
In Vitro Bactericidal Capacity Human Polymorphonu...
12
Journal of Clinical Investigation Vol. 46, No. 4, 1967 In Vitro Bactericidal Capacity of Human Polymorphonu- clear Leukocytes: Diminished Activity in Chronic Granulomatous Disease of Childhood * P. G. OUIE,t J. G. WHITE, B. HOLMES, AND R. A. GOOD t (From the Departments of Pediatrics and Microbiology, University of Minnesota Medical School, Minneapolis, Ainn.) Summary. Diminished bactericidal capacity was found to be characteristic of polymorphonuclear leukocytes (PMN) from five children with the clinical syndrome of granulomatous disease of childhood. The PMN from these children demonstrated nearly normal phagocytic capacity, and the majority of viable bacteria, after 2 hours of incubation in the phagocytosis system, were found associated with leukocytes. The morphology of the unstimulated polymorphonuclear leukocytes from patients with chronic granulomatous disease was similar to those from normal persons of similar ages by light and electron microscopy. In addition, the total lysozyme and phagocytin activity of leukocyte extracts from these patients was similar to those from equal numbers of leukocytes from controls. A striking difference in the cytoplasmic response after phagocytosis char- acterized the PMN of the patients with granulomatous disease. Whereas degranulation, vacuole formation, and rapid bacterial digestion were the rule in the PMN from controls, little degranulation and persistence of intact bac- teria in the cytoplasm characterized disease. The deficiency of bactericidal capacity and the minimal degranulation after active phagocytosis by the PMN of these children with an inherited syn- drome suggest that separate metabolic processes are involved in phagocytosis and in intracellular digestion. Continuing study of the metabolic function of leukocytes from these children should provide an opportunity for increased understanding of the metabolic basis for degranulation and intracellular di- gestion in phagocytic cells. Introduction The necessity of sufficient quantities of phago- cytic cells for bacterial resistance has been estab- * Submitted for publication October 31, 1966; accepted December 30, 1966. Supported in part by National Foundation, American Heart Association, and U. S. Public Health Service (AI-06931, HE-02085, AI-00798, and NB-02042) grants and the Commission on Streptococcal and Staphylococcal Diseases, Armed Forces Epidemiological Board, Office of the Surgeon General, Dept. of the Army, Washing- ton, D. C. Presented in part at the 58th Annual Meeting of the American Society for Clinical Investigation, Atlantic City, N. J., May 2, 1966. t John and Mary R. Markle Scholar in Academic wished by clinical experience with patients leuko- penic from a variety of causes. A small number of patients, however, suffer recurrent bacterial disease in spite of a vigorous leukocyte response to infection. Adequate bactericidal function of phagocytic cells, as well as the quantity of avail- able leukocytes, appears to be a critical factor in bacterial resistance. Medicine. Recipient of U. S. Public Health Service Career Development Award (5-K3-AI-10, 109-05). Address requests for reprints to Dr. P. G. Quie, Dept. of Pediatrics, University of Minnesota Medical School, Minneapolis, Minn. 55455. : American Legion Memorial Heart Research Pro- fessor of Pediatrics and Microbiology. 668
Transcript of In Vitro Bactericidal Capacity Human Polymorphonu...

Journal of Clinical InvestigationVol. 46, No. 4, 1967
In Vitro Bactericidal Capacity of Human Polymorphonu-clear Leukocytes: Diminished Activity in Chronic
Granulomatous Disease of Childhood *
P. G. OUIE,t J. G. WHITE, B. HOLMES,ANDR. A. GOODt(From the Departments of Pediatrics and Microbiology, University of Minnesota Medical
School, Minneapolis, Ainn.)
Summary. Diminished bactericidal capacity was found to be characteristicof polymorphonuclear leukocytes (PMN) from five children with the clinicalsyndrome of granulomatous disease of childhood. The PMN from thesechildren demonstrated nearly normal phagocytic capacity, and the majorityof viable bacteria, after 2 hours of incubation in the phagocytosis system,were found associated with leukocytes.
The morphology of the unstimulated polymorphonuclear leukocytes frompatients with chronic granulomatous disease was similar to those from normalpersons of similar ages by light and electron microscopy. In addition, thetotal lysozyme and phagocytin activity of leukocyte extracts from thesepatients was similar to those from equal numbers of leukocytes from controls.
A striking difference in the cytoplasmic response after phagocytosis char-acterized the PMNof the patients with granulomatous disease. Whereasdegranulation, vacuole formation, and rapid bacterial digestion were the rulein the PMNfrom controls, little degranulation and persistence of intact bac-teria in the cytoplasm characterized disease.
The deficiency of bactericidal capacity and the minimal degranulation afteractive phagocytosis by the PMNof these children with an inherited syn-drome suggest that separate metabolic processes are involved in phagocytosisand in intracellular digestion. Continuing study of the metabolic functionof leukocytes from these children should provide an opportunity for increasedunderstanding of the metabolic basis for degranulation and intracellular di-gestion in phagocytic cells.
Introduction
The necessity of sufficient quantities of phago-cytic cells for bacterial resistance has been estab-
* Submitted for publication October 31, 1966; acceptedDecember 30, 1966.
Supported in part by National Foundation, AmericanHeart Association, and U. S. Public Health Service(AI-06931, HE-02085, AI-00798, and NB-02042) grantsand the Commission on Streptococcal and StaphylococcalDiseases, Armed Forces Epidemiological Board, Officeof the Surgeon General, Dept. of the Army, Washing-ton, D. C.
Presented in part at the 58th Annual Meeting of theAmerican Society for Clinical Investigation, AtlanticCity, N. J., May 2, 1966.
t John and Mary R. Markle Scholar in Academic
wished by clinical experience with patients leuko-penic from a variety of causes. A small numberof patients, however, suffer recurrent bacterialdisease in spite of a vigorous leukocyte responseto infection. Adequate bactericidal function ofphagocytic cells, as well as the quantity of avail-able leukocytes, appears to be a critical factor inbacterial resistance.
Medicine. Recipient of U. S. Public Health ServiceCareer Development Award (5-K3-AI-10, 109-05).
Address requests for reprints to Dr. P. G. Quie, Dept.of Pediatrics, University of Minnesota Medical School,Minneapolis, Minn. 55455.
: American Legion Memorial Heart Research Pro-fessor of Pediatrics and Microbiology.
668

LEUKOCYTEACTIVITY IN CHRONICGRANULOMATOUSDISEASE OF CHILDHOOD
The present investigation was designed to studythe in vitro functional capacity of the polymorpho-nuclear leukocytes during the early stages ofcellular-bacterial interaction under conditions thatwere optimal for phagocytosis and bacterial kill-ing. Patients included in the study were thosewith disease syndromes characterized by persis-tent or recurrent bacterial infections.
The capacity of polymorphonuclear leukocytesto phagocytize and kill bacteria in vitro was com-parable to normal controls in most of these pa-tients; however, one group of patients, all appar-ently suffering from the same clinical disease,showed a defect in leukocyte function. These pa-tients presented a clinical syndrome originally de-fined as "a fatal granulomatous disease of child-hood" when separated from other granulomatousprocesses of known etiology (1, 2). Other stud-ies have established the clinical identity of thesepatients and the familial nature of this disorder(3, 4). Unlike the polymorphonuclear leukocytesof normal persons and persons with many differ-ent diseases, PMNfrom the patients of this groupdemonstrated phagocytic capacity but impairedability to kill phagocytized bacteria.
The activity of bactericidal factors lysozymeand phagocytin was quantitatively comparable inextracts of leukocytes from patients with this dis-ease and from normal controls. It was observed,however, that polymorphonuclear leukocytes frompatients with granulomatous disease of childhooddemonstrated little degranulation after phagocy-tosis of bacteria. Although the intracytoplasmicbacteria were surrounded by membranes, typicalphagocytic vacuoles were not observed in the poly-morphonuclear leukocytes from patients with thisdisease.
Methods
Twenty-nine patients with recurrent bacterial diseaseor chronic systemic disease associated with increasedsusceptibility to bacterial infection were studied. Anadditional 22 children and adults without bacterial in-fections were included as normal controls.
Polymorphonuclear leukocyte function. Phagocyticand bactericidal capacities of human PMNwere deter-mined by the Maaloe method (5) with the modificationsdescribed by Cohn and Morse (6) and Hirsch andStrauss (7).
Human peripheral leukocytes were prepared by dex-tran sedimentation of heparinized venous blood. Ten ml
of blood containing 2 mg heparin was mixed with 5 ml6% dextran in saline' and incubated at room tempera-ture for 1 hour. The plasma containing leukocytes, plate-lets, and few erythrocytes was withdrawn. Leukocyteswere deposited by centrifugation at 1,000 rpm (Interna-tional centrifuge model U.V. head 219) and were washedwith heparinized saline. After the first wash the cellsuspension was counted in a hemocytometer, and theproportion of polymorphonuclear leukocytes was deter-mined by chamber differential. The leukocytes werecentrifuged and suspended in Hanks balanced salt solu-tion 2 with 0.1% gelatin to give a concentration of 5 X 108PMNper ml.
The bacterial species used in these studies wereStaphylococcus aureus strain 502A and Paracolon hafnia.Biologic characteristics of the staphylococcal strain havebeen reported previously (8). The P. hafnia strain wasrecently recovered from the osteomyelitic lesion of one ofthe patients (D.B.). The bacterial strains were culturedovernight in Penassay broth (Difco) and then suspendedto give an optical density of 0.6 at 620 mAt in a ColmanJr. photocolorimeter. This optically adjusted suspen-sion was diluted 1-50 in balanced salt solution with 0.1%gelatin. This dilution of staphylococci or paracolon bac-teria contained 3 to 6 X 107 bacteria per ml. Both thestaphylococci and paracolon strains required opsonin forengulfment, and this was provided by fresh human adultsera. Sera from four or more healthy adult volunteerswere pooled, divided into 1-ml aliquots, frozen, and storedfor no longer than 30 days. An aliquot of pooled serawas thawed immediately before use and diluted to 20% inbalanced salt solution.
Phagocytic tests were done in 15 X 75 siliconized tubes.Each tube contained 0.5 ml leukocyte suspension, 0.1 mlbacteria suspension, and 0.4 ml opsonin. This providedapproximately one bacterium per PMNand a final con-centration of 10% serum.
Each assay included control tubes of leukocytes andbacteria without opsonin and tubes held stationary todetermine extracellular bacterial killing. The tubes forassay of bactericidal activity were incubated at 370 Cwith an end over end rotation. The total viable bacteriaat the beginning of and during the incubation period wasdetermined by transferring samples with a calibrated0.002-ml platinum loop to 1 ml distilled water for celllysis and dilution. At the end of the incubation period(usually 120 minutes), the tubes containing the phagocyticmixtures were centrifuged at 800 X g for 5 minutes.Samples were removed from the supernatant fraction fordetermination of extracellular bacteria, and portions ofthe washed resuspended leukocyte pellet were placed indistilled water for lysis and dilution as a measure ofleukocyte-associated bacteria.
Sera from patients with increased susceptibility to in-fection were tested for opsonic activity by using dilutionsof the opsonin fraction in phagocytic mixtures containingstaphylococci and leukocytes from normal donors. Each
1 Cutter Labs., Chattanooga, Tenn.2 Baltimore Biological Labs., Baltimore, Md.
669

QUIE, WHITE, HOLMES, AND GOOD
TABLE I
Phagocytic and bactericidal capacity of polymorphonuclear leukocytes (PMN) for Staphylococcus aureus
Viable bacteria ( X 106) per ml
Supernatantfluid after
Total phagocytic mixture centrifugation ResuspendedSource of 800 X g for leukocyte
PMN 0 30 min 60 min 120 min 10 minutes pellet
D.B. 4.0 3.50 3.6 2.20 0.26 2.00Control 2.2 0.12 0.1 0.09 0.12 0.01J.B. 5.0 2.5 2.70 2.00 0.80 1.20Control 3.9 0.9 0.15 0.07 0.04 0.03L.J. 4.0 1.4 1.50 0.50 0.24 1.70Control 5.8 0.26 0.18 0.09 0.04 0.08K.S. 2.5 2.5 1.80 1.10 0.40 0.70Control 2.0 1.6 0.18 0.06 0.04 0.02T.W. 3.5 2.0 2.00 2.4 0.60 1.10Control 5.8 0.8 0.29 0.2 0.15 0.20
serum was compared with a sample of pooled normalsera and tested at final concentrations of 10%, 5%, and1% in the phagocytosis system.
Morphology and cytochemistry of leukocytes. Smearsof the leukocyte-bacteria mixtures were made on glassslides and stained with Wright's stain in standardfashion.
Viability of leukocytes during the incubation periodwas determined by incubation of a loopful of bacteria-leukocyte suspension and 1% trypan blue on a glass slideunder a mineral oil-sealed cover slip for 1 minute. Fail-ure of nuclear staining was regarded as evidence forviability.
Leukocytes from patients and from normal controlswere fixed and stained with Sudan black and periodicacid-Schiff. Slides were also prepared for histochemicaldetermination of peroxidase, alkaline phosphatase, andacid phosphatase with standard methods described byHayhoe (9).
Preparation for electron microscopy. Parallel tubesof bacteria-leukocyte mixtures from patients and con-
trols, incubated as described above, were removed at 30and 60 minutes. The tubes were transferred immediatelyto a refrigerated centrifuge (40 C) and sedimented at800 rpm for 5 minutes. Supernatant media were de-canted, and 3 ml of cold (40 C) 3% glutaraldehyde in0.05 ml cacodylate buffer with 1%o sucrose, pH 7.3, was
added to each cell pellet. After 15 minutes the pelletswere loosened from the base of the tubes, the glutaralde-hyde was decanted, and the cells were washed with caco-dylate buffer. Phosphate-buffered 1% osmic acid, pH 1.3,was then added, and the pellets of cells were incubated inthis fixative for 1A hours. The preparations were dehy-drated and embedded by techniques previously recordedfrom this laboratory (10), and after sectioning they wereexamined with a Phillips 200 electron microscope.
Assay for bactericidal activity of leukocyte extracts.The method for preparation of leukocyte extracts forassay of lysozyme and phagocytin was that described by
Hirsch and Church (11). Leukocytes in the plasma layerafter dextran sedimentation were partially separatedfrom platelets by differential centrifugation and fromerythrocytes by lysis with hypotonic saline and neutrali-zation with hypertonic saline. After differential count-ing of the leukocytes, they were centrifuged, and theleukocyte pellets were frozen and thawed six times. Asaline extract of the disrupted leukocytes was made byincubation in saline for 30 minutes at 370 C at a con-centration of approximately 107 leukocytes per ml. Thesaline-insoluble residue was separated by centrifugationat 10,000 X g for 15 minutes, and the supernatant (salineextract) was used for assay of lysozyme by the methodof Shugar (12).
The sediment was washed with saline, suspended in 1ml of 0.01 M citric acid, and incubated for 30 min-utes at 370 C with constant shaking. After centrifugationat 10,000 X g, the supernatant (citric acid extract) wasassayed for phagocytin activity by the method of Hirsch(13).
Results
Comparison of bactericidal capacity of polymor-phonuclear leukocytes from patients with chronicgranulomatous disease and from normal controls.A comparison of the number of viable staphylo-cocci after incubation for 30, 60, and 120 minuteswith PMNfrom five children with chronic granu-lomatous disease and with PMN from normalcontrols is shown in Table I. In preparationswith PMNfrom the patients with this syndrome,at least 50%o of the organisms inoculated remainedas viable colony-forming units, even after 120minutes' incubation. In contrast, less than 10%oand frequently less than 1 % of the staphylococci
670
LEUKOCYTEACTIVITY IN CHRONICGRANULOMATOUSDISEASE OF CHILDHOOD
TABLE II
Phagocytic and bactericidal capacity of polymorphonuclear leukocytes for Paracolon hafnia
Viable bacteria (X 106) per ml
Supernatantfluid after
Total phagocytic mixture centrifugation ResuspendedSource of 800 X g for leukocyte
PMN 0 30 min 60 min 120 min 10 minutes pellet
D.B. 5.5 3.0 3.00 2.70 1.60 2.60Normal 6.0 0.7 0.19 0.04 0.03 0.01J.B. 4.0 3.00 3.00 2.50 1.00 1.50Normal 4.4 1.00 0.30 0.05 0.03 0.02L.J. 6.0 4.9 4.80 4.20 2.20 2.20Normal 5.9 1.3 0.13 0.07 0.01 0.09K.S. 3.7 3.5 2.50 2.60 0.40 2.00Normal 3.4 0.5 0.06 0.05 0.03 0.01T.W. 8.5 7.0 3.6 2.00 0.60 3.00Normal 8.8 0.4 0.1 0.40 0.17 0.33
incubated with PMNfrom normal controls wereviable after 60 minutes.
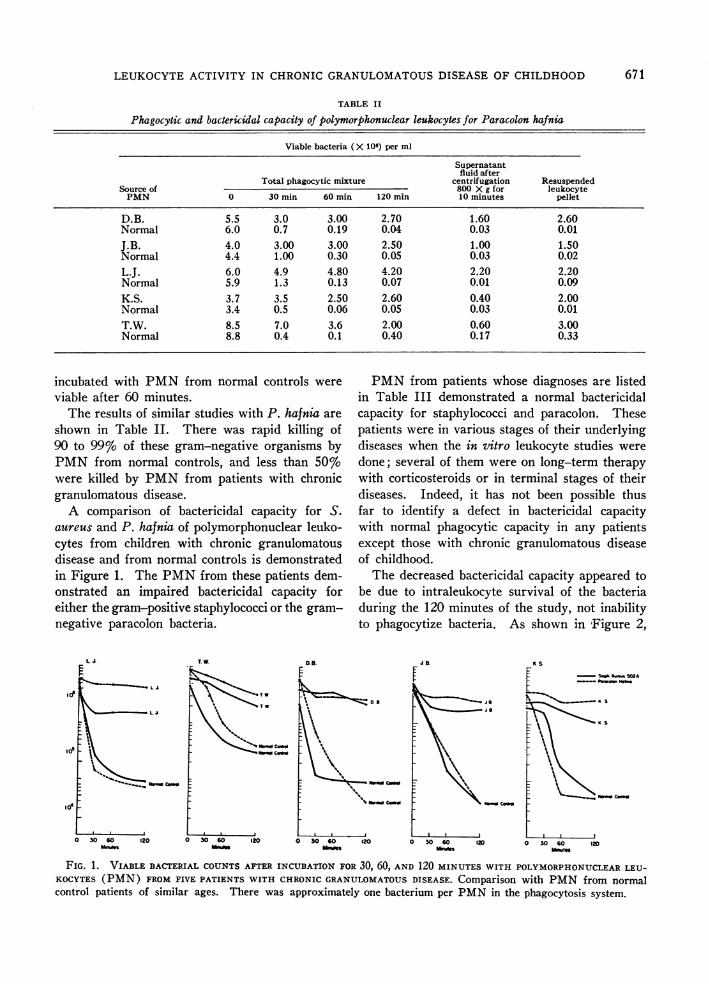
The results of similar studies with P. hafnia areshown in Table II. There was rapid killing of90 to 99%o of these gram-negative organisms byPMNfrom normal controls, and less than 50%owere killed by PMNfrom patients with chronicgranulomatous disease.
A comparison of bactericidal capacity for S.aureus and P. hafnia of polymorphonuclear leuko-cytes from children with chronic granulomatousdisease and from normal controls is demonstratedin Figure 1. The PMNfrom these patients dem-onstrated an impaired bactericidal capacity foreither the gram-positive staphylococci or the gram-negative paracolon bacteria.
T. W.
idI
PMNfrom patients whose diagnoses are listedin Table III demonstrated a normal bactericidalcapacity for staphylococci and paracolon. Thesepatients were in various stages of their underlyingdiseases when the in vitro leukocyte studies weredone; several of them were on long-term therapywith corticosteroids or in terminal stages of theirdiseases. Indeed, it has not been possible thusfar to identify a defect in bactericidal capacitywith normal phagocytic capacity in any patientsexcept those with chronic granulomatous diseaseof childhood.
The decreased bactericidal capacity appeared tobe due to intraleukocyte survival of the bacteriaduring the 120 minutes of the study, not inabilityto phagocytize bacteria. As shown in Figure 2,
0.8. K. &
.~~~~~~ s
Sus S
I'
r [ Sng unu
0 30 60 1 0 ° 30 60 120 030 o0 120 0 30 60 Om 30 6012oMONin WOBWSMnue Seusigs Mintes
FIG. 1. VIABLE BACTERIAL COUNTSAFTER INCUBATION FOR 30, 60, AND 120 MINUTES WITH POLYMORPHONUCLEARLEU-KOCYTES(PMN) FROMFIVE PATIENTS WITH CHRONICGRANULOMATOUSDISEASE. Comparison with PMNfrom normalcontrol patients of similar ages. There was approximately one bacterium per PMNin the phagocytosis system.
671
D2A

QUIE, WHITE, HOLMES, AND GOOD
%Viable Bacteria after 120 Minutes Incubationwith Polymorphonuclear Leucocytes
Staph Paracolon Staph ParacolonAureus Hafnia Aureus Hafnia
D. B. Normal control
%Viable Bacteria after 120 Minutes Incubationwith Polymorphonuclear Leucocytes
TABLE III
Patients studied with normal bactericidalactivity of PMN
PatientsDiagnosis studied Age range
yearsNormal children 10 2-14Normal adults 12 20-40Plasma cell hepatitis 1 22Dysgammaglobulinemia 1 14Lupus erythematosus 1 12Rheumatoid arthritis 1 13Ataxia telangiectasia 1 2Diabetes with nephrosis 1 9Chddiak-Higashi syndrome 1 9Aldrich's syndrome 2 3-4Hodgkin's disease 1 11Hemolytic anemia 2 2Sarcoidosis 2 22-40Cystic fibrosis 2 8-10Down's syndrome 2 1-4Recurrent pulmonary disease 4 2-15Brain damage (moribund) 2 2-15
Total 42
Staph ParacolonAureus Hafnia
L.J.
Staph ParacolonAureus Hafnia
Normal control
FIG. 2. LOCATION OF THE VIABLE BACTERIA AFTER IN-CUBATION FOR 120 MINUTES WITH POLYMORPHONUCLEARLEUKOCYTESFROMTWOOF THE PATIENTS WITH GRANULO-MATOUSDISEASE. Comparison with PMNfrom normalcontrols. Note that most of the bacteria still viable after120 minutes' incubation in the phagocytic system were lo-cated in the leukocyte pellet of the patients with granu-lomatous disease.
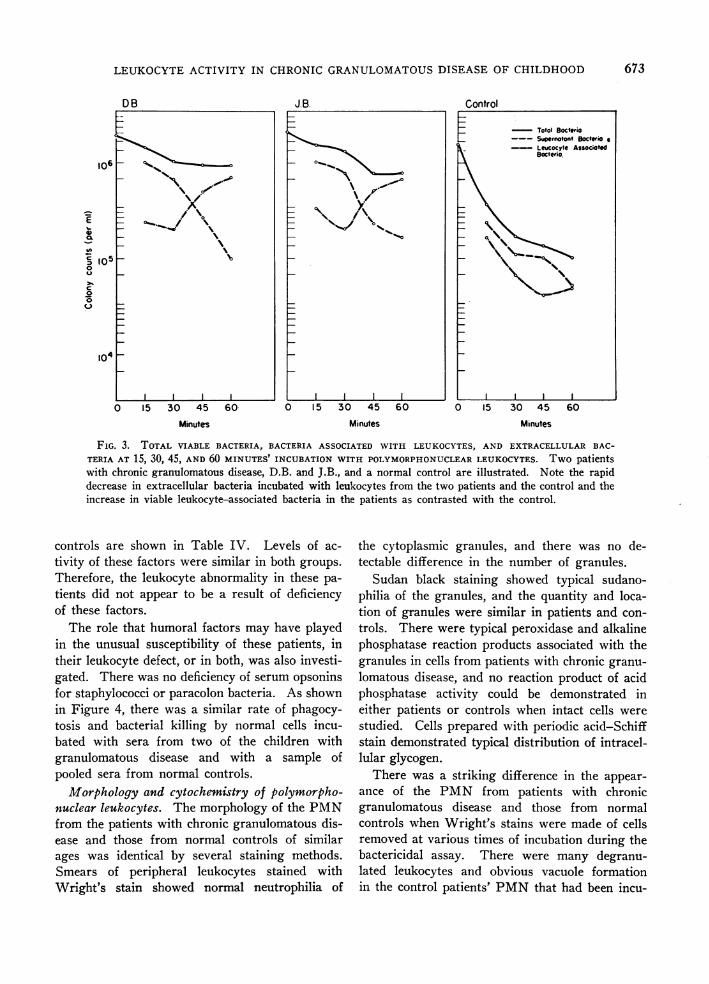
the greatest number of viable bacteria after 2hours' incubation was found associated with theleukocytes. Figure 3 shows the rate of phagocy-tosis during the first 60 minutes of incubation withPMNfrom two patients with granulomatous dis-ease and a normal control. There was a rapiddecrease in the number of supernatant bacteria
with PMNfrom the patients as well as the con-trols. The viable bacteria in preparations withPMNfrom patients with chronic granulomatousdisease were found associated with the leukocytesduring the first few minutes of incubation, andthere was no evidence for delayed phagocytosisof S. aureus or P. hafnia in the presence of normalserum in this in vitro system.
Attempts to delineate the nature of the abnor-mality in the polymorphonuclear leukocytes in-cluded the assay of bactericidal factors lysozymeand phagocytin. Comparison of the activities ofthese granule-associated factors in the extractsof leukocytes from three children with granuloma-tous disease and in extracts from two normal
TABLE IV
Enzyme activity of leukocyte extracts
Total % Lyso- Phago-Patient leukocytes PMN zyme* cytint
L.J. Granulomatous 4.2 X107 60 12 20disease
D.B. Granulomatous 5.7 X107 40 48 40disease
T.W. Granulomatous 5.6 X107 35 24 40disease
L.S. Normal adult 4.6 X107 40 12 40E.A. Normal adult 4.0 X107 55 24 10
* Reciprocal of dilution of leukocyte extract in distilled water thatgave activity equivalent to 2 u egg white lysozyme.
t Reciprocal of dilution of leukocyte extract in citric acid that killedgreater than 50% of 1 X106 salmonella per ml.
100
80
60OS0
40
20
0
30
500/
E
40
20
0
672
LEUKOCYTEACTIVITY IN CHRONICGRANULOMATOUSDISEASE OF CHILDHOOD
DB J.B. Control
0 15 30 45
Minutes
60 0 15 30 45 60 0 15 30 45 60
Minutes Minutes
FIG. 3. TOTAL VIABLE BACTERIA, BACTERIA ASSOCIATED WITH LEUKOCYTES, AND EXTRACELLULARBAC-
TERIA AT 15, 30, 45, AND 60 MINUTES' INCUBATION WITH POLYMORPHONUCLEARLEUKOCYTES. Two patientswith chronic granulomatous disease, D.B. and J.B., and a normal control are illustrated. Note the rapiddecrease in extracellular bacteria incubated with leukocytes from the two patients and the control and theincrease in viable leukocyte-associated bacteria in the patients as contrasted with the control.
controls are shown in Table IV. Levels of ac-
tivity of these factors were similar in both groups.
Therefore, the leukocyte abnormality in these pa-
tients did not appear to be a result of deficiencyof these factors.
The role that humoral factors may have playedin the unusual susceptibility of these patients, intheir leukocyte defect, or in both, was also investi-gated. There was no deficiency of serum opsoninsfor staphylococci or paracolon bacteria. As shownin Figure 4, there was a similar rate of phagocy-tosis and bacterial killing by normal cells incu-bated with sera from two of the children withgranulomatous disease and with a sample ofpooled sera from normal controls.
Morphology and cytochemistry of polymorpho-nuclear leukocytes. The morphology of the PMNfrom the patients with chronic granulomatous dis-ease and those from normal controls of similarages was identical by several staining methods.Smears of peripheral leukocytes stained withWright's stain showed normal neutrophilia of
the cytoplasmic granules, and there was no de-tectable difference in the number of granules.
Sudan black staining showed typical sudano-philia of the granules, and the quantity and loca-tion of granules were similar in patients and con-
trols. There were typical peroxidase and alkalinephosphatase reaction products associated with thegranules in cells from patients with chronic granu-
lomatous disease, and no reaction product of acidphosphatase activity could be demonstrated ineither patients or controls when intact cells were
studied. Cells prepared with periodic acid-Schiffstain demonstrated typical distribution of intracel-lular glycogen.
There was a striking difference in the appear-
ance of the PMN from patients with chronicgranulomatous disease and those from normalcontrols when Wright's stains were made of cellsremoved at various times of incubation during thebactericidal assay. There were many degranu-lated leukocytes and obvious vacuole formationin the control patients' PMNthat had been incu-
106
E
- 00
Ca
-41
to
00c0s
5~~_*
A/..,
I l
673

QUIE, WHITE, HOLMES, AND GOOD
30 60 0 30
Minutes Minutes
60
Control
0 30 60Minutes
FIG. 4. COMPARISONOF SERUMAS OPSONIN FOR STAPHYLOCOCCUSAUREUSFROMTWOOF THE PATIENTS WITH
CHRONICGRANULOMATOUSDISEASE AND SERUMPOOLED FROM NORMALCONTROLS. Note the similar efficient bac-
tericidal capacity of the normal PMNwith 10% serum from either patient and controls. There was also a simi-lar decreased rate of bactericidal activity with lower concentrations of sera from the patients and from the controls.
bated with staphylococci or paracolon bacteria for60 minutes. Paracolon organisms were rapidlydigested, and even at 30 minutes' incubation therewere few intact intracellular bacteria. In con-
trast, when PMNfrom the children with chronicgranulomatous disease were incubated with para-
colon organisms, the intracellular bacteria ap-
peared relatively intact and there had been littledegranulation of the cytoplasm of the phagocytes.
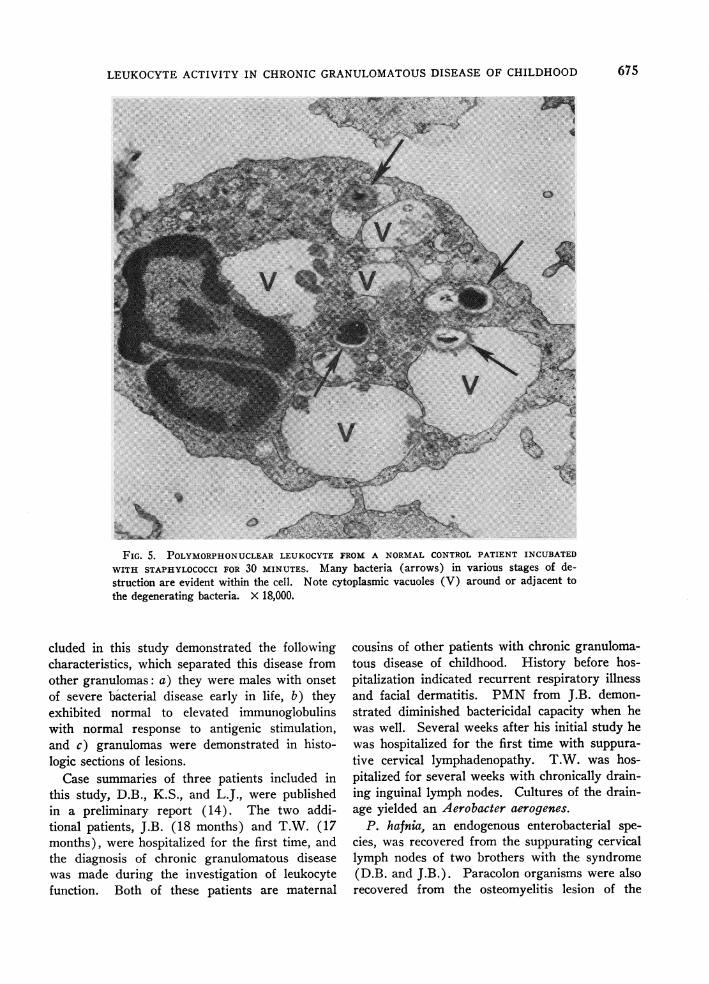
This difference in morphology was most strik-ingly demonstrated in studies with the electronmicroscope. Figure 5 shows a PMNfrom a nor-
mal control after 30 minutes' incubation with
staphylococci. Extensive degranulation and vacu-
ole formation are obvious. The early stages of
digestion of staphylococci in the large vacuoles
can be seen. Paracolon organisms were almost
completely destroyed within the neutrophil vacu-
ole at the same time interval.
Figure 6 shows a PMNfrom one of the patientswith granulomatous disease. The intracellular
location of the bacteria is apparent within phago-cytic vacuoles. However, unlike Figure 5, there
is little degranulation of the neutrophil and vir-tually no evidence of digestion of the intracellularbacteria. Even the paracolon bacteria, whichwere rapidly digested by the PMNfrom normalcontrols, were found to be morphologically intactafter 60 minutes' incubation with PMNfrom pa-
tients with granulomatous disease (Figure 7).
Discussion
This investigation of the bactericidal capacityof polymorphonuclear leukocytes from patientswith increased susceptibility to bacterial infectionallowed determination of engulfment of bacteriaand the fate of ingested organisms. A consistentdefect in bactericidal capacity after ingestion ofbacteria was demonstrated in five patients with a
disease entity termed chronic granulomatous dis-ease of childhood. This syndrome was thoroughlystudied and separated as a specific disease entityby Berendes, Bridges, and Good (1, 2) and was
described by Landing and Shirkey (3) and Car-son and associates (4). All of the patients in-
E
0-C-
40c
0w
674
LEUKOCYTEACTIVITY IN CHRONICGRANULOMATOUSDISEASE OF CHILDHOOD
i
FIG. 5. POLYMORPHONUCLEARLEUKOCYTEFROM A NORMALCONTROLPATIENT INCUBATEDWITH STAPHYLOCOCCIFOR 30 MINUTES. Many bacteria (arrows) in various stages of de-struction are evident within the cell. Note cytoplasmic vacuoles (V) around or adjacent tothe degenerating bacteria. X 18,000.
cluded in this study demonstrated the followingcharacteristics, which separated this disease fromother granulomas: a) they were males with onsetof severe bacterial disease early in life, b) theyexhibited normal to elevated immunoglobulinswith normal response to antigenic stimulation,and c) granulomas were demonstrated in histo-logic sections of lesions.
Case summaries of three patients included inthis study, D.B., K.S., and L.J., were publishedin a preliminary report (14). The two addi-tional patients, J.B. (18 months) and T.W. (17months), were hospitalized for the first time, andthe diagnosis of chronic granulomatous diseasewas made during the investigation of leukocytefunction. Both of these patients are maternal
cousins of other patients with chronic granuloma-tous disease of childhood. History before hos-pitalization indicated recurrent respiratory illnessand facial dermatitis. PMNfrom J.B. demon-strated diminished bactericidal capacity when hewas well. Several weeks after his initial study hewas hospitalized for the first time with suppura-tive cervical lymphadenopathy. T.W. was hos-pitalized for several weeks with chronically drain-ing inguinal lymph nodes. Cultures of the drain-age yielded an Aerobacter aerogenes.
P. hafnia, an endogenous enterobacterial spe-cies, was recovered from the suppurating cervicallymph nodes of two brothers with the syndrome(D.B. and J.B.). Paracolon organisms were alsorecovered from the osteomyelitis lesion of the
675
file

QUIE, WHITE, HOLMES, AND GOOD
-4 -.
FIG. 6. POLYMORPHONUCLEARLEUKOCYTEFROMA CHILD WITH CHRONIC GRANULOMATOUSDISEASE INCUBATED WITH STAPHYLOCOCCI FOR 1 HOUR. Several bacteria (arrows) arevisible in the cytoplasm. Little degranulation is evident. X 22,500.
metacarpal and calcaneous of D.B. A maternallyrelated cousin of these two boys (K.S.) sufferedsevere recurrent infiltrative pulmonary diseaseover a 6-year period. He was hospitalized dur-ing part of the time of this study for drainage ofa rectal abscess, from which an aerobacter specieswas cultured.
The bacteria associated with the suppurative le-sions in these children were species indigenous tothe upper respiratory and gastrointestinal tractsof man and species that are usually rapidly phago-cytized and killed by polymorphonuclear leuko-cytes in vitro and presumably in vivo. Therefore,the existence of an abnormality of function ofleukocytes was postulated on the basis of clinicalevidence when this disease entity was described(2). This prediction is borne out in the present
study by the demonstration of prolonged viabilityof S. aureus and P. hafnia in the polymorpho-nuclear leukocytes of these patients.
All of these children had male family memberswho also demonstrated the syndrome of chronicgranulomatous disease. Brothers of two of thechildren (L.J. and K.S.) died from sepsis andwith granulomatous disease in infancy. Two ofthe patients (D.B. and J.B.) were brothers andmaternal cousins of K.S. Patient T.W. is thematernal cousin of two brothers, one living andone dead, who presented the clinical features ofchronic granulomatous disease.
As was the case with patients previously de-scribed, these five patients with chronic granulo-matous disease were normal in capacity to re-spond to antigenic stimulation with heterologous
676

LEUKOCYTEACTIVITY IN CHRONICGRANULOMATOUSDISEASE OF CHILDHOOD
FIG. 7. POLYMORPHONUCLEARLEUKOCYTE FROM A CHILD WITH CHRONIC GRANULOMATOUSDISEASE INCUBATED FOR 1 HOURWITH PARACOLANHAFNIA. Intact intracellular bacteria areevident (arrows). X 46,000.
antigens and had normal or elevated levels of cir-culating antibody and complement and the normalspectrum of immunoglobulins. Ability to developdelayed hypersensitivity was also found to be nor-mal. The patients also demonstrated typical poly-morphonuclear leukocytosis during episodes ofsystemic illness. Their total peripheral leukocytecounts ranged from 6 to 30,000 per mm3. Therewas obvious suppuration of lesions, and PMNmigrated normally to the skin windows when theinflammatory cycle in these patients was studiedby the technique of Rebuck and Crowley (15).Furthermore, the phagocytic capacity of poly-morphonuclear leukocytes appeared to be normalas determined by observation of intracellular
bacteria on stained smears of PMN-bacteriamixtures.
The significance of prolonged viability of bac-teria in polymorphonuclear leukocytes in our pa-tients in the pathogenesis and the presence ofgranulomas in the tissues is uncertain. It isknown that long continued presence of intracellu-lar viable microorganisms commonly results inchronic inflammatory response. For example,there are many species of microorganisms thathave the capacity to survive in human PMN, e.g.,tubercle bacillus, brucella, and listeria. The pres-ence of these organisms commonly results in achronic granulomatous process (16). Therefore,the prolonged presence of bacteria or bacterial
677
QUIE, WHITE, HOLMES, AND GOOD
products that are ordinarily quickly detoxified anddigested by normal PMNmay be basic to thedevelopment of a granulomatous inflammatory re-sponse in these patients with diminished capacityfor intracellular digestion of ubiquitous bacteria.These bacteria then would behave in children withchronic granulomatous disease in a fashion simi-lar to tubercle bacilli or brucella in infected indi-viduals having normal function of their poly-morphonuclear leukocytes.
The metabolic basis for the defect in bactericidalcapacity is not known; however, there was a strik-ing and consistent difference in the extent of cyto-plasmic reaction to phagocytosis in the PMNfrompatients with granulomatous disease and controls.In the controls, there was extensive degranulationand vacuole formation with visible disintegrationof the ingested bacteria, even after short periodsof incubation. The polymorphonuclear leukocytesfrom patients with chronic granulomatous diseaseof childhood did not respond to phagocytosis withsimilar extensive degranulation. In the electronmicroscopic examination, there were visible mem-branes surrounding ingested particles, but withintact granules in the surrounding cytoplasm. Inaddition, bacteria in PMNfrom the granuloma-tous patients were generally intact, indicating fail-ure or delay of digestive processes. The presenceof intact intracellular organisms in the electronmicrographs support data obtained by colonycounts of viable bacteria associated with leuko-cytes after differential centrifugation of incubatedphagocyte-bacteria mixture.
The morphologic evidence of intact cytoplas-mic granules after phagocytosis is of particularinterest, since the total quantity of the bactericidalfactors lysozyme and phagocytin in extracts ofthe leukocytes from the patients and from normalcontrols was comparable. These bacterial factors,as well as many of the hydrolytic digestive en-zymes, are known to be associated with the leuko-cyte granules (17). It has been demonstratedthat after phagocytosis there is a release of en-zymes from the granule fraction into the super-natant fraction as active soluble enzyme (18).Hence, the demonstration of minimal degranula-tion after phagocytosis within leukocytes withdefective antibacterial activity suggested a lackof availability of bactericidal factors and digestiveenzymes rather than absence of these factors.
Evidence that phagocytosis and degranulationin cells after particle ingestion is associated withseveral metabolic changes has been presented (16,18). The studies presented here provide evi-dence for a distinct separation of the metabolicevents involved in phagocytosis and those neces-sary for degranulation and particle digestion.Thus, these patients provide a unique opportunity,permitting investigation of relationships betweenmetabolic events that are related to phagocytosisper se and those that are associated with degrantu-lation and digestion of ingested material.
Acknowledgments
The technical help of Miss 0. Linda Schneider wasessential for these studies. We are indebted to Dr.Dorothy Sundberg for histochemical studies on bloodsmears.
References
1. Berendes, H., R. A. Bridges, and R. A. Good. Afatal granulomatosus of childhood: the clinicalstudy of a new syndrome. Minn. Med. 1957, 40,309.
2. Bridges, R. A., H. Berendes, and R. A. Good. Afatal granulomatous disease of childhood: the clini-cal, pathological, and laboratory features of a newsyndrome. Amer. J. Dis. Child. 1959, 97, 387.
3. Landing, B. H., and H. S. Shirkey. A syndrome ofrecurrent infection and infiltration of viscera bypigmented lipid histiocytes. Pediatrics 1957, 20,431.
4. Carson, M. J., D. L. Chadwick, C. A. Brubaker, R. S.Cleland, and B. H. Landing. Thirteen boys withprogressive septic granulomatosis. Pediatrics 1965,35, 405.
5. Maal0e, O. On the Relation between Alexin andOpsonin. Copenhagen, Ejnar Munksgaard, 1946.
6. Cohn, Z. A., and S. I. Morse. Interactions betweenrabbit polymorphonuclear leukocytes and staphylo-cocci. J. exp. Med. 1959, 110, 419.
7. Hirsch, J. C., and B. Strauss. Studies on heat-labileopsonin in rabbit serum. J. Immunol. 1964, 92,145.
8. Shinefield, H. R., J. C. Ribble, M. Boris, and H. F.Eichenwald. Bacterial interference: its effect on
nursery-acquired infection with Staphylococcusaureus. I. Preliminary observations on artificialcolonization of newborns. Amer. J. Dis. Child.1963, 105, 646.
9. Hayhoe, F. G. J., D. Quaglino, and R. Doll. Cytol-ogy and cytochemistry of acute leukaemias. Spec.Rep. Ser. med. Res. Coun. (Lond.) 1964, no. 304,11.
678
LEUKOCYTEACTIVITY IN CHRONICGRANULOMATOUSDISEASE OF CHILDHOOD
10. White, J. G., and W. Krivit. The ultrastructurallocalization and release of platelet lipids. Blood1966, 27, 167.
11. Hirsch, J. G., and A. B. Church. Adrenal steroidsand infection: the effect of cortisone administra-tion on polymorphonuclear leukocytic functions andon serum opsonins and bactericidins. J. clin. Invest.1961, 40, 794.
12. Shugar, D. The measurement of lysozyme activityand the ultra-violet inactivation of lysozyme. Bio-chim. biophys. Acta (Amst.) 1952, 8, 302.
13. Hirsch, J. G. Further studies on preparation andproperties of phagocytin. J. exp. Med. 1960, 111,323.
14. Holmes, B., P. G. Quie, D. B. Windhorst, and R. A.Good. Fatal granulomatous disease of childhood.
An inborn abnormality of phagocytic function.Lancet 1966, 1, 1225.
15. Rebuck, J. W., and J. H. Crowley. A method ofstudying leukocytic functions in vivo. Ann. N. Y.Acad. Sci. 1955, 59, 757.
16. Cohn, Z. A., and K. F. Austen. Contribution ofserum and cellular factors in host defense reactions.II. Cellular factors in host resistance. New Engl.J. Med. 1963, 268, 1056.
17. Cohn, Z. A., and J. G. Hirsch. The isolation andproperties of the specific cytoplasmic granules ofrabbit polymorphonuclear leukocytes. J. exp. Med.1960, 112, 983.
18. Cohn, Z. A., and J. G. Hirsch. The influence ofphagocytosis on the intracellular distribution ofgranule-associated components of polymorpho-nuclear leukocytes. J. exp. Med. 1960, 112, 1015.
679


















