
Incident reporting, analysing, investigating and learning ... · Datix is the electronic incident...
45
Incident reporting, analysing, investigating and learning policy and procedures Page 1 of 45 Ratified by: Safety and Risk Committee Review date: Jan22 Please specify standard/criterion numbers and tick other boxes as appropriate The priorities were agreed by the Trust Board in December 2017 to support the Trust’s vision. The priorities listed below will ensure there is a shared understanding about what needs to be delivered. Monitoring Information Our Priorities Patient Experience Delivering safe and high quality care Assurance Framework People, attract, develop and retain Finance/Performance Making best use of resources Efficiency and Effectiveness Working in partnership CQC Fundamental Standards - Regulation: 9, 10, 11, 12, 13, 14, 15,16, 17,20 Equality, diversity, human rights implications assessed Other (please specify): Policy Information Routine Update New Policy Significant Changes Incident reporting, analysing, investigating and learning policy and procedures Post holder responsible for Procedural Document Head of Governance Author of Policy and Procedure Head of Governance Division/ Department responsible for Procedural Document Corporate Governance Contact details Telephone: Email: Date of original document December 2018 Impact Assessment performed Yes Ratifying body and date ratified Incident Review Group October 2019 Safety and Risk Committee: October 2019 Review date October 2022 Expiry date October 2022 Date document becomes live October 2019 Controlled document This document has been created following the Royal Devon and Exeter NHS Foundation Trust Development, Ratification & Management of Procedural Documents Policy. It should not be altered in any way without the express permission of the author or their representative.
Transcript of Incident reporting, analysing, investigating and learning ... · Datix is the electronic incident...

Incident reporting, analysing, investigating and learning policy and procedures Page 1 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Please specify standard/criterion
numbers and tick other boxes
as appropriate
The priorities were agreed by the Trust Board in December 2017 to support the Trust’s vision. The priorities listed below will ensure there is a shared understanding about what needs to be delivered.
Monitoring Information Our Priorities
Patient Experience Delivering safe and high quality care
Assurance Framework People, attract, develop and retain
Finance/Performance Making best use of resources
Efficiency and Effectiveness Working in partnership
CQC Fundamental Standards - Regulation: 9, 10, 11, 12, 13, 14, 15,16, 17,20
Equality, diversity, human rights implications assessed
Other (please specify):
Policy Information
Routine Update New Policy
Significant Changes
Incident reporting, analysing, investigating and learning policy and procedures
Post holder responsible for Procedural Document
Head of Governance
Author of Policy and Procedure Head of Governance
Division/ Department responsible for Procedural Document
Corporate Governance
Contact details Telephone:
Email:
Date of original document December 2018
Impact Assessment performed Yes
Ratifying body and date ratified
Incident Review Group October 2019 Safety and Risk Committee: October 2019
Review date
October 2022
Expiry date October 2022
Date document becomes live October 2019
Controlled document This document has been created following the Royal Devon and Exeter NHS Foundation Trust Development, Ratification & Management of Procedural Documents Policy. It should not be altered in any way without the
express permission of the author or their representative.

Incident reporting, analysing, investigating and learning policy and procedures Page 2 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Full History:
Status: Final
Version Date Author (Title not name)
Reason
1.0 December 2018 Head of Governance Adoption of policy provided by RD&E
1.1 June 2019 Head of Governance Revision from feedback.
1.2 July 2019 Head of Governance Revision of tables after feedback from Consultants.
1.3 September 2019 Head of Governance Comments added to draft policy
2.0 September 2019 Head of Governance Policy Approved at IRG 09.09.19
2.0 October 2019 Head of Governance Approved at S&RC
2.1 October 2019 Head of Governance Slight Amends from S&RC
2.2 November 2019 Head of Governance Amendments added – Safeguarding, Information Governance and flowchart.
Associated Trust Policies/ Procedural documents :
Safeguarding Children Policy
Raising Concerns and Complaints Policy
Disciplinary & Procedures Policy
Incident Response Plan
Fire Safety Policy
Health and Safety Policy
Standard Infection Control Precautions Policy
Safeguarding Adults Policy
Risk Management Policy
Supporting Staff in an Incident, Complaint or Claim Policy
Raising Concerns Policy Incorporating Freedom to
speak up and Whistleblowing
Information Governance Policy and Framework
Key Words: incident, incident report, reporting, DATIX
In consultation with and date: Incident Review Group – July 2019 Trained Investigators – July 2019 Senior nurses July 2019 Governance Staff July 2019 Safety and Risk Committee July 2019
Contact for Review: Head of Governance
Executive Lead Signature Chief Nurse
Incident reporting, analysing, investigating and learning policy and procedures Page 3 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
1. CONTENTS
1. CONTENTS ............................................................................................................... 3
2. INTRODUCTION ........................................................................................................ 4
3. PURPOSE .................................................................................................................. 4
4. DEFINITIONS............................................................................................................. 4
5. DUTIES AND RESPONSIBILITIES OF STAFF ......................................................... 6
6. INCIDENT REPORTING, ANALYSIS, INVESTIGATION AND LEARNING ............. 11
7. STAFF...................................................................................................................... 18
8. TRAINING REQUIREMENTS FOR STAFF .............................................................. 18
9. ARCHIVING ARRANGEMENTS .............................................................................. 18
10. PROCESS FOR MONITORING COMPLIANCE WITH AND EFFECTIVENESS OF THE POLICY ...................................................................................................................... 19
11. REFERENCES ......................................................................................................... 19
12. APPENDIX 1: DEFINITION OF A SERIOUS INCIDENT WITHIN THE NHS FRAMEWORK .................................................................................................................... 21
13. APPENDIX 2: CORE LIST OF NEVER EVENTS 2018 ........................................... 22
14. APPENDIX 3: INCIDENT REPORTING – WHAT SHOULD BE REPORTED? .......... 26
15. APPENDIX 4: GRADING MATRIX – DEFINITIONS FOR CONSEQUENCE OF INCIDENT (ACTUAL AND FUTURE POTENTIAL) ............................................................ 28
16. APPENDIX 12: PROCEDURE FOR REPORTING INCIDENTS INVOLVING MEDICAL DEVICES ........................................................................................................... 33
17. APPENDIX 13: PROCESS FOR REPORTING AND INVESTIGATING SUSPECTED MISAPPROPRIATION OF MEDICINES .............................................................................. 34
18. APPENDIX 14: DUTY OF CANDOUR PROCESS ................................................. 35
19. APPENDIX 15: DUTY OF CANDOUR STICKER .................................................... 36
20. APPENDIX 16: DUTY OF CANDOUR LETTER TEMPLATE ...................................... 37
21. APPENDIX 17 CARDIAC ARREST REPORTING FLOWCHART ........................... 38
22. APPENDIX 18: REPORTING ................................................................................... 39
23. APPENDIX 19 Just Culture guide .......................................................................... 42
24. APPENDIX 20: EQUALITY IMPACT ASSESSMENT TOOL .................................... 43
Incident reporting, analysing, investigating and learning policy and procedures Page 4 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
2. INTRODUCTION
2.1. The Northern Devon Healthcare NHS Trust (hereafter referred to as the Trust) is committed to delivering quality patient care, ensuring high standards of health and safety, and minimising loss by providing a system of incident reporting which allows all staff to record any incident which causes harm, damage or loss or has the potential to do so.
2.2. Incident reporting presents an important opportunity to learn from past events
and ensure steps are taken to minimise recurrences.
2.3. There is overwhelming evidence that NHS organisations with a high level of incident reporting are more likely to learn and subsequently increase safety for patients, staff and visitors.
2.4. Failure to comply with this policy could result in disciplinary action.
3. PURPOSE
3.1. This policy sets out the Trust systems, processes and expectations in relation to incident reporting and learning to include the:
Process for reporting all incidents involving staff, patients and others.
Process for reporting to external agencies.
Process for investigating incidents according to level of harm and future harm /
risk. Process for involving and communicating with internal and external
stakeholders to share safety lessons.
Process for the aggregated analysis of incidents, complaints and claims. Process by which the organisation ensures local and organisational learning
and changes in practice resulting from individual incidents and aggregated analysis.
Process for ensuring communication is open, honest, occurs as soon as possible and is well documented and that our legal duties for Duty of Candour are applied and monitored.
Training requirements for staff.
3.2. Compliance with this policy will ensure that incidents are systematically identified, recorded, reported to management and appropriately investigated. This will result in learning and thus improving safety for patients, staff and visitors.
4. DEFINITIONS
4.1. Incident / Accident An Incident / Accident is defined as an occurrence or unplanned event (act or omission), where there is injury, loss of life, loss or damage to persons or property. Examples of an incident / accident: patient safety / clinical incident, personal accident, security, fire, theft, vandalism, staff shortage.
4.2. Near Miss
A near miss is defined as any event or circumstance that was prevented or narrowly avoided injury or harm, which had it occurred, could have had a detrimental impact. A near miss also encompasses the failure of clinical policy where no harm has come to the patients.
Incident reporting, analysing, investigating and learning policy and procedures Page 5 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
4.3. Serious Incident (SI) A serious incident in the SI Framework is defined as: ‘events in healthcare where the potential for learning is so great, or the
consequences to patients, families and carers, staff or organisations are so
significant, that they warrant using additional resources to mount a
comprehensive response. Serious incidents can extend
beyond incidents which affect patients directly and include incidents which may
indirectly impact patient safety or an organisations ability to deliver ongoing
healthcare.
For a full definition setting out the circumstance in which a serious
incident must be declared, go to Appendix 1. The incidents would be
StEIS reportable.
4.4. Serious Harm
Serious harm would relate to incidents where permanent harm has occurred.
4.5. Never Event Never events are serious, largely preventable patient safety incidents that should
not occur if the available preventative measures have been implemented (a full list
of never events is attached in Appendix 2).
4.6. Others Students, trainees, visitors, contractors, agency staff, volunteers, general public, and
undertakings sharing the premises with the Trust.
4.7. Datix
Datix is the electronic incident reporting system that enables reporting, analysis
and collation of incident, complaints, risk and claims data.
4.8. Incident Investigation
An incident investigation is the act or process of examination or enquiry and
analysis into an adverse event in order to understand, how and why it occurred
as well as identify mitigating actions to prevent future occurrence.
4.9. Levels of investigations
The level of investigation should be proportionate to the individual incident.
The national framework describes these levels as concise and
comprehensive.
Informal Managers Investigation – suited to no harm / minor incidents which are
managed within the team by the local manager.
Concise investigation – suited to less complex incidents which can be
managed by individuals or a small group of individuals at a local level.
Comprehensive – suited to complex issues which should be
managed by a multidisciplinary team involving experts and fully
trained investigators.
Independent – suited to incidents where the integrity of the internal investigation is
likely to be challenged or where it will be difficult for an organisation to conduct an
objective investigation internally.

Incident reporting, analysing, investigating and learning policy and procedures Page 6 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
4.10. Complications
Complications are any deviation from the normal course. Medical complications are
an unfavourable evolution or consequence of a disease, a health condition or a
therapy. A complication may be iatrogenic. However if a complication is a direct
result of human error, negligence, poor system or equipment design or unnecessary
treatment it is a clinical incident.
4.11. Human Factors
Enhancing clinical performance through an understanding of the effects of teamwork, tasks, equipment, workspace, culture and organisation on human behaviour and abilities and application of that knowledge in clinical settings.
5. DUTIES AND RESPONSIBILITIES OF STAFF
5.1. Chief Executive
The Chief Executive has overall responsibility, on behalf of the Trust Board, for ensuring the implementation of this policy throughout the organisation.
5.2. Chief Nurse
Has delegated responsibility from the Chief Executive for Risk Management and
therefore has Executive responsibility for the development and implementation of
incident reporting processes.
5.3. The Senior Information Risk Owner (SIRO)
The SIRO is the Senior Management Board Member responsible for Information
Governance (IG) in the Trust and ensures IG incidents are reported and
investigated in line with the Trust incident reporting processes. In the Trust the
SIRO is the Medical Director.
5.4. The Caldicott Guardian The Caldicott Guardian is a senior clinician who oversees the arrangements for
the use and sharing of clinical information and advises on options for the lawful
and ethical processing of information as required and represents confidentiality
issues at Board level.
5.5. Head of Governance
Provide leadership of the Governance processes within the Trust.
To lead on the risk management systems, ensuring routes for risk identification and reporting are clearly articulated and implemented:
Responsible for ensuring the functioning of the corporate systems detailed
within the policy and support the identifying, recording, reporting to
management, appropriately investigating and learning from incidents.
Undertake the corporate collation and analysis of incidents, liaise with external and
internal stakeholders where necessary, generate trend reports of incident
types/themes.
Ensure reporting in line with the Care Quality Commission (CQC) regulatory framework.

Incident reporting, analysing, investigating and learning policy and procedures Page 7 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
5.6. Head of Quality and Safety Provide clinical leadership of the investigation and incident reporting:
Undertake the clinical collation and analysis of incidents, liaise with external and internal stakeholders where necessary, generate trend reports of incident types/themes.
Provide a source of advice and support for investigation leads when investigating and preparing the reports
Ensure Duty of Candour requirements are fulfilled
Undertake regular meetings with the CCG
5.7. Medications Safety Officer All medicines incidents will be reported to the Trust Chief Pharmacist who currently holds the Medications Safety Officer role, Clinical Pharmacy Manager, Medicines Governance and Safety Pharmacist and relevant Pharmacist/s via DATIX for screening and onward prioritisation, investigation and / or escalation, following the medicines incidents procedure for investigating and escalation.
5.8. Controlled Drug Accountable Officer
All incidents involving controlled drugs must be notified to the Trust’s Chief Pharmacist (MSO), the Clinical Pharmacy Manager who will inform the Trust’s Accountable Officer for Controlled Drugs in line with the Controlled Drugs Policy.
5.9. Information Governance (IG) Manager
The Information Governance Manager and the Information Governance team have delegated responsibility from the SIRO and are responsible for ensuring IG Serious Incidents (SI) are reported and investigated in line with National NHS Guidance on reporting, managing and investigating IG SI’s.
5.10. Associate Directors of Operations / Associate Medical Directors/Divisional
Nurses Are responsible for ensuring the Divisional structures support the systems for identifying, recording, reporting to management, appropriately investigating and learning from incidents. They are also responsible for the timely Duty of Candour to be undertaken with their divisions.
5.11. Risk Lead
The Risk Lead will act as gatekeeper for incidents, review all potential incidents for escalation. The Risk Lead will have oversight of the Incident and Investigation process, leading the Risk and Incident team.
5.12. Serious Incident Lead
The SI Lead will manage the SI reporting process. Notify the Commissioner via StEIS of reportable incidents, and the Commissioner
will have a process in place for informing Specialist Commissioners where an
incident relates to a patient’s treatment commissioned by them.
Ensure quality reports are produced and written within the specified time frames.
Support the lead investigators to complete their investigations and write the reports
Incident reporting, analysing, investigating and learning policy and procedures Page 8 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Make the decisions as to whether an incident is a SI using the relevant criteria
Set appropriate terms of reference for each SI Investigation
Liaise with external stakeholders
Produce Status and ad-hoc reports as required
Maintain accurate records of the investigation and ensure all archiving of documentation is undertaken appropriately.
5.13. Investigations Administrator
Escalate Incidents as appropriate
Review all investigation reports to ensure quality is maintained and all other advisors are provided with the report for their input
Reports are anonymised appropriately
The administration of investigations on DATIX is completed
Provide administrative support for the Incident Review Group
Liaise with external stakeholders – Clinical Commissioning Group Safety team for Quality Reviews on SI Reports
Produce reports on investigations on themes, trends and key issues for Groups and Committees as required
5.14. Responsible Managers
Ensuring the Incident Management Policy is implemented
Ensure staff report incidents;
Escalate or investigate incidents according to the incident categorisation and take immediate action to reduce risk of reoccurrence;
Acting as ‘Responsible Manager’ for the incidents recorded on DATIX.
To ensure you review the grading as soon incident recorded
Ensuring action taken and learning identified from their local incident investigations are recorded on the DATIX system.
In the case of an incident involving a patient, informing the patient and their carer or relatives of any incident as soon as possible in line with the Duty of Candour Policy.
Acting in an open and transparent way with relevant persons in relation to care and treatment provided under Duty of Candour in line with the Duty of Candour Policy.
Regularly reviewing incident reports with staff to identify these and implement changes that may be required to avoid a recurrence of the incident.
Maintaining the ‘Current Status’ of the incident investigation on the DATIX system.
Providing feedback to staff of the outcomes of the local incident investigation.
Ensuring the severity of the incident is correct.
Promote patient safety and a just culture towards incident management
Notify the Facilities Clinical Services Manager of any of reportable medical equipment incidents who will notify the Medicines and Healthcare products Regulatory Agency (MHRA).
5.15. DATIX & Incident Team
Will maintain the database on which all incident reports will be stored (Datix).
Support staff to report and manage incidents.
Ensure each incident report form is screened upon submission to ensure a consistent approach to the coding to maintain data quality and to ensure information is passed to relevant clinical and non-clinical staff.
Ensure the procedures for managing the incident report information on DATIX
Incident reporting, analysing, investigating and learning policy and procedures Page 9 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
are robust and effective.
Identifying and escalating high risk incidents to the Investigations Team for further investigation in line with this policy.
Ensure patient safety incident data is routinely upload to the National Reporting and Learning System (NRLS) held by NHS Improvement.
Support staff to run routine and ad-hoc reports as appropriate.
5.16. Lead Investigator
Must be fully trained in undertaking investigations using Root Cause Analysis (RCA) techniques.
Undertakes an investigation using RCA tools and techniques which establishes how an incident has occurred, the root cause of that incident and establish how recurrence may be reduced or eliminated.
Formulate recommendations to manage care and service delivery issues.
Provide an investigation report within the allotted timeframe as a record of the investigation process that sets out clearly the investigation findings, recommendations and actions agreed by the operational team.
To keep a full investigation pack of all documents used for the investigation, including all statements taken, photographs and notes relied upon to formulate the report.
5.17. Divisional Governance Co-ordinators
Promote consistent, accurate and timely categorisation and grading of incidents on Datix within the Division by ensuring teams responsible for the reviewing and categorisation of all incidents within timescales.
Ensure compliance with required timescales and escalate concerns of non-compliance.
Are responsible for ensuring that all actions are monitored via the Divisions governance processes thus ensuring timely completion.
Co-ordinate the dissemination of Trust wide learning at specialist level.
Ensure there is compliance with Duty of Candour, and establish responsibility for contact for the patient/carer during the investigation process.
5.18. Staff
Are responsible for reporting and escalating incidents in accordance with this policy and co-operating where appropriate in any subsequent investigations.
Are responsible for application of duty of candour when appropriate
Engage in learning and outcomes from investigations.
Staff concerned about the delivery of care/service to patients have a duty to express their concerns to their line manager, through the incident reporting system or as outlined within the Raising Concerns Policy Incorporating Freedom to Speak Up and Whistleblowing
Staff concerned about the safety of their environment have a duty to raise their concerns, in line with the Health and Safety Policy.
5.19. Health and Safety manager/LSMS
Notify the Health and Safety Executive of reportable incidents under the Reporting and Injuries, Diseases, Dangerous Occurrence Regulations (RIDDOR).
Ensure all RIDDOR investigations are investigated in line with the investigation process.
5.20. Legal Claims Manager
To act as liaison between Trust staff and the Legal Team that we have an

Incident reporting, analysing, investigating and learning policy and procedures Page 10 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
agreed Service Level Agreement with to undertake our legal advice and activities with.
To ensure draft SI reports are sent to the Trust Solicitor as required i.e. those where an Inquest is required or those where a claim has been made.
5.21. Specialist Advisors
Specialist Advisors such as Tissue Viability, Falls, Pharmacy and Health and Safety leads may identify incidents for escalation through themes or specific issues whilst validating any incidents.
Will provide expert input into investigations where required.
5.22. Staff Side Safety Representatives
Under the Terms of the Safety Committees and Safety Representatives
Regulations 1977, the Trust recognises the right of Staff Side Safety
Representatives to investigate health and safety related incidents and dangerous
occurrences.
5.23. Safety and Risk Committee
Will receive reports from the Incident Review Group in relation to compliance with
undertaking investigations, subsequently implementing actions and exploring
themes arising from investigations
Will receive the full reports of never event investigations and give assurance to the
Governance Committee that the investigation is robust.
5.24. Incident Review Group (IRG)
Will review all investigations of incidents, inquests, claims and complaints
categorised as meeting the SI criteria or are externally reported, where harm and a
lapse in care is identified.
The Group will:
Monitor whether the incident was notified correctly and in a timely manner.
Monitor the use of root cause analysis tools within the investigation.
Monitor the quality and timeliness of the investigation process.
Review the appropriateness and completion of planned actions of reports scrutinised through IRG.
Review the correct level of communication and consultation with relevant parties/forums has been undertaken.
They will provide a forum for sharing organisational learning from investigations, incidents, complaints and claims and aggregate analysis, both qualitative and quantitative feeding into the Divisions as well as to the Safety and Risk Committee.
Sample concise investigation reports each quarter to ensure adherence with this policy,
Commission a lessons learnt newsletter to disseminate learning from investigations.
Monitor all overdue actions for moderate and major incidents, complaints and claims.
Monitor all overdue investigations which are moderate and above to understand the delay
Monitor compliance with duty of candour.
Review quarterly audits of completed actions and their effectiveness.
Incident reporting, analysing, investigating and learning policy and procedures Page 11 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Through the above monitoring provide assurance to Safety and Risk Committee.
5.25. Safety Huddle
The safety huddle meets on a weekly basis and consists of the Chief Nurse, Deputy Chief Nurse, Head of Quality and Safety, Deputy Medical Director and Risk Lead.
Will review 72 hour investigation reports to identify whether escalation to SI is required.
Will identify appropriate leads for the investigation lead and relevant clinical investigator to support and advise the SI Lead.
Will support Investigation leads with any issues or blockages raised through the
investigation process.
5.26. Health and Safety Group
Receive reports on RIDDOR investigations to ensure learning is identified.
Analyse trend data to ensure learning is being put into place to reduce the likelihood of RIDDOR incidents occurring.
5.27. Information Governance Steering Group (IGSG)
The IGSG is the senior group in the Trust responsible for ensuring Trust
compliance with Information Governance. This includes legal and NHS policy
requirements. The IGSG will ensure: -
That IG Incidents are notified to the ICO, NHS Digital, DHSC and other regulators through the DSP Toolkit correctly and in a timely manner
The timeliness of the investigation process
Ensure appropriateness and completion of planned actions
Information Governance training is mandatory for all staff annually
5.28. Divisional Groups (Divisional Governance / Specialty Governance)
Will review Divisional concise and comprehensive reports, formulate action plans for these investigations and monitor them to completion ensuring completion is met within timeframes.
Will review Trustwide SI, and Divisional quarterly trend graphs to ensure appropriate learning and feedback to all staff at Divisional level
6. INCIDENT REPORTING, ANALYSIS, INVESTIGATION AND LEARNING
6.1. Reporting of Incidents
All incidents will be reported on the Trust Electronic Incident Reporting system (Datix) immediately or as soon as safe to do so (link via Trust Intranet).
The information reported on the incident form must be factual and accurate. No opinions or guesswork should be included. This is a legal document and must be factual.
Staff who intentionally fail to report an incident will be subject to management processes..
Incidents cover a wide range of events and may affect patients, staff and others both clinical and non-clinical. For a non-exhaustive list of incident types see Appendix 3.

Incident reporting, analysing, investigating and learning policy and procedures Page 12 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Incident reports should, wherever possible, be completed by the member of staff who first becomes aware of the incident. If that person is unable to do this due to personal injury or other circumstances the form must be completed by another person on their behalf.
Any incident that relates to an external organisation will be forwarded by the DATIX & Incident Team to ensure they are made aware of the incident and refer that incident to the external body for appropriate action.
Any incident received from an external organisation including General Practitioner (GP) practices and CCG Yellow Cards will be entered onto the Datix system by the DATIX & Incident Team and allocated to the relevant department to investigate.
Any unexpected death arising from the Trust’s Mortality Review Process will be subject to a full mortality review. The outcome will be reviewed by the Deputy Medical Director and Associate Medical Director (AMD) for consideration of further escalation in line with this policy.
In some circumstances allegations can be raised through other forums, such as Whistleblowing or the Freedom to Speak up Guardians where it is alleged that an incident has occurred. Where allegations have been made an incident form must be completed and consideration must be given to whether they meet the StEIS reportable criteria.
6.2. Immediate Response to the Incident
The initial response to any incident must be to make the situation safe thus preventing further harm to patients, visitors and/or staff/ others.
Incidents resulting in unexpected death (catastrophic), serious injury (major) or suspected never events must always be reported immediately to the Chief Nurse, Head of Quality and Safety and/or Duty Manager out of hours who will escalate as appropriate.
For incidents which involve medical devices do not disassemble, clean, decontaminate or alter control settings. Clearly identify defective item(s) and attach a yellow decontamination label and contact the Medical Equipment Manager (see Appendix 12 for the process).
For medication incidents where patient harm has been identified or is suspected the medication must be retained if possible and the batch number (lot number) and manufacturer must be recorded on the Datix Form and the Medication Incidents – Standard Operating Procedure must be followed.
Where medication is suspected to be defective e.g. clouding or particulates in an intravenous (IV) fluid product this must also be retained, taken out of use and an incident form completed including batch (lot) number and manufacturer.
For incidents where misappropriation of medication is suspected the procedure outlined in Appendix 13 will be followed.
Where appropriate photographs of defective equipment or to show the

Incident reporting, analysing, investigating and learning policy and procedures Page 13 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
environment can be taken and uploaded to the incident form, to help inform any investigation.
6.3. Police Involvement
The police are likely to investigate incidents where there is evidence, or suspicion of, a criminal offence having been committed, for example if an incident has arisen from or involves criminal intent, or gross negligence.
The incident must be escalated as set out in section 5.2 and reported to the commissioning body, plus informing the Health and Safety Manager.
Referral to the police should be undertaken by the Health and Safety Manager/LSMS senior member of staff, on-call Manager or on-call Director.
In circumstances of unexpected death or serious harm requiring investigation by the police, the incident should be managed in accordance with the Memorandum of Understanding. This protocol should be activated when an incident requires investigation by the police and the Health and Safety Executive jointly. Wherever possible, SI investigations should continue alongside criminal proceedings but this should be considered in discussion with the police. In exceptional cases (i.e. following a formal request by police, Coroner or judge) the investigation may be put on hold and this should be discussed with those involved.
6.4. Hidden Incidents
Occasionally an incident may be reported which is sensitive or confidential which needs to be hidden from view on the system. Any request to undertake the hiding of incidents must be made via the Head of Governance through the DATIX system.
6.5. Duty of Candour - Being Open when Patients are Harmed
When moderate, severe harm or death incidents occur or prolonged pain or Psychological harm ie experienced by the patient, the Duty of Candour process must be followed as set out in the Duty of Candour Section in Appendices 15,16 & 17. This is a contractual duty as well as being a legal duty under the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014: Regulation 20.
If an incident occurs which does not result in moderate or above harm the patient should still be offered an apology and an explanation given in line with being open principles. Organisations are said to be open when the prevailing culture visibly encourages key behaviours. These include honesty, openness, appropriate sharing of information and a willingness to learn from experiences to change how the organisation functions. Any letters associated with the Duty of Candour should be linked to the incident on DATIX.
6.6. Incident Grading, and Escalation
Not all incidents need to be investigated to the same extent or depth. Categorising incidents according to the actual impact and the potential future risk to patients/visitors/staff/others and the organisation establishes the level of local investigation and causal analysis that should be carried out.
Incident reporting, analysing, investigating and learning policy and procedures Page 14 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
All incidents categorised as major or catastrophic (See Appendix 4) or in the Red area of the matrix will be escalated immediately to the Chief Nurse, Deputy Medical Director, Head of Midwifery, Head of Governance, SI Lead, DATIX and Incident Team and Divisional Senior Management team both via automated email but also via the internal escalation process for serious incidents. (Follow the flowchart Appendix 5).
A decision must be made by the SI Lead or the Safety Huddle as to whether an incident is reportable to the Commissioners as a Serious Incident (SI) meeting StEIS criteria; where possible this will be within 48 hours of the incident. Where appropriate, the SI Lead will:
Inform the Chief Nurse and Medical Director (if appropriate) at an early
stage. Ensure, though the Divisional Governance Co-ordinators that there is
compliance with Duty of Candour, they will establish responsibility of contact for the patient/carer during the investigation process.
The on-call Director needs to consider whether the incident is a significant or major incident as defined in the major incident plan and consider evoking the plan.
The Head of Communications will be required to advise and provide support on internal and external communications.
All incidents are reviewed by the DATIX Support Administrator prioritised by severity. Responsible Managers/Ward Managers or their deputy will review their incidents within 48 hours and escalate for investigation where appropriate.
6.7. Reporting of Information Governance incidents
Information Governance incidents are incidents in which information held by the Trust could have been, or has been, compromised. They can result in regulatory action by the Information Commissioner‘s office (ICO) including Civil Monetary Penalties (fines) of up to £17.7 million, as well as claims against the Trust.
All incidents of Information Governance breaches will be recorded using DATIX. Advice must be sought from the IG Team on whether an IG event is reportable to the ICO and DHSC. Any incident reported to the ICO is automatically StEIS reportable. All IG SI incidents will be fully investigated in accordance with this policy and graded as moderate or above. The Information Governance Manager will report a summary of Information Governance incidents to the Information Governance Steering Group (IGSG). Detailed reports will be produced on individual Information Governance related Serious Incidents (IG SI). An IG SI is detailed as failures in the security, integrity, accuracy or availability of information often described as data loss and/or information governance related issues to include:
a. Any incident which involves actual or potential failure to meet the requirements
of the Data Protection Act 2018.
b. This includes unlawful disclosure or misuse of confidential data, recording or
Incident reporting, analysing, investigating and learning policy and procedures Page 15 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
sharing of inaccurate data, information security breaches and inappropriate invasion of people‘s privacy and/or the Common Law of Confidentiality.
c. Such personal data breaches which could lead to identity fraud or have other significant impact on individuals.
d. Applies irrespective of the media involved and includes both electronic media and paper records
It is a legal obligation to notify personal data breaches of the GDPR under Article 33 within 72 hours, to the ICO, unless it is unlikely to result in a risk to the rights and freedoms of individuals. The DSP Toolkit Incident Reporting Tool must be used for reporting as this will report IG SI incidents to NHS Digital, DHSC, ICO and other regulators.
Incidents or events that have a significant impact on the continuity of essential services (under the NIS Regulations) must also be reported within 72 hours. Any incident reportable under the NIS Regulations may also be reportable as a personal data breach under the GDPR reporting requirements (above).
The IG Manager will investigate and prepare a report in consultation with the Caldicott Guardian, Data Protection Officer (DPO) or Senior Information Risk Owner (SIRO) to ensure that IG SIs are reported in accordance with Trust policy and National NHS guidance. All Level 2 reportable ICO incidents will also be StEIS reported.
6.8. Investigation Appropriate to the Severity of the Incident
Major, Catastrophic (Actual Harm) or SI incidents (future potential) on the grading matrix The greatest effort should be concentrated on serious incidents where major or
catastrophic harm has occurred. To identify whether the incident is reportable on
StEIS a 72 hour report will be completed. If the incident meets the criteria it is
reported on StEIS and an SI investigation report is completed. For non-reportable
incidents, the screening tools are completed and a Concise Investigation report is
completed (Appendix 10). StEIS incidents must be the subject of a comprehensive
investigation using Root Cause Analysis (RCA) methodologies completed within 45
working days on the Investigation Template (Appendix 11). A full evidence pack
must be kept of any documentation supporting the findings in the report including
any notes taken and investigative tools used. These will be returned to the SI Lead
(either as a hard copy or electronically) where they will be stored and made
available if further investigation or legal action arises.
The Safety Huddle, SI Lead or Head of Midwifery for Maternity Incidents, will
identify trained investigators to co- ordinate the review of each comprehensive
incident; 1 investigator and a subject matter expert will be appointed, where
necessary 2 investigators may be assigned. At this point the Terms of Reference
(TORs) for the investigation must be given to the investigator. The investigators
will be trained in undertaking investigations using RCA techniques and
independent of the specialty where the incident occurred, a subject matter expert
will be allocated as required.

Incident reporting, analysing, investigating and learning policy and procedures Page 16 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Investigation Process The investigation should confirm the facts using the incident, falls or Information Governance screening tool around:
What happened?
How did it happen?
Why did it happen?
Moderate incidents (Actual Harm)
A concise investigation using the concise investigation tool must be
undertaken within the Division, and any resulting investigation must be
completed within 45 working days on the investigation template. (Appendix
10).
No harm or minor incidents It is the responsibility of the person in charge of an area to undertake the
informal managers investigation within 45 working days and ensure that all
necessary immediate remedial action is taken and documented in the
management section on the electronic incident report.
The managers investigation section is sent to the reporter once the investigation
is closed on the system if the reporter has requested feedback.
Externally reportable Incidents Certain incidents require reporting to external agencies, detail of such incidents and responsibilities for reporting are included in Appendix 18. All externally reported incidents will be graded as a minimum of moderate due to the potential reputation risk, however, this may be higher against another domain. The report will be reviewed by the Incident Review Group where it is StEIS reportable or where there has been harm and lapses in care. Redacting Reports Including the patients names that they have asked to be known by, makes the report more personal so this should be include if we have consent from patient / relative it is fine to us to use the preferred name and to not redact this at the end. Professionals names and experts used should just state job titles and not names or initials. In the appendix there should be a table with job titles and names of individuals so this can be easy identified if needed, however when sharing with the patient / family this page will be removed. Sharing Reports The patient or relative will be consulted on how they would like to be referred to in the report (Mr/Mrs/name or possibly initials), this will be the name used throughout the report. The patient or relative must be made aware of how far this report may be shared, it could go to the CCG and other organisations and be seen by many different people or it could go through a legal process. The patient may wish for the report to be redacted if the report is to be shared outside this organisation.
6.9. Templates
There are a range of templates available for varying different investigations, the most relevant template should be used to suit the investigation.
• Incident Screening Tool Template
Incident reporting, analysing, investigating and learning policy and procedures Page 17 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
• Falls Investigation Screening Tool Template • Information Governance Screening Tool Template • Concise Investigation Tool Template • 72 Hour Report Template • SI Reporting Template • Safeguarding 72 hour template • Safeguarding Concise Report Template
6.10. Ensuring Local and Organisational Learning
Root Cause Analysis Investigations All investigation reports will include an action plan which will link to the causative
factors and recommendations identified during the investigation.
The Incident Review Group, will routinely review outstanding concise and SI actions and receive exception reports via the Governance Co-ordinators/Maternity Risk Manager. The Governance Co-ordinators/Maternity Risk Manager are in turn responsible for working through open actions in the Division with the senior management teams to ensure the timely closure of actions through local governance processes.
The Risk Lead will undertake spot checks of implemented action plans, and report findings to the Incident Review Group and subsequently to the Safety and Risk Committee which will advise the Governance Committee and thereby the Board of Directors.
6.11. Lessons Learnt Newsletter The Incident Review Group will produce a lessons learnt newsletter setting out key themes, trends and learning from investigations. This will give information on key learning and topics of interest, highlighting key information staff need to be aware of. This newsletter will be disseminated through the Divisions by the Governance Co-ordinators posted on the Trust Intranet.
6.12. Aggregated Analysis Reporting
Aggregate Analysis Reports of Incident, Complaint, Claim and other Patient Feedback Quarterly aggregated trends, will be produced for the Incident Review Group and Divisions setting out both quantitative and qualitative analysis of these elements. The report will include: - Quantitative Analysis The report will include a quantitative summary of complaints, claims and incidents identifying trends where possible. The content will include the following information: Complaints Overview. Number of complaints per rolling year. Total number of complaints received per month. Top 5 complaints by main subject. Total number of complaints received by severity. Summary analysis and lessons for learning. Claims Overview. On-going claims.

Incident reporting, analysing, investigating and learning policy and procedures Page 18 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
New claims this quarter. Claims closed this quarter. Inquest details. Summary analysis and lessons for learning. Incidents Overview. Total number of reported incidents. Breakdown of incident type. Top 10 reported incidents Trustwide. Total number of reported incidents by severity. Concise report trends/ SI Summaries Summary analysis and lessons for learning. Qualitative Analysis Where specific trends are identified the contributors to the report will be responsible for providing an explanation (if possible) for the trend. This may require making reference to external data sets and/or a comparison to previous quarterly figures.
7. STAFF
7.1. It is recognised that incidents can have a significant impact on staff who were involved or who may have witnessed the incident.
7.2. Staff involved in the investigation process should have the opportunity to access professional advice to ensure that support is offered to all staff involved promptly. Further guidance can be found in the Supporting Staff involved in an incident, complaint or claim Policy.
7.3. The Just Culture Guide (Appendix19) should be used to promote fair and
consistent staff treatment. In the very rare circumstances where a member of staff has committed a criminal or malicious act, the staff member should be advised at an early stage to enable them to obtain separate legal advice and/or representation.
7.4. Further support may be arranged if required through staff support or occupational health.
8. TRAINING REQUIREMENTS FOR STAFF
8.1. All staff will receive training on incident reporting via their line management at local induction and through periodic risk updates.
Staff leading investigations will receive training in Root Cause Analysis methodology. Training is facilitated by the Investigation Team as required. A record of staff trained to lead investigations is held within the Investigations team.
9. ARCHIVING ARRANGEMENTS
The original of this policy will remain with the Governance team. An electronic copy will be maintained on the Trust Intranet. Archived electronic copies will be stored on the Trust's Governance Department/policies and procedural documents, and will be
Incident reporting, analysing, investigating and learning policy and procedures Page 19 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
held indefinitely. A paper copy (where one exists) will be retained for 10 years.
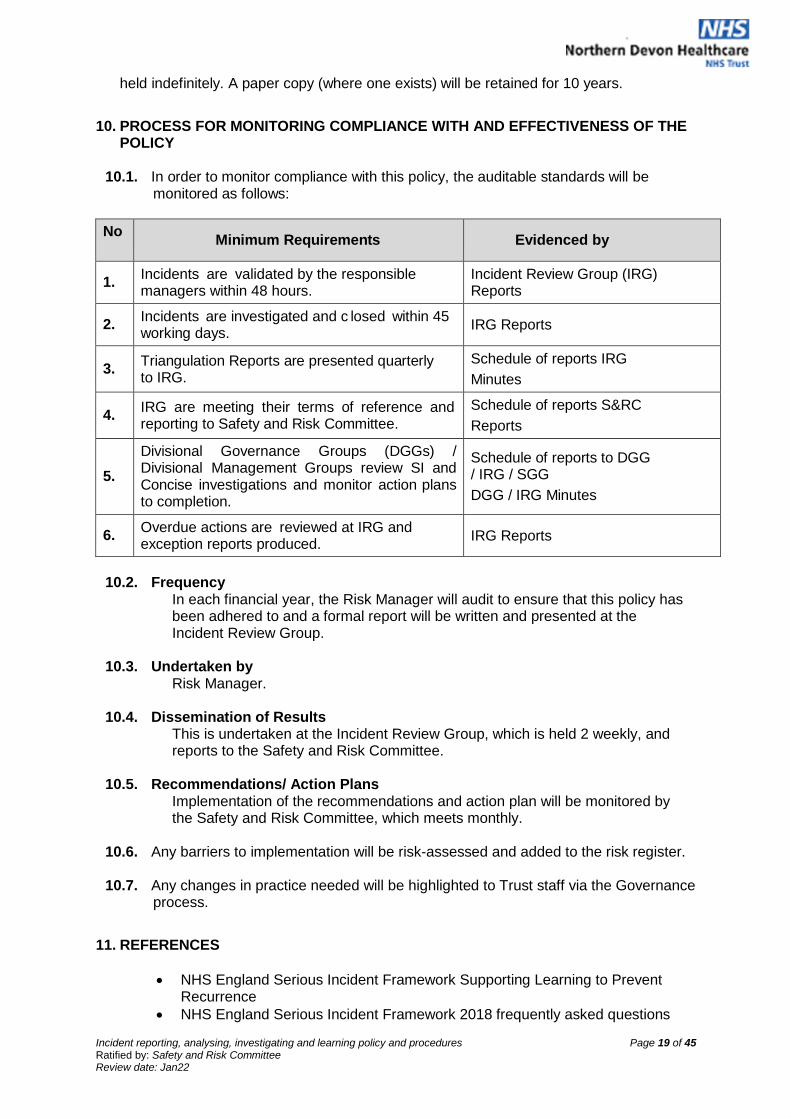
10. PROCESS FOR MONITORING COMPLIANCE WITH AND EFFECTIVENESS OF THE POLICY
10.1. In order to monitor compliance with this policy, the auditable standards will be monitored as follows:
No
Minimum Requirements
Evidenced by
1. Incidents are validated by the responsible managers within 48 hours.
Incident Review Group (IRG) Reports
2. Incidents are investigated and c losed within 45 working days.
IRG Reports
3. Triangulation Reports are presented quarterly to IRG.
Schedule of reports IRG
Minutes
4. IRG are meeting their terms of reference and reporting to Safety and Risk Committee.
Schedule of reports S&RC
Reports
5.
Divisional Governance Groups (DGGs) / Divisional Management Groups review SI and Concise investigations and monitor action plans to completion.
Schedule of reports to DGG / IRG / SGG
DGG / IRG Minutes
6. Overdue actions are reviewed at IRG and exception reports produced.
IRG Reports
10.2. Frequency
In each financial year, the Risk Manager will audit to ensure that this policy has been adhered to and a formal report will be written and presented at the Incident Review Group.
10.3. Undertaken by Risk Manager.
10.4. Dissemination of Results This is undertaken at the Incident Review Group, which is held 2 weekly, and reports to the Safety and Risk Committee.
10.5. Recommendations/ Action Plans Implementation of the recommendations and action plan will be monitored by the Safety and Risk Committee, which meets monthly.
10.6. Any barriers to implementation will be risk-assessed and added to the risk register.
10.7. Any changes in practice needed will be highlighted to Trust staff via the Governance process.
11. REFERENCES
NHS England Serious Incident Framework Supporting Learning to Prevent Recurrence
NHS England Serious Incident Framework 2018 frequently asked questions
Incident reporting, analysing, investigating and learning policy and procedures Page 20 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
NHS England Revised Never Events Policy and Framework
Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 2013. London: Stationery Office. http://www.legislation.gov.uk/uksi/2013/1471/contents/made
National Patient Safety Agency Incident Decision Tree – NPSA
NHS Digital Guide to the Notification of Data Security and Protection Incidents. Reporting incidents post the adoption of GDRP 25 May 2018 and NIS Directive 10 May 2018.
https://www/dsptoolkit.nhs.uk/Help/29 Social Care Act 2012. London: Stationery Office.
http://www.legislation.gov.uk/ukpga/2012/7/contents/enacted
Safety Committees and Safety Representatives Regulations 1977. London: Stationery Office. http://www.legislation.gov.uk/ukpga/2012/7/contents/enacted
Data Protection Act 1998. London: Stationery Office. http://www.legislation.gov.uk/ukpga/1998/29/contents
Memorandum of Understanding
Managing Safety Incidents in NHS Screening Programmes https://www.gov.uk/government/publications/managing-safety-incidents-in-nhs-screening- programmes
Incident reporting, analysing, investigating and learning policy and procedures Page 21 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
12. APPENDIX 1: DEFINITION OF A SERIOUS INCIDENT WITHIN THE NHS FRAMEWORK
Serious incidents in the NHS include:
Acts and/or omissions occurring as part of NHS funded healthcare (including in the community) that result in: o - Unexpected or avoidable death of one or more people. This includes o Suicide / self-inflicted death; and o Homicide by a person in receipt of mental health care within the recent
past o Unexpected or avoidable injury to one or more people that has resulted in
serious harm; o Unexpected or avoidable injury to one or more people that requires further
treatment by a healthcare professional in order to prevent: - o The death of the service user; or o serious harm; o Actual or alleged abuse; sexual abuse, physical or psychological ill-
treatment or acts of omission which constitute neglect, exploitation, financial or material abuse, discriminative and organisational abuse, self-neglect, domestic abuse, human trafficking and modern day slavery where:
o Healthcare did not take appropriate action / intervention to safeguard against such abuse occurring; or
o Where abuse occurred during the provision of NHS funded care. o This includes abuse that resulted in (or was identified through) a Serious
Case Review (SCR), Safeguarding Adult Review (SAR), Safeguarding Adult Enquiry or other externally led investigation, where delivery of NHS funded care caused / contributed towards the incident.
A never event – all never events are defined as serious incidents although not all never events necessarily result in serious harm or death. o An incident (or series of incidents) that prevents, or threatens to prevent,
an organisation’s ability to continue to deliver an acceptable quality of healthcare services, including (but not limited to) the following:
o o Failures in security, integrity, accuracy or availability of information often
described as data loss and / or information governance related issues o Property damage o Security breach / concern o Incidents in population-wide healthcare activities like screening and
immunisation o programmes where the potential for harm may extend to a large
population; o Inappropriate enforcement / care under the Mental Health Act (1983) and
the Mental Capacity Act (2005) including Mental Capacity Act, Deprivation of Liberty Safeguards (MCA DOLS)
o Systematic failure to provide an acceptable standard of safe care (this may include incidents, or series of incidents, which necessitate ward / unit closure or suspension of services)
o Activation of Major Incident Plan (by provider, commissioner or relevant agency)
o Major loss of confidence in the service, including prolonged adverse media coverage or public concern about the quality of healthcare or an organisation.
Incident reporting, analysing, investigating and learning policy and procedures Page 22 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
13. APPENDIX 2: CORE LIST OF NEVER EVENTS 2018 1. Wrong site surgery
An invasive procedure performed on the wrong patient or at the wrong site (eg wrong knee, eye, limb, tooth). The incident is detected at any time after the start of the procedure.
Includes: Interventions that are considered to be surgical but may be done outside a surgical environment – for example, wrong site block (including blocks for pain relief), biopsy, interventional radiology procedure, cardiology procedure, drain insertion and line insertion (eg peripherally inserted central catheter (PICC)/ Hickman lines). This also includes teeth extracted in error that are immediately re-implanted.
Excludes:
removal of wrong primary (milk) teeth unless done under a general anaesthetic
interventions where the wrong site is selected because the patient has unknown/unexpected anatomical abnormalities; these should be documented in the patient’s notes
wrong level spinal surgery
wrong site surgery due to incorrect laboratory reports/results or incorrect referral
letters
contraceptive hormone implant in the wrong arm.
2. Wrong implant / prosthesis
Placement of an implant/prosthesis different from that specified in the procedural plan, either before or during the procedure. The incident is detected any time after the implant/prosthesis is placed in the patient.
Excludes: placed implant/prosthesis is intentionally different from that specified in the
surgical plan, based on clinical judgement at the time of the procedure specified implant/prosthesis is placed as planned but later found to be
suboptimal implant/prosthesis is different from the one specified due to incorrect pre-
procedural measurements or incorrect interpretation of the pre-procedural data – for example, wrong intraocular lens placed due to wrong biometry or using wrong dataset from correct biometry.
Includes: implantation of an intrauterine contraceptive device different from the one in the
procedural plan.
3. Retained foreign object post-operation
Retention of a foreign object in a patient after a surgical/invasive procedure.
‘Surgical/invasive procedure’ includes interventional radiology, cardiology, interventions related to vaginal birth and interventions performed outside the surgical environment – for example, central line placement in ward areas.
‘Foreign object’ includes any items subject to a formal counting/checking process at the start of the procedure and before its completion (such as for swabs, needles,

Incident reporting, analysing, investigating and learning policy and procedures Page 23 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
instruments and guide wires) except where items:
not subject to the formal counting/checking process are inserted any time before the procedure, with the intention of removing them during the procedure but they are not removed
subject to the counting/checking process are inserted during the procedure and then intentionally retained after its completion, with removal planned for a later time or date as clearly recorded in the patient’s notes
are known to be missing before completion of the procedure and may be inside the patient (eg screw fragments, drill bits) but action to locate and/or retrieve them is impossible or more damaging than retention.
4. Mis-selection of a strong potassium containing solution
Mis-selection refers to; When a patient intravenously receives a strong potassium solution rather than
an intended different medication.
5. Administration of medication by the wrong route The patient is given one of the following: Intravenous chemotherapy by the intrathecal route
oral/enteral medication or feed/flush by any parenteral route intravenous administration of an epidural medication that was not intended to be
administered by the intravenous route
6. Overdose of insulin due to abbreviations or incorrect device
Overdose refers to when:
a patient is given a 10-fold or greater overdose of insulin because the words ‘unit’ or ‘international units’ are abbreviated; such an overdose was given in a care setting with an electronic prescribing system
a healthcare professional fails to use a specific insulin administration device – that is, an insulin syringe or pen is not used to measure the insulin
a healthcare professional withdraws insulin from an insulin pen or pen refill and then administers this using a syringe and needle.
7. Overdose of methotrexate for non-cancer treatment
Overdose refers to when:
patient is given a dose of methotrexate, by any route, for non-cancer
treatment that is more than the intended weekly dose; such an overdose was
given in a care setting with an electronic prescribing system.
8. Mis-selection of high strength midazolam during conscious sedation
Mis-selection refers to when:
a patient is given an overdose of midazolam due to the selection of a high strength preparation (5 mg/mL or 2 mg/mL) instead of the 1 mg/mL preparation, in a clinical area performing conscious sedation
excludes clinical areas where the use of high strength midazolam is appropriate; these are generally only those performing general anaesthesia, intensive care, palliative care, or areas where its use has been formally risk-assessed in the organisation.
9. Failure to install functional collapsible shower or curtain rails (mental health only)
Incident reporting, analysing, investigating and learning policy and procedures Page 24 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
10. Falls from poorly restricted windows
A patient falling from poorly restricted window. This applies to:
windows ‘within reach’ of patients; this means windows (including the window sills) that are within reach of someone standing at floor level and that can be exited/fallen from without needing to move furniture or use tools to climb out of the window
windows located in facilities/areas where healthcare is provided and that patients can and do access
where patients deliberately or accidentally fall from a window where a fitted restrictor is damaged or disabled, but not where a patient deliberately disables a restrictor or breaks the window immediately before they fall
where patients can deliberately overcome a window restrictor using their hands or commonly available flat-bladed instruments as well as the ‘key’ provided.
11. Chest or neck entrapment in bedrails
Entrapment of a patient’s chest or neck between bedrails or in the bedframe or
mattress, where the bedrail dimensions or the combined bedrail, bedframe and
mattress dimensions do not comply with Medicines and Healthcare products
Regulatory Agency (MHRA) guidance.
12. Transfusion or transplantation of ABO-incompatible blood components or organs
Unintentional transfusion of ABO-incompatible blood components.
Excludes: where ABO-incompatible blood components are deliberately transfused
with appropriate management.
Unintentional ABO mismatched solid organ transplantation.
Excludes: situations in which clinically appropriate ABO-incompatible solid organs are
deliberately transplanted.
In this context, ‘incompatible’ antibodies must be clinically significant. If the recipient has donor-specific anti-ABO antibodies and is therefore likely to have an immune reaction to a specific ABO-compatible organ, the inadvertent transplantation of that organ without appropriate management is a Never Event.
13. Misplaced naso- or oro-gastric tubes
Misplacement of a naso- or oro-gastric tube in the pleura or respiratory tract that is not
detected before starting a feed, flush or medication administration.
14. Scalding of patients
Patient being scalded by water used for washing/bathing
Excludes:
scalds from water being used for purposes other than washing / bathing
(e.g. from kettles).
Incident reporting, analysing, investigating and learning policy and procedures Page 25 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
15. Unintentional connection of a patient requiring oxygen to an air flowmeter This applies when a patient who requires oxygen is connected to an air
flowmeter when the intention was to connect them to an oxygen flowmeter.
Excludes:
unintentional connection to an air cylinder instead of an oxygen cylinder
as robust barriers to prevent this have not yet been identified.
16. Undetected oesophageal intubation This Never Event has been temporarily suspended pending further clarification

Incident reporting, analysing, investigating and learning policy and procedures Page 26 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
14. APPENDIX 3: INCIDENT REPORTING – WHAT SHOULD BE REPORTED?
Incident Reporting – What should be reported?
An incident is defined as:
Any event that gives (or may give) rise to personal injury or to property loss or
damage. This covers a broad range of events, some examples of which are given
below.
Incidents not only cover events where harm has been caused but also those where a
hazard is identified but no harm has occurred, either due to luck or an error being realised
in time and measures being taken to prevent harm occurring. These are often referred to
as near misses. These are reported in the same way as incidents resulting in harm as it is
expected that for every incident where harm occurs there will be many where no harm is
caused, therefore, these incidents can provide a wealth of learning information.
Any incident identified retrospectively through either audit or mortality reviews will also be reported.
Clinical Incidents / Near Misses
Delays to treatment / care
Failure to obtain valid consent
Inadequate observations / checks undertaken
Medical devices failure / availability
Mislabelled samples / incorrect results
Significant or unexpected complications of a clinical procedure / treatment
Hospitalisation of patients undergoing research trials
Unexpected death*
Blood Transfusion Incidents
*Incidents resulting in unexpected death or serious injury must always be
reported immediately to a senior member of staff (on call manager and named or
on call Consultant as appropriate).
Medication Errors / Near Misses
Prescription error
Administration error
Omission
Inadequate storage
Missing drugs
Adverse Reaction
Personal Accidents / Near Misses
Slips, trips and falls
Needlestick / inoculation injuries (including bites / scratches)
Back injury / musculo-skeletal injuries
Occupational Health / Near Misses
Occupational acquired infection
Occupational acquired dermatitis

Incident reporting, analysing, investigating and learning policy and procedures Page 27 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Infection Control / Near Misses
Infection control outbreaks
Infection control status not handed over
Transfer of patients with infections (C Difficile)
Hospital acquired wound infections Violence, Abuse, Harassment / Near Misses
Verbal abuse
Physical assault
Racial / sexual harassment or any other equality related
Threatening behaviour *All incidents involving an actual assault must be reported to Security who will inform the police
Security Incidents / Near Misses
Absconded / missing patients
Theft / damage to Trust or personal property (including fraud)*
Unsecured premises / windows
Suspicious persons *All incidents involving theft must be reported to Security who will inform the police
Documentation / Near Misses
Inadequate / incomplete health records
Misfiled documentation
Delay in obtaining documentation
Illegible / incorrect documentation
Information Governance / Data Security / Near Misses
Loss / theft inadequately protected electronic data i.e. laptop, unencrypted data stick
Loss / theft of confidential paper documents
Unauthorised access or disclosure of confidential information
Integrity of data is compromised
Capacity Issues
Bed shortages
Staff shortages
Inadequate access to equipment
Pressure Damage
Pressure Ulcers
Moisture Associated skin damage (Moisture Lesions)
Anything that is a cause for concern for patient safety.
Incident reporting, analysing, investigating and learning policy and procedures Page 28 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
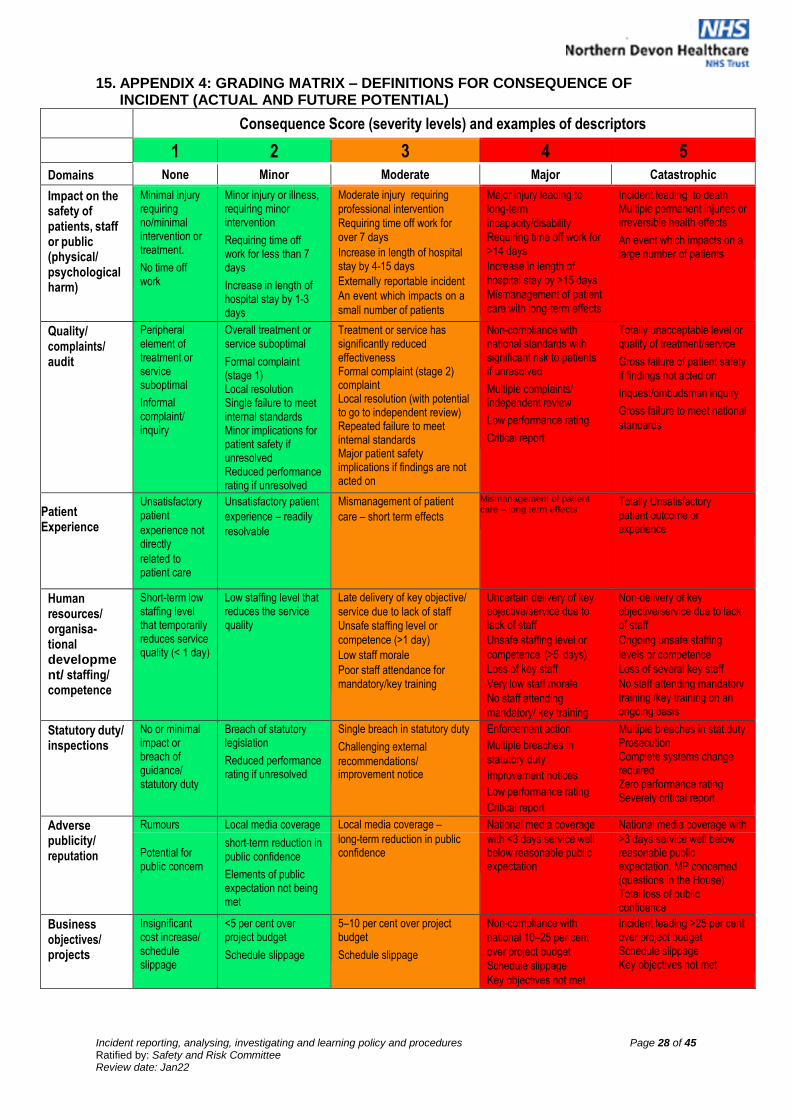
15. APPENDIX 4: GRADING MATRIX – DEFINITIONS FOR CONSEQUENCE OF INCIDENT (ACTUAL AND FUTURE POTENTIAL)
Consequence Score (severity levels) and examples of descriptors
1 2 3 4 5
Domains None Minor Moderate Major Catastrophic
Impact on the safety of patients, staff or public (physical/ psychological harm)
Minimal injury requiring no/minimal intervention or treatment.
No time off work
Minor injury or illness, requiring minor intervention
Requiring time off work for less than 7 days
Increase in length of hospital stay by 1-3 days
Moderate injury requiring
professional intervention
Requiring time off work for
over 7 days
Increase in length of hospital stay by 4-15 days
Externally reportable incident
An event which impacts on a
small number of patients
Major injury leading to
long-term
incapacity/disability
Requiring time off work for >14 days
Increase in length of
hospital stay by >15 days
Mismanagement of patient
care with long-term effects
Incident leading to death Multiple permanent injuries or irreversible health effects
An event which impacts on a large number of patients
Quality/ complaints/ audit
Peripheral element of treatment or service suboptimal
Informal complaint/ inquiry
Overall treatment or service suboptimal
Formal complaint (stage 1) Local resolution Single failure to meet internal standards Minor implications for patient safety if unresolved Reduced performance rating if unresolved
Treatment or service has significantly reduced effectiveness Formal complaint (stage 2) complaint Local resolution (with potential to go to independent review) Repeated failure to meet internal standards Major patient safety implications if findings are not acted on
Non-compliance with national standards with significant risk to patients if unresolved
Multiple complaints/ independent review
Low performance rating
Critical report
Totally unacceptable level or quality of treatment/service
Gross failure of patient safety if findings not acted on
Inquest/ombudsman inquiry
Gross failure to meet national
standards
Patient experience
Patient Experience
Unsatisfactory patient
experience not directly
related to patient care
Unsatisfactory patient
experience – readily
resolvable
Mismanagement of patient
care – short term effects
Mismanagement of patient care – long term effects
Totally Unsatisfactory patient outcome or experience
Human resources/ organisa- tional development/ staffing/ competence
Short-term low staffing level that temporarily reduces service quality (< 1 day)
Low staffing level that reduces the service quality
Late delivery of key objective/
service due to lack of staff
Unsafe staffing level or
competence (>1 day)
Low staff morale
Poor staff attendance for mandatory/key training
Uncertain delivery of key objective/service due to lack of staff
Unsafe staffing level or
competence (>5 days)
Loss of key staff
Very low staff morale
No staff attending
mandatory/ key training
Non-delivery of key objective/service due to lack of staff
Ongoing unsafe staffing
levels or competence
Loss of several key staff
No staff attending mandatory training /key training on an ongoing basis
Statutory duty/ inspections
No or minimal impact or breach of guidance/ statutory duty
Breach of statutory legislation
Reduced performance rating if unresolved
Single breach in statutory duty
Challenging external
recommendations/ improvement notice
Enforcement action
Multiple breaches in
statutory duty
Improvement notices
Low performance rating
Critical report
Multiple breaches in stat.duty Prosecution Complete systems change required Zero performance rating Severely critical report
Adverse Rumours Local media coverage Local media coverage – National media coverage National media coverage with publicity/ reputation
Potential for public concern
short-term reduction in public confidence
Elements of public expectation not being met
long-term reduction in public confidence
with <3 days service well below reasonable public expectation
>3 days service well below reasonable public expectation. MP concerned (questions in the House) Total loss of public confidence
Business objectives/ projects
Insignificant cost increase/ schedule slippage
<5 per cent over project budget
Schedule slippage
5–10 per cent over project budget
Schedule slippage
Non-compliance with
national 10–25 per cent
over project budget
Schedule slippage
Key objectives not met
Incident leading >25 per cent over project budget Schedule slippage Key objectives not met

Incident reporting, analysing, investigating and learning policy and procedures Page 29 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Finance including claims
Small loss Risk of claim remote
Loss of 0.1–0.25 per cent of budget Claim less than £10,000
Loss of 0.25–0.5 per cent of budget
Claim(s) between £10,000 and £100,000
Uncertain delivery of key objective/Loss of 0.5–1.0 per cent of budget
Claim(s) between £100,000 and £1 million
Purchasers failing to pay
Non-delivery of key objective/ Loss of >1 per cent of budget
Failure to meet specification/ slippage
Loss of contract / payment by results. Claim(s) >£1 million
Service/ business
Loss/interruptio
n of >1 hour
Minimal or no
Loss/interruption of >8 hours
Minor impact on
Loss/interruption of >1 day Moderate impact on environment
Loss/interruption of >1 week
Permanent loss of service or facility
interruption Environmental impact
impact on the environment
environment Major impact on environment
Catastrophic impact on environment
Information Governance
No personal data lost
Limited demographic data Less than 10 people
Celebrity /VIP involved. Basic demographic data Limited clinical information 10-50 people
Sensitive personal data, high level of stress / financial loss, 51 – 100 people
Highly sensitive personal data, multiple occurrences of loss, 100 + people
Likelihood Score
1 2 3 4 5
Descriptor Rare Unlikely Possible Likely Almost certain
Frequency How often might it/does it happen
Might happen or recur occasionally
Will probably happen/recur but it is not a persisting issue
Will undoubtedly happen/recur, possibly frequently
This will probably never happen/recur (< once per year)
Do not expect it to happen/ recur but it is possible it may do so
Examples of frequency
Not expected to occur for years or <once/year
Expected to occur at least annually
Expected to occur at least monthly
Expected to occur at least weekly
Expected to occur at least daily
Grading Matrix
Action guidance summary
For Red incident / near misses – Inform the Chief Nurse, Risk Lead, Head of Quality and Safety, and Patient Experience Matron, On-call Senior Manager. Carry out full root cause analysis investigation; formulate action plan and remedial actions. Full investigation / report required
For concise incidents / near misses – Inform Head of Quality and Safety, Risk Manager within 48 hours via automated trigger at grading stage. Carry out a moderate screening tool to ascertain whether a full investigation is required, within 45 days, formulate action plan and remedial actions.
For green incidents – Incident form to be completed and graded within 48 hours. Person
in charge of area to discuss with staff involved. Document any remedial actions on the
electronic copy of the incident form.
Rare 1 Unlikely 2 Possible 3 Likely 4 Almost certain 5
5 Catastrophic 5 10 15 20 25
4 Major 4 8 12 16 20
3 Moderate 3 6 9 12 15
2 Minor 2 4 6 8 10
1 None 1 2 3 4 5

Incident reporting, analysing, investigating and learning policy and procedures Page 30 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Incident Grading Step Guide Stage 1 Actual Impact - The actual impact of the incident is selected from the
consequence table.
The consequence table identifies harm to patients / visitors / staff, number
of persons affected at one time and the impact to the organisation. The
most serious consequence rating (None – Catastrophic) across the three
columns is picked. For example if semi-permanent harm has been caused
and it has affected 25 people the incident would be judged as Major
impact.
Stage 2 Future Potential - The chance of recurrence of a similar incident within
the Trust is selected from the likelihood table (choice of Rare – Certain).
The most likely consequence of a similar incident if it does happen again is
selected (choice of 5 as in stage 1).
This may be different to the actual impact identified in Step 1, for example
the incident may have resulted in no harm occurring on this occasion
because an error was identified and rectified, however, in other
circumstances it would probably have resulted in semi-permanent harm.
Plot the likelihood and consequence on the 5 by 5 matrix to ascertain grade.
In practice categorisation at both stages is subjective and will depend on the
knowledge of the ward/ department manager/ supervisor.
Expert advice (usually by consulting more senior staff or specialist e.g. Infection Control,
Manual Handling Trainer, Occupational Health) should be sought when necessary and
wherever practicable a consensus view should be arrived at by two or more persons with
relevant knowledge.
For additional advice/ support consult the DATIX and incident team.
The initial categorisation of an incident should be undertaken quickly, it is not necessary
for the assessor to be in possession of all the facts at the time of grading. It is always
possible to re- categorise as the facts and issues emerge.
The level of investigation and analysis required for individual events must be dependent
upon the incident categorisation of potential future risk and not whether the incident
resulted in harm or not.

Incident reporting, analysing, investigating and learning policy and procedures Page 31 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
15.1. APPENDIX 5A: INVESTIGATION PROCESS (FLOWCHART)
Investigation Process Flow Chart
None Minor Catastrophic Major Moderate
Grade against grading matrix
Informal Managers investigation
What happened?
Why it happened
Mitigation / Actions
Lessons learnt
Further investigation required?
Feedback/ Sharing
Personal/ Team/ Reporter
Speciality Governance Process
Trend & theme reports
Concise investigation
tool. Completed within
45 working days
Further investigation required
(Significant lapses)
IRG (Externally reportable)
Feedback/ Sharing
IRG Lessons Learnt Newsletter
Discussions at Audit, Team,
Governance and Departmental
Meetings
Escalate immediately
Complete 72 hour report
StEIS reporting decision
Investigation using root cause
analysis methodology and
completed within 45 working
days
Incident Review Group
Commissioners
Feedback/ Sharing
IRG Lessons Learnt Newsletter
Discussions at Audit, Team, Governance
and Departmental Meetings
External / Family sharing
More
Info
YES
NO
YES
YES
NO YES
NO
NO
Use screening tools for incident
Divisional Action planning
Speciality Governance
Divisional Sign Off Legal Review
Complete Duty of Candour within 48 working hours
Local Management Speciality/ Divisional
Management
Divisional/ Organisational Management
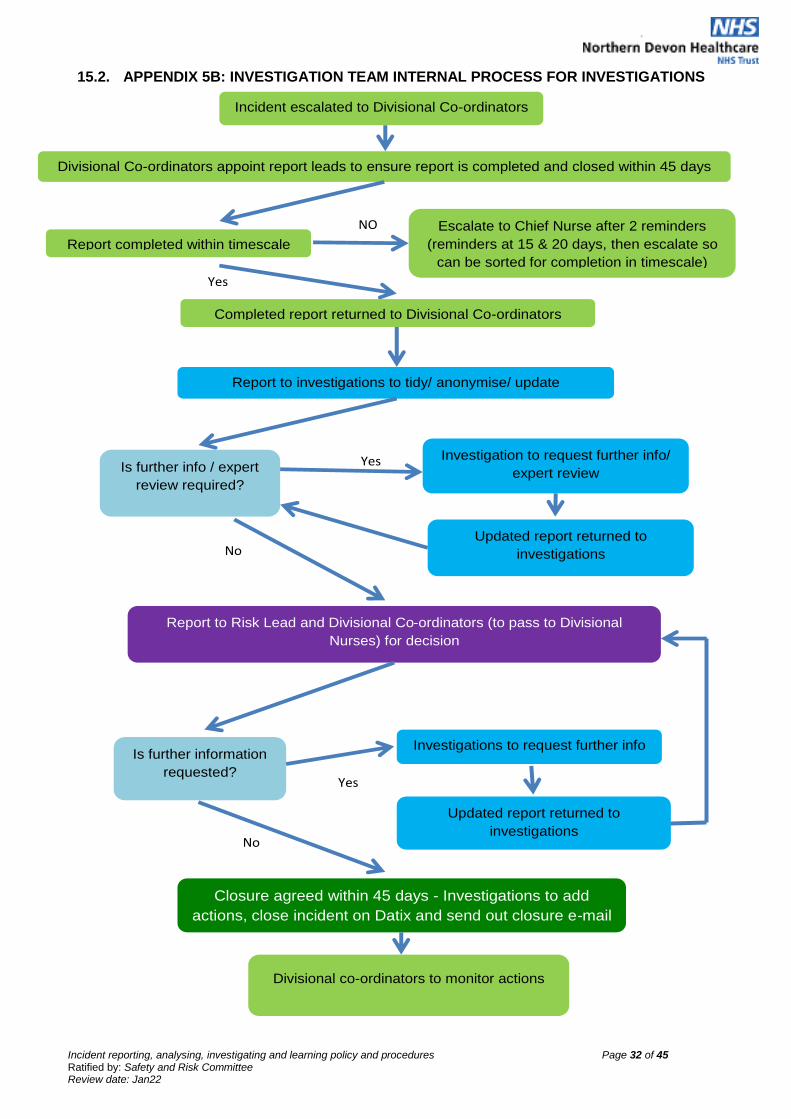
Incident reporting, analysing, investigating and learning policy and procedures Page 32 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
15.2. APPENDIX 5B: INVESTIGATION TEAM INTERNAL PROCESS FOR INVESTIGATIONS
Incident escalated to Divisional Co-ordinators
Divisional Co-ordinators appoint report leads to ensure report is completed and closed within 45 days
Completed report returned to Divisional Co-ordinators
Report to investigations to tidy/ anonymise/ update
Is further info / expert
review required?
Updated report returned to
investigations
Report to Risk Lead and Divisional Co-ordinators (to pass to Divisional
Nurses) for decision
Is further information
requested?
Investigation to request further info/
expert review
Investigations to request further info
Closure agreed within 45 days - Investigations to add
actions, close incident on Datix and send out closure e-mail
Divisional co-ordinators to monitor actions
Updated report returned to
investigations No
Yes
No
Yes
Report completed within timescale
Escalate to Chief Nurse after 2 reminders
(reminders at 15 & 20 days, then escalate so
can be sorted for completion in timescale)
NO
Yes
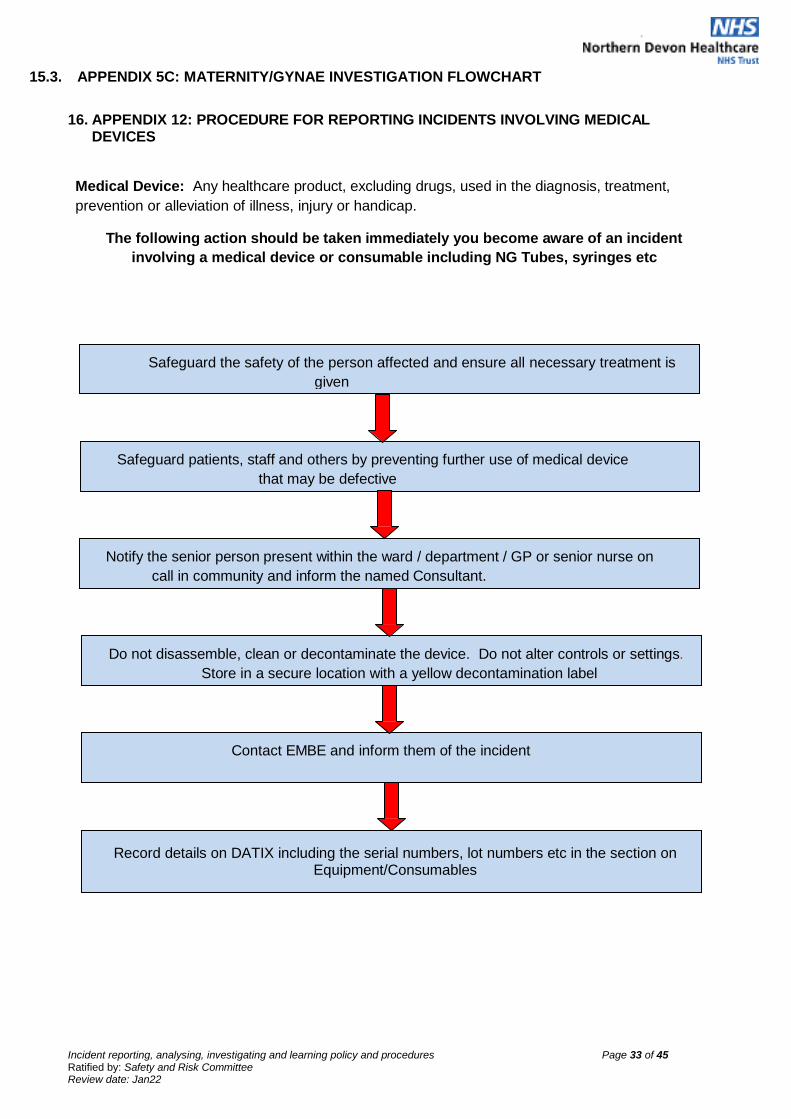
Incident reporting, analysing, investigating and learning policy and procedures Page 33 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Safeguard the safety of the person affected and ensure all necessary treatment is
given
15.3. APPENDIX 5C: MATERNITY/GYNAE INVESTIGATION FLOWCHART
16. APPENDIX 12: PROCEDURE FOR REPORTING INCIDENTS INVOLVING MEDICAL DEVICES
Medical Device: Any healthcare product, excluding drugs, used in the diagnosis, treatment,
prevention or alleviation of illness, injury or handicap.
The following action should be taken immediately you become aware of an incident
involving a medical device or consumable including NG Tubes, syringes etc
Safeguard patients, staff and others by preventing further use of medical device
that may be defective
Notify the senior person present within the ward / department / GP or senior nurse on
call in community and inform the named Consultant.
Do not disassemble, clean or decontaminate the device. Do not alter controls or settings.
Store in a secure location with a yellow decontamination label
Contact EMBE and inform them of the incident
Record details on DATIX including the serial numbers, lot numbers etc in the section on Equipment/Consumables
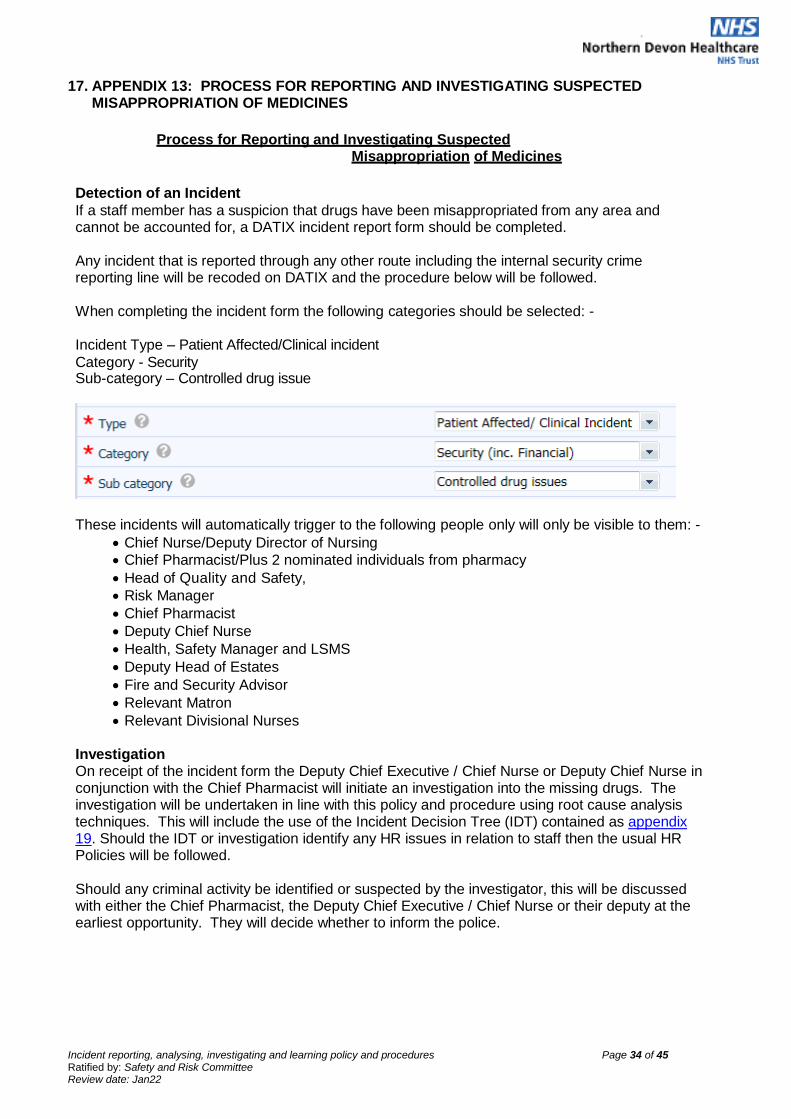
Incident reporting, analysing, investigating and learning policy and procedures Page 34 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
17. APPENDIX 13: PROCESS FOR REPORTING AND INVESTIGATING SUSPECTED MISAPPROPRIATION OF MEDICINES
Process for Reporting and Investigating Suspected
Misappropriation of Medicines
Detection of an Incident
If a staff member has a suspicion that drugs have been misappropriated from any area and cannot be accounted for, a DATIX incident report form should be completed.
Any incident that is reported through any other route including the internal security crime reporting line will be recoded on DATIX and the procedure below will be followed.
When completing the incident form the following categories should be selected: -
Incident Type – Patient Affected/Clinical incident
Category - Security Sub-category – Controlled drug issue
These incidents will automatically trigger to the following people only will only be visible to them: -
Chief Nurse/Deputy Director of Nursing
Chief Pharmacist/Plus 2 nominated individuals from pharmacy
Head of Quality and Safety,
Risk Manager
Chief Pharmacist
Deputy Chief Nurse
Health, Safety Manager and LSMS
Deputy Head of Estates
Fire and Security Advisor
Relevant Matron
Relevant Divisional Nurses Investigation On receipt of the incident form the Deputy Chief Executive / Chief Nurse or Deputy Chief Nurse in conjunction with the Chief Pharmacist will initiate an investigation into the missing drugs. The investigation will be undertaken in line with this policy and procedure using root cause analysis techniques. This will include the use of the Incident Decision Tree (IDT) contained as appendix 19. Should the IDT or investigation identify any HR issues in relation to staff then the usual HR Policies will be followed.
Should any criminal activity be identified or suspected by the investigator, this will be discussed with either the Chief Pharmacist, the Deputy Chief Executive / Chief Nurse or their deputy at the earliest opportunity. They will decide whether to inform the police.

Incident reporting, analysing, investigating and learning policy and procedures Page 35 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
18. APPENDIX 14: DUTY OF CANDOUR PROCESS
Process to be followed for Duty of Candour
This is a contractual duty as well as being a legal duty under the Health and Social Care Act 2008
(Regulated Activities) Regulations 2014: Regulation 20. The legal duty of candour applies to patient safety
incidents that occur during care provided and that results in moderate harm, severe harm or death,
Prolonged pain or Psychological Harm. However, low / no harm incidents should still be reported to the
patient if appropriate and an apology given.
Verbal
Apology
as soon as
practically
possible
Written Apology
Within 10 working
days of incident
Immediate mitigating actions
1. Escalation – to line manager
2. Ascertain level of harm
(Moderate, Major or Catastrophic impact)
As outlined in the GMC/NMC Guidance 2015
3. Tell the patient* something has gone wrong.
4. Apologise to the patient and give them the duty of candour information leaflet.
5. Offer an appropriate remedy or support to put things
right (if possible).
6. Explain fully to the patient the short or long- term
effects of what has happened.
7. Identify a point of contact for the patient to use
during the investigation process and document these
in the patient information leaflet. This would usually be
the manager of the service/department
8. Invite the patient to be involved in the
investigation process.
9. Document the conversation in both the medical
and nursing notes. In an inpatient setting populate
the Duty of candour sticker (Appendix 15) and
apply to the medical and nursing notes. In the
community setting, chose the duty of candour
assessment in RIO, populate with the relevant
information and add to the patients progress notes.
10. On a daily basis the divisional co-coordinators for each division will access the medium and high harm incident Datix dashboard. Once patients have been identified the medical record will be accessed to determine the patients involvement in the investigation. A template letter (Appendix 16) will be populated by the divisional coordinators and signed by the divisional nurse.
11. Outline the Trust's investigation process.
12. Signed copy of letter to be uploaded to DATIX and initial Duty of Candour action closed.
*Patient: or, where appropriate, the patient's advocate, carer or family
INCIDENT
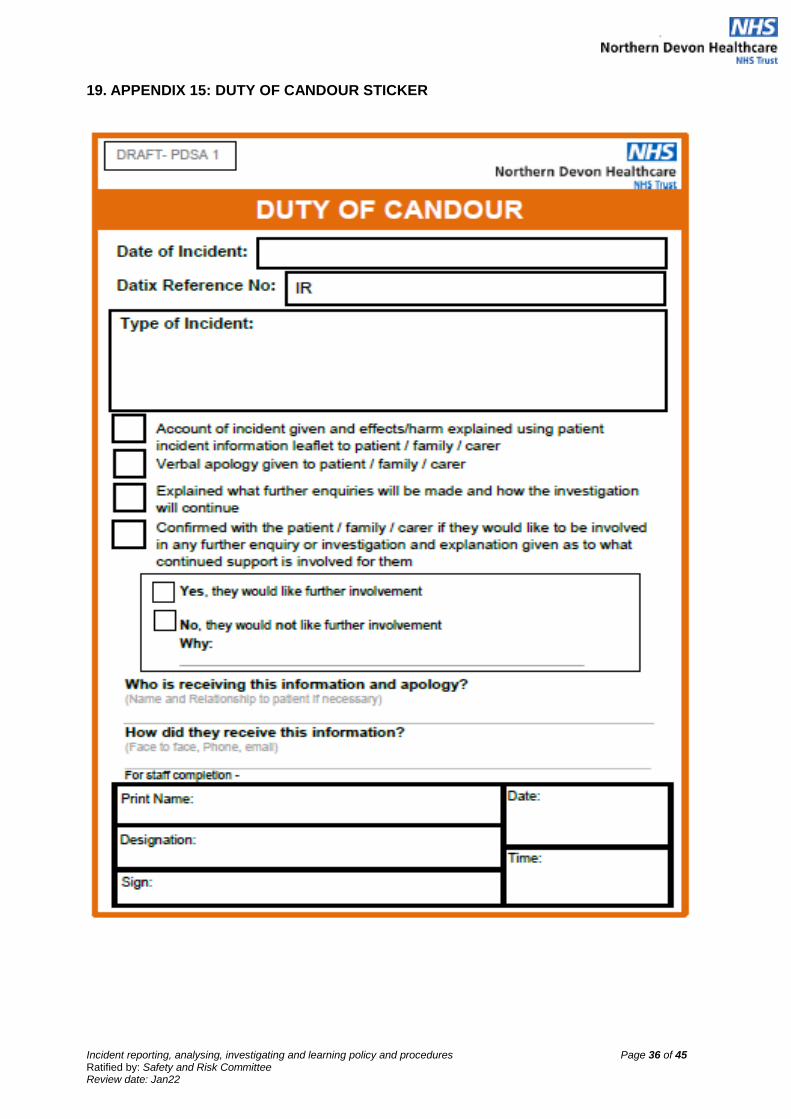
Incident reporting, analysing, investigating and learning policy and procedures Page 36 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
19. APPENDIX 15: DUTY OF CANDOUR STICKER
Incident reporting, analysing, investigating and learning policy and procedures Page 37 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
20. APPENDIX 16: DUTY OF CANDOUR LETTER TEMPLATE
Private and Confidential NAME ADDRESS ADDRESS ADDRESS ADDRESS POSTCODE DATE
North Devon District Hospital Raleigh Park
Barnstaple, Devon EX31 4JB
Direct line: 01271 XXXXX
Our ref: XXXXX
Dear NAME I am writing further to our telephone conversation on date, and would like to thank you for taking the time to speak with me regarding your mother’s/father’s, etc care and treatment. I would like to take this opportunity of sending you my sincere condolences on the sad loss of your mother/father, etc (if appropriate). As explained in our discussions the main reason for my call was to advise you that there were aspects of your mother’s/father’s, etc care and treatment which the Trust would wish to review. This review is called a 72 hour report/a Concise Investigation)/a SI (serious incident requiring investigation). This investigation is a formal framework where particular events are revisited, simply with the aim of identifying what happened, why it happened and if there is anything which could be put in place to reduce the chance of it happening again. The Trust is required to advise you of this review, and I would also like to reassure you that the Trust would want to advise you of the process, in the spirit of openness and honesty. As discussed in my telephone call once the 72 hour report/Concise Investigation/SI (serious incident requiring investigation) is finalised, hopefully in date (month/year), I will send you a copy, and should you wish to meet with the staff involved in the investigation I would be happy to arrange this, if you would feel it beneficial. However in the meantime please do not hesitate to call me on my direct line (01271) XXXXXX or via email on [email protected] should you wish to discuss any aspect of the investigation or report.
Yours sincerely NAME Divisional coordinator on behalf of the Divisional Nurse

Incident reporting, analysing, investigating and learning policy and procedures Page 38 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
21. APPENDIX 17 CARDIAC ARREST REPORTING FLOWCHART
Incident reporting, analysing, investigating and learning policy and procedures Page 39 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
22. APPENDIX 18: REPORTING
REPORTING ‘SIGNIFICANT EVENTS’ / INCIDENTS EXTERNALLY AND INVOLVING OTHER STAKEHOLDERS IN INVESTIGATING
The Commissioners
The Investigations Team will report incidents to the CCG via the StEIS reporting system.
This includes all incidents set out in Appendix 1.
The Health and Safety Executive
RIDDOR (Reporting of Injuries, Diseases and Dangerous Occurrences Regulations)
reportable incidents are notified to the HSE via the Health and Safety Manager. If the serious
incident requires joint investigation by the organisation and the HSE and the Police, the
Memorandum of Understanding will be activated.
The NRLS (National Reporting and Learning System)
All patient safety incidents / near misses are uploaded weekly from Datix by the DATIX and
incident Team.
The MHRA (Medicines and Healthcare Products Regulatory Agency)
The Facilities Clinical Services Manager report in conjunction with Medical Electronics
any significant events / concerns with Medical Devices.
Care Quality Commission [CQC]
The requirement to report incidents is typically met by reporting incidents to the National
Reporting and Learning System (NRLS). However, the Head of Governance will notify the
appropriate regulator, about incidents that indicate, or may indicate, risks to on-going
compliance with registration requirements, or that lead, or may lead to changes in the details
about the organisation in the regulators register according to the CQC regulatory framework.
Reporting Serious Adverse Blood Reactions and Incidents (SABRE)
The Trust Transfusion Team (Transfusion Practitioner, Blood Bank Manager, Blood
Conservation Specialty Doctor and Quality Manager) in line with the UK Blood Safety and
Quality Regulations 2005 and the EU Blood Safety Directive will report serious adverse
incidents and serious adverse reactions related to blood and blood components to the
MHRA, the UK Competent Authority for Blood Safety. This information is vital to the work
that the Serious Hazards of Transfusion (SHOT) uses to compile its reports.
IRMER (Ionising Regulations for Medical Exposure to Radiation) Reportable Incidents
IRMER incidents are reported by the Trust Radiation Protection Advisor. The Human Tissue Authority
Incidents relating to the collection or storage of human tissue for research should be reported
on Datix and the HTA indictor must be selected. The Trust’s HTA Lead will notify the HTA of
all incidents that are described in the HTA Reportable Incidents in the Post Mortem Sector
document http://www.hta.gov.uk/_db/_documents/Guidance_for_reporting_HTARIs.pdf
Early Notification Scheme for maternity incidents (NHS resolution)
NHS Resolution require all providers to report all maternity incidents that occur on or after 1
April 2017 which are likely to result in severe brain injury. These cases have the potential to
become high value compensation claims and are defined below:
Babies born at term (≥37 completed weeks of gestation), following labour, with a
severe brain injury diagnosed in the first seven days of life, namely babies that have

Incident reporting, analysing, investigating and learning policy and procedures Page 40 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
one or more of the following:
Diagnosed with grade III hypoxic ischaemic encephalopathy (HIE);
Actively therapeutically cooled;
Have all three of the following signs: decreased central tone; comatose; seizures of
any kind.
The above criteria have been identified by the Royal College of Obstetricians and
Gynaecologists (RCOG) (Each Baby Counts Programme) as being potential markers for
avoidable severe brain injury at birth.
Healthcare Safety Investigation Branch (HSIB)
HSIB •conduct a portion of investigations each year to provide safety recommendations, they
provide thorough, independent, impartial and timely investigations into clinical incidents.
Sharing what they learn across the whole of the healthcare system for the benefit of everyone
who is cared for by it and works in it.
The HSIB investigate incidents that meet the Each Baby Counts criteria or their defined
criteria for maternal deaths. Each Baby Counts (RCOG) 1. Intrapartum stillbirth;
2. Early neonatal death: when the baby died within the first week of life (i.e. days 0–6) of any
cause; 3. Severe brain injury diagnosed in the first seven days of life.
• diagnosed with grade III hypoxic ischaemic encephalopathy (HIE)
OR
• Was therapeutically cooled (active cooling only)
OR
• Had decreased central tone AND was comatose AND had seizures of any kind
The Trust notifies the HSIB when an incident meets these criteria.
Screening
The Trust Hospital Based Programme Coordinator will follow the Guidelines for Managing
Safety Incidents in NHS Screening Programmes in the event of an incident.
Guidelines for Managing Safety Incidents in NHS Screening Programmes
Information Governance, Caldicott and Data Protection
Information Governance SIs will be reported via the DSP toolkit in line with NHS Digital Guide
to the Notification of Data Security and Protection Incidents by the Information Governance
Manager / Deputy. National NHS Reporting Guidelines.
Public Health England
Infection, Prevention and Control – where incidents have the potential to affect population
health, will seek advice from the local PHE Centre. Depending on the nature of the incident,
other public health organisations such as local authorities may need to be involved. Such
incidents will include those with a health protection component, such as failures in
decontamination. The PHE Centre health protection staff will provide a risk assessment and
advise on appropriate action.
If more than one organisation is involved in a significant event, the organisation that has
discovered the incident will make the initial report. A meeting will then be arranged to include
all key stakeholders. A lead professional will be identified to manage, lead and co-ordinate
the incident, procedure and investigation. All key stakeholders will contribute and work
together with the nominated lead and lessons will be shared with all stakeholders. The
Memorandum of Understanding Concordat Agreement outlines the arrangements for

Incident reporting, analysing, investigating and learning policy and procedures Page 41 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
investigations involving the NHS, Police and HSE.
Defects and Failures
The Estates Management Team will report incidents that relate to a defect or failure involving
engineering plants, infrastructure and/or non-medical devices, a defect and failure report will
also be submitted to the Department of Health via the defect and failure portal

Incident reporting, analysing, investigating and learning policy and procedures Page 42 of 45 Ratified by: Safety and Risk Committee Review date: Jan22
Page 42 of 45
23. APPENDIX 19 Just Culture guide
Incident reporting, analysing, investigating and learning policy and procedures Page 43 of 45 Ratified by: Safety and Risk Committee – Review date: October 2022
24. APPENDIX 20: EQUALITY IMPACT ASSESSMENT TOOL
Name of document
Incident reporting, analysing, investigating and learning policy and procedures
Division/Directorate and service area Trustwide
Name, job title and contact details of
person completing the assessment
Julie Poyner, Head of Governance
Date completed: 20/09/2019
The purpose of this tool is to:
identify the equality issues related to a policy, procedure or strategy summarise the work done during the development of the document to reduce
negative impacts or to maximise benefit highlight unresolved issues with the policy/procedure/strategy which cannot be
removed but which will be monitored, and set out how this will be done.
1. What is the main purpose of this document?
This policy sets out the Trust systems, processes and expectations in relation
to incident reporting and learning
Compliance with this policy will ensure that incidents are systematically identified,
recorded, reported to management and appropriately investigated. This will result in
learning and thus improving safety for future patients, staff and visitors.
2. Who does it mainly affect? (Please insert an “x” as appropriate:)
Carers ☒ Staff ☒ Patients ☒ Other (please specify)
3. Who might the policy have a ‘differential’ effect on, considering the “protected characteristics” below? (By differential we mean, for example that a policy may have a noticeably more positive or negative impact on a particular group e.g. it may be more beneficial for women than for men)
Please insert an “x” in the appropriate box (x)
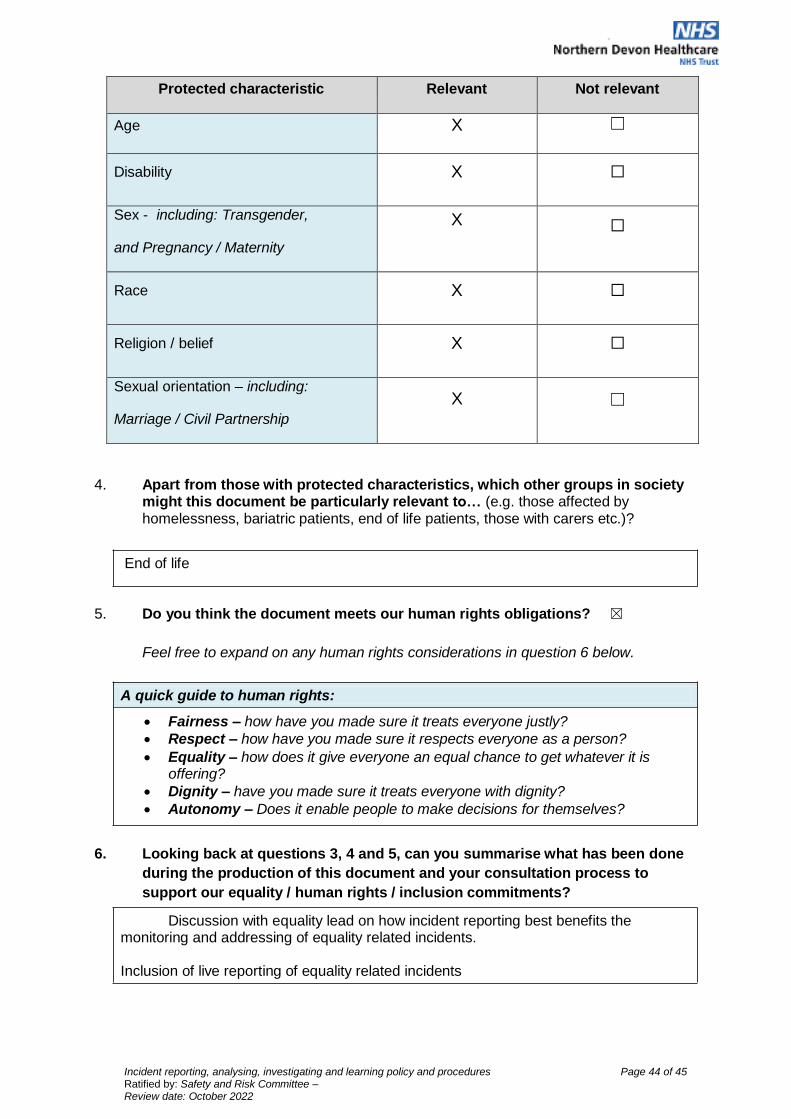
Incident reporting, analysing, investigating and learning policy and procedures Page 44 of 45 Ratified by: Safety and Risk Committee – Review date: October 2022
Protected characteristic Relevant Not relevant
Age X ☐
Disability X ☐
Sex - including: Transgender, and Pregnancy / Maternity
X ☐
Race X ☐
Religion / belief X ☐
Sexual orientation – including: Marriage / Civil Partnership
X
☐
4. Apart from those with protected characteristics, which other groups in society might this document be particularly relevant to… (e.g. those affected by homelessness, bariatric patients, end of life patients, those with carers etc.)?
End of life
5. Do you think the document meets our human rights obligations? ☒
Feel free to expand on any human rights considerations in question 6 below.
A quick guide to human rights:
Fairness – how have you made sure it treats everyone justly?
Respect – how have you made sure it respects everyone as a person?
Equality – how does it give everyone an equal chance to get whatever it is offering?
Dignity – have you made sure it treats everyone with dignity?
Autonomy – Does it enable people to make decisions for themselves?
6. Looking back at questions 3, 4 and 5, can you summarise what has been done
during the production of this document and your consultation process to
support our equality / human rights / inclusion commitments?
Discussion with equality lead on how incident reporting best benefits the monitoring and addressing of equality related incidents.
Inclusion of live reporting of equality related incidents
Incident reporting, analysing, investigating and learning policy and procedures Page 45 of 45 Ratified by: Safety and Risk Committee – Review date: October 2022
7. If you have noted any ‘missed opportunities’, or perhaps
noted that there remains some concern about a
potentially negative impact please note this below and how this will be
monitored/addressed.
“Protected characteristic”: None
Issue:
How is this going to be
monitored/ addressed in the
future:
Group that will be responsible
for ensuring this carried out:
All equality impact assessments will need the involvement of somebody beyond the policy author to provide insight and guidance. If you need help with any aspect of this assessment, please contact either (for patient related policies/procedures/strategies) or (for human resources). Both can be contacted via (if you are using the generic email please can you indicate whether you feel this is predominantly patient or staff related).
Please note: apart from seeking guidance during the development of the policy/strategy, etc., this impact assessment form also needs to be approved by an appropriate equality lead prior to final ratification of the policy.

















