INCIDENTAL DIAGNOSTIC OF A RIM-LIKE ADRENAL ......14. Minder WH. Acute adrenal insufficiency in a...
7
INCIDENTAL DIAGNOSTIC OF A RIM-LIKE ADRENAL CALCIFICATION WITHOUT TUBERCULOSIS OR ADRENAL INSUFFICIENCY D. Peretianu, Cristina Daniela Staicu Department of Endocrinology, SCM Povernei, Bucharest, Romania A 75 years old woman was referred to abdominal echography for pain related to biliary- duodenal motriceal dysfunction. The ultrasound discovered a dense (hyperechogenic) image under (posterior of) the 8th segment of the liver. The dense process was supposed to be a calcification situated medial from the right kidney in the cranial 1/3 length of it. Specific clinical and biological data related to possible adrenal destruction were analyzed: the patient was in good condition, body mass index was 29. She had no tuberculosis during her life. The current arterial pressure was 145/80 mm Hg. All laboratory data, including basal cortisol were normal. Cortisolemia at 8 a.m. was 523 nmol/l. The diagnosis was made by CT scan: clear and only organ-disseminated calcification in adrenals appeared as a rim. The management of this case was related to follow-up of adrenal lesions by abdominal ultrasound. The calcification of one adrenal raised several issues for discussion: the role of ultrasound vs CT in adrenal lesions, the prevalence of calcifications in adrenal glands, the importance of the calcification process. Calcifications of adrenals are seldom found in primary autoimmune cortical atrophy associated with Addison's disease, but they are supposed to be more frequent in adrenal tuberculosis; calcification suggests a former local tuberculosis process, associated with pulmonary tuberculosis and with borderline adrenal insufficiency. Various etiologies and mechanisms for adrenal calcifications (infectious, tumor, hemorrhage, parasitic) are discussed. To our knowledge, the rim-like appearance of the adrenal calcification was described only in one patient. In conclusion, incidental diagnostic of adrenal gland calcifications was reported in patients without adrenal insufficiency, signaled by ultrasound and detailed by CT, associated with normal adrenal function. Therefore, we consider that calcifications in the right adrenal in our patient could mean a process of cicatrisation or healing after an autoimmune aggression, only on the right adrenal gland. Key words: adrenal calcification, tumor, Addison, tuberculosis, computed tomography, abdominal ultrasound. 215 Case Report *Correspondence to: D. Peretianu, MD, Department of Endocrinology, SCM Povernei, Bucharest, Romania, 42 Povernei st, tel: + 40-21-312 79 09. Acta Endocrinologica (Buc), vol. III, no. 2, p. 215-221, 2007
Transcript of INCIDENTAL DIAGNOSTIC OF A RIM-LIKE ADRENAL ......14. Minder WH. Acute adrenal insufficiency in a...

INCIDENTAL DIAGNOSTIC OF A RIM-LIKE ADRENALCALCIFICATION WITHOUT TUBERCULOSIS OR ADRENAL
INSUFFICIENCY
D. Peretianu, Cristina Daniela Staicu
Department of Endocrinology, SCM Povernei, Bucharest, Romania
A 75 years old woman was referred to abdominal echography for pain related to biliary-duodenal motriceal dysfunction. The ultrasound discovered a dense (hyperechogenic) imageunder (posterior of) the 8th segment of the liver. The dense process was supposed to be acalcification situated medial from the right kidney in the cranial 1/3 length of it. Specificclinical and biological data related to possible adrenal destruction were analyzed: the patientwas in good condition, body mass index was 29. She had no tuberculosis during her life. Thecurrent arterial pressure was 145/80 mm Hg. All laboratory data, including basal cortisolwere normal. Cortisolemia at 8 a.m. was 523 nmol/l. The diagnosis was made by CT scan:clear and only organ-disseminated calcification in adrenals appeared as a rim. Themanagement of this case was related to follow-up of adrenal lesions by abdominalultrasound.
The calcification of one adrenal raised several issues for discussion: the role ofultrasound vs CT in adrenal lesions, the prevalence of calcifications in adrenal glands, theimportance of the calcification process.
Calcifications of adrenals are seldom found in primary autoimmune cortical atrophyassociated with Addison's disease, but they are supposed to be more frequent in adrenaltuberculosis; calcification suggests a former local tuberculosis process, associated withpulmonary tuberculosis and with borderline adrenal insufficiency. Various etiologies andmechanisms for adrenal calcifications (infectious, tumor, hemorrhage, parasitic) arediscussed. To our knowledge, the rim-like appearance of the adrenal calcification wasdescribed only in one patient.
In conclusion, incidental diagnostic of adrenal gland calcifications was reported inpatients without adrenal insufficiency, signaled by ultrasound and detailed by CT,associated with normal adrenal function. Therefore, we consider that calcifications in theright adrenal in our patient could mean a process of cicatrisation or healing after anautoimmune aggression, only on the right adrenal gland.
Key words: adrenal calcification, tumor, Addison, tuberculosis, computed tomography,abdominal ultrasound.
215
Case Report
*Correspondence to: D. Peretianu, MD, Department of Endocrinology, SCM Povernei, Bucharest,
Romania, 42 Povernei st, tel: + 40-21-312 79 09.
Acta Endocrinologica (Buc), vol. III, no. 2, p. 215-221, 2007

INTRODUCTION
The phenomenon of calcifications in tissues was described as calciphylaxia inthe years 1950 by Selye, as a condition related to the tissues hypersensitivity tocalcium, linked to a morbid process (1). Most frequently, calcifications, even inendocrine glands, are related to hyperparathyroidism (2). However, calcifications inendocrine glands seem to be more related to local conditions, probably related toinflammations and/or cicatrisation (3).
We present a patient without any sign of endocrine disease, any inflammatorydisease, in which a calcification of the adrenal rim was discovered accidentally.
Case presentationA 75 years old woman was sent for a routine abdominal ultrasound
investigation, as she was accusing pains in the right hypochondrial area. The painwas supposed to be related to biliary-duodenal motriceal dysfunction.
The ultrasound discovered a dense (hyperechogenic) image under (posteriorof) the 8th segment of the liver (Fig. 1). The dense process was supposed to be acalcification situated medial from the right kidney in the cranial 1/3 length of it (Fig.2).
Laboratory data were all normal, including glycemia, creatininemia, BUN,ESR, haemoglobin, transaminases, calcemia and magnesiemia, total lipids, HDLand LDL - cholesterolemia and triglyceridemia.
The patient was in good condition, body mass index was 29. She had no anyform of tuberculosis during her life. The current arterial pressure was 145/80 mm Hg.
D. Peretianu and Cristina Daniela Staicu
216
Figure 1. Hyperechogenic image under (posterior of) the 8th liver segment.

Based on the ultrasound view, the patient was referred to a CT scan. Thediagnosis was based on that scan of the area: clear and only organ-disseminatedcalcification in adrenals (Fig. 3 a-c).
Specific analysis related directly to adrenals was normal, too:Cortisolemia at 8 a.m. was 523 nmol/l (laboratory normal: 171-563 nmol/l).
DISCUSSION
The role of ultrasound vs CT in adrenal lesionsOur patient was referred to the CT scan after a routine abdominal ultrasound.
From this statement results that adrenal ultrasound has no diagnostic value orprognosis. That was set up even by others (4). Even so, in some patients, a routineultrasound could detect strange images which led to a CT scan referral.
The prevalence of calcifications in adrenal gland Over the time, a “Medline” search from 1950 - October 2006, around 300
papers which have as key words both “calcification” and “adrenal gland” have beenpublished.
With the widespread use of computed tomography, these days, it is not unusualto find calcifications within the adrenal glands (5). In all the journals from Medlinesearch, it could be observed there are many varieties of adrenal lesions that maycalcify. The specificity is not the current issue of these calcifications.
Calcification in adrenal glands
217
Figure 2. The relationship of hyperechogenity with the right kidney.

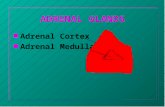
THE PATHOPHYSIOLOGICAL IMPORTANCE OF THE CALCIFICATIONPROCESS
Calcifications have been described in many glands and endocrine diseases formany years. However, no unification pathology for these calcifications exists.
For example, after puberty epiphyses begin to deposit calcium (6), withoutchanging their function, and in the elderly most of the epiphyses are entirelycalcified. Most of craniopharyngiomas have calcifications (7), but their significancewas not explored. The triad “pancreatic calcification, steatorrhea and diabetesmellitus” was found in less than 1/3 patient with chronic pancreatitis (8).
D. Peretianu and Cristina Daniela Staicu
218
Figure 3 a-c. Coronal (a) and sagittal (b)reconstructions from an axial CTscan (c) without contrast,showing the globular rim-like,irregular calcification whichinvolves the right cortical adrenalgland. Note the normal medulladensity. The liver, right kidneyand caval vein and aorta are notinvolved by the calcification. Theleft adrenal was normal (notshown).

We consider that calcification in endocrine glands represents a process ofcicatrisation, especially in the thyroid (9).
The types of adrenals calcificationEarly studies suggested that calcification in adrenals mended haemorrhage
(10), arterial infarction (11) or adrenal vein thrombosis (12), even in recent AIDSpatients (13). In those times, the calcifications were considered as a mainpathological process which leads to adrenal insufficiency (14) and which could beused for Addison’s disease (15) diagnostic.
However, some authors presented that adrenals calcification are never foundin primary cortical atrophy associated with Addison’s disease (16,17), but aresupposed to be more presented (from rarely (17) to around 50% (18) or 62.5% (19))in adrenal tuberculosis; they said that calcification in adrenal areas suggests aformer local tuberculosis process, associated with pulmonary tuberculosis and withadrenal insufficiency.
Another pathological process with calcification is encountered in adrenaltumours. So far (see Medline), more than 50 papers on this subject have beenpublished. In many adrenals carcinomas (20, 21), adrenal myelolipomas and seldomin adenomas associated with Cushing’s syndrome (20), calcifications weredescribed. On the other hand, in large non-functioning adenomas calcificationswere also recorded in 30% patients, one with calcification of the rim of the tumour(21), not of the rim of the gland itself! The difference between tuberculosis andtumours, as phenotypical appearance, is the prevalence of bilateralism (22)(tuberculosis 91% vs. tumours 9%) and the low attenuation in the centre withperipheral rim enhancement which was more commonly seen in tuberculosis (47%)than in primary tumours (9%).
A special sort of adrenal calcification was recorded in Wolman disease (23):lack of lysosomal lipase, accumulation of LDL, peroxidation, cytolysis andnecrosis, followed by calcification of dead adrenal cells. Therefore, some (23)consider that calcification in adrenals means accumulation in a dead cell of freecytosolic Ca2+ .
This later analysis leads to the hypothesis that calcium is involved somehowin adrenal cytolysis. Indeed, calcium (in many experimental conditions) is involvedin lymphocyte TC apoptosis (24) when the antigenic-ligand bridge between thecytotoxic lymphocyte and the antigen (the cell) is realised in a calcium medium.However, the lysis does not depend on calcium, but on magnesium, and the lethalhit is calcium-magnesium independent. Thus, the presence of calcium in a cell lysismedium should suggest other pathophysiological implications.
The rim-like appearance of the adrenal was described only in one patient. Thefirst patient, recorded in Medline, was a newborn with bilateral involvement (25).
In fact, most of the authors described the calcifications as non occupying onlythe cortex; they described the calcification as occupying the whole gland (17),including the medulla or with speck calcification (in myelolipoma) or disseminatedcalcification in carcinomas, (20) or as irregularly shaped regions of various sizes
Calcification in adrenal glands
219

scattered throughout the tumours (21, 22). More, even medulla tumours withpheochromocytoma presented disseminated calcifications (21). Calcification maybe seen in all types of neurogenic tumours (27), including all medullo-adrenaltumours, described as central small punctate calcifications or as dense intratumouralcalcifications.
These pathological changes were viewed as “degenerative changes” (21).ConclusionsIncidental diagnostic of adrenal gland was also reported (28) in patients
without adrenal insufficiency, but there was no report as isolated adrenal process.In our patient, it is clear that calcification is presented only at the cortex, medulla isnot involved, appearing different from those CT adrenals seen and described asatrophic Addison’s disease (29).
Therefore, we consider that calcifications in our patient could mean a processof cicatrisation or healing on the right adrenal gland.
Acknowledgments: Corin Badiu MD is gratefully acknowledged for fruitfuldiscussion and constructive criticism.
References
1. Khafif RA. DeLima C. Silverberg A. Frankel R. Calciphylaxis and systemic calcinosis. Collective
review. Arch.Intern.Med 1990; 150 (5): 956-959.
2. Peretianu D. Manifestari osoase. In: Bistriceanu M., Popescu M., (eds.), Manifestari viscerale în
patologia endocrina. Edit. Medicala Universitara, Craiova 2005; 118-133.
3. Tamaki T. Takumi I. Kitamura T. Osamura RY. Teramoto A. Pituitary stone-case report.
Neurologia Medico-Chirurgica 2000; 40 (7): 383-386.
4. Hamper UM, Fishman EK, Hartman DS, Roberts JL, Sanders RC. Primary adrenocortical
carcinoma: sonographic evaluation with clinical and pathologic correlation in 26 patients. AJR Am J
Roentgenol 1987; 148 (5): 915-919.
5. Hindman N, Israel GM. Adrenal gland and adrenal mass calcification. Eur Radiol 2005; 15 (6):
1163-1167.
6. Labhart A. The pineal body and the circumventricular organs. In: Labhart A., ed., Clinical
Endocrinology. Springer, Berlin 1986; 78.
7. Fleisher N. Disorders of the hypothalamus and anterior pituitary. In: Stein JH et al, eds., Internal
Medicine. Brown Co, Boston 1983; 1727.
8. Greenberger NJ, Toskes PP, Isselbacher KJ. Acute and chronic pancreatitis. In: Wilson JD et al,
eds., Harrison's Principles of Internal Medicine. McGraw-Hill, New York 1992; 1379.
9. Peretianu D. Aspecte ecografice în tiroidita Hashimoto. Rev. Rom. Ultrasonografie 2004; 6 (2-3):
97-104.
10. Stevens RC, Tomsykoski AJ. Bilateral adrenal haemorrhage and calcification. AMA Am J Dis
Child 1954; 87 (4): 475-477.
11. Parker RA. Nontuberculous adult adrenal calcification due to arterial infarction. Stanford Med Bull
1959; 17 (1): 13-15.
D. Peretianu and Cristina Daniela Staicu
220

12. Zirinsky K, Auh YH, Rubenstein WA, Morrison HS, Sherman SJ, Kazam E. Computed
tomography appearance of adrenal vein thrombosis. J Comput Tomogr 1987; 11 (2): 216-218.
13. Duch FM, Repele CA, Spadaro F, dos Reis MA, Rodrigues DB, Ferraz ML, Teixeira Vde P.
Adrenal gland morphological alterations in the acquired immunodeficiency syndrome. Rev Soc Bras
Med Trop 1998; 31 (3): 257-261.
14. Minder WH. Acute adrenal insufficiency in a two-year old boy in consequence of calcification of
adrenal glands. Ann Paediatr 1954; 182 (4): 218-229.
15. Baum G, Graser H. Adrenal calcification; contribution on diagnosis and therapy of Addison's
disease. Med Monatsschr 1954; 8 (8): 548-549.
16. Doppman JL, Gill JR Jr, Nienhuis AW, Earll JM, Long JA Jr. CT findings in Addison's disease.
J Comput Assist Tomogr 1982; 6 (4): 757-761.
17. Labhart A, Groscurth P, Hedinger C, Kistler G, Lasndolt AM, Prader A, Siebenmann R, Zachmann
M. The adrenal cortex. In: Labhart A., ed., Clinical Endocrinology. Springer, Berlin 1986; 378.
18. Vita JA, Silverberg SJ, Goland RS, Austin JH, Knowlton AI. Clinical clues to the cause of
Addison's disease. Am J Med 1985; 78 (3): 461-466.
19. Sun ZH, Nomura K, Toraya S, Ujihara M, Horiba N, Suda T, Tsushima T, Demura H, Kono A.
Clinical significance of adrenal computed tomography in Addison's disease. Endocrinol Jpn 1992; 39
(6): 563-569.
20. Rockall AG, Babar SA, Sohaib SAA, Isidori AM, Diaz-Cano S, Monson JP, Grossman AB,
Reznek RH. CT and MR imaging of the adrenal glands in ACTH-independent Cushing syndrome.
RadioGraphics 2004; 24: 435-452.
21. Newhouse JH, Heffess CS, Wagner BJ, Imray TJ, Adair CF, Davidson AJ. Large degenerated
adrenal adenomas: radiologic-pathologic correlation. Radiology 1999; 210: 385-391.
22. Yang ZG, Guo YK, Li Y, Min PQ, Yu JQ, Ma ES. Differentiation between tuberculosis and
primary tumors in the adrenal gland: evaluation with contrast-enhanced CT. Eur Radiol 2006; 16 (9):
2031-2036.
23. Fitoussi G, Negre-Salvayre A, Pieraggi MT, Salvayre R. New pathogenetic hypothesis for
Wolman disease: possible role of oxidized low-density lipoproteins in adrenal necrosis and
calcification. Biochem. J 1994; 301: 267-273.
24. Peretianu D., Saragea M. Fluxul informational antigenic. In: Imunitatea in teoria si practica
medicinii. Vol.I. (The Immunity in the theory and practice of medicine). D.Peretianu, M.Saragea,
(eds.), Editura ALL, Bucuresti 1996; 128-227.
25. Rinsho Hoshasen. Bilateral rim-like calcification of the adrenal glands in a newborn infant (article
in Japanese) 1976; 21 (7): 637-643.
26. Karasawa R, Hotta M, Aiba M, Takano K. Cushing's syndrome due to a large adrenocortical
adenoma with histological features simulating ACTH-independent macronodular adrenocortical
hyperplasia. Pathol Int 2004; 54 (4): 273-278.
27. Rha SE, Byun JY, Jung SE, Chun HJ, Lee HG, Lee JM. Neurogenic tumors in the abdomen: tumor
types and imaging characteristics Radiographics, 2003; 23: 29-43.
28. Bergman SM, Scouras GP. Incidental bilateral adrenal calcification. Urology 1983, 22 (6):665-666.
29. Ammini AC, Gupta R, Mukopadhyay C, Shah P, Sandhu MS, Vijayaraghavan M, Berry M.
Computed tomography morphology of the adrenal glands of patients with Addison's disease.
Australas Radiol 1996; 40 (1): 38-42.
Calcification in adrenal glands
221