Improving Quality and Ef ciency for Intussusception...
10
Improving Quality and Efficiency for Intussusception Management After Successful Enema Reduction Mehul V. Raval, MD, MS a , Peter C. Minneci, MD, MHSc b , Katherine J. Deans, MD, MHSc b , Kelli J. Kurtovic, MS c , Ann Dietrich, MD d , D. Gregory Bates, MD e , Shawn J. Rangel, MD, MSCE f , R. Lawrence Moss, MD b , Brian D. Kenney, MD, MPH b abstract OBJECTIVES: The purpose of this project was to implement a protocol facilitating discharge from the emergency department (ED) after successful radiologic ileocolic intussusception reduction in a pediatric referral center. METHODS: A multidisciplinary team identified drivers for successful quality improvement including educational brochures, a standardized radiologic report, an observation period in the ER with oral hydration challenges, and follow-up phone calls the day after discharge. Patient outcomes were tracked, and quarterly feedback was provided. RESULTS: Of 80 patients identified over a 24-month period, 34 (42.5%) did not qualify for discharge home due to need for surgical intervention (n = 9), specific radiologic findings (n = 11), need for additional intravenous hydration (n = 4), or other reasons (n = 7). Of 46 patients who qualified for discharge, 30 (65.2%) were successfully sent home from the ED. One patient returned with recurrent symptoms that required repeat enema reduction. Sixteen patients were observed and discharged within 23 hours. Adherence with discharge from the ED improved over time. Discharge from the ED was associated with cost savings and improved net margins at the hospital level for each encounter. CONCLUSIONS: A sustainable multidisciplinary quality improvement project to discharge intussusception patients from the ED after air-contrast enema reduction was successfully integrated in a high-volume referral center through education, standardized radiologic reporting, and protocoled follow-up. Intussusception remains one of the most common causes of intestinal obstruction in young children and infants. Treatment of intussusception has evolved over time from a predominantly operative disease to one managed nonoperatively most of the time with high success with radiologically guided enema reduction. 1 Traditional practice after successful enema reduction of intussusception includes surgical admission for observation to ensure toleration of enteral diet advancement and to monitor for recurrence of intussusception, which occurs in ,10% of patients. 2 Absolute indications for admission in the setting of intussusception include perforation, failed enema reduction, and successful enema reduction with identification of a lead point that would merit semiurgent resection to prevent recurrent obstruction. Relative indications for admission after successful enema reduction of intussusception are poorly defined but include a prolonged prodrome of symptoms, presence of bloody stools, and dehydration. Several institutions a Division of Pediatric Surgery, Department of Surgery, Children’ s Healthcare of Atlanta, Emory University School of Medicine, Atlanta, Georgia; b Division of Pediatric Surgery, Department of Surgery, and e Department of Radiology, Nationwide Children’ s Hospital, The Ohio State University School of Medicine, Columbus, Ohio; c Quality Improvement Services, Nationwide Children’ s Hospital, Columbus, Ohio; d Ohio University College of Medicine, Athens, Ohio; and f Division of Pediatric Surgery, Department of Surgery, Boston Children’ s Hospital, Harvard Medical School, Boston, Massachusetts Dr Raval conceptualized and designed the project, led data analysis on a quarterly basis, coordinated day-to-day conduction of the project, and drafted the initial manuscript; Drs Minneci, Deans, Dietrich, Bates, Rangel, and Moss provided clinical guidance toward concept and design including aim and key driver definition, protocol development, and implementation; assisted with data interpretation, and assisted with manuscript revision; Ms Kurtovic assisted with project conception, development, and design; served as the primary data collector; and critically reviewed the manuscript; Dr Kenney conceptualized and designed the project with Dr Raval, oversaw data feedback to staff, and critically revised the final manuscript; and all authors approved the final manuscript as submitted. www.pediatrics.org/cgi/doi/10.1542/peds.2014-3122 DOI: 10.1542/peds.2014-3122 Accepted for publication May 19, 2015 Address correspondence to Mehul V. Raval, MD, MS, Division of Pediatric Surgery, Department of Surgery, Emory University School of Medicine, Children’ s Healthcare of Atlanta, 1405 Clifton Rd NE, Atlanta, GA 30322. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2015 by the American Academy of Pediatrics PEDIATRICS Volume 136, number 5, November 2015 QUALITY REPORT by guest on September 1, 2018 www.aappublications.org/news Downloaded from
Transcript of Improving Quality and Ef ciency for Intussusception...
Improving Quality and Efficiency forIntussusception Management AfterSuccessful Enema ReductionMehul V. Raval, MD, MSa, Peter C. Minneci, MD, MHScb, Katherine J. Deans, MD, MHScb, Kelli J. Kurtovic, MSc, Ann Dietrich, MDd,D. Gregory Bates, MDe, Shawn J. Rangel, MD, MSCEf, R. Lawrence Moss, MDb, Brian D. Kenney, MD, MPHb
abstractOBJECTIVES: The purpose of this project was to implement a protocol facilitatingdischarge from the emergency department (ED) after successful radiologicileocolic intussusception reduction in a pediatric referral center.
METHODS: A multidisciplinary team identified drivers for successful qualityimprovement including educational brochures, a standardized radiologicreport, an observation period in the ER with oral hydration challenges, andfollow-up phone calls the day after discharge. Patient outcomes were tracked,and quarterly feedback was provided.
RESULTS: Of 80 patients identified over a 24-month period, 34 (42.5%) did notqualify for discharge home due to need for surgical intervention (n = 9),specific radiologic findings (n = 11), need for additional intravenous hydration(n = 4), or other reasons (n = 7). Of 46 patients who qualified for discharge, 30(65.2%) were successfully sent home from the ED. One patient returned withrecurrent symptoms that required repeat enema reduction. Sixteen patientswere observed and discharged within 23 hours. Adherence with dischargefrom the ED improved over time. Discharge from the ED was associated withcost savings and improved net margins at the hospital level for eachencounter.
CONCLUSIONS: A sustainable multidisciplinary quality improvement project todischarge intussusception patients from the ED after air-contrast enemareduction was successfully integrated in a high-volume referral center througheducation, standardized radiologic reporting, and protocoled follow-up.
Intussusception remains one of themost common causes of intestinalobstruction in young children andinfants. Treatment of intussusceptionhas evolved over time froma predominantly operative disease toone managed nonoperatively most ofthe time with high success withradiologically guided enemareduction.1 Traditional practice aftersuccessful enema reduction ofintussusception includes surgicaladmission for observation to ensuretoleration of enteral diet advancementand to monitor for recurrence of
intussusception, which occurs in,10% of patients.2
Absolute indications for admission inthe setting of intussusception includeperforation, failed enema reduction,and successful enema reduction withidentification of a lead point that wouldmerit semiurgent resection to preventrecurrent obstruction. Relativeindications for admission aftersuccessful enema reduction ofintussusception are poorly defined butinclude a prolonged prodrome ofsymptoms, presence of bloody stools,and dehydration. Several institutions
aDivision of Pediatric Surgery, Department of Surgery,Children’s Healthcare of Atlanta, Emory University School ofMedicine, Atlanta, Georgia; bDivision of Pediatric Surgery,Department of Surgery, and eDepartment of Radiology,Nationwide Children’s Hospital, The Ohio State UniversitySchool of Medicine, Columbus, Ohio; cQuality ImprovementServices, Nationwide Children’s Hospital, Columbus, Ohio;dOhio University College of Medicine, Athens, Ohio; andfDivision of Pediatric Surgery, Department of Surgery,Boston Children’s Hospital, Harvard Medical School, Boston,Massachusetts
Dr Raval conceptualized and designed the project,led data analysis on a quarterly basis, coordinatedday-to-day conduction of the project, and drafted theinitial manuscript; Drs Minneci, Deans, Dietrich,Bates, Rangel, and Moss provided clinical guidancetoward concept and design including aim and keydriver definition, protocol development, andimplementation; assisted with data interpretation,and assisted with manuscript revision; Ms Kurtovicassisted with project conception, development, anddesign; served as the primary data collector; andcritically reviewed the manuscript; Dr Kenneyconceptualized and designed the project with DrRaval, oversaw data feedback to staff, and criticallyrevised the final manuscript; and all authorsapproved the final manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-3122
DOI: 10.1542/peds.2014-3122
Accepted for publication May 19, 2015
Address correspondence to Mehul V. Raval, MD, MS,Division of Pediatric Surgery, Department ofSurgery, Emory University School of Medicine,Children’s Healthcare of Atlanta, 1405 Clifton Rd NE,Atlanta, GA 30322. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,1098-4275).
Copyright © 2015 by the American Academy ofPediatrics
PEDIATRICS Volume 136, number 5, November 2015 QUALITY REPORT by guest on September 1, 2018www.aappublications.org/newsDownloaded from
have reported success with earlydischarge from the emergencydepartment (ED) for intussusceptionpatients successfully reduced withenema.2–6 Wide practice variationexists across major children’shospitals in the United States,resulting in inconsistent costs andresource utilization.7 Traditionalpractice at our center, a high-volume,tertiary, free-standing, pediatricreferral center, was to admit allpatients with intussusception forobservation. We instituted a qualityimprovement (QI) initiative toincrease the proportion of patientsdischarged from the hospital from theED after successful enema reduction.The purpose of this article is todescribe the implementation toolsused and lessons learned from this QIproject.
METHODS
Setting
This QI effort took place atNationwide Children’s Hospital(Columbus, OH). The hospital isa quaternary care pediatric referraland research center with .450inpatient beds. There are.83 000 EDvisits and nearly 26 000 surgicalprocedures performed at NationwideChildren’s Hospital annually. Thegeneral pediatric surgical servicemaintains a daily census thataverages 60 to 90 patients caredfor by 15 attending surgeons.
Planning the Intervention
To increase the number of patientsdischarged from the ED aftersuccessful enema reduction ofileocolic intussusception,a multidisciplinary team was createdwith representation from surgical,radiologic, and ED services. An aim todischarge 50% of patients from theED who met clinical grounds fordischarge was established afterreview of available literature andcomparison with ED discharge ratesat comparison children’s hospitals.A time frame for measurement within
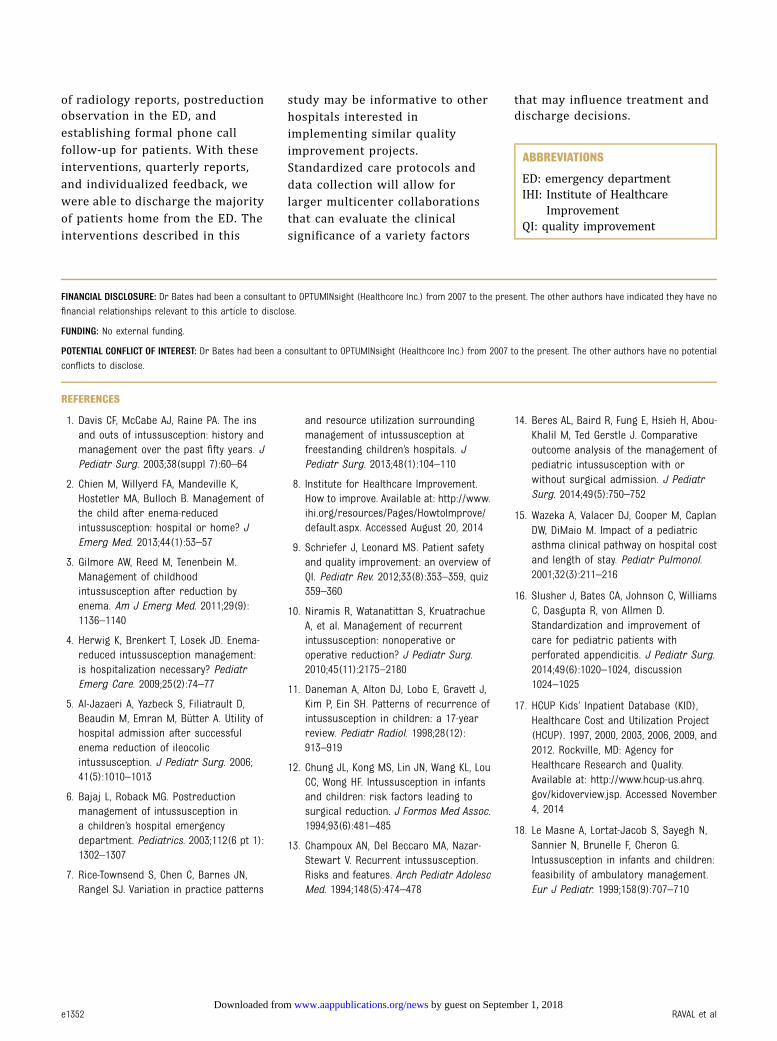
6 months of project initiation withsustainability beyond 1 year wasoutlined. Key drivers focused oneducation and standardization wereidentified, and specific interventionswere designed (Fig 1). Educationbegan with a presentation to all 15surgical faculty members to reviewprotocols in place at variouschildren’s hospitals. National practicevariation was explored, and practicehabits and indications for admissionwere discussed. In addition, all EDattending staff members were briefedat the start of the project at a sectionmeeting, and e-mails were sent to allproviders including surgical and EDattending staff and fellows.
On the basis of consensus among themultidisciplinary faculty, absoluteand relative criteria for admissionwere developed. Patients excludedfrom consideration for dischargewere those who failed enemareduction, required operativeintervention, or had evidence ofpathologic lead points or residualobstruction on imaging studies.Absolute criteria for admissionincluded 3 failed reduction attemptsby radiologist, family unable to returnto the ED if the patient had recurrentsymptoms, or the patient remainedsymptomatic in the ED after
successful reduction. Symptoms weredefined as vomiting, lethargy, pain,and intolerance of oral liquids.Relative criteria for admissionincluded fevers, bloody stools, andprolonged duration of symptomsbefore presentation (.12 hours).These criteria were printed ontolaminated, pocket-sized cards thatwere distributed to ED staff andsurgical house staff.
Standardization began with creationof a uniform radiology dictationtemplate and report that includedclinically relevant data points aboutthe enema reduction of theintussusception. Figure 2 showsa screen shot of the standardizedreport. The report was completed bythe radiologist who performed theenema reduction. The clinical dataelements of the template wereprovided in conversation with the EDprovider ordering the study or directinterview with the family. The reportsummary was intended to influencedisposition. The report delineatesseveral items from the history andclinical work-up such as the presenceof bloody stools and the duration ofsymptoms prior to presentation.Additional details such as themaximum pressure required forpneumatic air contrast enema
FIGURE 1Aim and key drivers diagram for instituting a QI project to increase the number intussusceptionpatients discharged from the ED at a high-volume pediatric center after successful air enemareduction. AVS, after visit summary.
e1346 RAVAL et al by guest on September 1, 2018www.aappublications.org/newsDownloaded from

reduction and the number ofreduction attempts are also reported.With input from radiology staff, it wasdecided that maximum insufflationpressure of 120 mm Hg for reductionas well as .2 attempts at reductionwithin the initial session were criteriafor admission. Of note, all air contrastenemas were performed by eitherattending radiologists or pediatricradiology fellows with attendingradiologist present at the table side.
There was also a concerted effort tostandardize postreductionmanagement in the ED. An agreementwas made with ED staff that a 3- to 4-hour postreduction observation
period would be the standard. Carewithin the ED was facilitated with anintussusception pathway order setthat enabled nurses to provide clearliquids and move patients alongrecovery postreduction. At the end ofthe observation period, if the ED staffdetermined the patient needed moretime for recovery, a surgicaladmission was indicated. Othervariables considered in the decision-making process for discharge fromthe ED included an assessment of thefamily’s ability to return to ED if thepatient had recurrent symptoms thatincluded emesis, pain, and failure totolerate liquids.
Any surgical, radiology, or ED staffmember could request surgicaladmission based on clinical judgmentrelated to relative criteria foradmission including fevers, bloodystools, and prolonged prodrome ofsymptoms before reduction. Thus,any ethical dilemma or concern overpatient safety defaulted to surgicaladmission. Furthermore, all patientswere evaluated by a pediatric surgicalattending or fellow before dischargehome from ED. Another educationaltool that was incorporated intopractice was an ED intussusceptiondischarge instruction brochuretailored to families for discharge fromthe ED. Patients who were dischargedfrom the ED received a follow-upphone call from an ED nurse the dayafter discharge to ensure safety andto answer questions.
Study of the Intervention
Data collection was performedprospectively, and quarterly reportswere provided to the entiremultidisciplinary team andhighlighted during ED and surgicaldivision meetings. Providers witha propensity to admit patients wereapproached regarding admissionpatterns and for further clarificationregarding grounds for admission andto provide clinical outcome follow-upfrom the admissions. Specificfeedback was provided to ED stafffrom the ED liaison on the project,and feedback was provided tosurgical staff by the rounding surgeonthe day after admission. Reasons thatprecluded consideration of dischargefrom the ED were collected. Forpatients deemed appropriatecandidates for discharge from the ED,the number actually discharged fromthe ED was reported back to projectteam members.
Analysis
An exact Cochran-Armitage test wasperformed to evaluate whether therewas a statistically significant trendover time in the proportion ofpatients meeting criteria for going
FIGURE 2Screenshot of a sample standardized radiologic report developed for air-enema reduction of in-tussusception demonstrating the level of detail provided for each patient.
PEDIATRICS Volume 136, number 5, November 2015 e1347 by guest on September 1, 2018www.aappublications.org/newsDownloaded from

home who in fact went home. Ageometric chart (g-chart) was usedto demonstrate rarely occurringevents while monitoring a processover time. Time spent in the ED wastracked for patients discharged andadmitted, and median times werecompared using Student’s t test.Financial projections on costsavings were determined usinga combination of local data andestimates from the publishedliterature.7 Local data includedcharges, direct and indirect costs,average payments, contributionmargin (difference between whatwas charged and patient care costs),and net margins (differencebetween patient care cost and whatthe hospital was paid). For allstatistical analyses a P value ,.05was considered significant. Thisproject was considered exemptfrom full internal review boardreview under the auspices of a QIproject.
RESULTS
Of the 80 patients with ileocolicintussusception between January 1,2013, and December 31, 2014, 34(42.5%) did not qualify for dischargehome. Table 1 shows the reasons forexclusion from consideration fordischarge from the ED. The most
common reasons included need forsurgical intervention (n = 9), need for.2 reduction attempts ora challenging reduction (n = 6),radiologic findings such as anedematous terminal ileum or possiblelead point on imaging (n = 5),hemodynamic instability requiringadditional intravenous hydration(n = 4), and travel distance to thehospital precluding prompt return ifneeded (n = 4). Other reasons forexclusion were history of bloodybowel movements (n = 2) andexceedingly young age of the patient(n = 1).
Of 46 patients who qualified fordischarge, 30 (65.2%) were senthome from the ED. Seven patientsreturned to the hospital with only1 having recurrent intussusceptionthat required repeat enema reduction.The other 6 returned to the hospital2 to 10 days postdischarge formanagement of their viral symptomswith no radiologic or surgicalinterventions. Of the 16 patientswho qualified for discharge but wereadmitted and then discharged within23 hours, none required furtherintervention, and 1 returned afterdischarge with no interventionsperformed. An exact Cochran-Armitage test for trend yieldeda P value of 0.004, indicating theproportion of patients meeting
criteria for going home who in factwent home increased significantlyover time (Fig 3). A geometric chart(g-chart) is used to demonstraterarely occurring events whilemonitoring a process over time.Figure 4 depicts a g-chart wherethe number of admissions betweendischarges from the ED is shownalong the y-axis. After the start ofthe project, there were 4 patientsadmitted before a patient wasdischarged. Thus the first datapoint graphed is a value of 5(meaning the fifth patient wasdischarged). This was followed byan admission and then anotherdischarge (thus the next pointgraphed was a 2 representing2 patients until the event ofdischarge was again encountered).This was followed by 2 admissionsand a discharge (thus the nextpoint graphed was a 3). Thispattern continued until August2014 when there was a string ofpatients discharged from the EDwithout an admission (thus a seriesof points graphed at 1, whichrepresents the baseline for thechart and reflects the desiredoutcome). Although time isrepresented on the x-axis, theaxis is not to scale.
Patients admitted from the ED hada median ED length of stay of 5.4hours compared with patients whowere discharged from the ED whohad a median ED length of stay of 6.8hours (P = .014). Thus, the dischargepractice resulted in ∼1.4 hours ofadditional ED occupancy per patientbut avoided an admission. Time ofday or day of the week was notassociated with admission patterns.Compared with patients dischargedfrom the ED, patients who wereadmitted had higher average charges($6066 vs $2937) and generatedhigher average payments ($3379 vs$1764) but incurred higher averagedirect costs ($1690 vs $666) andaverage indirect costs ($1588 vs$619). Thus, patients admitted fromthe ED had an average contribution
TABLE 1 Quarterly Breakdown of Details Regarding Intussusception Patients Who Were Excludedand Included for Consideration for Discharge Home From the ED from January 2013 toDecember 2014
2013 2014
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Number of patients deemed not to meet criteriafor going home
3 4 4 3 7 6 1 6
Operative intervention required 2 1 4 2Edema of terminal ileum or possible lead point
noted on imaging1 1 1 2
Required .2 attempts at reduction of difficultreduction
1 1 1 1 1 1
Bloody bowel movement 1 1Distance from hospital/family issues 2 2 2Hemodynamic instability requiring additional
resuscitation (eg, dehydration)3 1 1
Young age 1Number of patients who met criteria for going home 4 4 4 2 4 11 11 6Number of patients who actually went home 0 2 2 2 2 8 9 5
Q, quarter.
e1348 RAVAL et al by guest on September 1, 2018www.aappublications.org/newsDownloaded from

margin (difference between chargesand costs) of $1689 compared with$1098 for patients discharged fromthe ED. Ultimately, the average net
margin per patient (differencebetween costs and payment) was$101 for admission from the ED and$480 for discharge from the ED.
Using local average net marginfigures, the hospital made anadditional $11 370 by introducingthis QI project.
FIGURE 3Proportion of patients discharged from the ED to home who met criteria for discharge by quarter from January 2013 to December 2014.
FIGURE 4A geometric chart demonstrating the number of admissions between discharges from the ED from January 2013 to December 2014.
PEDIATRICS Volume 136, number 5, November 2015 e1349 by guest on September 1, 2018www.aappublications.org/newsDownloaded from

DISCUSSION
This multidisciplinary QI project todischarge intussusception patientsmeeting protocol criteria from the EDafter enema reduction wassuccessfully integrated into a high-volume pediatric referral center, withmore than half of eligible patientsbeing discharged from the ED. Resultsdemonstrated increasing staffparticipation over time with thepotential for reduced resourceutilization, significant cost savings,and improved patient satisfaction.
The success of this QI project wasfacilitated by the use of the Instituteof Healthcare Improvement (IHI)Model for Improvement, whichfocuses on design andimplementation.8 This model outlinesstrategies such as forming a team thatincludes a clinical leader, contentexperts, and those responsible for theday-to-day execution of the project.Under the leadership of our directorof surgical quality improvement,a multidisciplinary team wasassembled that also includedstakeholders from emergencymedicine and radiology. Nursepractitioners in the ED and from thesurgical service were involved invetting the patient informationbrochures. The day-to-day executionof the project was facilitated byclinical fellows on the pediatricsurgical service along with the on-callsurgical staff members. The IHI modelalso outlines the importance ofclearly setting aims that havea defined timeline and achievablegoal. The aim outlined in this projectwas determined after performinga retrospective analysis ofintussusception admissions over the2 years preceding project initiationand identifying the number ofpatients who would have mettheoretical grounds for dischargehome from the ED. The IHI modeloutlines selecting and implementingspecific interventions. In this project,the changes made to our systemincluded development of educational
brochures for patients and families,creation of a standardized radiologyreporting template for enemareductions, and standardization ofpostreduction care in the ED andpostdischarge.
The second component of successfulQI as described by the IHI modelinvolves implementation andmonitoring. We used a plan-do-study-act cycle to provide feedback tohealth care providers on a quarterlybasis.9 Once in place, the projectbenefitted from rapid feedbackbecause the first quarter ofimplementation had no patientsdischarged from the ED despiteextensive groundwork that was inplace before initiation. Staff fromsurgery and the ED were who weredirectly involved in the care ofpatients admitted to the hospitalwere queried as to the indications foradmission and for sources ofdisagreement with the protocol.Additional education and discussionresulted in improved compliance withthe project. Continuous QI is closelytied to behavioral change at theindividual level, which can befostered by close observation fortrends and consistent feedback.
Using these methods, 65% of patientswho met criteria for discharge fromthe ED were, in fact, discharged. Overtime, the proportion of patients beingdischarged from the hospitalincreased during the project in thesetting of a practice that historicallyadmitted all patients. Reservationwith discharging patients from the EDafter successful enema reductioncomes from the concern over missingearly recurrences. Timing ofintussusception recurrence can rangefrom hours to years, and reliablepredictors of recurrence havenot been identified.5,10,11 Themanagement of recurrentintussusception has been repeatenema reduction with excellentoutcome, even after multiplerecurrences. It remains a challenge toidentify patients at high risk for
recurrence. Previous reports havesuggested that duration ofsymptoms for .24 hours beforeevaluation may be a risk factor forrecurrence or need for surgicalintervention, but other studieschallenge this assumption.12,13
Regardless, return to the hospitalfor evaluation of recurrentintussusception typically occurspromptly with shorter duration ofsymptoms and fewer symptoms onevaluation for recurrences.13 Thismay be due to increased caregivervigilance and early recognition ofclinical symptoms. We found thatonly 1 of the 30 patients dischargedfrom the ED had recurrentintussusception, which wassuccessfully managed witha repeat air contrast enemafacilitated through the ED. Of the16 patients who met criteria fordischarge home from the ED butwere admitted for observation, 1developed recurrentintussusception and returned tothe system.
Similar results have beendemonstrated at several other majorchildren’s centers. Bajaj et al sharedresults of 78 children managed at theChildren’s Hospital of Colorado andfound that all intussusceptionrecurrences occurred after dischargefor both the 35% of patients admittedfor 23 hour admission and for the65% of patients discharged aftera 7-hour observation period.6 Acomparison of practice patterns at 2Canadian institutions demonstratedsimilar recurrence rates and numbersof patients ultimately requiringsurgical intervention betweenpatients admitted for observationand those discharged after successfulenema reduction.14 Chien et alreviewed a 7-year experience atPhoenix Children’s Hospitalencompassing 98 patients anddetermined that a 6-hour observationperiod was a safe alternative tomandatory admission for patientswith successfully reduced ileocolicintussusception.2 This study provides
e1350 RAVAL et al by guest on September 1, 2018www.aappublications.org/newsDownloaded from

a QI roadmap used at a centerinterested in emulating theseoutcomes to improve hospitalefficiency.
Cost reduction associated with QI andstandardized pathways and protocolshas been well demonstrated formany pediatric populations anddiseases.15,16 With intussusception,cost savings have been demonstratedat hospitals that have initiatedprotocols to discharge from theED. According to the HealthcareUtilization Project Kids’ InpatientDatabase, nearly 3600 patients wereadmitted for intussusception in theUnited States in 2012.17 Using theonline Healthcare Utilization Projectquery system, the median cost of anadmitted intussusception patient was$3719. Annual aggregate charges andcosts are estimated at $78 million and$24 million for these admissions.Using the Pediatric HealthInformation System, patients treatedat hospitals amenable to dischargefrom the ED demonstrated 41%lower median cumulative hospitalcosts compared with hospitals thatfavored admission ($1540,interquartile range: $881–$2524 vs$2612, interquartile range:$2013–$3735; P , .0001).7 Thesefigures include readmissionencounters. Data from this study andsubsequent work were used to createestimates for cost savings for our QIproject. The estimated cost savings of∼$1000 per patient for dischargefrom the ED compared withadmission used in this study isconsistent with data published fromFrance and Canada.14,18 Usingconservative costs estimates,discharge from the ED confers anestimated cost savings of $1072 perpatient, which translates to a costsavings of .$32 100 during thecourse of this project. If all eligiblepatients had been discharged fromthe ED, potential savings would haveexceeded $49 300. Even moreinteresting is the fact that localfinancials demonstrate a higher netmargin for patients discharged from
the ED as opposed to those admitted($480 for each patient dischargedvs $101 for each admitted). Thus,even though admitting a patientgenerates higher charges andpayments, overall cost-efficiencyimproved with discharge from theED, yielding better margins for thehospital.
Cultural obstacles were encounteredduring this process. Although almostall ED staff were supportive ofdischarge from the onset, severalsurgical attending staff witha tendency for admission during theinitial phases of the project slowlychanged their practice and favoreddischarge during the end of the 2-year period. One of the 15 surgicalattending staff members refused todischarge patients throughout theproject and accounted fora significant portion of admittedpatients who qualified for discharge.Education and data feedback thusfacilitated change for many but not allcare providers. Garnering widespreadadoption of optimal care pathwaysand QI efforts remains a criticalobstacle facing centers in the UnitedStates. Key lessons learned from thisproject were to keep the conversationat the forefront at division meetingsand to understand wherereservations and concerns are rooted.Despite a lack of uniform compliance,significant change was observed.
Implementing a standardizedprotocol and clearly identifying thegrounds for admission is the key tolearning more about intussusceptionand delineating the risk factors forrecurrence or risk factors indicatinga need for surgical intervention. Ourdata clearly demonstrate that somevariables serve as grounds foradmission that are difficult to alter,such as the ability of a patient toreturn to the ED if recurrentsymptoms develop. Other exclusionsmay be open to further investigation.For example, based on health careprovider preferences, we allowed forexclusion of patients from our
protocol that had specific clinicalfindings such as presentation withbloody bowel movements orprolonged symptom duration beforepresentation. Some studies havesuggested that duration of symptomsfor .24 hours before evaluation maybe a risk factor for recurrence orsurgical intervention, but otherstudies challenge thisassumption.12,13 Multicentercollaborative efforts are needed toelucidate the influence of thesevariables on outcomes and todetermine the nuances of optimalcare of patients with intussusception.Standardized data collection willfacilitate open discussion regardingcriteria for discharge, admission, andoperative intervention.
Limitations to this work include smallsample size and the limited durationof the QI project. Sustainability isa key hallmark of a successful QIproject, and entrenched practicepatterns are difficult to modify.Nonetheless, over time our successwith discharge of intussusceptionpatients from the ED improved from0% in the first quarter to a sustainedrate exceeding 70% in the last 3quarters. Another limitation is thegeneralizability of the QI project tohospitals that may have differentresources, size, and scope of care.Success was contingent on thecollaborative efforts of frontline careproviders from various disciplinesand included physicians, trainees, andnurses. This experience adds to thegrowing body of literature endorsingdischarge of successfully reducedintussusception patients from the EDand provides a guide to implementsimilar protocol and procedures.
CONCLUSIONS
For this QI project, we useda multidisciplinary team to identifyseveral key drivers of care formanagement of patients withintussusception. These includedprimary caregiver and health careprovider education, standardization
PEDIATRICS Volume 136, number 5, November 2015 e1351 by guest on September 1, 2018www.aappublications.org/newsDownloaded from
of radiology reports, postreductionobservation in the ED, andestablishing formal phone callfollow-up for patients. With theseinterventions, quarterly reports,and individualized feedback, wewere able to discharge the majorityof patients home from the ED. Theinterventions described in this
study may be informative to otherhospitals interested inimplementing similar qualityimprovement projects.Standardized care protocols anddata collection will allow forlarger multicenter collaborationsthat can evaluate the clinicalsignificance of a variety factors
that may influence treatment anddischarge decisions.
ABBREVIATIONS
ED: emergency departmentIHI: Institute of Healthcare
ImprovementQI: quality improvement
FINANCIAL DISCLOSURE: Dr Bates had been a consultant to OPTUMINsight (Healthcore Inc.) from 2007 to the present. The other authors have indicated they have no
financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: Dr Bates had been a consultant to OPTUMINsight (Healthcore Inc.) from 2007 to the present. The other authors have no potential
conflicts to disclose.
REFERENCES
1. Davis CF, McCabe AJ, Raine PA. The insand outs of intussusception: history andmanagement over the past fifty years. JPediatr Surg. 2003;38(suppl 7):60–64
2. Chien M, Willyerd FA, Mandeville K,Hostetler MA, Bulloch B. Management ofthe child after enema-reducedintussusception: hospital or home? JEmerg Med. 2013;44(1):53–57
3. Gilmore AW, Reed M, Tenenbein M.Management of childhoodintussusception after reduction byenema. Am J Emerg Med. 2011;29(9):1136–1140
4. Herwig K, Brenkert T, Losek JD. Enema-reduced intussusception management:is hospitalization necessary? PediatrEmerg Care. 2009;25(2):74–77
5. Al-Jazaeri A, Yazbeck S, Filiatrault D,Beaudin M, Emran M, Bütter A. Utility ofhospital admission after successfulenema reduction of ileocolicintussusception. J Pediatr Surg. 2006;41(5):1010–1013
6. Bajaj L, Roback MG. Postreductionmanagement of intussusception ina children’s hospital emergencydepartment. Pediatrics. 2003;112(6 pt 1):1302–1307
7. Rice-Townsend S, Chen C, Barnes JN,Rangel SJ. Variation in practice patterns
and resource utilization surroundingmanagement of intussusception atfreestanding children’s hospitals. JPediatr Surg. 2013;48(1):104–110
8. Institute for Healthcare Improvement.How to improve. Available at: http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx. Accessed August 20, 2014
9. Schriefer J, Leonard MS. Patient safetyand quality improvement: an overview ofQI. Pediatr Rev. 2012;33(8):353–359, quiz359–360
10. Niramis R, Watanatittan S, KruatrachueA, et al. Management of recurrentintussusception: nonoperative oroperative reduction? J Pediatr Surg.2010;45(11):2175–2180
11. Daneman A, Alton DJ, Lobo E, Gravett J,Kim P, Ein SH. Patterns of recurrence ofintussusception in children: a 17-yearreview. Pediatr Radiol. 1998;28(12):913–919
12. Chung JL, Kong MS, Lin JN, Wang KL, LouCC, Wong HF. Intussusception in infantsand children: risk factors leading tosurgical reduction. J Formos Med Assoc.1994;93(6):481–485
13. Champoux AN, Del Beccaro MA, Nazar-Stewart V. Recurrent intussusception.Risks and features. Arch Pediatr AdolescMed. 1994;148(5):474–478
14. Beres AL, Baird R, Fung E, Hsieh H, Abou-Khalil M, Ted Gerstle J. Comparativeoutcome analysis of the management ofpediatric intussusception with orwithout surgical admission. J PediatrSurg. 2014;49(5):750–752
15. Wazeka A, Valacer DJ, Cooper M, CaplanDW, DiMaio M. Impact of a pediatricasthma clinical pathway on hospital costand length of stay. Pediatr Pulmonol.2001;32(3):211–216
16. Slusher J, Bates CA, Johnson C, WilliamsC, Dasgupta R, von Allmen D.Standardization and improvement ofcare for pediatric patients withperforated appendicitis. J Pediatr Surg.2014;49(6):1020–1024, discussion1024–1025
17. HCUP Kids’ Inpatient Database (KID),Healthcare Cost and Utilization Project(HCUP). 1997, 2000, 2003, 2006, 2009, and2012. Rockville, MD: Agency forHealthcare Research and Quality.Available at: http://www.hcup-us.ahrq.gov/kidoverview.jsp. Accessed November4, 2014
18. Le Masne A, Lortat-Jacob S, Sayegh N,Sannier N, Brunelle F, Cheron G.Intussusception in infants and children:feasibility of ambulatory management.Eur J Pediatr. 1999;158(9):707–710
e1352 RAVAL et al by guest on September 1, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2014-3122 originally published online October 12, 2015; 2015;136;e1345Pediatrics
KenneyDietrich, D. Gregory Bates, Shawn J. Rangel, R. Lawrence Moss and Brian D. Mehul V. Raval, Peter C. Minneci, Katherine J. Deans, Kelli J. Kurtovic, Ann
Successful Enema ReductionImproving Quality and Efficiency for Intussusception Management After
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/136/5/e1345including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/136/5/e1345#BIBLThis article cites 16 articles, 2 of which you can access for free at:
Subspecialty Collections
subhttp://www.aappublications.org/cgi/collection/quality_improvement_Quality Improvements_subhttp://www.aappublications.org/cgi/collection/interdisciplinary_teamInterdisciplinary Teamse_management_subhttp://www.aappublications.org/cgi/collection/administration:practicAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on September 1, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2014-3122 originally published online October 12, 2015; 2015;136;e1345Pediatrics
KenneyDietrich, D. Gregory Bates, Shawn J. Rangel, R. Lawrence Moss and Brian D. Mehul V. Raval, Peter C. Minneci, Katherine J. Deans, Kelli J. Kurtovic, Ann
Successful Enema ReductionImproving Quality and Efficiency for Intussusception Management After
http://pediatrics.aappublications.org/content/136/5/e1345located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on September 1, 2018www.aappublications.org/newsDownloaded from