Improving Vascular Services A Case for Centralisation of ... · Cardiac and Stroke Networks in...
136
Cardiac and Stroke Networks in Lancashire & Cumbria Improving Vascular Services A Case for Centralisation of Vascular Services in Lancashire and Cumbria Version Final Date Sept 2010-March 2011 Author Natalie Park Email [email protected]
Transcript of Improving Vascular Services A Case for Centralisation of ... · Cardiac and Stroke Networks in...
Cardiac and Stroke Networks in Lancashire & Cumbria
Improving Vascular Services
A Case for Centralisation of Vascular Services in Lancashire and Cumbria
Version Final Date Sept 2010-March 2011 Author Natalie Park Email [email protected]
2
Contents Chapter 1 - Background 1.1 Review of Vascular Services in Lancashire and Cumbria 1.2 The Case for Change 1.3 Important Factors that Influence Patient Outcomes 1.4 Benefits of Centralisation 1.5 Impact 1.6 Risks
4
Chapter 2 - Epidemiology 2.1 Impact of Risk Factors-Epidemiological Information 2.2 Age 2.3 Diabetes 2.4 Obesity and Diabetes 2.5 Smoking 2.6 Targets for Reducing CVD
8
Chapter 3 - Vascular Procedures 3.1 What are Vascular Services? 3.2 Main Procedures to Consider
9
Chapter 4 - Present Providers 4.1Present Provider Landscape 4.2 Current Patient Flows 4.3 Information on all Sites Currently Providing Vascular Services
11
Chapter 5 - Length of Stay 5.1 Reducing Length of Hospital Stay by Centralisation 5.2 Length of Hospital Stay 5.3 Current Average Length of Stay in the Lancashire & Cumbria Network
20
Chapter 6 - Numbers of Specialists Required 6.1 Numbers of Surgeons Required for the Population 6.2 Numbers of Interventional Radiologists 6.3 Vascular Specialists 6.4 Vascular Nurse Specialists
22
Chapter 7 - Links with other Specialities 7.1 Critical Links - Specialties Supporting a Vascular Service 7.2 The Impact on Major Trauma and Stroke 7.3 Other Service Considerations 7.4 Amputations Amputee Rehabilitation in a Centralised Unit
23
Chapter 8 - Workload Requirements 8.1 Activity and Length of Stay Assessment 8.2 Day Case & GP Referral 8.3 Procedure Volume Requirement 8.4 Current Activity Across the Network 8.5 Figures Based on Minimum Population 8.6 Required Theatre Capacity
25
3
Chapter 9 - Proposed Models 9.1 Recommendations of the Review 9.2 Proposals & Network Formation 9.3 Proposals made by the Vascular Clinical Advisory Group 9.4 Formation of Vascular Network 9.5 Proposed Model Options One and Two 9.6 Workforce Planning 9.7 Patient & Public Involvement
28
Chapter 10 - Costs of Vascular Services 10.1 Tariff and Numbers of Vascular Procedures Commissioned 10.2 Procurement 10.3 Increased use of EVAR & Cost Implications 10.4 Reduced Aortic Aneurysm Repair Length of Stay Due to Increased Uptake of
Endovascular Aneurysm Repairs 10.5 Financial Implications for Providers 10.6 Reduced Length of Stay Following CEA 10.7 Productive Bed Use 10.8 Ambulance Implications
35
Chapter 11 - Implementation Plans 11.1 Implementation Timetable
38
Chapter 12 - Recommendation Checklist for Vascular Reviews Recommendations from other North West Reviews
38
Appendices Appendix 1 - Vascular procedure Levels 1- 4 Appendix 2 - Quality Standards Appendix 3 - Maps and location of each site within the review Appendix 4 Present Patient Pathways Newly Revised Patient Pathways Appendix 5 - Average Theatre Times and Procedures Appendix 6 - Rehab Amputation Team Appendix 7 - SUS data Appendix 8 - Information Provided by each PCT on Vascular Procedures
Commissioned 2009/10
4041
104110116123124126127
4
Chapter 1 Background 1.1 Review of Vascular Services in Lancashire and Cumbria
The focus of this review is to improve quality and safety for patients. Evidence based standards have been agreed which seek to ensure the highest standards of quality and patient safety. Implementation of those standards will require a change from the way services are currently provided.
This document explores the complexities of vascular interventions and its clinical interdependencies and sets out options for providing services across the Network.
1.2 The Case for Change
The initial impetus for a review of vascular services arises from the unsuccessful business case for an Abdominal Aortic Aneurysm (AAA) Screening Programme within Cumbria and Lancashire. There are around 6,000 deaths each year in England and Wales resulting from ruptured
AAAs. 95% of ruptured AAAs are in men over 65 Vascular disease (including death from ruptured AAAs) accounts for 40 per cent of
deaths in the UK. Vascular disease is as common as both cancer and heart disease.
The Evidence The Multicentre Aneurysm Screening Study (MASS) provided strong evidence for both the clinical benefit and the cost-effectiveness of a screening programme for abdominal aortic aneurysms (AAAs) in men. MASS concluded: The results support the expectation of very few emergency operations, and principally elective operations, being performed following the introduction of a screening programme. For a typical district general hospital, a screening programme would be expected to lead to two additional elective AAA operations per month, and to save 11 AAA-related deaths per year. Implications for Delivery of AAA Services Within Lancashire and Cumbria, the AAA Screening Programme will only be implemented when a full review of present vascular surgical providers has been completed and delivery of surgical repair of screen-detected aneurysms are seen to be being performed with the lowest possible mortality rates and best patient outcomes. Significant reductions in peri-operative deaths have been proven to be achieved through the centralised delivery of AAA repair. (Holt PJ, Poloniecki JD, Hinchliffe RJ, Loftus IM, Thompson MM. Model for the reconfiguration of specialized vascular services. The British journal of surgery 2008; 95(12):1469-74). Both The Vascular Society (VSGBI) and NCEPOD have recently published recommendations around emergency vascular provision. They stated that the best outcomes are achieved in specialist vascular units with dedicated vascular teams available 24 hours a day, seven days a week. (Abdominal Aortic Aneurysm: A Service in Need of Surgery, A report of the National Confidential Enquiry into Patient Outcome and Death, 2005: 11)
5
The present configuration of services in Cumbria and Lancashire does not promote the transfer of patients to high-volume centres so that these important advantages are available to them. The advent of screening for abdominal aortic aneurysms adds further importance to this work.
Crude Mortality Rates Displayed by Country for AAA Repair: Table 1 shows that the UK has the worst mortality rates. (7% in the UK, 2% in Italy) (The Vascular Society of Great Britain & Ireland. (2007). The provision of emergency vascular services) Table 1
Remodelling vascular services by reducing the number of providers would reduce mortality and morbidity after major vascular surgery by concentrating medical and nursing expertise.
1.3 Important factors that influence patient outcomes
Individual surgeons should maintain high volumes of surgery Surgeons that maintain high volumes of vascular surgery achieve mortality rates 2 - 4% lower than surgeons that perform low volumes of vascular surgery each year. (VSGBI 2009) There is also a clear link between the amount of surgery an individual surgeon does each year and their associated mortality outcomes. Studies have shown the principle reason high volume hospitals achieve better patient outcomes is because the surgeons tend to carry out high volumes of vascular procedures (Birkmeyer, J. D., Stukel, T. A., Siewers, A. E. Goodney, P. P., Wennberg, D. E. & Lucus, F. L. (2003). Surgeon volume and operative mortality in the United States. The New England Journal of Medicine, 349 (22): 2117-2127)
Modern surgical technologies
Presently across Lancashire and Cumbria, there is a significant variance in the uptake of minimally invasive vascular surgery. This means that the hospital where the patient has their surgery is a bigger determining factor in deciding the type of surgery they will have rather than their clinical need.
6
Some vascular procedures can be done using a modern, minimally invasive surgical method called endovascular surgery. Evidence shows that this type of surgery reduces length of hospital stay, reduces the risk of acquiring a hospital infection and most significantly, reduces surgical mortality by around 3% compared to traditional surgical methods.
Vascular surgery should be undertaken by a specialist vascular surgeon.
Institutions should perform high volumes of vascular surgery.
Hospitals performing high volumes of vascular surgery achieve significantly lower mortality than hospitals performing low volumes. (VSGBI 2009) A wealth of evidence supports the view that patients are less likely to suffer from post-operative strokes or die, when they have their carotid endarterectomy surgery at a hospital that performs a higher annual number of procedures.
(Feasby, T. E., Quan, H. & Ghali, W. A. (2002). Hospital and surgeon determinants of carotid endarterectomy outcomes. Archives of Neurology, 59: 1877-1881) (Holt, P. J. E., Poloniecki, J. D., Loftus, I. M. & Thompson, M. M. (2007). Meta-analysis and systematic review of the relationship between hospital volume and outcome following carotid endarterectomy. European Journal of Vascular and Endovascular Surgery, 33: 645-651)
In Lancashire and Cumbria the numbers of vascular procedures are classed as low volume - and mortality and length of stay compare badly to the rest of the UK.
1.4 The Benefits of Centralisation of Vascular Services
Central units would perform all elective and emergency arterial surgery Rapid access to diagnostics and interventions forms part of a high quality service. The need for this has been an important driver for centralisation, as it requires around the clock working, which larger units are better placed to provide. The units would be staffed by vascular specialists and would operate 24 hours a day,
seven days a week Performing all complex procedures at central units would ensure all patients have their
surgery at a high volume hospital by an experienced vascular specialist, using the latest technology and techniques
Centralisation should ensure improved facilities for patient care (dedicated vascular wards), investigation (larger radiology units with 24/7 interventional radiology) and treatment (vascular operating theatres and staff, vascular anaesthetists, improved facilities for endovascular management, better critical care).
When centralisation occurs, outpatient clinics and day surgery can continue in the hospitals that no longer have the primary service. The centralisation of vascular services to a small number of large centres is perhaps a radical option to consider but offers a number of potential benefits that are unlikely to be achieved through any other model, including: One or more specialist treatment centre for each vascular screening programme which
could provide administrative efficiencies Centralisation of resources, with the potential to reduce overall costs and improve
efficiency Dedicated vascular anaesthetic input High volumes of complex procedures per centre. Evidence for some procedures indicates
that the more procedures that are carried out the better the outcomes
7
Training of junior staff would be facilitated with concentrated high volume work Individual surgeon volumes more likely to be maintained despite the predicted shift away
from open surgical techniques towards endovascular technologies Potential cost savings in avoidance of duplication of complex equipment both within and
external to theatre Provision of comprehensive and sustainable 24/7 vascular radiology services.
Benefits for Academia and Research Central units would act as leading centres of research. This would mean greater opportunities for surgeons and specialists who want to pursue a joint career in academia and surgery. It would also help attract junior medical staff who will be the vascular specialists of the future. It is hoped that ongoing research can help define future management and treatment strategies for vascular diseases.
1.5 Impact
Centralisation of vascular services to one or more intervention centres within Lancashire and Cumbria with outreach for outpatients and day cases would mean: Patients would potentially need to travel further for their operation, as would their visitors Patients would be treated at a centre carrying out higher volumes of complex work, which
is linked to improved outcomes Patients would be treated by a surgeon or interventional radiologist carrying out large
volumes of complex work Patients would be able to access the full range of procedures 24/7 Fewer clinical staff overall would be needed.
1.6 Risks There are a number of risks inherent to this approach, including: Potential difficulties include, concerns on the part of hospitals losing vascular surgery and
insufficient capacity on a single site to manage the increase in workload and possibly a reluctance of surgeons to move sites.
The review has identified a shortage of trained interventional radiologists and, whilst work is underway to develop interventional radiology as a recognized sub-specialty, it is likely to take some years before this position changes. This issue exists even if the recommendations of this review are not followed through
Destabilisation of current providers through shifts in activity Management of patients who are too unstable to transfer for example post partum
haemorrhage may be delayed as the patient would either need to be transferred to the intervention centre or the surgeon would have to travel to the DGH
Creation of a two-tier service, with patients living further away from large centres failing to access care
Negative impact on relationships with other specialties for example renal and stroke services
Impact and cost implication of transferring patients Less contact/dialogue with primary care
8
Chapter 2 - Epidemiology 2.1 Impact of Risk Factors - Epidemiological Information
Population - the total population of Cumbria and Lancashire is just over two million and includes six Primary Care Trusts (PCTs) and five Acute Hospital Trusts, some of which link in with other sites to provide their Vascular cover. Cumberland Infirmary (CIC) in Carlisle takes vascular patients from Dumfries and
Galloway, which has a population of 148,000. Royal Preston Hospital (RPH) works as part of an emergency 1 in 6 rota to offer
emergency cover to Wigan, Bolton and Southport. The combined population of Wigan and Bolton PCTs is over 600,000. (Southport will be part of the Cheshire and Mersey Review)
This makes the combined population detailed within this review to 2.7 million 2.2 Age
The prevalence of vascular disease increases with age. The complexity, outcome and costs of vascular intervention are age-dependant. Average life expectancy continues to rise and this factor alone suggests that demand for vascular services is likely to continue to increase with time. Demographic changes are predicted within the two counties, particularly Cumbria,
which is projected to have a greater number of older people than the national average, which in itself predicts an aging population.
2.3 Diabetes
Diabetes prevalence almost doubled between 1994 and 2003. Vascular disease is the major cause of morbidity in diabetes and the risks of disease progression are higher. It is likely that the great increase in the number of patients with diabetes over the next decade will have the biggest impact on vascular services. Many of these patients present as an emergency, and are at high risk of amputation. Prompt treatment of the infected diabetic foot can minimise the risk of subsequent amputation. The BHF Health Survey for England 2006 suggests that around 1% of men aged 16 to 34 years have diagnosed diabetes compared with 13.5% of those aged 75 and over. In Lancashire diabetes is described as significantly worse than the England
average. For Cumbria the rates remain close to the England average. 2.4 Obesity and Diabetes
Lack of exercise, poor diet and increasing age are all associated with an increasing incidence of Type 2 diabetes. The epidemic of obesity is likely to have the biggest impact on the prevalence of diabetes in the next decade, and may well cause a dramatic rise. These factors all contribute to the development of hyperlipidaemia and hypertension, both potent risk factors for vascular disease. Childhood obesity has also been linked to the development of diabetes and hypertension in later life. In 1993 15% of adults were classified as obese; this rose to 24% by 2007. (HSE 2007) In Lancashire and Cumbria current levels of obesity in adults and Children are very
similar to Englands average.
9
2.5 Smoking
Smoking is a major cause of vascular disease and over 80% of vascular patients are current or ex-smokers. Although there was a rapid decline in the proportion of smokers during the 1980s, when 39% of adults smoked, this decline then levelled off in both men and women aged less than 65 years. Smokers are at greater risk of complications from vascular interventions because of cardiac and respiratory co-morbidity and the longer-term success of vascular intervention is reduced in patients who continue to smoke. (HSE 2007) In Lancashire and Cumbria current numbers of smokers is very similar to
Englands average. 2.6 Target for Reducing Mortality From Cardiovascular Disease
Over the last ten years across England there have been decreases in early death rates for heart disease and stroke.
In Lancashire early deaths from heart disease and stroke and deaths from smoking
are described as significantly worse than the England average. For Cumbria the rates remain close to the England average.
Chapter 3 Vascular Procedures 3.1 What are Vascular Services?
Vascular surgery treats diseases of the arterial, venous and lymphatic systems. Surgery for venous disease is mostly high volume, low risk, and demand driven work. In contrast, diseases of the arteries are complex, time consuming and expensive to treat. Treatment options for arterial surgery are evolving as new technologies are introduced. Vascular services encompass all of the HRG 3.5 codes as well as a range of interventional radiology procedures that do not fall naturally within current codes. Vascular services can be broadly split into three distinct categories and four levels of complexity. A full explanation of the vascular procedure level classifications can be found in Appendix 1. Vascular services include the treatment of aneurysm and other abnormal blood vessels, limb ischaemia, carotid artery disease, peripheral and visceral arterial disease, thoracic outlet surgery and venous disease. Surgery can also include vascular access work mainly used for renal patients requiring haemodialysis. Interventional radiology for vascular disease involves a range of minimally invasive image-guided techniques for stenting and repair of vessels. Interventional radiology is a developing specialism and the service offered across Lancashire and Cumbria varies greatly from hospital to hospital. Most sites offer some interventional radiology procedures, but the range of procedures offered and the degree to which interventional radiology is used at each site varies significantly.
10
3.2 Main Procedures to Consider
Treatment of Abdominal Aortic Aneurysm Repairs Open Repair The traditional operation involves cutting open the abdomen to replace the aneurysm with an artificial piece of artery (a graft). This is a major operation and carries some risk.
Endovascular Repair- EVAR This involves inserting a graft within the aneurysm through small groin incisions using X-rays to guide the graft into place. The advantage of this type of repair is that there is no abdominal surgery. This technique is therefore safer than the traditional operation and the patient spends less time in hospital.
Femoropopliteal and Femorodistal Bypass The blocked artery is exposed both above and below the blockage. Normally a vertical incision is made in the groin to expose the common femoral artery. A second incision of similar length is made to expose the artery below the blockage. A tube used to perform the bypass, the bypass tube is joined to the artery at groin level and again to the artery below.
11
Carotid Endarterectomy- CEA The carotid artery is opened up and the thickened lining and atheroma which is making the artery narrow is removed.
Amputations The vast majority of amputations are performed because the arteries of the legs have become blocked due to atherosclerosis. Most common in diabetics and smokers which causes atherosclerosis (about 30-40% of amputations are performed in patients with diabetes).
Chapter 4 Present providers 4.1 Present Provider Landscape
The Review process was facilitated by the Cardiac and Stroke Networks in Lancashire and Cumbria and began in September 2010. Progress to date includes: Appointment of Vascular Clinical Lead A Project Initiation Document was produced and agreed by the Vascular Clinical Advisory
Group The Vascular Project Steering Group was established which were both formed to inform
the review process. Both groups met on average every six weeks Full Terms of Reference for both advisory groups were developed An over-arching clinical network was agreed which will continue upon completion of the
review with one network covering all centralised sites be that one/two or three sites in total
As part of the Vascular Review, each site completed a detailed quality standards questionnaire (modelled on the Quality Standards devised by the West Midlands Vascular Review) detailing the present vascular service provided at each of these sites (Appendix 2)
Epidemiological landscape was reviewed Full travel times and population analysis was undertaken of each site presently providing
vascular services as well as other sites that presently do not (Appendix 3) Clinical pathways were reviewed by the clinical group and new pathways have been
agreed (Appendix 4) Full analysis of average Theatre Times for Vascular Procedures (Appendix 5) Full data analysis of all vascular procedures at each site (Appendix 7) Full data of services commissioned by each PCT( Appendix 8)
12
A Vascular Coding Sub-Group was formed to address issues that the review uncovered regarding the coding of vascular procedures - it is envisaged that this group will continue to meet through out the review process
A Service Specification was developed and fully ratified by the clinical group Stakeholder and GP engagement is underway Public and patient engagement is underway Local authority and relevant stakeholders have been consulted.
Vascular Surgical Services are presently provided within the Lancashire and Cumbria on five sites and formal working networks are already in place, meaning that an out of hours service is available to the full population- detailed as below. There are a total of seven sites within the review they are: Royal Preston Hospital Lancashire Teaching Hospitals NHS Foundation Trust (LTHTR) Royal Lancaster Infirmary University Hospitals of Morecambe Bay NHS Trust (UHMBT) Cumberland Infirmary North Cumbria University Hospitals NHS Trust (NCUH) Royal Blackburn Infirmary East Lancashire Hospitals NHS Trust (ELHT) Royal Bolton Hospital Royal Bolton Hospitals NHS Foundation Trust (RBHT) Blackpool Victoria Hospital Blackpool Teaching Hospitals NHS Foundation Trust (BTHT) Royal Albert Edward Infirmary Wrightington, Wigan & Leigh NHS Foundation Trust (WWLT) Within the process it became apparent that network arrangements were already in place between the Blackpool and Lancaster sites, as well as the Preston site networking with Wigan, Bolton and Southport. The Wigan and Bolton sites became part of our review process and Southport part of the Cheshire and Mersey review. There is an agreement that patients from Dumfries and Galloway will be included within this review as described below.
Present Provider Arrangements This information was formulated from the Quality Standards Questionnaire which was completed by the five sites presently providing Vascular Services Presently Royal Preston Hospital is part of the Northwest Emergency Vascular
Network which also includes Wigan, Bolton and Southport Hospitals and means in emergencies the patient would be transferred to whichever appropriate site was on call.
Arrangements at Cumberland Infirmary (CIC) - the present model to cover emergencies
in CIC includes two surgeons from Dumfries and Galloway, for this model these surgeons travel to work at CIC and all patients are brought to this one site. This Solway Basin Network was established in 1999 and was formed to provide high quality vascular services for the population of North Cumbria and parts of South West Scotland, due to the geographical location of North Cumbria and Dumfries and Galloway there are essential clinical links, providing emergency and more recently elective services to a population of circa 400,000.
It has now also been agreed that all elective aortic treatment will be undertaken at CIC.
Discussions have taken place between NHS Dumfries & Galloway (D&G) and NCUH to agree joint arrangements, including the detail of patient pathways, shared care between D&G and NCUH clinicians, funding arrangements, etc. NCUH is undertaking internal redesign of clinical services to provide the theatre and bed capacity for D&G patients, as well as patients from west Cumbria. (From April 2011 this activity will be ~ 15 cases per annum, growing to ~30 p.a. following full implementation of the AAA screening programme).
13
Blackpool Victoria Hospital has a formal partnership to cover emergencies with Royal Lancaster Infirmary. Patients presenting acutely to Blackpool are referred and transferred when there is not a Blackpool Consultant available. Over the last three years the two trusts have explored the possibilities of formalising this combined working arrangement, convened a Joint Vascular Steering Group and presented an options appraisal to the Chief Executive Officers of both trusts. An agreed clinical model has since been developed with a view to the vascular service working as one combined unit across both trust sites, covering the entire population base of 700,000.
Details on all the sites presently providing Vascular Services Below is a sample map of one of the sites included in the review Royal Blackburn Hospital (colour coded for the three travel time zones). All the site maps are shown in Appendix 3. They show the travel times for 45, 60 and 90 minutes from each site these maps with the isochrones are important as they not only show travelling distances achievable to each site but also the population residing within these zones as detailed in Section 4.3. (The maps are formed using advance travel analysis provided by Navteq 2006 and in the appendix all maps show the location and travel times to all of the Acute Trusts included in the Review).
4.2 Current Patient Flows
Detailed patient flows and cross site networking is shown in the flow charts on page 14 and 15. The numbers of beds/surgeons and major arterial procedures presently undertaken at each site is shown in the boxes below for each site within the Review.
14
Current Patient flows - (North) NCUH/UHMBT/BTHT
Data-average from last 3 yrs
(Elective AAA contract ~15 per year from 04/2011) Emergency Emergency
Rehab
CARLISLE
2 Vasc/General Surgeons 2 IR
PopulationCumbria PCT
519195
Level 3 Procedures Carotid 30 EVAR 8 AAA Repair- 31
10 Ward Beds 6 ICU 2 HDU
4 ICU 2 HDU
Whitehaven 2 Vasc/General Surgeons
Dumfries & Galloway 2 Vasc/Gen Surgeons
PCT Population 148,000
LANCASTER
3 Vasc/Gen Surgeons 2 FT Vasc Surgeons
2 IR
Population North Lancs PCT 338,854
Level 3 Procedures Carotid 55 EVAR 16 AAA Repair-33
20 Ward Beds 6 ICU 2 HDU
17 Ward Beds 8 ICU 4 HDU
BLACKPOOL
2 FT Vasc Surgeons 2 IR
Barrow
Kendal
3 ICU 3 HDU
Population Blackpool PCT 156,889
Level 3 Procedures Carotid 53 EVAR 10 AAA Repair- 8
15
Current Patient Flows - (South) LTHTR- (Wigan and Bolton)/ELHT
PRESTON
3 Vasc Surgeons 3 IR
Population Central Lancs PCT 469,219
Level 3 procedures Carotid 185 EVAR 32 AAA Repair-15
10 Ward Beds 14 ICU 10 HDU
Southport 2 Surgeons
1 IR
Chorley
4 HDU
Rehab
Wigan- 2 Surgeons / 2 IRLevel 3 procedures
Carotid- 27 EVAR- 6
AAA Repair- 12
Bolton- 2 Surgeons / 2 IR Level 3 procedures
Carotid- 24 EVAR- 6
AAA Repair- 20
Emergency Emergency Emergency
BLACKBURN
3 FT Vasc Surgeons 1 Vasc/ General Surgeon
3 IR
Population Blackburn with Darwen PCT 166,998 Level 3 procedures
Carotid- 99 EVAR- 13 AAA Repair- 27 12 Ward
Beds 14 ICU 12 HDU
Burnley
4 HDU
Population East Lancs PCT 388,769
16
4.3 Information on all Sites Currently Providing Vascular Services
The full details of services, population coverage and travel times to each site are shown in the tables below. It is important to be mindful not only of numbers of present and projected vascular throughput but also local demographics such as; age, ethnicity and the geography. Whilst many parts of Lancashire benefit from easy access to the motorway network, travel across large rural areas of Lancashire and Cumbria can cause difficulties in relation to equitable access to services.
ELHT in Blackburn Population ELHT serves population of Blackburn with Darwen PCT 166,998 and East Lancs PCT
388,769. Total 555,767 Population within the 45 minute radius - 2,664,134 Population within the 60 minute radius - 5,002,465 Population within the 90 minute radius - 8,523,792 Travel times from Royal Blackburn Hospital - within 45, 60 and 90 minutes all sites -Preston, Blackpool, Chorley, Burnley, Bolton, and Wigan can all be reached. Carlisle cannot. There is a high Asian and British Asian population in this area - (these being Blackburn (with 23% BME), Pendle (16.1%) - England average 5.7%) Numbers of Surgeons and Interventional Radiologists Surgeons- 3 FT Vasc /1 vasc /general - Total 4 Interventional Radiologist Total 3
Beds - Generic ICU beds 14/HDU beds 12/4 HDU beds - Burnley site/Ward beds - 12
Cumberland Infirmary, Carlisle NCUH, work in partnership with 2 Consultants from Dumfries and Galloway to provide on call cover for both areas. Population NCUH serves population of Cumbria PCT 519,195 and covers Dumfries and Galloway
PCT 148,000 (Solway Basin network). Total 667,195 Population within the 45 minute radius - 173,231 Population within the 60 minute radius - 224,553 Population within the 90 minute radius - 586,228 Cumbria is England's second largest county and has the third highest levels of population sparsity. Parts of West Cumbria and Barrow show a poorer than average performance across a range of health indices. The Barrow district has a life expectancy significantly lower than the national average and that of the North West.
17
Travel times from Carlisle - No other hospital is within the 45 or 60 minute radius. Lancaster can be reached within the 90 minute radius. Cumbrias geography can cause difficulties in relation to providing equitable access to services Numbers of Surgeons and Interventional Radiologists Surgeons - 4 vasc/general - Total 4 (2 Cumberland Infirmary, 2 West Cumberland
Hospital) Interventional Radiologist - Total 2 Beds - Generic ICU beds 6/HDU beds 2/Ward beds -10
BTHT in Blackpool Presently work in partnership with UHMBT to provide on call cover. Population BTHT serves population of Blackpool PCT 156889 parts of North Lancashire PCT, and
parts of Cumbria PCT (due to present arrangement with UHMBT) Population within the 45 minute radius - 919,229 Population within the 60 minute radius 2,052,006 Population within the 90 minute radius 5,872,354 Travel times from Blackpool - Within 45, 60 and 90 minutes Preston, Chorley, Blackburn, Wigan, Bolton and Lancaster can all be reached, Carlisle cannot. Numbers of Surgeons and Interventional Radiologists Surgeons- 2 FT vascular - Total 2 Interventional Radiologist - Total 2
Beds - Generic ICU beds 8/HDU beds 4/Ward beds - up to 17
UHMBT in Lancaster Population UHMBT serves population of North Lancashire PCT 338,854 as well as parts of
Blackpool PCT and parts of Cumbria PCT Population within the 45 minute radius - 731,863 Population within the 60 minute radius - 1,868,371 Population within the 90 minute radius - 5,823,080 Travel times from Lancaster - Within 45 and 60 minutes Preston, Chorley, Blackburn, Blackpool, Kendal. Carlisle can be reached within 90 mins Presently work in partnership with BTH to provide on call cover.
18
Numbers of Surgeons and Interventional Radiologists Surgeons - 2 FT vasc, 3 Vasc /gen -Total 5. Interventional Radiologist - Total 2 Beds - Generic ICU beds 6/HDU beds 2/Ward beds - up to 20
LTHTR in Preston Presently LTHTR, work as part of North West Emergency Vascular Network to provide on call cover (other sites in Network are Wigan, Bolton, and Southport). LTHTR serves population of Central Lancashire PCT (population 469,219) as well as Ashton, Wigan and Leigh PCT, Bolton PCT and Sefton PCT as part of the NW network. High Asian and British Asian population in this area -Preston (15.5%) - England average 5.7%. Population Population within the 45 minute radius - 2, 245,016 Population within the 60 minute radius - 2,257,066 Population within the 90 minute radius- data not available Travel times from Preston - Within 45, 60 and 90 minutes all other sites in Lancashire and Cumbria (including Chorley, Blackburn, Blackpool, Lancaster, Burnley, Wigan, Bolton, and Southport) can be reached, Carlisle cannot. Numbers of Surgeons and Interventional Radiologists Surgeons- 3 FT vascular surgeons. Interventional Radiologist - Total 3
Beds - Generic ICU beds 10/HDU beds 14 (Chorley Site 4 HDU/Ward beds - 10)
Cross Boundary Indications Wigan and Bolton are currently part of the North West Emergency Vascular Network and currently link in with Lancashire Teaching Hospitals they will be considered as part of this review as will Dumfries and Galloway who have a formal link with North Cumbria University Hospitals.
Wigan Population Serves the population of Ashton Wigan and Leigh PCT- 318,567 Population within the 45 minute radius - 3,771,969 Population within the 60 minute radius - 5,886,065 Population within the 90 minute radius- data not available
19
Travel times from Wigan - Within 45 and 60 minutes all other sites in Lancashire and Cumbria (Including Chorley, Blackburn, Blackpool, Lancaster, Burnley, Wigan, Bolton, and Southport) can be reached, Carlisle cannot. Numbers of Surgeons and Interventional Radiologists Surgeons- 2 Interventional Radiologist -2
Bolton Population Serves the population of Bolton PCT - 290,715 Population within the 45 minute radius 4,183,093 Population within the 60 minute radius - 6,480,060 Population within the 90 minute radius - data not available Travel times from Bolton- Within 45 and 60 minutes all other sites in Lancashire and Cumbria (including Chorley, Blackburn, Blackpool, Lancaster, Burnley, Wigan, Bolton, and Southport) can be reached, Carlisle cannot. Numbers of Surgeons and Interventional Radiologists Surgeons- 2 Interventional Radiologist -2
Dumfries and Galloway Population Serves the population of Dumfries and Galloway PCT- 148,000 but cover a population circa 400,000. Dumfries and Galloway Hospital has an agreement with NCUH to cover emergency AAA Repairs. From April 2011 this will also include elective repairs - activity will be ~15 cases per annum, growing to ~30 per annum following full implementation of the AAA screening programme. Numbers of Surgeons and Interventional Radiologists
Surgeons - 2 Interventional Radiologist - 0
20
A full travel time and population analysis was also undertaken of other sites that presently do not provide full vascular services- these sites are:
Chorley and South Ribble District Hospital based in Chorley Furness General Hospital based in Barrow in Furness West Cumberland Hospital based in Whitehaven Westmorland General Hospital based in Kendal Burnley District General Hospital based in Burnley
See Appendix 3 for the maps of these sites and 45 / 60 and 90 min travelling distances of these five sites.
Chapter 5 Length of Stay 5.1 Reducing Length of Hospital Stay by Centralisation
The most recent VASCUNET data shows the UK lagging behind its European and international counterparts. The UK has the longest length of stay in Europe for elective AAA surgery. (VASCUNET Second Annual Vascular Surgery Database Report 2008) Also, length of stay in England has been shown to be significantly longer at hospitals performing lower volumes of elective AAA repairs compared with those performing high volumes. Length of stay has also been studied in relation to the type of procedure performed. VASCUNET data demonstrated that Endovascular Aortic Repair (EVAR) required significantly shorter post-operative stays in hospital compared with open repairs. (VASCUNET Second Annual Vascular Surgery Database Report 2008)
The length of stay for patients following vascular surgery varies across Lancashire and Cumbria. It is likely that length of stay is higher than it could be due to the relatively low volume of EVAR undertaken. The length of stay in Lancashire and Cumbria could be reduced by performing vascular surgery at specialist centres that are more likely to adopt better surgical technologies, which are proven to reduce lengths of stay.
5.2 Length of Hospital Stay
It has been found that, in addition to lower mortality rates, higher-volume hospitals also have a reduced length of hospital stay. Furthermore, patients are more likely to be discharged home, as opposed to nursing care, from higher-volume hospitals and less likely to be readmitted as an emergency. It may be possible to off set costs involved in the centralisation of Vascular Services by reducing length of stay hence cost savings.
21
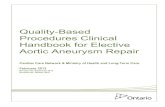
5.3 Current Average Length of Stay in the Lancashire and Cumbria Network The graph shows the average length of stay for all sites within our review for the main Vascular Procedures. Source- SUS data (outliers taken out)
(Average length of stay can be affected by available Primary care resources to discharge patients out to and a longer length of stay in no way reflects on the care provided at a
specific site).
AverageLengthofStay
0
5
10
15
20
25
30
35
40
Varico
seVe
ins
Bypa
ssRe
nal
Am
puta
tions
Varico
seVe
ins
Bypa
ssRe
nal
Am
puta
tions
Varico
seVe
ins
Bypa
ssRe
nal
Am
puta
tions
Varico
seVe
ins
Bypa
ssRe
nal
Am
puta
tions
Varico
seVe
ins
Bypa
ssRe
nal
Am
puta
tions
Varico
seVe
ins
Bypa
ssRe
nal
Am
puta
tions
Varico
seVe
ins
Bypa
ssRe
nal
Am
puta
tions
BLACKPOOL,FYLDEANDWYRE
HOSPITALS
EASTLANCASHIREHOSPITALS
LANCASHIRETEACHINGHOSPITALS
MORECAMBEBAYHOSPITALS
NORTHCUMBRIAACUTE
BOLTON WWL
TrustAverage
C&LVaricoseVeinsAverage
C&LBypassAverage
C&LRenalAverage
C&LAmputationsAverage
Procedures - Average Length of Stay for Lancashire and Cumbria AAA Repair 14 days (range 12 18 days) EVAR 7 days (range 3 10 days) Carotid 5 days (range 3 7 days) Amputations 30 days (range 21 34 days) Within our Network area Wigan and Blackpool has the lowest length of stay (consistently below the area average for Carotid, AAA and EVAR)
22
Chapter 6 Number of Specialists Required
Population Coverage Required The Population of Lancashire and Cumbria including the populations of Dumfries and Galloway, Bolton and Wigan.
Primary Care Trust Population Blackburn with Darwen 166,998 Blackpool 156,889 Central Lancashire 469,219 East Lancashire 388,769 North Lancashire 338,854 Cumbria 519,195 (Total 2,039,924) Wigan 318,567 Bolton 290,715 Dumfries and Galloway 148,000 Total population 2,797,206
Data from a survey by the VSGBI in 2009 suggested that one vascular surgeon is needed per 150,000 population, with an equivalent number of interventional radiologists. However The Vascular Clinical Advisory Group advocates 1 per 125,000 as this equates to a one in eight rota for a site covering 1 million population.
6.1 Numbers of Surgeons required for the Population
Many patients with vascular disease present as an emergency, and in the past have often been managed by a general surgeon. This is no longer acceptable. Every patient with a vascular emergency should expect to be treated by a trained vascular specialist (VSGBI 2009).
Across Lancashire and Cumbria we presently have 19 vascular surgeons, however only eight are full time vascular surgeons the rest are part Vascular and part General. These figures do not include surgeons from Wigan, Bolton or the two surgeons from Dumfries and Galloway that presently networks with NCUH to include these surgeons = 25 in total.
6.2 Numbers of Interventional Radiologists
Interventional radiology is recognised as a discipline within radiology, although not all interventional radiologists work in the vascular field. Vascular surgical specialists work closely with their radiology colleagues. Currently there are 12 interventional radiologists working within the five sites in Lancashire and Cumbria and a further three including the Wigan and Bolton sites = 16 in total.
6.3 Vascular Specialists
There is a growing consensus that the vascular specialist of the future will have operative and interventional skills, rather than being principally a surgeon. The Vascular Society has put forward proposals to address the training needs of surgeons who wish to become a vascular specialist, to ensure that this is accommodated within MMC (Modernising Medical Careers) arrangements. In March 2007, the Royal College of Radiologists and the Royal Colleges of Surgeons of England, Edinburgh and Glasgow produced a joint statement aimed at addressing the needs for provision of interventional radiology and vascular surgery and benefiting the development of both specialties.
23
The paper describes the concept of a vascular specialist as an umbrella term, encompassing a variety of clinicians with a shared set of core experience related to vascular disease based on demonstrating competence in the relevant knowledge, skills and professional attitudes.
With both vascular surgeons and interventional radiologists trained in interventional radiology techniques, fewer patients would require open surgery for vascular disease, thus freeing up theatre capacity and reducing patient length of stays.
6.4 Vascular Nurse Specialists
The Vascular Nurse Specialists contribute to both inpatient and outpatient care. They have a key role to play in liaising between team members. The Vascular Nurse Specialist usually provides independent care and advice using agreed protocols. Nurse specialists may provide independent care to patients through lifestyle advice clinics, claudication clinics, leg ulcer clinics and diabetic foot clinics. They play an important role in vascular research and audit and are involved in the training and education of both community and hospital nursing staff. Each of the five sites within Lancashire and Cumbria presently employ one or more
Vascular Nurse Specialist.
Chapter 7 Links with Other Specialties 7.1 Critical Links Specialties Supporting a Vascular Service
In order to provide Lancashire and Cumbria residents with a world-class service, patients undergoing specialist vascular surgery should also have access to interventional cardiology, interventional radiology, a specialist intensive care unit, specialist vascular anaesthetists, diabetic and neurology specialists, cardiac surgery and a step down intensive care facility. It is also desirable that patients have access to a renal unit that includes dialysis facilities. Currently in Lancashire and Cumbria, the services supporting vascular surgery vary from hospital to hospital. Arterial surgery is major surgery that requires the very best services available onsite to support it. It is important, to consider other services within the review as it is members of the vascular MDT who carry out this work.
7.2 The Impact on Major Trauma and Stroke
Vascular Surgery cannot be seen in isolation, it has close links with major trauma and stroke services.
Trauma There is presently a review of Trauma Services taking place in Lancashire and Cumbria.
The location of major trauma centres in Cumbria and Lancashire should be a key factor in the decision-making process regarding vascular service delivery. In the future it is likely that patients with a major injury will be taken by ambulance to the nearest trauma centre for specialist treatment, in many of these instances, patients will need access to a specialist emergency vascular service.
Stroke Acute stroke services are provided in stroke units which are based at all sites. Clear pathways will need to be established so that patients can have timely access to Carotid Endarterectomy (CEA) surgery which would only be available at the intervention centres.
24
The future provision of vascular services in Cumbria and Lancashire needs to ensure that patients who have a major injury or a stroke receive the quality of care they need. It is likely that in order to achieve this, the format of where and how vascular services are provided will need to consider the changes to major trauma and stroke services in Cumbria and Lancashire.
7.3 Other Service Considerations
It is important to consider other services within the review as it is members of the vascular MDT who carry out this work, i.e. vascular surgeons and vascular interventional radiologists. Vascular cover is needed 24/7 for patients undergoing surgery for stroke/patients undergoing limb salvage surgery for diabetes/renal inpatient units/vascular access.
Renal Access The best form of access for chronic haemodialysis is an autogenous arteriovenous fistula. This is usually performed by vascular surgeons. The majority of this work is planned, but there are also urgent cases where patients are failing dialysis access. Most of these can be treated within a few days, by either surgical or interventional radiology techniques. It has been estimated that one dedicated vascular access operating list is necessary for each 120 patients on dialysis (including peritoneal dialysis) assuming 3 - 4 patients can be operated upon per list. Most patients can be operated on under local anaesthesia and many of the operations can be performed as a day case procedure. In March 2010 the total number of patients across Cumbria and Lancashire on dialysis treatment was 681 - this does not include Wigan and Bolton patients. In addition there is a need for up to two interventional radiology sessions per week per 100 patients on dialysis for preoperative imaging, postoperative surveillance and for percutaneous angioplasty or thrombectomy of failing or thrombosed AV fistulae and grafts. The VSGBI 2009 expects 281 procedures per million population - this equates to 756 vascular access procedures per year for our population.
Diabetes Diabetic patients have a high risk of peripheral arterial disease. Some patients can be managed in primary care; a minority require interventional treatment, either with interventional radiology or surgery. For some patients, disease may progress to critical limb ischaemia, which can lead to amputation. Early intervention and opinion of vascular surgeons can significantly reduce the number of amputations carried out. Patients with diabetes should have local access to a specialised foot clinic, with input from vascular surgeons.
7.4 Amputations - Amputee Rehabilitation in a Centralised Unit Leg amputation is currently defined as amputation above, below and through the knee. A recent aim of the Vascular Societys Quality Improvement Framework is to raise the profile of leg amputation, with the target of reducing peri-operative mortality below 5%. As with other vascular procedures evidence shows better outcomes and reduced length of stay from centres that perform a higher number of procedures.
25
A centralised unit for vascular services and thus amputation surgery would provide a significant opportunity for the post operative and early rehabilitation of amputees to be combined into a central location, concentrating skill levels and patient numbers; economies of scale. Currently no unit has enough amputees to warrant a ward or partly dedicated for amputee rehabilitation where intense rehabilitation is engaged by patients with an amputee rehabilitation team. The amputee rehabilitation team would be engaged with the patient as soon as amputation surgery has been proposed or as soon after emergency surgery as is practically possible, i.e. the same working day or the next working day. The amputee would come under shared care between the treating vascular surgeon and the rehabilitation physician. Appendix 6.
Chapter 8 Workload Requirements 8.1 Activity and Length of Stay Assessment
The Chart below shows the main Vascular and Arterial Procedures yearly averages across all sites including length of stay. This data has been taken from Hospital Episode Statistics (HES) and looks at the last three financial years (07/08, 08/09 and 09/10). Our extracted data is from Q HRGs (HRG version 3.5).
Procedure Average Total Yearly Activity
Average Length of Stay in L&C
Bed Days
Open AAA 140 14 1960 EVAR 85 7 595 Carotid 472 5 2360 Renal artery 30 5 150 Amputations 320 30 9600 Peripheral Bypass 1913 6 11478 Total / 365 72 Beds
**Please note: The above table shows only the main vascular procedures and is by no means an exhaustive list - it is only intended as a guide and only shows the very minimum requirement that would be needed. The VSGBI (2009) note that based on current experience and depending on local case-mix, a population of 500,000 will require 20 - 25 beds on a dedicated vascular ward, excluding rehabilitation, short stay, day case and ITU/HDU beds. Using this equation the population of Lancashire and Cumbria would require
between 100 - 125 vascular in patient beds. This equates to about 3 - 5 vascular wards.
Our present capacity is only for 69 vascular ward beds. (The beds at Bolton and
Wigan sites are general with none specifically designated for vascular so are not included within this 69).
For ITU and HDU patients, the VSGBI 2009 recommends one vascular ITU and one HDU
bed per 500,000 population. For our region that equates to 5 - 6 dedicated vascular HDU
26
and 5 - 6 dedicated vascular ITU beds across Lancashire and Cumbria. Presently across our region, there are not any HDU/ICU beds dedicated to vascular patients.
It is important to be aware of any other specialties based at each site may also require
critical care beds and this needs to be considered when deciding the placement of the Intervention Centres.
8.2 Day Case and GP Referral
It is the view of the Vascular Clinical Advisory Group that all Day Cases continue in the DGH as is the present arrangement and only procedures that require an inpatient stay should be referred to the intervention centre.
GP Referral GPs would continue to refer all vascular patients to their local hospital in the same way as they do now. Patients whose local hospital is also a central unit would continue to be referred to that hospital by their GP. The hospital would continue to act as their local hospital, meaning certain patients with venous, lymphatic and arterial disease would be referred directly to the central unit for treatment. Patients presenting at any other local hospital who need an elective arterial procedure would have most of their pre-surgery investigation at that local hospital before being transferred to a central unit for treatment. All patients would receive the same high quality standards of service regardless of whether they are transferred from a local hospital to the nearest central unit, or referred directly to the central unit by their GP.
8.3 Procedure Volume Requirements
It is well established that a strong relationship exists between higher annual volume of procedures and lower mortality for elective and emergency endovascular aneurysm repair, mirroring similar robust relationships between volume and outcome in open AAA repair. In conjunction with the development of aneurysm screening programmes these highlight the need for regionalisation of AAA service provision to high-volume centres offering a full range of vascular services including advanced endovascular intervention. The same evidence supports centralisation for Carotid Endarterectomy and amputation. (VSGBI 2009)
Minimum Recommended Number of Procedures per site Figures below from other Vascular Service Reviews
Annual volume Source AAA CE
Yorkshire &Humber 32 35 Literature review West Midlands >20 >30 Vascular Society guidance London >100 >50 Literature review NW EVAR guidance Minimum of
20-30 EVAR equates to 40-60 AAA
total procedures
Not covered in this
document
Holt et al 2009
Leapfrog group >50 >100 Literature review
27
8.4 Current Activity across the Network
Abdominal Aortic Aneurysm Repair The total numbers of all emergency and elective Abdominal Aortic Aneurysm repairs the past three years averages at 225 procedures per annum for the whole of Review area including Wigan and Bolton. (Please note the numbers of repairs is expected to increase when AAA screening is introduced) Of the total number of 225, 140 are open AAA repairs (101 open elective and 39 open non elective). Modelling of AAA services has highlighted the significant reduction in mortality that could be achieved in England through regionalisation of these procedures to high-volume centres. Minimum volume criteria of 50 elective AAA cases per annum should be set to ensure safe practice. (Holt PJ, Poloniecki JD, Gerrard D et al). Meta-analysis and systematic review of the relationship between volume and outcome in abdominal aortic aneurysm surgery. Br J Surg 2007; 94: 395-403).
EVAR The total numbers of all emergency and elective EVAR procedures for the past three years averages at 85 procedures per annum for the whole of Review area including Wigan and Bolton.
A strong relationship has been shown in favour of hospitals that perform EVAR at high annual volumes. Despite the evidence showing EVAR has lower mortality rates and significantly shorter hospitals stays compared with traditional open surgery. Presently in our area only 85 of aneurysm repairs per year are currently by EVAR (79 elective, 6 non elective). This represents only 38% of the total numbers of repairs completed by Endovascular repair. An EVAR unit should expect to serve a population that will generate a minimum of 20-30 EVAR procedures annually. It is generally accepted that between 50% and 80% of all AAA procedures should be EVAR. (Holt, P E., Poloniecki, J. D., Khalid, U., Hinchcliffe, R. J., Loftus, I. M. & Thompson, M. M. (2009). Effect of endovascular aneurysm repair on the volume outcome relationship in aneurysm repair. Circulation, published online Sept 2009-10-26)
Carotid Endarterectomy- (CEA) The total number of all emergency and elective Carotid procedures for the past three years averages at 472 procedures per annum for the whole of Review area including Wigan and Bolton. Minimum Numbers of Procedures recommended per site is 35 per year. Statistical modelling of the volume-outcome effect for carotid endarterectomy for 10 years of a statewide database. Griswold, M.E., Chang, D.C., Perler, A.P. 59:12, 2002. The Vascular Clinical Advisory Group has agreed a minimum of 35 per site Presently there are 472 Carotid Procedures on average per year within the review area. (385 elective, 87 non elective).
28
8.5 Figures Based on Minimum Population
The minimum population for an independent vascular unit is 800,000. Each emergency vascular service should employ a minimum of 1 WTE vascular surgical specialist per 150,000 population and should serve a minimum population of 800,000 as a whole. (VSGBI 2009) (Although the Vascular Clinical Advisory Group informing the review is recommending 1 per 125,000) There is no data recommending the maximum patient coverage. Including the populations of Wigan and Bolton takes the population to 2,797,206 which
would require a minimum of 19 vascular surgeons and 19 interventional radiologists. However, to cover on call rotas, the review recommends 22 of each (as described in Chapter 9)
To include the vascular surgeons and interventional radiologists currently available within
all these sites would give us a present total of 25 surgeons and 16 interventional radiologists
This again highlights a shortfall of interventional radiologists
8.6 Required Theatre Capacity - Appendix 4
Average Theatre Times for Main Vascular and Arterial Procedures (including anaesthetic time). Please note: The table shows only the main vascular procedures and is by no means an exhaustive list- it is only intended as a guide and only shows the very minimum requirement that would be needed.
Chapter 9 Proposed Models 9.1 Recommendations of the Review
Patient Pathways Reconfiguration of vascular services required a review of current referral pathways and patterns, to ensure the provision of comprehensive vascular care to the local population. A full pathway review has been completed as part of this review process. See Appendix 3 This shows the current pathway and then the new pathway agreed by the Clinical Advisory Group, all the pathways looked at primary prevention through to after care and end of life if appropriate. Pathways included for: Emergency AAA Elective AAA Carotid Stenosis Ischaemic legs Varicose Veins Leg ulcers Vascular Access
Please note that the pathway for Vascular Access remains under review and will hopefully be complete by the end of this Vascular Reconfiguration process.
29
9.2 Proposals and Network Formation
Proposed structure of the vascular clinical model The Vascular Clinical Advisory Group membership included a range of clinicians from across all the sites involved in the review. Its aim was to offer best clinical advice on the provision of safe, high quality evidence based services for vascular patients to the Lancashire and Cumbria Vascular Services Review. A number of factors were considered to determine the optimal number of central units to provide a high quality, safe and equitable service. Factors considered were: Minimal numbers of procedures needed at each site, and current and future volume
projections of arterial procedures Number of surgeons Co-dependencies Geography of Lancashire and especially Cumbria The ability to maintain surgical rotas in line with all VSGBI 2009 recommendations.
Proposed structure
The central Unit would deal with all vascular inpatient activity and all other vascular procedures and Day Case would continue in the DGHs.
30
9.3 Proposals Made by the Vascular Clinical Advisory Group
Numbers of procedures per site Below is the agreed Minimum number procedures per site (these are the Minimum Recommendations numbers set out by the VSGBI 2009 and agreed by the Vascular Clinical Advisory Group) to maintain highest quality standards and patient outcomes Minimum Numbers agreed for Lancashire and Cumbria Minimum of AAA Procedures - minimum 50 per site Minimum number of EVAR Procedures - minimum 20 - 30 per site Minimum number of Carotid Procedures -minimum 35 per site VSGBI 2009, highlights that on average eight AAA procedures are generated per year per 100,000 population and an average of 8.2 Carotid procedures per year per 100,000 population. (Our data averages at 8.3 AAA procedures and 17 Carotid procedures per 100,000)* *Total Population Coverage - 2,797206 (including the population of Bolton and Wigan PCTs).
9.4 Formation of Vascular Network
The proposed model will operate as an effective cohesive system, comprising of centralised vascular units across Lancashire and Cumbria, so that the workload, access to beds and training etc can be shared. Each unit should work in partnership to provide a comprehensive vascular service for a defined local population. The central vascular units would be the source of excellence for intervention ensuring that standards of clinical and non-clinical governance are robust and ensure vascular services would be delivered consistently across the network.
31
Proposed Model Options One and Two
OPTION ONE is for two centres in total This option means ONE Intervention Centre in the North and ONE in the South of the Network area Figures for ONE proposed northern centre Minimum Number of Procedures It is envisaged that the intervention centre in the North of the network will cover a population of 700,000 using our current figures from the network area covering a population of 700,000 would generate on average 58 AAA repairs per year and 122 Carotid procedures per year. This is higher than the minimum procedure requirements and would make this a viable option. **Theatre Requirements (This needs further investigation- see appendix 5 shows average theatre times from ELHT and UHMBT). It is estimated that 2 - 3 vascular theatres would be required for this option. Emergency access needs to be considered. Numbers of Beds Needed According to VSGBI (2009) standards, to cover the population of 700,000 would require 25 -30 designated ward beds and 1 - 2 ICU and 1 -2 HDU beds. (The number of required ICU/HDU beds may reduce once the NAASP is underway and the number of ruptured aneurysms reduces). The Carlisle site presently has (up to) 10 designated vascular beds and no designated Critical Care beds. A further 15 - 20 ward beds and 2 - 4 critical care beds would be required. Numbers of Surgeons and Interventional Radiologists needed The VSGBI (2009) recommend one surgeon and one interventional radiologist per 150,000 population but also notes that Vascular on call rotas should be no more onerous than 1 in 6, therefore this site would need a minimum of six surgeons and six Interventional Radiologists.
32
Figures for ONE Intervention Centre in the South of the Network area Minimum Number of Procedures Having only one Intervention Centre in the South of the Network would cover a population of just over two million. Using our current figures from the network an intervention centre covering a population of two million would generate on average 166 AAA repairs per year and 349 Carotid procedures per year. **Theatre Requirements (This needs further investigation- see Appendix 5 shows average theatre times from ELHT and UHMBT). It is estimated 4 - 6 vascular theatres would be required at each site for this option. Emergency access needs to be considered. Numbers of Beds needed at each site According to VSGBI (2009) standards, to cover the population of 2 million would require 80 -100 designated ward beds and 4 ICU and 4HDU beds. (The number of required ICU/HDU beds may reduce once the NAAASP is underway and the number of ruptured aneurysms reduces). Numbers of Surgeons and Interventional Radiologists needed The VSGBI (2009) recognises that centres dealing with populations in excess of 1 million people will have to deal with higher volumes of emergency cases and in such cases the emergency rota should be no more onerous than 1 in 8. The VSGBI 2009 recommends there should be one interventional radiologist and one vascular surgeon per 150,000 - however the Vascular Clinical Advisory Group has agreed one per 125,000, this is in line with concurrent reviews, so for a population of two million this equates to 14 - 16 of each needed to cover this population number. The whole network area presently has 25 vascular surgeons in total and 12 interventional radiologists in total. A minimum of six of surgeons and six interventional radiologists would be required in the centre in the North of the network leaving a shortfall of 8 - 10 IRs (for the two site option). There is a National shortage of trained interventional radiologists and, whilst work is underway to develop interventional radiology as a recognized sub-specialty, it is likely to take some years before this position changes. An obvious solution is training vascular surgeons to become vascular specialists encompassing IR skills.
33
Views of Vascular Clinical Advisory Group for Lancashire and Cumbria. Assessment of the two site model was not seen as a viable option by Vascular Clinical Advisory Group, (Feb 2011) the advisory group dismissed the two site option and recommended the proposal of the 3 site option as set out below. The recommendation was that one site will be in the North of the region due to geography and travelling distances and two sites will be based in the South of the network area. It was felt two sites were needed in the South of the network as the population coverage would be over two million. OPTION TWO is for three centres in total This option is for ONE Intervention Centre in the North of the Network area and TWO Intervention Centres in the South of the Network area Figures for one proposed Northern Centre (All figures for a Northern centre remain unchanged from option one - see above - they remain unchanged due to the geography and travelling times) Figures for the TWO proposed sites in the South Minimum Number of Procedures The two intervention centres in the South of the network if equally split would cover a population of just over one million each. Using our current figures from the network area each intervention centre covering a population of one million would generate on average 83 AAA repairs per year and 174 Carotid procedures per year. This is higher than the minimum procedure requirements and would make this a viable option. Numbers of Beds needed at each site According to VSGBI (2009) standards, to cover the population of one million would require 40 - 50 designated ward beds and two ICU and two HDU beds. (The number of required ICU/HDU beds may reduce once the NAASP is underway and the number of ruptured aneurysms reduces). **Theatre Requirements (This needs further investigation- see appendix 5 shows average theatre times from ELHT and UHMBT). It is estimated four vascular theatres would be required at each site for this option. Emergency access needs to be considered. Numbers of Surgeons and Interventional Radiologists needed The VSGBI (2009) recognises that centres dealing with populations in excess of one million
34
people will have to deal with higher volumes of emergency cases and in such cases the emergency rota should be no more onerous than 1 in 8 therefore each Southern site would need a minimum of eight surgeons and eight interventional radiologists. This three centred approach requires a total of 22 surgeons and 22 radiologists. As highlighted in Figure 8.5, the whole network population as it stands would require 19 vascular surgeons and 19 interventional radiologists, however to cover three on call rotas of (1) 1 in 6 and (2) 1 in 8, requires a total of 22 surgeons and 22 interventional radiologists this would mean a shortfall of six interventional radiologists across the network area. Presently there are 25 surgeons and only 16 interventional radiologists; it may be that some of the vascular surgeons could develop their skills to become vascular specialists as described on page 18. This three site plan and network formation is a viable option and will provide an enhanced joined up approach to vascular services and improved diagnostics, in line with Vascular Society recommendations and will also build on the present good clinical network arrangements in place across the network area.
**Theatre Requirements. It is hard to determine what the theatre requirements will be and this needs further investigation, the figures given in the tables in Appendix 5 were based on average theatre times for the main procedures which were received from ELHT and UHMBT See Appendix 5 Current times are not particularly good for vascular surgery, with finishes typically scheduled around 4:30 to 5:00pm. Extending this to 6:00pm the so-called three session day may be better. Staggering the start times of theatres also may be more efficient and avoid delays, as would greater use of weekends for elective work. While outside the influence of vascular surgeons alone, the establishment of league tables for late starts among surgeons in a unit have been found to improve their keeping to time. Vascular surgeons should support such local measures. Ref- Clinical Response to the downturn NHS Confederation 2010, pg 16 9.6 Workforce Planning
There are a number of key considerations in terms of future workforce and recruitment that will impact on vascular services and should be taken into consideration in recommending future models of service provision. These are:
Vascular surgery is moving towards single specialty status. This will result in fewer junior doctor posts. Whilst services are primarily consultant-led and a reduction in junior doctor posts could be counterbalanced through the appointment of non-training grades, it is likely to impact on the ability of all existing services to maintain current levels of medical cover.
European Working Time Directive (EWTD) is enshrined in UK law. For Junior Doctors, a
EWTD compliant rota requires a minimum of 6 junior doctors, even when on-call is not on site. This would require significant additional workforce capacity to deliver the service. This is an important consideration when looking at the sustainability of services with fewer consultants than this.
There is a shortage of trained interventional radiologists and, whilst work is underway to
develop interventional radiology as a recognised sub-specialty, it is likely to take some years before this position changes.
Whilst there are no firm plans in place or agreed implementation dates, the intention is that
in future vascular consultants will be vascular specialists, with skills in both surgery and vascular interventional radiology- This presents a potential solution - certainly in the interim and perhaps in the longer term and could have a significant impact on the
35
workforce within vascular centres, although these changes will take some years to materialize.
9.7 Patient and Public Engagement
Patient and public consultation work is ongoing - a core script and press release have been formulated, public questionnaires have been completed and a public consultation document is presently being formulated. This work is being led by East Lancashire PCT Communication and Engagement team. This process is an extremely important part of the Vascular Review process and individual documents have been produced which can be seen upon request. Equality Impact Assessments have been completed and the review team have attended Overview and Scrutiny meetings. This work is ongoing.
Chapter 10 Costs of Vascular Services The following recommendations were produced by the Vascular Society to highlight where resources could be released in NHS vascular services, while maintaining or enhancing quality Many unnecessary costs in vascular surgery derive from extended lengths of stay. Reducing these represents a clear area where cost efficiency and quality can be improved simultaneously. Remodelling vascular services by reducing the number of providers would reduce mortality and morbidity after major vascular surgery by concentrating medical and nursing expertise, increasing unit volumes and driving greater systematisation. The costs involved in the centralisation of services would be offset through improved outcomes by reducing the cost of post-operative morbidity and hence length of stay. A first phase of remodelling has already resulted in the number of vascular units in England being more than halved to just over 100. Vascular services are fully tariff based (with the exception of some interventional radiology procedures which the Clinical Advisory Group has recommended are addressed as part of this review). With the assumption that the recommendations will change the distribution of current services but not increase or decrease overall volumes, the net cost of the options to PCTs would be zero. It would seem reasonable to expect the centralised units to meet the proposed standards from within existing tariff income, as this has been shown to be possible. 10.1 Tariff and Numbers of Vascular Procedures Commissioned
As part of the review we engaged with all PCTs that commission vascular services within the review area. The information that each PCT provided can be found in Appendix 8. At first glance, the figures provided differ greatly from the vascular data that we gained from SUS*, however the data provided by the PCTs covers spells rather than actual procedures and includes excess bed days. The list provided by the PCTs shows that the total costs for vascular procedures are 26,585,958. The data clearly needs further investigation and the review recommends that this is addressed when centralising - a coding sub-group, led by consultant Vascular Surgeon, Mark Tomlinson, from UHMBT has already been established within the review process, it is envisaged that this work will continue as part of the network, which is discussed on page 37. *SUS data is shown in Appendix 7.
36
Stakeholder Engagement We are set to engage with a wide range of stakeholders and have maintained a transparent approach throughout the review, sharing all key documents on a regular basis.
10.2 Procurement
There is scope for increasing economies of scale in procurement through joint working between vascular surgery and other specialties, particularly as provision becomes more concentrated. Shared procurement with cardio-thoracic surgery in particular should be explored by surgeons locally, particularly around hybrid theatres, high-end imaging and anaesthesia, as well as nursing and critical care. The over-regulation of basic devices results in very high costs for relatively simple devices such as endovascular stent grafts for aortic aneurysm repair. There is possibly some scope for vascular surgeons to agree to further limit the number of these devices available (although the range is already fairly small) or for manufacturers to agree to a set procedure price in order to continue supplying to the NHS. Ref- Clinical Response to the downturn NHS Confederation 2010. pg 16
Centralisation is associated with fewer complications and reduced length of stay which are both associated with reduced costs.
10.3 Increased Use of EVAR and Cost Implications
The Payment by Result (PbR) spell price for endovascular aneurysm repair is similar as for open aneurysm repair. However endovascular aneurysm repair requires less critical care compared with open surgery but incurs costs for non-tariff devices (stents). The cost of the stent needed for endovascular aneurysm repair surgery is estimated at 6k per stent device*. Critical care costs are negotiated separately by each provider but are estimated at 1,500 per day*. *(The financial review of the implications of a Cardiovascular Review commissioned by London 2010)
It is estimated that high volume units with a dedicated high dependency unit (circa 600 per day) will use one day in an intensive treatment unit and two days in the high dependency unit for open surgery, and lower volume units without the high dependency unit facility will use three days in an intensive treatment unit. In comparison, endovascular aneurysm repair requires one day in a high dependency unit before transfer to the ward. EVAR is associated with reduced length of stay and therefore lower costs overall.
10.4 Reduced Aortic Aneurysm Repair Length of Stay Due to Increased Uptake of
Endovascular Aneurysm Repairs
Endovascular aneurysm repair is associated with a lower length of stay compared with open repair techniques. Patients receiving abdominal aortic aneurysm repair surgery using endovascular surgery have a lower length of stay compared to those receiving open surgery. The average length of stay within Lancashire and Cumbria for both types of technique: EVAR = 7 days Open AAA = 14 days Difference = 7 days
37
10.5 Financial Implications for Providers
There is a seven day length of stay difference for each procedure. The number of bed days saved across Lancashire and Cumbria in reduced length of stay could be significant - presently only 35% of AAA repairs are done by EVAR with a LOS at seven days as opposed to 14 days for open repairs. Increasing the numbers of EVAR procedures from 35% which it presently is in Lancashire and Cumbria to between 50% - 80% the figure proposed by the VSGBI will mean cost savings as length of stay could be halved. If the percentage of EVAR was to increase in line with VSGBI and local targets to 50 - 80% 896 to 1435 bed days could be saved. Increasing to 50% EVAR could save 896 bed days; Increasing to 80% of all AAA repairs could save 1,435 bed days.
10.6 Reduced Length of Stay Following Carotid Endarterectomy Surgery
The average length of stay in Lancashire and Cumbria for carotid endarterectomy ranges from three to seven days with an average of five days. Average lengths of stay for carotid endarterectomy in Lancashire and Cumbria compare unfavourably to figures from Europe. Centralising services will enable providers to reduce this gap. Centralisation of vascular services has been shown to drive down length of stay for lower extremity by pass and amputations, which will also produce cost savings.
10.7 Productive Bed Use
The use of same-day admission reduces length of stay and can provide savings in the numbers of beds needed to run a service. Protected beds - another model that has potential to be spread more widely is the establishment of protected beds to drive higher throughput for certain conditions. Protected beds for angioplasty have, where used, resulted in surgeons completing a greater number of cases per day. Beds outside of the acute unit for rehabilitation and low intensity care would also help the appropriate level of care to be delivered cost-effectively. Ref- Clinical Response to the downturn NHS Confederation 2010, pg 15.
10.8 Ambulance Costs
Centralisation will require close liaison with the North West Ambulance Service (NWAS). However, until it is determined where the intervention centres will be placed it is not possible to know the impact and costs that will be involved in patient transportation. The outcomes of the subsequent Trauma Review will also need to be configured into any service agreements regarding the Ambulance requirements.
38
Consideration also needs to be given to The Joint Royal Colleges Ambulance Committee (JRCALC) guidelines which include the possible diagnosis of AAA and ischaemic legs as an area where consideration could be given for paramedics to directly refer the patient to specialist vascular services. This is an important potential development, which could further support the centralisation option. It is recommended that this is clarified in part two of the review.
Chapter 11 Implementation Plans 11.1 Implementation Timetable
A key issue now is how to move towards an implementation plan if the Clinical Advisory groups recommendations are accepted. The kinds of vascular services under discussion are unlikely to attract the attention of the independent sector as the need for ICU and specialist beds may present a barrier. If the approach adopted is one of co-operation, there are several alternatives: 1. A tendering approach is adopted with providers within a defined area being asked to put
forward a business case based on the service specification 2. The providers are simply asked to go away and discuss amongst themselves where the
centres will be and to put a business case based on the service specification back to commissioners.
3. Commissioners try and broker discussions between the sites to ensure that any decision
takes into account issues of choice, accessibility and safety. In order to implement these recommended improvements to vascular services, it is recognised that some hospitals may not have capacity to accommodate all arterial surgery immediately. To overcome this issue, there should be a transition plan enabling designated central vascular units to initially perform abdominal aortic aneurysm repairs and carotid endarterectomise with lower extremity arterial bypass surgery being moved later to the central units over a planned, organised period of time.
Chapter 12 - Recommendation Checklist for Vascular Reviews
Comments below taken from the North West Specialised Commissioning Team
Recommendation for North West Reviews
Local barriers to change should be identified at the earliest opportunity and steps taken to address these. (The review has engaged with stakeholders from primary and secondary care patients, public and staff throughout the review process)
Implementation planning should form an integral part of the review process. There should be named leads for this process and explicit timelines. (This has been identified and will be implemented once the model has been agreed)
Successful remodelling is more likely if early agreement between provider Trusts can be secured. (This work is ongoing)
39
Commissioners should look to remodel vascular services into a networked arrangement whereby all elective and emergency arterial surgery is located in a single unit. (Centralisation of services with an umbrella network is the aim of the review)
The other components of vascular care should remain within DGHs to enable residents to benefit from fast access to specialised care but retain local availability of less specialised procedures and access to vascular opinion. (Within this model GP referral and outpatients would continue to be at the local DGHs.
Central to this is the concept that the clinicians involved in the service operate as a single clinical team, working within MDT arrangements, with all members delivering care in both the central arterial intervention centre and in the DGHs. All should contribute to the delivery of a 24hr service through sustainable rotas. (This has been agreed and will be implemented once the model has been agreed)
The detail of the service arrangement should be considered by the clinical advisory groups.(The Vascular Clinical Advisory Group has developed a model and service specification)
The transfer of aortic surgery and carotid endarterectomy should take place at the earliest possible opportunity.- (This review recommends a staged approach to centralisation)
40
Appendix 1 Vascular Procedures are categorised into four levels: Level 1 Describes work that falls into vascular HRG codes but is non-specialised in nature and can be legitimately done in a hospital without a vascular inpatient unit, provided there are formal links with a vascular unit for advice. Level 2 Level 2 makes up the vast majority of vascular services. All other arterial and venous surgery, requiring input from a vascular surgeon or interventional radiologist and all miscellaneous procedures not included within Level 1, above. This includes lower and upper limb arterial surgery, venous surgery and amputations. Hospitals treating these patients musts have 24/7 consultant surgical cover and should have 24/7consultant interventional radiology cover, particularly if dealing with emergency admissions. There are potentially however, significant workforce issues in delivering 24/7 IR for this group
of patients. This is a critical factor to consider when reviewing service configuration options.
Level 3 AAA & CEA surgery and IR Whilst the surgical and IR skills needed for AAA and CEA are the same as those needed for other arterial work and cannot therefore be viewed in isolation, these procedures are low volume and there is clear evidence linking volume and outcome. Hospitals treating these procedures must have 24/7 consultant surgical and interventional radiology cover in order to deal with emergency admissions and complications of treatment. Level 4 Very complex, rare or requiring other highly specialist input, such as cardio thoracic surgeons. Including: Treatment of aortic arch and thoracoabdominal aneurysms Treatment of aortic dissections Thoracic aortic stent grafts Open or endovascular surgery for thoracic and thoracoabdominal aortic aneurysms Surgery for carotid body tumours Treatment of infected aortic grafts Treatment of mid-aortic syndrome Complex revision of arterial surgery Treatment of vascular malformations Deep vein reconstruction Treatment of difficult aneurysms by fenestrated and branched aortic stenting Laparoscopic aortic surgery
41
Appendix 2 Quality Standards
QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH
Who is the nominated lead consultant vascular specialist?
Mr Haytham Al-khaffaf MR. THEO OJIMBA Mr G. Thomson Consultant Vascular Surgeon
Mr MARK TOMLINSON
Mr Vittorio Perricone
Is there a consultant vascular surgeon available at all times?
Yes-There are four vascular surgeons who share 1 in 4 rota YES.August2010Rotaattached
At Lancashire Teaching Hospitals NHS Foundation Trust (LTH) there is a Consultant Vascular Surgeon available during normal working hours at all times. LTH participates in the NHS North West Emergency Vascular Network to ensure availability out of normal working hours.
Yes- Also cover BLACKPOOL VICTORIA HOSPITAL on a 1 in 2 basis out of hours
Yes. We do work in collaboration with Royal Lancaster in order to provide continuous care for the vascular patients. More specifically, outside working hours, the vascular surgeons on call at Royal Lancaster cover also for vascular emergency at Blackpool every Monday and Wednesday and on alternate weekends.
42
QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH
How many vascular surgeons are there in your team?
FOUR
There are a total of 6 vascular surgeons within the service, 4 at North Cumbria University Hospitals NHS Trust + 2 in Dumfries & Galloway Hospita