Improvement Studies in Emergency Department of Sporting Student Insurance Hospital
84
Improvement Studies in Emergency Department of Sporting Student Insurance Hospital Prepared by Dr. Gamal Essawy Dr. Sayed El-Taweel Dr. Amal El-Sharawy Dr. Nehal Yakout . Dr.Manal Saleh Dr. Ahmed Mustafa Dr. Aser Khamis Dr. Islam Galal
description
Improvement Studies in Emergency Department of Sporting Student Insurance Hospital. Prepared by Dr. Gamal Essawy Dr. Sayed El-Taweel Dr. Amal El-Sharawy Dr. Nehal Yakout . Dr.Manal Saleh Dr. Ahmed Mustafa Dr. Aser Khamis Dr. Islam Galal. content. Introduction Aim of this report - PowerPoint PPT Presentation
Transcript of Improvement Studies in Emergency Department of Sporting Student Insurance Hospital

Improvement Studies in Emergency Department of
Sporting Student Insurance Hospital
Prepared byDr. Gamal Essawy
Dr. Sayed El-TaweelDr. Amal El-Sharawy
Dr. Nehal Yakout .Dr.Manal Saleh
Dr. Ahmed MustafaDr. Aser KhamisDr. Islam Galal

content
Introduction Aim of this report Data collection &findings. SWOT analysis Evaluation of the current situation Conducting an improvement plan. Limitations Conclusions Future work

Introduction
History: Sporting student school hospital was opened in 1938, belonging to Jewish community, the hospital was nationalized in 1964 and it was conducted to HIO since 1994.


Introduction
Background: Sporting student school hospital is located In
Alexandria. It follow the Health Insurance organization, provides health care services for school students of Alexandria, and consider as a referral hospital for Kafr El-sheikh, and Behaira governorate in collaboration with Gamal Abdel Nasser hospital.

Introduction The hospital consists of three buildings: -outpatient’s clinic -emergency. -and inpatients area. The inpatients building consist of:• male-female surgical dept.• medical dept.• pediatric dept.• neonatal ICU.( new )• Pediatric ICU.• Haemdialysis unit.• orthopedic department.• 4 operation theaters

Introduction
The total hospital capacity beds are two hundred beds, with occupancy rate 70-75%.
Total hospital personnel is 500 .150 physicians, and 170 nurses.

Introduction
ER:
Consists of 8 beds, observation room, x-ray room, laboratory room, small waiting room.
ER service is available 24hours a day.
The waiting area accommodate for nearly about 20 persons. Usually 25 persons are waiting at a time.
the mean average waiting time 20 - 40 minutes. Till receiving the whole service.

Aim of this report
The aim of this project is to identify the state of current services in the ER and the evidence relating to patient satisfaction in emergency medicine, thereby providing useful information for clinicians, and helping to guide future strategies for assessment and improvement in this area.

Data collection & The Findings

Statistical data collected from ER (2009)
Number of patients seen in ER (2009))

TYPES OF CASES SEEN MONTHLY IN ER (2009)
Surgery
Orthopedic

Inpatients refereed from ER (2009)

16%
84%
COMPARISON BETWEEN PERCENTAGE OF MEDICAL AND SURGICAL CASES TREATED IN ER (2009)

SWOT ANALYSIS

Strengths
It a specialized hospital dedicated to a certain niche (school aged children) mostly all of specialties are offered by highly qualified trained doctors (specialists and consultants).

Strengths
New GM cooperative, with Quality education background and 20 years experience in the same hospital. [GROWING LEADERS IN YOUR OWN BACKYARD].

Strengths
The Hospital has a Vision and mission announced, written and distributed all over department’s walls.

Strengths
Analyzing the mission we found it was: highly credible, clear to understand, covering all important aspects of the hospital and it is service oriented.

Organized social services activities dealing with all the needy cases.
High Hospital average occupation rate 75%.
Adequate hospital infrastructures. Strong informal communication
channels among hospital departments.
Strengths

Separate building, easily accessible.
Emergency lab, X ray room available 24hours a day.
Nurses are well trained with long experience in ER.
Teamwork spirit among staff.
New ER building well designed, well equipped with good landscape is about to be opened in 3 months )still under construction).
(ER)Strengths





Weaknesses
Centralized decision making rendering the organization into a rigid form delaying important decisions .
No clear plan for staffing, recruitment, training and education of the Hospital staff.
More than 40% of hospital staff are clerks and administrative personnel.
Poor marketing system with minimal data and information about other competitors and their market share.

Customer service is only based upon social workers and social activities with No feed back about customer service and almost all of working staff got no training on communication skills.
No proper implementation of an Information Technology System ending into insufficient conducted statistical studies about the hospital health indicators.
Weaknesses

No implementation of a good quality system. )Current status has to be measured) though some steps has been taken in that long path.
Insufficient accountability regarding medical errors.
Unavailable of ideal standards that required protecting patient's confidentiality and privacy.
Weaknesses

ER building is not suitable, small area not adequate to actual demands, only one way for both entrance and exit, small waiting area with poor ventilation, no enough available rooms for every service needed )no isolation room- one examination room- no office for head of department), Bathrooms are located outside the ER building and also no alternative electric source to ER department.
(ER)
Weaknesses

Department has no clear mission, goals or objectives clear to the staff working in it.
Head of department is a part timer not dedicated to ER )ER manager overloaded with other technical job).
No specialized ER doctors
( ER)Weaknesses

Generally understaffing of hospital’s nurses including ER department.
No Job description available for any staff member in ER.
High turn over scale among ER doctors.
( ER)
Weaknesses

Performance appraisal system is not based on real indicators )activity, productivity, efficiency or effectiveness).
Lack of work innovations and creativity working atmospheres with weak incentives to ER doctors.
( ER)Weaknesses

No guidelines, organizational chart, Protocols, policies or procedures available to the working staff in their own working area.
Medical Records still needs to be much systematized, still multiple patient’s records for a single patient could be found.
no ER sheet for patients with clear plan ttt and discharge strategy .
( ER)
Weaknesses

National politically supported trend for development, improvement and expansion of health insurance.
Planning and implementing of a new Health insurance law.
Collaboration with Alexandria University in different fields such as research and training...etc.
Opportunities

highly qualified university professors contracted to perform operations in the hospital.
Opportunity to get involved in different educational programs provided by different health institutes
Opportunities

Threats

Threats
Centralized politically affected decision making, this renders decisions difficult to be made in time.
New legislations may lead to uncertainty of the expected effect.
New legislations will raise competition with private sector.

other well equipped university &private hospitals sharing the same specialties market.
High staff income in private hospital sector. Insufficient central funding resources. Lack
of external fund resources for development of nurses and other hospital employees.
Unpredicted unexpected diseases or disasters that need contingency plans to deal with e.g. swine flu…..
Threats

Evaluation of the current situation in ER

The methodology used was through:
Evaluation of the current process flow chart and its effect on service provision.
An analysis of the customer satisfaction state whether internal or external.
An analysis of the workload of nursing personnel.
An analysis of all the results of the previous sections.
Application of various prioritizing and decision making techniques to draw conclusions on main areas of improvement that can benefit from quality improvement efforts

Generate a process flow chart for the current state of
service provision in ER.

Patient Arrival Ambulance Arrival
Triage by Inspection
Is patient at Risk?
RegistrationNO
Waiting Area
Examination RoomPatient Triage
Yes
Is patient Diagnosed?
Investigations
Interpretation of results Yes
NO
Is patient severely ill?
Initial treatment NO
Out clinic follow-up
Is service available?
Admission
Yes
Yes
Referral
NO
ER Flow chart

Patient/customer satisfaction survey:
Methodology: Questionnaire.
Delivery: self completed.
Timing: During ED visits.
Respondent: Patient or accompanying person.
Sample: 100 patients' random samples.
Results:

0%
20%
40%
60%
80%
100%
Patint's satisfaction survey results
Satisfied 74% 66% 81.50% 37% 81% 73% 26.75% 37.75% 9.50%
Unsatisfied 26% 34% 18.50% 63% 19% 27% 73.25% 62.25% 91.50%
Overall
satisfaction
willingness
to return
Examinatio
nTriage Registration
Staff
attitude
Safety,scur
ity&sanitati
on
Waiting
area
Waiting
time

Main Findings:
important Factors are: )Waiting time, information, personnel attitude [care, courtesy, concern] and pleasant environment).
Doctor's manners and waiting times are the main cause of patient's satisfaction.

patient's dissatisfaction could be attributed to work overload in ER regarding nurses.
Significant process of care measures: triage status, significant problems )poor explanation of problem cause and test results, not informed when to resume normal activities or when to re-attend( are strong causes of patient's dissatisfaction, this could be attributed to work overload in ER regarding nurses.
Least satisfaction was noticed for the layout and infrastructures conditions of the waiting area )entrances, cleanliness, toilets availability e.g.)
Main Findings:

Only 37% of patients were satisfied with the triage area.
Least satisfaction was noticed for the layout and infrastructures conditions of the waiting area )entrances, cleanliness, toilets availability e.g.)

This work reveals three interventions worthy of further study are:
Improving interpersonal. Attitudinal and communicational skills in ED staff. Short training courses maybe highly effective in this regard.
Provision of more information and explanation.
More reduction of the perceived waiting time.

Methodology: Questionnaire.
Delivery: self completed.
Timing: During working hours.
Respondent: all types of ED staff (doctors, nurses, clerks, security personnel).
Sample: 30 patients' random samples.
Employee satisfaction survey:

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Satisfied 30% 17.20% 66% 81% 38.75%
Unsatisfied 70% 82.80% 34% 19% 61.25%
Work overloadQuality
implemtationJob Satisfaction Communication
Infra structure&layout
convenience
EMPLOYEE SATISFACTION SURVEY RESULTS

Most of employees are satisfied with their jobs despite of the work overload and the low financial benefits.
Lack of suitable environment and convenient layout of the department caused great deal of the staff dissatisfaction.
Main Findings:

Communication channels seem to be working well. The amazing issue was the unavailability of ED flow
chart, error reporting system, any guidelines or Sop's regarding ED, however job duties were fully known and workers complaints were strictly handled. As a whole, though a documented quality system in not well implemented, yet an informal system is in place that monitors the performance of the unit which can be built upon for improvement efforts.

Service target method ( Regarding ER Nurses)

The daily nurse tasks; Registration=2minutes/patient. Triage=2minutes/patient. Vital signs=5minutes/patient. Doctors assistance in
examination=7minutes/patient. Treatment execution=5minutes/patient. Monitoring & observation=3minutes/patient. After care =1minute/patient. Other duties=5minutes/patient.

Nurse working time
60minutes×6hours×6days×48weeks= 103680minutes/year.
Expected ER patients
180p/d×365day=65700patient/year.

The standard working load for each task Registration=103680/2=51840. Triage=103680/2=51840. Vital signs=103680/5=20736. Doctors assistance in
examination=103680/7=14811. Treatment execution=103680/5=20736. Monitoring & observation=103680/3=34560. After care=103680/1=103680. Other duties=103680/5=20736.

Number of nurses needed for each task / year=Expected patients/year ÷Standard working load Registration=65700/51840=1.26 Triage=65700/51840=1.26 Vital signs=65700/20736=3.16 Doctors assistance in examination=65700/14811=4.4 Treatment execution=65700/20736=3.16 Monitoring & observation=65700/34560=1.9 After care=65700/103680=0.6 Other duties)=65700/20736=3.16

Number of nurses needed /day
=1.26+1.26+3.16+4.4+3.16+1.9+0.6+3.16=19 nurses/day
N.B.: The actual nurses’ number in ER is 11nurses

Conducting an improvement plan

Brainstorming (to identify our targeted problems to improve)
1) Unsuitable layout and infrastructures conditions of the waiting area (entrances, cleanliness, toilets availability e.g.)
2) Lack of a well activated organ gram with a clear job description to all staff members.
3) No clear plan for staffing, recruitment, training and education of the Hospital staff.
4) Poor marketing system with minimal data and information about other competitors and their market share.
5) Poor customer service system 6) Communication skills should be increased to all staff members 7) No proper information system technology 8) No specialized ER doctor 9) No job description available 10) No innovation environment 11) High turn over among staff

12) Medical Recording system needs to be much supported. 13) Nurse shortage (numbers) 14) Shortage in quality improvement programs 15) Lack of information and explanations provided to patients. 16) Non suitable perceived waiting time. 17) Incentives and performance appraisal is not based on real indicators
(activity, productivity, efficiency or effectiveness). 18) No Clinical guidelines, protocols, policies &procedures available at ER. 19) Flexible Organ gram should be formulated. 20) Head of ER not fully dedicated to his work and needs to have a clear job
description and to be trained on his managerial duties. 21) ER should have Mission, Vision and strategies (this should be done through
complete collaboration between ER staff members). 22) Suitable environment should be considered (e.g. air-conditioning,
cleanliness, toilets availability, good furniture……)

Ishikawa (Cause &Effect) diagram:
ER Improvement
Staffing LayoutCommunication
& Training
Marketing Quality Implantation
IT management
•Lean training•Install a sign leading patients to triage.•Ensure that the profile of triage nurse is “most experienced”
•Change layout to support continuous flow•Larger area for triage•Improved physical space design•Entrance management into ED
•Plan for staffing recruitment,•Having two triage nurses at all times, instead of two clerks•Reduce charge nurse non-essential duties.
•Electronic display for updates e.g. •Wait announcements etc.•Re-consider the amount of info at
triage.
•Implement Standard Work•Quality system is needed•Error system
•Marketing plan.•Bench marketing.•Search about market share.

which problems should we
direct first?

Poly votingPROBLEMSVOTING RANKING
1 )Unsuitable layout and infrastructures conditions of the waiting area (entrances, cleanliness, toilets availability e.g.)
0
2 )Lack of a well activated organ gram with a clear job description to all staff members.
1
3 )No clear plan for staffing, recruitment, training and education of the Hospital staff
34
4 )Poor marketing system with minimal data and information about other competitors and their market share.
0

5 )Poor customer service system1
6 )Communication skills should be increased to all staff members
1
7 )No proper information system technology52
8 )No specialized ER doctor0
9 )No job description available1
10 )No innovation environment0

11 )High turn over among staff0
12 )Medical Recording system needs to be much supported
0
13 )Nurse shortage (numbers)61
14 )Shortage in quality improvement programs43
15 (No Clinical guidelines, protocols, policies &procedures available at ER
0

16 (Flexible Organogram should be formulated.0
17 (ER should have Mission, Vision and strategies (this should be done through complete collaboration between ER staff members).
0
18 (Suitable environment should be considered (e.g. air-conditioning, cleanliness, toilets availability, good furniture……)
0
19 (Head of ER not fully dedicated to his work and needs to have a clear job description and to be trained on his managerial duties.
0

20 (Incentives and performance appraisal is not based on real indicators (activity, productivity, efficiency or effectiveness).
0
21 )Lack of information and explanations provided to patients.
0
22 )Non suitable perceived waiting time25
N.B.: The unsuitable layout was least voted upon in this project since this problem will
be resolved by the new ER building which is under construction.

Priority Matrix (to prioritize our problems)PROBLEMS IMPORTANCE FEASABILITY FREQUENCY TOTAL RANKING
17870762241
26545651755
37451671923
46254611774
57562702072

Result:
Top 2 ranked problems to start with are:
Nurse shortage. Long perceived waiting time.

Action Plan for solving the nurse shortage problem
Task Responsible person
Due date
1 -Separate the work elements that can exclusively be carried out only by nurses, assuring that they have more time to carry out their essential (value adding) duties. (new job descriptions to be formulated)
ER head nurse
1 MONTH
2 -Standardize (to the degree possible) the tasks of the charge nurse (SOP'S)
ER head nurse
6 MONTHS
3 -Use flexible staffing to respond to patient surge (physician/triage/clerking) (new staffing and recruitment should be applied).
GM1 YEAR

4 -Carry out registration and triage simultaneously, where possible (new procedure should be added at registration level).
ER head nurse1 MONTH
5 -Paramedical may take a role at different stations in ER process of work (e.g. triage, resuscitation room……)
ER MANAGER6 MONTHS
6-Reduce clerical work at triage.ER HEAD NURSE
1 MONTHS

7 -Applying skill mix could eliminate some current tasks to be done by nurse's assistant.
HOSPITAL HEAD NURSE
1 MONTH
8 -Extra incentives for ER staff based on a performance appraisal system are not guided by real indicators (activity, productivity, efficiency or effectiveness).
GM1 MONTH
9 -Annual staffing & recruitment plans (nurses) based on actual studied for hospital needs.
GM1 YEAR

Action Plan for solving the unsuitable perceived waiting time problem:
Task Responsible person
Due date
1 -Provide more signs/maps guiding patients (explaining wait time situation) to save triage nurse time.
ER manager2 MONTHS
2 -Install a visual board (electronic display) to make waiting room announcements
ER manager3 MONTHS
3 -Redesign perimeter of triage and registration desks (glass window around them dampens the sound and hampers communication).
ER manager3 MONTHS

4 -Ensure that the profile of triage nurse is “most experienced” in her role, where
assessment is made .
ER manager1 MONTHS
5 -Re-consider the amount of info at triageER manager1 MONTH
6 -Re-design the flow to avoid traveling and over processing.
ER manager1 MONTH
7- Categorize ER patients according to the severity level of their medical condition. Patients are assigned a triage number of 1 to 5 (1 being most emergent, and 5 being the least) when they report to the triage nurse.
ER manager2 MONTH

8- Introduce demand-dependent mini-triage.ER head nurse
1 MONTH
9-No tools in the world can provide sustainability without a change in the culture, mindset and behaviors of the personnel. Provide training and informative lectures
aiming to obtain that result (
GM 6 MONTHS
10-Provide pleasant environment in the waiting area.
ER manager3 MONTHS

Limitations
Although a lot of effort was invested in this study of Hospital Emergency Department, limitations attributable to multiple factors exist due to:
Limited time span of the study. Limited availability of resources. Limited scope of the study: issues related to cultural,
mindset and behavioral change were not covered. The project did not consider any financial implications or
commitments from the hospital management.

CONCLUSIONS

Complex TechnologyLAB, CT, MRI
IncreasedProcessing
Time
Complex Work-upsUnfamiliar PatientsUnknown Problems
Need for Specialists
FewerPhysicians
FewerHospitals
DecreasedCapacity
Fewer nurses
FewerED’s
Variability
ER OverloadER OverloadIncreasedDemand
PopulationNumber
PopulationAge
PopulationDistribution
Changing PreferencesFor ED care
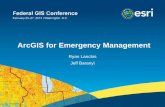
Chart explaining ER overload problems

one of the key challenges to health care access in hospitals is the growing overcrowding of the Emergency Departments (ERs), leading to the medical personnel overload, and the excessive waiting times to receive proper care .
These adverse effects directly impact the patient satisfaction levels, the ability of the medical professionals to attend promptly to patients’ health issues, and generate unnecessary costs .
Addressing the sources of waste and improving the process provides better care and higher patient satisfaction, as well as increases operational efficiency and the ability of the medical professionals to intervene on time.

FUTURE WORK
No tools in the world can provide sustainability without a change in the culture, mindset and behaviors of the personnel. Unlike machines and processes that can be changed and improved relatively quickly, changing outlooks and mindsets takes plenty of time and skill

,We would like to express our appreciation to hospital staff and in particularDr. Ayman Morsy ,the General Manager
,for his great support, helps in collecting the data numerous discussions, and guidance throughout the
work . We also extend our thanks to.Dr Khaled Abul Ela for his
cooperation .
Special thanks to our supervisorProf. Dr. Moshira RatebProf. Dr. Moshira Rateb for her assistance, stimulation, guidance and empowering
throughout the whole process of the work.
We would like to express our appreciation to hospital staff, and in particular Dr. Ayman Morsy the General Manager, for his great support, helps in collecting the data, numerous discussions, and guidance throughout the
work . We also extend our thanks to Dr. Khaled Abul Ela for his
cooperation .
Special thanks to our supervisor Prof. Dr. Moshira RatebProf. Dr. Moshira Rateb for her assistance, stimulation, guidance and empowering throughout the whole process of the work.

Special thanks to our
Prof., Dr. Said RatebProf., Dr. Said Rateb MD, FRCS,
The spirit father of healthcare management program for his great effort and ideas for this program to see light and his kindly teaching course and arrangement of the whole program.