IMPLICATIONS FOR THE USE OF POSTURAL ANALYSIS AS A ... · lower extremities. Such movements would...
8
IMPLICATIONS FOR THE USE OF POSTURAL ANALYSIS AS A CLINICAL DIAGNOSTIC TOOL: RELIABILITY OF QUANTIFYING UPRIGHT STANDING SPINAL POSTURES FROM PHOTOGRAPHIC IMAGES Nadine M. Dunk, BSc;' Jennifer Lalonde, BSc,'' and Jack P. Callaghan, PhD' ABSTRACT Objectives: A repeated measures design was used to test the reliability of standing spine postures within subjects using a biologically relevant measure determined by digitization of images and to compare the results to a previously tested vertical reference method. Methods: Twenty subjects attended 3 sessions consisting of 5 trials each. Photographs of the sagittal and posterior views of normal upright standing were taken. Landmarks were digitized and cervieal, thoracic, and lumbar spinal angles were calculated using the algebraic dot product, lntraclass correlation coefficients were used to evaluate intrasubject reliability across sessions. Results: According to the intraelass correlation coefficients, posture had good to excellent reliability in the sagittal view and provided a more stable measure of spinal angles than the posterior view. Mean repositioning erTors were less than 6 and 2 in the sagittal and posterior views, respectively. Conclusions: Although the repeatability of posture was improved in the sagittal view, when a biologic measure was used instead of an external vertieal reference to calculate spinal angles, individual subject posture was still variable. This brings into question the effectiveness and validity of using surface skin markers to track postural changes due to clinical interventions. If the postural analysis approach is to be used lo detect changes due to clinical treatment, such ehanges must be larger than the baseline repositioning errors seen in healthy subjects. (J Manipulative Physiol Ther 2005;28:3X6-392) Key Indexing Terms: Spine: Posture; Back Pain: RcUahiiity: Digitization T he use of upright standing posture as a diagnostic approach has been implemented to aid in clinical treatment. The use of posture to assess the need for treatment has the underlying requirement that it is a repeat- •' PhD Candidate. Department of Kinesiology. Faculty of Applied Health Sciences, University of Waterloo. Waterloo. Ontario. Canada N2L 3GI. ''Department of Kinesiology, Faculty of Applied Health Sciences. University of Waterloo. Waterloo. Ontario. Canada N2L 3G1. *• Associate Professor, Department of Kinesiology, Faeulty of Applied Health Sciences, University of Waterloo. Waterloo, Ontario. Canada N2L 3Cil. Sources of support: This suidy was funded by the Natural Sciences and Engineering Research Council of Canada (NSERC). Submit requests for reprints to: Jaek P. Callaghan, PhD. Department of Kinesiology, Faculty of Applied Health Sciences, University of Waterloo, Waterloo, Ontario, Canada N2L 3G1 (e-mail: callaghaUvitwatiTloo.ca). Paper submitted January 27, 2004; in revised fonii March 15, 2005. 0l6l-4754/$30.00 Copyright a 2005 by National University of Health Sciences. doi: 10.1016/j.Jmpt.2005.06.006 386 able measure (ie. if asses.sments are done on different days, the same conclusion will be reached). It is also necessary that posture is con.sistent to be sensitive enough to detect systematic changes due to treatment or other influencing events. Furthermore, a fundatnental assumption has to be made—that standing postural misalignments are associated with the presence of cervical, thoracic, or lumbar pain or disease, a fmding not well supported by the literature.'"'' Several companies (eg. Biotonix, PosturePro, and Chi- roVision) have developed computerized postural analysis systems used to guide clinical treattnents and exercise programs in the treatment of conditions such as low back pain. The approach involves digitizitig an image of a client's relaxed upright standing posture and calculating various spinal angles in the anterior, posterior, and sagittal views as deviations from a vertical reference. A recent study"" examined the ability of this method to provide a stable measure of an individual's posture. Consistently large coefficients of variance (CV) and low intraelass correlation coefficients (ICC) reflected the poor repeatability of externally referenced postures within a day and between days. This brings into question the benefit and validity of using this approach as a clinical diagnostic tool.
Transcript of IMPLICATIONS FOR THE USE OF POSTURAL ANALYSIS AS A ... · lower extremities. Such movements would...

IMPLICATIONS FOR THE USE OF POSTURAL ANALYSIS AS A
CLINICAL DIAGNOSTIC TOOL: RELIABILITY OF
QUANTIFYING UPRIGHT STANDING SPINAL POSTURES
FROM PHOTOGRAPHIC IMAGES
Nadine M. Dunk, BSc;' Jennifer Lalonde, BSc,'' and Jack P. Callaghan, PhD'
ABSTRACT
Objectives: A repeated measures design was used to test the reliability of standing spine postures within subjects usinga biologically relevant measure determined by digitization of images and to compare the results to a previously testedvertical reference method.
Methods: Twenty subjects attended 3 sessions consisting of 5 trials each. Photographs of the sagittal and posteriorviews of normal upright standing were taken. Landmarks were digitized and cervieal, thoracic, and lumbar spinal angleswere calculated using the algebraic dot product, lntraclass correlation coefficients were used to evaluate intrasubjectreliability across sessions.
Results: According to the intraelass correlation coefficients, posture had good to excellent reliability in the sagittal viewand provided a more stable measure of spinal angles than the posterior view. Mean repositioning erTors were less than 6and 2 in the sagittal and posterior views, respectively.
Conclusions: Although the repeatability of posture was improved in the sagittal view, when a biologic measure wasused instead of an external vertieal reference to calculate spinal angles, individual subject posture was still variable. Thisbrings into question the effectiveness and validity of using surface skin markers to track postural changes due to clinicalinterventions. If the postural analysis approach is to be used lo detect changes due to clinical treatment, such ehanges mustbe larger than the baseline repositioning errors seen in healthy subjects. (J Manipulative Physiol Ther 2005;28:3X6-392)Key Indexing Terms: Spine: Posture; Back Pain: RcUahiiity: Digitization
T he use of upright standing posture as a diagnosticapproach has been implemented to aid in clinicaltreatment. The use of posture to assess the need for
treatment has the underlying requirement that it is a repeat-
•' PhD Candidate. Department of Kinesiology. Faculty ofApplied Health Sciences, University of Waterloo. Waterloo.Ontario. Canada N2L 3GI.
''Department of Kinesiology, Faculty of Applied HealthSciences. University of Waterloo. Waterloo. Ontario. CanadaN2L 3G1.
*• Associate Professor, Department of Kinesiology, Faeulty ofApplied Health Sciences, University of Waterloo. Waterloo,Ontario. Canada N2L 3Cil.
Sources of support: This suidy was funded by the NaturalSciences and Engineering Research Council of Canada (NSERC).
Submit requests for reprints to: Jaek P. Callaghan, PhD.Department of Kinesiology, Faculty of Applied Health Sciences,University of Waterloo, Waterloo, Ontario, Canada N2L 3G1(e-mail: callaghaUvitwatiTloo.ca).
Paper submitted January 27, 2004; in revised fonii March 15,2005.
0l6l-4754/$30.00Copyright a 2005 by National University of Health Sciences.doi: 10.1016/j.Jmpt.2005.06.006
386
able measure (ie. if asses.sments are done on different days,the same conclusion will be reached). It is also necessary thatposture is con.sistent to be sensitive enough to detectsystematic changes due to treatment or other influencingevents. Furthermore, a fundatnental assumption has to bemade—that standing postural misalignments are associatedwith the presence of cervical, thoracic, or lumbar pain ordisease, a fmding not well supported by the literature.'"''
Several companies (eg. Biotonix, PosturePro, and Chi-roVision) have developed computerized postural analysissystems used to guide clinical treattnents and exerciseprograms in the treatment of conditions such as low backpain. The approach involves digitizitig an image of a client'srelaxed upright standing posture and calculating variousspinal angles in the anterior, posterior, and sagittal views asdeviations from a vertical reference. A recent study""examined the ability of this method to provide a stablemeasure of an individual's posture. Consistently largecoefficients of variance (CV) and low intraelass correlationcoefficients (ICC) reflected the poor repeatability ofexternally referenced postures within a day and betweendays. This brings into question the benefit and validity ofusing this approach as a clinical diagnostic tool.

Journal of Manipulative and Physitilugleal TherapeuticsVolume 28. NumbcT 6
Dunk et alReliability and Posture Analysis
387
Measuring spinal angles with respect to a verticalreference may be susceptible to error from balance controlmovements such as postural sway and lateral shifting in thelower extremities. Such movements would alter the spinaldeviations calculated with no change in spine curvature.Furthermore, this method could be susceptible to reposi-tioning errors caused by a slight alteration of camera orsubject position. Thus, we were driven to use a biologicallyrelevant measure of spinal angles to examine an individual'sability to reliably assume the same relaxed upright postureon different occasions.
Several studies have examined the repeatability of spinalpostures using various methods, such as spinal pantographs,clinometers,^ a rastersterograph imaging system,'" and asitnple plumbline technique." These studies have usedbiologically relevant methods of detennining spinal anglesand have suggested acceptable reproducibility of normalrelaxed upright standing posture. Spinal position sense'"' andlumbosacral repositioning'"^ have also been documented withsimilar eonelusions that posture is reasonably reproducible.Gilleard et al'** used a motion analysis system and markers onthe head, thorax, and pelvis to investigate the repeatability ofpostural alignment over a period of 32 weeks. Using ICCcoefficients, they documented poor repeatability for thecervicothoracic spine {ICC = 0.376) and good repeatabilityfor the thoracolumbar spine (ICC ^ 0.636).
The purpose of this study was to determine the reliabilityof posture within subjects using a biologically relevantmeasure of spinal angles determined by digitization ofimages in the sagittal and posterior views. A secondarypurpose was to assess the relative improvement of thecurrent biologically relevant method over the previousvertical reference method to provide a stable measure ofspinal angles. Furthermore, repositioning errors wereexamined to determine the baseline variability of uprightstanding that would need to be exceeded to detect anychanges due to clinical intervention.
METHODS
SubjectsTwenty healthy young adults were recruited from a
university student population. There were 10 women (age,21.8 ± 0.6 years; height, 163.6 ± 6.8 cm; mass, 57.5 ±8.5 kg) and 10 men (age, 22.6 + 1.3 years; height, 179.1 ±3.3 cm; mass, 76.7 ± 5.1 kg). All subjeets were screened toensure the absence of any activity-limiting events of lowback pain during the previous 12 months. Subjects gaveinfonned consent to the protocol, which had receivedapproval from the University Office of Research.
Study ProtocolParticipants were required to attend 3 individual sessions,
each consisting of 5 trials of 2 views (sagittal and posterior)
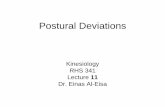
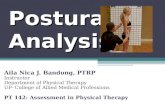
Fig I. Images were taken of each subject in the sagittal (A) andposterior (B) views. Digitized landmarks are seen as white dotsconnected to produce vectors. Angles between the vectorsrepresent the cerxical (I), thoracic (2). and lumbar (3) anglesand were calculated itsing the algebraic dot product.
of upright standing posture. Beeause there were no differ-ences observed between the repeatability of angles meas-ured in the posterior and anterior views in a previous study.the anterior view was eliminated from this study. The firstand second sessions were conducted in the moming andafternoon of the same day. with the third session in themoming 1 week later. Subjects were instructed to stand in arelaxed upright posture on a sheet of paper so that their feetin both views could be traced. This was to ensure that thesame foot position was achieved upon retesting to eliminateany errors induced by camera/subject alignment changes.
Five photographs of both the sagittal (right side) andposterior views (Fig lA and B) were taken with a2-megapixel digital camera (PowerShot SI00 digital cam-era. Canon. Lake Success. NY) with a resolution of 640 x480 in each session. The view trials were randomized foreaeh session to ensure that order was not a factor. After eachtrial, participants were asked to walk around freely withinthe testing area and then reposition themselves on thepretraced feet in a relaxed upright posture. The camera wasfixed on a tripod 172 cm from the participant andmaintained at a height specific to each participant so thathis or her entire spine length was in view. A level was usedto maintain camera position between sessions.
Reflective tin markers, which were visible in the sagittalview, were attached to each participant by a headband (torepresent CI) and to the skin at the level of Tl, T12, and SI.Each fin consisted of two retleetive markers placed 6 cmapart. Single refleetive markers visible in the posterior viewwere taped 5 cm on either side of the fin on the headband, tothe skin 13 cin on either side of the Tl fin, and 10 cm oneither side of the fins located at T12 and SI (Fig I).
Digitization of images and calculation of angles wereperformed using customized software (GOBER, University

3S8 ["-'''"'̂ '̂ i aiy and Posturt Analysis
Journal of Manipulative and Physiological TTier3peutlcsJuly/August 2005
Table I. Mean values ami SDs (degrees/ collapsed across all trials for each an^ie in each view
Angle
fcrvicai
Thoracic
Lumbar
Session
I
231231T
••>
Women
28.49(11.90)
31.04(14.05)32.74 (9.05)
-37.30 (6.69)-37.65 (5.39)-34.95 (6.39)
34.60(5.77)31.30 (5.5X)
34.02(8.12)
Sagittal
Men
33.34(12.13)
34.35 (8.78)35.63 (6,70)
-38.23 (6.62)-36.96(6.10)-38,23 (6.29)
27.59 (9.56)29.43 (9.21)26.06(10.32)
Women
0.45 (2.06)
0.51 (2.16)0.80(1.52)
-1.60(1.35)-1.87(1.17)-1.37(1,02)-0.62 (1.23)-0.32(1-63)-O . i l (0.94)
l\istcrior
Men
0.78(1.57)
0.82(1.39)1,24(1.76)
-1.53 (0.84)-1.31 (0.92)-1.86(1.06)-0.93(1.26)-1.56(1.05)-0.37(1.38)
B
Sagittal Cervical Sagittai Sagittal LumbarThoracic
View and Spinal Segment
1,5
1
0,5
0
-0.5-
' -1
-1,5
-2
-2,5PosteriorCervical
i
Posterior Posterior LumbarThoracic
View and Spinal Segment
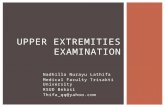
Fig 2. Mean spinal angles am! SDs for the .sagittal (A) and the poslerior (B) views within each ofthe 3 sessions for one subject.
of Walerloo, Waterloo. Ontario). The following markerswere digitized: sagittal view, proximal, and distal reflectivemarkers on the fins located on the headband, Tl. T12. andSI (Fig IA); posterior view, right, and left reflectivemarkers located on either side of the tins (Fig IB). Themarker coordinates were used to create vectors (Fig 1) andthe angle between the veetors was calculated using thealgebraic dot product to yield eervieal, thoracic, and lumbarflexion and lateral bend angles for a total of 6 angles.
Repositioning errors were determined for eaeh subjectwithin and across sessions. Within-session repositioningerrors were ealeulated as the difference in magnitude olanglebetween all eombinations of pairs of trials within a givensession, leading tu a total of 10 repositioning errors for eaehsession. For example, for a given subject in a given session,differences were found between the angle in trial 1 and thosein trial 2. 3, 4, and 5, then trial 2 and 3. 4 and 5, and so onuntil 10 repositioning errors had been calculated. Between-session errors were detennincd in a similar manner, as allcombinations of pairs of trials across any two sessions.
Statistical AnalysisThree-way analyses of variance (ANOVA) (dependent
variable = sex x trial x session; u = .05) with repeatedmeasures on 2 factors (trial and session) were performed foreach spinal angle in both views to examine any ditlereneesin angle. To evaluate intrasubject reliability across sessions,ICCs (2.1)'^ were eaiculated for each of the 3 angles in bothviews. To examine marker placement as a source ofvariability. ICCs were also calculated for each session forall 3 angles in both views. Coefficients of variance (CV)were calculated across sessions to examine individualsubjeet variability over the entire testing period.
RESULTS
Results from the ANOVA revealed no significant effectsof sex or session on all 3 angles in both the sagittal andposterior views (Table 1). There were no significant trialeffects for all 3 angles in both views, with the exception of

Journal of Manipulative and Physiological TherapeuticsVolume 28. Number 6
Dunk el alReliability and Posture Analysis
389
Table 2. Coefficients
FlF2F3F4F5F6F7F8F9FIOAverageMlM2M3M4M5M6M7M8M9MIOAverage
of variation
Cet^ical
5,4613,8518,629,094.906.74
36,8652,7311.3714.4417.416,50
23,9233.92
8.646.23
14,7317,8213.3711,707,87
14,47
(%) of the angles
Sagittal
Thoracic
6.4716.2410,078.895.097.058.177.14
14.5317.5910.136.177.06
10.618.957.195.369.70
13.189.107.838.52
across .sessions for each
Lumbar
12,819.33
12.9711.8119,747,909.126.478.26
16.4311,486,30
27,0315,1635.627.147,91
16,5010,8326.6415.3216,84
subject
Cervical
520,2350,30
425,0222.4149,14
273,4930,35
1151,90131,5058,40
271.2728.13
255.49349,75
85,77377,10
28.0228.16
148,85103,44
1236.82264.15
Posterior
Thoracic
77.9850.3076.3422,4149,1461,8630.3560.8325.2258,4051,2828.1343.7564,7361,5575,9528,0228.1660.9460,1185,0253,64
Lumbar
213,42158,14499,79138.23197.44473.15
82.50510,44366,54375,72301.54
34.8774.3269,74
326,2066,5393.32
422.9957.68
118,48253,53151,76
/•", Female; M. male.
12,00D Within Session Average
• Between Session Average
-2,00Sagittal Cervical Sagittal Thoracic Sagittal Lumbar Posterior Cervical Posterior Thoracic Posterior Lumbar
Spinal Segment and View
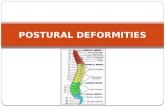
Fig 3. Mean repositioning errors across all subjects within and between sessions. Within-session repositioning errors were calculated asthe difference in magnitude of angle between all combinations of pairs of trials within a given session. Between-session errors weredetermined in a .similar manner, as ail eombinations of pairs of trials across any two ses.iions.
the cervical angle in the sagittal view (P ^ .001) and thethoracic angle in the posterior view (P = .025), Aninteraction between session and trial was found for thecervical angle in the posterior view (P = .017). Because of
inconsistency observed in some subjects (Fig 2) and the trialeffects determined from the ANOVA results, CVs werecalculated across sessions to examine individual subjectvariability {Table 2). The bulk ofthe CVs in the sagittal view

390 DunkclalRcliiibihtv .ind Posture Analysis
Jciumal ot'Mariipulaiive :iTui PliysJologicHl ThcrapculicsJuly/Augusl 2005
Table 3. Inliaclass correlationhonien across trial and svs.sion
Angle
CenicalTlinracicLunihar
Sagittal
Wbiiicn
O.S370.638O.f)39
cocfficicnl vdliivsfor each angle in
Men
0.7460.7270,722
tor men and
each view
Ptistcrior
Worn on
0.5760.6060.157
Men
0.3600.3100.333
\CC <.0.4. poor: ICC between 0,4 and 0.75, fair to good; ICC>0.75. excellent.
were below the eommonly acceptable range of 20% to 40%for gait studies.'^ However, most the CVs in the posteriorview were well above this acceptable range.
Individual subject mean repositioning errors ranged from0.80 to 16.11 atid 0.33 to 3.72 in the sagittal andposterior views, respectively. Between-session mean repo-sitioning errors were generally much larger than within-session errors (Fig 3). The posterior view had repositioningerrors that were less than 2 , whereas the sagittal viewtended to have larger values up to 6 (Fig 3).
The ICCs calculated across trial and session ranged frompoor to excellent agreement for all 3 angles in both views(Table 3). Intraelass correlation coefficients below 0.4 areconsidered poor and ICCs greater than 0,75 are consideredexcellent.'^ Angles in the posterior view were generally lessrepeatable than those in the sagittal view (Table 3). In ihesagittal view, individual subject posture was moderatelyrepeatable (ICC range, 0.6-0.75). apart from the femalecei-vical angle, which showed excellent repeatability. Theseresults indicate that on a day-by-day basis, posture in thesagittal view was moderately to excellently repeatable,whereas posture docunientcd in the posterior view exhibitedpoor to moderate repeatability.
Intraelass correlation coefficients were also calculatedacross subjects on a session-by-session basis for each of the 3angles in both views. This was done to examine posturerepeatability without the variability due to marker placctncntbecause markers were not removed and reapplicd within asession. The ICCs calculated within a session ranged from0.546 to 0.982. In the sagittal view, within-session repeat-ability was excellent (ICC range, 0.751-0.982) for all angles,except for the male cervical angle in session 3 (ICC, 0.550).Posture was found to range from moderate to excellentrepeatability in the posterior view (ICC range, 0.546-0.961).These results indicate that repeatability of posture is moderateto excellent on a given day and that marker placement couldplay a role in between-day repeatability, although efforts weremade to ensure consistent placement.
DISCUSSION
Posture was highly variable using a biologically relevantmeasure to document spinal angles. However, the sagittal
view provided a more stable measure of spinal angles thanthe posterior view and could have potential to be a methodof tracking changes due to clinical interventions, dependingon the expected magnitude of treatment effect.
The present study's method of calculating spinal anglesdocumented a higher repeatability of posture in the sagittalview (ICC range, 0.638-0.837) when compared with aprevious study conducted by Dunk et al.^ When measuringsagittal spinal angles as deviations frorn a vertical reference,posture repeatability was found lo be poor to moderate (ICCrange, 0.269-0.567).^ This indicates that the verticalreference method was likely susceptible to error frompostural sway which would alter the spinal deviationscalculated with no change in spine curvature. Although thissource of variability is eliminated using the biologicreference, posture in the posterior view was poorly tomoderately repeatable regardless of the method used tocalculate spinal angles. Intraciass correlation coeffieientsranged from 0.134 to 0.691 for the vertical reference methodand from 0.157 to 0.606 for the biologic reference method.
Although the results of the cun-ent study are moreencouraging than the previous study, there are other sourcesof variability that have not been directly addressed.Although one researcher was responsible for the placementof the markers and positioning of the headband on thesubjects, there could be some variability in placement fromsession to session. Intraelass coirelation coefficients werecalculated within a session and tended to be higher than theICCs calculated across sessions, indicating that markerplacement may have had some effect on the repeatability ofposture. It is not possible to specifically factor out themarker and posture variability on a day-by-day comparison.However, angles documented in session 3 were notsignificantly ditTerent from those in sessions I and 2 wheremarks on the skin were still visible for marker placementfrom the morning to the aftemoon sessions. Furthennore, arecent study found high intraexaminer reliability of markerplacement after a 1-hour training period,"^ which suggeststhat marker placement does not contribute substantially tothe between-day variability seen in the current study. Itshould be noted that because the angles calculated in theposterior view fluctuate approximately a zero value, markerand headband placement as well as manual digitizationerrors would have a greater effect on the reliability of spinalangles calculated in the posterior view. The manual digitiz-ing process of the markers may also induce variability intothe measurements. However, it has been established thatmanual digitization is highly reliable within a givenobserver, both within and across days.''' Furthennore. thereseareher responsible for the manual digitizing process inthe current study underwent a training protocol that hasbeen shown to maintain precision at high levels withincreased accuracy.""
A further limitation of this study was the use of pain-free,healthy individuals to assess an approach primarily intended

Jmrmal of Maiiipulalive and Physiological TlierapeulicsVolume 2S. Number 6
Dunk ei 1̂and Pusiure Analysis
391
for use with an injured or pain-report ing population. Thecurrent methodology hinges on the relative variability ofback pain individuals and those that are pain-free. In anextensive review of the literature, Essendrop et ai~' foundthat no definite conclusions can be made about thereproducibility of measures of trunk posture and motion inpatients as compared with healthy subjects. They noted,however, that when pain is not included as a parameter (ie,pain is not changing), patients can be tested for range ofmotion as reliably as healthy subjects. Other studies haveshown that the degree of between-subject variability inmeasurements of lumbar lordosis for a patient population issimilar'^'" or slightly greater'' than a normal healthypopulation. Therefore, assessing the feasibility of a pos-ture-based assessment on a control sample seems warranted.
Several other studies have adopted a test-retest protocol toexamine the reproducibility of a specific biological measure-ment tool to document upright standing posture. Althoughseveral studies using radiography to measure cervicallordosis showed no significant differences in cervical align-ment of the pre- and posttest radiographs," """ patientpositioning was standardized by the practitioner betweensessions,"*^ or participants were asked to look in a mirrorwhile the head was fixed.'''^ Still, Harrison et al" found nosignificant ditTerences in prc-and posttest radiographs in theircontrol group over a 10- to 14-week period when theparticipants were asked to reposition tbe head in a neutralrelaxed posture. Furthermore, Refshauge et al"'' showedexcellent reproducibility of certain measures of cervical andcervicothoracie curvature using skin markers. Their methodof measuring the cervical angle as the angle betv.'een themarkers at C2 and C7. with C4 as the vertex, was lessrepeatable than other measurements used. They suggestedthat a likely explanation for the variable rehability was thesmall distance between the 3 vertebral levels and that minordigitizing errors would produce relatively large changes inangle. Therefore, it is possible that some methods ofdocumenting upright standing posture are more repeatablethan others.
Willner^ used a spinal pantograph to measure kyphosisand lordosis of the spine and found that the mean differ-ences between the different observations ranged from 0' to7 . Swinkels and Dolan'" assessed a person's ability toreproduce an upright standing posture using a 3-spaceFastrak with sensors placed at Tl, T7. LI, and S2. Althoughmean repositioning errors were less than 4 , ICCs rangedfrom 0.102 to 0.748 for within-day and 0.114 to 0.781 forbetween-day agreement. In addition, Brumagne et al''^found an overall mean lumbosaeral repositioning accuracyof 1.87 and ICCs for test-retest reliability of 0.72 and 0.64for an electrogoniometer and 3D video analysis, respec-tively. Mean repositioning errors were calculated for thecurrent study and were found to be less than 6 for thesagittal view and less than 2 for the posterior view fornormal healthy subjects. Therefore, clinical interventions
that use a noninvasive postural analysis approach wouldhave to produce magnitudes of change that exceed at least a6 change in the sagittal view or a 2 change in the posteriorview to be reliably detected.
CONCLUSIONS
Although the repeatability of posture was improved in thesagittal view when a biological measure was used instead ofan external reference to calculate spinal angles, individualsubject posture was still variable. This brings into questionthe effectiveness and validity of using a surface skin markersystem to track postural changes due to clinical interven-tions. If disorders can be detected in the sagittal view, thenusing this approach with biologically relevant angles appearsto have value. However, this comes with the limitation thatany changes due to clinical treatment should be larger thanthe baseline repositioning errors seen in healthy subjects.
REFERENCES
1. Griegel-Morris P, Larson K, Miicllcr-Klaus K, Oatis CA.lticidence of common postural abnormalilies in the cervical,shoulder, atid thoracic regions and their association with painin two age groups of healthy subjects. Pliys Ther 1992:72:425-31.
2. Grimmer K. An investigation of poor cervical resting posture.Aust J Physiother 1997;43:7-I6.
3. Raine S, Twomey LT Head and shoulder posture variations in160 asymptomatic women and men. Arch Phys Med Reliabit1997;78:l2l5-23.
4. Zonnenberg AJ, Van Maanen CJ, Oostendorp RA, Elvers JW.Body posture photographs as a diagnostic aid for musculoske-Ictal disorders related to teniporomandibular disorders (TMD).Cranio 1996:14:225-32.
5. Youdas JW, Garrett TR. Egan KS, Themeau TM. Lumbarlordosis and pelvic inclinatioti in adults with chronic low backpaiti. Phys Ther 2000:80:261 -75.
6. Murrie VL, Dixon AK, Hollingworth W. Wilson H. Doyle TA.Lumbar lordosis: sttidy of patients with and wilhoiit low backpain. Clin Anat 2003:'l6:144-7.
7. Dunk NM. Chung YY, Compton DS, fallaglian .IP. Thereliability of quantitying upright standing postures as a baselinediagnostic clinical tool. .1 Manipulative Physiol Ther 2004:27:91-6.
8. Willner S. Spinal pantograph: a non-invasive technique fordeseribing kyphosis and lordosis in the thoraco-lumbar spine,Acta Orthop Scand 1981:52:525-9.
9. Bullock-Saxton J. Postural alignment in standing: a repeat-ability sUidy. Aust J Pliysiother 1993:39:25-9.
10. Goh S. Price Rl. Leedman PJ, Singer KP Rasterstereographicanalysis of the thoracic sagittal curvature: a reliability study.J Musculoskelet Res 1999:3:137-42.
IL McLean IP, Gillan MG, Ross JC, Aspden RM. Porter RW. Acomparison of methods for measuring tmnk list. A simpleplumbline is the best. Spine 1996:21:1667-70.
12. Swinkels A, Dolan P. Regional assessment of joint positionsense in the spine. Spine 199S;23:590-7.
13. Brumagne S, Lysens R, Spaepen A. Lumbosaeral repositioningaccuracy in standing posture: a combined elecirogoniometrieand videographic evaluation. Clin Biomech 1999:14:361-3.

392 Dunk ct illReliability and Posture Analysis
Journal of Manipulative and Physiological TherapeuticsJuly/August 2005
14. Gilleard WL. Crosbie J. Smith R. Static trunk posture in sittingand standing during pregnancy and early postpartum. ArchPhys Med Rchabil 2002;83:1739-44.
15. Siirout PE, Fleiss JL, Intraclass correlations: uses in assessingrater reliability. Psycho! Bull I979;H6:42O.8.
16. Winter DA. Kinematic and kinetic patterns in human gait:variability and compensating effects. Hum Mov Sei 1984;3:51-76.
17. Fleiss JL. The design and analysis of clinical experiments.Toronto: John Wiley and Sons; 1986.
18. Woo TK, Pearsall DJ. Postural estimates from digital images:inter- and intra-tester reliability. Proceedings ofthe IV WorldCongress of Biomechanics. Calgary: World Council of Bio-mechanies [Aug 4-8].
19. Sullivan D. Bryden P, Callaghan JP, Inter- and intra-observerreliability of calculating cumulative lumbar spine loads.Ergonomics 2002:45:788-97.
20. Sullivan D. Bryden P, Callaghan JP. Reliability of manualdigitization for the calculation of cumulative loads in tbelumbar spine. Proceedings of the XVI International AnnualOccupational Ergonomics and Safety Conference. Toronto:International Society for Occupational Ergonomies and Safety;2002 [June 9-12].
21. Essendrop M. Maul I. Laubli T, Riihimaki H, Scbibye B.Measures of low back function: a review of reproducibiiitystudies. Clin Biomech 2002:17:235-49.
22. Ng JK, Richardson CA. Kippers V, Pamianpour M. Compar-ison of lumbar range of movement and lumbar lordosis inback pain patients and matched controls. J Rehabil Med2002:34:109-13.
23. Harrison DD, Jackson BL, Troyanovich S, Robertson G, deGeorge D, Barker WF. The efficacy of cervical extension-compression traction combined with diversified manipulationand drop table adjustments in the rebabilitation of cervicallordosis: a pilot study. J Manipulative Physiol Ther 1994;17:454-64,
24. Plaugher G, Cremata EE, Phillips RB, A retrospectiveconsecutive case analysis of pretreatment and comparativestatic radiological parameters following chiropractic adjust-ments. J Manipulative Physio! Ther 1990;13:498-506.
25. Sandham A. Repeatability of head posture recordings fromlateral cepbalometric radiographs. Br J Orthod 1988; 15:157-62.
26. Refshauge K, Goodsel! M. Lee M, Consistency of cervical andcervicothoracic posture in standing. Aust J Pbysiotber 1994;40:235-40.