In vitro activity of new macrolides against respiratory...
7
OF RTI In vitro activity of new macrolides against respiratory pathogens MlCHEL G BERGERON, MD, FRCPC FULL POTENTI AL OF THE MACROLIDES HAS BEEN LIMITED .l due to the incidence of side effects, variable oral absorption, short half-life necessitating qid dosing, and limited spectrum of activity against several pathogens, including Haemophilus injluenzae. In contrast to older macrolides, which often have been cons id ered as sec- ond choice drugs with a very narrow spectrum of activ- ity, clarithromycin and other newer macrolides, including azithromycin, roxithromycin , rokitamycin and dirithromycin, can now be considered as broad spectrum antimicrobial agents and will now be used as first choice drugs for the treatment of several infectious diseases. This review eval ua tes the comparative activity of clarithromycin with other macrolides, and several anti- microbial agents used for the treatment of respiratory pathogens. STRUCTURE/FUNCTION ACTIVITY Macrolides are natural or semi-synthetic agents characterized by a classic macrocyclic ring of lactone type co mpo sed of 12 t.o 16 atoms from which the name is derived ( Table 1). Erythromycin is a 14-ring macrolide (13 carbon and one oxygen). Introducing chemical modifications at. C6. Cs. Cg, C11 and C12 in the basic molecule has allowed for more stability in acid medium, better absorption and improved pharmacol - ogy. and better in vitro and in vivo antibacterial activity in inf ected. inflamed and purulent sites which are often ac idic. Clarithromycin differs from erythromycin by an 0- methyl substitution at position 6 of the lactone ring. Clarithromycin is metabolized by the liver in vivo to an active metabolite. 14-hydroxy clarithromycin (Figure 1). This metabolite is more active in vitro against several pathogens including beta -lactamase negative and posi- tive H injluenzae strains. All macrolides inhibit RNA-dependent protein syn- thesis. can block transpeptidation and/or transloca- tion and bind reversibly to ribosomal 50s subunit, specif ically the P site. In vitro lincomycin and chloram- phenicol compete with erythromycin and can be an- tagonistic. ANTIBACTERIAL ACTIVITY The macrolides can be bacte ri cida l or bacteriostatic. depending on concentration . microbial species, inocu - lum size and growth phase of bacteria. In general, their activity is increased by an alkal ine environment. This can be explained by the fact. U1at. U1e penetration of weak bases like macrolides through the bacte ri al wall is better when they are ionized. Being acid-stable. the newer macrolides. like clarithromycin. have an im- proved in vitro activity over that of old er macrolides in such an enviromnenl. In vitro activity of clarithromycin and its 14 -hy- droxy metabolite against H in.fluenzae: One of the major factors lin1iting the use of erythromycin in respir - atory tract infections has been it.s poor in vitro aclivity against H iqjluenzae. In a recently publis h ed study (1). Department of Microbiology. Laval University. Laboratory and lrif ecLious Diseases Service. Centre HospiLalier de l"Universile Laval. Quebec. Quebec Correspondence: Dr Michel G Bergeron. Laboratory and l'1fectious Diseases Service. Centre Hospitali.er de l"Universit.e Laval. 2705 boulevard Laurier. SLe-Foy. Quebec. Quebec G 1 V 4G2. Telephone (418) 654- 2705. Fax (418) 654 -2715 CAN J INFECT DIS VOL 4 SUPPL A APRIL 1993 13A
Transcript of In vitro activity of new macrolides against respiratory...

OF RTI
In vitro activity of new macrolides against
respiratory pathogens MlCHEL G BERGERON, MD, FRCPC
~E FULL POTENTIAL OF THE MACROLIDES HAS BEEN LIMITED
.l due to the incidence of side effects, variable oral absorption, short half-life necessitating qid dosing, and limited spectrum of activity against several pathogens, including Haemophilus injluenzae. In contrast to older macrolides, which often have been considered as second choice drugs with a very narrow spectrum of activity, clarithromycin and other newer macrolides, including azithromycin, roxithromycin, rokitamycin and dirithromycin, can now be considered as broad spectrum antimicrobial agents and will now be used as first choice drugs for the treatment of several infectious diseases.
This review evaluates the comparative activity of clarithromycin with other macrolides, and several antimicrobial agents used for the treatment of respiratory pathogens.
STRUCTURE/FUNCTION ACTIVITY Macrolides are natural or semi-synthetic agents
characterized by a classic macrocyclic ring of lactone type composed of 12 t.o 16 atoms from which the name is derived (Table 1). Erythromycin is a 14-ring macrolide (13 carbon and one oxygen). Introducing chemical modifications at. C6. Cs. Cg, C11 and C12 in the basic molecule has allowed for more stability in acid medium, better absorption and improved pharmacology. and better in vitro and in vivo antibacterial activity in infected. inflamed and purulent sites which are often acidic.
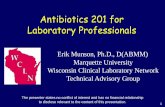
Clarithromycin differs from erythromycin by an 0-methyl substitution at position 6 of the lactone ring. Clarithromycin is metabolized by the liver in vivo to an active metabolite. 14-hydroxy clarithromycin (Figure 1). This metabolite is more active in vitro against several pathogens including beta-lactamase negative and positive H injluenzae strains.
All macrolides inhibit RNA-dependent protein synthesis. can block transpeptidation and/or translocation and bind reversibly to ribosomal 50s subunit, specifically the P site. In vitro lincomycin and chloramphenicol compete with erythromycin and can be antagonistic.
ANTIBACTERIAL ACTIVITY The macrolides can be bactericidal or bacteriostatic.
depending on concentration . microbial species, inoculum size and growth phase of bacteria. In general, their activity is increased by an alkaline environment. This can be explained by the fact. U1at. U1e penetration of weak bases like macrolides through the bacterial wall is better when they are ionized. Being acid-stable. the newer macrolides. like clarithromycin. have an improved in vitro activity over that of older macrolides in such an enviromnenl. In vitro activity of clarithromycin and its 14-hydroxy metabolite against H in.fluenzae: One of the major facto rs lin1iting the use of erythromycin in respiratory tract infections has been it.s poor in vitro aclivity against H iqjluenzae. In a recently published study (1).
Department of Microbiology. Laval University. Laboratory and lrifecLious Diseases Service. Centre HospiLalier de l"Universile Laval. Quebec. Quebec
Correspondence: Dr Michel G Bergeron. Chi~[ Laboratory and l '1fectious Diseases Service. Centre Hospitali.er de l"Universit.e Laval. 2705 boulevard Laurier. SLe-Foy. Quebec. Quebec G 1 V 4G2. Telephone (418) 654-2705. Fax (418) 654-2715
CAN J INFECT DIS VOL 4 SUPPL A APRIL 1993 13A

BERGERON
TABLE 1 Macrolides of today and tomorrow
Cycle
12C 14C
15C 16C
Macrolides
Methymycin. neomethycin. YC-17. litorin Natural compounds: erythromycin A and F.
oleandomycin Semi-synthetic agents: roxithromycin.
dirithromycin, flurithromycin. clarithromycin , davercin
Azithromyc in (azalide) Natural compounds: josamycin. kitasamycin.
spiramycin. midecamycin Semi-synthetic agents: rokitamycin.
miokamycin
we evaluated U1e in vitro activity of clarithromycin and its major 14-hydroxy metabolite, alone or in combination. against beta-lactamase positive and negative strains of H injluenzae.
Two hundred and U1ree strains selected from our previous study on the epidemiology of H irifl.uenzae resistance in Canada (2) were evaluated. Characteristics of the strains studied are presented in Table 2.
Antibiotic susceptibility testing was done according to the National Committee for Clinical Laboratory Standards (NCCLS) (3) . In short. log-phase broth dilu tion susceptibility testing was performed with a microdilution method using Haemophilus Test Media (HTM). HTM was prepared as described by Jorgensen et al (4).
Erythromycin : R1 =H, R2=H2
Clarithromycin (A-56268): R1 =CH 3 , R2=H2
14-0H Metabolite (A-62671): R 1 =CH3 , R2=0H
F igure 1) Chemical structures of erythromycin. clarithromycin and its 14-hydroxy metabolite
l4A
TABLE 2 Summary of Haemophilus influenzae strains evaluated
Beta-lactamase production status: Positive Negative
Strains isolated from:
Blood Ear Cerebrospinal fluid Eye
Sputum
TABLE 3
Number(%)
71 (35) 132 (65)
61 (30) 53 (26.1) 45 (22.2) 19 (9.4)
25 (12.3)
Susceptibility of H influenzae to clarithromycin and 14-hydroxy clarithromycin (mg/L)
MICro MIC9o Range MBC90 Range Clarithromycin
Al l strains (n=203) 4 8 2-8 8 1-16
Serotype B (n=l05) 4 4 2-8 8 0.5-£ Serotype non-B (n=98) 4 8 2-8 8 1-16
14-hydroxy clarithromycin All strains (n=203) 2 2 1-4 2 0.5-16 Serotype B (n= l 05) 2 2 1-4 2 1-8 Serotype non-B (n=98) 2 4 1-4 4 0.5-16 Reproduced with permission from Bergeron eta/ (1)
The checkerboard technique was used to determine the activity of combinations of clarithromycin and 14-hydroxy clarithromycin (5). The technique was performed in 96-well microplates containing HTM. Fractional inhibitory concentrations (FICs) were calculated for each agent by dividing the minimum inhibitory concentration (MIC) of the agent in combination by the MIC of the agent alone.
The FIC index was defined as the sum of the individual FICs at the most effective concentrations. The com-
TABLE 4 In vitro effect of the combination of clarithromycin and 14-hydroxy clarithromycin against H influenzae by site: Results of checkerboard
Source of Beta-lactamase Beta-lactamase H positive strains negative strains influenzae Additive Synergistic Additive Synergistic isolates (%~ (%~ (%~ (%~
Blood 12 (92.3) 1 (7.7) 45 (95.7) 2 (4.3) Ear 7 (77.8) 2 (22.2) 40 (97.6) l (2.4) CSF 6 (85.7) 1 (14.3) 26 (78.8) 7 (21 .2) Eye 16(94.1) 1 (5.9) 1 (100) 0 Sputum 19 (100) 0 4 (100) 0
Total 60 (92.3) 5 (7 .7) 116 (92.1) 10 (7 .9) Overall, ac tivity was additive in 92% (176/ 191) and synergistic in 8% (15/ 191). No antagonism was demonstrated. CSF Cerebrospinal fluid. Reproduced with permission from Bergeron eta/ (1)
CAN J INFECT DIS VOL 4 SUPPL A APRIL 1993

bination was defined as synergistic if the FIC index was 0.5 or less, additive if it was 1, and antagonistic if the FIC index was 4.0 or greater.
The MIC5o, MICgo and minimum bactericidal concentration (MBC) for clarithromycin and 14-hydroxy clarithromycin are presented in Table 3. There were no major differences in the susceptibility between B and non-B serotypes. Moreover, for the non-B serotypes or for the different biotypes, no special pattern of susceptibility was observed.
Results of the checkerboard tests for the combination of clarithromycin and 14-hydroxy clarithromycin are presented in Table 4. Overall, activity was additive in 92% (176 of 191) and synergistic in 8% (15 of 191). There was no difference in the activity of clarithromycin against beta-lactamase positive and negative strains. The site of isolation did not influence the susceptibility of H irifl.uenzae to the combination of clarithromycin and 14-hydroxy clarithromycin.
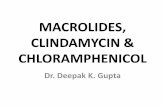
The effect of the combination clarithromycin and 14-hydroxy clarithromycin was also demonstrated using growth curves on strain 133, a strain against which the combination was shown to be synergistic (Figure 2).
Overall. when compared to macrolides available and under investigation, the 14-hydroxy clarithromycin was shown to be the most effective drug against H irifl.uenzae (Table 5) (1.6). Approximately 25 to 30% or more H injluenzae strains are developing resistance to ampicillin in many regions of the world (2,7,8); therefore, clarithromycin may prove to be a potential alternative to ampicillin .
Based on pharmacokinetic considerations, Hanson et al (9) and Hoover et al (10) have proposed interpretive susceptibility criteria for clarithromycin. Interpretive criteria for in vitro testing of clarithromycin have now been established by the NCCLS (11). Table 6 shows the interpretive criteria for all pathogens including H injiuenzae. Using these criteria, H influenzae is usually susceptible to clarithromycin on HTM incubated in normal atmosphere. As demonstrated in the study presented here, the anti-haemophilus activity of clarithromycin is significantly enhanced by the presence of its active major metabolite, 14-hydroxy clarithromycin.
In this study all of 203 clinically obtained H irifl.uenzae strains (including beta-lactamase positive strains) were susceptible to clarithromycin and to its major human metabolite. 14-hydroxy clarithromycin. Clarithromycin and its metabolite were additive or even synergistic in killing these same H influenzae strains. Overall , the isolation site, the production or absence of beta-lactamase, the serotype and the biotype did not modify the susceptibility of either drug or their combination.
Other data suggest that these in vitro results with clarithromycin will correlate with favorable in vivo outcomes. When orally administered to gerbils with experimental H irifl.uenzae otitis media. clarithromycin and
CAN J INFECT DIS V OL 4 SUPPL A APRIL 1993
Y·DO In vitro activity of new macrolides
10
I
LOG r ~~~-::--._, CFU/mL
1 111
4
2
o ~~~--L-~--L-~~--~~~~~-L-o.o 4.0 1.0 12.0 111.0 20.0 24.0
Time (h)
Figure 2 ) Growth curves of strain 133 ojH influenzae exposed to the combination clarithromycin and 14-hydroxy clarithromycin. This combination has been shown to be synergistic with an FIC oj0.5. • 14-hydroxy 0.5 ~tg/rnL: 0 Clarithromycin 1 ~tg/mL: • Clarithromycin 1 119/ rnL + 14-hydroxy 0.5 pg/ rnL: 0 Growth without antibiotic
TABLE 5 Range and MIC9o (mg/ L) of macrolides against H intluenzae
MIC (mg/L) Dru s Ran e MIC90 Erythromycin (14C)* 1-16 4 Clarithromycin (14C)t 2-8 8 14-hydroxy clarithromycin ( 14C) t 1-4 2 Roxithromycin (14C)* 8-16 16 Azithromycin (15C)* 0.12-8 4 Rokithromycin (16C)* 4-16 >16 • Neu eta/ (6): t Bergeron eta/ (1)
TABLE 6 Criteria for susceptibility testing of clarithromycin
MIC (mg/L) Zone diameter (mm)* S I R S I R
Al l microorganisms $2 (except Haemophilus and Staphvlococcus)
Haemophilus $8 species
~8 ~ 18 14-17 $13
~32 ~ 13 1 1-12 $1 0
'According to NCCLS, December 1992, 15 ~g disc. All microorganisms. except H influenzae, were tested using Mueller-Hinton agar. H influenzae were tested on Haemophilus Test Medium. /Intermediary: R Resistant: S Susceptible
14-hydroxy clarithromycin were synergistic or additive in reducing middle ear colony counts and increasing cure rates (12). Several clinical studies of patients with H irifl.uenzae respiratory infections have compared clarithromycin treatment against oral cephalosporins. The clinical and bacteriological responses achieved with clarithromycin were equivalent to those obtained with ceflxirne. cefuroxime and cefaclor (13).
Other pathogens against which additive or synergis tic activity of the combination clarithromycin and 14-hydroxy clarithromycin has been shown include Moraxella catarrhalis, Legionella pneumophila. Strepto-
l5A

BERG ERO N
TABLE 7 Resistance (%) of pneumococci to penicillin and erythromycin throughout the world
E Penicillin (%)
Canada (1984-86) 1.3 USA (1979-87) 5.1 Europe (1981-86) 0.4 1.3 Spain (1982-89) 7.9 35.9 *France (1990) 29.0 12.0 Middle East I 2.9
Saudi Arabia (1985-86)
Asia/Malaysia (1984-85) 2.0 2.0 Africa (1983-86) 1.9 7.0
Adapted from Kluman eta/ (13). "Data from Geslin et of (14)
TABLE 8 Minimum inhibitory concentration breakpoints for susceptibility testing of pneumococcus
MIC (mg/L) Cote o PenG E Tetra TMP/SMZ Susceptible Intermediate
50.06 sO. 12-1
50.5 54 50.5/9.5
Resistant >1 ~ 1 ~8 s1/l9 Ery Erythromycin; Pen G Penicillin G; Tetra Tetracycline: TMP/SMZ Trimethoprim-sulphamethoxazole
coccus pyogenes. Enterococcus faecal is, Staphylococcus aureus and Streptococcus pneumoniae ( 14).
MACROLIDES AND PNEUMOCOCCI The pneumococci are still today one of the most
virulent and most important pathogens responsible for severe pneumonia. This pathogen, which has been generally considered to be uniformly susceptible to penicil lin and erythromycin, is now becoming resistant to both agents. Table 7 reveals the worldwide distribution of pneumococci resistant to either agent. While in Canada most S pneumoniae strains are still susceptible to both drugs, the percentage of resistance to penicillin has reached 36% in Spain while close to 30% are now resistant to erythromycin in France (15,16). While the penicillin-resistant strains are usually susceptible to erythromycins and vice versa, strains resistant to erythromycin are also resistant to all macrolides. Table 8 lists the MIC breakpoints for susceptibility testing of pneumococci. Clarithromycin has also been demonstrated to have the lowest MIC of the macrolides against pneumococci (Table 9) (17) . Other streptococci, including Streptococcus agalactiae and S pyogenes, are exclusively susceptible to all macrolides (6).
MACROLIDES AND M CATARRHALIS M catarrhalis is now considered one of the most
commonly recovered pathogens in upper (otitis) and lower respiratory tract infections. A recent report from England and Scotland shows that 91% of the isolates were resistant to ampicillin (18) . Most strains of
16A
TABLE 9 Macrolides versus penicillin against penicillin-resistant and penicillin-susceptible strains of pneumococci
MIC90 (mg/L) Antimicrobial Penicillin-resistant Penicillin-susceptible Erythromycin 0.12 0.12 Clarithromycin 0.06 0.06 Azithromycin 0.12 0.12 Penici llin 1.0 0.03
Adapted from Neal eta/ (15)
TABLE 10 In vitro activity of selected antimicrobials against Mycoplasma pneumoniae
MIC (mg/L) Dru Ran e MIC90 (m / L) Erythromycin (14C)* 0.008-0.08 0.015 Clarithromycin (14C)* 0.008-0.002 0.008 Roxithromycin (14C)* 0.008-0.03 0.03 Tetracyc line t 0.39-12.5 6.25 Ofloxacint 0.2-1.56 0.78 Ciprofloxacin t 0.2-6.25 1.56 "Results from Felmingham D. First International Conference on Macro/ides, Azalides and Streptogramins. Santa Fe. New Mexico. 1992;1and from Arai S. Antimicrob Agents Chemother 1992;36:1322-4
M catarrhalis were exclusively susceptible to amoxicillin-clavulanate, cefaclor, loracarbef, ceftxime, and tetracycline. The MICgo for old or new macrolides has been in the region of 0.25 mg/L. with the exception of roxithromycin where the MICgo has been around 1 mg/L, suggesting that macrolides may be used for the treatment of this infection.
MACROLIDES AGAINST BORDETELLA PERTUSSIS, ANAEROBES, MYCOPLASMA, CHLAMYDIA,
LEGIONELLA AND MYCOBACTERIUM SPECIES Bordetella pertussis is uniformly susceptible lo all
macrolides. Gram-negative anaerobes including Bacteroides .fragilis, Bacteroides oralis and Fusobacterium species have variable susceptibility patterns to old and newer macrolides . MICs of these agents range between 0.25 and 30 mg/L or greater for most pathogens.
Macrolides have good in vitro activity against Mycoplasma pneumoniae (Table 10) and much lower MICs for this pathogen than tetracycline or quinolones (19) . Clarithromycin's MIC against Chlamydia pneumoniae is 0.03 mg/L and compares favorably with erythromycin (0.125 mg/L), roxithromycin (0.25 mg/L), azithromycin (0.25 mg/L), doxycycline (0.125 mg/L) and ofloxacin (0.5 mg/L) (20). Against Legionella pneumophila, all macrolides are effective. The MIC of clarithromycin for this organism was between 0 .25 and l mg/L. ln the pig model of L pneumophila, clarithromycin was shown to have better in vivo activity than erythromycin (14) . In the beige mouse infected with Mycobacterium avium in-
CAN J INFEC T DIS VOL 4 SUPPL A APRIL 1993

USE O LY • DO NOT COPY In vitro activity of new m acrolides
tracellulare, clarithromycin was shown to be more active than ciprofloxacin, rifampin and amikacin. In the rabbit foot Mycobacte1ium leprae infection , clarithromycin was more effective than roxithromycin and azithromycin (14). Whether these animal experiments will be applicable in humans remain to be proven. Against other Mycobacterium species including Mycobacterium jortuitum and Mycobacterium chelonae, clarithromycin was also superior to azithromycin and roxithromycin (14) .
MACROLIDES AGAINST NONRESPIRATORY PATHOGENS
Other pathogens including Listeria monocytogenes , Neisseria gonorrhoeae, Rhodococcus equi, Borrelia burgdoljeri, Clostridium perjringens, Gardnerella vaginalis , Mobiluncus species, Campylobacier jejuni. Helicobacter pylori and Propionibacterium acnes are also susceptible to most macrolides (14) . Rickettsiae species including Rickettsiae rickettsii and Rickettsiae conorii are less susceptible to macrolides (MIC. 1 to 8 mg/L) than to tetracycline (MIC, 0.25 mg/L) . Other pathogens against which further investigation may be of interest include Corynebacterium species, Rhodococcus equi, Rochalimea quintana and cats scratch bacillus. In animal models inflicted with Toxoplasma gondii. Trepan-
ACKNOWLEDGEMENTS: The secretarial work of Odette Guibord and the research assistance of Ma1i.he Bernier are greatly appreciated.
REFERENCES 1. Bergeron MG. Bernier M. L'Ecuyer J. In vitro activity of
clarithromycin and its 14-hydroxy m etabolite against 203 strains of Haernophilus irifluenzae. Infection 1992;20: 164-7 .
2. Tremblay LD. L'Ecuyer J . Provencher P. Bergeron MG. Canadian Study Group: Susceptibility of Haernophilus ir!fluenzae to antimicrobial agents used in Canada. Can Med Assoc J 1990: 143:895-900.
3 . National Committee for Clinical Laboratory Standards. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically. 2nd edn . Approved Standards NCCLS Documen t M7-A2. Villanova. PA: NCCLS. 1990.
4. Jorgensen JH, Redding JS. Maher LA. Howell AW. Improved medium for antimicrobial susceptibility testin g of Haernophilus ir!fluenzae. J Clin Microbic\ 1987:25:2075- 113.
5. Eliopoulos GM. Moellering RC Jr. Antimicrobial combinations. In : Lorian V. ed. Antibiotics in Laboratory Medicine. Baltimore: Willi ams and Wilkins Co. 1991 :432-92.
6. Neu HC. Chin NX. Gu JW. The in vitro activity of n ew streptogramins. RP 59500. RP 57669 and RP 54476. alone and in combination. J Antimicrob ChemoU1er 1992:30(Suppl A) :83-94.
7. Doem GV. Jones RN. Antimicrob ial susceptibility testing of Haernophilus injluenzae, Branharnella caiarrhalis . and Neisseria gonorrhoeae. Antimicrob Agents Chem ollier 1988:32: 17 4 7-53.
8. Kanellakopoulou K. Giamarellou H . Avlamis A.
CAN J INFECT DIS VOL 4 SUPPL A APRIL 1993
ema pallidum and B burgdoljeri. azithromycin appears to be slighUy superior.
With their respective protein binding of 50 lo 70% for azithromycin. 65 to 70% for clarithromycin and 90% or greater for roxithromycin , one may have to waH for further in vivo compa risons between these new generation macrolides to understand the real significance of the differen ces noted in the in vitro activity of those compounds. Moreover. these agents have marked pharmacokinetic differences which may further modify their in vivo activity. Penetration of newer macrolides into polymorphonuclear leukocytes is excellent (21). Some investigations even s uggest that macrolides may have immunomodulatory functions (22).
SUMMARY Clarithromycin and its microbiologically active 14-
hydroxy metabolite have additive and. at Urnes. synergistic , activity against H injluenzae. suggesting the potential clinical utility of clarithromycin for U1e treatment of H injluenzae infections. This increased antibacterial activity of the new macrolides and llieir potential use against a multitude of paU1ogens s uggest that clarithromycin and newer macrolides can now be called broad s pectrum antibiotics.
Surveillance study of resistance in Haemophilus species in Greece. Eur J Clin Microbial Infect Dis 1988:7: 186-8 .
9. Hanson CW. Bailer R. Gade E. Rode RA. Fernandes PB. Regression analysis. proposed interpretive zone size standards. and quality control guidelines for a new macrolide antimicrobial agent. A-56268 (TE-03 1) . J Clin Microbial 1987:25: 1079-82.
10. Hoover WW. Barrett MS. Jones RN. Clari lhromycin in vitro activity enhanced by its major metabolite. 14-hydroxy claiitllromycin . Oiagn Microbic\ Infect Dis 1992: 15:259-66.
11. National Committee for Clinical Laboratory Standards. Performed standards for antimicrob ial susceptib ility . NCCLS M 100/S4 Villanova: NCCLS. December 1992.
12. Hardy OJ, Swanson RN. Rode RA, Marsh K. Shipkowi tz NA. Clement JJ. Enh ancement of tile in vitro and in vivo activities of c\arilliromycin against Haemophilus ir!fluenzae by 14-hydroxy clmiU1romycin . its major m etabolite in humans. Antimicmb Agen ts Chemolhcr 1990:34:1407- 13.
13. Hardy OJ. Guay DRP. Jones R. ClariU1romycin. a unique macrolide: A pharmacokinetic. microbiologic and clinical overview. Oiagn Microbiollnfect Dis 1992:15:39-53.
14 . Mouton Y. Van der Auwera P. Premiere confe rence int.ernation ale sur les m acr olides. azal ides et slreptogramines. La Lettrc de l'infectiologie 1992:10:334-41.
15. Kluman KP. Pneumococcal resistance to antibiotics. Clin Microbial Rev 1990:3:17 1-6.
16 . Geslin P. Buu-Hoi A. Fremaux A. Acar JF. Antim icrobial resistance in Slreplococcus pnewnoniae: An epidemiological survey in France. 1970- 1990. Clin lnf Dis 1992: 15:95-8.
17. Neal TJ. O'Donoghue MA. Ridgway EJ. Allen KD. In vitro activity of len antimicrobial agents against pen ici llin -
17A

BERGERON
USEO J. resistant Streptococcus pneumoniae. J Antimicrob Chemother 1992;30:39-46.
18. Fung CP, Powell M, Seymour A. Yuan M, Williams JD. The antimicrobial susceptibility of Moraxella catarrhalis isolated in England and Scotland in 1991. J Antimicrob Chemother 1992;30:47-55.
19. Arai S, Gohara Y, Kuwano K, Kawashima T. Antimycoplasmal activities of new quinolones, tetracyclines, and macrolides against Mycoplasma pneumoniae. Antimicrob Agents Chemother 1992;36: 1322-4.
20. Hammerschlag MR. Qumei KK, Roblin PM. In vitro
18A
activities of azithromycin. clarithromycin. L-ofloxacin. and other antibiotics against Chlamydia pneumoniae. Antimicrob Agents Chemother 1992;36: 1573-4.
21. Ishiguro M, Koga H. Kohno S , Hayashi T, Yamaguchi K. Hirota M. Penetra tion of macro !ides into human polymorphonuclear leucocytes . J Antimicrob Chemother 1989;24:719-29.
22 . Joone GK. Van Rensburg. Anderson R. Investigation of the in vitro uptake. intraphagocytic biological activity and effects on neutrophil superoxide generation of dirithromycin compared with erythromycin. J Antimicrob Chemother 1992;30:509-23.
CAN j INFECT DIS V OL 4 SUPPL A APRIL 1993

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com