Impact of state nurse practitioner scope-of-practice regulation on … · 2016-08-18 · Impact of...
15
Impact of state nurse practitioner scope-of-practice regulation on health care delivery: Systematic review Ying Xue, DNSc, RN a, *, Zhiqiu Ye, BS b , Carol Brewer, PhD, RN, FAAN c , Joanne Spetz, PhD d,e a University of Rochester, School of Nursing, Rochester, NY b Department of Public Health Sciences, University of Rochester Medical Center, Rochester, NY c University at Buffalo, School of Nursing, Buffalo, NY d Philip R. Lee Institute for Health Policy Studies, Department of Family and Community Medicine, School of Medicine, University of California, San Francisco, San Francisco, CA e Department of Social and Behavioral Sciences, School of Nursing, University of California, San Francisco, San Francisco, CA article info Article history: Received 19 May 2015 Revised 10 August 2015 Accepted 30 August 2015 Available online 9 September 2015 Keywords: Nurse practitioner Scope-of-practice regulation Primary care abstract Background: One proposed strategy to expand primary care capacity is to use nurse practitioners (NPs) more effectively in health care delivery. However, the ability of NPs to provide care to the fullest extent of their education is moderated by state scope-of-practice (SOP) regulations. Purpose: The purpose of this study was to examine the impact of state SOP reg- ulations on the following three key issues: (a) NP workforce, (b) access to care and health care utilization, and (c) health care costs. Methods: Systematic review. Results/Discussion: States granting NPs greater SOP authority tend to exhibit an increase in the number and growth of NPs, greater care provision by NPs, and expanded health care utilization, especially among rural and vulnerable pop- ulations. Our review indicates that expanded NP practice regulation can impact health care delivery by increasing the number of NPs in combination with easing restrictions on their SOP. Conclusions: Findings show promise that removing restrictions on NP SOP regu- lations could be a viable and effective strategy to increase primary care capacity. Cite this article: Xue, Y., Ye, Z., Brewer, C., & Spetz, J. (2016, FEBRUARY). Impact of state nurse practitioner scope-of-practice regulation on health care delivery: Systematic review. Nursing Outlook, 64(1), 71-85. http://dx.doi.org/10.1016/j.outlook.2015.08.005. Introduction Provisions of the Patient Protection and Affordable Care Act (ACA), particularly those dealing with Medicaid expansion and payment reform, are expected to increase the demand for primary care within a health care system already facing severe physician workforce shortages. These shortages impede the ca- pacity to deliver sufficient care to an aging and more diverse population, with growing chronic disease burden, particularly among poor and minority pop- ulations (Bodenheimer, Chen, & Bennett, 2009). Although one recent state-level analysis suggested that the current physician workforce supply in both pri- mary care and most specialties is sufficient to meet * Corresponding author: Ying Xue, University of Rochester, School of Nursing, 601 Elmwood Ave., Box SON, Rochester, NY 14642. E-mail address: [email protected] (Y. Xue). 0029-6554/$ - see front matter Ó 2016 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.outlook.2015.08.005 Available online at www.sciencedirect.com Nurs Outlook 64 (2016) 71 e 85 www.nursingoutlook.org
Transcript of Impact of state nurse practitioner scope-of-practice regulation on … · 2016-08-18 · Impact of...

Available online at www.sciencedirect.com
Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 5www.nursingoutlook.org
Impact of state nurse practitioner scope-of-practiceregulation on health care delivery: Systematic review
Ying Xue, DNSc, RNa,*, Zhiqiu Ye, BSb, Carol Brewer, PhD, RN, FAANc,Joanne Spetz, PhDd,e
aUniversity of Rochester, School of Nursing, Rochester, NYbDepartment of Public Health Sciences, University of Rochester Medical Center, Rochester, NY
cUniversity at Buffalo, School of Nursing, Buffalo, NYdPhilip R. Lee Institute for Health Policy Studies, Department of Family and Community Medicine, School of Medicine, University of California,
San Francisco, San Francisco, CAeDepartment of Social and Behavioral Sciences, School of Nursing, University of California, San Francisco, San Francisco, CA
a r t i c l e i n f o
Article history:Received 19 May 2015Revised 10 August 2015Accepted 30 August 2015Available online 9 September2015
Keywords:Nurse practitionerScope-of-practice regulationPrimary care
* Corresponding author: Ying Xue, UniversityE-mail address: [email protected]
0029-6554/$ - see front matter � 2016 Elsevihttp://dx.doi.org/10.1016/j.outlook.2015.08.005
a b s t r a c t
Background:One proposed strategy to expand primary care capacity is to use nursepractitioners (NPs) more effectively in health care delivery. However, the abilityof NPs to provide care to the fullest extent of their education is moderated bystate scope-of-practice (SOP) regulations.Purpose: The purpose of this study was to examine the impact of state SOP reg-ulations on the following three key issues: (a) NP workforce, (b) access to careand health care utilization, and (c) health care costs.Methods: Systematic review.Results/Discussion: States granting NPs greater SOP authority tend to exhibit anincrease in the number and growth of NPs, greater care provision by NPs, andexpanded health care utilization, especially among rural and vulnerable pop-ulations. Our review indicates that expanded NP practice regulation can impacthealth care delivery by increasing the number of NPs in combination with easingrestrictions on their SOP.Conclusions: Findings show promise that removing restrictions on NP SOP regu-lations could be a viable and effective strategy to increase primary care capacity.
Cite this article: Xue, Y., Ye, Z., Brewer, C., & Spetz, J. (2016, FEBRUARY). Impact of state nurse practitioner
scope-of-practice regulation on health care delivery: Systematic review. Nursing Outlook, 64(1), 71-85.
http://dx.doi.org/10.1016/j.outlook.2015.08.005.
Introduction
Provisions of the Patient Protection and AffordableCare Act (ACA), particularly those dealing withMedicaid expansion and payment reform, are expectedto increase the demand for primary care within ahealth care system already facing severe physician
of Rochester, School ofr.edu (Y. Xue).
er Inc. All rights reserved
workforce shortages. These shortages impede the ca-pacity to deliver sufficient care to an aging and morediverse population, with growing chronic diseaseburden, particularly among poor and minority pop-ulations (Bodenheimer, Chen, & Bennett, 2009).Although one recent state-level analysis suggested thatthe current physician workforce supply in both pri-mary care and most specialties is sufficient to meet
Nursing, 601 Elmwood Ave., Box SON, Rochester, NY 14642.
.

Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 572
future demand (Glied & Ma, 2015), the analysisassumed an increase in physician workload and didnot examine potential variation in supply and demandacross local areas within states. Indeed, a within-statesmall area analysis examining the impact of ACA re-forms using the same source of data suggested thatabout 44 million Americans live in areas where theexpected increase in demand for primary care willexceed 5% and almost seven million reside in areaswhere the expected demand will increase by morethan 10% (Huang & Finegold, 2013). The Health Re-sources and Services Administration (HRSA) estimatesthat the supply of primary care physicians (PCPs) willnot meet future demand, with a projected shortage ofapproximately 20,400 full-time equivalent physiciansby 2020 (HRSA, 2013). Within this backdrop of healthcare reform and physician workforce shortages,transforming the delivery of primary care, particularlyfor newly eligible Medicaid enrollees, has become a toppriority for many state policy makers (AcademyHealth,2015), with most state governors addressing this issuein their State of the State speeches in 2014 (NationalAcademy for State Health Policy, 2015).
One policy recommendation aimed at expandingprimary care capacity is to use nurse practitioners(NPs) more effectively (Dower, Moore, & Langelier,2013; Naylor & Kurtzman, 2010; Pohl, Hanson,Newland, & Cronenwett, 2010). A projected increasein the NP workforce (HRSA, 2013), along with theessential and steadily growing contributions of NPs toprimary care (Druss, Marcus, Olfson, Tanielian, &Pincus, 2003; Kuo, Loresto, Rounds, & Goodwin, 2013),especially their historic and evolving role in improvingaccess to primary care for vulnerable populations(Morgan, Everett, & Hing, 2015), offers compelling evi-dence for this policy recommendation.
HRSA has projected a 30% increase in primary careNPs from 55,400 in 2010 to 72,100 NPs by 2020, whichcombined with an increase in physician assistants(PAs) could substantially reduce the projected shortageof full-time equivalent physicians from 20,400 to 6,400if NPs and PAs are effectively integrated into the pri-mary care system (HRSA, 2013). Perhapsmost critical tohealth care reform, NPs have historically played a vitalrole in improving access to primary care for vulnerablepopulations (Morgan et al., 2015). NPs are key providersin 1,202 federally funded community health centersand 250 nurse-managed health clinics that embraceteam-based care to serve >22 million minority andlow-income patients (Hansen-Turton, Bailey, Torres, &Ritter, 2010; National Association of CommunityHealth Centers, 2014). A recent analysis suggestedthat increasing nurse-managed health centers andexpanding patient panel size in patient-centeredmedical homes could substantially mitigate primarycare provider shortages (Auerbach et al., 2013).
In addition, expanding the role and scope of practice(SOP) of NPs in the delivery of primary care (e.g., in-dependent practice and prescription authority) has hada significant impact on access to primary care and
improved management of chronic diseases amongvulnerable populations, including Medicaid enrollees(Adashi, Geiger, & Fine, 2010; Landon et al., 2007).Supporting an expanded SOP for NPs is an extensivebody of evidence that has consistently demonstratedcomparable performance between NPs and PCPs onclinical outcomes, including reduction of symptoms,improvement in health and functional status, andmortality (Naylor & Kurtzman, 2010; Paradise, Dark, &Bitler, 2011). In addition, patients seen by NPs gener-ally report higher satisfaction (Jennings, Clifford, Fox,Oconnell, & Gardner, 2015).
However, the ability of NPs to provide essentialprimary care to the fullest extent of their education ismoderated by state SOP regulation, which is governedby state law under the state’s Nurse Practice Act and isadministered and regulated by each state’s Board ofNursing. The National Council of State Boards ofNursing has developed a national standard (theConsensus Model) to provide guidance for states toadopt uniform APRN (advanced practice registerednurse) regulation on licensure, accreditation, certifi-cation, and education (National Council of State Boardsof Nursing, 2014), and the National Governors Associ-ation recommended that states consider expandingSOP regulations to grant NPs authority in full practice(National Governors Association, 2012).
Yet, among the 24 states predicted to have an in-crease in demand for primary care providers above thenational average due to the implementation of theACA, 17 have restrictive NP SOP regulations (Huang &Finegold, 2013). To assist state policy makers in mak-ing evidence-based decisions on legislative reformsconcerning the expansion of the NP role in health caredelivery, we conducted a systematic review on theimpact of state NP SOP regulations on health care de-livery, specifically focusing on the following three keyissues: (a) NP workforce, (b) access to care and healthcare utilization, and (c) health care costs.
Methods
Search Strategy
We searched the electronic databases PubMed,CINAHL, PsycINFO, and Cochrane library for the periodup to January 31, 2015. In addition, we manuallysearched Google Scholar and the references of pub-lished studies. The search in title or abstract comprisedthe terms SOP, legislation, regulation, NP(s), advancedpractice nurse(s), or APRN(s). As health care systemand regulatory issues are different across countries, werestricted the publications to those that addressedthese issues in the United States. Additional inclusioncriteria were (a) published in English, (b) empiricalquantitative study, (c) directly examined the effect ofstate SOP regulations on health care delivery, and (d)acceptable risk of bias inmethodological approach. We

Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 5 73
included studies with both time-series and cross-sectional research designs. Although studies withcross-sectional designs may be less desirable forassessing regulatory effects, they can nonethelessprovide valuable insights if confounding factors wereconceptually sound and controlled for in the analysis.Studies with bivariate analysis were thereforeexcluded, as results are inconclusive without adjustingfor potential confounding factors.
Study Screening and Data Extraction
Two authors independently screened the retrievedstudies for eligibility by title and abstract. Screeningwas not blinded to authors, institutions, or manuscriptjournals. If an abstract did not provide sufficient in-formation, evaluation of the full text was performedand study eligibility was determined. Data on studycharacteristics and key findings of individual studieswere also independently extracted by two authors.Disagreements in study screening and data extractionwere resolved by consensus.
Assessment of Risk of Bias
Two authors independently assessed risk of bias instudy methods that might threaten internal validity,including study design, data sources, measurement,and statistical analysis. Disagreements between thetwo reviewers were resolved through discussion.
Data Synthesis
Meta-analysis was not performed because the studiesincluded in the review are heterogeneous in topic andmethodology. Thematic summaries were conductedindependently by two authors to extract the commonthemes across studies with disagreements resolved byconsensus.
Results
Characteristics of Studies
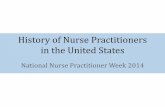
Our search identified 529 published articles, whichwere screened initially for eligibility by title and ab-stract. Of these, 22 were selected for further assess-ment for eligibility by examining the full articles. Sevenof the 22 articles were excluded because of potentialhigh risk of bias in the methodological approach,leaving 15 articles in the present review and synthesis.A flow diagram of search and study selection is shownin Figure 1. Characteristics of the selected studies aresummarized in Table 1. These studies were publishedfrom 1997 to 2015. Findings were generally consistentacross study periods. Nine studies used a time-seriesdesign, and six employed a cross-sectional design.Most studies used national data sets and employed
multiple regression analysis; a few studies adjusted forclustering effects, and one study used multilevelmodeling to examine factors on state and individuallevels simultaneously.
SOP regulation was measured in two ways in thereviewed studies. Some studies employed an indexmeasure based on a scoring system for various SOPregulation components, such as practice status, pre-scription authority, and independent reimbursement.However, most studies used categorical coding forpresence or absence of the same or similar compo-nents. To compare and synthesize results acrossreviewed studies more effectively, we used a three-level classification for NP SOP regulation defined bythe American Association of Nurse Practitioners: (a)full SOP regulation (independent practice and pre-scriptive authority), (b) reduced SOP regulation (re-quires a collaborative agreement with physicians for atleast one practice component such as prescription),and (c) restrictive SOP regulation (requires supervision,delegation, or team management by physicians;American Association of Nurse Practitioners, 2015).
Risk of Bias
A total of seven studies were excluded because of riskof bias after full-article review. Six studies wereexcluded because they used bivariate analyses withoutadjusting for potential confounders, and one studywasexcluded because a substantial amount ofmissing dataconsiderably diminished the validity of study findings.The risk of bias among the included studies wasdeemed acceptable.
The Impact of State SOP Regulation on NP Workforce
Eight studies included in this review examined the ef-fects of state SOP regulations on the NP workforce,including supply, mobility, and geographic distribu-tion. Consistent evidence has shown that the numberof NPs and growth of the NP workforce were highest instates with greater practice authority. Evidence fromfour studies indicates that states with more favorableNP practice environments have higher per capita NPs(Auerbach, 2000; Kuo et al., 2013; Reagan & Salsberry,2013; Stange, 2014). By 2010, states with full SOP regu-lations had an average of 25 more NPs per 100,000population (95% confidence interval [1.2, 48.3])compared with states with the most restrictive SOPregulations (Kuo et al., 2013).
One study found that growth of the NP workforcefrom 2001 to 2008 was significantly higher in stateswith full SOP regulations: 100% growth in states withfull SOP regulations, 92% in states with reduced regu-lations, and 73% in states with restrictive regulations(Reagan & Salsberry, 2013). Another study found thatgrowth in the number of NPs per capita was 14.8%higher in states with the least restrictive SOP regula-tions compared with states with the most restrictionsbetween 2006 and 2010 (Kuo et al., 2013). Consistent

Records identified through databases searching
(n =634)
Additional records identified through search of Google
Scholar and references (n=8)
Records after duplicates removed(n = 529)
Records screened(n =529)
Records excluded (n=506):n=35, research outside the U.S.n=349, not empirical or quantitative studyn=122, did not examine the effect of state SOP regulations on healthcare delivery
Full-text articles assessed for eligibility
(n =22)
Full-text articles excluded (n=7): n=6, bivariate analysisn=1, substantial missing data
Studies included in quantitative review and
synthesis(n =15)
Figure 1 e Flow diagram of search and study selection.
Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 574
with these findings, states with regulations grantingNPs independent practice or prescription authority had30% and 13% higher enrollments in APRN programs,respectively (Kalist & Spurr, 2004). In addition, stateSOP regulation has been associated with NPs’ migra-tion, with NPs more likely to move from states withoutcontrolled substances prescription authority to stateswith this authority (Perry, 2012).
Two studies reported moderate effects of state SOPregulations on the geographic distribution of NPs.States that granted independent practice and third-party reimbursement had a more equitable distribu-tion of NPs per capita across counties than states thatdid not (Lin, Burns, & Nochajski, 1997). Moreover, in astudy examining the distribution of NPs in urban andrural areas, a trendwas observed in which NPswere 1.5times more likely to practice in rural areas in stateswith full SOP regulations compared with states withrestrictive regulations (Kaplan, Skillman, Fordyce,McMenamin, & Doescher, 2012).
The Impact of State SOP Regulation on Care Provisionby NPs
Five studies provide evidence indicating that stateswith expanded practice authority showed the greatest
growth and advancement of NP primary care provi-sion. NPs had more authority in prescribing selectedmedications in states with less restrictive SOP regula-tory environment (Pan, Straub, & Geller, 1997). From1998 to 2010, the number of NPs providing primary carefor Medicare fee-for-service patients increased from0.6% to 5.3% in states with full SOP regulations, from0.2% to 3% in states with reduced SOP regulations, andfrom 0.2% to 2.5% in states with restrictive SOP regu-lations. These differential growth rates resulted in asizable gap in NP care provision across states by 2010;the odds of Medicare fee-for-service beneficiarieshaving an NP as a primary care provider was 2.5 timeshigher in states with the least restrictive NP SOPregulation than those in states with the most restric-tive regulation (Kuo et al., 2013).
Evidence further suggests that less restrictive SOPregulationwas linkedwith promoting care provision byNPs in rural and medically underserved areas. Ruralhospitals located in states granting prescriptive au-thority to NPs were 30% more likely than rural hospi-tals in states without this authority to establish aprovider-based rural health clinic, which are designedto stimulate the use of NPs and PAs to improve accessto primary care in underserved rural areas (Krein,1999). Community health centers, which are key

Table 1 e Characteristics of Studies
Study Purpose Study Designand Data
Measure for NPSOP Regulation
StatisticalAnalysis
Comments
Auerbach,2000
One aim examinedthe impact ofstate SOPregulation on thenumber of NPs.
Cross-sectionaltime seriesanalysis usingmultiple data setsincluding NSSRNfrom 1987 to 1996.
Index measure ofstate NP SOPregulatoryenvironment onlegal authority,reimbursement,and prescriptiveauthority,developed bySekscenski et al.*
State-level multipleregressionanalysis.
Examined theimpact of SOPregulation on thenumber of PCPsand NPsseparately. Didnot specify NPclinical specialty.Did not control forthe effect of thenumber of PAs inthe model.
Duekeret al., 2005
Examined howvariation in theprofessionalindependence ofAPRNs affects theearnings ofAPRNs,physicians, andPAs.
Cross-sectionaltime seriesanalysis usingCurrentPopulation Survey1988e2002.
Whether APRNshave independentprescriptiveauthority forcontrolledsubstances.
Individual-levelmultipleregressionanalysis includingstate-fixedeffects.
Analysis wasconducted for thesample of APRNs.Specialty APRNs’salary is usuallyhigher than NPs,and this was notadjusted for in theanalysis leadingto potential biasin the results. Thestudy did notspecify whetherthe physiciansample wascomposed of allprimary carephysicians anddid not describehow physiciansand PAs wereidentified fromthe data. Allincomes werecapped at 100,000in the originaldata; physicians’income was morelikely affected bythis measure.
Kalist andSpurr, 2004
Examined whetherlegislation on SOPof APRNs affectsenrollment inAPRN Master’sprograms.
Cross-sectionaltime seriesanalysis usingdata fromNational Leaguefor Nursingreports onenrollment inMaster’sprograms from1989 to 1995.
Two measures: (a)prescriptionauthority (high vs.low: whether NPscan prescribecontrolledsubstance) and (b)professionalindependence(high vs. low:whether NPs canpracticeindependently orwhether theBoard of Medicinehas a role indetermining theSOP).
State-level multipleordinary leastsquaresregression,weighted by statepopulation.
The sampleconsisted ofAPRNs. Did notcontrol fornumber ofnursing schoolsthat had Master’sprograms innursing, a time-varying variablethat might affecttotal number ofenrollments in astate.
(continued on next page)
Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 5 75

Table 1 e (Continued )
Study Purpose Study Designand Data
Measure for NPSOP Regulation
StatisticalAnalysis
Comments
Kaplanet al., 2012
Examined thedistribution ofNPs and CRNAs inrural and urbanareas, andwhether SOPregulations wereassociated withthis distribution.
Retrospective cross-sectional designusing NationalProvider Identifierdata 2010.
Three-levelcategoricalvariable: (a) fullautonomous, (b)requiresphysiciancollaboration, and(c) requiresphysiciansupervision.
Individual-levelmultipleregressionanalysis.
Did not specify NPclinical specialty.The analysis wasconducted at theindividual level toexamine theassociationbetween NP SOPregulations andNP practicelocation (rural/urban). Theanalysis did notadjust for theclustering effectby state and onlycontrolled forgender and percapita NP supplyin a state. Themodel might haveomitted otherimportantcovariates.
Krein, 1999 One aim examinedwhether ruralhospitals locatedin states with amore favorablestate practiceenvironment forNPs and/or PAswere more likelyto establishprovider-basedrural healthclinics.
Cross-sectionaltime seriesanalysis usingmultiple data setsincluding AHRFfrom 1990 to 1995.
A dichotomizedvariable onwhether a stategrants NPsprescriptiveauthority.
Hospital leveldiscrete-timelogisticregression.
NP specialty was notspecified;however, it is verylikely to beprimary care asNPpractice settingwas rural healthclinics. Authorsacknowledgedthat the modelmight haveomitted importantcovariates.Indeed, the modeldid not control forthe supply of NPsand PAs.
Ku et al., 2015 Examined differentmedical staffingpatterns incommunityhealth centers,the impact ofstaffing onproductivity, staffroles, and thefactors, includingNP SOPregulation, thataffect staffingpatterns.
Cross-sectionalanalysis usingdata from 2012HRSA UniformData System andAHRF.
Three-levelcategoricalvariable: (a) fullSOP, (b) partialSOP (NPs couldtreat but notprescribe), and (c)restricted SOP(most NPs’ actionsmust beauthorized by aphysician).
Multivariateordinary leastsquaresregressionanalysis.
The sample ofadvanced-practice staffincludedNPs, PAs,and CNMs. NPspecialty was notspecified;however, it is verylikely to beprimary care aspractice settingwas communityhealth centers.Authorsacknowledgedthat the studymight misclassifystaff rolesbecause oflimitation in thedata.
(continued on next page)
Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 576

Table 1 e (Continued )
Study Purpose Study Designand Data
Measure for NPSOP Regulation
StatisticalAnalysis
Comments
Kuoet al., 2013
Assessed thegrowth in primarycare provision byNPs and how itvaried by practicesettings and by NPSOP regulations.
Cross-sectionaltime seriesanalysis usingMedicarebeneficiarysample claimsdata from 1998to 2010.
Three-levelcategoricalvariable: (a)independentpractice andprescriptionauthority, (b)allowingindependentpractice butrequiringsupervision forprescriptions, and(c) requiringphysiciansupervision forpractice andprescriptions.
Multilevel modelingincludingindividual patientand state-levelvariables.
NP sampleconsisted ofthose whoprovided primarycare to a 5%random sampleof Medicare fee-for-servicebeneficiaries inall states.Authorsacknowledgedthat “measuringonly NP chargeswould tend tounderestimatetotal NP activity.”They alsomentioned thatthey mightoverestimate theextent of primarycare servicesprovided by NPsby includingapproximately 5%of NPs in adultoutpatientsettings whowere not inprimary care.It is unclearwhether NPs instates with fullSOP were morelikely to submitbilling claimsthan NPs in otherstates withrestrictiveregulations.
Lin et al., 1997 One aim examinedthe relationshipbetween statelegalenvironments forNPs and theavailability andsupply of NPs.
Cross-sectionalstudy designusing State Boardof Nursing listingof NPs in 1994,the listing ofcertified NPsfrom AmericanNursesCredentialCenter for thosestates that didnot have thelisting, andAHRF 1993.
Categorical codingfor presence orabsence ofindependentpractice andthird-partyreimbursement.
County-levelmultipleregressionanalysis.
Did not specify NPclinical specialty.The unit ofanalysis wascounty, which isnot a desirablearea unit toexamineavailability ofproviders.
(continued on next page)
Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 5 77

Table 1 e (Continued )
Study Purpose Study Designand Data
Measure for NPSOP Regulation
StatisticalAnalysis
Comments
Pan et al., 1997 Examined theeffects of state NPSOP regulation onNP’s autonomy inprescribingselectedcategories ofmedications.
Cross-sectionaldesign using 1992national samplesurvey of certifiedNPs and CNSs.
Index measure forNP practiceenvironmentdeveloped by theNew York RuralHealth ResearchCenter.y Themeasure wasbased on legalrecognition,requirements foreducationalprogram andcertification,continuingeducation clause,grandfatherclause,regulatoryagency,prescribingauthority, scopeof practice, andreimbursementregulations, withscore rangesfrom 20 (least) to82 (most).
Individual-levelmultipleregressionanalysis.
More than 90% ofthe NP samplepracticed in theareas of adults,family/community,pediatric,gerontological/geriatric, and OB/GYN. State-levelvariables weredisaggregated atthe individuallevel.
Perry, 2009 Examined theimpact of changesin SOP regulationsfor NPs and PAson NPs’, PAs’, andphysicians’incomes.
Cross-sectionaltime seriesanalysis usingNSSRN 1992e2004(for NPs), AAPAAC1996e2004 (forPAs), and CPSannual social andeconomicsupplement1996e2005 (forphysicians).
Dichotomousvariable forpresence orabsence ofprescriptiveauthority forcontrolledsubstances andthird-partyreimbursementfor NPs and PAs,respectively.
Individual-levelmultipleregressionanalysis usedHubereWhitestandard errors toadjust for clustereffect.
Did not specify NPclinical specialty.The analysis wasdisaggregated onthe individuallevel withadjustment forstandard errorsusing HubereWhite method.Did not control foroverall supply ofNPs, PAs, orphysicians, whichmight have animpact onincome.
Perry, 2012 Examined theimpact of NPs’prescriptiveauthority forcontrolledsubstances on NPmigration choicesfrom state tostate.
Cross-sectionaltime seriesanalysis usingNSSRN 1992e2004.
Dichotomousvariable forpresence orabsence ofprescriptiveauthority forcontrolledsubstances.
Individual-levelmultipleregressionanalysis.
Did not specify NPclinical specialty.Lack oftheoreticalguidance onselection ofcovariates. It islikely that themodel omittedsome importantcovariates, suchas income.
(continued on next page)
Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 578

Table 1 e (Continued )
Study Purpose Study Designand Data
Measure for NPSOP Regulation
StatisticalAnalysis
Comments
Reagan andSalsberry,2013
Examined theimpact of state NPSOP regulation onthe number andgrowth of NPs.
Cross-sectionalanalysis usingAHRF 2008.
Three-levelcategoricalvariable: (a) nopracticerestrictions, (b)some restrictions(requirecollaborativeagreement forprescription), or(c) mostrestrictions(collaborativeagreement fordiagnosis,treatment, andprescription).
Health service arealevel leastsquared multipleregression,weighted by areapopulation.
Did not specify NPclinical specialty.The growth of NPswas evaluatedbased on thechanges in thenumber of NPsbetween 2000 and2008; however,covariates wereonly available forYear 2008.
Shi andSamuels, 1997
Examined therelationshipbetween statevariations in theregulation of NPs,PAs, and CNMsand theemployment ofthesepractitioners bycommunityhealth centers.
Cross-sectionaldesign using datafrom communityhealth centersurvey in 1992.
Index measuremethoddeveloped bySekscenski et al.*
Individualcommunityhealth centerelevel multipleregressionanalysis.
NP specialtywas notspecified;however, it is verylikely to beprimary care aspractice settingwas communityhealth centers. Itis unclearwhether theanalysis adjustedfor clusteringeffect ofcommunityhealth centers bystate. Authorsacknowledgedthat the analysismight omitpotentiallyimportantcovariates, suchas theemployment ofpractitioners,physicians, othercentercharacteristics(e.g., financialarrangement),and personalcharacteristics(e.g., ruralexposure).
(continued on next page)
Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 5 79

Table 1 e (Continued )
Study Purpose Study Designand Data
Measure for NPSOP Regulation
StatisticalAnalysis
Comments
Spetzet al., 2013
Examined variationin NP SOPregulations acrossstates on the costsof retail clinics.
Cross-sectionaltime seriesanalysis usingadministrativeclaims data from2004 to 2007. Thedata included 27states withdifferent types ofSOP regulationsfor NPs.
Three-levelcategoricalvariable: (a) NPspractice andprescribeindependently, (b)NPs practiceindependently,prescribe onlywhencollaborating withor supervised by aphysician, and (c)NPs practice andprescribecollaborativelywith a physician,or NPs aresupervised forpractice andprescribing by aphysician.
Individual-levelmultipleregressionanalysis.
NP specialtywas notspecified;however, it is verylikely to beprimary care aspractice settingwas retail clinics.Authorsacknowledgedthat the studymight havesample selectionbias. It is unclearwhether theanalysis adjustedfor cluster effectby state.
Stange, 2014 Examined theimpact of changesin NP workforceand SOPregulations forNPs and PAs onaccess, costs, andpatterns of healthcare utilization.
Cross-sectionaltime seriesanalysis usingstate licensingrecords, AHRF,and MEPS from1996 to 2008.
Used two differentmeasures for SOPregulations forNPs and PAs. Oneis an indexmeasure for theoverall practiceenvironment forNPs and PAs inthe state at asingle point intime, and thesecond is anindicator forwhether NPs andPAs are permittedto writeprescriptions forany controlledsubstances in agiven state andyear.
Fixed effectsordinary leastsquares multipleregressionanalysis and two-stage leastsquares multipleregressionanalysis.
Did not specify NPclinical specialty.Measurement forprovider supplywas based onlicense datawhich mightoverestimate thenumber ofpractitioners inactive practice.However, theauthordifferentiatedoutcomes inprimary care andnonprimary care(i.e., primary careoffice-basedvisits,nonprimary careoffice-based visitsetc.).The study onlyexamined oneaspect of access tocare, which ishaving a usualsource of care.
AAPAAC, American Academy of Physician Assistants Annual Census; AHRF, area health resource file; APRN, advance practiceregistered nurse; CNMs, certified nurse-midwives; CNSs, clinical nurse specialists; CRNAs, certified registered nurse anes-thetists; CPS, current population survey; HRSA, health resources and services administration; MEPS, Medical ExpenditurePanel Survey; NP, nurse practitioner; NSSRN, national sample survey of registered nurses; OB/GYN, obstetrician/gynecologist;PA, physician assistant; PCP, primary care physicians; SOP, scope-of-practice.* Sekscenski, E. S., Sansom, S., Bazell, C., Salmon, M. E., & Mullan, F. (1994). State practice environments and the supply ofphysician assistants, nurse practitioners, and certified nurse-midwives. New England Journal of Medicine, 331(19), 1266e1271.y Burns, P., Nochajski, T. (1995). Interrelationship of practice environment with the distribution of nurse practitioner and health relatedoutcomes. Buffalo, New York: New York Rural Health Research Center, State University of New York at Buffalo.
Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 580

Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 5 81
providers for medically underserved populations, weremore likely to hire additional NPs if located in stateswith more positive practice environments (Shi &Samuels, 1997). This finding was confirmed in arecent study by Ku, Frogner, Steinmetz, and Pittman,(2015) who found that SOP regulation was one of themost important determinants of staff composition infederally funded community health centers. Commu-nity health centers located in states with full SOP reg-ulations used slightly fewer physicians and slightlymore advanced practice staff including NPs, PAs, andcertified nurse-midwives. Community health centersbenefited from full SOP regulation by having moreflexibility in staffing choice, which is especially signif-icant given these centers are located in areas with ashort supply of PCPs (Ku et al., 2015).
The Impact of State SOP Regulation on Access to Careand Health Care Utilization
Only a single study, conducted by Stange (2014)examined the impact of state NP SOP regulations onprimary care access and utilization; fortunately, thestudy was rigorously designed and provided insightfulresults. Access to care was defined as whether an in-dividual had a usual source of care, and health careutilization was examined as the number of office-based visits (primary care, nonprimary care and over-all) and use of preventive care services, such as gettinga flu shot, checking blood pressure or cholesterol,having a breast examination, or having a pap smear, inthe past 12 months.
The study found a significant impact of NP SOPregulations on health care utilization but no conclusiveevidence of an impact on access to care. With regard tohealth care utilization, the study revealed four impor-tant findings. First, the study found no evidence that alarger supply of NPs alone had any effect on health careutilization. Second, granting prescriptive authority toNPs had a modest direct impact on health care utili-zation, increasing primary care and overall office-based visits by 3% among individuals who had atleast one visit. Third, this impact was moderated by NPsupply; specifically, the effect of full NP SOP regulationon increased health care utilization was greatest instates with a larger per capita supply of NPs, indicatingthat changes in both practice environment and pro-vider supply may be necessary to produce the greatestimpact on health care utilization. Finally, further sub-group analysis by insurance status indicated a trend inwhich the interactive effects of full NP SOP regulationtogether with larger NP supply on health care expen-diture was only apparent for the uninsured group butnot for the insured group.
Impact of State NP SOP Regulation on Health CareCosts
From a societal point of view, the cost of health caredelivery includes many facets, such as compensation
for health care providers, unit price of health careservices, health care utilization expenditures, andothers. Four of the reviewed studies provided infor-mation on the impact of state NP SOP regulations onhealth care costs, including health care providers’ in-come, office-based visit expenditures, and retail cliniccosts.
Two studies that examined the effects of NP SOPregulation on health care providers’ incomes arrived atpartially inconsistent results. Dueker, Jacox, Kalist, andSpurr (2005) found that granting prescriptive authorityto APRNs for controlled substances was associatedwith lower earnings for APRNs and physicians buthigher earnings for PAs. Perry (2009) found thatexpanded SOP regulation granting greater prescriptiveauthority for controlled substances for NPs was asso-ciated with slightly higher earnings for NPs but lowerearnings for physicians and PAs. The mixed findingsmight be explained, in part, by the different samplesused in these studies. The study by Dueker et al. (2005)focused on a sample of APRNs that included NPs,certified registered nurse anesthetists, certified nurse-midwives, and clinical nurse specialists, whereas thestudy by Perry (2009) involved a sample consistingexclusively of NPs. Future studies are needed to betterunderstand the impact of SOP regulation on healthcare providers’ incomes and the mechanisms under-lying this potential relationship.
According to conventional labor market theory,greater practice authority combined with increased NPsupply should reduce office-based visit unit price byincreasing market competition or improving produc-tivity through effective collaboration. However, Stange(2014) found that the expansion of NP SOP regulationdid not affect office-based visit price, which wasmeasured as the total charges per visit. As explained bythe author, this finding might be due to a noncompet-itive primary care market in which currentreimbursement-driven policies involve rigid price-setting, restrictions in NP service reimbursement, andincentives for physician involvement to bill at a higherrate. Alternatively, if health care demand is higher instates with full NP SOP regulations, then such regula-tory changes in practice environment along withincreased NP supply are less likely to affect office-based visit price, whichwas not examined in the study.
Spetz, Parente, Town, and Bazarko (2013) examinedthe economic impact of state SOP regulations in retailclinics where NPs provided primary care services. Theauthors evaluated a 14-day episode of health care useand costs that included both insurers’ expendituresand patients’ out-of-pocket payments for 10 of themost common clinical conditions across all health caresettings. They found that the weighted average 14-daycost was $543 per clinic visit in states with restrictiveSOP regulations, $484 in states with reduced SOP reg-ulations, and $509 in states with full SOP regulations.Consistent with expectations, retail clinic costs werehighest in states with the most restrictive NP practiceenvironments. However, the unexpected finding of

Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 582
higher costs in states granting NPs both independentpractice and prescription authority compared withstates with only independent practice authority mighthave been due to the greater number of prescriptions(and concomitant higher cost) in states granting pre-scription authority to NPs.
Discussion
Synthesis of the extant literature reveals an emergingpattern regarding the potential impact of NP SOPregulation on health care delivery. States granting NPsgreater SOP authority tend to exhibit (a) an increase inthe number and growth of NPs through higher APRNeducational enrollment and migration and (b) greaterprovision of primary care by NPs and expanded healthcare utilization, especially among rural and vulnerablepopulations. Research findings on the effects of full NPSOP regulation on health care costs are mixed.
Role of NP SOP Regulations in Health Care Delivery
State NP SOP regulations play a central role in NPs’ caredelivery. Our review indicates that a large supply ofNPs alone does not appear to have an impact on healthcare utilization, only when combined with greaterpractice authority is the expansion of the NPworkforcerelated to increases in health care utilization. Thegreater the supply of NPs, the stronger the effect of fullNP SOP regulation on NP primary care provision andhealth care utilization. Thus, the evidence is consistentwith the view that expandedNP practice regulation canimpact health care delivery by increasing the numberof NPs in combination with easing restrictions on theirSOP. Under restrictive SOP regulations, NPs cannotfunction as independent providers, and requirementsfor collaboration or supervision by physicians limithow and where NPs can deliver care. One qualitativestudy that was conducted across six states withdifferent types of NP SOP regulations provides illus-trative insights (Yee, Boukus, Cross, & Samuel, 2013).The study found that NPs in states with reduced orrestrictive SOP regulations performed the same typesof primary care services as NPs in states with full SOPregulation. However, restrictive state regulationsrequiring physician collaboration and supervisioncreated documentation requirements that restrictedNPs to be geographically close to physicians, therebylimiting their choice of practice location. As physiciansare more likely to be concentrated in urban/suburbansettings and in non-Health Professional Shortage Areas(HPSAs), these restrictive regulations disproportionallyimpacted underserved and rural communities.
The current review does not lend any evidencesupporting an association between NP SOP regulationand access to care, which is defined in one study ashaving a usual source of care among the general pop-ulation. Several factors, which were not examined in
the reviewed study, may help explain this finding.First, research has shown that having a usual source ofcare is primarily dependent on health insurance statusand ability to pay (DeVoe, Tillotson, & Wallace, 2009).Therefore, the effect of NP SOP regulation on having ausual source of care wouldmost likely bemoderated byhealth insurance status. Second, the effect of NP SOPregulation on having a usual source of carewould likelybe stronger in HPSAs where commensurate health fa-cilities, such as community health centers, wereavailable. Third, regardless of full SOP authority, NPsmight not be listed in provider directories, therebydiminishing the public’s awareness of the availabilityof care provision by NPs (Poghosyan et al., 2013).Fourth, access to care is a multidimensional conceptthat encompasses availability, accessibility, accom-modation, affordability, and acceptability (Penchansky& Thomas, 1981). Dimensions of access to care otherthan usual source of care, such as appointmentwaitingtime, might be more responsive to NP SOP regulationwhen the effect is assessed among the insuredpopulation.
Study results on the effects of NP SOP regulation onhealth care costs are inconclusive. One study reportedsubstantial cost reductions in retail clinics in stateswith less restrictive regulations, whereas anotherstudy found no evidence that less restrictive NP SOPregulation was associated with a decrease in office-based visit price. The expected health care cost re-ductions afforded by the effective use of NPs inproviding primary care can be obfuscated by a practiceknown as “incident billing,” in which services providedby an NP under a physician’s supervision can be billedexclusively under the physician’s provider number andreimbursement rate.
Two recent simulation studies provide further in-sights on the potential economic impact of state NPSOP regulations. One study estimated the potentialcost savings in primary care in Alabama and suggestedthat removing restrictions in NP/PA SOP regulationswould result in net saving of more than $729 millionover a 10-year period from 2013 to 2022, which was inlarge part due to decreases in compensating expendi-tures per primary care visit (Hooker & Muchow, 2015).The other study assessed the economic impact oflegislating full SOP regulations for APRNs in NorthCarolina and concluded that such legislation couldincrease the state’s economic output, gross domesticproduct, and tax revenue (Conover & Richards, 2015).
Implications
An important implication for state policy makers andstakeholders is that the differential growth rates in theNP workforce between states with and withoutrestrictive regulations could result in sizeable gaps inthe number of NPs across states, which, in combina-tion with changes to the regulatory environment,might translate into substantial state-level disparitiesin health care provision, utilization, and outcomes,

Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 5 83
especially in rural and vulnerable population areas.Although existing evidence is limited on the effect ofNP SOP regulation on access to care, the evidence isunequivocal with regard to increased health care uti-lization, including office-based visits and prescriptionsfilled. Although more research is needed on the impactof NP SOP regulation on lowering health care costs, onestudy has shown a reduction in retail clinic costsassociated with such state legislation.
Our review identified several major gaps in extantliterature that can inform future research. First, limitedresearch has been conducted on the geographic dis-tribution of NPs, nationally, in relation to vulnerable ormedically underserved populations, and, importantly,the extent to which state NP SOP regulation affects thisdistribution. Although NPs tend to be more likely toserve in low-income, minority, and rural areas whencompared with PCPs (Grumbach, Hart, Mertz, Coffman,& Palazzo, 2003), the distribution of NPs per capita inrelation to vulnerable populations is not well under-stood. Understanding how the regulatory environmentcan influence the distribution of NPs in relation tovulnerable populations is critical for the developmentof effective health policy directives and levers toimprove access to care and meet the growing demandfor primary care among vulnerable populations. Sec-ond, research on the effect of SOP regulation on accessto care and health care utilization should focus moreon the groups and areas where demand for access tocare and health care utilization is greatest, such asmedically underserved populations or HPSAs. Wecurrently do not know whether the observed increasesin health care utilization (such as office visits andprescriptions) in states with full NP SOP regulations arereaching those with the greatest health care needs.Third, research is needed to examine the effect of SOPregulations on the role of NPs in team-based care, anapproach that has been increasingly adopted toimprove efficiency and effectiveness of primary caredelivery. Initial evidence has indicated a potential linkbetween full SOP regulations and improved team work(Poghosyan, Boyd, & Knutson, 2014).
Limitations
The findings of our review must be interpreted withinthe context of limitations. The number of studiesexamining the impact of state NP SOP regulation oncare provision by NPs, access to care and health careutilization, and health care costs is small. Moreresearch is needed in these areas. In addition, reviewedstudies on NP workforce did not specify NP clinicalspecialty (i.e., primary care or specialty care). Recentevidence has shown that at least half of NPs did notpractice in primary care and instead were in specialtyclinical fields (Spetz, Fraher, Li, & Bates, 2015; U.S.Department of Health and Human Services, HealthResources and Services Administration, & NationalCenter for Health Workforce Analysis, 2014). To betterunderstand the role of NPs in health care delivery, it is
important that future studies differentiate NP primarycare and specialty care practice, thus providing morefine-tuned evidence to inform health care policy.Therefore, although a discernible pattern has emergedfrom the existing studies, more research is needed toreplicate these results and to more fully explore fac-tors, such as insurance status and NP service reim-bursement policies, that might moderate the effects ofNP SOP regulation on health care delivery.
Conclusion
In summary, our review of the available evidencerevealed several consistent and promising patternswith regard to the potential impact of state NP SOPregulation on health care delivery. This evidencegenerally supports recommendations consistent withrecent trends in which state legislatures have reducedrestrictions on SOP regulations to provide a more in-dependent NP practice environment as a viable andeffective strategy to increase primary care capacity andhealth care utilization and potentially reduce costs(Gadbois, Miller, Tyler, & Intrator, 2015). This is espe-cially critical for states that face substantial shortagesof PCPs and increased care demand from rural andmedically underserved communities.
Acknowledgments
The authors gratefully acknowledge funding from theNational Council of State Boards of Nursing (Y.X., PI).
r e f e r e n c e s
AcademyHealth. (2015). The AcademyHealth Listening Project:Improving the evidence base for Medicaid policymaking. Retrievedfrom http://academyhealth.org/files/publications/AcademyHealth%20Listening%20Project%202015%20Full%20Report.pdf.
Adashi, E. Y., Geiger, H. J., & Fine, M. D. (2010). Health care reformand primary caredThe growing importance of the communityhealth center. The New England Journal of Medicine, 362(22),2047e2050.
American Association of Nurse Practitioners. (2015). State practiceenvironment: States categorized by type. Retrieved from http://www.aanp.org/legislation-regulation/state-legislation-regulation/state-practice-environment/66-legislation-regulation/state-practice-environment/1380-state-practice-by-type.
Auerbach, D. I. (2000). Nurse practitioners and primary carephysicians: Complements, substitutes and the impact ofmanaged care. Harvard Health Policy Review, 1(1), 83e94.
Auerbach, D. I., Chen, P. G., Friedberg, M. W., Reid, R., Lau, C.,Buerhaus, P. I., & Mehrotra, A. (2013). Nurse-managed healthcenters and patient-centered medical homes could mitigateexpected primary care physician shortage. Health Affairs(Millwood), 32(11), 1933e1941.
Bodenheimer, T., Chen, E., & Bennett, H. D. (2009). Confrontingthe growing burden of chronic disease: Can the U.S. health

Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 584
care workforce do the job? Health Affairs (Millwood), 28(1),64e74.
Conover, C., & Richards, R. (2015). Economic benefits of lessrestrictive regulation of advanced practice nurses in NorthCarolina. Nursing Outlook, 63(5), 585e592.
DeVoe, J. E., Tillotson, C. J., & Wallace, L. S. (2009). Usual source ofcare as a health insurance substitute for U.S. adults withdiabetes? Diabetes Care, 32(6), 983e989.
Dower, C., Moore, J., & Langelier, M. (2013). It is time to restructurehealth professions scope-of-practice regulations to removebarriers to care. Health Affairs (Project Hope), 32(11), 1971e1976.
Druss, B. G., Marcus, S. C., Olfson, M., Tanielian, T., & Pincus, H. A.(2003). Trends in care by nonphysician clinicians in the UnitedStates. The New England Journal of Medicine, 348(2), 130e137.
Dueker, M. J., Jacox, A. K., Kalist, D. E., & Spurr, S. J. (2005). Thepractice boundaries of advanced practice nurses: Aneconomic and legal analysis. Journal of Regulatory Economics,27(3), 309e329.
Gadbois, E. A., Miller, E. A., Tyler, D., & Intrator, O. (2015). Trendsin state regulation of nurse practitioners and physicianassistants, 2001 to 2010. Medical Care Research and Review:MCRR, 72(2), 200e219.
Glied, S., & Ma, S. (2015). How will the Affordable Care Act affectthe use of health care services? The Commonwealth Fund VolNo.(February 2015), xx-xx.
Grumbach, K., Hart, L. G., Mertz, E., Coffman, J., & Palazzo, L.(2003). Who is caring for the underserved? A comparison ofprimary care physicians and nonphysician clinicians inCalifornia and Washington. Annals of Family Medicine, 1(2),97e104.
Hansen-Turton, T., Bailey, D. N., Torres, N., & Ritter, A. (2010).Nurse-managed health centers. The American Journal ofNursing, 110(9), 23e26.
Health Resources and Services AdministrationNational Center forHealth Workforce Analysis (2013). Projecting the supply anddemand for primary care practitioners through 2020. Rockville,Maryland: U.S. Department of Health and Human Services.
Hooker, R. S., & Muchow, A. N. (2015). Modifying state laws fornurse practitioners and physician assistants can reduce costof medical services. Nursing Economic$, 33(2), 88e94.
Huang, E. S., & Finegold, K. (2013). Seven million Americans live inareas where demand for primary care may exceed supply bymore than 10 percent. Health Affairs (Millwood), 32(3), 614e621.
Jennings, N., Clifford, S., Fox, A. R., Oconnell, J., & Gardner, G.(2015). The impact of nurse practitioner services on cost,quality of care, satisfaction and waiting times in theemergency departmentdA systematic review. InternationalJournal of Nursing Studies, 52(1), 421e435.
Kalist, D. E., & Spurr, S. J. (2004). The effect of state laws on thesupply of advanced practice nurses. International Journal ofHealth Care Finance and Economics, 4(4), 271e281.
Kaplan, L., Skillman, S., Fordyce, M., McMenamin, P., &Doescher, M. (2012). Understanding APRN distribution in theUnited States using NPI data. The Journal for Nurse Practitioners:JNP, 8(8), 626e635.
Krein, S. L. (1999). The adoption of provider-based rural healthclinics by rural hospitals: A study of market and institutionalforces. Health Service Research, 34(1 Pt 1), 33e60.
Ku, L., Frogner, B. K., Steinmetz, E., & Pittman, P. (2015).Community health centers employ diverse staffing patterns,which can provide productivity lessons for medical practices.Health Affairs (Millwood), 34(1), 95e103.
Kuo, Y. F., Loresto, F. L., Jr., Rounds, L. R., & Goodwin, J. S. (2013).States with the least restrictive regulations experienced thelargest increase in patients seen by nurse practitioners. HealthAffairs (Millwood), 32(7), 1236e1243.
Landon, B. E., Hicks, L. S., O’Malley, A. J., Lieu, T. A., Keegan, T.,McNeil, B. J., & Guadagnoli, E. (2007). Improving the
management of chronic disease at community health centers.The New England Journal of Medicine, 356(9), 921e934.
Lin, G., Burns, P., & Nochajski, T. (1997). The geographicdistribution of nurse practitioners in the United States. AppliedGeographic Studies, 1(4), 287e301.
Morgan, P., Everett, C., & Hing, E. (2015). Nurse practitioners,physician assistants, and physicians in community healthcenters, 2006e2010. Healthcare, 3(2), 102e107.
National Academy for State Health Policy. (2015). The state of statehealth policy: Governors’ state of the state addresses. Retrievedfrom http://www.nashp.org/sites/default/files/SoS_Final2.pdf.
National Association of Community Health Centers. (2014).America’s health centers. Retrieved from http://www.nachc.com/client/documents/America%27s_CHCs1014.pdf.
National Council of State Boards of Nursing. (2014). APRNs in the U.S. Retrieved from https://www.ncsbn.org/4213.htm.
National Governors Association. (2012). The role of nursepractitioners in meeting increasing demand for primary care.Retrieved from http://www.nga.org/cms/home/nga-center-for-best-practices/center-publications/page-health-publications/col2-content/main-content-list/the-role-of-nurse-practitioners.html.
Naylor, M. D., & Kurtzman, E. T. (2010). The role of nursepractitioners in reinventing primary care. Health Affairs(Millwood), 29(5), 893e899.
Pan, S., Straub, L. A., & Geller, J. M. (1997). Restrictive practiceenvironment and nurse practitioners’ prescriptive authority.Journal of the American Academy of Nurse Practitioners, 9(1), 9e15.
Paradise, J., Dark, C., & Bitler, N. (2011). Improving access to adultprimary care in Medicaid: Exploring the potential role of nursepractitioners and physician assistants. Retrieved from http://kaiserfamilyfoundation.files.wordpress.com/2013/01/8167.pdf.
Penchansky, R., & Thomas, J. W. (1981). The concept of access:Definition and relationship to consumer satisfaction. MedicalCare, 19(2), 127e140.
Perry, J. J. (2012). State-granted practice authority: Do nursepractitioners vote with their feet? Nursing Research Practice,2012, 482178.
Perry, J. J. (2009). The rise and impact of nurse practitioners andphysician assistants on their own and cross-occupationincomes. Contemporary Economic Policy, 27(4), 491e511.
Poghosyan, L., Boyd, D., & Knutson, A. R. (2014). Nursepractitioner role, independent practice, and teamwork inprimary care. The Journal for Nurse Practitioners: JNP, 10(7),472e479.
Poghosyan, L., Nannini, A., Smaldone, A., Clarke, S., O’Rourke, N.C., Rosato, B. G., & Berkowitz, B. (2013). Revisiting scope ofpractice facilitators and barriers for primary care nursepractitioners: A qualitative investigation. Policy, Politics &Nursing Practice, 14(1), 6e15.
Pohl, J. M., Hanson, C., Newland, J. A., & Cronenwett, L. (2010).Unleashing nurse practitioners’ potential to deliver primarycare and lead teams. Health Affairs (Millwood), 29(5), 900e905.
Reagan, P. B., & Salsberry, P. J. (2013). The effects of state-levelscope-of-practice regulations on the number and growth ofnurse practitioners. Nursing Outlook, 61(6), 392e399.
Shi, L., & Samuels, M. E. (1997). Practice environment and theemployment of nurse practitioners, physician assistants, andcertified nurse midwives by community health centers. Journalof Allied Health, 26(3), 105e111.
Spetz, J., Fraher, E., Li, Y., & Bates, T. (2015). How many nursepractitioners provide primary care? It depends on how youcount them. Medical Care Research and Review: MCRR, 72(3),359e375.
Spetz, J., Parente, S. T., Town, R. J., & Bazarko, D. (2013). Scope-of-practice laws for nurse practitioners limit cost savings thatcan be achieved in retail clinics. Health Affairs (Project Hope),32(11), 1977e1984.

Nur s Ou t l o o k 6 4 ( 2 0 1 6 ) 7 1e 8 5 85
Stange, K. (2014). How does provider supply and regulationinfluence health care markets? Evidence from nursepractitioners and physician assistants. Journal of HealthEconomics, 33, 1e27.
U.S. Department of Health and Human Services, HealthResources and Services Administration, & National Centerfor Health Workforce Analysis. (2014). Highlights from the
2012 National Sample Survey of Nurse Practitioners. Rockville,Maryland: U.S. Department of Health and HumanServices.
Yee, T., Boukus, E., Cross, D., & Samuel, D. (2013). Primary careworkforce shortages: Nurse practitioner scope-of-practice laws andpayment policies. Research Brief (Vol. 13). Washington, DC:National Institute for Health Care Reform.