Implant Retained Overdenture: Two-way Approach … · Continued bone loss in edentulous patients...
5
518 Journal of International Oral Health 2016; 8(4):518-522 Implant retained overdenture … Gupta H et al Case Report Received: 18 th November 2015 Accepted: 13 th February 2016 Conflicts of Interest: None Source of Support: Nil Implant Retained Overdenture: Two-way Approach (Case Study) Himanshu Gupta 1 , Sarita Aneja 1 , Milan Preet Singh 2 , Harshdeep Kaur 3 , Richa Singh Sengar 2 , Palak Gupta 4 Contributors: 1 Reader, Department of Prosthodontics, Maharaja Ganga Singh Dental College and Research Centre, Ganganagar, Rajasthan, India; 2 Post-graduate Student, Department of Prosthodontics, Maharaja Ganga Singh Dental College and Research Centre, Ganganagar, Rajasthan, India; 3 Post-graduate Student, Department of Prosthodontics, Surendera Dental College and Research Institute, Ganganagar, Rajasthan, India; 4 Post-graduate Student, Department of Orthodontics, Maharaja Ganga Singh Dental College and Research Centre, Ganganagar, Rajasthan, India. Correspondence: Dr. Aneja S. Department of Prosthodontics, Maharaja Ganga Singh Dental College and Research Centre, Ganganagar, Rajasthan, India. Email: [email protected] How to cite the article: Gupta H, Aneja S, Singh MP, Kaur H, Sengar RS, Gupta P. Implant retained overdenture: Two-way approach (case study). J Int Oral Health 2016;8(4):518-522. Abstract: Continued bone loss in edentulous patients causes a great challenge in prosthetic rehabilitation by conventional denture. Retention has been the most problematic area for mandibular complete denture especially when compared to maxillary complete denture, but retention and stability are greatly compromised in conventional dentures, especially if mandibular ridge is severely resorbed. Osseointegrated dental implants have been proven as a successful treatment modality while prescribing prosthodontic services to an edentulous patient. The predictability of the implant supported prosthesis has been established, and several techniques are present for successful restoration depending on the number of implants, bone quality, bone quantity, prosthesis movement, economical constraints, patients desires, etc. However, in cases of advanced ridge restoration in which facial tissue support is needed from the flanges of the prosthesis or when a removable type of prosthesis is preferred by the patient, an implant supported prosthesis is indicated. This case report describes the two techniques of mandibular implant retained overdenture fabrication, i.e., surgical driven implantology and prosthetically driven implantology. In surgical driven implantology, the implants were placed according to the available bone in the interforaminal region with the help of an orthopantogram which gives us two dimensional view, whereas in prosthetically driven implantology the implants were placed at the canine positions with the help of a duplicated prefabricated denture, which was then modified as a radiographic stent and surgical guide. A dentascan was made with the radiographic stent in position intraorally and the appropriate angulation was determined for the third dimension of implant angulation and then converted into a surgical guide to guide our implant placement. Key Words: Bone, edentulous, implant, mandible, overdenture, retention Introduction Osseointegrated dental implants are aesthetic, functional, and successful prosthesis for edentulous patients. The overdenture resolve speech and lip support problems. There are wide varied of implant supported prosthodontic rehabilitation options for the edentulous mandible. Treatment alternatives for edentulous mandible include (1) implant-supported fixed partial dentures, (2) implant-retained overdentures, and (3) implant-supported overdentures. 1 The advantage of implant retained overdenture are; ease for oral hygiene procedures; 2 control of denture movement enhancing function and phonetics; 3 the overdenture can be removed at bedtime to reduce effect of nocturnal parafunction; and increased masticatory efficiency, 4,5 increased maximum myoelectric output, higher jaw-closing force, and less age-related bone loss after implant-supported prosthetic reconstructions 6-12 than with a conventional complete denture. 13 The 10-year survival rates of implants to support mandibular overdenture tended to be slightly higher than survival rates of endosseous implants in the mandible used to support fixed full-arch bridges, fixed partial dentures or single crowns. 14 100% survival rate were seen under study conducted by Haraldson et al.; 15 Naert et al.; 16 ten Bruggenkate et al. 17 and least were seen by Engquist 18 87% and Versteegh et al. 19 74.8%. Based on the 2002 MacGill Consensus Statement on overdentures, two-implant overdenture is considered the standard of care for edentulous patients. 20 Bars, balls and magnets are various types of connector recommended for the procedures. Locators are type of connectors provide accurate seating of implant supported overdenture. However, ball socket connectors are simple, effective and getting more acceptability. Magnets and ball are less expensive than locators and telescopic crowns. Chewing comforts and patient satisfaction is low with magnetic connectors. 21,22 This article describes two different methods to fabricate two-implant supported overdentures using ball and socket attachment. Two healthy male patients medically and psychologically suited for implant surgery were selected. In the first case, mandibular denture was fabricated and, later on, implants were placed. While in the second case, initially implants were placed followed by fabrication of denture. Case Reports Case 1 A 58-year-old male reported with the chief complain of missing teeth in both upper and lower jaw with difficulty in Doi: 10.2047/jioh-08-04-22
Transcript of Implant Retained Overdenture: Two-way Approach … · Continued bone loss in edentulous patients...

518
Journal of International Oral Health 2016; 8(4):518-522Implant retained overdenture … Gupta H et al
Case ReportReceived: 18th November 2015 Accepted: 13th February 2016 Conflicts of Interest: None
Source of Support: Nil
Implant Retained Overdenture: Two-way Approach (Case Study)Himanshu Gupta1, Sarita Aneja1, Milan Preet Singh2, Harshdeep Kaur3, Richa Singh Sengar2, Palak Gupta4
Contributors:1Reader, Department of Prosthodontics, Maharaja Ganga Singh Dental College and Research Centre, Ganganagar, Rajasthan, India; 2Post-graduate Student, Department of Prosthodontics, Maharaja Ganga Singh Dental College and Research Centre, Ganganagar, Rajasthan, India; 3Post-graduate Student, Department of Prosthodontics, Surendera Dental College and Research Institute, Ganganagar, Rajasthan, India; 4Post-graduate Student, Department of Orthodontics, Maharaja Ganga Singh Dental College and Research Centre, Ganganagar, Rajasthan, India.Correspondence:Dr. Aneja S. Department of Prosthodontics, Maharaja Ganga Singh Dental College and Research Centre, Ganganagar, Rajasthan, India. Email: [email protected] to cite the article:Gupta H, Aneja S, Singh MP, Kaur H, Sengar RS, Gupta P. Implant retained overdenture: Two-way approach (case study). J Int Oral Health 2016;8(4):518-522.Abstract:Continued bone loss in edentulous patients causes a great challenge in prosthetic rehabilitation by conventional denture. Retention has been the most problematic area for mandibular complete denture especially when compared to maxillary complete denture, but retention and stability are greatly compromised in conventional dentures, especially if mandibular ridge is severely resorbed. Osseointegrated dental implants have been proven as a successful treatment modality while prescribing prosthodontic services to an edentulous patient. The predictability of the implant supported prosthesis has been established, and several techniques are present for successful restoration depending on the number of implants, bone quality, bone quantity, prosthesis movement, economical constraints, patients desires, etc. However, in cases of advanced ridge restoration in which facial tissue support is needed from the flanges of the prosthesis or when a removable type of prosthesis is preferred by the patient, an implant supported prosthesis is indicated. This case report describes the two techniques of mandibular implant retained overdenture fabrication, i.e., surgical driven implantology and prosthetically driven implantology. In surgical driven implantology, the implants were placed according to the available bone in the interforaminal region with the help of an orthopantogram which gives us two dimensional view, whereas in prosthetically driven implantology the implants were placed at the canine positions with the help of a duplicated prefabricated denture, which was then modified as a radiographic stent and surgical guide. A dentascan was made with the radiographic stent in position intraorally and the appropriate angulation was determined for the third dimension of implant angulation and then converted into a surgical guide to guide our implant placement.
Key Words: Bone, edentulous, implant, mandible, overdenture, retention
IntroductionOsseointegrated dental implants are aesthetic, functional, and successful prosthesis for edentulous patients. The overdenture resolve speech and lip support problems. There are wide varied of implant supported prosthodontic rehabilitation options for the edentulous mandible. Treatment alternatives for edentulous mandible include (1) implant-supported fixed partial dentures, (2) implant-retained overdentures, and (3) implant-supported overdentures.1 The advantage of implant retained overdenture are; ease for oral hygiene procedures;2 control of denture movement enhancing function and phonetics;3 the overdenture can be removed at bedtime to reduce effect of nocturnal parafunction; and increased masticatory efficiency,4,5 increased maximum myoelectric output, higher jaw-closing force, and less age-related bone loss after implant-supported prosthetic reconstructions6-12 than with a conventional complete denture.13 The 10-year survival rates of implants to support mandibular overdenture tended to be slightly higher than survival rates of endosseous implants in the mandible used to support fixed full-arch bridges, fixed partial dentures or single crowns.14 100% survival rate were seen under study conducted by Haraldson et al.;15 Naert et al.;16 ten Bruggenkate et al.17 and least were seen by Engquist18 87% and Versteegh et al.19 74.8%.
Based on the 2002 MacGill Consensus Statement on overdentures, two-implant overdenture is considered the standard of care for edentulous patients.20 Bars, balls and magnets are various types of connector recommended for the procedures. Locators are type of connectors provide accurate seating of implant supported overdenture. However, ball socket connectors are simple, effective and getting more acceptability. Magnets and ball are less expensive than locators and telescopic crowns. Chewing comforts and patient satisfaction is low with magnetic connectors.21,22
This article describes two different methods to fabricate two-implant supported overdentures using ball and socket attachment. Two healthy male patients medically and psychologically suited for implant surgery were selected. In the first case, mandibular denture was fabricated and, later on, implants were placed. While in the second case, initially implants were placed followed by fabrication of denture.
Case ReportsCase 1A 58-year-old male reported with the chief complain of missing teeth in both upper and lower jaw with difficulty in
Doi: 10.2047/jioh-08-04-22
519
Journal of International Oral Health 2016; 8(4):518-522Implant retained overdenture … Gupta H et al
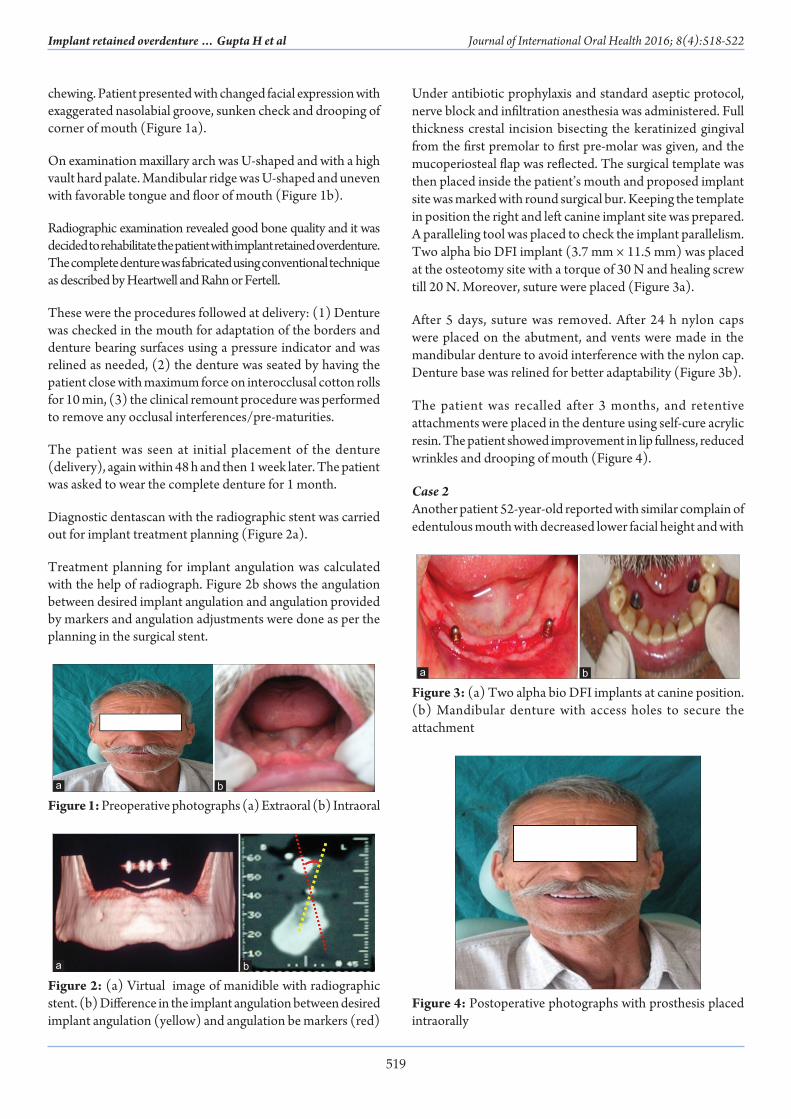
chewing. Patient presented with changed facial expression with exaggerated nasolabial groove, sunken check and drooping of corner of mouth (Figure 1a).
On examination maxillary arch was U-shaped and with a high vault hard palate. Mandibular ridge was U-shaped and uneven with favorable tongue and floor of mouth (Figure 1b).
Radiographic examination revealed good bone quality and it was decided to rehabilitate the patient with implant retained overdenture. The complete denture was fabricated using conventional technique as described by Heartwell and Rahn or Fertell.
These were the procedures followed at delivery: (1) Denture was checked in the mouth for adaptation of the borders and denture bearing surfaces using a pressure indicator and was relined as needed, (2) the denture was seated by having the patient close with maximum force on interocclusal cotton rolls for 10 min, (3) the clinical remount procedure was performed to remove any occlusal interferences/pre-maturities.
The patient was seen at initial placement of the denture (delivery), again within 48 h and then 1 week later. The patient was asked to wear the complete denture for 1 month.
Diagnostic dentascan with the radiographic stent was carried out for implant treatment planning (Figure 2a).
Treatment planning for implant angulation was calculated with the help of radiograph. Figure 2b shows the angulation between desired implant angulation and angulation provided by markers and angulation adjustments were done as per the planning in the surgical stent.
Under antibiotic prophylaxis and standard aseptic protocol, nerve block and infiltration anesthesia was administered. Full thickness crestal incision bisecting the keratinized gingival from the first premolar to first pre-molar was given, and the mucoperiosteal flap was reflected. The surgical template was then placed inside the patient’s mouth and proposed implant site was marked with round surgical bur. Keeping the template in position the right and left canine implant site was prepared. A paralleling tool was placed to check the implant parallelism. Two alpha bio DFI implant (3.7 mm × 11.5 mm) was placed at the osteotomy site with a torque of 30 N and healing screw till 20 N. Moreover, suture were placed (Figure 3a).
After 5 days, suture was removed. After 24 h nylon caps were placed on the abutment, and vents were made in the mandibular denture to avoid interference with the nylon cap. Denture base was relined for better adaptability (Figure 3b).
The patient was recalled after 3 months, and retentive attachments were placed in the denture using self-cure acrylic resin. The patient showed improvement in lip fullness, reduced wrinkles and drooping of mouth (Figure 4).
Case 2Another patient 52-year-old reported with similar complain of edentulous mouth with decreased lower facial height and with
Figure 4: Postoperative photographs with prosthesis placed intraorally
Figure 1: Preoperative photographs (a) Extraoral (b) Intraoralba
Figure 2: (a) Virtual image of manidible with radiographic stent. (b) Difference in the implant angulation between desired implant angulation (yellow) and angulation be markers (red)
ba
Figure 3: (a) Two alpha bio DFI implants at canine position. (b) Mandibular denture with access holes to secure the attachment
ba
520
Journal of International Oral Health 2016; 8(4):518-522Implant retained overdenture … Gupta H et al
decreased confidence (Figure 5a). On intra-oral examination, the maxillary and mandibular ridge are U-shaped and high well rounded. Patient asked for more definite treatment as compared to the conventional denture and was explained about different treatment options (Figure 5b).
The radiographic stent was made of self-cure acrylic resin over the primary cast with two orthodontic wires placed in relation to the site were implants will be placed in case of implant retained overdenture. Radiographic examination was carried out with the help of radiographic stent. Which revealed good bone quality, and it was decided to rehabilitate the patient with implant retained overdenture (Figure 6a).
Under antibiotic prophylaxis and standard aseptic protocol, nerve block and infiltration anesthesia was administered. In mandibular ridge Myraid Snap (3.3 mm × 11 mm) two implants were placed and suture was given. Suture was removed 1-week later. Patient was recalled after 3 months (Figure 6b).
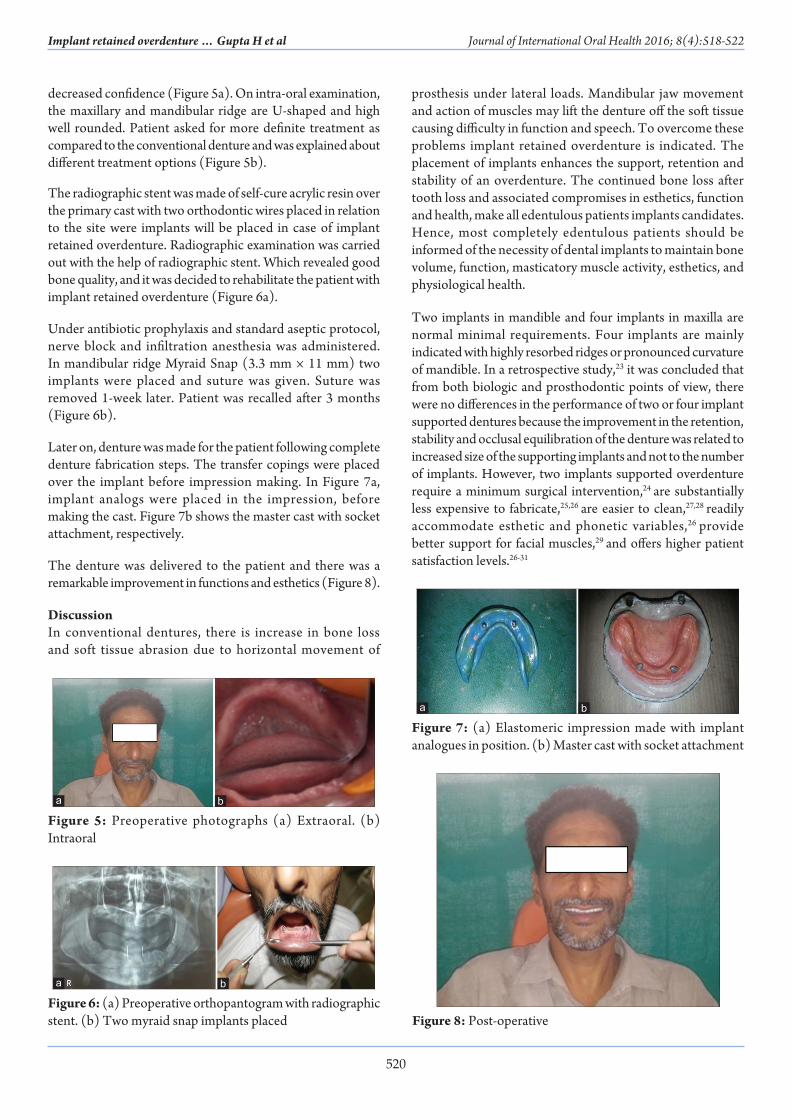
Later on, denture was made for the patient following complete denture fabrication steps. The transfer copings were placed over the implant before impression making. In Figure 7a, implant analogs were placed in the impression, before making the cast. Figure 7b shows the master cast with socket attachment, respectively.
The denture was delivered to the patient and there was a remarkable improvement in functions and esthetics (Figure 8).
DiscussionIn conventional dentures, there is increase in bone loss and soft tissue abrasion due to horizontal movement of
prosthesis under lateral loads. Mandibular jaw movement and action of muscles may lift the denture off the soft tissue causing difficulty in function and speech. To overcome these problems implant retained overdenture is indicated. The placement of implants enhances the support, retention and stability of an overdenture. The continued bone loss after tooth loss and associated compromises in esthetics, function and health, make all edentulous patients implants candidates. Hence, most completely edentulous patients should be informed of the necessity of dental implants to maintain bone volume, function, masticatory muscle activity, esthetics, and physiological health.
Two implants in mandible and four implants in maxilla are normal minimal requirements. Four implants are mainly indicated with highly resorbed ridges or pronounced curvature of mandible. In a retrospective study,23 it was concluded that from both biologic and prosthodontic points of view, there were no differences in the performance of two or four implant supported dentures because the improvement in the retention, stability and occlusal equilibration of the denture was related to increased size of the supporting implants and not to the number of implants. However, two implants supported overdenture require a minimum surgical intervention,24 are substantially less expensive to fabricate,25,26 are easier to clean,27,28 readily accommodate esthetic and phonetic variables,26 provide better support for facial muscles,29 and offers higher patient satisfaction levels.26-31
Figure 8: Post-operative
Figure 5: Preoperative photographs (a) Extraoral. (b) Intraoral
ba
Figure 6: (a) Preoperative orthopantogram with radiographic stent. (b) Two myraid snap implants placed
ba
Figure 7: (a) Elastomeric impression made with implant analogues in position. (b) Master cast with socket attachment
ba

521
Journal of International Oral Health 2016; 8(4):518-522Implant retained overdenture … Gupta H et al
A number of prospective studies have demonstrated that implant supported overdenture in mandible are a successful treatment. Recent studies have reported 5 years survival rates between 94% and 100%, marginal loss of <0.6 mm during a 5-year period and a higher degree of patient satisfaction.32,33
A number of patients, primarily older individuals would even prefer an implant supported overdenture to implant-supported fixed prosthesis if given the choice. Further in a comparative 5 year study, overdenture presented fewer complications and maintenance requirement than fixed prosthesis in the mandible. This indicates that implant supported overdenture treatment should not be considered a second class treatment, rather in patients with mandibular denture retention problems and the ability to tolerate a removable denture, it is often the therapy of choice.
Both the patients in the case report are satisfied with their dentures. However, the most common adjustment for all patients was denture contouring. The number of appointments for denture contouring was higher for patient in Case 1. This may be explained that, since gingival and bone healing after implant surgery may result in morphological changes of both soft and bone tissue, thus altering the support of the denture. The mean numbers of appointments and repairs needed for implant-supported mandibular overdentures in Case 1 was slightly higher than for Case 2.
The initial insertion of denture in Case 1 help the patient to get accustomed to the denture, make the difference in chewing efficiency, speech and retention of denture after the implants were placed. This treatment planning act as a phycological boon for the patient and patient could make the difference.
The denture of patient in Case 1 acts as a guide for placement of implant and there was no hinderance in the making of prosthesis. The implant placement in Case 2 was carried out with the expertise of the dentist and care was taken that there was least hinderance in making of prosthesis.
ConclusionOn comparing both the case reports, implants were Osseo integrated well in both the cases but it is advantageous to follow prosthetically driven approach since the patient’s acceptance improves as the clinician can access the exact angulation as to where the implants need to be placed without making a compromise in the patient’s appearance and function. Moreover the existing denture can be modified to act as radiographic stent, surgical guide as well as transitional prosthesis at the same time.
References1. Galind DF. The implant-supported milled-bar mandibular
overdenture. J Prosthodont 2001;10:46-51.
2. Zarb GA, Schmitt A. The edentulous predicament. II: The longitudinal effectiveness of implant-supported overdentures. J Am Dent Assoc 1996;127(1):66-72.
3. Worthington P, Bolender CL, Taylor TD. The Swedish system of osseointegrated implants: Problems and complications encountered during a 4-year trial period. Int J Oral Maxillofac Implants 1987;2(2):77-84.
4. Meng TR, Rugh TD. Biting force on overdenture and conventional denture patients. J Dent Res 1983;62:249.
5. Carr AB, Laney WR. Maximum occlusal force levels in patients with osseointegrated oral implant prostheses and patients with complete dentures. Int J Oral Maxillofac Implants 1987;2(2):101-8.
6. Jacobs R, van Steenberghe D. Masseter muscle fatigue during sustained clenching in subjects with complete dentures, implant-supported prostheses, and natural teeth. J Prosthet Dent 1993;69(3):305-13.
7. Boerrigter EM, Stegenga B, Raghoebar GM, Boering G. Patient satisfaction and chewing ability with implant-retained mandibular overdentures: A comparison with new complete dentures with or without preprosthetic surgery. J Oral Maxillofac Surg 1995;53(10):1167-73.
8. Geertman ME, Slagter AP, Van’t Hof MA, van Waas MA, Kalk W. Masticatory performance and chewing experience with implant-retained mandibular overdentures. J Oral Rehabil 1999;26(1):7-13.
9. Meijer HJ, Raghoebar GM, Van’t Hof MA, Geertman ME, Van Oort RP. Implant-retained mandibular overdentures compared with complete dentures; a 5-years’ follow-up study of clinical aspects and patient satisfaction. Clin Oral Implants Res 1999;10(3):238-44.
10. Awad MA, Locker D, Korner-Bitensky N, Feine JS. Measuring the effect of intra-oral implant rehabilitation on health-related quality of life in a randomized controlled clinical trial. J Dent Res 2000;79(9):1659-63.
11. Allen PF, McMillan AS, Walshaw D. A patient-based assessment of implant-stabilized and conventional complete dentures. J Prosthet Dent 2001;85(2):141-7.
12. von Wowern N, Gotfredsen K. Implant-supported overdentures, a prevention of bone loss in edentulous mandibles? A 5-year follow-up study. Clin Oral Implants Res 2001;12(1):19-25.
13. Bakke M, Holm B, Gotfredsen K. Masticatory function and patient satisfaction with implant-supported mandibular overdentures: A prospective 5-year study. Int J Prosthodont 2002;15(6):575-81.
14. Visse A, Raghoebar GM, Meijer HJ, Batenburg RH, Vissink A. Mandibular overdentures supported by two or four endosseous implants A 5-year prospective study. Clin Oral Impl Res 2005;16:19-25.
15. Haraldson T, Jemt T, Stålblad PA, Lekholm U. Oral function in subjects with overdentures supported by osseointegrated implants. Scand J Dent Res 1988;96(3):235-42.
16. Naert I, Quirynen M, Hooghe M, van Steenberghe D. A comparative prospective study of splinted and unsplinted Brånemark implants in mandibular overdenture therapy:

522
Journal of International Oral Health 2016; 8(4):518-522Implant retained overdenture … Gupta H et al
A preliminary report. J Prosthet Dent 1994;71(5):486-92.17. ten Bruggenkate CM, Muller K, Oosterbeek HS. Clinical
evaluation of the ITI (F-type) hollow cylinder implant. Oral Surg Oral Med Oral Pathol 1990;70(6):693-7.
18. Engquist B. Six years’ experience of splinted and non-splinted implants supporting overdentures in upper and lower jaws. In: Schepers E, Naert I, Theuniers G, (Editors). Overdentures on Oral Implants, Leuven: Leuven University Press; 1991. p. 27-41.
19. Versteegh PA, van Beek GJ, Slagter AP, Ottervanger JP. Clinical evaluation of mandibular overdentures supported by multiple-bar fabrication: A follow-up study of two implant systems. Int J Oral Maxillofac Implants 1995;10(5):595-603.
20. Boerrigter EM, Geertman ME, Van Oort RP, Bouma J, Raghoebar GM, van Waas MA, et al. Patient satisfaction with implant-retained mandibular overdentures. A comparison with new complete dentures not retained by implants – A multicentre randomized clinical trial. Br J Oral Maxillofac Surg 1995;33(5):282-8.
21. MacEntee MI, Walton JN, Glick N. A clinical trial of patient satisfaction and prosthodontic needs with ball and bar attachments for implant-retained complete overdentures: Three-year results. J Prosthet Dent 2005;93(1):28-37.
22. Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ, Gizani S, et al. The McGill Consensus Statement on Overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Montreal, Quebec, May 24-25, 2002. Int J Oral Maxillofac Implants 2002;17:601-2.
23. Sadig W. A comparative in vitro study on the retention and stability of implant-supported overdentures. Quintessence Int 2009;40(4):313-9.
24. Wismeijer D, Van Waas MA, Vermeeren JI, Mulder J, Kalk W. Patient satisfaction with implant supported mandibular overdentures. A comparison of three treatment
strategies witrh ITI dental implants. Int J Oral Maxillofac Surg 1997;26:263-7.
25. Mericske Stern R. Clinical evaluation of overdenture restorations supported by osseointegrated titanium implant: A retrospective study. Int J Oral Maxillofac Implants 1990;5(4):375-83.
26. Hobo S, Ishida E, Garcia L, (Editors). Osseointegration and Occlusal Rehabiitation, Tokyo: Quintessence; 1989.
27. Attard NJ, Zarb GA. Long-term treatment outcomes in edentulous patients with implant overdentures: The Toronto study. Int J Prosthodont 2004;17(4):425-33.
28. Heydecke G, Klemetti E, Awad MA, Lund JP, Feine JS. Relationship between prosthodontic evaluation and patient ratings of mandibular conventional and implant prostheses. Int J Prosthodont 2003;16(3):307-12.
29. Moberg LE, Köndell PA, Sagulin GB, Bolin A, Heimdahl A, Gynther GW. Brånemark System and ITI Dental Implant System for treatment of mandibular edentulism. A comparative randomized study: 3-year follow-up. Clin Oral Implants Res 2001;12(5):450-61.
30. den Dunnen AC, Slagter AP, de Baat C, Kalk W. Professional hygiene care, adjustments and complications of mandibular implant-retained overdentures: A three-year retrospective study. J Prosthet Dent 1997;78(4):387-90.
31. Parel SM. Implants and overdentures: The osseointegrated approach with conventional and compromised applications. Int J Oral Maxillofac Implants 1986;1(2):93-9.
32. Gotfredsen K, Holm B. Implant-supported mandibular overdentures retained with ball or bar attachments: A randomized prospective 5-year study. Int J Prosthodont 2000;13(2):125-30.
33. Al-Fahd AA, Alsourori A, Al-Qutabi A, Farouk M, Abbas N. Impact of screw retained versus cement retained implant-supported prosthesis on peri-implantitis: A systematic review and meta-analysis. Int Dent Med J Adv Res 2015;1:1-6.