Improving Patient Flow by Managing Variability Eugene Litvak, PhD Program for Management of...
28
Improving Patient Flow by Managing Variability Eugene Litvak, PhD Program for Management of Variability In Health Care Delivery, Boston University 2 nd Annual Ellison Pierce Symposium Positioning Your ORs For The Future Boston University School of Medicine May 19, 2006 8:00-8:30am
-
date post
22-Dec-2015 -
Category
Documents
-
view
213 -
download
0
Transcript of Improving Patient Flow by Managing Variability Eugene Litvak, PhD Program for Management of...

Improving Patient Flow by Managing Variability
Improving Patient Flow by Managing Variability
Eugene Litvak, PhDProgram for Management of Variability
In Health Care Delivery, Boston University
Eugene Litvak, PhDProgram for Management of Variability
In Health Care Delivery, Boston University
2nd Annual Ellison Pierce Symposium Positioning Your ORs For The Future
Boston University School of Medicine
May 19, 2006
Boston University School of Medicine
May 19, 20068:00-8:30am8:00-8:30am

20%
10%
20%
20%
1 2 3 4
What do you think is the largest source of your hospital’s census variability? What do you think is the largest source of your hospital’s census variability?
1. the emergency room
2. the elective OR schedule
3. the ED and elective OR schedules impact is equal
4. No idea
1. the emergency room
2. the elective OR schedule
3. the ED and elective OR schedules impact is equal
4. No idea
QUESTION:QUESTION:

50%
30%
20%
1 2 3
Does your hospital try to smooth scheduled patient flow? Does your hospital try to smooth scheduled patient flow?
1. Yes
2. No
3. Don’t know
1. Yes
2. No
3. Don’t know
QUESTION:QUESTION:
Why should we smooth scheduled patient flow?
Can we afford not to smooth scheduled patient flow?
Why should we smooth scheduled patient flow?
Can we afford not to smooth scheduled patient flow?

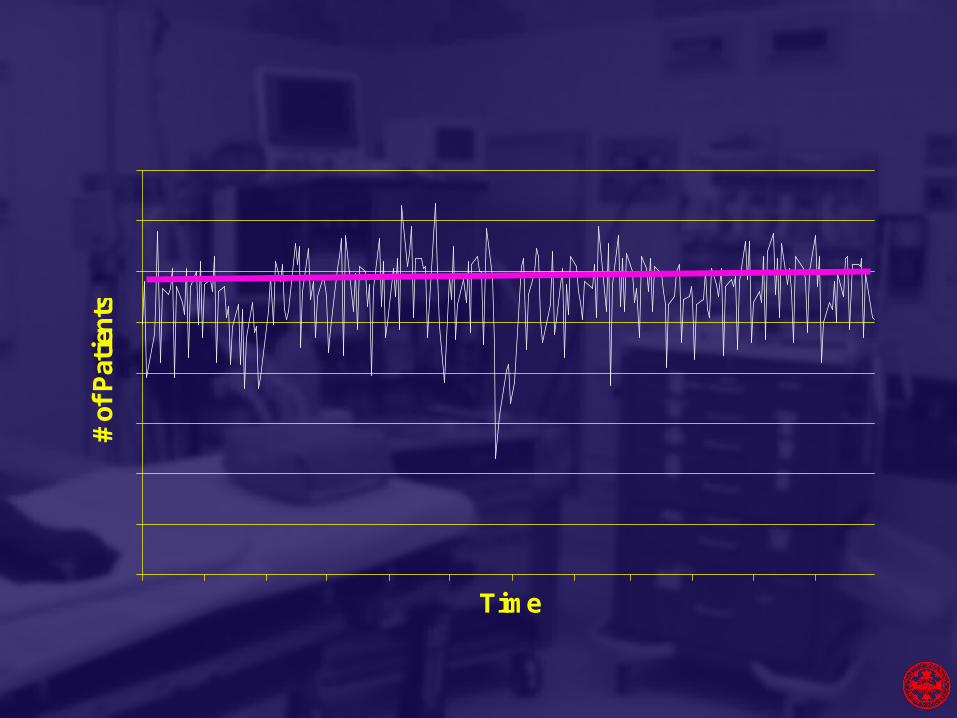
How unsmooth census looks like?How unsmooth census looks like?
Time
# of
Pat
ien
ts
Time
# of
Pat
ien
ts

Systemic Effects of Peak LoadsSystemic Effects of Peak Loads
• Internal Divert –Patients sent to alternative floors\Intensive Care locations
• Internal Delays – PACU backs up
• External Divert - ED divert
• Staff overload – medical errors and inability to retain staff
• System Gridlock – Increase in LOS
• Decreased throughput and revenue
• Internal Divert –Patients sent to alternative floors\Intensive Care locations
• Internal Delays – PACU backs up
• External Divert - ED divert
• Staff overload – medical errors and inability to retain staff
• System Gridlock – Increase in LOS
• Decreased throughput and revenue

Litvak E. & Long MC. Cost and Quality Under Managed Care: Irreconcilable Differences? American Journal of Managed Care, 2000; 6 (3): 305-312.
http://www.ajmc.com/files/articlefiles/AJMC2000MarLitvak305_312.pdf
Litvak E. "Optimizing patient flow by managing its variability". In Berman S. (ed.): Front Office to Front Line: Essential Issues for Health Care Leaders. Oakbrook Terrace, IL: Joint Commission Resources, 2005, pp. 91-111.

The Ideal Healthcare System (100% efficiency)
The Ideal Healthcare System (100% efficiency)
1. All patients have the same disease with the same severity.
2. All patients arrive at the same rate.
3. All providers (physicians, nurses) are equal in their ability to provide quality care.
1. All patients have the same disease with the same severity.
2. All patients arrive at the same rate.
3. All providers (physicians, nurses) are equal in their ability to provide quality care.
Variability as the source of system stress
Variability as the source of system stress
1. Clinical stress.
2. Patient flow stress.
3. Stress by variaton in proffesional abilities or teaching responsibilities.
1. Clinical stress.
2. Patient flow stress.
3. Stress by variaton in proffesional abilities or teaching responsibilities.

Natural Variability
Natural Variability
I) Clinical Variability
II) Flow Variability
III) Professional Variability
I) Clinical Variability
II) Flow Variability
III) Professional Variability
• Random• Can not be eliminated (or even
reduced)• Must be optimally managed
• Random• Can not be eliminated (or even
reduced)• Must be optimally managed
}
Why managing variability today is more important than
before?
Why managing variability today is more important than
before?

Designing and Testing Complex Mechanical Systems: Family CarDesigning and Testing Complex Mechanical Systems: Family Car
• Hitting a pothole vs. high speed impact against the wall
• Health care “financial bumper”
• Are the stresses an intrinsic part of health care delivery?
• Hitting a pothole vs. high speed impact against the wall
• Health care “financial bumper”
• Are the stresses an intrinsic part of health care delivery?
What makes hospital census variable?
What makes hospital census variable?
Time
# o
f P
ati
ents
-

• If ED cases are 50% of admissions
and…
• Elective-scheduled OR cases are 35% of admissions
then…
• Which would you expect to be the largest source of census variability?
• If ED cases are 50% of admissions
and…
• Elective-scheduled OR cases are 35% of admissions
then…
• Which would you expect to be the largest source of census variability?
What makes hospital census variable?
What makes hospital census variable?

The answer is…The answer is…
The ED and Elective-Scheduled OR have approximately equal effects on census variability.
Why?
Because of another (hidden) type of variability...
The ED and Elective-Scheduled OR have approximately equal effects on census variability.
Why?
Because of another (hidden) type of variability...

Artificial VariabilityArtificial Variability
• Non-random
• Non-predictable (driven by unknown individual priorities)
• Should not be managed, must be identified and eliminated
• Non-random
• Non-predictable (driven by unknown individual priorities)
• Should not be managed, must be identified and eliminated

Variability in the Census - Rising Volume
Variability in the Census - Rising Volume
Time
# of
Pat
ient
s -

Floors
ICU
ED
Variability and access to careVariability and access to care
Scheduled demand
Variability and Quality of Care*Variability and Quality of Care*
Inadequate numbers of nursing staff contribute to 24% of all sentinel events in hospitals. Inadequate orientation and in-service education of nursing staff are additional contributing factors in over 70% of sentinel events
Inadequate numbers of nursing staff contribute to 24% of all sentinel events in hospitals. Inadequate orientation and in-service education of nursing staff are additional contributing factors in over 70% of sentinel events
* Dennis S. O’Leary, JCAHO (personal communication)

Source: Carol Haraden, Ph.D., IHI

Variability and mortalityVariability and mortality
“Each additional patient per nurse was associated with a 7% increase in the likelihood of dying within 30 days of admission and a 7% increase in the odds of failure-to-rescue”*
* Linda H. Aiken, Sean P. Clarke, Douglas M. Sloane, Julie Sochalski, and Jeffrey H. Silber. Hospital Nurse Staffing and Patient Mortality, Nurse Burnout, and Job Dissatisfaction. JAMA, 2002; 288: 1987:1993
“Each additional patient per nurse was associated with a 7% increase in the likelihood of dying within 30 days of admission and a 7% increase in the odds of failure-to-rescue”*
* Linda H. Aiken, Sean P. Clarke, Douglas M. Sloane, Julie Sochalski, and Jeffrey H. Silber. Hospital Nurse Staffing and Patient Mortality, Nurse Burnout, and Job Dissatisfaction. JAMA, 2002; 288: 1987:1993
Litvak E, Buerhaus PI, Davidoff F, Long MC, McManus ML, Berwick DM. “Managing Unnecessary Variability in Patient Demand to Reduce Nursing Stress and Improve Patient Safety,” Joint Commission Journal on Quality and Patient Safety, 2005; 31(6): 330-338.

Example:Example:
Assumptions:
• 200 surgical beds
• average census for surgical beds 160
• staffing level 40 nurses (1 nurse per 4 patients)
• average residual from 160 patients census is 20% or 32 patients
• patients are distributed evenly between the nurses
How the mortality rate will change with 20% increase in surgical demand?
Assumptions:
• 200 surgical beds
• average census for surgical beds 160
• staffing level 40 nurses (1 nurse per 4 patients)
• average residual from 160 patients census is 20% or 32 patients
• patients are distributed evenly between the nurses
How the mortality rate will change with 20% increase in surgical demand?

Results:Results:
• 32 additional patients will be distributed evenly between 32 nurses: 1 additional patient per nurse or 4 + 1 = 5 patient per nurse
• these 32 nurses now will take care of 160 patients, whose mortality rate increases by 7%
• if these additional 32 patients will be distributed evenly between 16 nurses, then each such nurse will take care of 4 + 2 = 6 patients
• these 16 nurses now will take care of 96 patients, whose mortality rate increases by 14%
• 32 additional patients will be distributed evenly between 32 nurses: 1 additional patient per nurse or 4 + 1 = 5 patient per nurse
• these 32 nurses now will take care of 160 patients, whose mortality rate increases by 7%
• if these additional 32 patients will be distributed evenly between 16 nurses, then each such nurse will take care of 4 + 2 = 6 patients
• these 16 nurses now will take care of 96 patients, whose mortality rate increases by 14%
Root Cause Analysis of Emergency Department Crowding and Ambulance Diversion in Massachusetts,
Boston University, 2002: ED diversions study under Department of Public Health grant
http://www.mass.gov/dph/dhcq/pdfs/final_report_exec_summary.pdf
When the scheduled demand is significant, there was much stronger correlation between
scheduled admissions and diversions than between ED demand and diversions

Elective Surgical Requests vs Total Refusals
Elective Surgical Requests vs Total Refusals
0
1
2
3
4
5
6
7
8
9
10
elective surgical patients seeking ICU admission patients diverted or rejected from the ICU
Michael L. McManus, M.D., M.P.H.; Michael C. Long, M.D.; Abbot Cooper; James Mandell, M.D.; Donald M. Berwick, MD; Marcello Pagano, Ph.D.; Eugene Litvak, Ph.D. Impact of Variability in Surgical Caseload on Access to Intensive Care Services, Anesthesiology 2003; 98: 1491-1496.

Smoothing elective admissions:Success story
Smoothing elective admissions:Success story
Managing Patient Flow: A Focus on Critical Processes Managing Patient Flow: A Focus on Critical Processes
http://store.trihost.com/jcaho/product.asp?dept%5Fid=34&catalog%5Fitem=712http://store.trihost.com/jcaho/product.asp?dept%5Fid=34&catalog%5Fitem=712

St. John’s Hospital (OR) St. John’s Hospital (OR)
•Increased surgical annual case volume by 33% in the last three years.
•Increased personal surgical revenue by 4.6%
•OR overtime is record low 2.9%
•Reduced waiting time for available OR by 45%
•Dramatically improved OR nurse retention
•Increased ED throughput by ≈ 60% with no patient boarding
•Increased surgical annual case volume by 33% in the last three years.
•Increased personal surgical revenue by 4.6%
•OR overtime is record low 2.9%
•Reduced waiting time for available OR by 45%
•Dramatically improved OR nurse retention
•Increased ED throughput by ≈ 60% with no patient boarding