Implementation of the GMA to Optimize Neonatal Outcomes...
16
4/14/16 1 IMPLEMENTATION OF THE GENERAL MOVEMENTS ASSESSMENT (GMA) TO OPTIMIZE NEONATAL OUTCOMES Megan Iammarino, SPT Madalynn Wendland, PT, DPT, PCS, ATP OBJECTIVES Understand the purpose and method for administration of the General Movements Assessment (GMA) Recognize the importance for early identification of neurologic impairments Compare the psychometric properties of different neurologic assessments used in early infancy Identify clinical practice changes with implementation of the GMA at Cleveland Clinic Children’s Hospital for Rehabilitation (CCCHR) Describe how knowledge translation and knowledge brokering can be used to optimize implementation of the GMA IDENTIFYING A NEED In the US, the incidence of preterm birth is 1 out of 10 infants 1 Prevalence of survival for very pre-term birth, <32 weeks post-menstrual age (PMA) has increased to >85% 2 Despite advances in perinatal care, 50% of these infants experience neurobehavioral impairments 2 Neurological impairments are often missed, or diagnosis is delayed due to poor predictive validity of traditional neurological examination and brain imaging techniques 3,4
Transcript of Implementation of the GMA to Optimize Neonatal Outcomes...

4/14/16
1
IMPLEMENTATION OF THE GENERAL MOVEMENTS ASSESSMENT (GMA) TO OPTIMIZE NEONATAL OUTCOMES
Megan Iammarino, SPT Madalynn Wendland, PT, DPT, PCS, ATP
OBJECTIVES
¢ Understand the purpose and method for administration of the General Movements Assessment (GMA)
¢ Recognize the importance for early identification of neurologic impairments
¢ Compare the psychometric properties of different neurologic assessments used in early infancy
¢ Identify clinical practice changes with implementation of the GMA at Cleveland Clinic Children’s Hospital for Rehabilitation (CCCHR)
¢ Describe how knowledge translation and knowledge brokering can be used to optimize implementation of the GMA
IDENTIFYING A NEED
¢ In the US, the incidence of preterm birth is 1 out of 10 infants1 � Prevalence of survival for very pre-term birth, <32
weeks post-menstrual age (PMA) has increased to >85%2
� Despite advances in perinatal care, 50% of these infants experience neurobehavioral impairments2
¢ Neurological impairments are often missed, or diagnosis is delayed due to poor predictive validity of traditional neurological examination and brain imaging techniques3,4

4/14/16
2
FINDING AN EVIDENCE-BASED SOLUTION5
¢ Heinz Prechtl ¢ Developmental neurologist ¢ 1970’s – Working on developing a standardized
method for a neonatal neurological examination � Recognition of patterned fetal motor behavior � Observed high-risk infants moved differently when
compared to typically developing infants
¢ 1990’s – Development of General Movements Assessment � A new approach to assessing the young nervous
system using spontaneous movements
“SPONTANEOUS MOTILITY, AS THE EXPRESSION OF SPONTANEOUS NEURAL ACTIVITY, IS AN EXCELLENT MARKER OF NEURAL DYSFUNCTION CAUSED BY BRAIN IMPAIRMENT”6
…A WINDOW INTO THE BRAIN!
PRECHTL’S GENERAL MOVEMENT ASSESSMENT (GMA)
¢ An qualitative method of assessing the integrity of the developing nervous system, through the categorization of endogenously generated movement patterns in infants aged 26 weeks PMA to ~20 weeks post-term age (PTA)6
¢ Utilizes a trained observer’s Gestalt perception to assess and identify infants at risk for cerebral palsy and other developmental disabilities3,6-10 � ADHD, Autism Spectrum disorders, Rett syndrome

4/14/16
3
HO
W IS Y
OU
R GE
ST
AL
T? DEFINING A GENERAL MOVEMENT11
ANALYZING AT DIFFERENT AGES6

4/14/16
4
CASE EXAMPLE AT 2 WEEKS PTA
Normal Writhing GMs Cramped Synchronized GMs
CASE EXAMPLE AT 16 WEEKS PTA
Normal Fidgety GMs Absent Fidgety GMs
UTILIZING A DEVELOPMENTAL TRAJECTORY
F-‐ F-‐
AF
CS CS
Ch
PR
H
N
40 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Weeks Pos;erm Age
Writhing Movements
FMs + or +/-‐ FMs ++ or + éé

4/14/16
5
EFFECTING CHANGE12-14
24 weeks post-conception 40 weeks post-conception
WHAT ABOUT PRUNING?12-14
‘TRACT’-ING CHANGES12-15

4/14/16
6
CATS!!15,16
APPLYING TO REAL LIFE: AMBLYOPIA16
¢ Babies with amblyopia will fail to develop full acuity with depth perception if the problem is not corrected
¢ Using a patch minimizes competition of space for developing neural pathways from good eye
¢ Without intervention, the neural pathways associated with the good eye continue to strengthen and begin to displace weaker pathways connecting the weak eye, making that eye weaker
COMPARING GMA TO OTHER EXAMINATION TECHNIQUES7,10,17-19
Assessment Tool Sensitivity (%) Specificity (%)
General Movement Assessment
93-100 82-100
Magnetic Resonance Imaging
60-100 89-99
Cranial Ultrasound 74-80 83-‐97
Standard Neurological Examination
57-86 (Preterm) 68-‐96 (Term age)
45-‐83 (Preterm) 52-‐97 (Term age)

4/14/16
7
SHIFTING AWAY FROM TRADITIONAL NEUROLOGICAL EXAM6,11
¢ Sherrington’s work demonstrated that decerebrated animals respond reflexively to external stimulation
¢ If reflexive movement can be elicited in decerebrated animals, why rely on these reactions to tell us about the integrity of cortical functioning?
¢ Spontaneous activity is more sensitive an indicator of brain dysfunction than reactivity to sensory stimuli in reflex testing17
CONSIDERATIONS FOR THE PRACTICING PT2,20
GMA TIMP
Age Range 26 weeks – 5 months 32 weeks – 4 months
Stated Purpose
Documents spontaneous
movements to identify early CNS dysfunction
Evaluates motor control and organization of
posture and movement for functional activities
Components Tested
Spontaneous Movements
Both spontaneous behaviors (13 items)
and elicited behaviors (29 items)
Psychometric Properties
Criterion referenced 93-100% (sensitivity) 82-100 (specificity)
Norm referenced 62.5% (sensitivity) 77.4% (specificity)
ADMINISTERING THE GMA
¢ Non-invasive, global-visual Gestalt perspective minimizes the need for handling3,21,22
¢ One of the only assessments to categorize the quality of movement patterns observed6,23
The GMA stands out as one of the most cost-effective and sensitive tools available for prediction of long-term neurobehavioral
impairments that allows for early implementation of targeted interventions

4/14/16
8
CASE EXAMPLE AT 2 ½ YEARS OF AGE
CHANGING PRACTICES: SUMMARIZING OUR CASE
¢ Discharged from NICU after 39 days
¢ Term writhing video taken at 2 weeks PTA with subsequent referral to outpatient PT and Early Intervention Services
¢ Fidgety video taken at 16 weeks PTA (as part of outpatient PT visit) with subsequent referral to OT
¢ Current medical team includes: Neurology, Pediatric Physiatry, OT, PT and Early Intervention Providers
¢ Current medical management includes: � Oral baclofen � Botox injections � Equipment � Microcurrent
¢ Current functional abilities: � Began walking at 29 months � Still limited in play, self-care
and dressing skills ¢ Expected to participate in a
structured Constraint Induced Movement Therapy program this summer
HOW DID WE GET HERE?24 USING A KNOWLEDGE-TO-ACTION FRAMEWORK
¢ Identification of a clinical problem ¢ Obtaining administrative support ¢ Having ready access to knowledge materials ¢ Ongoing engagement with a knowledge broker ¢ Providing multi-faceted educational strategies

4/14/16
9
IDENTIFYING A TWO-PART PROBLEM
PROBLEM PART 1: DECIDING WHEN THE GMA IS NECESSARY
¢ Review of medical history ¢ Therapist observation of
atypical movement patterns during routine care � OT and PT receive automatic
referrals for high-risk infants or infants < 34 weeks PMA
PROBLEM PART 2: GETTING BUY IN
¢ Introducing the GMA to NICU leadership:
� Presentation of evidence to the Medical Director of Neonatology
� Presentation to the entire Neonatology Enterprise
¢ 3 NICUs in the Cleveland Clinic Health System
� Organization of regional presentation by Colleen Peyton PT, DPT, PCS University of Chicago Medicine, Comers Children’s Hospital
¢ Over 50 therapists, physicians, nurse practitioners and nurses attended this event

4/14/16
10
OBTAINING ADMINISTRATIVE SUPPORT
� Review of protocol
� Identifying logistical barriers
¢ Video consent
¢ Documentation templates
¢ Billing procedures
ACKNOWLEDGING DIFFERENCES IN DIFFERENT SETTINGS
¢ Videos taken prior to discharge during the pre-term writhing and/or the writhing phase
¢ Observation of movements help guide discharge planning
¢ Education is provided to the health care team, including the family
¢ Videos taken in the term writhing and fidgety phase
¢ Small part of overall assessment in terms of time spent during patient encounter
¢ Education provided to family with referrals made to other health care professionals as appropriate
NICU Outpatient
PREPARING FOR IMPLEMENTATION
¢ Equipment � Video camera and tripod � Memory card reader
¢ Storage � Physical and digital
4/14/16
11
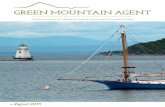
ENSURING ACCURATE RESULT6,18 Requirements Age Conditions
Preferred Behavioral
State
Any age • No crying, no NNS
< 36 weeks PMA • Quiet alert state*
> 36 weeks PMA • Quiet alert state
Position Any age • Supine on flat surface
Clothing Any age • No clothes with small diaper
Environment Any age • Neutral temperature, sound, lighting.
• Avoid engaging with baby during recording
• Use a tripod
HAVING READY ACCESS TO KNOWLEDGE MATERIALS25
¢ Knowledge Translation defined: � A dynamic process by which relevant research
information is made available and accessible to optimize practice.
¢ Strategies to transfer knowledge � Distributing educational materials/conference
presentations � Building a community of practice � Integrating content into academic curriculum
CREATING A NEW, EVIDENCE-BASED CLINICAL STANDARD OF PRACTICE
¢ If abnormal GMs are observed during NICU stay, infant is referred to NICU Transition Clinic
¢ Order written for OT/PT while in NICU � Families leave NICU with appointment in hand à
improved compliance with keeping appointments
¢ First appointment in NICU Transition Clinic prior to 6 weeks PTA for term writhing video vs. NICU follow-up clinic at ~4 months corrected age

4/14/16
12
ARRANGING THE OUTPATIENT VISIT
¢ Patient Services Representative follows-up with family prior to first appointment
¢ Evaluating therapist is scheduled on a rotating basis � If infant has discipline specific needs, appointment is
schedule accordingly
¢ NICU Transition Clinic held in outpatient therapy satellite � Helps with compliance if ongoing outpatient therapy is
recommended � Many referrals for ongoing outpatient services are made
after 13-15 weeks PTA (fidgety stage)
CHECKING IN WITH A KNOWLEDGE BROKER: ASSESSING IF IT IS MAKING A DIFFERENCE24,26
¢ Knowledge Broker defined: � A person who fills a role
to make research and practice more accessible to each other
¢ Changes of clinical practices began with an individual à organization à structure
0
5
10
15
20
25
30
35
40
45
50
55
Sep 2013-Aug 2014 Sep 2014-Aug 2015 Sep 2015- Feb 2016
MONTHLY NICU ADMISSION RATES AND
NUMBER OF GMA VISITS
NICU GMA Outpatient GMA NICU Admissions

4/14/16
13
PROVIDING MULTI-FACETED EDUCATION
GETTING TRAINED
� Course runs ~3.5 day
¢ Basic Certification
¢ Registration: ~$895
¢ Advanced Certification
¢ Registration: ~ $950
For more information: http://general-movements-trust.info/
47/dates
¢ Course runs ~2 days � General Movements
Assessment Certification
¢ Registration: ~$700
� Infant Motor Profile Course
¢ Registration: ~$425
For more information:
www.developmentalneurology.com
General Movements Trust Hadders-Algra
DEVELOPING A PROGRAM FOR NICU GRADUATES
¢ GMA Certification for outpatient therapists
¢ Development of clinical skills specific to treating NICU graduates: � Targeted continuing education,
mentoring, collaboration with NICU therapists
¢ NICU Family Support Group: Highest risk infants being followed in NICU Transition Clinic or Outpatient Therapy

4/14/16
14
BUILDING A COMMUNITY OF PRACTICE
¢ When possible, have more than one person on your team trained
¢ Find out who in your region is certified
� GMA Pow-Wows to maximize reliability post-certification
¢ Seek out advanced training once you have some practice6,22
¢ Provide opportunities to engage professional students and develop a mutually beneficially educational-clinical relationship
EDUCATING STUDENTS
¢ Doctor of Physical Therapy programs are tasked
with educating students as generalists27
¢ Providing detailed content regarding specialty
areas (including practice in the NICU) is often limited
¢ As part of a didactic evidence-based curriculum, Cleveland State University Doctor of Physical Therapy students are educated on the GMA
MAXIMIZING EDUCATIONAL POTENTIAL28

4/14/16
15
GETTING INVOLVED!
¢ Assisted in creation of IRB
¢ Created videotaping protocol documents
¢ Obtained basic certification through GM Trust
¢ Knowledge translation � In-service during clinical
affiliation � Involvement in local and
national conferences ¢ Professional development
¢ Review current literature and update annotated bibliography
¢ Input data into research registry
¢ Organize and attend GMA Pow-Wows for local practicing clinicians
¢ Establish protocol for tracking sheet
¢ More knowledge translation!
Personal Accomplishments:
Other Available Opportunities:
IN SUMMARY:
¢ The GMA is a cost-effective, objective assessment tool that can accurately identify neonates at risk for neurobehavioral sequelae
¢ Translation of knowledge surrounding the benefits of using the GMA helps streamline implementation of the GMA as a clinical standard of care
¢ The babies you see will thank you, as initiating early-targeted interventions can maximize long-term function and minimize disability
QU
ES
TIO
NS?

4/14/16
16
REFERENCES 1. Reproductive Health: Preterm Birth. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/reproductivehealth/maternalinfanthealth/pretermbirth.htm. Updated: December 4, 2015. Accessed April 3, 2016. 2. Noble Y, Boyd R. Neonatal assessments for the preterm infant up to 4 months corrected age: a systematic review. Developmental Medicine & Child Neurology. 2012; 54(2) 129-139. 3. Burger M, Louw Q. The predictive validity of general movements- a systematic review. European Journal of Paediatric Neurology. 2009; 13:408-420. doi: 10.1016/j.ejpn.2008.09.004 4. Einspieler C, Marschik P, Bos A, Cioni F, Prechtl HFR. Early markers for cerebral palsy: insights from the assessment of general movements. Future Neurol. 2012; 7(6): 709-717. doi: 10.2217/FNL.12.60
5. Einspieler CHeinz F. R. Prechtl (1927-2014). Official Website of the International Child Neurology Association. http://icnapedia.org/explore/articles/news/entry/2014/07/17/heinz-f-r-prechtl-1927-2014. Published July 17,2014. Accessed March 22, 2016. 6. Einspieler C, Prechtl HF. Prechtl's assessment of general movements: A diagnostic tool for the functional assessment of the young nervous system. Ment Retard Dev Disabil Res Rev. 2005;11(1):61-67. 7. Bosanquet M, Copeland L, Ware R, Boyd R. A systematic review of tests to predict cerebral palsy in young children. Developmental Medicine & Child Neurology. 2013;55(5):418-426. 8. Einspieler C, Sigafoos J, Bartl-Pokorny KD, Landa R, Marschik PB, Bölte S. Highlighting the first 5 months of life: General movements in infants later diagnosed with autism spectrum disorder or rett syndrome. Research in Autism Spectrum Disorders. 2014;8(3):286-291. 9. Hadders‐Algra M, MC Groothuis A. Quality of general movements in infancy is related to neurological dysfunction, ADHD, and aggressive behaviour. Developmental Medicine & Child Neurology. 1999;41(6):381-391. 10. Spittle AJ, Boyd RN, Inder TE, Doyle LW. Predicting motor development in very preterm infants at 12 months' corrected age: the role of qualitative magnetic resonance imaging and general movements assessments. Pediatrics 2009; 123:512-517.
11. Einspieler C, Prayer D, Prechtl. Fetal Behaviour: A Neurodevelopmental Approach. London: Mac Keith Press; 2012. 12. Eyre J. Corticospinal tract development and its plasticity after perinatal injury. Neuroscience & Biobehavioral Reviews. 2007;31(8):1136-1149. 13. Martin JH. The corticospinal system: From development to motor control. Neuroscientist. 2005;11(2):161-173. 14. Stiles J, Jernigan TL. The basics of brain development. Neuropsychol Rev. 2010; 20: 327-348. doi: 10.1007/s11065-010-9148-4
REFERENCES- CONTINUED 15. Friel KM, Chakrabarty S, Martin JH. Pathophysiological mechanisms of impaired limb use and repair strategies for motor systems after unilateral injury of the developing brain. Developmental Medicine & Child Neurology. 2013;55(s4):27-31. 16. Martin JH, Chakrabarty S, Friel KM. Harnessing activity-dependent plasticity to repair the damaged corticospinal tract in an animal model of cerebral palsy. Developmental Medicine and Child Neurology. 2011; 53(4): 9-13
17. Ferrari F, Cioni G, Einspieler C, Roversi MF, Bos AF, Paolicelli PB. Cramped synchronized movement in preterm infants as early marker for cerebral palsy. Arch. Pediatric Adolescent Medicine. 156, 460-467 (2002).
18. Spittle AJ, Doyle LW, Boyd RN. A systematic review of the clinimetric properties of neuromotor assessments for preterm infants during the first year of life. Developmental Medicine & Child Neurology. 2008;50(4):254-266. 19. Spittle AJ, Spencer-Smith MM, Cheong JL, et al. General movements in very preterm children and neurodevelopment at 2 and 4 years. Pediatrics. 2013;132(2):e452-8. 20. Snider LM, Majnemer A, Mazer B, Campbell S, Bos AF. A comparison of the general movements assessment with traditional approaches to newborn and infant assessment: Concurrent validity. Early Hum Dev. 2008;84(5):297-303.
21. Byrne E, Campbell SK. Physical therapy observation and assessment in the neonatal intensive care unit. Phys Occup Ther Pediatr. 2013; 33(1): 39-74
22. Einspieler C, Marschik PB, Prechtl HFR. Human motor behavior. Prenatal origin and early postnatal development. J Psychol. 2008; 216(3): 148-154. doi: 10.1027/0044-3409.216.3.148 23. Hadders-Algra M. Evaluation of motor function in young infants by means of the assessment of general movements: a review. Pediatric Physical Therapy. 2001: (13)1: 27-36 24. Schreiber J, Marchetti GF, Racicot B, Kaminski E. The use of a knowledge translation program to increase use of standardized outcome measures in an outpatient pediatric physical therapy clinic: administrative case report. Phys Ther. 2015; 95: 613-629.
25. Knoweldge translation in physical therapy: from theory to practice. Zidarov D, Thoms A, Poissant L. Disabil and Rehabil. 2013; 35(18): 1571-1577. doi: 10.3109/09638288.2012.748841. 26. Ward V, House A, Hamar S. Knowledge Brokering: The missing link in the evidence to action chain. Evid Policy. 2009; 5(3): 267–279. doi:10.1332/174426409X463811. 27. Schreiber J, Goodgold S, Moerchen V, Remec N, Aaron C, Kreger A. A description of professional pediatric physical therapy education. Pediatric Physical Therapy: The Official Publication Of The Section On Pediatrics Of The American Physical Therapy Association [serial online]. 2011 Summer 2011;23(2):201-204.
28. Blumberg P. Maximizing learning through course alignment and experience with different types of knowledge. Innov High Educ. (2009); 34: 93-103. doi: 10.1007/s10755-009-9095-2.