Impact of macroeconomic status on prehospital management ... · deprivation indices, and stroke....
12
ISSN 2044-9038 10.2217/CPR.13.68 © 2013 Future Medicine Ltd 701 part of Clin. Pract. (2013) 10(6), 701–712 Research Article Impact of macroeconomic status on prehospital management, in-hospital care and functional outcome of acute stroke in China Ruijun Ji 1 , David Wang 2 , Gaifen Liu 1 , Haipeng Shen 3 , Yilong Wang 1 , Hao Li 1 , Lee H Schwamm 4 & Yongjun Wang* 1 ; on behalf of China National Stroke Registry (CNSR) investigators 1 Tiantan Comprehensive Stroke Center, Beijing Tiantan Hospital, Capital Medical University, No.6 Tiantanxili, Dongcheng District, Beijing 100050, China 2 Illinois Neurological Institute, Peoria, IL, USA 3 Department of Statistics & Operation Research, University of North Carolina, Chapel Hill, NC, USA 4 Department of Neurology, Massachusetts General Hospital, Boston, MA, USA *Author for correspondence: Tel.: +86 10 6701 3383; Fax: +86 10 6709 8350; [email protected] Practice Points Socioeconomic status is a multidimensional concept that comprises different indicators and is an important predictor of stroke incidence and mortality. Prior studies mainly focused on the potential association between microindicators of socioeconomic status and stroke, such as education, income, occupation, material ownership and area-based deprivation indices, and stroke. There is limited knowledge on the potential impact of macroeconomic status on prehospital management, in-hospital quality of care and functional outcome after stroke. This study was based on the largest stroke registry in China, the China National Stroke Registry. Based on the average gross regional product (GRP) per capita in 2008, provinces in China were classified into: developed (GRP per capita above average level) and underdeveloped (GRP per capita below average level) areas. Two variables and ten performance measures were used as quality indicators for prehospital management and in-hospital care, respectively. A summary composite measure was calculated by using an opportunity-based score. Good functional outcome was defined as modified Rankin Scale score ≤2 at discharge. It was found that higher GRP per capita was associated with better prehospital management, higher quality of in-hospital care and improved functional outcome at
Transcript of Impact of macroeconomic status on prehospital management ... · deprivation indices, and stroke....

ISSN 2044-903810.2217/CPR.13.68 © 2013 Future Medicine Ltd 701
part of
Clin. Pract. (2013) 10(6), 701–712
Research Article
Impact of macroeconomic status on prehospital management, in-hospital care and functional outcome of acute stroke in China
Ruijun Ji1, David Wang2, Gaifen Liu1, Haipeng Shen3, Yilong Wang1, Hao Li1, Lee H Schwamm4 & Yongjun Wang*1; on behalf of China National Stroke Registry (CNSR) investigators
1Tiantan Comprehensive Stroke Center, Beijing Tiantan Hospital, Capital Medical University, No.6 Tiantanxili, Dongcheng District, Beijing 100050, China 2Illinois Neurological Institute, Peoria, IL, USA 3Department of Statistics & Operation Research, University of North Carolina, Chapel Hill, NC, USA 4Department of Neurology, Massachusetts General Hospital, Boston, MA, USA *Author for correspondence: Tel.: +86 10 6701 3383; Fax: +86 10 6709 8350; [email protected]
Practice Points � Socioeconomic status is a multidimensional concept that comprises different indicators
and is an important predictor of stroke incidence and mortality. Prior studies mainly
focused on the potential association between microindicators of socioeconomic status
and stroke, such as education, income, occupation, material ownership and area-based
deprivation indices, and stroke. There is limited knowledge on the potential impact of
macroeconomic status on prehospital management, in-hospital quality of care and
functional outcome after stroke.
� This study was based on the largest stroke registry in China, the China National Stroke
Registry. Based on the average gross regional product (GRP) per capita in 2008,
provinces in China were classified into: developed (GRP per capita above average level)
and underdeveloped (GRP per capita below average level) areas. Two variables and ten
performance measures were used as quality indicators for prehospital management and
in-hospital care, respectively. A summary composite measure was calculated by using
an opportunity-based score. Good functional outcome was defined as modified Rankin
Scale score ≤2 at discharge.
� It was found that higher GRP per capita was associated with better prehospital
management, higher quality of in-hospital care and improved functional outcome at

Clin. Pract. (2013) 10(6)702 future science group
Research Article | Ji, Wang, Liu et al.
Stroke is one of the leading causes of death and adult disability worldwide [1]. The importance of socioeconomic status (SES) as a predictor of stroke incidence, mortality and impact has been discussed previously [1–4]. However, SES is a multidimensional concept and comprises different indicators [2,5]. Prior studies mainly focused on microindicators of SES, such as education, income, occupation, material own-ership and area-based deprivation indices [2,6–13]. Although some studies provided evidence that higher macro indicators of SES, such as gross domestic product (GDP), was associated with reduced stroke incidence and mortality [3,14,15], little is known about the potential impact of macroeconomic status on prehospital manage-ment, in-hospital quality of care and functional outcome after stroke.
After implementing The Open Door Policy in the early 1980s, China has experienced high eco-nomic growth during the last three decades. The GDP per capita has risen from US$195 in 1980 to US$4428 in 2010 (according to the World Bank). However, due to historical reasons (The Open Door Policy originated in the southeast coastal area and then spread throughout the country), such fast-pace economic growth is unevenly distributed across China. According to the National Bureau of Statistics of China, Shanghai had the highest gross regional product (GRP; 13,698.15 billion Yuan) and the in-land province Guizhou had the lowest (3333.4 bil-lion Yuan) in 2008. Such disparity in economic growth did offer a unique opportunity to study the potential impact of macro economic status on stroke care and outcomes.
discharge after ischemic stroke (acute ischemic stroke/transient ischemic attack). Higher
GRP per capita was also associated with better prehospital management and functional
outcome at discharge after hemorrhagic stroke (subarachnoid hemorrhage/intracerebral
hemorrhage). However, macroeconomic status (GRP per capita) showed less impact on
in-hospital quality of care for hemorrhagic stroke.
Summary: Aim: To examine the association between gross regional product (GRP) per
capita and prehospital management, in-hospital quality of care and functional outcome after
stroke. Methods: The study was based on the China National Stroke Registry between 2007
and 2008. Based on the average GRP per capita in 2008, provinces in China were divided into
developed and underdeveloped areas. Two variables and ten performance measures were
used as quality indicators for prehospital management and in-hospital care, respectively. Good
functional outcome was defined as a modified Rankin Scale score ≤2 at discharge. A summary
composite measure was calculated by using an opportunity-based score. A generalized
estimation equation was performed to adjust for confounders. Results: For ischemic stroke (acute
ischemic stroke/transient ischemic attack), compared with patients in the underdeveloped area
(n = 7573), those in the developed area (n = 8516) received better prehospital management
(adjusted odds ratio [OR]: 1.03; 95% CI: 1.02–1.04; p < 0.001) and a higher quality of in-hospital
care (adjusted OR: 1.02; 95% CI: 1.01–1.03; p < 0.001). Higher GRP per capita was significantly
associated with better functional outcome (modified Rankin Scale score ≤2) at discharge after
ischemic stroke (adjusted OR: 1.11; 95% CI: 1.02–1.20; p < 0.001). A similar association between
GRP per capita and prehospital management (p < 0.001) and primary outcome (p < 0.001) was
found for hemorrhagic stroke (subarachnoid hemorrhage/intracranial hemorrhage). Conclusion:
Higher GRP per capita was associated with better prehospital, in-hospital quality of stroke care
and functional outcome at discharge after acute stroke.

703future science group www.futuremedicine.com
Impact of macroeconomic status on acute stroke outcome in China | Research Article
Using data from the largest stroke registry in China, the China National Stroke Registry (CNSR), we examined the association between macroeconomic status and prehospital manage-ment, in-hospital quality of care, and stroke outcomes at discharge.
Methods�� Ethics statement
This study was approved by an ethics committee at each site within the CNSR network.
�� Study populationThe methodology of CNSR has been described previously [16]. In brief, hospitals in China are classified into three grades:
� Grade I (community hospitals);
� Grade II (hospitals serving several communities);
� Grade III (central hospitals for a certain district or city).
In total, 242 potential sites, including 114 grade III, 71 grade II and 57 grade I hospitals, from both urban and rural areas, were initially identified by soliciting applications. The CNSR steering committee evaluated the research capabil-ity and commitment to the registry of each hos-pital with a preliminary survey. Finally, a total of 132 hospitals including 100 grade III and 32 grade II were selected, which cover 27 provinces and four municipalities across China. Trained research coordinators at each institute reviewed medical records daily to identify, consent and enroll con-secutively eligible patients. To be eligible for this study, subjects had to meet the following criteria:
� Age 18 years or older;
� Hospitalized with a primary diagnosis of suba-rachnoid hemorrhage (SAH), intracerebral hemorrhage (ICH), acute ischemic stroke (AIS) or transient ischemic attack (TIA) according to WHO criteria [17] and with computed tomography or MRI confirmation;
� Direct admission to hospital from a physician’s clinic or emergency department;
� Written informed consent from patients or their legal representatives.
�� GRP per capita groupsGRP is conceptually equivalent to GDP and mea-sures newly created value through production
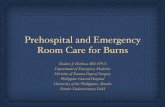
by regional production unit (‘province’ in this study). Based on the average GRP per capita in 2008 (25,377.38 Yuan ≈US$3,715.51), prov-inces in China were classified into: developed areas with GRP per capita above average levels (median interquartile range [IQR]: 38,872.6; 31,558.6.5–62,802.7 Yuan; Shanghai, Beijing, Tianjin, Zhejiang, Jiangsu, Guangdong, Shan-dong, Inner Mongolia, Fujian, Liaoning and Hong Kong) and underdeveloped areas with GRP per capita below average levels (median IQR: 17,116.2; 14,345.6–19,530.8 Yuan; Jilin, Hebei, Heilongjiang, Shanxi, Xinjiang, Hubei, Henan, Shaanxi, Chongqing, Ningxia, Hunan, Qinghai, Hainan, Sichuan, Guangxi, Jiangxi, Anhui, Tibet, Yunnan, Gansu and Guizhou) (Figure 1).
�� Measure of prehospital management & in-hospital quality of careIn this study, two variables were adopted to evaluate prehospital stroke management:
� Transportation mode to hospital, which was divided into emergency medical system (EMS) and private transportation (e.g., by taxi or private car);
� Time from symptom onset to hospital arrival, which was separated into ≤2 and >2 h.
According to prior studies [18], ten perfor-mance measures were used as quality indicators for in-hospital stroke care including:
� Intravenous tissue plasminogen activator in patients who arrive ≤2 h after symptom onset;
� Dysphagia screening prior to oral intake;
� Deep vein thrombosis (DVT) prophylaxis within 48 h of admission for nonambulatory patients;
� Antithrombotics within 48 h of admission;
� Rehabilitation assessment;
� Stroke education;
� Smoking cessation counseling;
� Discharge on anticoagulation for patients with atrial fibrillation;
� Discharge on antithrombotic medication;
� Discharge on cholesterol-reducing agent accord-ing to the National Cholesterol Education Panel Adult Treatment Panel III guidelines [19].
Patient adherence to individual performance measures was recorded and those with docu-mented reasons for ineligibility were excluded

Clin. Pract. (2013) 10(6)704 future science group
Research Article | Ji, Wang, Liu et al.
from the ana lysis for that measure. The results showed that the denominator, which indicated the total number of eligible patients, varied according to the measure. The proportion of eligible patients for each measurement was cal-culated by dividing the total number of patients receiving the intervention by the total number of patients who were eligible for the intervention. A summary composite measure of prehospital management and in-hospital quality of care was calculated by using an opportunity-based score [20], which was defined as the total number of measures performed in each subject divided by the total number of measures the subject was eligible for.
Stroke outcome assessmentIn the study, stroke outcomes at hospital dis-charge were evaluated. The primary outcome was a modified Rankin Scale (mRS) score of ≤2 at hospital discharge. Secondary outcomes included in-hospital mortality and in-hospital stroke-associated pneumonia (SAP). SAP was
defined as newly developed pneumonia (auscul-tatory respiratory crackles and fever [>38oC] or radiographic evidence or new purulent sputum) that occurred during the index hospitalization after acute stroke [21].
�� Statistical ana lysisThe association between macroeconomic status and prehospital management, in-hospital qual-ity of care and stroke outcomes was analyzed for ischemic stroke (AIS/TIA) and hemor-rhagic stroke (SAH/ICH), respectively. c2 test was used to compare the categorical variable and Mann–Whitney test or an independent t-test was employed to compare the continuous vari-able. Multivariate regression ana lysis using the generalized estimation equation (GEE) was per-formed to determine whether macroeconomic status (developed vs underdeveloped area) was associated with prehospital management, in-hospital quality of care and stroke outcomes. The GEE models considered clustering effects within hospitals [22] and adjusted for socio-demographics, risk factors (hypertension, dia-betes mellitus, dyslipidemia, atrial fibrillation, coronary heart disease, history of stroke/TIA and current smoking), stroke subtypes (AIS, TIA, SAH and ICH), Oxfordshire Commu-nity Stroke Project classification (partial ante-rior circulation infarct, total anterior circulation infarct; lacunar infarction and posterior circula-tion infarct) for ischemic stroke, admission NIH Stroke Scale score, length of hospital stay and hospital facilities (hospital grade, total number of beds in the hospital, academic status, equip-ment with emergency department, Neurointen-sive care unit and stroke unit). All tests were two-tailed and statistical significance was deter-mined at an a-level of 0.05. Statistical ana lysis was performed using SAS 9.1 (SAS Institute, NC, USA) and SPSS 16.0 (SPSS Inc., IL, USA).
Results�� Baseline characteristics
From September 2007 to August 2008, a total of 22,216 patients with acute cerebrovascu-lar events were enrolled in the CNSR. Among them, 767 were diagnosed with SAH, 5221 with ICH, 14,702 with AIS, 1387 with TIA and 139 with stroke of an undetermined type. For this study, 139 (0.6%) patients with stroke of an undetermined type were excluded. Based on average GRP per capita in 2008, study subjects
Underdeveloped areaDeveloped area
Figure 1. Developed and underdeveloped areas based on average national gross regional product per capita. Based on China's national average gross regional product per capita in 2008, provinces are classified into developed areas (Shanghai, Beijing, Tianjin, Zhejiang, Jiangsu, Guangdong, Shandong, Inner Mongolia, Liaoning, Fujian and Hong Kong) and underdeveloped areas (Jilin, Hebei, Heilongjiang, Shanxi, Xinjiang, Hubei, Henan, Shaanxi, Chongqing, Ningxia, Hunan, Qinghai, Hainan, Sichuan, Guangxi, Jiangxi, Anhui, Tibet, Yunnan, Gansu and Guizhou).

705future science group www.futuremedicine.com
Impact of macroeconomic status on acute stroke outcome in China | Research Article
(n = 22,077) were subgrouped into patients in developed areas (n = 11,828) and underdeveloped areas (n = 10,249). The baseline characteristics of the study population are listed in Table 1. The median age was 65 years (IQR: 55–74) and 38.8% were female. Compared with stroke patients in the underdeveloped areas, those in the developed areas were older (p < 0.001), more frequently had healthcare insurance (p = 0.001),
had a higher rate of hypertension (p < 0.001), diabetes mellitus (p < 0.001), hyperlipidemia (p = 0.005), atrial fibrillation (p < 0.001) and coronary artery disease (p < 0.001), a lower rate of smoking (p < 0.001), had more SAH (p < 0.001) and less TIA (p < 0.001), had a higher NIH Stroke Scale score on admission (p < 0.001) and were more likely to be treated in hospitals with better facilities (p < 0.001).
Table 1. Baseline characteristics by macroeconomic status.
Baseline characteristic Total(n = 22,077)
Developed areas(n = 11,828)
Underdeveloped areas (n = 10,249)
p-value
Sociodemographics, n (%)
Age, years, median (IQR) 65 (55–74) 66 (55–75) 63 (54–72) <0.001Gender (female) 8550 (38.7) 4633 (39.2) 3917 (38.2) 0.15Education level (high school or above) 5999 (27.2) 3177 (26.9) 2822 (27.5) 0.26Marital status (married) 19,798 (89.7) 10,566 (89.3) 9232 (90.1) 0.07Health insurance – – – <0.001Having no insurance (self-payment) 4725 (21.4) 2439 (20.6) 2286 (22.3) –Basic or government insurance 12,090 (54.8) 7153 (60.5) 4937 (48.2) –New rural cooperative insurance 4416 (20.0) 1722 (14.6) 2694 (26.3) –Commercial insurance 846 (3.8) 514 (4.3) 332 (3.2) –
Vascular risk factors, n (%)
Hypertension 13,927 (63.1) 7644 (64.6) 6283 (61.3) <0.001Diabetes mellitus 3876 (17.6) 2271 (19.2) 1605 (15.7) <0.001Hyperlipidemia 2146 (9.7) 1211 (10.2) 935 (9.1) 0.005Atrial fibrillation 1204 (5.5) 755 (6.4) 449 (4.4) <0.001Coronary artery disease 2588 (11.7) 1512 (12.8) 1076 (10.5) <0.001Family history of stroke 2753 (13.4) 1453 (13.3) 1300 (13.5) 0.70History of any stroke/transient ischemic attack 6408 (29.0) 3410 (28.8) 2998 (29.3) 0.49Current smoking 8551 (38.9) 4405 (37.5) 4146 (40.6) <0.001Prestroke disability (mRS ≥3) 1843 (8.3) 975 (8.2) 868 (8.5) 0.56
Stroke subtype, n (%)
Subarachnoid hemorrhage 767 (3.5) 486 (4.1) 281 (2.7) <0.001Intracranial hemorrhage 5221 (23.6) 2826 (23.9) 2395 (23.4) 0.36Acute ischemic stroke: 14,702 (66.6) 7870 (66.5) 6832 (66.7) 0.85
� Partial anterior circulation infarct 8168 (55.6) 4311 (54.8) 3857 (56.5) 0.07 � Total anterior circulation infarct 1327 (9.0) 721 (9.2) 606 (8.9) 0.57 � Lacunar infarction 2719 (18.5) 1495 (19.0) 1224 (17.9) 0.12 � Posterior circulation infarct 2488 (16.9) 1343 (17.1) 1145 (16.8) 0.67
Transient ischemic attack 1387 (6.3) 646 (5.5) 741 (7.2) <0.001
Admission NIHSS score, median (IQR)
Stroke severity on admission 5 (2–10) 5 (2–11) 4 (1–10) <0.001
Hospital facility, n (%)
Academic center 12,570 (56.9) 7131 (60.3) 5439 (53.1) <0.001Hospital with emergency department 14,677 (69.1) 8745 (78.7) 5932 (58.6) <0.001Hospital with N-ICU 16,885 (78.3) 9678 (85.6) 7207 (70.3) <0.001Hospital with stroke unit 12,189 (57.2) 7199 (64.7) 4990 (49.0) <0.001Hospital with stroke outpatient clinic 21,702 (98.3) 11,828 (100) 9874 (96.3) <0.001IQR: Interquartile range; mRS: Modified Rankin Scale; N-ICU: Neurointensive care unit; NIHSS: NIH Stroke Scale.

Clin. Pract. (2013) 10(6)706 future science group
Research Article | Ji, Wang, Liu et al.
�� GRP per capita & prehospital managementPrehospital management for ischemic stroke and hemorrhagic stroke are shown in Tables 2 & 3 and Tables 4 & 5, respectively. For ischemic stroke (AIS/TIA), patients in the developed areas were more likely to use EMS (18.0 vs 12.1%; p < 0.001) and present at hospital within 2 h from symptom onset (12.7 vs 9.9%; p < 0.001) (Table 2). After GEE adjustment, higher GRP per capita was significantly associated with bet-ter individual measures (p < 0.001) and com-posite measures of prehospital management for ischemic stroke (adjusted odds ratio [OR]: 1.03; 95% CI: 1.02–1.04; p < 0.001) (Table 3). A simi-lar association between GRP per capita and indi-vidual and composite measures of prehospital management were found for hemorrhagic stroke (SAH/ICH) (Tables 4 & 5).
�� GRP per capita & in-hospital quality of careIn-hospital quality of care for ischemic stroke and hemorrhagic stroke are shown in Tables 2 & 3 and Tables 4 & 5, respectively. For
ischemic stroke (AIS/TIA), patients in the developed areas received more evidence-based care of dysphagia screening (p < 0.001), DVT prophy laxis (p < 0.001), rehabilitation assess-ment (p < 0.001), discharge on antithrombotics (p < 0.001) and cholesterol-reducing medica-tions (p < 0.001); while patients in the under-developed areas received more evidence-based care in getting antithrombotic therapy within 48 h after hospitalization (p < 0.001), in-hos-pital stroke education (p = 0.004) and smoking cessation counseling (p = 0.002) (Table 2). The mean opportunity-based score of in-hospital quality of care was 0.62 (standard deviation: 0.25). After GEE adjustment, higher GRP per capita was significantly associated with higher opportunity-based score of in-hospital quality of care for ischemic stroke (adjusted OR: 1.02; 95% CI: 1.01–1.03; p < 0.001) (Table 3).
For hemorrhagic stroke (SAH/ICH), patients in the developed areas received more evidence-based care of DVT prophylaxis (p < 0.001) and rehabilitation assessment (p = 0.01); while patients in the underdeveloped areas received more evidence-based care in getting in-hospital
Table 2. Prehospital management, in-hospital quality of care and outcomes at discharge of ischemic stroke (acute ischemic stroke/transient ischemic attack) by macroeconomic status.
Measures of quality of care and outcome Total(n = 16,089)
Developed areas(n = 8516)
Underdeveloped areas (n = 7573)
p-value
Prehospital management, n (%)
Transportation to hospital via EMS 2453 (15.2) 1533 (18.0) 920 (12.1) <0.001Transportation to hospital within 2 h 1832 (11.4) 1082 (12.7) 750 (9.9) <0.001Opportunity-based score , mean (SD) 0.13 (0.25) 0.15 (0.27) 0.11 (0.23) <0.001
In-hospital quality of care†, n (%)
Intravenous thrombolysis with rt-PA 86 (10.8) 54 (10.8) 32 (10.8) 0.98Dysphagia screening 5555 (37.4) 3207 (41.2) 2348 (33.2) <0.001Deep vein thrombosis prophylaxis 3321 (63.2) 1923 (65.5) 1398 (60.2) <0.001Antithrombotics within 48 h after hospitalization 12,808 (82.8) 6620 (80.8) 6188 (85.1) <0.001Anticoagulation for atrial fibrillation 224 (25.5) 131 (23.9) 93 (28.1) 0.18Antithrombotics at discharge 11,060 (69.7) 5893 (70.4) 5167 (69.0) 0.05Cholesterol-reducing agents at discharge 5860 (61.0) 3181 (64.0) 2679 (57.8) <0.001Rehabilitation assessment 7393 (46.0) 4187 (49.2) 3206 (42.3) <0.001Stroke education 13,771 (85.6) 7247 (85.1) 6524 (86.1) 0.06Smoking cessation counseling 2989 (69.7) 1484 (67.3) 1505 (72.3) <0.001Opportunity-based score, mean (SD) 0.62 (0.25) 0.64 (0.26) 0.61 (0.24) <0.001
Outcomes at discharge, n (%)
mRS ≤2 at discharge 11,320 (70.4) 5914 (69.4) 5406 (71.4) 0.007In-hospital mortality 507 (3.2) 300 (3.5) 207 (2.7) 0.004In-hospital SAP 1697 (10.5) 941 (11.0) 756 (10.0) 0.03†The denominator was the total number of patients who were eligible for the specific measure and varied according to the measures.EMS: Emergency medical system; mRS: Modified Rankin Scale; rt-PA: Recombinant tissue plasminogen activator; SAP: Stroke-associated pneumonia; SD: Standard deviation.

707future science group www.futuremedicine.com
Impact of macroeconomic status on acute stroke outcome in China | Research Article
stroke education (p < 0.001) and smoking cessa-tion counseling (p = 0.001) (Table 4). After GEE adjustment, there was no significant association between macroeconomic status and opportu-nity-based score of in-hospital quality of care for hemorrhagic stroke (adjusted OR: 0.99; 95% CI: 0.98–1.01; p = 0.61) (Table 5).
�� GRP per capita & stroke outcomesThe median length of hospital stay of the over-all study population was 15 days (IQR: 10–21; ischemic stroke [AIS/TIA]: 14 [IQR: 10–20]; hemorrhagic stroke [SAH/ICH]: 18 [IQR: 11–26]). A total of 14,759 patients (66.9%) had good functional outcome (mRS ≤2) at discharge (11,320 for ischemic stroke and 3439 for hemorrhagic stroke); 1124 (5.1%) died dur-ing hospitalization (507 of ischemic stroke and 617 of hemorrhagic stroke); and 2655 (12.0%) had SAP during hospitalization (1697 for isch-emic stroke and 958 for hemorrhagic stroke). After GEE adjustment, higher GRP per capita was significantly associated with better func-tional outcome (mRS ≤2) at discharge (adjusted
OR: 1.11; 95% CI: 1.02–1.20; p < 0.001) and lower in-hospital SAP (adjusted OR: 0.88; 95% CI: 0.79–0.98; p = 0.03) after ischemic stroke (AIS/TIA) (Table 3). No significant asso-ciation was found between GRP per capita and in-hospital mortality (adjusted OR: 1.07; 95% CI: 0.87–1.31; p = 0.53). A similar asso-ciation between macroeconomic status and pri-mary and secondary outcomes was found for hemorrhagic stroke (SAH/ICH) (Table 5).
DiscussionTo the best of our knowledge, we are the first to systematically investigate the associa-tion between GRP per capita and prehospital management, in-hospital quality of care and functional outcome after acute stroke. It was found that higher GRP per capita was asso-ciated with better prehospital management, higher quality of in-hospital care and improved functional outcome at discharge after isch-emic stroke (AIS/TIA). A similar association between macroeconomic status and prehospi-tal manage ment, and functional outcome at
Table 3. Unadjusted and adjusted odds ratios for prehospital management, in-hospital quality of care and outcomes at discharge of ischemic stroke (acute ischemic stroke/transient ischemic attack) by macroeconomic status†.
Measures of quality of care and outcome Unadjusted OR (95% CI) p-value Adjusted OR‡ (95% CI) p-value
Prehospital management
Transportation to hospital by EMS (n = 16,089) 1.59 (1.45–1.73) <0.001 1.46 (1.33–1.60) <0.001Transportation to hospital within 2 h (n = 16,089) 1.32 (1.20–1.46) <0.001 1.29 (1.17–1.43) <0.001Opportunity-based score (n = 16,089) 1.04 (1.03–1.05) <0.001 1.03 (1.02–1.04) <0.001
In-hospital quality of care
Intravenous thrombolysis with rt-PA (n = 797) 1.00 (0.63–1.58) 0.99 1.09 (0.68–1.75) 0.73Dysphagia screening (n = 14,861) 1.41 (1.32–1.51) <0.001 1.37 (1.28–1.46) <0.001Deep vein thrombosis prophylaxis (n = 5258) 1.26 (1.12–1.41) <0.001 1.28 (1.14–1.44) <0.001Antithrombotics within 48 h after admission (n = 15,470) 0.73 (0.68–0.80) <0.001 0.76 (0.70–0.83) <0.001Anticoagulation for atrial fibrillation (n = 879) 0.80 (0.59–1.10) 0.17 0.86 (0.63–1.19) 0.37Antithrombotics at discharge (n = 15,860) 1.07 (1.01–1.15) 0.03 1.15 (1.08–1.24) <0.001Cholesterol-reducing agents at discharge (n = 9603) 1.30 (1.20–1.41) <0.001 1.34 (1.23–1.45) <0.001Rehabilitation assessment (n = 16,089) 1.32 (1.24–1.40) <0.001 1.28 (1.20–1.36) <0.001Stroke education (n = 16,089) 0.92 (0.84–1.00) 0.06 0.94 (0.86–1.03) 0.94Smoking cessation counseling (n = 4289) 0.79 (0.69–0.90) <0.001 0.81 (0.71–0.93) 0.002Opportunity-based score (n = 16,089) 1.02 (1.01–1.03) <0.001 1.02 (1.01–1.03) <0.001
Outcomes at discharge
mRS ≤2 at discharge (n = 16,089) 0.91 (0.85–0.98) 0.007 1.11 (1.02–1.20) <0.001In-hospital mortality (n = 16,089) 1.30 (1.09–1.56) 0.004 1.07 (0.87–1.31) 0.53In-hospital SAP (n = 16,089) 1.12 (1.01–1.24) 0.03 0.88 (0.79–0.98) 0.03†Patients in the underdeveloped areas were used as a reference. ‡The generalized estimation equation models adjusted for age, gender, education level, marital status, health insurance, stroke risk factors (hypertension, diabetes mellitus, dyslipidemia, atrial fibrillation, coronary heart disease, history of stroke/transient ischemic attack and current smoking), stroke subtypes (acute ischemic stroke and transient ischemic attack), Oxfordshire Community Stroke Project classification, admission NIH Stroke Scale score, hospital facilities (hospital grade, total number beds in the hospital, academic status and equipment within emergency department, neurointensive care unit, and stroke unit) and length of hospital stay. EMS: Emergency medical system; mRS: Modified Rankin Scale; OR: Odds ratio; rt-PA: Recombinant tissue plasminogen activator; SAP: Stroke-associated pneumonia.

Clin. Pract. (2013) 10(6)708 future science group
Research Article | Ji, Wang, Liu et al.
discharge, were found for hemorrhagic stroke (SAH/ICH). However, macroeconomic status showed less impact on in-hospital quality of care for hemorrhagic stroke.
Similar to prior studies [14], we found patients in the developed areas had older age of stroke onset. The evidence for the link between SES and stroke risk factors was not consistent for developed and developing countries. Studies in developed counties showed a higher prevalence of classic risk factors in the lower SES groups [4,23–25]; however, in developing countries, a direct relation has been observed between SES and risk factors such as high blood pressure and obesity [26]. An Indian study showed a remark-ably similar distribution of classic risk factors between the urban and rural communities [27]. Interestingly, in our study, a higher proportion of vascular risk factors was found among stroke patients in the developed areas (excepting smoking). Caution should be used when inter-preting the results. Although the information was collected by trained neurologists, we can-not rule out the potential reporting bias with under-reporting in the underdeveloped areas. Further studies on investigating the relation-ship between prevalence of classic stroke risk factors and macroeconomic status in China are needed. Additionally, we found more stroke patients in the developed areas had healthcare
insurance, especially for basic or government insurance, which is an indicator of healthcare investment by local government.
A Canadian study found a minimal effect of SES on travel patterns after stroke [28]. In our study, it was found that patients in the developed areas were more likely to use EMS and present at hospital within a shorter time in both the ischemic stroke (AIS/TIA) and hemorrhagic stroke (SAH/ICH) cohort. The prehospital delay of acute stroke in urban China had previously been investigated [29]. Generally, there is a longer prehospital delay and less use of EMS in China than that in the western coun-tries [30], and in our study, the situation was shown to be even worse in the underdeveloped areas. Due to the detrimental impact on stroke management and outcomes associated with pre-hospital delay, continuous efforts are needed to improve prehospital stroke management in China, especially for the underdeveloped areas.
The association between microindicators of SES and delivery of stroke care has been investigated and no consistent pattern has been found. Some studies suggested that socio-economic differences may exist in stroke care with patients with low SES receiving fewer rel-evant diagnostic examinations and less stroke care [6,9–11,31]. By contrast, other studies failed to verify such association [7,13,32]. In our study,
Table 4. Prehospital management, in-hospital quality of care and outcomes at discharge of hemorrhagic stroke (subarachnoid hemorrhage/intracranial hemorrhage) by macroeconomic status.
Measures of quality of care and outcome Total(n = 5988)
Developed areas (n = 3312)
Underdeveloped areas (n = 2676)
p-value
Prehospital management, n (%)
Transportation to hospital via EMS 1849 (30.9) 1105 (33.4) 744 (27.8) <0.001Transportation to hospital within 2 h 1257 (21.0) 718 (21.7) 539 (20.1) 0.15Opportunity-based score, mean (SD) 0.30 (0.30) 0.32 (0.29) 0.29 (0.31) <0.001
In-hospital quality of care†, n (%)
Dysphagia screening 1451 (31.5) 822 (31.9) 629 (31.1) 0.59Deep vein thrombosis prophylaxis 759 (62.4) 420 (67.3) 339 (57.2) <0.001Cholesterol-reducing agents at discharge 352 (100) 200 (100) 152 (100) –Rehabilitation assessment 2112 (35.3) 1214 (36.7) 898 (33.6) 0.01Stroke education 4391 (73.3) 2364 (71.4) 2027 (75.7) <0.001Smoking cessation counseling 819 (54.6) 405 (50.5) 414 (59.2) 0.001Opportunity-based score, mean (SD) 0.49 (0.33) 0.49 (0.33) 0.49 (0.32) 0.66
Outcomes at discharge, n (%)
mRS ≤2 at discharge 3439 (57.4) 1967 (59.4) 1472 (55.0) <0.001In-hospital mortality 617 (10.3) 378 (11.4) 239 (8.9) 0.002In-hospital SAP 958 (16.0) 543 (16.4) 415 (15.5) 0.36†The denominator was the total number of patients who were eligible for the specific measure and varied according to the measures. EMS: Emergency medical system; mRS: Modified Rankin Scale; SAP: Stroke-associated pneumonia; SD: Standard deviation.

709future science group www.futuremedicine.com
Impact of macroeconomic status on acute stroke outcome in China | Research Article
higher GRP per capita was shown to be associ-ated with higher quality of in-hospital care for ischemic stroke (AIS/TIA), but not for hemor-rhagic stroke (SAH/ICH) by using a composite measure score. This might be attributable to the fact that relatively less attention and effort has been paid to improve quality of care for hemorrhagic stroke as compared with isch-emic stroke. A prior study also indicated that performance-of-care measures were generally lower for ICH/SAH compared with AIS/TIA [33]. Although different indicators were used to measure in-hospital quality of care, compared with prior studies [33–35], our study suggested continuous efforts are needed to ensure optimal stroke care to both patient groups in China, especially for intravenous tissue plasminogen activator, anticoagulation for atrial fibrillation and dysphagia screening.
In China, the media, government and authorities have called the attention of the pub-lic and of clinicians to stroke. Unfortunately, based on data from the CNSR, only 2.4% of AIS patients were treated with either intrave-nous or intra-arterial thrombolysis [36]. In our opinion, potential reasons for this dismal record vary and can be classified into the following four categories:
� Prehospital delay;
� In-hospital delay;
� Lack of basic infrastructure;
� Lack of readiness of treating clinicians or patients/families for stroke thrombolysis treatment.
In the future, health and medical care promo-tion strategies to improve community awareness of stroke, expanded availability and utilization of ambulance services, implementation of stroke center certification project, creation of effec-tive clinical pathways for stroke thrombolysis, strengthening professional training on stroke thrombolysis, and establishment of telemedicine service are necessary and promising methods to expedite stroke thrombolysis in China.
Prior studies demonstrated that a higher GDP level was associated with reduced stroke mortal-ity [2,3,14,25]. In this study, we did not find a sig-nificant association between GRP per capita and in-hospital mortality. However, our study pro-vided evidence that higher GRP per capita was associated with improved functional outcome at discharge and reduced in-hospital SAP after stroke. Meanwhile, the finding was verified in both an ischemic (AIS/TIA) and hemorrhagic
Table 5. Unadjusted and adjusted odds ratios for prehospital management, in-hospital quality of care and outcomes at discharge of hemorrhagic stroke (subarachnoid hemorrhage/intracranial hemorrhage) by macroeconomic status†.
Measures of quality of care and outcome Unadjusted OR (95% CI) p-value Adjusted OR‡ (95% CI) p-value
Prehospital management
Transportation to hospital by EMS (n = 5988) 1.30 (1.16–1.45) <0.001 1.27 (1.13–1.43) <0.001Transportation to hospital within 2 h (n = 5988) 1.10 (0.97–1.24) 0.15 1.06 (1.01–1.26) 0.03Opportunity-based score (n = 5988) 1.03 (1.01–1.05) <0.001 1.02 (1.01–1.04) 0.02
In-hospital quality of care
Dysphagia screening (n = 4804) 1.04 (0.92–1.18) 0.57 1.01 (0.88–1.14) 0.93Deep vein thrombosis prophylaxis (n = 1217) 1.54 (1.22–1.95) <0.001 1.56 (1.23–1.97) <0.001Cholesterol-reducing agents at discharge (n = 352) – – – –Rehabilitation assessment (n = 5988) 1.15 (1.03–1.28) <0.001 1.15 (1.03–1.28) 0.01Stroke education (n = 5988) 0.80 (0.71–0.90) <0.001 0.80 (0.71–0.90) <0.001Smoking cessation counseling (n = 1501) 0.70 (0.57–0.86) 0.001 0.70 (0.57–0.87) 0.001Opportunity-based score (n = 5988) 1.00 (0.98–1.02) 0.66 0.99 (0.98–1.01) 0.61
Outcomes at discharge
mRS ≤2 at discharge (n = 5988) 1.20 (1.08–1.33) 0.001 1.41 (1.23–1.61) <0.001In-hospital mortality (n = 5988) 1.31 (1.11–1.56) 0.002 1.20 (0.98–1.46) 0.10In-hospital SAP (n = 5988) 1.06 (0.93–1.22) 0.35 0.93 (0.82–0.97) 0.01†Patients in the underdeveloped areas were used as a reference. ‡The generalized estimation equation models adjusted for age, gender, education level, marital status, health insurance, stroke risk factors (hypertension, diabetes mellitus, dyslipidemia, atrial fibrillation, coronary heart disease, history of stroke/transient ischemic attack and current smoking), stroke subtypes (subarachnoid hemorrhage and intracranial hemorrhage), admission NIH Stroke Scale score, hospital facilities (hospital grade, total beds in the hospital, academic status and equipment within emergency department, neurointensive care unit and stroke unit) and length of hospital stay. EMS: Emergency medical system; mRS: Modified Rankin Scale; SAP: Stroke-associated pneumonia.

Clin. Pract. (2013) 10(6)710 future science group
Research Article | Ji, Wang, Liu et al.
stroke (SAH/ICH) cohort. These benefits might be attributable to better prehospital management, in-hospital quality of care and hospital facilities in the developed areas. A positive relationship between hospital facilities, performance of care and stroke outcomes have been reported [12,37,38].
In the study, we found that the proportion of patients receiving antithrombotics within 48 h is higher than at discharge. For example, 85.1% of patients in underdeveloped areas received antithrombotics within 48 h but only 69% received them at discharge. There might be some potentials reasons:
� Antithrombotics within 48 h after onset includes the use of anticoagulation, such as low-molecular-weight heparins. After the acute phase, these medications would be stopped;
� Nonpersistence of secondary prevention medi-cations, especially in underdeveloped areas. We have carried out an ana lysis for 3-month per-sistence of five classic secondary stroke preven-tion medications, namely, antiplatelet agents, warfarin (for atrial fibrillation anticoagulation), antihypertensives, statins and diabetic agents. Finally, we found that 3-month persistence was highest for diabetic medications (82.7%), fol-lowed by antiplatelet agents (80.4%) and anti-hypertensives (79.2%). Three-month persis-tence was lowest for warfarin (31.7%) and statins (62.3%) [39];
� Side effects or hemorrhagic complications that prevent the persistent use of antiplatelet agents.
The strengths of the study include a relatively large sample size, complete patient-level informa-tion (prehospital management, in-hospital qual-ity of care and functional outcome at discharge) and verification of findings in both the ischemic (AIS/TIA) and hemorrhagic stroke (SAH/ICH) cohort. Our study has some limitations. First, like most registries, our registry required informed consent and selection bias was inevitable [40]. Patients who died before administration might not be included. Second, we used only one indi-cator of macroeconomic status (GRP per capita). Further studies on investigating the potential relationship between other indicators, such as gross national product per capita, total health expenditure per capita and unemployment rate, and quality of stroke care and outcomes are needed. Third, the effect of macroeconomic sta-tus on stroke care and outcomes may lag behind
the economic growth itself. It is unclear whether the time-span is long enough for the effect of economic status on stroke to fully take place. Finally, the baseline characteristics of our study were different from those of western countries, such as a younger age of onset, predominance of male gender, lower severity of neurological deficit. It is difficult to explain the reasons due to many differences in study design and population. In the future, if we can do a face-to-face comparison, maybe we can find more clues to interpret this phenomenon.
ConclusionWe systematically investigated the association between macroeconomic status (GRP per cap-ita) and prehospital management, in-hospital quality of care and stroke outcomes at dis-charge. Higher GRP per capita was found to be associated with better prehospital manage-ment, higher quality of in-hospital care and improved functional outcome at discharge after ischemic stroke (AIS/TIA). A similar associa-tion between macroeconomic status and pre-hospital management and functional outcome at discharge were found for hemorrhagic stroke (SAH/ICH). However, macroeconomic status showed less impact on in-hospital quality of care for hemorrhagic stroke.
Future perspectiveOur study should encourage studies to pay more attention to the potential impact of macro-economic status on quality of stroke care and stroke outcome. The findings might be helpful for the Chinese government to develop strategies and reallocate resources to improve stroke pre-vention and management throughout the coun-try. Future studies may consider determining the financial impact of having worse outcomes in less developed areas.
Financial & competing interests disclosureThe China National Stroke Registry is funded by the Ministry of Science and Technology (2006BA101A11) and the Ministry of Health of the People’s Republic of China (2009CB521905). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.

711future science group www.futuremedicine.com
Impact of macroeconomic status on acute stroke outcome in China | Research Article
Ethical conduct of research The authors state that they have obtained appropriate insti tutional review board approval or have followed the princi ples outlined in the Declaration of Helsinki for all
human or animal experimental investigations. In addi-tion, for investi gations involving human subjects, informed consent has been obtained from the participants involved.
References1 Kim AS, Johnston SC. Global variation in the
relative burden of stroke and ischemic heart disease. Circulation 124(3), 314–323 (2011).
2 Cox AM, McKevitt C, Rudd AG, Wolfe CD. Socioeconomic status and stroke. Lancet Neurol. 5(2), 181–188 (2006).
3 Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 8(4), 355–369 (2009).
4 Cesaroni G, Agabiti N, Forastiere F, Perucci CA. Socioeconomic differences in stroke incidence and prognosis under a universal healthcare system. Stroke 40(8), 2812–2819 (2009).
5 Daly MC, Duncan GJ, McDonough P, Williams DR. Optimal indicators of socioeconomic status for health research. Am. J. Public Health 92(7), 1151–1157 (2002).
6 Langagergaard V, Palnum KH, Mehnert F et al. Socioeconomic differences in quality of care and clinical outcome after stroke: a nationwide population-based study. Stroke 42(10), 2896–2902 (2011).
7 McKevitt C, Coshall C, Tilling K, Wolfe C. Are there inequalities in the provision of stroke care? Analysis of an inner-city stroke register. Stroke 36(2), 315–320 (2005).
8 Allin S, Masseria C, Mossialos E. Measuring socioeconomic differences in use of health care services by wealth versus by income. Am. J. Public Health 99(10), 1849–1855 (2009).
9 Weir NU, Gunkel A, McDowall M, Dennis MS. Study of the relationship between social deprivation and outcome after stroke. Stroke 36(4), 815–819 (2005).
10 Jakovljevic D, Sarti C, Sivenius J et al. Socioeconomic status and ischemic stroke: The FINMONICA Stroke Register. Stroke 32(7), 1492–1498 (2001).
11 Kapral MK, Wang H, Mamdani M, Tu JV. Effect of socioeconomic status on treatment and mortality after stroke. Stroke 33(1), 268–273 (2002).
12 Saposnik G, Jeerakathil T, Selchen D, Baibergenova A, Hachinski V, Kapral MK. Socioeconomic status, hospital volume, and stroke fatality in Canada. Stroke 39(12), 3360–3366 (2008).
13 Lofmark U, Hammarstrom A. Education-related differences in case fatality among elderly with stroke. Neuroepidemiology 31(1), 21–27 (2008).
14 Sposato LA, Saposnik G. Gross domestic product and health expenditure associated with incidence, 30-day fatality, and age at stroke onset: a systematic review. Stroke 43(1), 170–177 (2012).
15 Strong K, Mathers C, Bonita R. Preventing stroke: saving lives around the world. Lancet Neurol. 6(2), 182–187 (2007).
16 Wang Y, Cui L, Ji X et al. The China National Stroke Registry for patients with acute cerebrovascular events: design, rationale, and baseline patient characteristics. Int. J. Stroke 6(4), 355–361 (2011).
17 Stroke – 1989. Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on stroke and other cerebrovascular disorders. Stroke 20(10), 1407–1431 (1989).
18 Reeves MJ, Parker C, Fonarow GC, Smith EE, Schwamm LH. Development of stroke performance measures: definitions, methods, and current measures. Stroke 41(7), 1573–1578 (2010).
19 Executive summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 285(19), 2486–2497 (2001).
20 Peterson ED, Delong ER, Masoudi FA et al. ACCF/AHA 2010 Position Statement on Composite Measures for Healthcare Performance Assessment: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures (Writing Committee to develop a position statement on composite measures). Circulation 121(15), 1780–1791 (2010).
21 Davenport RJ, Dennis MS, Wellwood I, Warlow CP. Complications after acute stroke. Stroke 27(3), 415–420 (1996).
22 Zeger SL, Liang KY. Longitudinal data ana-lysis for discrete and continuous outcomes. Biometrics 42(1), 121–130 (1986).
23 Kuper H, Adami HO, Theorell T, Weiderpass E. The socioeconomic gradient in the incidence of stroke: a prospective study in
middle-aged women in Sweden. Stroke 38(1), 27–33 (2007).
24 Grimaud O, Dufouil C, Alperovitch A et al. Incidence of ischaemic stroke according to income level among older people: the 3C study. Age Ageing 40(1), 116–121 (2011).
25 Addo J, Ayerbe L, Mohan KM et al. Socioeconomic status and stroke: an updated review. Stroke 43(4), 1186–1191 (2012).
26 Colhoun HM, Hemingway H, Poulter NR. Socio-economic status and blood pressure: an overview ana lysis. J. Hum. Hypertens. 12(2), 91–110 (1998).
27 Sridharan SE, Unnikrishnan JP, Sukumaran S et al. Incidence, types, risk factors, and outcome of stroke in a developing country: the Trivandrum Stroke Registry. Stroke 40(4), 1212–1218 (2009).
28 Ahuja C, Mamdani M, Saposnik G. Influence of socioeconomic status on distance traveled and care after stroke. Stroke 43(1), 233–235 (2012).
29 Jin H, Zhu S, Wei JW et al. Factors associated with prehospital delays in the presentation of acute stroke in urban China. Stroke 43(2), 362–370 (2012).
30 Evenson KR, Foraker RE, Morris DL, Rosamond WD. A comprehensive review of prehospital and in-hospital delay times in acute stroke care. Int. J. Stroke 4(3), 187–199 (2009).
31 Lazzarino AI, Palmer W, Bottle A, Aylin P. Inequalities in stroke patients’ management in English public hospitals: a survey on 200,000 patients. PLoS ONE 6(3), e17219 (2011).
32 Kerr GD, Higgins P, Walters M et al. Socioeconomic status and transient ischaemic attack/stroke: a prospective observational study. Cerebrovasc. Dis. 31(2), 130–137 (2011).
33 Smith EE, Liang L, Hernandez A et al. Influence of stroke subtype on quality of care in the Get With The Guidelines-Stroke Program. Neurology 73(9), 709–716 (2009).
34 Schwamm LH, Fonarow GC, Reeves MJ et al. Get With the Guidelines – stroke is associated with sustained improvement in care for patients hospitalized with acute stroke or transient ischemic attack. Circulation 119(1), 107–115 (2009).

Clin. Pract. (2013) 10(6)712 future science group
Research Article | Ji, Wang, Liu et al.
35 Reeves MJ, Fonarow GC, Zhao X, Smith EE, Schwamm LH. Quality of care in women with ischemic stroke in the GWTG program. Stroke 40(4), 1127–1133 (2009).
36 Wang Y, Liao X, Zhao X et al. Using recombinant tissue plasminogen activator to treat acute ischemic stroke in China: ana lysis of the results from the Chinese National Stroke Registry (CNSR). Stroke 42(6), 1658–1664 (2011).
37 Abilleira S, Ribera A, Permanyer-Miralda G, Tresserras R, Gallofre M. Noncompliance with certain quality indicators is associated with risk-adjusted mortality after stroke. Stroke 43(4), 1094–1100 (2012).
38 Ryan AM, Doran T. The effect of improving processes of care on patient outcomes: evidence from the United Kingdom’s quality and outcomes framework. Med. Care 50(3), 191–199 (2012).
39 Ji R, Liu G, Shen H et al. Persistence of secondary prevention medications after acute ischemic stroke or transient ischemic attack in Chinese population: data from China National Stroke Registry. Neurol. Res. 35(1), 29–36 (2013).
40 Tu JV, Willison DJ, Silver FL et al. Impracticability of informed consent in the Registry of the Canadian Stroke Network. N. Engl. J. Med. 350(14), 1414–1421 (2004).