Improving Quality: Anticoagulation Therapy · DVT/PE - Prophylaxis – ACCP 9th guidelines changes:...
49
1 Improving Quality: Improving Quality: Anticoagulation Therapy Anticoagulation Therapy Improving Quality: Improving Quality: Anticoagulation Therapy Anticoagulation Therapy Mark Wurster, MD Founder and Chief Medical Officer Standing Stone, Inc. Scope of the Problem Scope of the Problem • Adverse Drug Events (ADEs) 15 illi t bl ADE i – 1.5 million preventable ADEs in United States annually – Anticoagulants account for 4% of preventable ADEs and 10% of potential ADEs potential ADEs. Committee on Identifying and Preventing Medication Errors. Aspden P, Wolcott J, Bootman JL, Cronenwett LR, Editors. Preventing Medication Errors: Quality Chasm Series. Washington, DC: National Academies Press; July 2006. Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events: Implications for prevention. ADE Prevention Study Group. JAMA. 1995;274:29-34.
Transcript of Improving Quality: Anticoagulation Therapy · DVT/PE - Prophylaxis – ACCP 9th guidelines changes:...

1
Improving Quality: Improving Quality: Anticoagulation TherapyAnticoagulation Therapy
Improving Quality: Improving Quality: Anticoagulation TherapyAnticoagulation Therapy
Mark Wurster, MDFounder and Chief Medical Officer
Standing Stone, Inc.
Scope of the ProblemScope of the Problem• Adverse Drug Events (ADEs)
1 5 illi t bl ADE i– 1.5 million preventable ADEs in United States annually
– Anticoagulants account for 4% of preventable ADEs and 10% of potential ADEspotential ADEs.
Committee on Identifying and Preventing Medication Errors. Aspden P, Wolcott J, Bootman JL, Cronenwett LR, Editors. Preventing Medication Errors: Quality Chasm Series. Washington, DC: National Academies Press; July 2006.
Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events: Implications for prevention. ADE Prevention Study Group. JAMA. 1995;274:29-34.

2
Scope of the ProblemScope of the Problem
• Adverse Drug Events (ADEs)
– Heparin and warfarin constitute 2 of the top 3 medications requiring ER visits due to complications
– Anticoagulants are frequently it d i di l l ticited in medical malpractice
litigation
Wu KW, Pantaleo N. Am J Health-Syst Pharm 60(3):253-259, 2003
Scope of the ProblemScope of the Problem• Anticoagulation remains underused
– Despite 29 studies showing efficacy of p g yanticoagulation for stroke prevention in patients with Atrial Fibrillation:
– In study of 12 stroke centers from 2003-2007,
– Less than 10% of patients were therapeutically anticoagulated
– 30% not on any anticoagulation therapy– 30% not on any anticoagulation therapy
– 61% not on warfarin; of those treated, 29% subtherapeutic
– Result: 597 pts c/ strokes; 60% disabled, 20% died
Gladstone, DJ, et al. Publication pending, Stroke 2009

3
Scope of the ProblemScope of the Problem
• Anticoagulation remains underused
– HCFA/CMS data: 40,000 strokes/ $600,000,000 annually could be prevented by proper use
– 1-2 million patients treated; 4-6 million patients have indications for treatmentp
– Less than half of pts on treatment are in therapeutic range
Scope of the ProblemScope of the Problem
• Need for improved anticoagulationmanagement widely recognized:
– Centers for Medicare
– AHRQ
– American College of Chest Physicians
– Joint Commission
– Leapfrog Coalition
– Third party providers

4
Scope of the ProblemScope of the Problem
• Need for improved anticoagulation t id l i dmanagement widely recognized
– Examples from the Internet:• (google mail banner)- “www._______.com - Our
Experienced Lawyers Will Review Your Heparin Case For Free”.
• (another site)- “_______ assists attorneys evaluating cases involving anticoagulant therapy by considering the answers to these top ten questions and others applicable to the case:
Scope of the ProblemScope of the Problem1. Was the patient an appropriate candidate for
anticoagulation?
2 Did the patient comply with outpatient blood2. Did the patient comply with outpatient blood tests needed to monitorresponse to the anticoagulants?
3. Were standardized protocols used to order anticoagulation?
4. How often were clotting times tested?
5. Were abnormally elevated clotting times acted upon with dosageadjustments?

5
Scope of the ProblemScope of the Problem
6. Were there any signs of bleeding while the patient was on anticoagulation?
7. How quickly did the healthcare team respond to bleeding?
8. Did the nurses give Heparin or Coumadin as ordered?
9. Is there evidence that hemorrhage was the cause of the patient’scause of the patient sdeath, or was some other cause more likely?
10.What type of medical expert is most appropriate to review the case?”
• 2008 - National Patient Safety Goal 3E
Joint Commission RequirementsJoint Commission Requirements
– Reduce the likelihood of patient harm associated with the use of anticoagulation therapy.
• Full compliance required by all accredited systems as of 1/1/2009accredited systems as of 1/1/2009.

6
Case #1Case #1
• 68 yo female admitted for left knee replacementreplacement
– Surgery successful; on post-op day 15, pt found dead at home
– Post mortem exam: cause of death massive pulmonary embolusmassive pulmonary embolus
– What may have happened? Was anything in this situation preventable?
DVT/PE - ProphylaxisDVT/PE - Prophylaxis
• Current ACCP guidelines - 9th Editiong
– Address what to do
– When to do it
– What to useWhat to use
– What not to use
CHEST 2012; 141(2)(Suppl):e227S–e277S453.

7
DVT/PE - ProphylaxisDVT/PE - Prophylaxis
• What to use – Low Molecular Weight Heparins (LMWH)Heparins (LMWH)
– Enoxaparin – 30 mg SubQ twice daily, or 40 mg SubQ daily
– Dalteparin – 2500-5000 int units SubQ dailyy
– Tinzaparin –not approved for VTE prophylaxis
GeertsGeerts, WH, et al. Prevention of Venous , WH, et al. Prevention of Venous ThromboembolismThromboembolism. . ChestChest. 2008; 133:381S. 2008; 133:381S--453.453.
DVT/PE - ProphylaxisDVT/PE - Prophylaxis
• What to use – Fondaparinux
• Parenteral Factor Xa inhibitor
– Indicated for:
– DVT/PE
– VTE prophylaxis
Geerts, WH, et al. Prevention of Venous Thromboembolism. Chest. 2008; 133:381S-453.

8
DVT/PE - ProphylaxisDVT/PE - Prophylaxis
• What to use – Fondaparinuxp
• Dosing- varies by indication and body weight
– VTE prophylaxis: 2.5 mg SubQ daily, in pts > 50kg
– DVT/PE treatment: 5 mg SubQ daily (pts < 50kg)
7.5 mg SubQ daily (pts 50-100kg)
10 mg SubQ daily (pts > 100kg)
Geerts, WH, et al. Prevention of Venous Thromboembolism. Chest. 2008; 133:381S-453.
DVT/PE - ProphylaxisDVT/PE - Prophylaxis
• What to use – Low dose unfractionated heparin (LDUH or UFH)unfractionated heparin (LDUH or UFH)
– Dosing- 5,000 units SubQ bid or tid
– Compared to LMWH, LDUH is associated with increased risk of heparin induced thrombocytopeniaheparin induced thrombocytopenia
Geerts, WH, et al. Prevention of Venous Thromboembolism. Chest. 2008; 133:381S-453.

9
DVT/PE - ProphylaxisDVT/PE - Prophylaxis
• What to use – Warfarin
– Dosing- varies due to medications, genetic phenotype, diet. If used for prophylaxis:
– VTE prophylaxis: INR goal should be 2 5 with acceptable INR range of 2 32.5, with acceptable INR range of 2-3.
Geerts, WH, et al. Prevention of Venous Thromboembolism. Chest. 2008; 133:381S-453.
DVT/PE - ProphylaxisDVT/PE - Prophylaxis
• What to use – Rivaroxaban
– Dosing- 10 mg po daily:
– VTE prophylaxis: for hip replacement: duration is 35 days
F k l d i i 12– For knee replacement: duration is 12 days
CHEST 2012; 141(2)(Suppl):e227S–e277S453.

10
DVT/PE - ProphylaxisDVT/PE - Prophylaxis• What NOT to do:
N thi id f h l i– Nothing – avoidance of prophylaxis results in avoidable morbidity and mortality
– Rely on Aspirin alone
– Rely on mechanical devices alone, unless patient has high risk of bleeding
Geerts, WH, et al. Prevention of Venous Thromboembolism. Chest. 2008; 133:381S-453.
DVT/PE - ProphylaxisDVT/PE - Prophylaxis
• What TO do: Prevent the Event!
For patients undergoing:– For patients undergoing:
• Major general, gynecologic, or urologic surgery-use LMWH, unfractionated heparin (UFH) or fondaparinux
• Consider Intermittent Pneumatic Compression as adjunct
Geerts, WH, et al. Prevention of Venous Thromboembolism. Chest. 2008; 133:381S-453.

11
• What to do: Prevent the Event!
For patients undergoing:
DVT/PE - ProphylaxisDVT/PE - Prophylaxis
– For patients undergoing:
• Hip or knee arthroplasty, hip fx repair-use LMWH, fondaparinux, or warfarin (goal INR 2.5), for at least 10 daysleast 10 days
• Consider Intermittent Pneumatic Compression as adjunct
Geerts, WH, et al. Prevention of Venous Thromboembolism. Chest. 2008; 133:381S-453.
DVT/PE - ProphylaxisDVT/PE - Prophylaxis
• What TO do: Prevent the Event!
– For patients with acute medical illness – use LMWH, UFH or fondaparinux
• Consider Intermittent Pneumatic C i dj tCompression as adjunct
Geerts, WH, et al. Prevention of Venous Thromboembolism. Chest. 2008; 133:381S-453.

12
DVT/PE - ProphylaxisDVT/PE - Prophylaxis• What TO do: Prevent the Event!
Thromboproph la is is also– Thromboprophylaxis is also important for patients in the following situations:
• Intensive Care Unit
• Major trauma
• Spinal cord injury
GeertsGeerts, WH, et al. Prevention of Venous , WH, et al. Prevention of Venous ThromboembolismThromboembolism. . ChestChest. 2008; 133:381S. 2008; 133:381S--453.453.
DVT/PE - ProphylaxisDVT/PE - Prophylaxis– ACCP 9th guidelines changes:
• Post op ortho Rx duration 10 35• Post-op ortho Rx duration- 10-35 days; consider new DTI’s
• Low risk medical pts may not require Rx
• Outpts with CA but no other risks-no routine prophylaxis
CHEST 2012; 141(2)(Suppl):e278SCHEST 2012; 141(2)(Suppl):e278S––e325Se325S..CHEST 2012; 141(2)(Suppl):e278SCHEST 2012; 141(2)(Suppl):e278S––e325Se325S..

13
Case #2Case #2
• 59 yo male admitted for CABG
S f l d– Surgery successful; on post-op day 5, pt c/o of sudden pain in R leg
– PE: R LE cool, c/ diminished DP pulse
L b L t BUN C WNL CBC H/H– Lab: Lytes BUN Cr WNL; CBC: H/H 9.2/29, WBC 11.5, Plts 63,000
– What may have happened?
Case #2Case #2
• Heparin Induced Thrombocytopenia
Severe adverse drug reaction to– Severe adverse drug reaction to heparin
– Caused by antibody mediated reaction
A i t d ith i ifi tl– Associated with significantly increased risk of thrombosis
Warkentin TE, Levine MN, Hirsh J, et al. Heparin-induced thrombocytopenia in patients treated with low molecularweight heparin or unfractionated heparin. N Engl J Med 1995; 332:1330–1335

14
Heparin Induced Thrombocytopenia
Heparin Induced Thrombocytopenia
• Early detection is effective
– Consider regularly scheduled platelet counts (every 2-3 days) for all patients on UFH or LMWH.
– A reduction in platelet counts of greater than 50% from baseline should trigger gguse of alternative agent for anticoagulation until laboratory evaluation confirms or rules out HIT.
Franchini M. Heparin Induced Thrombocytopenia: An Update. Thrombosis Journal 2005, 3:14
Heparin Induced Thrombocytopenia
Heparin Induced Thrombocytopenia
• If HIT is suspected:
– Clinical suspicion is key- don’t wait for confirmation
– If suspected, immediately stop all heparin, LMWH
Start alternative agent for– Start alternative agent for anticoagulation; must not cross react with HIT associated antibodies.
Chong BH: Heparin-induced thrombocytopenia. J Thromb Haemost 2003, 1:1471-1478.
Franchini M. Heparin Induced Thrombocytopenia: An Update. Thrombosis Journal 2005, 3:14

15
Heparin Induced Thrombocytopenia
Heparin Induced Thrombocytopenia
• Treatment- alternative agents
A d t f HIT t t t ll– Approved agents for HIT treatment; all directly inhibit thrombin activity or formation
• Argatroban
• Lepirudin• Lepirudin
• Danaparoid
Chong BH: Heparin-induced thrombocytopenia. J Thromb Haemost 2003, 1:1471-1478.
Chong BH: Heparin-induced thrombocytopenia. J Thromb Haemost 2003, 1:1471-1478.
Franchini M. Heparin Induced Thrombocytopenia: An Update. Thrombosis Journal 2005, 3:14
HIT – TreatmentHIT – Treatment• Argatroban
Dosing - initial dose is 2– Dosing - initial dose is 2 μg/kg/minute given intravenously
– Adjust dose to achieve an aPTT 1.5 to 3 times the baseline value.
– Drug of choice for patients with renal insufficiency
Franchini M. Heparin Induced Thrombocytopenia: An Update. Thrombosis Journal 2005, 3:14Chong BH: Heparin-induced thrombocytopenia. J Thromb Haemost 2003, 1:1471-1478.

16
HIT – TreatmentHIT – Treatment• Danaparoid
– Dosing - intravenous bolus dose of 2500 U followed by 400 U/hour for 4 hours, then 300 U/hour for 4 hours and subsequently 200 U/hour until anticoagulation is no longer requiredq
– Adjust the dose to maintain plasmaanti-Xa levels within 0.5–0.8 U/mL.
Franchini M. Heparin Induced Thrombocytopenia: An Update. Thrombosis Journal 2005, 3:14Chong BH: Heparin-induced thrombocytopenia. J Thromb Haemost 2003, 1:1471-1478.
HIT – TreatmentHIT – Treatment• Lepirudin
– Dosing - 0.4 mg/kg as a bolus f ll d b 0 15 /k /hfollowed by 0.15 mg/kg/hour
– Adjust the dose to achieve an aPTT of 1.5 to 3 times the baseline value.
– Drug of choice for patients withDrug of choice for patients with liver dysfunction, or requiring cardiac surgery
Franchini M. Heparin Induced Thrombocytopenia: An Update. Thrombosis Journal 2005, 3:14Chong BH: Heparin-induced thrombocytopenia. J Thromb Haemost 2003, 1:1471-1478.

17
Anticoagulation : Anticoagulation : New Guidelines andNew Guidelines andNew AnticoagulantsNew Anticoagulants
Anticoagulation : Anticoagulation : New Guidelines andNew Guidelines andNew AnticoagulantsNew Anticoagulantsgggg
Aaron Dush, PharmD, CACPSpecialty Practice Pharmacist, Anticoagulation
The Ohio State UniversityyComprehensive Cancer Center-
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
9th Edition CHEST Guidelines February 2012
9th Edition CHEST Guidelines February 2012
Wh t f th What are some of the new recommendations
What are some of the changes
How do we apply these to patient care

18
Methodology for the Development of Antithrombotic Therapy and Prevention of Thrombosis Guidelines: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl 53S
Methodology for the Development of Antithrombotic Therapy and Prevention of Thrombosis Guidelines: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl 53S

19
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based
Clinical Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based
Clinical Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
2.1. For patients sufficiently healthy to be treated as outpatients, we suggest initiating Vitamin K Antagonist (VKA) therapy with warfarin 10 mg daily for the first 2 days followed by dosing based on INRfollowed by dosing based on INR measurements rather than starting with the estimated maintenance dose (Grade 2C).
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of
Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice
Guidelines Chest February 2012 141:2 suppl e152S-e184S
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of
Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice
Guidelines Chest February 2012 141:2 suppl e152S-e184S
3.1. For patients taking VKA therapy with consistently stable INRs, we suggest an INR testing frequency of up to 12 weeks rather than every 4 p yweeks (Grade 2B)

20
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
3.2. For patients taking VKAs with previously stable therapeutic INRs who present with a single out-of-range INR of ≤ 0.5 below or above therapeutic, we suggest continuing the current dosesuggest continuing the current dose and testing the INR within 1 to 2 weeks (Grade 2C).
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
3.3. For patients with stable therapeutic INRs presenting with a single subtherapeutic INR value, we suggest against routinely administering bridging with heparin (Grade 2C).

21
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
9.1. (a) For patients taking VKAs with INRs between 4.5 and 10 and no evidence of bleeding, we suggest against the routine use of vitamin K (G d 2B)(Grade 2B)
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
(b) For patients taking VKAs with INRs > 10.0 and with no evidence of bleeding, we suggest that oral vitamin K be administered (Grade (2C).

22
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e152S-e184S
9 3 For patients with VKA-associated major9.3. For patients with VKA-associated major bleeding, we suggest rapid reversal of anticoagulation with four-factor PCC rather than with plasma (Grade 2C).
We suggest the additional use of vitamin K 5 ggto 10 mg administered by slow IV injection rather than reversal with coagulation factors alone (Grade 2C).
Case 1Case 1 LP is an 52 yo male with a history of
recurrent thrombotic events on chronic warfarin therapy
Patient has been stable within his desired therapeutic INR range of 2-3 on his current total weekly dose (TWD) of warfarin for 6
thmonths
Today he presents in clinic with an INR 1.6
What should be done?

23
Case 1Case 1 According to the new CHEST guidelines:
– The patient’s current TWD should be continued and the patient should follow-up in 1-2 weeks
– Bridge therapy does not need to be initiated at this time
Antithrombotic Therapy for Atrial Fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e531S-e575S
Antithrombotic Therapy for Atrial Fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e531S-e575S

24
Antithrombotic Therapy for Atrial Fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e531S-e575S
Antithrombotic Therapy for Atrial Fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e531S-e575S
2 1 8 For patients with AF including those with2.1.8. For patients with AF, including those with paroxysmal AF, who are at low risk of stroke (eg, CHADS2 score = 0), we suggest no therapy rather than antithrombotic therapy (Grade 2B). For patients who do choose antithrombotic therapy, we suggest aspirin (75 mg to 325 mg once daily)we suggest aspirin (75 mg to 325 mg once daily) rather than oral anticoagulation (Grade 2 B) or combination therapy with aspirin and clopidogrel (Grade 2B).
Antithrombotic Therapy for Atrial Fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e531S-e575S
Antithrombotic Therapy for Atrial Fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e531S-e575S
2.1.9. For patients with AF, including those with2.1.9. For patients with AF, including those with paroxysmal AF, who are at intermediate risk of stroke (eg, CHADS2 score = 1), we recommend oral anticoagulation rather than no therapy (Grade 1B). We suggest oral anticoagulation rather than aspirin (75 mg to 325 mg once daily) (Grade 2B) or combination therapy with aspirin and clopidogrel (Grade 2B). For py p p g ( )patients who are unsuitable for or choose not to take an oral anticoagulant (for reasons other than concerns about major bleeding), we suggest combination therapy with aspirin and clopidogrel rather than aspirin (75 mg to 325 mg once daily) (Grade 2B).

25
Antithrombotic Therapy for Atrial Fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e531S-e575S
Antithrombotic Therapy for Atrial Fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e531S-e575S
2.1.10. For patients with AF, including those with l AF h t hi h i k f t k (paroxysmal AF, who are at high risk of stroke (eg,
CHADS2 score ≥ 2), we recommend oral anticoagulation rather than no therapy (Grade 1A), aspirin (75 mg to 325 mg once daily) (Grade 1B), or combination therapy with aspirin and clopidogrel (Grade 1B). For patients who are unsuitable for or choose not to take an oral anticoagulant (for reasons other than concerns about major bleeding), we recommend combination therapy with aspirin and clopidogrel rather than aspirin (75 mg to 325 mg once daily). (Grade 1B)
Antithrombotic Therapy for Atrial Fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e531S-e575S
Antithrombotic Therapy for Atrial Fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e531S-e575S
2.1.11. For patients with AF, including those with paroxysmal AF, for recommendations in favor of oral anticoagulation, we suggest dabigatran 150 mg twice daily rather than adjusted-dose VKA therapy (target INR range, 2.0 – 3.0) (Grade 2B).
Remarks: Dabigatran is excreted primarily by theRemarks: Dabigatran is excreted primarily by the kidney. It has not been studied and is contraindicated in patients with severe renal impairment (estimated creatinine clearance of ≤ 30 mL/min). Clinicians should be aware that there is no antidote for dabigatran.

26

27
Dabigatran (Pradaxa®)PI: Pradaxa (dabigatran)oral tablets; Boehringer Ingelheim; Ridgefield, CT,
2010
Dabigatran (Pradaxa®)PI: Pradaxa (dabigatran)oral tablets; Boehringer Ingelheim; Ridgefield, CT,
2010
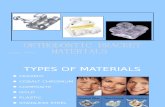
Direct thrombin inhibitor indicated to reduce the risk of stroke and systemic embolism in patients y pwith non-valvular atrial fibrillation
CrCl Dose
>30 mL/min 150mg BID
15-30 mL/min 75mg BID*
* Based on pharmacokinetic modeling
<15 mL/min or hemodialysis Unknown
Dabigatran (Pradaxa®)Stangier J. Clin Pharmacokinet 2008;47:285-295
Dabigatran (Pradaxa®)Stangier J. Clin Pharmacokinet 2008;47:285-295
Bi il bilit 6 5%Bioavailability 6.5%
tmax 1.5-3 h (healthy patients)
3.7-4.5 h (day of surgery)
Vd 60-70 L
Elimination 80% renal unchangedg
t½ 12-17 h
Protein binding 35%

28
Dabigatran (Pradaxa®)Stangier J. Clin Pharmacokinet 2008;47:285-295
Dabigatran (Pradaxa®)Stangier J. Clin Pharmacokinet 2008;47:285-295
Holding for Procedures
Creatinine Clearance Hold for:
≥ 50 mL/min 1-2 days
< 50 mL/min 3-5 days
Consider holding longer for major surgery, spinal puncture,placement of spinal/epidural catheter
Dabigatran (Pradaxa®)Dabigatran (Pradaxa®)
No cytochrome P-450 activity
Interaction with P-glycoprotein
No dietary interactions
Larger Therapeutic Indexa ge e apeut c de
No monitoring recommended

29
Rivaroxiban (Xarelto®)PI: Xarelto (dabigatran) oral tablets; Bayer HealthCare AG, 51368
Leverkusen, Germany
Rivaroxiban (Xarelto®)PI: Xarelto (dabigatran) oral tablets; Bayer HealthCare AG, 51368
Leverkusen, Germany
Rivaroxaban selectively inhibits factor Xa to reduce the risk of stroke and systemic embolism in patients with non-valvular atrial fibrillation and to reduce the risk of deepvalvular atrial fibrillation and to reduce the risk of deep vein thrombosis post knee and hip replacement surgery
Indication CrCl Dose
A-Fib > 50 ml/min 20 mg daily
A-Fib 15 - 50 ml/min 15 mg daily
Post-Hip Replacement 10 mg dailyPost Hip Replacement 10 mg daily
(rec. duration of 35 days)
Post- Knee Replacement
10 mg daily
(rec. duration of 12 days)
“The Ideal Anticoagulant”“The Ideal Anticoagulant”Warfarin Dabigatran Rivaroxiban
Oral dosage form
Predictable, rapid effect
Few drug interactions
Reversibility
InexpensiveInexpensive
No need for monitoring
Once daily dosing

30
Other Considerations for New Anticoagulants
Other Considerations for New Anticoagulants
No reversal agentg
Adverse reactions
Still bleeding risk
Dyspepsia (35% with dabigatran)
Renal DosingRenal Dosing
Lack of monitoring
Other Considerations for New Anticoagulants
Other Considerations for New Anticoagulants
Compliance Compliance
Faster return to baseline (short half-life syndrome)
Cost
Twice daily dosing (dabigatran)

31
Perioperative Management of Antithrombotic Th A tith b ti Th dTherapy: Antithrombotic Therapy and
Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based
Clinical Practice Guidelines
Chest February 2012 141:2 suppl e326S-Chest February 2012 141:2 suppl e326Se350S
Case 2Case 2 JP is a 49yo female
Thrombosis of the main portal vein May 2011,
Rescanned February 2012 still showing portal vein Rescanned February 2012 still showing portal vein thrombosis.
Hx of stage I ER/PR positive breast cancer.
Mastectomy and sentinel lymph node biopsy was performed on 01/30/2008
No findings on Mammogram December 2011 No findings on Mammogram December 2011.
Adjuvent hormone therapy with tamoxifen March 2008-May 2011. Changed to letrozole May 2011.
Thrombosis risk tamoxifen vs. letrozole (1.7% vs 1.1%)

32
Case 2Case 2
Patient having laparoscopic surgery for small recurrent ventral hernia
How do we handle her anticoagulation?
First question – When do we stop her anticoagulation?
First question – When do we stop her anticoagulation?
How long prior to her procedure should her How long prior to her procedure should her warfarin be stopped?
If bridged – when should her bridge therapy be stopped?

33
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
2.1. In patients who require temporary interruption of a VKA before surgery, we recommend stopping VKAs approximately 5 days before surgery instead of stopping VKAs a shorterinstead of stopping VKAs a shorter time before surgery (Grade 1C).
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
4.3. In patients who are receiving bridging anticoagulation with therapeutic-dose SC LMWH, we suggest administering the last preoperative dose of LMWH approximately 24 hours before surgery instead of 1224 hours before surgery instead of 12 hours before surgery (Grade 2C).

34
What is the patients risk of a recurrent thrombotic event?
What is the patients risk of a recurrent thrombotic event?
High Riskg
Moderate Risk
Low Risk
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S

35
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
High Risk Patientsg s at e ts2.4. In patients with a mechanical heart valve, atrial fibrillation, or VTE at high risk for thromboembolism, we suggest bridging anticoagulation instead of no bridging during interruption of VKA therapy (Grade 2C).
Remarks: Patients who place a higher value on avoiding perioperative bleeding than on avoiding perioperative thromboembolism are likely to decline heparin bridging.
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based
Clinical Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based
Clinical Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Low Risk PatientsLow Risk Patients
In patients with a mechanical heart valve, atrial fibrillation, or VTE at low risk for thromboembolism, we suggest no-bridging instead of bridging g g g ganticoagulation during interruption of VKA therapy (Grade 2C).

36
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Moderate Risk PatientsModerate Risk Patients
In patients with a mechanical heart valve, atrial fibrillation, or VTE at moderate risk for thromboembolism, the bridging or no-bridging approach chosen is, as in the higher- and lower-risk patients, based on an assessment of individual patient- and surgery-related factors.
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Moderate Risk – Who do we consider bridge therapy?
•Patients with a mechanical bileaflet aortic valve and additional stroke risk factors comprising prior stroke or systemic embolism or transient ischemic attack, hypertension, diabetes, congestive heart failure, or age > 75 years
•Patients with atrial fibrillation and a CHADS2 score of 3 or 4 or i th b b li d i i t ti f f i
Answer: All Moderate Risk patients should be considered for bridge therapy
prior thromboembolism during interruption of warfarin
•Patients with VTE within the past 3 to 12 months, nonsevere thrombophilia, active cancer, and recurrent VTE

37
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based
Clinical Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based
Clinical Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Other considerations
High-bleeding-risk procedures
Renal function

38
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
What dose of Low-Molecular-Weight-gHeparin (LMWH) do we use to bridge?
No published randomized, controlled trials on bridge therapy
In observational studies high-risk patients typically received therapeutic dose LMWH
BRIDGE Study
Prevention of VTE in Nonsurgical Patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e195S-e226S
Prevention of VTE in Nonsurgical Patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Chest February 2012 141:2 suppl e195S-e226S
4.2.2. In outpatients with solid tumors who have additional risk factors for VTE and who are at low risk of bleeding, we suggest prophylactic-dose LMWH or LDUH over no prophylaxis (Grade 2B).
Remarks: Additional risk factors for venousRemarks: Additional risk factors for venous thrombosis in outpatients with cancer include previous venous thrombosis, immobilization, hormonal therapy, angiogenesis inhibitors, thalidomide, and lenalidomide

39
What do we do with our patient
What do we do with our patient
What risk category does she fall in? What risk category does she fall in?
What other risk factors does she possess?
What is the bleeding risk for this patient’s procedure?
What was decidedWhat was decided
After discussion with the patient’s Oncologist, it was determined to bridge this patient with enoxaparin
Deemed patient was moderate risk
Acute event 3-12 months ago
Recent scan showing chronic thrombus
Patient is on hormonal therapy
Bleeding risk deemed low for procedure

40
What about post-procedure?What about post-procedure?
When do we restart the patients warfarin th ?therapy?
When do we restart the patient’s bridge therapy?
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
2.2. In patients who require temporary interruption of a VKA before surgery, we recommend resuming VKAs approximately 12 to 24 hours after surgery (evening of or next morning) and when there is adequate hemostasiswhen there is adequate hemostasis instead of later resumption of VKAs (Grade 2C).

41
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
Perioperative Management of Antithrombotic Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines Chest February 2012 141:2 suppl e326S-e350S
4 4 In patients who are receiving bridging4.4. In patients who are receiving bridging anticoagulation with therapeutic-dose SC LMWH and are undergoing high-bleeding-risk surgery, we suggest resuming therapeutic-dose LMWH 48 to 72 hours after surgery instead of resuming LMWH within 24 hours after surgery (Grade 2C). In patients who are receiving bridging anticoagulation with therapeutic dose SCbridging anticoagulation with therapeutic-dose SC LMWH and are undergoing non-high-bleeding-risk surgery, we suggest resuming therapeutic-dose LMWH approximately 24 hours after surgery instead ofresuming LMWH more than 24 hours after surgery.
Summary of Bridge Therapy
Summary of Bridge Therapy
Bridging guidelines still vagueBridging guidelines still vague
Still no published randomized, controlled clinical trials with bridge therapy (BRIDGE Study ongoing)
Each patient still needs assessed individually
Guidelines will not encompass all patients and all patient risk factors

42
Improving Quality: Improving Quality: Anticoagulation TherapyAnticoagulation Therapy
Improving Quality: Improving Quality: Anticoagulation TherapyAnticoagulation Therapy
Mark Wurster, MDFounder and Chief Medical Officer
Standing Stone, Inc.
The New AgentsThe New Agents• Unresolved issues –
• ‘Short half-life syndrome’
• Emergency reversal
• Drug/Treatment costs
• Efficacy of outcomes vs. AC carey
• Post marketing surveillance will be crucial

43
DabigatranDabigatran• Pradaxa (Dabigatran)- current
situation
• Numerous case reports of complications are being reported in US, New Zealand, Australia
• In December 2011, FDA requested additional information from physicians regarding PradaxaPradaxa
• Case reports are limited in terms of information gained, especially in terms of relative risk compared to other therapeutic options
The New Agents- Clinical UseThe New Agents- Clinical Use• Dabigatran Case Series – A
prospective, observational cohort st dstudy
• Purpose-
• To evaluate the clinical outcomes of patients receiving anticoagulationpatients receiving anticoagulation therapy with dabigatran, using warfarin therapy as a comparison

44
Dabigatran Case SeriesDabigatran Case Series• Setting-
• Staten Island / Long Island Jewish hospital-
• Anticoagulation clinic currently follows approximately 2200 patients,follows approximately 2200 patients, the majority of which are POC testers
Dabigatran Case SeriesDabigatran Case Series• Design-
• Beginning 11/2010, all patients switched from warfarin to dabigatran followed prospectively for one year, with retrospective chart reviews covering one year prior while on warfarin
• Cohort design allows each patient to serve as Co o t des g a o s eac pat e t to se e astheir own control
• Endpoints- bleeds, thromboses, or other Rx complications that required med to be D/C’ed

45
Dabigatran Case SeriesDabigatran Case Series
• Design-
• Endpoints- bleeds, thromboses, or other treatment related complications that required medication to be discontinuedmedication to be discontinued
• Results were compared by means of Fisher’s exact test
Dabigatran Case SeriesDabigatran Case Series
• Preliminary Results-
• For 113 eligible patients after 6 months of warfarin therapy, followed by 6 months of dabigatran therapy:
• For almost all patients, reasons listed for switching therapy included physician orswitching therapy included physician or patient convenience; in one case, a patient who planned to be overseas needed an alternative to regular INR monitoring

46
Dabigatran Case SeriesDabigatran Case Series
• Preliminary Results-
• During warfarin treatment phase, one patient was admitted to the hospital for diagnosis of ‘warfarin t i it ’toxicity’
Dabigatran Case SeriesDabigatran Case Series
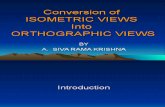
14
Events Requiring Medication Stoppage
4
6
8
10
12
14
# of Events (p <0.0014)
0
2
Warfarin Treatment
Phase
Dabigatran Treatment
Phase

47
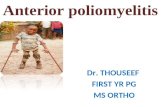
Dabigatran Case SeriesDabigatran Case SeriesOther (skin rash)8%
Frequency of Dabigatran Complications by Type
Hemorrhage38%
GastroIntestinal Sx
31%
8%
Thrombosis23%
number of events = 13
Dabigatran Case SeriesDabigatran Case Series
• Preliminary Results-
• During dabigatran treatment phase: one death (GI bleed), four other bleeding episodes (two GI bleeds, one rectus sheath hemorrhage, one intracranial h h ) D Vhemorrhage), one Deep Venous Thrombosis, one atrial thrombus, one Transient Ischemic Attack, one skin rash, and four GI reactions

48
Dabigatran Case SeriesDabigatran Case Series• Preliminary Results
• Incidence of endpoints during warfarin therapy phase was 0.83%
• Incidence of endpoints during dabigatran therapy phase was 11.5 %
• The difference was HIGHLY statistically significant
• (p < 0.0014)
• Relative risk of adverse event with dabigatran = 13.8
Dabigatran Case SeriesDabigatran Case Series
• Preliminary Results
• Why are the differences so striking, compared to prior studies?
• Sampling error?
• ‘Usual care’ versus study related close observation?
• Use in inappropriate subjects?
• Poor warfarin use in prior studies (TTR in RE-LY was 64% with huge variation internationall,y compared to 70% for warfarin clinic in this study)

49
Dabigatran Case SeriesDabigatran Case Series• The current study is still active –
• Goals for final report – continueGoals for final report continue observation of patients for a further 6 months, with emphasis on:
• Demographics
• Renal Function
• Co morbidities• Co-morbidities
• Concomitant medications
• Other possible factors that may influence appropriate patient selection for the medication