
ASISTM and the Faulkes Telescope Project: Bringing Deep Space into the Classroom.
Upload
lenard-sullivanCategory
view
219download
2
Implementing a K-RAS mutation testing
service for colorectal cancer
Cate FaulkesMolecular Biology DepartmentRoyal Surrey County Hospital
April 2010
Royal Surrey County Hospital NHS Foundation Trust

Van Cutsem et. al. 2009, Karapetis 2008
Colorectal cancer 3rd most common cancer worldwide. Approximately 25% of patients present with
metastatic colorectal cancer (mCRC). Metastatic disease develops in 40-50% of
newly diagnosed patients. Treatment is typically by surgery and
chemotherapy. Now includes EGFR targeted monoclonal
antibodies e.g. cetuximab & panitumumab.

Vincenzi B et. al. 2010, Bardelli & Siena 2010, commons.wikimedia.org
EGFR signalling pathway disrupted by EGFR targeted monoclonal antibodies
EGFR targeted mAbs competitively inhibit ligand binding thus inhibiting the phosphorylation cascade leading to activation of transcription factors.
This therefore inhibits cellular processes such as cell proliferation and migration.
Also has cytotoxic effect via antibody dependent cellular cytotoxicity.

Not everyone with mCRC responds to EGFR targeted therapies
Only 10-20% of tumours respond to EGFR targeted therapy.
35-45% of colorectal tumours have at least one activating mutation in the K-RAS gene, thus constitutively activating cell signalling downstream of EGFR, so resistant to EGFR targeted therapies.

Kareptis et. al. 2008, Chang et. al. 2009, Bardelli, Siena 2009 & Siena 2010
Not everyone with mCRC responds to EGFR targeted therapies
In patients with wild type K-RAS tumours, such drugs double overall and progression free survival rates.
Mutations occur predominantly in codons 12 and 13 and less commonly in codons 61 and 146.
Current NICE guidelines recommend testing for K-RAS mutations in all mCRC cases.
K-RAS mutations don’t explain all non-responders: 5-10% thought to be due to B-RAF mutations, others unexplained.
Without Cetuximab
With Cetuximab
Overall survival rate
Median 4.8 months
Median 9.5 months
Progression free survival rate
Median 1.9 months
Median 3.7 months

Introduction of a K-RAS testing service at RSCH Prior to September 2009 all K-RAS testing
for patients at RSCH was carried out by commercial lab or part of drug trial.
Introduced in-house testing following requests from local oncologists, to improve service to patients, meeting NICE guidelines for treatment.
Rapid turnaround times crucial when making decisions regarding targeted therapies. Samples do not need to be sent away and the results can be made available by LIMS (WinPath).

Methods consideredDideoxy sequencing
Pyrosequencing
High Resolution Melt Analysis (HRM)
DxS TheraScreen® K-RAS mutation kit
Approx sensitivity
20% 5% 5% 1%
CE marked No Yes No Yes
Detects all mutations
Yes Yes Yes No: 7 most common
Cost Mid range Cheap Cheap Expensive
Capital purchase
Yes Yes No but need 2nd method to verify seq changes
No

Why choose DxS TheraScreen® K-RAS mutation kit: mutation frequency
Detects the 7 most common mutations in codons 12 and 13 of K-RAS gene by real time PCR (approx 97%).
Cosmic (www.sanger.ac.uk)
www.shands.org
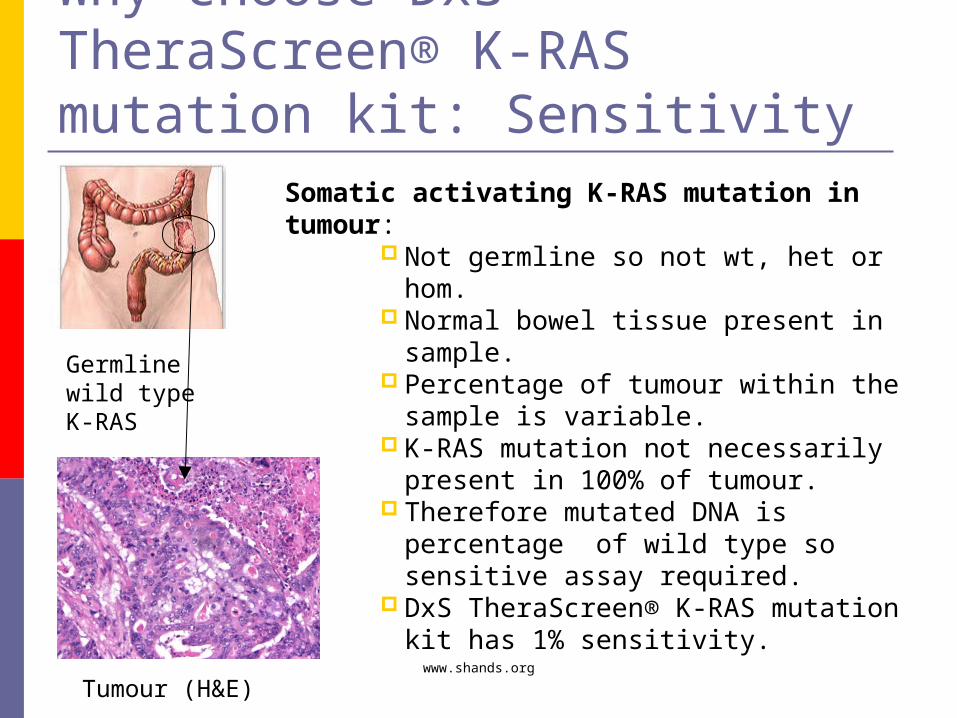
Why choose DxS TheraScreen® K-RAS mutation kit: Sensitivity
Germline wild type K-RAS
Somatic activating K-RAS mutation in tumour:
Not germline so not wt, het or hom. Normal bowel tissue present in
sample. Percentage of tumour within the
sample is variable. K-RAS mutation not necessarily
present in 100% of tumour. Therefore mutated DNA is
percentage of wild type so sensitive assay required.
DxS TheraScreen® K-RAS mutation kit has 1% sensitivity.
Tumour (H&E)

How DxS TheraScreen® K-RAS mutation kit works
1 control assay and 7 mutation assays each with ARMS primers, a FAM labelled Scorpion probe and HEX labelled exogenous control reaction to ensure no inhibition present. Mixed standard is positive control for all assays.
Control assay used to test sample suitability.
7 mutation assays and control assay run simultaneously.
Difference between mutation Ct and control Ct (ΔCt) determines whether sample has K-RAS mutation or is wild type.
ΔCt=1.48
Mixed standards
Sample control assay
Sample 12 VAL

Comparison study Tested 13 samples, 11 of which agreed with results from
other laboratories. Both discrepancies were samples originally tested as wild
type but our assay detected a mutation. 1 non-concordant sample was re-cut and re-extracted then
retested at RSCH and the lab in question. Both results agreed with our original results, showing a mutation.
The other remains unresolved, however may be due to a sensitivity issue as it was originally tested by pyrosequencing and we found a low level mutation.
Conclusion:CE marked kit run on Roche Lightcycler 480 with Adapt software containing algorithms for determining mutation status. Assay was considered fit for purpose.

WorkflowPathologist reviews H&Es, selects appropriate block & ascertains tumour load.
DNA extracted from FFPE tissue using Qiagen DNA mini kit.
Sample assessment protocol (DxS kit) to ascertain DNA suitability.
Mutation detection assay (DxS kit).
Results reported.
Expected turnaround time within 7 working days.

Percentage turnaround times for K-RAS testing at RSCH (37 cases)
87% cases reported within 7 days receipt.
Arrived 23.12.09Low DNA conc- re-extracted QC problem
with kit

K-RAS mutation frequency of 50 patients tested at RSCH (includes comparison study)
38% patients tested carry KRAS mutation which falls within 35-45% K-RAS mutations cited in literature.

Summary DxS kit is a rapid, robust and sensitive method. Our testing service enables treatment choices to
be made as early as possible for the patient. Oncologists are pleased with the shorter turn
around times. If anyone is interested in using our service please
contact Dr Louise Lavender (01483 571122 ext6839, [email protected]).

The Future Develop an HRM method for codons 12
and 13 and test alongside DxS TheraScreen® K-RAS mutation kit.
Any sample wild type by DxS TheraScreen® K-RAS mutation kit, but mutant by HRM confirm by sequencing or pyrosequencing.
Devolop HRM method for codon 61 of K-RAS gene.

Acknowledgements Dr Gary Middleton (Oncologist): patient
samples. Dr Stefano De Sanctis (Histopathologist):
Tumour assessment. Dr Louise Lavender (Head of Molecular
Biology) : Support. Dave Brettle and Bruno Ping: DNA
extraction.

References Van Cutsem E, et al. Cetuximab and chemotherapy as initial
treatment for metastatic colorectal cancer. N Engl J Med. 2009; 360:1408-1417.
Bardelli A & Siena S. Molecular mechanisms of resistance to Cetuximab and Panitumumab in colorectal cancer, J Clin Oncol. 2010;Jan:e published.
Vincenzi B, et al. Cetuximab: From bench to bedside, Curr Cancer Drug Targets. 2010;Jan:e published.
Karapetis CS et al. K-RAS mutations and benefit from cetuximab in advanced colorectal cancer, N Engl J Med. 2008;359:1757-1765.
Chang YS et al. Fast simultaneous detection of K-RAS mutations in colorectal cancer. BMC Cancer. 2009;9:175-185.
Siena S, et al. Biomarkers predicting clinical outcome of epidermal growth factor receptor-targeted therapy in metastatic colorectal cancer. J Natl Cancer Inst. 2009;101:1-17.


















