Implant Impression Techniques in Dentistry - jdsor.comjdsor.com/2016VOL7-3/A9.pdf · Implant...
5
Journal of Dental Sciences and Oral Rehabilitation, July-September 2016;7(3):137-141 137 JDSOR Implant Impression Techniques in Dentistry 1 Shweta Singh, 2 Alok Kumar ABSTRACT An important factor for the success with implant-supported restoration is the passive fit between the superstructure and the abutments. Impression procedure proves to be a vital initial step in achieving an accurate, passively fitting prosthesis. Before the fabrication of prosthesis, the transfer (closed tray) and pick-up (open tray) techniques have been advised to reproduce accu- rate intraoral relationship of implants. This article deals with the procedure of different implant impression techniques and its clinical factors affecting implant impression. Keywords: Closed tray, Open tray, Splinted impression technique. How to cite this article: Singh S, Kumar A. Implant Impression Techniques in Dentistry. J Dent Sci Oral Rehab 2016;7(3):137-141. Source of support: Nil Conflict of interest: None INTRODUCTION Dental implants have become a quite successful method for restoration of fully and partially edentulous patients. Impression procedure becomes exacting in implantology as compared to fixed partial denture because of lack of periodontal ligament fibers in implants. The criti- cal aspect is to record the spatial intraoral orientation of the implant, rather than replicating minute surface detail. Passive fit between the connector of the prosthesis and the implant body is the key to success. Therefore, impression making and reciprocating three-dimensional (3D) position of implant to the working model should be precise. Several impression techniques have been advocated to achieve a definitive cast that will ensure the passive fit of prosthesis on osseointegrated implants. There are two primary techniques: The indirect (closed tray) technique and the direct (open tray) technique. 1 The indirect tech- nique may be less difficult clinically; however, it has been shown to have greater instability in transferring the implant position. In the direct technique, the impression coping lies CASE REPORT 1 Senior Lecturer, 2 Reader 1,2 Departmemt of Prosthodontics, Institute of Dental Sciences Bareilly, Uttar Pradesh, India Corresponding Author: Alok Kumar, Reader, Department of Prosthodontics, Institute of Dental Sciences, Bareilly, Uttar Pradesh, India, e-mail: [email protected] 10.5005/jp-journals-10039-1127 within the impression. This reduces the effect of implant angulation, the deformation of the impression material upon recovery from mouth, and removes the concern for replacing the coping back into its respective space in the impression. 2 The direct technique may be carried out by using splinted or nonsplinted implant impression copings. Acrylic resin, pattern resin, plaster, composite can be chosen for splinting of impression copings. CLOSED TRAY IMPRESSION PROCEDURE Healing abutment was removed with manual screwdriver (Fig. 1). Impression coping was placed manually rotat- ing to assure that the lobes are aligned into the internal connection of the implant (Fig. 2). Once it was seated the manual screwdriver was used to fasten. A radiograph Fig. 1: Removal of Healing Abutment Fig. 2: Square impression coping secured to implant
-
Upload
truongdiep -
Category
Documents
-
view
257 -
download
3
Transcript of Implant Impression Techniques in Dentistry - jdsor.comjdsor.com/2016VOL7-3/A9.pdf · Implant...
Implant Impression Techniques in Dentistry
Journal of Dental Sciences and Oral Rehabilitation, July-September 2016;7(3):137-141 137
JDSORJDSOR
Implant Impression Techniques in Dentistry1Shweta Singh, 2Alok Kumar
ABSTRACT
An important factor for the success with implant-supported restoration is the passive fit between the superstructure and the abutments. Impression procedure proves to be a vital initial step in achieving an accurate, passively fitting prosthesis. Before the fabrication of prosthesis, the transfer (closed tray) and pick-up (open tray) techniques have been advised to reproduce accu-rate intraoral relationship of implants. This article deals with the procedure of different implant impression techniques and its clinical factors affecting implant impression.
Keywords: Closed tray, Open tray, Splinted impression technique.
How to cite this article: Singh S, Kumar A. Implant Impression Techniques in Dentistry. J Dent Sci Oral Rehab 2016;7(3):137-141.
Source of support: Nil
Conflict of interest: None
INTRODUCTION
Dental implants have become a quite successful method for restoration of fully and partially edentulous patients. Impression procedure becomes exacting in implantology as compared to fixed partial denture because of lack of periodontal ligament fibers in implants. The criti-cal aspect is to record the spatial intraoral orientation of the implant, rather than replicating minute surface detail. Passive fit between the connector of the prosthesis and the implant body is the key to success. Therefore, impression making and reciprocating three-dimensional (3D) position of implant to the working model should be precise.
Several impression techniques have been advocated to achieve a definitive cast that will ensure the passive fit of prosthesis on osseointegrated implants. There are two primary techniques: The indirect (closed tray) technique and the direct (open tray) technique.1 The indirect tech-nique may be less difficult clinically; however, it has been shown to have greater instability in transferring the implant position. In the direct technique, the impression coping lies
CaSe RepORt
1Senior Lecturer, 2Reader1,2Departmemt of Prosthodontics, Institute of Dental Sciences Bareilly, Uttar Pradesh, India
Corresponding Author: Alok Kumar, Reader, Department of Prosthodontics, Institute of Dental Sciences, Bareilly, Uttar Pradesh, India, e-mail: [email protected]
10.5005/jp-journals-10039-1127
within the impression. This reduces the effect of implant angulation, the deformation of the impression material upon recovery from mouth, and removes the concern for replacing the coping back into its respective space in the impression.2 The direct technique may be carried out by using splinted or nonsplinted implant impression copings. Acrylic resin, pattern resin, plaster, composite can be chosen for splinting of impression copings.
CLOSED TRAY IMPRESSION PROCEDURE
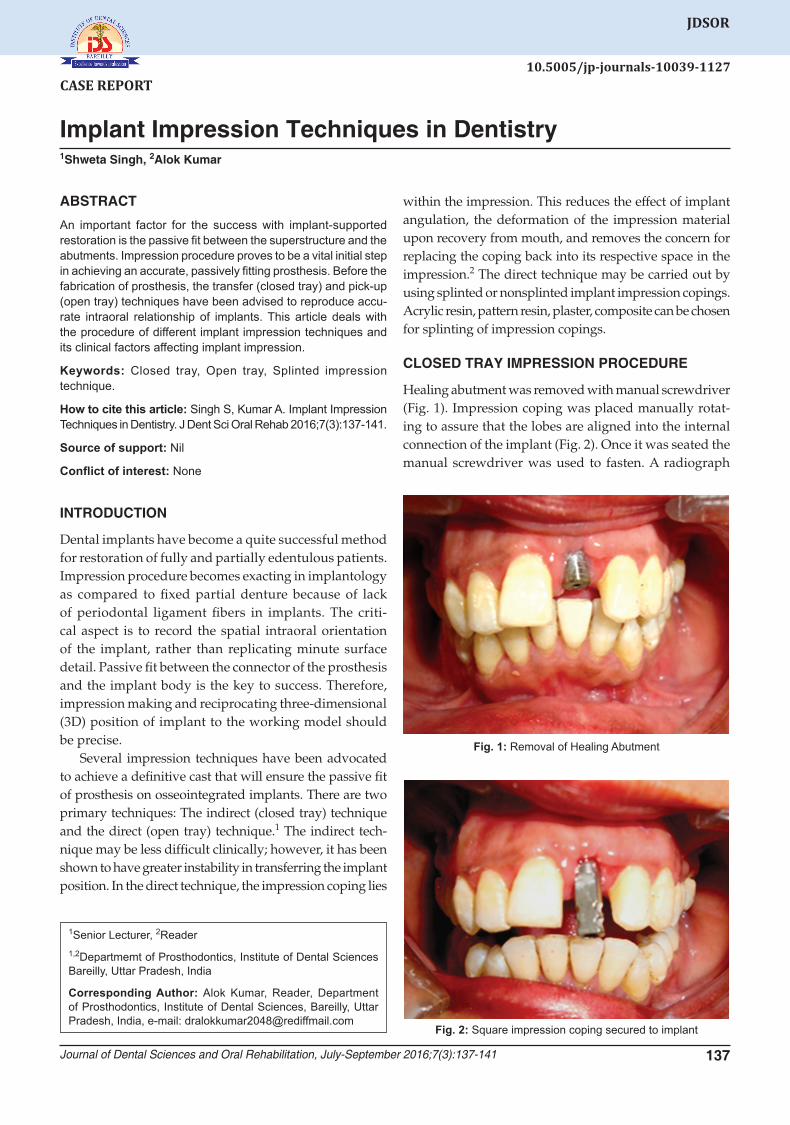
Healing abutment was removed with manual screwdriver (Fig. 1). Impression coping was placed manually rotat-ing to assure that the lobes are aligned into the internal connection of the implant (Fig. 2). Once it was seated the manual screwdriver was used to fasten. A radiograph
Fig. 1: Removal of Healing Abutment
Fig. 2: Square impression coping secured to implant
Shweta Singh, Alok Kumar
138
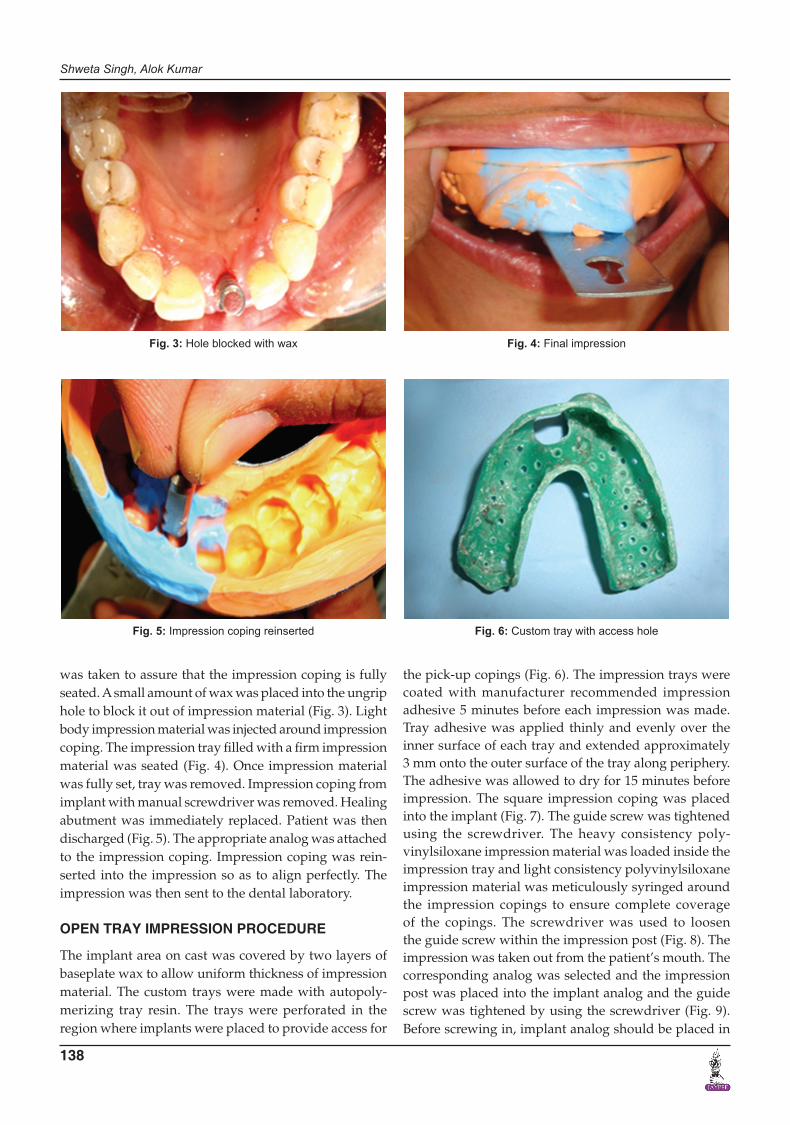
was taken to assure that the impression coping is fully seated. A small amount of wax was placed into the ungrip hole to block it out of impression material (Fig. 3). Light body impression material was injected around impression coping. The impression tray filled with a firm impression material was seated (Fig. 4). Once impression material was fully set, tray was removed. Impression coping from implant with manual screwdriver was removed. Healing abutment was immediately replaced. Patient was then discharged (Fig. 5). The appropriate analog was attached to the impression coping. Impression coping was rein-serted into the impression so as to align perfectly. The impression was then sent to the dental laboratory.
OPEN TRAY IMPRESSION PROCEDURE
The implant area on cast was covered by two layers of baseplate wax to allow uniform thickness of impression material. The custom trays were made with autopoly-merizing tray resin. The trays were perforated in the region where implants were placed to provide access for
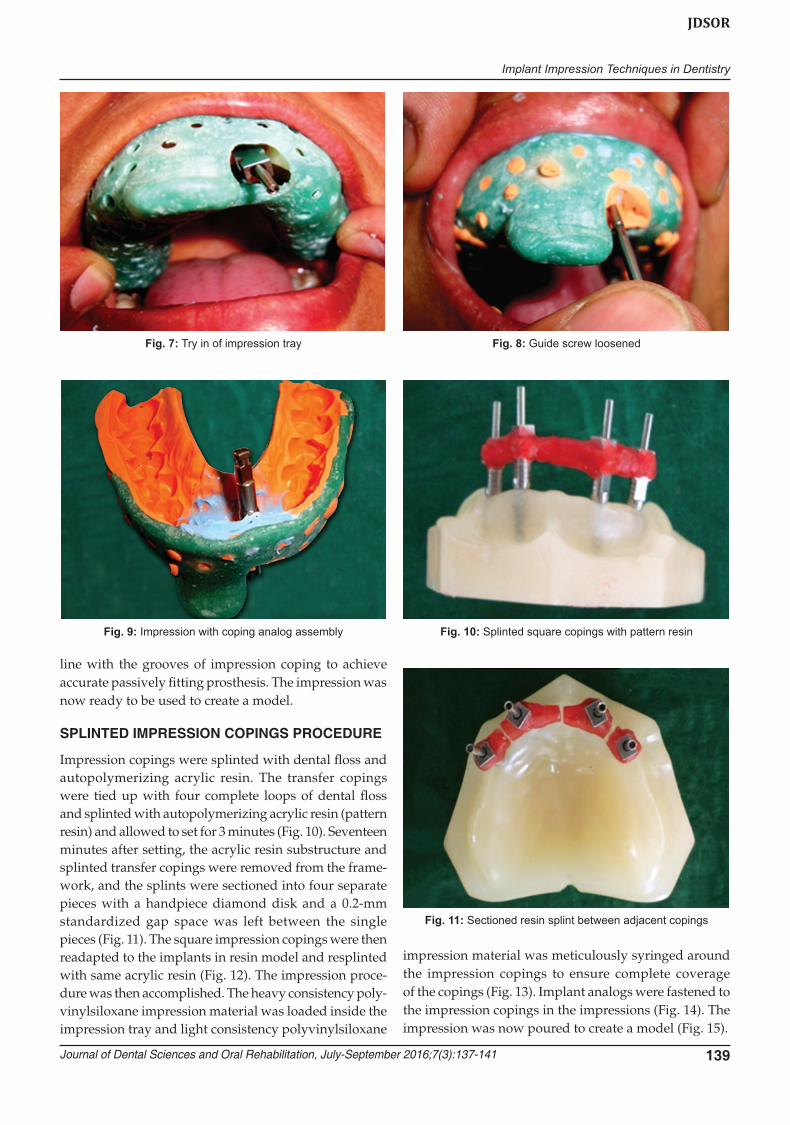
the pick-up copings (Fig. 6). The impression trays were coated with manufacturer recommended impression adhesive 5 minutes before each impression was made. Tray adhesive was applied thinly and evenly over the inner surface of each tray and extended approximately 3 mm onto the outer surface of the tray along periphery. The adhesive was allowed to dry for 15 minutes before impression. The square impression coping was placed into the implant (Fig. 7). The guide screw was tightened using the screwdriver. The heavy consistency poly-vinylsiloxane impression material was loaded inside the impression tray and light consistency polyvinylsiloxane impression material was meticulously syringed around the impression copings to ensure complete coverage of the copings. The screwdriver was used to loosen the guide screw within the impression post (Fig. 8). The impression was taken out from the patient’s mouth. The corresponding analog was selected and the impression post was placed into the implant analog and the guide screw was tightened by using the screwdriver (Fig. 9). Before screwing in, implant analog should be placed in
Fig. 3: Hole blocked with wax Fig. 4: Final impression
Fig. 5: Impression coping reinserted Fig. 6: Custom tray with access hole
Implant Impression Techniques in Dentistry
Journal of Dental Sciences and Oral Rehabilitation, July-September 2016;7(3):137-141 139
JDSOR
line with the grooves of impression coping to achieve accurate passively fitting prosthesis. The impression was now ready to be used to create a model.
SPLINTED IMPRESSION COPINGS PROCEDURE
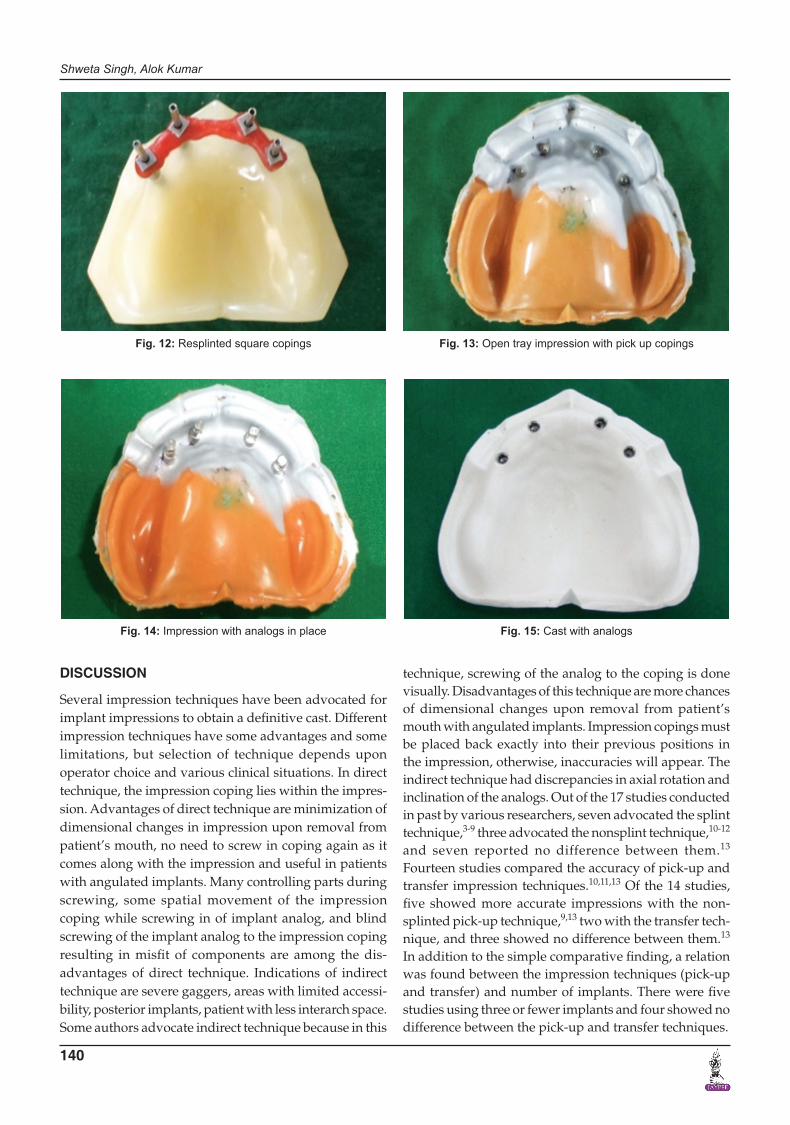
Impression copings were splinted with dental floss and autopolymerizing acrylic resin. The transfer copings were tied up with four complete loops of dental floss and splinted with autopolymerizing acrylic resin (pattern resin) and allowed to set for 3 minutes (Fig. 10). Seventeen minutes after setting, the acrylic resin substructure and splinted transfer copings were removed from the frame-work, and the splints were sectioned into four separate pieces with a handpiece diamond disk and a 0.2-mm standardized gap space was left between the single pieces (Fig. 11). The square impression copings were then readapted to the implants in resin model and resplinted with same acrylic resin (Fig. 12). The impression proce-dure was then accomplished. The heavy consistency poly-vinylsiloxane impression material was loaded inside the impression tray and light consistency polyvinylsiloxane
impression material was meticulously syringed around the impression copings to ensure complete coverage of the copings (Fig. 13). Implant analogs were fastened to the impression copings in the impressions (Fig. 14). The impression was now poured to create a model (Fig. 15).
Fig. 7: Try in of impression tray Fig. 8: Guide screw loosened
Fig. 9: Impression with coping analog assembly Fig. 10: Splinted square copings with pattern resin
Fig. 11: Sectioned resin splint between adjacent copings
Shweta Singh, Alok Kumar
140
DISCUSSION
Several impression techniques have been advocated for implant impressions to obtain a definitive cast. Different impression techniques have some advantages and some limitations, but selection of technique depends upon operator choice and various clinical situations. In direct technique, the impression coping lies within the impres-sion. Advantages of direct technique are minimization of dimensional changes in impression upon removal from patient’s mouth, no need to screw in coping again as it comes along with the impression and useful in patients with angulated implants. Many controlling parts during screwing, some spatial movement of the impression coping while screwing in of implant analog, and blind screwing of the implant analog to the impression coping resulting in misfit of components are among the dis-advantages of direct technique. Indications of indirect technique are severe gaggers, areas with limited accessi-bility, posterior implants, patient with less interarch space. Some authors advocate indirect technique because in this
technique, screwing of the analog to the coping is done visually. Disadvantages of this technique are more chances of dimensional changes upon removal from patient’s mouth with angulated implants. Impression copings must be placed back exactly into their previous positions in the impression, otherwise, inaccuracies will appear. The indirect technique had discrepancies in axial rotation and inclination of the analogs. Out of the 17 studies conducted in past by various researchers, seven advocated the splint technique,3-9 three advocated the nonsplint technique,10-12 and seven reported no difference between them.13 Fourteen studies compared the accuracy of pick-up and transfer impression techniques.10,11,13 Of the 14 studies, five showed more accurate impressions with the non-splinted pick-up technique,9,13 two with the transfer tech-nique, and three showed no difference between them.13 In addition to the simple comparative finding, a relation was found between the impression techniques (pick-up and transfer) and number of implants. There were five studies using three or fewer implants and four showed no difference between the pick-up and transfer techniques.
Fig. 12: Resplinted square copings Fig. 13: Open tray impression with pick up copings
Fig. 14: Impression with analogs in place Fig. 15: Cast with analogs

Implant Impression Techniques in Dentistry
Journal of Dental Sciences and Oral Rehabilitation, July-September 2016;7(3):137-141 141
JDSOR
CONCLUSION
Selection of appropriate impression technique to obtain accurate definitive cast depends upon implant angulation, depth, number, position in arch, interarch space, impres-sion material, operator’s choice. Closed tray (transfer, indirect) technique using tapered impression copings is an easy and simple technique ideal for single implant impres-sions and multiple parallel implants in patients with limited mouth opening. Open tray (pick-up, direct) tech-nique using square impression copings is more accurate method usually preferred in multiple implants with differ-ent angulations. The removal of rigidly splinted internal configuration impression copings may be impossible in highly angulated multiple implants, thereby necessitat-ing use of sandblasted nonsplinted impression copings.
REFERENCES
1. Del Acqua MM, Chavez AM, Amarat AL, Compagnoni MM, Mollo FA. Comparison of impression techniques and materi-als for an implant-supported prosthesis. Int J Oral Maxillofac Implants 2010 Jul-Aug;25(4):771-776.
2. Liou AD, Nicholls JI, Yuodelis RA, Brudvik JS. Accuracy of replacing three tapered transfer impression copings in two elastomeric impression materials. Int J Prosthodont 1993 Jul-Aug;6(4):377-383.
3. Assif D, Fenton A, Zarb G, Schmitt A. Comparative accuracy of implant impression procedures. Int J Periodontics Restora-tive Dent 1992;12(2):112-121.
4. Assif D, Marshak B, Schmidt A. Accuracy of implant impres-sion techniques. Int J Oral Maxillofac Implants 1996 Mar-Apr;11(2):216-222.
5. Vigolo P, Majzoub Z, Cordioli G. Evaluation of the accuracy of three techniques used for multiple implant abutment impres-sions. J Prosthet Dent 2003 Feb;89(2):186-192.
6. Naconecy MM, Teixeira ER, Shinkai RS, Frasca LC, Cervieri A. Evaluation of the accuracy of 3 transfer techniques for implant-supported prostheses with multiple abutments. Int J Oral Maxillofac Implants 2004 Mar-Apr;19(2):192-198.
7. Vigolo P, Fonzi F, Majzoub Z, Cordioli G. An evaluation of impression techniques for multiple internal connection implant prostheses. J Prosthet Dent 2004 Nov;92(5):470-476.
8. Assuncao WG, Filho HG, Zaniquelli O. Evaluation of transfer impressions for osseointegrated implants at various angula-tions. Implant Dent 2004 Dec;13(4):358-366.
9. Cabral LM, Guedes CG. Comparative analysis of 4 impres-sion techniques for implants. Implant Dent 2007 Jun;16(2): 187-194.
10. Inturregui JA, Aquilino SA, Ryther JS, Lund PS. Evaluation of three impression techniques for osseointegrated oral implants. J Prosthet Dent 1993 May;69(5):503-509.
11. Phillips KM, Nicholls JI, Ma T, Rubenstein J. The accuracy of three implant impression techniques: a three-dimensional analysis. Int J Oral Maxillofac Implants 1994;9:533-540.
12. Burawi G, Houston F, Byrne D, Claffey N. A comparison of the dimensional accuracy of the splinted and unsplinted impression techniques for the Bone-Lock implant system. J Prosthet Dent 1997 Jan;77(1):68-75.
13. Lee H, Hochstedler JL, Ercoli C. The accuracy of implant impressions: a systematic review. J Prosthet Dent 2008 Oct;100(4):285-291.