Implementing Optimal Cancer Care Pathways Forum · 6 Implementing optimal cancer care pathways...
32
Clinical Excellence Division Queensland Health Central Integrated Regional Cancer Service Implementing Optimal Cancer Care Pathways Forum 8 May 2017
Transcript of Implementing Optimal Cancer Care Pathways Forum · 6 Implementing optimal cancer care pathways...

ClinicalExcellence
Division
Queensland HealthCentral Integrated Regional Cancer Service
Implementing Optimal Cancer Care Pathways Forum
8 May 2017

e:e [email protected]:p 07 3131 1690
e:f 07 3131 1513e:a Lobby 1, Level 4 - Citilink Building
GPO Box 48Brisbane, QLD 4001
Contact CIRCS

Welcome
Welcome to the Implementing Optimal Cancer Care Pathways forum, facilitated by Central Integrated Regional Cancer Service (CIRCS), Healthcare Improvement Unit (HIU) and Cancer Council Queensland.
The implementation of Optimal Cancer Care Pathways (OCCPs) will contribute to achieving Service Direction 1 of the Cancer Care Statewide Health Service Strategy 2014 by promoting the use of evidence-based treatment protocols, guidelines and standards and ensuring people affected by cancer are well-informed throughout their cancer journey.
The pathway for cancer patients is complex and sometimes poorly comprehended by those involved. It usually involves multiple healthcare providers and covers a range of institutions, both public and private.
The OCCPs map the journey for 15 specific tumour types, aiming to foster an understanding of the whole pathway and its distinct components to promote quality cancer care and patient experiences. The patient is the constant in the journey and the health system has a responsibility to deliver care in an appropriate and coordinated manner1.
A wide range of clinicians, peak health organisations, consumers and carers were consulted and/or participated in the development of each of the OCCPs. These pathways were facilitated by the National Cancer Expert Reference Group and supported by the Australian Health Ministers’ Advisory Council. Now, each Australian state and territory is tasked with implementation.
The forum is designed to provide you with tools, information and support that will enable you to implement OCCPs in your local context. We are here to acknowledge the challenges faced by the current health system and work together on solutions to enable delivery of optimal cancer care.
I hope you find the forum informative and inspiring.
Adj Prof Liz Kenny AOMedical DirectorCIRCSQueensland Health
4 Implementing optimal cancer care pathways forum
Contents
Program ........................................................................................................................ 5
About the forum ............................................................................................................ 6
What are OCCPs? .......................................................................................................... 6
Why and how to use OCCPs ........................................................................................... 6
Expected use and impact .............................................................................................. 7
Improving patient communication and care .................................................................. 7
Using the tools in this booklet ....................................................................................... 7
OCCPs information flyer ................................................................................................ 8
Plan, Do, Study, Acte: A suggested quality improvement framework ................................ 9
The plan ....................................................................................................................... 10
Blank plan .................................................................................................................... 12
The report ..................................................................................................................... 14
Assessing your service .................................................................................................. 16
Step 1 - Prevention and early detection ..................................................................... 17
Step 2 - Presentation, initial investigations and referral ............................................ 18
Step 3 - Diagnosis, assessment and treatment planning ........................................... 19
Step 4 - Treatment .................................................................................................... 20
Step 5 - Care after initial treatment and recovery ...................................................... 21
Step 6 - Managing recurrent or progressive disease .................................................. 22
Step 7 - End-of-life care ............................................................................................. 23
Useful resources ........................................................................................................... 24
References .................................................................................................................... 26
Notes ............................................................................................................................ 27
Implementing optimal cancer care pathways forum 5
Program
8:30am Registration, tea/coffee & networking
9:00am Early morning session
Official welcome Adj Prof Liz Kenny AO - Medical Director, CIRCS
Facilitator’s welcome & housekeepingKaryn Schluter-White - Karyn Schluter-White & Associates
An introduction to Optimal Cancer Care Pathways Professor Kwun Fong - Clinical Manager, Pulmonary Malignancy Unit, The Prince Charles Hospital & Director, UQ Thoracic Research Centre
The cancer problemJoanne Aitken - Research Manager & Director of Registries, Cancer Council Queensland
My story Jodi Fraser - Consumer
10:30am Morning tea & networking
10:50am Late morning session
Introduction to Health Pathways
Mandy Pengilly - General Manager, Operations & Bernadette Praske - Senior Project Manager, Clinical Excellence, Darling Downs & West Moreton Primary Health Network
A quality improvement framework &implementation tools
Peter McGuire - Service Performance Manager & Barbara Page, Research & Quality Manager, CIRCS
The Victorian experienceMarita Reed - Program Manager, Quality & Cancer Outcomes, Department of Health & Human Services Victoria
12:30pm Lunch break & networking
1:30pm Afternoon session
Breakout discussion - What are the challenges and key enablers in my local context?
Karyn Schluter-White - Karyn Schluter-White and Associates
Breakout discussion - What solutions could be appropriate to overcome any barriers identified, including sharing of strategies between areas?
Karyn Schluter-White - Karyn Schluter-White and Associates
3:00pm Afternoon tea & networking
3:20pm Final session
Continuing the conversationPeter McGuire - Service Performance Manager & Barbara Page - Research & Quality Manager, CIRCS
3:50pm Close
6 Implementing optimal cancer care pathways forum
OCCPs detail key principles and recommendations for optimal care at critical points in the cancer continuum, from prevention and identification through to survivorship or end-of-life care.
Detailed pathways, as well as quick reference guides and patient guides, have been developed for 15 tumour typese:
• acute myeloid leukaemia• breast cancer• colorectal cancer• endometrial cancer• head and neck cancers• hepatocellular carcinoma• high-grade glioma cancer• Hodgkin lymphoma and diffuse large B-cell lymphoma• lung cancer• melanoma• non-melanoma skin cancers• oesophagogastric cancer• ovarian cancer• pancreatic cancer• prostate cancer.
Why and how to use OCCPs2
About the forum
This forum was convened by a partnership between Queensland Health (CIRCS and HIU) and Cancer Council Queensland (CCQ). The workshop is for all people in Queensland wanting to improve cancer care by implementing OCCPs.
What are OCCPs?
OCCPs are national guides to the best cancer care for specific tumour types.
They describe the key stages in a patient’s cancer journey and expected optimal care at each stage to ensure all people affected by cancer get the highest-quality care, regardless of where they live or have their treatment.
Implementing optimal cancer care pathways forum 7
OCCPs can be used by clinicians and health professionals as an information resource and tool to promote discussion and collaboration with people affected by cancer.
Patient versions (“what to expect” guides) have been developed to help patients and other people affected by cancer to understand the usual stages during and after treatment and what to expect at each stage. Ideally, newly-diagnosed patients will be told about the pathways and given a copy of the relevant “what to expect” guide by their GP or specialist at or soon after diagnosis.
Improving patient communication and care
Everyone involved in our cancer services contributes to safe and high-quality patient care and positive patient experiences. By following and referring to the OCCPs at critical points, we will ensure consistency, coordination and quality of care for patients across the cancer care continuum. Patient treatment regimens will vary, but the principles and expectations of optimal cancer care are constant.
OCCPs can be used by health services and professionals as a tool to identify gaps in current cancer services and inform quality improvement initiatives across all aspects of the care pathway. Using the pathways will help us plan and coordinate service delivery by identifying the investigations, therapies, clinical expertise, facilities and support needed at each key point of the patient journey, and resources required to enable optimal patient care and support.
Pathways can be used to promote multidisciplinary discussion, as well as to support collaboration and communication with people affected by cancer.
Expected use and impact
Using the tools in this booklet
The tools and information in this booklet are provided to help implement OCCPs. We suggest you make modifications to suit your local needs.
Templates are not intended to be completed by one person in an office. Better value will come from sharing your plan, discussing the key issues, analysing options for improvement and collaborating on solutions.
8 Implementing optimal cancer care pathways forum
OCCPs information flyer1
Optimal Cancer Care Pathways
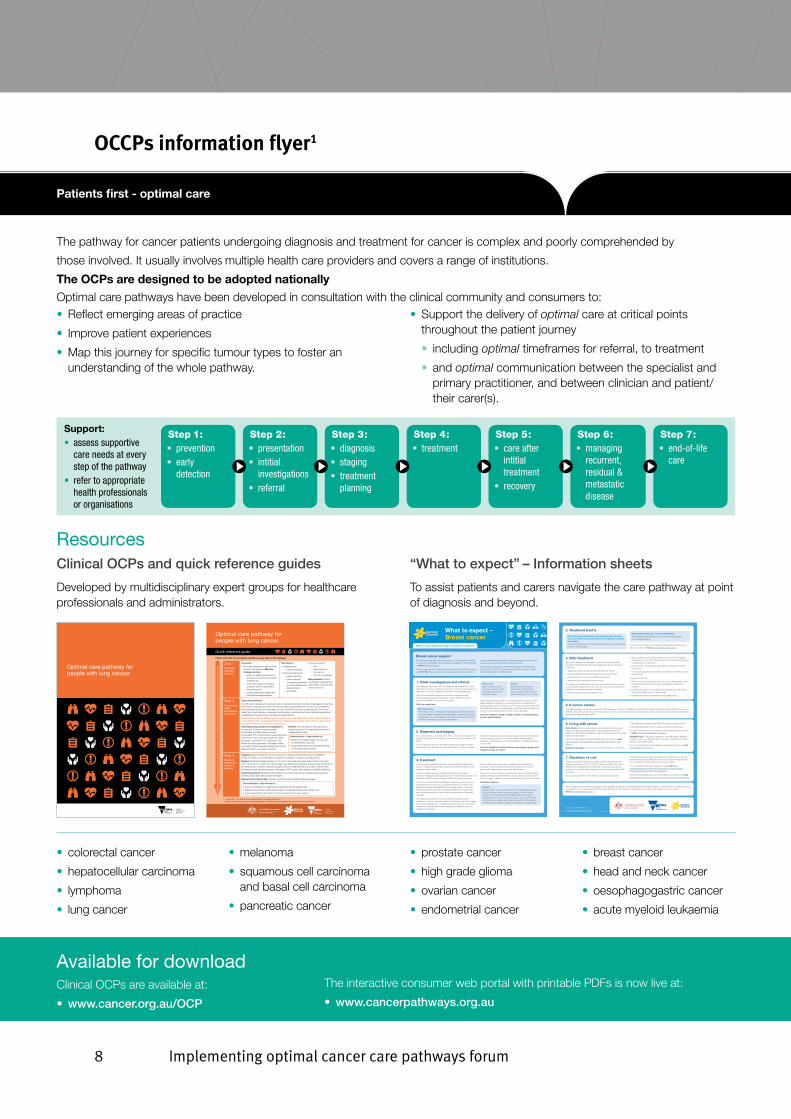
The pathway for cancer patients undergoing diagnosis and treatment for cancer is complex and poorly comprehended by
those involved. It usually involves multiple health care providers and covers a range of institutions.
The OCPs are designed to be adopted nationally
Optimal care pathways have been developed in consultation with the clinical community and consumers to:• Reflect emerging areas of practice
• Improve patient experiences
• Map this journey for specific tumour types to foster anunderstanding of the whole pathway.
• Support the delivery of optimal care at critical pointsthroughout the patient journey
• including optimal timeframes for referral, to treatment
• and optimal communication between the specialist andprimary practitioner, and between clinician and patient/their carer(s).
Support: • assess supportive
care needs at every step of the pathway
• refer to appropriate health professionals or organisations
Step 1: • prevention• early
detection
Step 3: • diagnosis• staging• treatment
planning
Step 6: • managing
recurrent, residual & metastatic disease
Step 2: • presentation• intitial
investigations• referral
Step 5: • care after
intitial treatment
• recovery
Step 4: • treatment
Step 7: • end-of-life
care
ResourcesClinical OCPs and quick reference guides
Developed by multidisciplinary expert groups for healthcare professionals and administrators.
“What to expect” – Information sheets
To assist patients and carers navigate the care pathway at point of diagnosis and beyond.
Available for downloadClinical OCPs are available at:
• www.cancer.org.au/OCP
The interactive consumer web portal with printable PDFs is now live at:
• www.cancerpathways.org.au
• colorectal cancer
• hepatocellular carcinoma
• lymphoma
• lung cancer
• melanoma
• squamous cell carcinomaand basal cell carcinoma
• pancreatic cancer
• prostate cancer
• high grade glioma
• ovarian cancer
• endometrial cancer
• breast cancer
• head and neck cancer
• oesophagogastric cancer
• acute myeloid leukaemia
Optimal care pathway for people with lung cancer
Sup
po
rt: A
sses
s su
pp
ort
ive
care
nee
ds
at e
very
ste
p o
f th
e p
athw
ay a
nd r
efer
to
ap
pro
pri
ate
heal
th p
rofe
ssio
nals
or
org
anis
atio
ns.
Optimal care pathway for people with lung cancer
Signs and symptoms:
The following unexplained or persistent signs or symptoms lasting more than three weeks (or less than three weeks in people with known risk factors) require urgent referral for a chest x-ray: unexplained haemoptysis or persistent new/changed cough, chest/shoulder pain, breathlessness, hoarseness, weight loss, finger clubbing, unresolved chest infection, abnormal chest signs, features suggestive of metastasis from a lung cancer, and signs of pleural effusion.
Persistent haemoptysis and/or signs of superior vena cava obstruction require urgent referral to a specialist linked to a multidisciplinary team. Massive haemoptysis and/or signs of stridor require immediate referral to an emergency department.
Diagnosis: May be obtained from bronchoscopy including endobronchial ultrasound (EBUS), CT-guided biopsy, excisional biopsy or biopsy of metastasis, or sputum cytology (rarely).
Staging: Radiological staging based on CT scan of the chest and upper abdomen and one of the brain. Other tests to confirm the cancer stage may include bronchoscopy, thoracoscopy, thoracotomy, mediastinoscopy, endobronchial/oesophageal ultrasound (EBUS/EUS) and nuclear medicine tests including bone and positron emission tomography (PET) scans, with biopsies to establish pathology.
Treatment planning: All patients with suspected or proven lung cancer should be discussed by a multidisciplinary team before treatment begins.
Research and clinical trials: Consider enrolment where available and appropriate.
Prevention:
• All current smokers should be offered advice to quit smoking. Effective strategies include:
– advice on quitting smoking and structured interventions by health professionals
– individual or group counselling programs such as Quit (refer to www.quit.org.au)
– nicotine replacement therapy andother pharmacological agents.
Please note that not all patients will follow every step of this pathway:
1 Lead clinician – the clinician who is responsible for managing patient care. The lead clinician may change over time depending on the stage of the care pathway and where care is being provided.
Risk factors:
• Lifestyle factor:
– tobacco smoking
• Environmental factors:
– passive smoking
– radon exposure
– occupational exposure (such as asbestos and diesel exhaust)
– air pollution
• Personal factors:
– age
– family history of lung cancer
– chronic lung disease
Early detection: No form of population screening has been shown to improve lung cancer outcomes.
Step 3Diagnosis, staging and treatment planning
Step 2Presentation, initial investigations and referral
Step 1Prevention and early detection
Quick reference guide
Communication – lead clinician to:
• discuss a timeframe for diagnosis and treatment with the patient/carer
• explain the role of the multidisciplinary team in treatment planning and ongoing care
• provide appropriate information or refer to support services as required.
General/primary practitioner investigations: Chest x-ray; if cancer is suspected refer immediately. Contrast spiral computed tomography (CT) of the chest and upper abdomen if the chest x-ray is clear and symptoms persist. Immediate referral if the CT is abnormal. Test results should be provided to the patient within one week. The first specialist appointment should take place within two weeks of referral.
Referral: Refer all patients with suspected or proven lung cancer to a specialist linked with a multidisciplinary team.
Communication – lead clinician to:1
• explain to the patient/carer who they are being referred to and why
• support the patient and carer while waiting for specialist appointments.
What to expect during each stage of treatment and beyond
What to expect –Breast cancer
1. Initial investigations and referralYour general practitioner (GP) will assess any symptoms you maynotice (for example, a change in the size or shape of your breast or a new lump), conduct a physical examination and arrange tests.
Your GP should also discuss your needs (including physical, psychological, social and information needs) and recommend sources of reliable information and support.
Tests you may have:
MammographyA low-dose x-ray of the breasts. Each breast is pressed between two x-ray plates to spread the breast tissue so that clear pictures can be taken. A mammography can detect changes that are too small to be felt during a physical examination.
Ultrasound High-frequency sound waves are used to create an image of the tissues inside the breast.
BiopsySmall samples of cells are removed from the breast lump, using a needle, and are examined under a microscope.
Tests should be done within two weeks. If breast cancer or other abnormalities are present, you will be referred to a specialist for further testing within two weeks. Your GP will provide the clinic with information about your medical history, whether there is a history of cancer in your family, and the results of the initial tests.
It can be helpful to bring a family member or friend with you to your appointments.
Breast cancer supportFor free resources about breast cancer, or to find support available in your area, call Breast Cancer Network Australia on 1800 500 258 or visit www.bcna.org.au.
You can also speak to qualified cancer nurses at the Cancer Council on 13 11 20. They can answer your questions about the effects of
cancer, explain what will happen during treatment and link you to support groups and other community resources.
If you need an interpreter, call TIS (Translating and Interpreting Service) on 13 14 50. For support and advice for carers, call the Carers Association on 1800 242 636.
2. Diagnosis and stagingYour specialist may conduct further tests to find out the stage of the cancer (how big it is and whether it has spread to other parts of the body).
You should also meet with a health professional (usually a breast care nurse), who will discuss your needs with you during and after
treatment (including physical, psychological, social and information needs) and may refer you to another health professional (for example, a social worker or a physiotherapist) for different aspects of your care.
It can be helpful to contact cancer peer support groups and support groups for carers.
3. TreatmentTo ensure you receive the best care, your specialist will arrange for a team of health professionals to plan your treatment based on yourpreferences and needs.
The team will be made up of health professionals who have experience managing and supporting women with breast cancer. Your specialist will tell you when the team will be discussing your case.
Your doctor should discuss the different treatment options with you including the likely outcomes, expected timeframes, possible side effects and the risks and benefits. For younger women, your team should also discuss the option of fertility preservation and provide clear information about the risk of early menopause and hormonal changes.
You might want to ask for more time before deciding on your treatment, or ask for a second opinion. Your doctor may also suggest you consider taking part in a clinical trial. If you wish, you can ask for a referral to a fertility service and/or genetic counsellor to help you evaluate your options.
Let your team know about any complementary therapies you are using or thinking about trying. Some therapies may not be appropriate, depending on your medical treatment.
There are a number of ways to treat breast cancer including surgery, radiation therapy and chemotherapy or drug therapy. Usually, more than one type of treatment is recommended to get the best outcome.
Treatment options:
Surgery Surgery is the most common treatment for early breast cancer. It involves either breast-conserving surgery, where only the cancer and a small amount of healthy tissue is removed, or mastectomy, where the breast is removed. You should be fully informed of your options and offered the option of immediate or delayed reconstructive surgery if undergoing a mastectomy.
For more information visitwww.cancerpathways.org.au
3. Treatment Cont’d
Chemotherapy, targeted/biological therapy (for example, trastuzumab) or hormone/endocrine therapy (for example, tamoxifen)This may benefit some women with breast cancer. Could be given before or after surgery.
Radiation therapy (also called radiotherapy) This treatment may benefit some women with early breast cancer (after surgery).
For more information about treatment and treatment side effects ask your doctor or visit www.bcna.org.au/resources.
4. After treatment After your treatment is completed, your doctor should provide you with a treatment summary that details the care you received including:
• diagnostic tests that were performed and their results
• types of treatment used and when they were performed
• treatment plans from other health professionals
• supportive care services provided to you.
To monitor your health and make sure the cancer has not returned, you may need regular check-ups. You and your GP should receive a follow-up care plan that tells you about:
• the type of follow-up that is best for you
• types of tests that you may continue to have (it is not usuallynecessary to have a lot of body scans but annual breast imaging, if appropriate, is important)
• care plans for managing any side effects of treatment should they occur
• how to get specialist medical help quickly if you think the cancerhas returned.
Your doctor should:
• discuss your needs with you and refer you to appropriate health professionals and/or community organisations, if support is required
• provide information on the signs and symptoms to look out for that might mean a return of the cancer
• provide information on prevention and healthy living.
6. Living with cancerSide effects: Some people experience side effects (for example, weight changes or tiredness) that continue beyond the end of treatment. Side effects sometimes might not begin until months after treatment has finished.
For more information about side effects ask your doctor or visit http://cancervic.org.au/about-cancer/survivors/long-term-side-effects.
Advance care plan: Your doctor may discuss with you the option
of developing an advance care plan. An advance care plan is a
formal way of setting out your wishes for future medical care.
For more information about advance care planning ask your doctor or visit www.advancecareplanning.org.au.
Palliative care: This type of treatment could be used at different stages to help you with pain relief, to reduce symptoms or to help improve your quality of life.
For more information about palliative care ask your doctor or visit www.palliativecare.com.au.
5. If cancer returnsSometimes breast cancer can come back after treatment. Everyone is different, and the risk of cancer returning will be influenced by many different things including the type of breast cancer. This is why it is important you have regular check-ups that include a physical examination and breast imaging if appropriate.
7. Questions of costThere can be cost implications at each stage of the cancer care pathway, including costs of treatment, accommodation and travel. There can be substantial out-of-pocket costs if you are having treatment in a private health service, even if you have private healthinsurance.
You can discuss these costs with your doctor and/or private
health insurer for each type of treatment you may have. If you are experiencing financial difficulties due to your cancer treatment you can contact the social worker at your local hospital.
For more information about treatment costs visit http://canceraustralia.gov.au/affected-cancer/living-cancer/dealing-practical-aspects-cancer/costs-treatment.
For more information about accommodation and travel costs visit www.cancercouncil.com.au/get-support/practical-support-services.
Some breast cancers are found through mammographic screening. The BreastScreen Australia Program is available free of charge to women from age 40. It is recommended that if you are aged 50–74 you consider undergoing a screening mammogram every two years. Visit www.breastscreen.org.au
Patients first - optimal care
Implementing optimal cancer care pathways forum 9
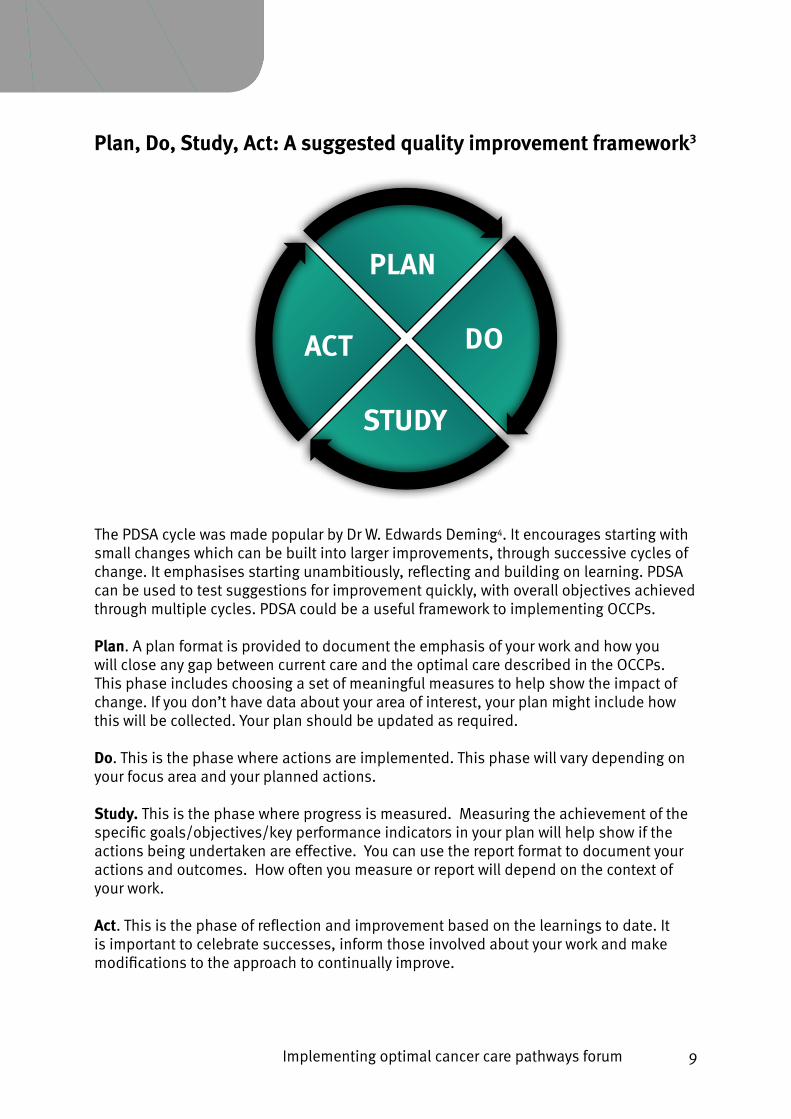
Plan, Do, Study, Act: A suggested quality improvement framework3
PLAN
DOACT
STUDY
Optimal Cancer Care Pathways
The pathway for cancer patients undergoing diagnosis and treatment for cancer is complex and poorly comprehended by
those involved. It usually involves multiple health care providers and covers a range of institutions.
The OCPs are designed to be adopted nationally
Optimal care pathways have been developed in consultation with the clinical community and consumers to:• Reflect emerging areas of practice
• Improve patient experiences
• Map this journey for specific tumour types to foster anunderstanding of the whole pathway.
• Support the delivery of optimal care at critical pointsthroughout the patient journey
• including optimal timeframes for referral, to treatment
• and optimal communication between the specialist andprimary practitioner, and between clinician and patient/their carer(s).
Support: • assess supportive
care needs at every step of the pathway
• refer to appropriate health professionals or organisations
Step 1: • prevention• early
detection
Step 3: • diagnosis• staging• treatment
planning
Step 6: • managing
recurrent, residual & metastatic disease
Step 2: • presentation• intitial
investigations• referral
Step 5: • care after
intitial treatment
• recovery
Step 4: • treatment
Step 7: • end-of-life
care
ResourcesClinical OCPs and quick reference guides
Developed by multidisciplinary expert groups for healthcare professionals and administrators.
“What to expect” – Information sheets
To assist patients and carers navigate the care pathway at point of diagnosis and beyond.
Available for downloadClinical OCPs are available at:
• www.cancer.org.au/OCP
The interactive consumer web portal with printable PDFs is now live at:
• www.cancerpathways.org.au
• colorectal cancer
• hepatocellular carcinoma
• lymphoma
• lung cancer
• melanoma
• squamous cell carcinomaand basal cell carcinoma
• pancreatic cancer
• prostate cancer
• high grade glioma
• ovarian cancer
• endometrial cancer
• breast cancer
• head and neck cancer
• oesophagogastric cancer
• acute myeloid leukaemia
Optimal care pathway for people with lung cancer
Sup
po
rt: A
sses
s su
pp
ort
ive
care
nee
ds
at e
very
ste
p o
f th
e p
athw
ay a
nd r
efer
to
ap
pro
pri
ate
heal
th p
rofe
ssio
nals
or
org
anis
atio
ns.
Optimal care pathway for people with lung cancer
Signs and symptoms:
The following unexplained or persistent signs or symptoms lasting more than three weeks (or less than three weeks in people with known risk factors) require urgent referral for a chest x-ray: unexplained haemoptysis or persistent new/changed cough, chest/shoulder pain, breathlessness, hoarseness, weight loss, finger clubbing, unresolved chest infection, abnormal chest signs, features suggestive of metastasis from a lung cancer, and signs of pleural effusion.
Persistent haemoptysis and/or signs of superior vena cava obstruction require urgent referral to a specialist linked to a multidisciplinary team. Massive haemoptysis and/or signs of stridor require immediate referral to an emergency department.
Diagnosis: May be obtained from bronchoscopy including endobronchial ultrasound (EBUS), CT-guided biopsy, excisional biopsy or biopsy of metastasis, or sputum cytology (rarely).
Staging: Radiological staging based on CT scan of the chest and upper abdomen and one of the brain. Other tests to confirm the cancer stage may include bronchoscopy, thoracoscopy, thoracotomy, mediastinoscopy, endobronchial/oesophageal ultrasound (EBUS/EUS) and nuclear medicine tests including bone and positron emission tomography (PET) scans, with biopsies to establish pathology.
Treatment planning: All patients with suspected or proven lung cancer should be discussed by a multidisciplinary team before treatment begins.
Research and clinical trials: Consider enrolment where available and appropriate.
Prevention:
• All current smokers should be offered advice to quit smoking. Effective strategies include:
– advice on quitting smoking and structured interventions by health professionals
– individual or group counselling programs such as Quit (refer to www.quit.org.au)
– nicotine replacement therapy andother pharmacological agents.
Please note that not all patients will follow every step of this pathway:
1 Lead clinician – the clinician who is responsible for managing patient care. The lead clinician may change over time depending on the stage of the care pathway and where care is being provided.
Risk factors:
• Lifestyle factor:
– tobacco smoking
• Environmental factors:
– passive smoking
– radon exposure
– occupational exposure (such as asbestos and diesel exhaust)
– air pollution
• Personal factors:
– age
– family history of lung cancer
– chronic lung disease
Early detection: No form of population screening has been shown to improve lung cancer outcomes.
Step 3Diagnosis, staging and treatment planning
Step 2Presentation, initial investigations and referral
Step 1Prevention and early detection
Quick reference guide
Communication – lead clinician to:
• discuss a timeframe for diagnosis and treatment with the patient/carer
• explain the role of the multidisciplinary team in treatment planning and ongoing care
• provide appropriate information or refer to support services as required.
General/primary practitioner investigations: Chest x-ray; if cancer is suspected refer immediately. Contrast spiral computed tomography (CT) of the chest and upper abdomen if the chest x-ray is clear and symptoms persist. Immediate referral if the CT is abnormal. Test results should be provided to the patient within one week. The first specialist appointment should take place within two weeks of referral.
Referral: Refer all patients with suspected or proven lung cancer to a specialist linked with a multidisciplinary team.
Communication – lead clinician to:1
• explain to the patient/carer who they are being referred to and why
• support the patient and carer while waiting for specialist appointments.
What to expect during each stage of treatment and beyond
What to expect –Breast cancer
1. Initial investigations and referralYour general practitioner (GP) will assess any symptoms you maynotice (for example, a change in the size or shape of your breast or a new lump), conduct a physical examination and arrange tests.
Your GP should also discuss your needs (including physical, psychological, social and information needs) and recommend sources of reliable information and support.
Tests you may have:
MammographyA low-dose x-ray of the breasts. Each breast is pressed between two x-ray plates to spread the breast tissue so that clear pictures can be taken. A mammography can detect changes that are too small to be felt during a physical examination.
Ultrasound High-frequency sound waves are used to create an image of the tissues inside the breast.
BiopsySmall samples of cells are removed from the breast lump, using a needle, and are examined under a microscope.
Tests should be done within two weeks. If breast cancer or other abnormalities are present, you will be referred to a specialist for further testing within two weeks. Your GP will provide the clinic with information about your medical history, whether there is a history of cancer in your family, and the results of the initial tests.
It can be helpful to bring a family member or friend with you to your appointments.
Breast cancer supportFor free resources about breast cancer, or to find support available in your area, call Breast Cancer Network Australia on 1800 500 258 or visit www.bcna.org.au.
You can also speak to qualified cancer nurses at the Cancer Council on 13 11 20. They can answer your questions about the effects of
cancer, explain what will happen during treatment and link you to support groups and other community resources.
If you need an interpreter, call TIS (Translating and Interpreting Service) on 13 14 50. For support and advice for carers, call the Carers Association on 1800 242 636.
2. Diagnosis and stagingYour specialist may conduct further tests to find out the stage of the cancer (how big it is and whether it has spread to other parts of the body).
You should also meet with a health professional (usually a breast care nurse), who will discuss your needs with you during and after
treatment (including physical, psychological, social and information needs) and may refer you to another health professional (for example, a social worker or a physiotherapist) for different aspects of your care.
It can be helpful to contact cancer peer support groups and support groups for carers.
3. TreatmentTo ensure you receive the best care, your specialist will arrange for a team of health professionals to plan your treatment based on yourpreferences and needs.
The team will be made up of health professionals who have experience managing and supporting women with breast cancer. Your specialist will tell you when the team will be discussing your case.
Your doctor should discuss the different treatment options with you including the likely outcomes, expected timeframes, possible side effects and the risks and benefits. For younger women, your team should also discuss the option of fertility preservation and provide clear information about the risk of early menopause and hormonal changes.
You might want to ask for more time before deciding on your treatment, or ask for a second opinion. Your doctor may also suggest you consider taking part in a clinical trial. If you wish, you can ask for a referral to a fertility service and/or genetic counsellor to help you evaluate your options.
Let your team know about any complementary therapies you are using or thinking about trying. Some therapies may not be appropriate, depending on your medical treatment.
There are a number of ways to treat breast cancer including surgery, radiation therapy and chemotherapy or drug therapy. Usually, more than one type of treatment is recommended to get the best outcome.
Treatment options:
Surgery Surgery is the most common treatment for early breast cancer. It involves either breast-conserving surgery, where only the cancer and a small amount of healthy tissue is removed, or mastectomy, where the breast is removed. You should be fully informed of your options and offered the option of immediate or delayed reconstructive surgery if undergoing a mastectomy.
For more information visitwww.cancerpathways.org.au
3. Treatment Cont’d
Chemotherapy, targeted/biological therapy (for example, trastuzumab) or hormone/endocrine therapy (for example, tamoxifen)This may benefit some women with breast cancer. Could be given before or after surgery.
Radiation therapy (also called radiotherapy) This treatment may benefit some women with early breast cancer (after surgery).
For more information about treatment and treatment side effects ask your doctor or visit www.bcna.org.au/resources.
4. After treatment After your treatment is completed, your doctor should provide you with a treatment summary that details the care you received including:
• diagnostic tests that were performed and their results
• types of treatment used and when they were performed
• treatment plans from other health professionals
• supportive care services provided to you.
To monitor your health and make sure the cancer has not returned, you may need regular check-ups. You and your GP should receive a follow-up care plan that tells you about:
• the type of follow-up that is best for you
• types of tests that you may continue to have (it is not usuallynecessary to have a lot of body scans but annual breast imaging, if appropriate, is important)
• care plans for managing any side effects of treatment should they occur
• how to get specialist medical help quickly if you think the cancerhas returned.
Your doctor should:
• discuss your needs with you and refer you to appropriate health professionals and/or community organisations, if support is required
• provide information on the signs and symptoms to look out for that might mean a return of the cancer
• provide information on prevention and healthy living.
6. Living with cancerSide effects: Some people experience side effects (for example, weight changes or tiredness) that continue beyond the end of treatment. Side effects sometimes might not begin until months after treatment has finished.
For more information about side effects ask your doctor or visit http://cancervic.org.au/about-cancer/survivors/long-term-side-effects.
Advance care plan: Your doctor may discuss with you the option
of developing an advance care plan. An advance care plan is a
formal way of setting out your wishes for future medical care.
For more information about advance care planning ask your doctor or visit www.advancecareplanning.org.au.
Palliative care: This type of treatment could be used at different stages to help you with pain relief, to reduce symptoms or to help improve your quality of life.
For more information about palliative care ask your doctor or visit www.palliativecare.com.au.
5. If cancer returnsSometimes breast cancer can come back after treatment. Everyone is different, and the risk of cancer returning will be influenced by many different things including the type of breast cancer. This is why it is important you have regular check-ups that include a physical examination and breast imaging if appropriate.
7. Questions of costThere can be cost implications at each stage of the cancer care pathway, including costs of treatment, accommodation and travel. There can be substantial out-of-pocket costs if you are having treatment in a private health service, even if you have private healthinsurance.
You can discuss these costs with your doctor and/or private
health insurer for each type of treatment you may have. If you are experiencing financial difficulties due to your cancer treatment you can contact the social worker at your local hospital.
For more information about treatment costs visit http://canceraustralia.gov.au/affected-cancer/living-cancer/dealing-practical-aspects-cancer/costs-treatment.
For more information about accommodation and travel costs visit www.cancercouncil.com.au/get-support/practical-support-services.
Some breast cancers are found through mammographic screening. The BreastScreen Australia Program is available free of charge to women from age 40. It is recommended that if you are aged 50–74 you consider undergoing a screening mammogram every two years. Visit www.breastscreen.org.au
Patients first - optimal care
The PDSA cycle was made popular by Dr W. Edwards Deming4. It encourages starting with small changes which can be built into larger improvements, through successive cycles of change. It emphasises starting unambitiously, reflecting and building on learning. PDSA can be used to test suggestions for improvement quickly, with overall objectives achieved through multiple cycles. PDSA could be a useful framework to implementing OCCPs.
Plan. A plan format is provided to document the emphasis of your work and how you will close any gap between current care and the optimal care described in the OCCPs. This phase includes choosing a set of meaningful measures to help show the impact of change. If you don’t have data about your area of interest, your plan might include how this will be collected. Your plan should be updated as required.
Do. This is the phase where actions are implemented. This phase will vary depending on your focus area and your planned actions.
Study. This is the phase where progress is measured. Measuring the achievement of the specific goals/objectives/key performance indicators in your plan will help show if the actions being undertaken are effective. You can use the report format to document your actions and outcomes. How often you measure or report will depend on the context of your work.
Act. This is the phase of reflection and improvement based on the learnings to date. It is important to celebrate successes, inform those involved about your work and make modifications to the approach to continually improve.

10 Implementing optimal cancer care pathways forum
The plan
• For example, the OCCP for people with high grade glioma.• Step 2 - Presentation, initial investigations and referrals and Step 3 -
Diagnosis, assessment and treatment planning.
Focus area
• What is going on?• What data sources prove there is a problem?• Be visual (use diagrams and charts).• Make the problem clear.
Current conditions
Use the simplest problem-analysis tool to find the root cause of the problem, for examplee:• Seven Basic Tools of Quality (7 QC Tools).• Lean, Six Sigma, Kepner-Tragoe, Shainen, Taguchi or TRIZ tools.• Other tools of your choice.
Problem anaylsis
• Why are you talking about it?• What is the case for change?• What is the problem you are trying to solve or analyse?• Be very concise – communicate WHY you are addressing this issue.
Background
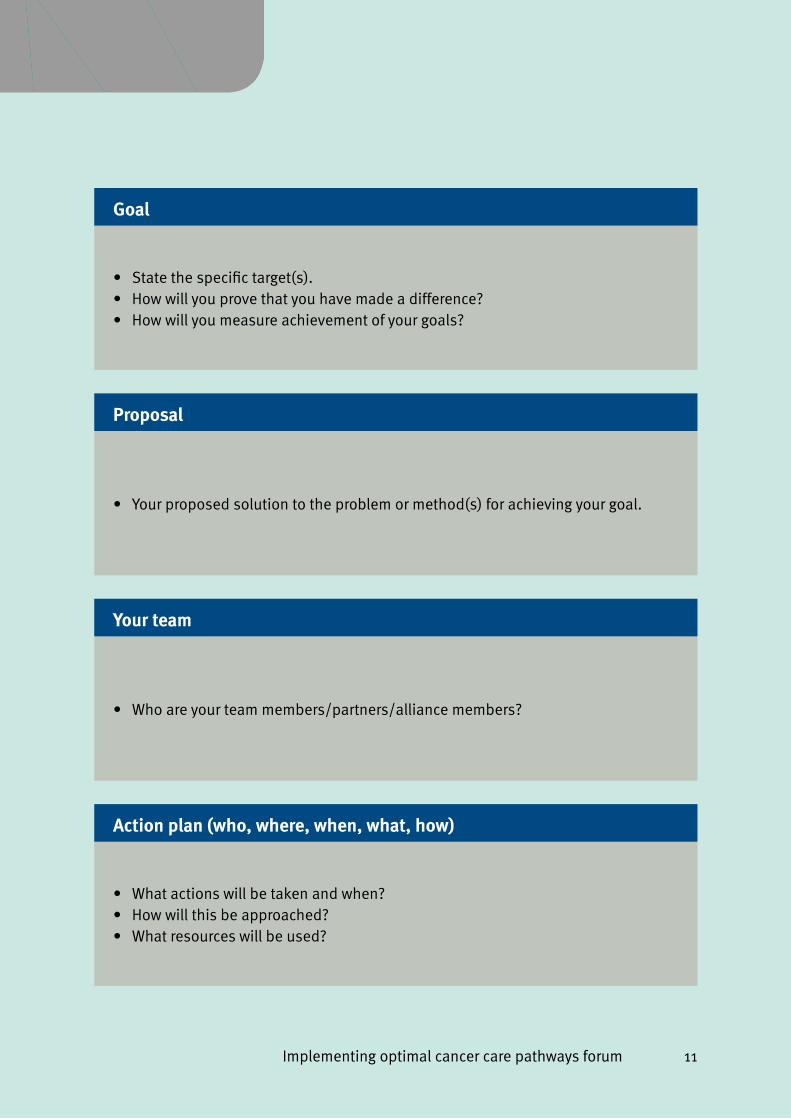
The plan below is modified from the A3 one-page project report tool5 and will help you to begin planning your implementation of OCCPs. Using this plan will enable you to structure problem solving and support communication through a common understanding of issues. It is provided to help you decide how to best implement OCCPs in your context.
Implementing optimal cancer care pathways forum 11
• Your proposed solution to the problem or method(s) for achieving your goal.
Proposal
• Who are your team members/partners/alliance members?
Your team
• What actions will be taken and when?• How will this be approached?• What resources will be used?
Action plan (who, where, when, what, how)
• State the specific target(s). • How will you prove that you have made a difference?• How will you measure achievement of your goals?
Goal
12 Implementing optimal cancer care pathways forum
Blank plan
Focus area
Current conditions
Problem anaylsis
Background
Below is a blank copy of the plan5 for you to write notes during the forum.
Implementing optimal cancer care pathways forum 13
Proposal
Your team
Action plan (who, where, when, what, how)
Goal
14 Implementing optimal cancer care pathways forum
The report
• Copy from the plan
Original conditions
• Copy from the plan
Problem analysis
• Copy from the plan
Goals
• Copy from the plan
Focus area
The report5 is a tool to help communicate progress towards implementing OCCPs in your setting. On one A3 page you can describe your original plan, overview the actions taken to date, measure progress against your stated aims/objectives and state how your work will evolve in the future. This page also shows the use of all four stages of the PDSA quality improvement cycle.
PLA
N
Implementing optimal cancer care pathways forum 15
• Provide a brief summary of work completed to date
Activities completed and in progress (who, where, when, what, how)
DO• Specify what data and information you have gathered to measure achievement
of your goals• State what changes can be observed
Performance measures
STUDY• What activites will be done next (after this report)?• Describe any changes to your approach• State who will receive this report• State any remaining challenges
Future activities (who, where, when, what, how)
ACT
16 Implementing optimal cancer care pathways forum
Assessing your service
The following pages contain example questions to help assess your area of care. Answering these questions will help complete the “current conditions” and “problem analysis” sections of the 1-page plan. You should select and tailor the questions most relevant to your local needs.
Questions for all stages of the pathway • Are the optimal time frames met for each tumour type?• Is care tailored for populations with special needs, for example Aboriginal and
Torres Strait Islander people, people from Culturally and Linguistically Diverse Backgrounds, older people, adolescents and young adults.
• Are supportive care needs assessed and what supportive care is provided/available?
• Are there any stages of the optimal care pathway where supportive care could be improved?
• Does your service use a validated screening tool (such as the National Comprehensive Cancer Network Distress Thermometer and Problem Checklist)?
Questions to help you define your focus area/s5
• What are you trying to achieve?• What is the problem/project? What are the root causes of the problem?• What does good care look like?• What data do you have to prove there’s a problem?• If you make a change, how will you know it has made an improvement?
Step 1e: Prevention and early detection
Implementing optimal cancer care pathways forum 17
Step 1 - Prevention and early detection
• Are there screening programs for the tumour type/s you are interested in? • If yes, what is the uptake for people in your area? Is there room for
improvement in uptake of proven screening programs?• What prevention activities are undertaken in your local context? What
improvements could be made to services that promote reduction to modifiable risk factors?
• Are there prevention and early detection programs that could be improved?• Are there areas of unmet need for preventative care services?• What services exist for people at increased cancer risk? What is the current
level of service utilisation?• Are there opportunities for better management of people at increased risk?
Step 2 - Presentation, initial investigations and referral

18 Implementing optimal cancer care pathways forum
Step 2 - Presentation, initial investigations and referral
• Are you familiar with the tumour-specific recommended timeframes in the OCCPs?
• What percentage of patients meet the recommended timeframe between referral and first specialist assessment?
• Are systems in place to support rapid access to specialist assessment?• Are there opportunities for improvements toe:
• Referral pathways?• Referral systems?• Referral practices?
• Do referral documents provide the required information?• Are patient/carer needs met in relation to communication aboute:
• Explaining who the patient is being referred to and why?• Support while waiting for the specialist appointment?
Step 3 - Diagnosis, assessment and treatment
planning
Implementing optimal cancer care pathways forum 19
Step 3 - Diagnosis, assessment and treatment planning
• What methods of diagnosis are used for the tumours type/s?• What are the wait times for diagnostic imaging and diagnostic procedures?• What are the timeframes between referral and diagnosis?• What percentage of patients are discussed at a multidisciplinary team (MDT)
meeting?• What percentage of MDT discussions occur prior to the first treatment?• What percentage of MDT discussions are documented, with an agreed
treatment plan written?• What percentage of patients have an agreed, MDT developed treatment plan
provided to the patients GP?• How often does the MDT meeting have all the required members?• To what extent is support offered/provided to develop an advance care plan,
where appropriate?• What percentage of patients are screened for eligibility for clinical trials?• What percentage of patients are enrolled in clinical trials?• What percentage of patients are given written information about their cancer
and their treatment plan?• Are cancer stage and cancer recurrence recorded?• Are patient/carer needs met in relation to communication aboute:
• A timeframe for diagnosis and treatment;• The role of the multidisciplinary team in treatment planning and ongoing
care; and• Appropriate written information or referral to support services required?
Step 4 - Treatment
20 Implementing optimal cancer care pathways forum
Step 4 - Treatment
• Is treatment intent recorded? For example, longer term survival, maintenance of quality of life, symptom palliation.
• What are the wait times fore:• Surgery?• Radiotherapy?• Systemic therapies?• Specialist palliative care?• Supportive care?• Other treatments?
Appropriate dates to measure could include from referral, from decision to treat or from MDT discussion date.
• What are the wait times between treatments?• What are utilisation rates for each treatment type?• What barriers prevent the uptake of treatments where indicated?• Is support offered/provided to develop an advance care plan?• How often is the treatment plan discussed with the patient’s GP?• Are patient/carer needs met in relation to communication aboute:
• Discussing treatment options including intent of treatment, prognosis, treatment risks and benefits; and
• Discussing advance care planning where appropriate?• What type of treatment outcomes are recorded?• What type of treatment outcomes are most important to patients?
Step 5 – Care after initial treatment and recovery

Implementing optimal cancer care pathways forum 21
Step 5 - Care after initial treatment and recovery
• What percentage of patients and their GP receive a treatment summary?• Do treatment summaries appropriately covere:
• Diagnostic tests performed and results?• Tumour characteristics?• Type and date of treatments?• Interventions and treatment plans from other health professionals?• Supportive care services provided?• Contact information for key care providers?
• What percentage of patients have a documented follow-up care plan outlininge:• Medical follow-up required (tests, ongoing surveillance);• Care plans for managing late effects of treatment; and• A process for rapid re-entry to medical services for suspected
recurrence?• Which aspects of follow-up care could be improved?• How often does communication by the lead clinician meet patient/carer needs
in relation toe:• Explaining the treatment summary and follow-up care plan; and• Providing information/support about secondary prevention/healthy living?
• For what percentage of patients does the lead clinician discuss the follow-up care plan with the patient’s GP?
Step 6 – Managing recurrent or progressive disease

22 Implementing optimal cancer care pathways forum
Step 6 - Managing recurrent or progressive disease
• Are there systems in place to support rapid re-entry to specialist care for patients with suspected recurrence?
• What is the wait time for first specialist appointment for patients with a recurrent cancer?
• Do systems support referral to palliative care, based on need, rather than prognosis?
• What percentage of patients are offered support to develop an advance care plan?
• What percentage of patients have an advance care plan?• Is there appropriate support to have end of life discussions with patients and
carers?• What percentage of patients with recurrent/progressive disease are discussed
at a multidisciplinary team meeting?
Step 7 – End-of-life care

Implementing optimal cancer care pathways forum 23
Step 7 - End-of-life care
• What palliative care services exist in your area/setting?• Are systems in place for appropriate referral to specialist palliative care?• Are GPs involved in patients’ palliative care?• What barriers exist that would hinder the uptake of multidisciplinary palliative
care?• Is appropriate support provided to patients who choose home-based
palliative care?• How often does communication meet patient/carer needs in relation toe:
• Being open about the prognosis and discussing palliative care options; and• Establishing a transition plan to ensure patient needs and goals are
addressed in the appropriate environment?
24 Implementing optimal cancer care pathways forum
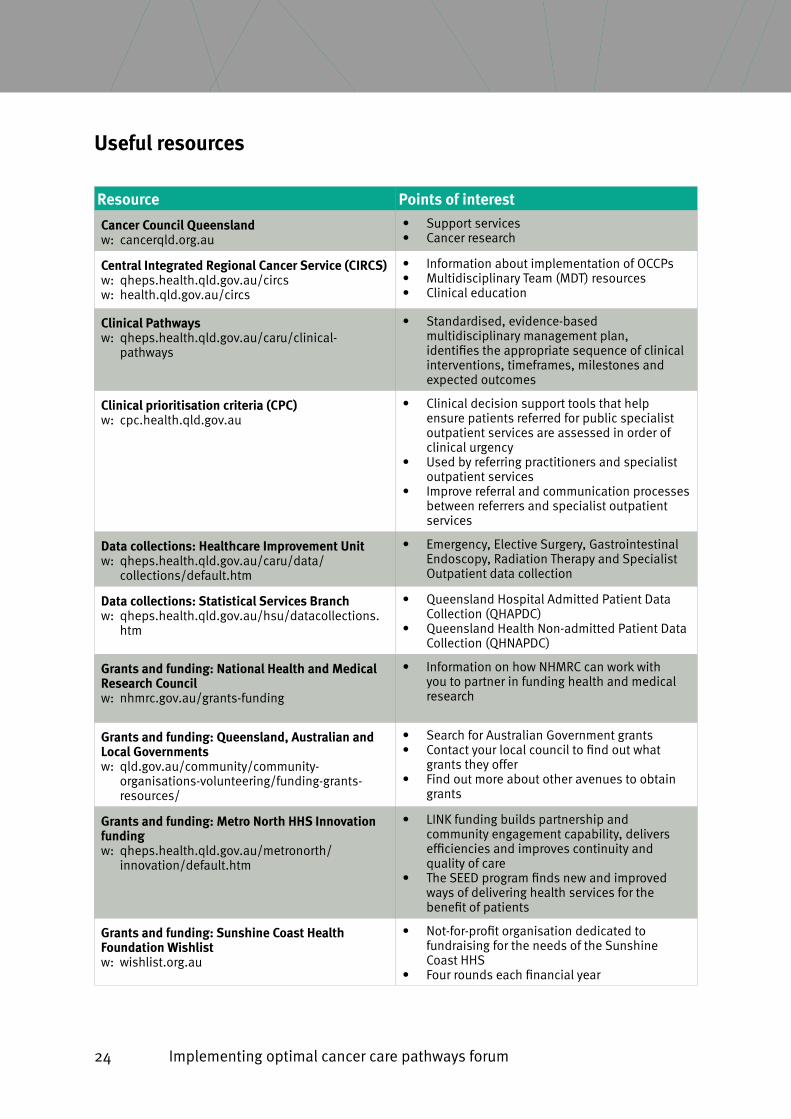
Useful resources
Resource Points of interest
Cancer Council Queenslande:w cancerqld.org.au
• Support services• Cancer research
Central Integrated Regional Cancer Service (CIRCS)e:w qheps.health.qld.gov.au/circse:w health.qld.gov.au/circs
• Information about implementation of OCCPs• Multidisciplinary Team (MDT) resources• Clinical education
Clinical Pathwayse:w qheps.health.qld.gov.au/caru/clinical-
pathways
• Standardised, evidence-based multidisciplinary management plan, identifies the appropriate sequence of clinical interventions, timeframes, milestones and expected outcomes
Clinical prioritisation criteria (CPC)e:w cpc.health.qld.gov.au
• Clinical decision support tools that help ensure patients referred for public specialist outpatient services are assessed in order of clinical urgency
• Used by referring practitioners and specialist outpatient services
• Improve referral and communication processes between referrers and specialist outpatient services
Data collections: Healthcare Improvement Unite:w qheps.health.qld.gov.au/caru/data/
collections/default.htm
• Emergency, Elective Surgery, Gastrointestinal Endoscopy, Radiation Therapy and Specialist Outpatient data collection
Data collections: Statistical Services Branche:w qheps.health.qld.gov.au/hsu/datacollections.
htm
• Queensland Hospital Admitted Patient Data Collection (QHAPDC)
• Queensland Health Non-admitted Patient Data Collection (QHNAPDC)
Grants and funding: National Health and Medical Research Council
e:w nhmrc.gov.au/grants-funding
• Information on how NHMRC can work with you to partner in funding health and medical research
Grants and funding: Queensland, Australian and Local Governments
e:w qld.gov.au/community/community-organisations-volunteering/funding-grants-resources/
• Search for Australian Government grants• Contact your local council to find out what
grants they offer• Find out more about other avenues to obtain
grants
Grants and funding: Metro North HHS Innovation funding
e:w qheps.health.qld.gov.au/metronorth/innovation/default.htm
• LINK funding builds partnership and community engagement capability, delivers efficiencies and improves continuity and quality of care
• The SEED program finds new and improved ways of delivering health services for the benefit of patients
Grants and funding: Sunshine Coast Health Foundation Wishlist
e:w wishlist.org.au
• Not-for-profit organisation dedicated to fundraising for the needs of the Sunshine Coast HHS
• Four rounds each financial year
Implementing optimal cancer care pathways forum 25
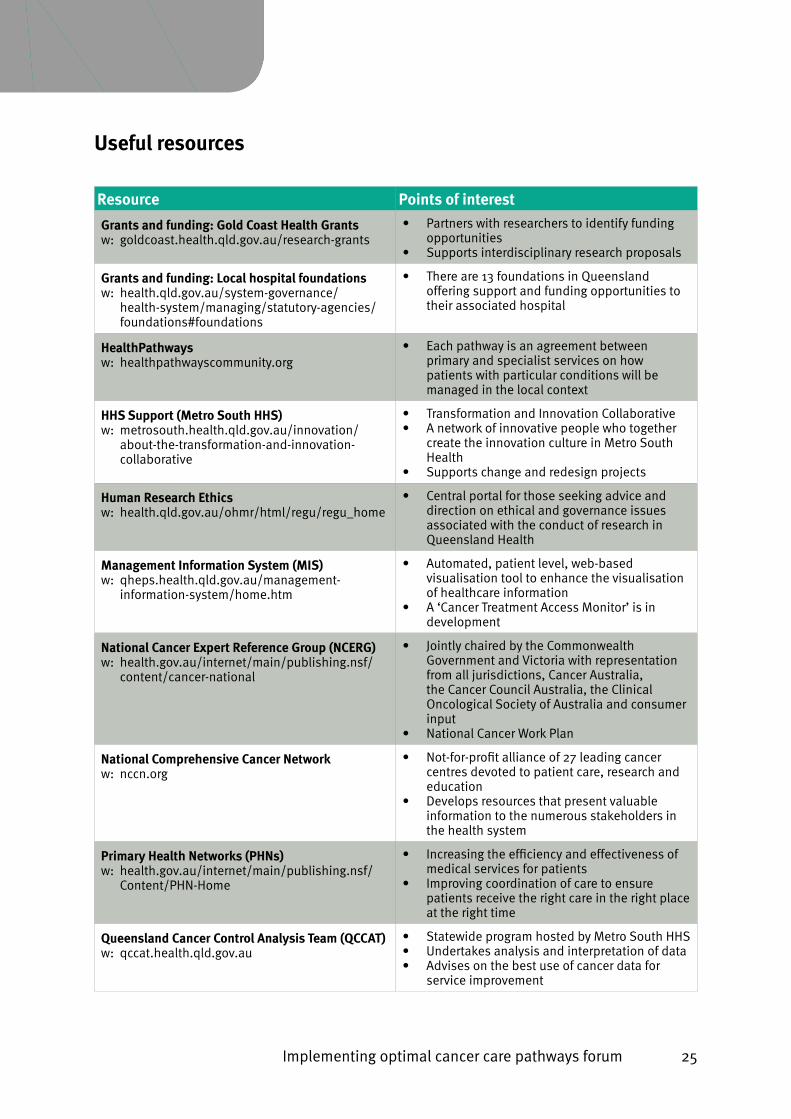
Useful resources
Resource Points of interest
Grants and funding: Gold Coast Health Grantse:w goldcoast.health.qld.gov.au/research-grants
• Partners with researchers to identify funding opportunities
• Supports interdisciplinary research proposals
Grants and funding: Local hospital foundationse:w health.qld.gov.au/system-governance/
health-system/managing/statutory-agencies/foundations#foundations
• There are 13 foundations in Queensland offering support and funding opportunities to their associated hospital
HealthPathwayse:w healthpathwayscommunity.org
• Each pathway is an agreement between primary and specialist services on how patients with particular conditions will be managed in the local context
HHS Support (Metro South HHS) e:w metrosouth.health.qld.gov.au/innovation/
about-the-transformation-and-innovation-collaborative
• Transformation and Innovation Collaborative• A network of innovative people who together
create the innovation culture in Metro South Health
• Supports change and redesign projects
Human Research Ethicse:w health.qld.gov.au/ohmr/html/regu/regu_home
• Central portal for those seeking advice and direction on ethical and governance issues associated with the conduct of research in Queensland Health
Management Information System (MIS)e:w qheps.health.qld.gov.au/management-
information-system/home.htm
• Automated, patient level, web-based visualisation tool to enhance the visualisation of healthcare information
• A ‘Cancer Treatment Access Monitor’ is in development
National Cancer Expert Reference Group (NCERG)e:w health.gov.au/internet/main/publishing.nsf/
content/cancer-national
• Jointly chaired by the Commonwealth Government and Victoria with representation from all jurisdictions, Cancer Australia, the Cancer Council Australia, the Clinical Oncological Society of Australia and consumer input
• National Cancer Work Plan
National Comprehensive Cancer Networke:w nccn.org
• Not-for-profit alliance of 27 leading cancer centres devoted to patient care, research and education
• Develops resources that present valuable information to the numerous stakeholders in the health system
Primary Health Networks (PHNs)e:w health.gov.au/internet/main/publishing.nsf/
Content/PHN-Home
• Increasing the efficiency and effectiveness of medical services for patients
• Improving coordination of care to ensure patients receive the right care in the right place at the right time
Queensland Cancer Control Analysis Team (QCCAT)e:w qccat.health.qld.gov.au
• Statewide program hosted by Metro South HHS• Undertakes analysis and interpretation of data• Advises on the best use of cancer data for
service improvement
26 Implementing optimal cancer care pathways forum
References
1. Cancer Council Victoria. (2017). Optimal Care Pathways. from httpe://www.cancervic.org.au/for-health-professionals/optimal-care-pathways
2. Department of Health. (2016). Factsheete: Why and how to use optimal cancer care pathways. In Department of Health (Ed.). Canberra, Australiae: Australian Government.
3. The Royal Australian College of General Practitioners. (2006). Plan, do, study, act cycle. In J. Litt (Ed.), Putting prevention into practice (Green Book) (2nd ed.). South Melbourne, Victoriae: The Royal Australian College of General Practitioners.
4. The W. Edwards Deming Institute. (2016). PDSA Cycle. from httpse://deming.org/management-system/pdsacycle
5. Lean Enterprise Institute, I. (2010). A3 Template. Cambridge, MA, USAe: Lean Enterprise Institute, Inc.
Implementing optimal cancer care pathways forum 27
Notes
28 Implementing optimal cancer care pathways forum
Notes
Implementing optimal cancer care pathways forum 29
Notes
30 Implementing optimal cancer care pathways forum
Notes
Who are we? Cancer Council Queensland is the state’s leading non-government community organisation in cancer control. Our research shows one in two Queenslanders will be diagnosed with cancer in their lifetime. We’re here to ensure no one goes on a cancer journey alone.
We understand that a cancer diagnosis can have an enormous impact on your patients. Cancer Council Queensland supports all Queenslanders affected by cancer - from patients and their families, caregivers and Health Professionals.
Cancer Council 13 11 20 is a free and confidential service available Monday to Friday 9am – 5pm (excluding public holidays) where your patients can speak to a qualified cancer care professional about anything to do with cancer. We are here to support and work with you and your patients.
The services we offer include;
Emotional support• Speak with a qualified cancer care professional about anything to do with cancer.
• Talk to someone who has had cancer through our peer support network.
• Access our Cancer Counselling Service.
Practical support• Financial and legal assistance.
• Travel and accommodation assistance.
• Access to our wig and turban service.
Access to information – we offer excellent online publications and resources.
What we can do for you?
cancerqld.org.auAll Queenslanders, all cancers