Incidence of ESBL Producers amongst Gram-negative Bacilli … · monitor in vitro susceptibility of...
6
© JAPI • MAY 2011 • VOL. 59 1 Abstract Objectives: This study was conducted in 9 centers spread over India from January 1 to December 31, 2007 to monitor in vitro susceptibility of Gram-negative bacilli to Group I carbapenem, ertapenem and other antimicrobials in intra-abdominal infections and to identify early changes in susceptibility pattern of community or hospital acquired organisms, with a focus on ESBL producers. Material and Methods: Gram-negative bacilli isolated from intra-abdominal samples of patients with documented intra-abdominal infections were processed for identification by conventional/ automated methods and antimicrobial susceptibility by Micro-Scan (Siemens) MIC panel against 12 antimicrobials (3 rd and 4 th generation cephalosporins, Groups I and II carbapenems, amikacin, levofloxacin, amoxicillin-clavulanic acid and piperacillin-tazobactam). Results: A total of 588 isolates were identified, of which 351 (60%) were E. coli and 114 (19%) were Klebsiella spp. 79% of E. coli and 70% of Klebsiella spp. were ESBL producers in general. 110 of E. coli and 35 of Klebsiella isolates were from community-acquired intra-abdominal infections. 80% of E. coli and 63% of Klebsiella isolates from community-acquired infections were ESBL producers, against 79% of E. coli and 73% of Klebsiella isolates from hospital-acquired infections. Amongst the ESBL-positive isolates of E. coli, 94% were susceptible in vitro to ertapenem, 96% to imipenem and 76% to piperacillin-tazobactam. For ESBL-positive isolates of Klebsiella spp., the corresponding figures were 80%, 94% and 59% respectively. Conclusion: The study showed a high incidence of ESBL-producers amongst Enterobacteriaceae isolates from intra-abdominal infections in both community-acquired and hospital-acquired settings across India. Ertapenem was comparable with imipenem against ESBL-positive E. coli isolates, while imipenem was more effective than ertapenem against ESBL-positive Klebsiella isolates. 1 AMRI Hospitals, Salt Lake, Kolkata; 2 PD Hinduja National Hospital, Mumbai; 3 Christian Medical College, Vellore; 4 Global Hospitals, Hyderabad; 5 Sri Ramchandra Medical College, Chennai; 6 Sir Ganga Ram Hospital, Delhi; 7 Choithram Hospital, Indore; 8 SGPGI, Lucknow; 9 Manipal Hospitals, Bangalore Received: 17.03.2010; Revised: 19.05.2010; Accepted: 22.06.2010 Rationale T he emergence of drug-resistant organisms in both hospitals and the community is a major concern. Surveillance studies have provided important information about changes in the spectrum of microbial pathogens and trends in the antimicrobial resistance paerns in nosocomial and community-acquired infections and continued monitoring of antimicrobial resistance paerns in hospitals is essential to guide effective empirical therapy. One of the considerations of hospital formulary commiees when considering new antibiotics is the potential for altering the bacterial flora epidemiology, especially resistance rates. Large multi-centre studies are useful for tracking trends over wide geographic areas and over long periods of time. However, most of these studies are not designed to identify early changes in susceptibility paerns or to determine the importance of specific risk factors in promoting resistance. In addition, such studies are not ideally suited to monitor the effect of introduction of new antibiotic because of variable use across the participating centers. The purpose of SMART (Study for Monitoring Antimicrobial Resistance Trends) is two-fold: 1. To monitor the susceptibility of organisms causing intra-abdominal infections).Recent data indicate that the organisms causing these infections exhibit a high degree of susceptibility to drugs as ertapenem but long term surveillance is required to monitor for any important changes in susceptibility of common pathogens; Aims and Objectives SMART (Study for Monitoring Antimicrobial Resistance Trends), 2007 was conducted worldwide to 1. Monitor, globally and longitudinally, the in vitro susceptibility of Gram-negative bacilli to Group I carbapenem, ertapenem and other antimicrobials in intra-abdominal infections, focusing on isolates causing intra-abdominal infections in patients admied in all sections of the hospital; 2. Identify early changes in susceptibility patterns based on bacterial population MICs, of community or hospital acquired organisms, with a focus on ESBL producers. The present publication focuses on the observations of SMART in India where the study was conducted in 9 centers spread all over the country from January 1 to December 31, 2007. Original Article Incidence of ESBL Producers amongst Gram-negative Bacilli Isolated from Intra-abdominal Infections across India (Based on SMART Study, 2007 Data) BN Chaudhuri 1 , C Rodrigues 2 , V Balaji 3 , R Iyer 4 , U Sekar 5 , Chand Waal 6 , DS Chitnis 7 , TN Dhole 8 , Sangeeta Joshi 9
Transcript of Incidence of ESBL Producers amongst Gram-negative Bacilli … · monitor in vitro susceptibility of...
© JAPI • mAy 2011 • VOL. 59 1
AbstractObjectives: This study was conducted in 9 centers spread over India from January 1 to December 31, 2007 to monitor in vitro susceptibility of Gram-negative bacilli to Group I carbapenem, ertapenem and other antimicrobials in intra-abdominal infections and to identify early changes in susceptibility pattern of community or hospital acquired organisms, with a focus on ESBL producers.Material and Methods: Gram-negative bacilli isolated from intra-abdominal samples of patients with documented intra-abdominal infections were processed for identification by conventional/ automated methods and antimicrobial susceptibility by micro-Scan (Siemens) mIC panel against 12 antimicrobials (3rd and 4th generation cephalosporins, Groups I and II carbapenems, amikacin, levofloxacin, amoxicillin-clavulanic acid and piperacillin-tazobactam).Results: A total of 588 isolates were identified, of which 351 (60%) were E. coli and 114 (19%) were Klebsiella spp. 79% of E. coli and 70% of Klebsiella spp. were ESBL producers in general. 110 of E. coli and 35 of Klebsiella isolates were from community-acquired intra-abdominal infections. 80% of E. coli and 63% of Klebsiella isolates from community-acquired infections were ESBL producers, against 79% of E. coli and 73% of Klebsiella isolates from hospital-acquired infections. Amongst the ESBL-positive isolates of E. coli, 94% were susceptible in vitro to ertapenem, 96% to imipenem and 76% to piperacillin-tazobactam. For ESBL-positive isolates of Klebsiella spp., the corresponding figures were 80%, 94% and 59% respectively.Conclusion: The study showed a high incidence of ESBL-producers amongst Enterobacteriaceae isolates from intra-abdominal infections in both community-acquired and hospital-acquired settings across India. Ertapenem was comparable with imipenem against ESBL-positive E. coli isolates, while imipenem was more effective than ertapenem against ESBL-positive Klebsiella isolates.
1AmRI Hospitals, Salt Lake, Kolkata; 2PD Hinduja National Hospital, mumbai; 3Christian medical College, Vellore; 4Global Hospitals, Hyderabad; 5Sri Ramchandra medical College, Chennai; 6Sir Ganga Ram Hospital, Delhi; 7Choithram Hospital, Indore; 8SGPGI, Lucknow; 9manipal Hospitals, BangaloreReceived: 17.03.2010; Revised: 19.05.2010; Accepted: 22.06.2010
Rationale
The emergence of drug-resistant organisms in both hospitals and the community is a major concern. Surveillance studies
have provided important information about changes in the spectrum of microbial pathogens and trends in the antimicrobial resistance patterns in nosocomial and community-acquired infections and continued monitoring of antimicrobial resistance patterns in hospitals is essential to guide effective empirical therapy.
One of the considerations of hospital formulary committees when considering new antibiotics is the potential for altering the bacterial flora epidemiology, especially resistance rates. Large multi-centre studies are useful for tracking trends over wide geographic areas and over long periods of time. However, most of these studies are not designed to identify early changes in susceptibility patterns or to determine the importance of specific risk factors in promoting resistance. In addition, such studies are not ideally suited to monitor the effect of introduction of new antibiotic because of variable use across the participating centers.
The purpose of SmART (Study for monitoring Antimicrobial Resistance Trends) is two-fold: 1. To monitor the susceptibility of organisms causing
intra-abdominal infections).Recent data indicate that the organisms causing these infections exhibit a high degree of susceptibility to drugs as ertapenem but long term surveillance is required to monitor for any important changes in susceptibility of common pathogens;
Aims and ObjectivesSmART (Study for monitoring Antimicrobial Resistance
Trends), 2007 was conducted worldwide to1. monitor, globally and longitudinally, the in vitro susceptibility
of Gram-negative bacilli to Group I carbapenem, ertapenem and other antimicrobials in intra-abdominal infections, focusing on isolates causing intra-abdominal infections in patients admitted in all sections of the hospital;
2. Identify early changes in susceptibility patterns based on bacterial population mICs, of community or hospital acquired organisms, with a focus on ESBL producers.
The present publication focuses on the observations of SmART in India where the study was conducted in 9 centers spread all over the country from January 1 to December 31, 2007.
Original Article
Incidence of ESBL Producers amongst Gram-negative Bacilli Isolated from Intra-abdominal Infections across India (Based on SMART Study, 2007 Data)BN Chaudhuri1, C Rodrigues2, V Balaji3, R Iyer4, U Sekar5, Chand Wattal6, DS Chitnis7, TN Dhole8, Sangeeta Joshi9
2 © JAPI • mAy 2011 • VOL. 59
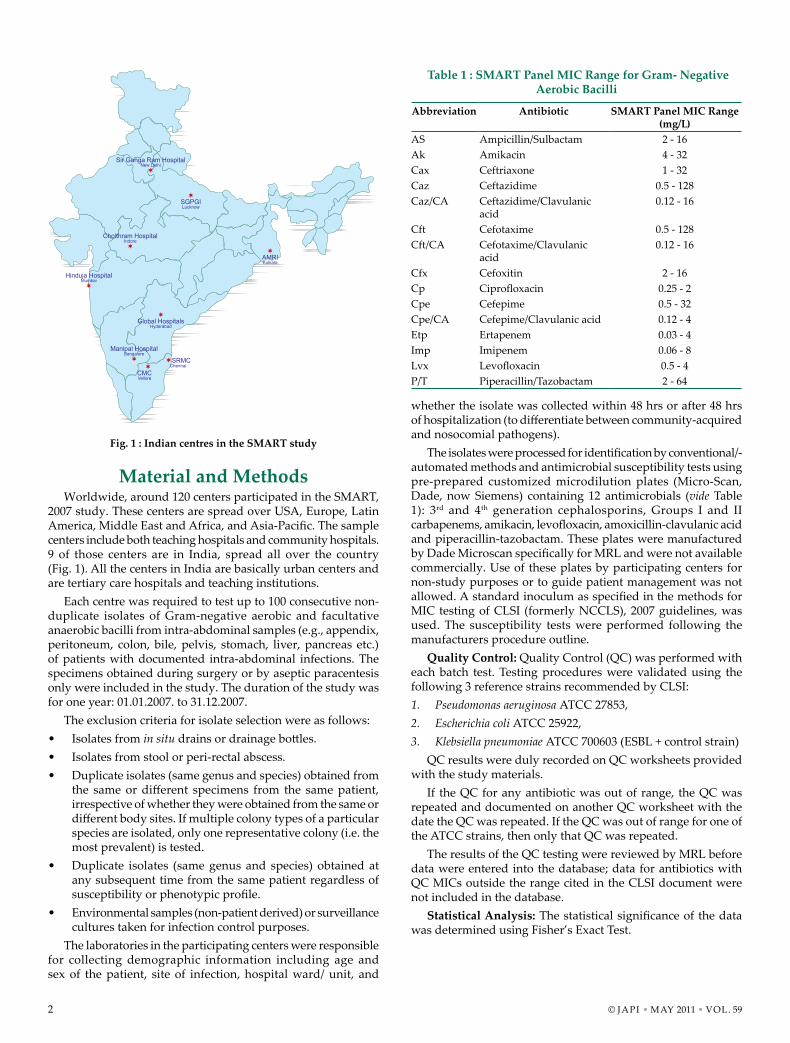
whether the isolate was collected within 48 hrs or after 48 hrs of hospitalization (to differentiate between community-acquired and nosocomial pathogens).
The isolates were processed for identification by conventional/-automated methods and antimicrobial susceptibility tests using pre-prepared customized microdilution plates (micro-Scan, Dade, now Siemens) containing 12 antimicrobials (vide Table 1): 3rd and 4th generation cephalosporins, Groups I and II carbapenems, amikacin, levofloxacin, amoxicillin-clavulanic acid and piperacillin-tazobactam. These plates were manufactured by Dade Microscan specifically for MRL and were not available commercially. Use of these plates by participating centers for non-study purposes or to guide patient management was not allowed. A standard inoculum as specified in the methods for mIC testing of CLSI (formerly NCCLS), 2007 guidelines, was used. The susceptibility tests were performed following the manufacturers procedure outline.
Quality Control: Quality Control (QC) was performed with each batch test. Testing procedures were validated using the following 3 reference strains recommended by CLSI:1. Pseudomonas aeruginosa ATCC 27853,2. Escherichia coli ATCC 25922,3. Klebsiella pneumoniae ATCC 700603 (ESBL + control strain)
QC results were duly recorded on QC worksheets provided with the study materials.
If the QC for any antibiotic was out of range, the QC was repeated and documented on another QC worksheet with the date the QC was repeated. If the QC was out of range for one of the ATCC strains, then only that QC was repeated.
The results of the QC testing were reviewed by mRL before data were entered into the database; data for antibiotics with QC mICs outside the range cited in the CLSI document were not included in the database.
Statistical Analysis: The statistical significance of the data was determined using Fisher’s Exact Test.
Material and MethodsWorldwide, around 120 centers participated in the SmART,
2007 study. These centers are spread over USA, Europe, Latin America, Middle East and Africa, and Asia-Pacific. The sample centers include both teaching hospitals and community hospitals. 9 of those centers are in India, spread all over the country (Fig. 1). All the centers in India are basically urban centers and are tertiary care hospitals and teaching institutions.
Each centre was required to test up to 100 consecutive non-duplicate isolates of Gram-negative aerobic and facultative anaerobic bacilli from intra-abdominal samples (e.g., appendix, peritoneum, colon, bile, pelvis, stomach, liver, pancreas etc.) of patients with documented intra-abdominal infections. The specimens obtained during surgery or by aseptic paracentesis only were included in the study. The duration of the study was for one year: 01.01.2007. to 31.12.2007.
The exclusion criteria for isolate selection were as follows:• Isolates from in situ drains or drainage bottles.• Isolates from stool or peri-rectal abscess.• Duplicate isolates (same genus and species) obtained from
the same or different specimens from the same patient, irrespective of whether they were obtained from the same or different body sites. If multiple colony types of a particular species are isolated, only one representative colony (i.e. the most prevalent) is tested.
• Duplicate isolates (same genus and species) obtained at any subsequent time from the same patient regardless of susceptibility or phenotypic profile.
• Environmental samples (non-patient derived) or surveillance cultures taken for infection control purposes.
The laboratories in the participating centers were responsible for collecting demographic information including age and sex of the patient, site of infection, hospital ward/ unit, and
Fig. 1 : Indian centres in the SMART study
Table 1 : SMART Panel MIC Range for Gram- Negative Aerobic Bacilli
Abbreviation Antibiotic SMART Panel MIC Range (mg/L)
AS Ampicillin/Sulbactam 2 - 16Ak Amikacin 4 - 32Cax Ceftriaxone 1 - 32Caz Ceftazidime 0.5 - 128Caz/CA Ceftazidime/Clavulanic
acid0.12 - 16
Cft Cefotaxime 0.5 - 128Cft/CA Cefotaxime/Clavulanic
acid0.12 - 16
Cfx Cefoxitin 2 - 16Cp Ciprofloxacin 0.25 - 2Cpe Cefepime 0.5 - 32Cpe/CA Cefepime/Clavulanic acid 0.12 - 4Etp Ertapenem 0.03 - 4Imp Imipenem 0.06 - 8Lvx Levofloxacin 0.5 - 4P/T Piperacillin/Tazobactam 2 - 64
© JAPI • mAy 2011 • VOL. 59 3
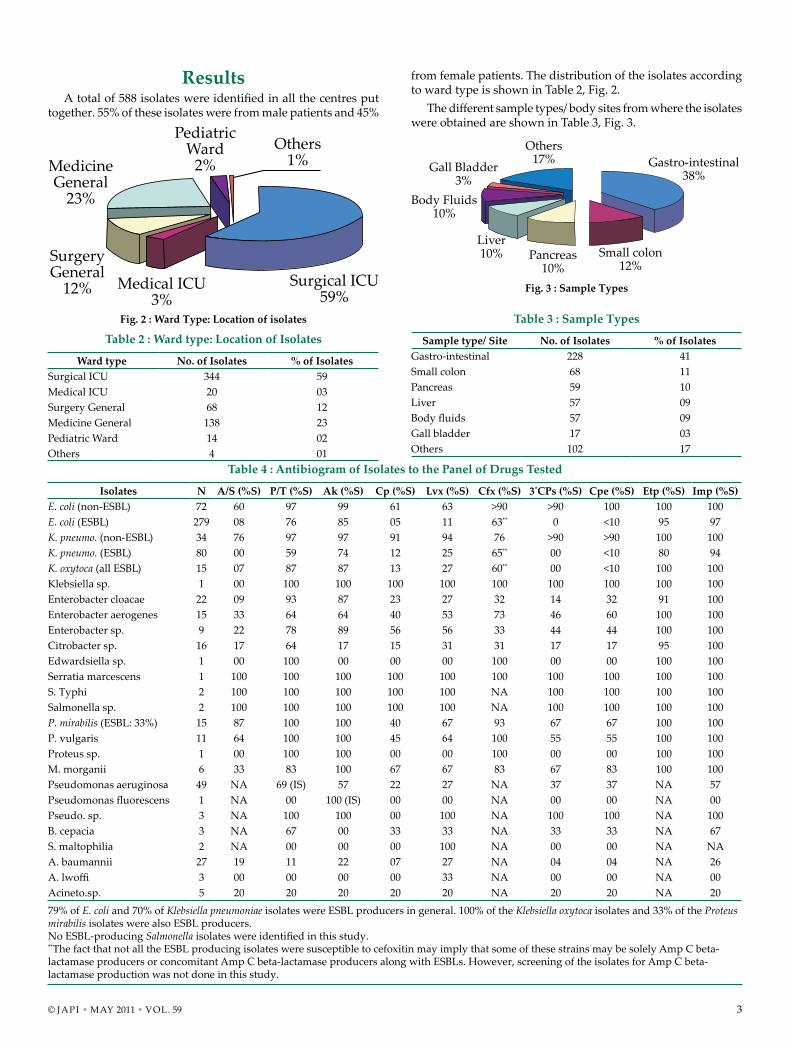
Fig. 2 : Ward Type: Location of isolates
Table 2 : Ward type: Location of Isolates
Ward type No. of Isolates % of IsolatesSurgical ICU 344 59medical ICU 20 03Surgery General 68 12medicine General 138 23Pediatric Ward 14 02Others 4 01
Fig. 3 : Sample Types
Table 3 : Sample Types
Sample type/ Site No. of Isolates % of IsolatesGastro-intestinal 228 41Small colon 68 11Pancreas 59 10Liver 57 09Body fluids 57 09Gall bladder 17 03Others 102 17
Table 4 : Antibiogram of Isolates to the Panel of Drugs Tested
Isolates N A/S (%S) P/T (%S) Ak (%S) Cp (%S) Lvx (%S) Cfx (%S) 3*CPs (%S) Cpe (%S) Etp (%S) Imp (%S)E. coli (non-ESBL) 72 60 97 99 61 63 >90 >90 100 100 100E. coli (ESBL) 279 08 76 85 05 11 63** 0 <10 95 97K. pneumo. (non-ESBL) 34 76 97 97 91 94 76 >90 >90 100 100K. pneumo. (ESBL) 80 00 59 74 12 25 65** 00 <10 80 94K. oxytoca (all ESBL) 15 07 87 87 13 27 60** 00 <10 100 100Klebsiella sp. 1 00 100 100 100 100 100 100 100 100 100Enterobacter cloacae 22 09 93 87 23 27 32 14 32 91 100Enterobacter aerogenes 15 33 64 64 40 53 73 46 60 100 100Enterobacter sp. 9 22 78 89 56 56 33 44 44 100 100Citrobacter sp. 16 17 64 17 15 31 31 17 17 95 100Edwardsiella sp. 1 00 100 00 00 00 100 00 00 100 100Serratia marcescens 1 100 100 100 100 100 100 100 100 100 100S. Typhi 2 100 100 100 100 100 NA 100 100 100 100Salmonella sp. 2 100 100 100 100 100 NA 100 100 100 100P. mirabilis (ESBL: 33%) 15 87 100 100 40 67 93 67 67 100 100P. vulgaris 11 64 100 100 45 64 100 55 55 100 100Proteus sp. 1 00 100 100 00 00 100 00 00 100 100m. morganii 6 33 83 100 67 67 83 67 83 100 100Pseudomonas aeruginosa 49 NA 69 (IS) 57 22 27 NA 37 37 NA 57Pseudomonas fluorescens 1 NA 00 100 (IS) 00 00 NA 00 00 NA 00Pseudo. sp. 3 NA 100 100 00 100 NA 100 100 NA 100B. cepacia 3 NA 67 00 33 33 NA 33 33 NA 67S. maltophilia 2 NA 00 00 00 100 NA 00 00 NA NAA. baumannii 27 19 11 22 07 27 NA 04 04 NA 26A. lwoffi 3 00 00 00 00 33 NA 00 00 NA 00Acineto.sp. 5 20 20 20 20 20 NA 20 20 NA 2079% of E. coli and 70% of Klebsiella pneumoniae isolates were ESBL producers in general. 100% of the Klebsiella oxytoca isolates and 33% of the Proteus mirabilis isolates were also ESBL producers.No ESBL-producing Salmonella isolates were identified in this study. **The fact that not all the ESBL producing isolates were susceptible to cefoxitin may imply that some of these strains may be solely Amp C beta-lactamase producers or concomitant Amp C beta-lactamase producers along with ESBLs. However, screening of the isolates for Amp C beta-lactamase production was not done in this study.
ResultsA total of 588 isolates were identified in all the centres put
together. 55% of these isolates were from male patients and 45%
from female patients. The distribution of the isolates according to ward type is shown in Table 2, Fig. 2.
The different sample types/ body sites from where the isolates were obtained are shown in Table 3, Fig. 3.
PediatricWard
2%Others
1%MedicineGeneral
23%
SurgeryGeneral
12% Medical ICU3%
Surgical ICU59%
Others17% Gastro-intestinal
38%
Small colon12%
Pancreas10%
Liver10%
Body Fluids10%
Gall Bladder3%

4 © JAPI • mAy 2011 • VOL. 59
The list of different isolates obtained and the antibiogram of the 588 isolates to the 12 antibiotics tested in the Study are shown in Table 4.
Of the 588 isolates identified, 351 (60%) were E. coli; 130 (22%) Klebsiella spp. (K. pneumoniae: 114, K. oxytoca: 15, other sp.:1); 56 (9.5%) Enterobacter spp. (E. cloacae: 22, E. aerogenes: 15, other spp.: 9); 53 (9%) Pseudomonas spp. (P. aeruginosa: 49, other spp.:4); 35 (6%) Acinetobacter spp. (A. baumannii: 27, other spp.: 8); 33 (5.6%) Proteae (P. mirabilis: 15, P. vulgaris: 11, M. morganii: 6, other sp.:1); 16 (2.7%) Citrobacter spp. (C. freundii: 13, other spp.: 3): Vide Table 4.
Out of the drugs tested, except for carbapenems, all the others showed a statistically significant drop (p<0.0001) in sensitivity for ESBL variants as compared to the non-ESBL strains. Only carbapenems, maintained their efficacy even in the presence of ESBLs and their sensitivity patterns did not show any significant difference between the two types. In comparison, drugs like amikacin and piperacillin-tazobactam showed statistically significant (p<0.005) drop in the sensitivities for ESBL variants vis-à-vis non-ESBL strains.
All the non-ESBL strains of E. coli were susceptible to Group I carbapenem, ertapenem and Group II carbapenem, imipenem (100% susceptibility to both) and their susceptibilities to amikacin and piperacillin-tazobactam were 99% and 97% respectively.
In case of ESBL-positive E. coli isolates, high susceptibilities to imipenem and ertapenem were noted (97% and 95% respectively), whereas the susceptibility to non-carbapenem antibiotics namely amikacin and piperacillin-tazobactam were reduced (85% and 76% respectively) Although this differences was not significant for the carbapenems (p>0.05).
A similar pattern was observed in case of K. pneumoniae
strains where only carbapenems maintained their efficacy in the presence of ESBLs and their sensitivity patterns did not show marked difference between ESBL and non-ESBL variants. In case of non-ESBL K. pneumoniae strains, the susceptibilities towards carbapenems, amikacin and piperacillin-tazobactam were 100%, 97% and 97% respectively. For ESBL-positive K. pneumoniae strains, there was a slight difference in their susceptibilities towards imipenem (94%, p>0.05), but more pronounced with ertapenem (80%, p<0.005), while their susceptibilities towards amikacin and piperacillin-tazobactam were 74% and 59% respectively, much less than the non-ESBL strains.
Amongst the non-fermenters, 43% of P. aeruginosa and 33% of the B. cepacia isolates were imipenem resistant. On the other hand, as high as 74% of Acinetobacter baumannii isolates and 80-100% of other Acinetobacter isolates were resistant to imipenem. However, screening of the carbapenem resistant non-fermenters for metallo-beta lactamase (mBL) production and susceptibility of those isolates to aztreonam were not included in this study.
The important features observed in isolates obtained from patients within and after 48 hours of hospitalization, so as to determine the differences between “community-acquired” and hospital-acquired isolates, are shown in Table 5.
110 E. coli and 35 Klebsiella pneumoniae isolates were from “community-acquired” intra-abdominal infections. 80% of E. coli and 63% of Klebsiella pneumoniae isolates from “community-acquired” infections were ESBL producers against 79% of E. coli and 73% of Klebsiella pneumoniae isolates from hospital-acquired infections.
There were slight differences in susceptibility patterns of “community-acquired” and hospital-acquired ESBL-positive isolates of E. coli and K. pneumoniae (vide Table 5); however,
Table 5: Features of Isolates Obtained < 48 hrs and > 48 hrs of Hospitalization
Isolates N < 48 hrs. of hospitalization (% S) > 48 hrs. of hospitalization (% S)E. coli (non-ESBL) 72 22 (Carbapenems, Amikacin 100, Pip-taz. 95) 50 ( Carbapenems 100, Amikacin & Pip-taz. 98)E. coli (ESBL) 279 88 (Imipenem 99, Ertapenem 94, Pip-taz., Amikacin
80)191 (Imipenem 95, Ertapenem 93, Amikacin 87, Pip-taz. 74)
K. pneumo. (non-ESBL) 34 13 (Carbapenems, Amikacin, Pip-taz. 100) 21 (Carbapenems 100, Amikacin, Pip-taz. 95) K. pneumo. (ESBL) 80 22 (Imipenem 86, Ertapenem 77, Amikacin 82,
Pip-taz. 68)58 (Imipenem 96, Ertapenem 81, Amikacin 71, Pip-taz. 55)
K. oxytoca (all ESBL) 15 2 (Carbapenems, Amikacin, Pip-taz. 100) 13 (Carbapenems 100, Amikacin, Pip-taz. 85)Klebsiella sp. 1 --- 1 (Carbapenem, Amikacin, Pip-taz. 100)Enterobacter spp. 56 21 (Imipenem 100, Ertapenem 95, Amikacin 70,
Pip-taz. 75)35 (Imipenem 100, Ertapenem 96, Amikacin 70, Pip-taz 80)
Citrobacter sp. 16 4 (Carbapenems 100, Amikacin, Pip-taz. 75) 12 (Carbapenems 100, Amikacin, Pip-taz. 80)Edwardsiella sp. 1 --- 1 (Carbapenem, Pip-taz. 100, Amikacin 0)Serratia marcescens 1 --- 1 (All sensitive)S. Typhi 2 1 (All sensitive) 1 (All sensitive)Salmonella sp. 2 --- 2 (All sensitive)P. mirabilis (ESBL: 33%) 15 4 (Carbapenems, Amikacin, Pip-taz. 100) 11 (Carbapenems, Pip-taz. 100, Amikacin 82)P. vulgaris 11 2 (All sensitive) 9 (Carbapenems, Amikacin, Pip-taz. 100)Proteus sp. 1 --- 1 (Carbapenems, Amikacin, Pip-taz. 100)m. morganii 6 1 (Carbapenems, Amikacin, Pip-taz. 100) 5 (Carbapenems, amikacin 100, Pip-taz. 70)Pseudomonas aeruginosa
49 8 (Imipenem 63, Amikacin 75, Pip-taz 63 IS) 41 (Imipenem 54, Amikacin 55, Pip-taz. 70 IS)
Pseudo. spp. 4 1 (Imipenem, Amikacin, Pip-taz. 100) 3 (Imipenem, Pip-taz 75, Amikacin 100)B. cepacia 3 --- 3 (Imipenem, Pip-taz. 67, Amikacin 0) S. maltophilia 2 --- 2 (Only Levofloxacin S)Acinetobacter spp. 35 5 (Imipenem 40, Amikacin 23, Pip-taz 15) 30 (Imipenem 25, Amikacin 18, Pip-taz. 13)
© JAPI • mAy 2011 • VOL. 59 5
none achieved statistical significance (p>0.05 for all pairs). No difference in ertapenem or imipenem sensitivity was observed between “community-acquired” and hospital-acquired ESBL-positive isolates of Klebsiella oxytoca and Proteus mirabilis (vide Table 5).
No significant differences (p>0.05) were observed in the imipenem sensitivity for “community-acquired” and hospital-acquired isolates of Pseudomonas and Acinetobacter spp.
Discussion and ConclusionThe study showed an alarming incidence of ESBL-producers
amongst Enterobacteriaceae isolates from intra-abdominal infections in both “community-acquired” and hospital-acquired settings across India, especially in case of E. coli and K. pneumoniae isolates.
However, the observation of high prevalence of ESBL producers and carbapenem resistant non-fermenters in the “community” could at least partially be attributed to the definition used, i.e., infection within 48 hours and after 48 hours of hospitalization in the centers. Given the nature of the hospitals engaged as centers for the study in India, being predominantly tertiary care set-ups admitting patients already treated in some other institutions, rather than straight from the community. Hence the data may not be representative of the true community scenario.
Another limitation is that all contributing centers are urban centers located in major cities of India. Hence, the data is not representative of rural settings/ small towns
Ertapenem was comparable with imipenem against ESBL-positive E. coli isolates, while imipenem was more effective than ertapenem against ESBL-positive Klebsiella pneumoniae isolates. No difference in Group I and Group II carbapenem susceptibility was, however, observed in case of ESBL-positive K. oxytoca and P. mirabilis isolates in all settings.
A significant observation in the study was that no ESBL-producing Salmonella isolates were identified. In fact, all the Salmonella isolates were susceptible to all the antibiotics included in this study.
The study also identified a high incidence of carbapenem resistance in the case of the non-fermenting Gram-negative isolates, especially, P. aeruginosa and Acinetobacter spp.
The study did not screen isolates for Amp C beta lactamase and mBL production. These tests may be included in the future studies to get a better idea of the incidence of such strains in intra-abdominal infections.
The high incidence of ESBL producing Enterobacteriaceae as well as carbapenem resistant non-fermenters in the community indicates a grave situation that needs to be tackled urgently by• Complete eradication of infectious agents before affected
patients are discharged.• Patient contacts and hospital personnel to properly
decontaminate their hands with disinfectants (or simply with soap and water) prior to leaving hospital premises.
• Hospitals to treat and decontaminate its waste, effluents, and sewage before disposal or before releasing those in
public sewerage. The high incidence of nosocomial infection with multi-drug
resistant bugs should be prevented and controlled by: • Continuous surveillance of hospital, especially ICUs, OT’s
and wards housing high-risk patients.• Disinfection of medical devices and hospital environment.• Maintenance of strict asepsis during invasive procedures. • ‘Standard Precautions’ in wards and laboratories. • Proper disposal of hospital waste. • Patient isolation-/-segregation or barrier nursing to prevent
transmission of infection.• Hand hygiene with chlorhexidine or alcohol - based
disinfectants before and between patient contacts: this is the most important measure.
• Policies for antibiotic stewardship Note a. The results of this study were presented in a poster session
(poster no. GN 103) at the 7th International symposium on Antimicrobial agents and Resistance (ISAAR) held in Bangkok, Thailand on march 18-20,2009
b. There was a publication in Antimicrobial agents and chemotherapy, Aug 2009,p 3280-3284 titled ‘Emergence of High Levels of Extended-Spectrum-_-Lactamase-Producing
Gram-Negative Bacilli in the Asia-Pacific Region: Data from the Study for monitoring Antimicrobial Resistance Trends (SmART) Program, 2007’
AcknowledgementThis study was sponsored by merck & Co., Inc. USA. We
thank Dr. mahua Ganguly and Dr. Ankur Gupta of mSD, India for their scientific and editorial support.
References1. Spencer RC, Bauernfeind A, Garcia-Rodriquez J, et al. Surveillance
of the current resistance of nosocomial pathogens to antibacterials. Clin. Microbiol Infect 1997;3(Suppl 1):S21-S35.
2. Sahm, DF, marsilio, mK & Piazza, G (1999). Antimicrobial resistance in key bloodstream bacterial isolates: electronic surveillance with The Surveillance Network database USA. Clinical Infectious Diseases 1996;29:259-63.
3. Jones, RN The emergent need for Basic Research, education, and surveillance of antimicrobial resistance. Problems facing the report from the American Society for microbiology Task Force on Antibiotic Resistance. Diagnostic Microbiology and Infectious Diseases 1996;25:153-61.
4. Livermore D, Carter m, Bagel S, et al. In vitro activities of ertapenem (mK-0826) against recent clinical bacteria collected in Europe and Australia. Antimicrob Agent Chemother 2001;45:1860-7.
5. Fuchs PC, Barry AL, Brown SD. In-vitro antimicrobial activity of a carbapenem, mK-0826 (L-749,345) and provisional interpretive criteria for disc tests. J Antimicrob Chemother 1999;43:703-6.
6. Goldstein EJC, Citron Dm, merriam CV, Warren y, Tyrrell KL. Comparative in vitro activities ertapenem (mK-0826) against 1,001 anaerobes isolated from human intra-abdominal infections. Antimicrob Agent Chemother 2000;44:2389-94.
7. Wexler Hm, molitoris D, Finegold Sm. In vitro activities of mK-826 (L-749, 345) against 363 strains of anaerobic bacteria. Antimicrob Agents Chemother 2000;44:2222-4.
8. Pankuch GA, Davies TA, Jacobs mR, Appelbaum PC. Antipneumococcal activity of ertapenem (mK-0826) compared to those of other agents. Antimicrob Agent Chemother 2002;46:42-46.
9. Kohler J, Dorso KL, young K, et al. In vitro activities of the potent, broad-spectrum carbapenem mK-0826 (L-749, 345) against broad-spectrum β-lactamase and extended-spectrum β-lactamase producing Klebsiella pneumoniae and Escherichia coli clinical isolates.
6 © JAPI • mAy 2011 • VOL. 59
Antimicrob Agents Chemother 1999;43:1170-6.10. Jacoby G, Han P, Tran J. Comparative in vitro activities of
carbapenem L-749, 345 and other antimicrobials against multiresistant gram-negative clinical pathogens. Antimicrob Agents and Chemother 1997;41:1830-1.
11. Solomkin J, Choe K, Christou N, et al. Results of a prospective, randomized, triple-blind study of ertapenem vs. piperacillin/tazobactam for complicated intra-abdominal infection [Abstract]. 11th European Congress of Clinical microbiology and Infectious Diseases 2001 Apr 1-4; Istanbul, Turkey; 2001;1460.
12. Graham D, Lucasti C, malafaia O, et al. Ertapenem once daily versus piperacillin/tazobactam 4 times per day for treatment of complicated skin and skin-structure infections in adults: results of a prospective, randomized, double-blind study. Clinical Infectious Diseases 2002;11:1460-1468.
13. Roy S, Higareda I, Angel-muller E, et al. Results of a phase III randomized, double-blind study of ertapenem (ETP) vs piperacillin/
tazobactam (P/T) for acute pelvic infection (Inf) in women [Abstract]. 41st Interscience Conference on Antimicrobial Agents and Chemotherapy; 2001 Sep 23; Chicago, Illinois; 2001: L-888.
14. Tomera, Kevin m, et al. Ertapenem versus ceftriaxone followed by appropriate oral therapy for treatment of complicated urinary tract infections in adults: results of a prospective, randomized, double-blind, multicenter study. Antimicrob Agents Chemother 2002;46:2895-2900.
15. Guillermo O, Caballero-Lopez J, Friedland I, et al. A study evaluating the efficacy, safety, and tolerability of ertapenem versus ceftriaxone for the treatment of community-acquired pneumonia in adults. Clinical Infectious Diseases 2002;34:1076-83.
16. Hawser SP, Bouchillon SK, Hoban DJ, etal. Emergence of High Levels of Extended-Spectrum Beta-Lactamase-Producing Gram-Negative Bacilli in the Asia-Pacific Region: Data from the Study for monitoring Antimicrobial Resistance Trends (SmART) Program, 2007. Antimicrob Agents Chemother 2009;53:3280-3284.
Dr. Vithalrao Nadgouda Best All India Annual Thesis AwardThe Association of Physicians of India
Indian College of Physicians
DR. VITHALRAO NADGOUDA BEST ALL INDIA ANNUAL THESIS AWARD
1. The award is open to the physicians from various medical institutions / hospitals from India within one year of passing the mD / DNB examination in medicine / General medicine / Internal medicine as on the last date for submission of the application for the above award is 31st may, 2011.
2. There shall be two awards: the first award shall comprise of Rs. 15,000/- along with a certificate and the second award shall comprise of Rs. 10,000/- along with a certificate.
Full format is available on API and JAPI websites: www. apiindia.org / www.japi.org
Dr. Milind Y. Nadkar Dr. B. R. Bansode Hon. General Secretary Joint Secretary
The Award of Fellowship of Indian College of PhysiciansNominations are invited for the award of Fellowship of Indian College of Physicians
Full format is available on API and JAPI websites: www. apiindia.org / www.japi.org
Last date to receive nomination for FICP : 31st may 2011
Dr. Milind Y. Nadkar Dr. B. R. Bansode Hon. General Secretary Joint Secretary
DOCTOR 2010 - Medical SoftwareCOMPATIBLE WITH WINDOWS 7, VISTA, XP, DESKTOP, LAPTOP AND NETBOOK
CLINICAL: Case sheets, speciality sheets, Inpatient, ICU, Lab, PDR, Auto Casesummary, Certificates, letters, USS, X-ray, Pathology, Endoscopy, Echo, Proc. reports, very little typing needed. Prescription Autodose, Allergy, disease-contraindication, interaction alert, Fonts option (Hindi Tamil etc) Overdose treatment, Ther. level, dose in organ failures Store Recall at a single click.ADMINISTRATIVE : Appointment scheduler; OP Card, Pt. List, Statisics, Finance billing; salary, room, manpwr management; Drugstore, Inventory. Secure, NETWORK ready. Auto backup.Store/Link photos, X-ray, ECG, Videos; Change Header/Footer; Diet advisor-autocalory calculatorEDUCATIVE: Disease guidelines medical graphs; Patient education videos & prinouts. Reliable. Saves Life, Time and money. Hospital pack, and excl. medicine, surgery, OBG, clinic packs available.Address : MEDISOFT, Achutha Warrier Lane, Cochin-682035. http://www.medisoftindia.comE-mail : [email protected] Ph.: 09847294414 © IPR.All Rights Reserved