65 increased by one year for both menand women. By contrast, the evidence from the 1980s sup-ports the “delay in morbidity” hypothesis, with very slightchanges in the expected years disabled in the community(an increase of 0.2 year for males and a decrease of 0.1 yearfor females) and no change in the expected number of yearsspent institutionalized. Evidence on changes in active lifeexpectancy in France during the 1980s shows no expansionof morbidity. Robine, Mormiche, and Sermet (1998) founda large (2.5-year) increase in life expectancy at birth from1981 to 1991. There was no change in the expected yearswith a severe disability for women, but men showed a de-cline of 0.3 year (from 1.5 to 1.2 years). The expected num-ber of years with moderate disability declined slightly overthe period (by 0.1 year for women and 0.2 year from men).
Singer and Manton (1998) suggested an alternative tothese demographic measures of health status, namely dis-ability rates. Manton, Corder, and Stallard (1997) havedocumented a rapid decline in disability rates among theelderly. On the assumption that Medicare costs are corre-lated strongly with disability, these declines imply substan-tial cost savings. If the rate declines documented for the pe-riod 1982–1994 persist into the future, Singer and Mantonpredicted that the disability-adjusted support ratio in 2070would be unchanged from its 1994 level. The large cost in-creases generated by population aging would be entirely
A
Dol
lars
20 40 60 80
0
2,000
4,000
6,000
Taxes
Benefits
20 40 60 80
6,000
4,000
2,000
0
Age
Do
lla
rs
Taxes
Benefits
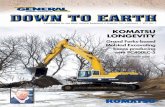
FIGURE 1. AVERAGE MEDICARE TAXES AND BENEFITS BY AGE IN 1997
Sources: Taxes estimated form Current Population Survey. Benefits estimated from Medicare’s New Beneficiary Follow-Up Survey.
Note: Premium contributions are not shown.

LONGEVITY AND MEDICARE EXPENDITURES 219
which highlights a central feature of their methodology. Thisis an approximation of the more complex methodology em-ployed by the Trustees. The distinctive age patterns of Medi-care taxes and benefits are shown in Figure 1. In the agemodel, to estimate aggregate taxes and benefits in any futureyear, I multiply the age profiles shown in this figure by popu-lation forecasts.
The age model projects aggregate taxes for t years in thefuture as
T t z t e y K tvt( ) ( ) ( ) ( , )= × × ×�
=� �
� 20
64
,
where z(t) is the Medicare tax rate, v is the rate of productiv-ity growth in the economy, y(a) is the average wage of thoseage a in 1997, and K(a, t) is the population age a in year1997 + t.
Aggregate costs are projected as
H t e h K tit( ) ( ) ( , )= × � ×
=� �
� 65
120
,
where i is the rate of medical care inflation in the economy,h(a) is the average Medicare cost of those age a in 1997, andK(a, t) is the population age a in year 1997 + t.
For a � 65, let K(a, t) = E(t) × k(a, t), where E(t) is thenumber of enrollees (defined here as the population over age
65), and k(a, t) is the proportional age distribution of enroll-ees in year 1997 + t. Then we can express aggregate benefitpayments as
H t e E t h k tit( ) ( ) ( ) ( , )= × × � ×
=� �
� 65
120
.
Here we see that total Medicare expenditures are decom-posed into three multiplicative factors: a general price-levelfactor, the number of enrollees, and the average cost per en-rollee. This average cost is the sum of the product of the ageprofiles of health care use and the age distribution of theenrollees.
The impact of the baby boomers on average costs is evi-dent in Figure 2. The solid line shows the average age ofMedicare enrollees (on the left-hand axis); the dotted lineshows the average costs per enrollee (on the right-hand axis)based on the age model outlined above. When the babyboomers begin to retire, they enter the Medicare system asrelatively inexpensive enrollees and drive average costsdownward. As they age, they become more expensive (trav-eling along the h(a) curve of Figure 1) and cause averagecosts per enrollee to rise.
For ease of exposition, I have not modeled changes inproductivity or in the price of medical care. I have assumedthat v and i in the age model are both zero over the entire
Date
Age
in Y
ears
(So
lid L
ine)
2000 2020 2040 2060
74.0
74.5
75.0
75.5
76.0
76.5
5,600
5,800
6,000
6,200
6,400
Predicted A
verage Cost R
eflecting Only C
hanges in Health
Status (Dotted L
ine)
FIGURE 2. AVERAGE AGE AND PREDICTED AVERAGE COSTS OF MEDICARE ENROLLEES

220 DEMOGRAPHY, VOLUME 38-NUMBER 2, MAY 2001
projection period. Hence, in these simulations, increases inenrollees’ average costs will be due only to demographiccauses (including changes in the health status of the elderly)throughout the 75-year projection period (as they are in thelast 50 years of the Trustees’ model).
How well has the simple age model captured the es-sence of the Trustees’ methodology? The age model uses in-puts similar to those employed by the Trustees in their 1997report: mortality forecasts with life expectancy at birth in-creasing by nearly five years to 80.85 years in 2070 (basedon life tables constructed by the Office of the Actuary of theSocial Security Administration), immigration forecasts(900,000 net annual immigrants), fertility forecasts (declin-ing from a current level of 2.02 to a long-run average of1.9), and an age profile of Medicare costs based on the agefactors used by Medicare for cost reimbursements of HMOson the basis of their patient population. The latter profile(see Table 2) is meant to approximate the use of age in theTrustees’ estimate of future HI costs. I also use the age pro-file of hospital discharges from 1995; the resulting cost pat-terns are quite similar.
The estimates from the age model are quite similar tothose of the Trustees, as seen in Figure 3. Panel A contrastspredictions of the annual growth rate in Medicare costs;panel B contrasts predictions of the growth rate in the num-ber of enrollees; panel C contrasts predictions of the growthrate in the costs per enrollee. In the initial decades, the agemodel consistently underestimates the growth rates in enroll-ees and average costs as forecast by the Trustees. Presum-ably this result is due to short-term effects not captured bythe age model. After 2020, however, the age model generallytracks the Trustees’ forecast.
PROJECTIONS USING COSTS BY TIME UNTILDEATH
Of course no individual’s death date can be known with anycertainty, but demographers can predict the distribution oftime until death in a population. The cohort life table value ofe(�) is the mean time until death for a group of individuals ofage �. The value of 1q� is the proportion of individuals at age� that will die this year. The entire distribution of time untildeath {� = 0 to � = �} is given by the distribution of deaths
� years in the future to those currently of age �. In life tablenotation, the time-until-death distribution for individuals ofage � is
l(� + �) × �(� + �) / l(�) for � = 0,…,�,
where l(x) is the proportion of a cohort surviving to exactage x and u(x) is the force of mortality at exact age x.
The time series of the time-until-death distribution is es-timated on the basis of forecasts of future U.S. mortalityrates. The forecast is taken from the Office of the Actuary,Social Security Administration. This mortality forecast wasused in the 1995 Trustees’ Reports in forecasting the Medi-care system’s finances.4
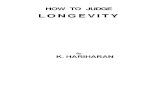
Figure 4 shows the effect of increasing longevity on thetime-until-death distribution for those age 65 in 1937, 1997,and 2057. The distribution is shifting outward over time be-cause of a decline in mortality (historical and forecast). In1937 the life expectancy at age 65 was 12.5 years; by 1997 ithad risen to 17.5 years; and by 2057 it is predicted to reach19.9 years. This improvement in health status means that av-erage Medicare use by persons age 65 will decline over time.
The aggregate cost estimate from a time-until-deathmodel would be
H t e h K tit( ) ( ) ( , )= � × ×
�� �
= × × ×�e E t k t hit ( ) ( , ) ( )� �
�,
where i is the rate of medical care inflation in the economy,h(�) is the average Medicare costs of those � years beforedeath in the baseline year, K(�,t) is the population � yearsbefore death t years in the future, E(t) is the number of en-rollees, and k(�,t) is the percentage distribution of the en-rollee population by time until death in t years in the future.
The time-until-death model implies a very different timepath of average costs per enrollee than does the age model.The solid line in Figure 5 shows the average time until deathof Medicare enrollees (on the left-hand axis) over the pro-jection period. In 1997 the average Medicare enrollee wasexpected to live another 11.2 years. Over time, the Medicarepopulation moves further away from death and from the costsassociated with being close to death. The dashed line showsthe decline in average costs per enrollee (on the right-handaxis) implied by shifts in the time-until-death distribution.This distribution is changing because of both increasing lon-gevity and the aging of the baby boomers.
COMPARISON OF COST PROJECTIONS
Figure 6 contrasts aggregate Medicare costs estimated bythe age model and by the time-until-death model. Bothmodels use the conservative longevity forecast by the Trust-ees: an increase in life expectancy to 80.9 years in 2070.Cost projections in the age model are 14% higher in 2070than those in the time-until-death model. Even at the rela-
TABLE 2. MEDICARE COSTS BY AGE
Age Risk Adjuster (Sexes Combined) Relative Costs
65–69 0.49 1.00
70–74 0.64 1.30
75–79 0.81 1.65
80–84 0.98 1.98
85–89 1.15 2.33
90–94 1.22 2.47
95+ 1.18 2.38
Source: Health Care Financing Administration, Risk Factor Tables,Announcement of Calendar Year 2000 Medicare + Choice Payment Rates,March 1, 1999.
4. I obtained the data on-line from the Berkeley Mortality Database(http://demog.berkeley.edu/wilmoth/mortality). These data are not correctedfor possible age misreporting.

LONGEVITY AND MEDICARE EXPENDITURES 221
Gro
wth
Rate
(%
)
0
1
2
3
4
5
A. Annual Rate of Increase in Medicare Costs
Gro
wth
Rate
(%
)
0
1
2
3
4
B. Rate of Increase in Enrollees
Gro
wth
Rate
(%
)
-1
0
1
2
3
4
C. Rate of Increase in Average Cost per Enrollee Due to Age/Sex Composition of Enrollees
Trustees’ ModelAge Model
Trustees’ ModelAge Model
Trustees’ ModelAge Model
2000 2020 2040 2060
Date
2000 2020 2040 2060
Date
2000 2020 2040 2060
Date
5
4
3
2
1
0
4
3
2
1
0
4
3
2
1
0
–1
FIGURE 3. RATES OF INCREASE
Note: Model is run on the assumption that medical prices rise at the rate of general inflation.

222 DEMOGRAPHY, VOLUME 38-NUMBER 2, MAY 2001
Time Until Death
Per
cen
tag
e
0 10 20 30 40 50
0
1
2
3
4
193719972057
19371997
2057
tively modest gains in life expectancy forecast by the Trust-ees, we find significant differences in cost estimates be-tween these models.
To recognize that the cost savings from declines in age-specific mortality rates can be in the range of 14%, as indi-cated by the simulations, consider the following analytic ap-proximation. Between 1997 and 2070, the life expectancy ofpersons age 65 is expected to increase by three years, from17.65 to 20.65 (Berkeley Mortality Database 2000). In theTrustees’ view, the three years gained in life expectancy arequite costly: they occur in the 80+ age range, where coststypically are 40% higher than for the average enrollee. In thealternative view, the three years gained in life expectancy arequite inexpensive: they occur in the relatively low-cost yearswell before the end of life, where costs typically are 70%lower than for the average enrollee. Using these rough esti-mates, we can see that the Medicare Trustees would over-state costs by about 17% [1.17 = (17.65 + 3 × 1.40) / (17.65+ 3 × .30)].
To assess the impact of increasing longevity on Medi-care financing, I ran three simulations of alternative mortal-ity forecasts, using the age model and the time-until-deathmodel. Lee and Carter (1992) developed a method for mod-eling and forecasting mortality rates based on a single, time-varying parameter: the general mortality level index. I use
Lee-Carter methods to derive alternative time series of thisindex, which yield mortality rates and the time-until-deathdistributions. The baseline forecast uses Lee and Carter’soriginal forecast of the mortality level index, based on theirestimate of the historical trend in this index. Life expectancyat birth is predicted to reach 86.6 in 2070; this figure is quitesimilar to the middle forecast of the most recent Census Bu-reau projections (Hollmann, Mulder, and Kallan 2000). Thesecond forecast assumes that mortality declines half as fastas predicted by Lee and Carter (1992). It roughly approxi-mates the middle forecast from the Trustees, in which e(0)reaches 82.0 in 2070. The third forecast assumes that mor-tality declines twice as fast as in Lee and Carter’s originalforecast (that is, the general mortality level index falls twiceas fast as originally predicted), with e(0) reaching 93.5 in2070.5
FIGURE 4. TIME-UNTIL-DEATH DISTRIBUTION FOR PERSONS AGE 65: 1937, 1997, AND 2057
5. The estimate of a life expectancy of 93.5 in 2070 may strike some asimplausibly high. Such an increase implies declines in age-specific mortal-ity of 2.3% per year for persons age 80–84, 2.0% for those age 85–89, and1.7% for those age 90–94. These rates of decline are certainly rapid but notunprecedented. Kannisto et al. (1994) examined evidence on the rates ofdecline in age-specific mortality for the elderly populations in 27 countries.Observed rates of decline from the 1960s to 1980s in female age-specificmortality in Japan [80–84, 85–89, 90–94], Finland [80–84, 85–89, 90–94],and Iceland [85–89, 90–94] all exceed these predicted rates of decline.

LONGEVITY AND MEDICARE EXPENDITURES 223
The results of the three simulations are presented in Fig-ure 7, which shows changes in Medicare taxes as a percent-age of payroll. Rising Medicare costs will greatly outstriprevenues from taxes and premiums; I express this shortfallin terms of changes in the tax rate. This is merely a conve-nience because future shortfalls also could be met by increas-ing premiums or reducing benefits. Premiums are assumedto equal 25% of SMI (physician reimbursements) as estab-lished by the Balanced Budget Act of 1997. Recall that forease of exposition, all simulations assume that medical careinflation and productivity growth rate equal zero.
This graph is the central result of the paper and revealsthree key findings. First, Medicare tax rates do not changemuch over the next 15 years. In these simulations, medicalprices are assumed to be rising at the rate of general infla-tion so that only changes in demography affect Medicare.These results indicate that any short-term financial crisis fac-ing Medicare does not stem from demographics. The effectsof the baby boomers’ retirement are seen in the steady rise intax rates, beginning in about 2015.
Second, we note a large variation in tax rates predictedby the age model for the three longevity forecasts. Tax ratesin 2070 vary from a low of 12%, assuming a moderate in-crease in longevity [e(0) = 82.0], to a high of 19%, assuming
a more rapid increase in longevity [e(0) = 93.5]. By contrast,the time-until-death model shows relatively moderate differ-ences in tax rates: 10 to 12%. Under the moderate increasesin longevity forecast by the Trustees, cost projections basedon age would exceed by about 15% the projections based ontime until death. Under more rapid increases in longevity,cost projections based on age would greatly exceed thosebased on time until death: by 32% with e(0) = 86.6 in 2075and by 57% with e(0) = 93.5.
To see that the modest tax increases forecast by the time-until-death model are consistent with rapid increases in lon-gevity, we can return to the simplified analytical calculations(considered above). Currently the average 65-year-old canexpect to live another 17.6 years. According to official esti-mates, by 2070 the average 65-year-old can expect to live20.6 years. This gain of three years, or a 16% increase in theaverage life span over 65, would raise lifetime costs by amodest 5.6%, on the assumption that costs of persons morethan 10 years away from death are about one-third the costsof the average enrollee [5% = 3 × .33 / 17.65]. Even a dra-matic doubling of the life span over 65 would raise lifetimecosts by only about one-third.
In addition to comparing the tax estimates for 2070, wecan summarize the tax differences over the entire 75-year
Date
Average T
ime U
nti
l D
eath
in
Years
(Soli
d L
ine)
2000 2020 2040 2060
11.2
11.4
11.6
11.8
12.0
12.2
12.4
12.6
5,600
5,800
6,000
6,200
6,400
Pred
icte
d a
verage c
ost
refl
ecti
ng o
nly
ch
an
ges
in h
ealt
h s
tatu
s (D
ott
ed
Lin
e)
Pred
icte
d A
verage C
ost R
efle
ctin
g O
nly
Ch
an
ges in
Health
Sta
tus (D
otte
d L
ine)
FIGURE 5. AVERAGE TIME UNTIL DEATH AND PREDICTED AVERAGE COSTS OF MEDICARE ENROLLEES

224 DEMOGRAPHY, VOLUME 38-NUMBER 2, MAY 2001
Date
Ta
x R
ate
2000 2020 2040 2060
6
8
10
12
14
16
18
20
e(0) = 76.1
86.6
93.5
82.0
86.6
93.5
82.0
Time-Until-Death ModelAge Model
FIGURE 6. ESTIMATE OF AGGREGATE MEDICARE COSTS IN AGE AND TIME-UNTIL-DEATH MODELS
FIGURE 7. EFFECT OF INCREASING LONGEVITY ON MEDICARE TAX RATES
Notes: Model is run on the assumption that medical prices rise at the rate of general inflation. Trustees’ mortality forecast is used.
Date
Bil
lio
ns
of
19
97
Do
lla
rs
2000 2020 2040 2060
200
300
400
500
Time-Until-Death ModelAge Model
e(0) = 76.1 e(0) = 81.7
Age Model
Time-Until-Death Model
500
400
300
200

LONGEVITY AND MEDICARE EXPENDITURES 225
projection period by taking the net present value of taxespaid. I discount by two percentage points over the rate ofproductivity growth (which is assumed to be zero). Usingthe age model, the Trustees would project a $3.8 trillionshortfall in taxes over the next 75 years if longevity in-creased very rapidly (e(0) reaching 93.5 in 2070). By con-trast, the time-until-death model shows a shortfall of $740billion, roughly one-fifth the deficit the Trustees wouldhave forecast.
Third and finally, we see an interesting transitional ef-fect of increasing longevity in the time-until-death modelsimulation. In the short run, the more rapid the increase inlongevity, the lower the health care costs. It is obvious fromcomparative steady-state analysis that health costs will behigher in low-mortality populations: living longer is moreexpensive. Yet there are important transitional effects be-tween steady states. When mortality decreases, the cost sav-ings from declines in age-specific costs occur before the costincreases from the growth in numbers of elderly persons.This occurs because the number of elderly persons at anyage is the cumulative product of past survivorship rates ap-plied to a birth cohort. Thus some time must pass before theelderly population increases as a result of the new survivor-ship rates.
To understand this phenomenon in its most vivid terms,imagine that mortality was suddenly and completely elimi-nated. Medicare decedents, who previously had accountedfor nearly 30% of Medicare costs, would now become survi-vors with significantly lower costs. Hence total costs woulddecline by about 25% in the first year of this zero-mortalityregime. Over time, however, Medicare costs would risesteadily as the number of Medicare enrollees rose to an infi-nite or very large finite number.
CONCLUSION
By relying on a fixed age schedule of Medicare costs, theMedicare Trustees implicitly predicted an expansion of mor-bidity as longevity increases. Their cost projections are quitesensitive to increases in longevity. I presented an alternativeforecast relying on a fixed time-until-death schedule of Medi-care costs. Administrative data have shown that Medicarecosts rise dramatically during the final decade of life. Myforecast assumes that the future is characterized neither by anexpansion nor by a compression of this period of high costsand (by implication) of morbidity, but by postponement tolater in life. The hypothetical cost savings due to delay inmorbidity, however, are not large enough to offset the finan-cial strains projected in Medicare owing to population aging.
REFERENCES
Berkeley Mortality Database. Retrieved February 1, 2000
(www.demog.berkeley.edu).
Board of Trustees, Federal Hospital Insurance Trust Fund. 2000.
2000 Annual Report of the Board of Trustees of the Federal
Hospital Insurance Trust Fund. Washington, DC: U.S. Govern-
ment Printing Office.
Board of Trustees, Federal Supplementary Medical Insurance Trust
Fund. 2000. 2000 Annual Report of the Board of Trustees of the
Federal Supplementary Medical Insurance Trust Fund. Wash-
ington, DC: U.S. Government Printing Office.
Crimmins, E.M., Y. Saito, and D. Ingegneri. 1997. “Trends in Dis-
ability-Free Life Expectancy in the United States, 1970–90.”
Population and Development Review 23:555–72.
Cutler, D.M. and E. Meara. 1999. “The Concentration of Medical
Spending: An Update.” NBER Working Paper 7279, National
Bureau of Economic Research, Cambridge, MA.
Fries, J.F. 1980. “Aging, Natural Death, and the Compression of
Morbidity.” New England Journal of Medicine 303:130–35.
———. 1984. “The Compression of Morbidity: Miscellaneous
Comments About a Theme.” The Gerontologist 24:354–59.
Fuchs, V.R. 1984. “Though Much Is Taken: Reflections on Aging,
Health, and Medical Care.” Milbank Memorial Fund Quarterly
62:143–66.
Garber, A.M., T.E. MaCurdy, and M.L. McClellan. 1998. “Medical
Care at the End of Life: Diseases, Treatment Patterns, and
Costs.” NBER Working Paper 6748, National Bureau of Eco-
nomic Research, Cambridge, MA.
Hollmann, F.W., T.J. Mulder, and J.E. Kallan. 2000. “Methodology
and Assumptions for the Population Projections of the United
States: 1999 to 2100.” Population Division Working Paper 38,
Bureau of the Census, U.S. Department of Commerce, Wash-
ington, DC.
Kannisto, V., J. Lauritsen, A.R. Thatcher, and J.W. Vaupel. 1994.
“Reductions in Mortality at Advanced Ages: Several Decades
of Evidence From 27 Countries.” Population and Development
Review 20:793–810.
Lee, R.D. 1994. “Fertility, Mortality, and Intergenerational Trans-
fers: Comparisons Across Steady States.” Pp. 135–57 in The
Family, the Market, and the State in Ageing Societies, edited by
J. Ermisch and N. Ogawa. Oxford: Oxford University Press.
Lee, R.D. and L. Carter. 1992. “Modeling and Forecasting U.S.
Mortality.” Journal of the American Statistical Association
87:659–71.
Lubitz, J., J. Beebe, and C. Baker. 1995. “Longevity and Medicare
Expenses.” New England Journal of Medicine 332:999–1003.
Lubitz, J. and R. Prihoba. 1984. “The Use of Medicare Services in
the Last Two Years of Life.” Health Care Financing Review
5:117–31.
Lubitz, J. and G. Riley. 1993. “Trends in Medicare Payments in the
Last Year of Life.” New England Journal of Medicine
238:1092–96.
Manton, K., L. Corder, and E. Stallard. 1997. “Chronic Disability
Trends in Elderly United States Populations: 1982–1994.” Pro-
ceedings of the National Academy of Science 94:2593–98.
Olshansky, S.J., M.A. Rudberg, C.K. Cassel, and J.A. Brody. 1991.
“Trading Off Longer Life for Worsening Health: The Expansion
of Morbidity Hypothesis.” Journal of Aging and Health 3:194–
216.
Robine, J.-M., P. Mormiche, and C. Sermet. 1998. “Examination
of the Causes and Mechanisms of the Increase in Disability-Free
Life Expectancy.” Journal of Aging and Health 10:171–91.
Singer, B.H. and K.G. Manton. 1998. “The Effects of Health
Changes on Projections of Health Service Needs for the Elderly
Population of the United States.” Proceedings of the National

226 DEMOGRAPHY, VOLUME 38-NUMBER 2, MAY 2001
Academy of Sciences 95:15618–22.
U.S. Office of Management and the Budget. 2000. Historical
Tables, Budget of the United States Government, Fiscal Year
2001. Washington, DC: U.S. Government Printing Office.
White, J. 1999. “Uses and Abuses of Long-Term Medicare Cost
Estimates.” Health Affairs 18(1):63–79.