
Impact of Health Sector Reforms on Utilization of Health ......
15
International Journal of Research in Social Sciences Vol. 8 Issue 1, January 2018, ISSN: 2249-2496 Impact Factor: 7.081 Journal Homepage: http://www.ijmra.us , Email: [email protected] Double-Blind Peer Reviewed Refereed Open Access International Journal - Included in the International Serial Directories Indexed & Listed at: Ulrich's Periodicals Directory ©, U.S.A., Open J-Gage as well as in Cabell’s Directories of Publishing Opportunities, U.S.A 819 International Journal of Research in Social Sciences http://www.ijmra.us , Email: [email protected] Impact of Health Sector Reforms on Utilization of Health Care Services in Rural Assam (India) Dr. Nirmala Devi * Abstract Objective: To analysis the impact of health reforms on the pattern of utilization of health care services and to identify the factors affecting choice of health care facilities based on a cross section study in rural Assam. Methods: In this paper an attempt has been made to present some preliminary results of the significant changes that occurred during 1887-88, 1995-96 and 2004. The study has used the published reports of 42 nd (1887-88), 52 nd (1995-96) and 60 th (2004) round of National Sample Survey Organization (NSSO). To identify the factors affecting accessibility to public health care facilities the study relied upon a household survey conducted in Nagaon and Nalbari district of Assam during 2014-15. A binary logistic regression model has been used to identify the factors affecting accessibility to public health care facilities. Results: The analysis imply that the dependence and utilization of public health care facilities for outpatient care has declined drastically in Assam since the period from 1987-88 to 2004. In case * Assistant Professor of Economics, Arya Vidyapeeth College, Guwahati, Assam, M.A, B.Ed, M. Phil, Ph.D
Transcript of Impact of Health Sector Reforms on Utilization of Health ......
International Journal of Research in Social Sciences Vol. 8 Issue 1, January 2018, ISSN: 2249-2496 Impact Factor: 7.081
Journal Homepage: http://www.ijmra.us, Email: [email protected]
Double-Blind Peer Reviewed Refereed Open Access International Journal - Included in the International Serial
Directories Indexed & Listed at: Ulrich's Periodicals Directory ©, U.S.A., Open J-Gage as well as in Cabell’s
Directories of Publishing Opportunities, U.S.A
819 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
Impact of Health Sector Reforms on
Utilization of Health Care Services in Rural
Assam (India)
Dr. Nirmala Devi*
Abstract
Objective:
To analysis the impact of health reforms on the pattern of utilization of health care services and
to identify the factors affecting choice of health care facilities based on a cross section study in
rural Assam.
Methods:
In this paper an attempt has been made to present some preliminary results of the significant
changes that occurred during 1887-88, 1995-96 and 2004. The study has used the published
reports of 42nd
(1887-88), 52nd
(1995-96) and 60th
(2004) round of National Sample Survey
Organization (NSSO). To identify the factors affecting accessibility to public health care
facilities the study relied upon a household survey conducted in Nagaon and Nalbari district of
Assam during 2014-15. A binary logistic regression model has been used to identify the factors
affecting accessibility to public health care facilities.
Results:
The analysis imply that the dependence and utilization of public health care facilities for
outpatient care has declined drastically in Assam since the period from 1987-88 to 2004. In case
* Assistant Professor of Economics, Arya Vidyapeeth College, Guwahati, Assam, M.A,
B.Ed, M. Phil, Ph.D

ISSN: 2249-2496 Impact Factor: 7.081
820 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
of inpatient care the dependence is very high on public health facilities but the rate of utilization
has declined since the inception of health reform measures. Results of the binary logistic
regression model indicate that the non-poor, highly educated people have greater likelihood of
using private health facilities than their counterparts.
Conclusions:
The state requires greater public investment for improving the quality of care in the government
health facilities. Moreover, there is a need to regulate the private health care market as majority
of the rural population depends on public hospitals for treatment.
Keywords: Choice of health care, rural health, utilization of health care services, health sector
reforms, inpatient care, outpatient
1. Background
India has made a number of policy changes in the health sector since the inception of economic
reform measures in 1991. There has been a decline in the role of state since the period from
1980s‟ but a significant change was noticed only after 1991. The health sector reforms have
resulted in significant changes in the overall health care delivery system together with changes in
the health care financing scenario of India. In order to resolve the problem of inefficiencies in
public healthcare system, reforms were carried out either by pushing for privatization or
operating in public private partnership mode. Public private partnership (PPP) has been called
upon to improve equity, efficiency, accountability, quality and accessibility of the entire health
system (Bhatt, 2000; Sen et al., 2004). Opening up of the health sector to insurance is another
form of privatization that has been openly embraced in the post reforms period (see Ahuja, 2004;
Acharya and Ranson, 2005; Mudgal et al., 2005; Hasio, 2013; Selvaraj and Karan, 2012; Fan et
al., 2012; Desai, 2009, Rao, 2004; Ellis et al., 2000). The need for a more broad based medical
insurance coverage has been initiated with the aim of absorbing the financial shocks caused by
lump-sum expenditure on medical treatment (Rao, 2004; Ahuja 2004). However reforms seem to
have had a severe impact on India‟s health scenario. Reforms introduced user fees, provision of
clinical and ancillary services to the private sector and public private partnership (Duggal, 2005,
cited in Baru et al., 2010). The policy of levying user fees had a negative impact on the poor and
ISSN: 2249-2496 Impact Factor: 7.081
821 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
marginalized communities (Ghosh, 2008; Baru et. al., 2010). The growth oriented structural
adjustment programme supported a perfectly competitive market set-up. But this model did not
fit the medical care sector in India because the ordinary people in need of medical care need it
immediately and have no time to gather information about these services through repeated
transactions (Guhan, 1995).
The case for Assam
A study of the macroeconomic conditions and health policy reforms on public expenditure on
health among the Indian states reveals that during the period between 1987 to 1992 growth rates
in public expenditure was negative for all the states including Assam. In the 2nd
phase (1993-
1998), the introduction of the structural adjustment programme has adverse impact on the health
sector of most of the states. During this period the growth rate in per capita health expenditure
was negative in some of the states like Assam and Uttar Pradesh which was mainly due to
financial stress in these states, resulting in cut in expenditure on health (Hooda, 2013). There was
a reduction in the central transfer of funds to almost all states so as to contain the fiscal deficit.
This resulted in reduction in the resource pool of the state governments because of which the
state governments were forced to cut down their budgetary allocation on different sectors
specifically the health sector (Selvaraju and Annigeri, 2001, Tulasidhar, 1993, Ghuman et al.
2009, Choudhury and Nath, 2012). Sarma (2004) in a study related to health expenditure in
Assam has noted that in times of fiscal hardship public expenditure has been squeezed more in
the health sector than in any other sector. In the above context the paper analysis the impact of
economic reforms on
a. the pattern of utilization of health care services and
b. identifies the factors affecting choice of health care facilities based on a cross section study in
Assam.
2. Methods
In this paper an attempt has been made to present some preliminary results of the significant
changes that occurred during 1887-88 (42nd
round), 1995-96 (52nd
round) and 2004 (60th
round),
based on data National Sample Survey Organization (NSSO) data. The paper also provides

ISSN: 2249-2496 Impact Factor: 7.081
822 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
evidences from a cross-section study in two districts of Assam namely Nagaon and Nalbari
during 2014-15. The village level data is used to identify the factors affecting accessibility to
public health care providers. The two districts are selected on the basis of ranking of districts
based on selected socio-economic indicators of health. Further a review of literature was done to
identify the forward and backward development blocks from Nalbari and Nagaon. Subsequently,
Kaliabor Development Block was selected from Nagaon district and Barbhag Development
Block was selected from Nalbari district. Later, from the list of revenue villages, Bamuni Pathar
from Kaliabor Development Block and Balagaon from Barbhag Development Block were
randomly selected for the study. A census enumeration of the village showed a total of 247
households and 278 households in Bamunipathar and Balagaon The study collected information
from 40 per cent of the households from both the villages i.e. 99 households from Bamunipathar
and 111 households from Balagaon1. However, for identifying the factors affecting choice of
health care providers whether public or private, the collection of data is restricted to only those
who have sought care in health facilities (either government or private) thus excluding treatment
through home remedial measures, self-prescribed medicines or traditional healers. The total
number of such respondent from both the villages constituted of 402 respondents. A binary
logistic regression model has been used to identify the various factors affecting choice of health
care facilities.
3. Changes in the pattern of utilization of health care services in Assam: An analysis
based on National Sample Survey Organization (NSSO)
The NSSO collected data on utilization of health care services from both public and private
health care providers. Based on the reports, the public health care providers include government
hospitals, government clinics, government dispensaries, primary health centres (PHCs) and the
community health centres (CHCs), state and central government assisted ESI hospitals and
dispensaries. The „private‟ sources on the other hand include private doctors, nursing homes,
private hospitals, charitable institutions etc.
3.1 Utilization of health care services for non-hospitalized treatment among the rural population
of Assam:
1 The study is a part of Ph.D. research and the sample that has been taken is a part of the total sample of the study.
ISSN: 2249-2496 Impact Factor: 7.081
823 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
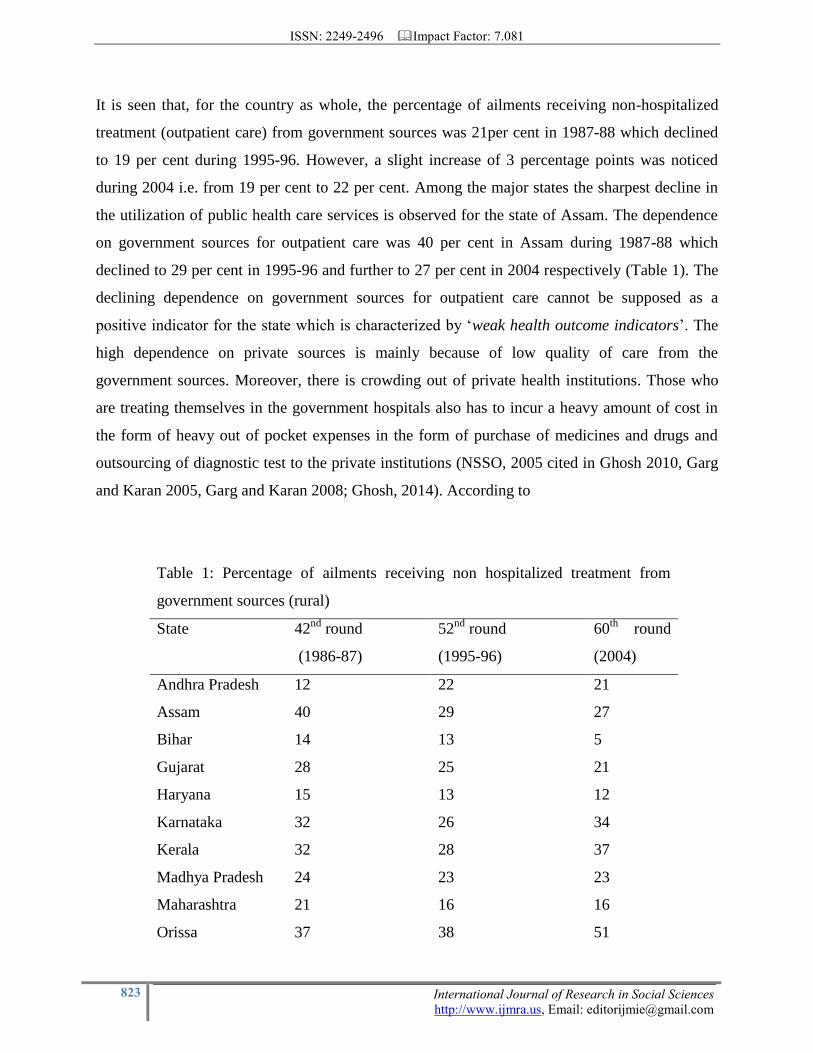
It is seen that, for the country as whole, the percentage of ailments receiving non-hospitalized
treatment (outpatient care) from government sources was 21per cent in 1987-88 which declined
to 19 per cent during 1995-96. However, a slight increase of 3 percentage points was noticed
during 2004 i.e. from 19 per cent to 22 per cent. Among the major states the sharpest decline in
the utilization of public health care services is observed for the state of Assam. The dependence
on government sources for outpatient care was 40 per cent in Assam during 1987-88 which
declined to 29 per cent in 1995-96 and further to 27 per cent in 2004 respectively (Table 1). The
declining dependence on government sources for outpatient care cannot be supposed as a
positive indicator for the state which is characterized by „weak health outcome indicators‟. The
high dependence on private sources is mainly because of low quality of care from the
government sources. Moreover, there is crowding out of private health institutions. Those who
are treating themselves in the government hospitals also has to incur a heavy amount of cost in
the form of heavy out of pocket expenses in the form of purchase of medicines and drugs and
outsourcing of diagnostic test to the private institutions (NSSO, 2005 cited in Ghosh 2010, Garg
and Karan 2005, Garg and Karan 2008; Ghosh, 2014). According to
Table 1: Percentage of ailments receiving non hospitalized treatment from
government sources (rural)
State 42nd
round
(1986-87)
52nd
round
(1995-96)
60th
round
(2004)
Andhra Pradesh 12 22 21
Assam 40 29 27
Bihar 14 13 5
Gujarat 28 25 21
Haryana 15 13 12
Karnataka 32 26 34
Kerala 32 28 37
Madhya Pradesh 24 23 23
Maharashtra 21 16 16
Orissa 37 38 51

ISSN: 2249-2496 Impact Factor: 7.081
824 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
Punjab 12 7 16
Rajasthan 46 36 44
Tamil Nadu 28 25 29
Uttar Pradesh * 8 10
West Bengal 16 15 19
India average 21 19 22
Source: NSSO 42nd
round, 52nd
round and 60th
round
*estimated are not available
Table 2: Percentage of ailments receiving hospitalized treatments from
government sources (rural)
State 42nd
round
(1986-87)
52nd
round
(1995-96)
60th
round
(2004)
Andhra Pradesh 29 23 27
Assam 83 74 74
Bihar 47 25 14
Gujarat 49 32 31
Haryana 51 31 21
Karnataka 55 46 40
Kerala 41 40 36
Madhya Pradesh 73 53 59
Maharashtra 40 31 29
Orissa 80 91 79
Punjab 45 40 29
Rajasthan 77 65 52
Tamil Nadu 55 41 41
Uttar Pradesh 52 47 27
West Bengal 76 82 79
India average 57 45 35
Source: NSSO 42nd
round, 52nd
round and 60th
round

ISSN: 2249-2496 Impact Factor: 7.081
825 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
Ghosh (2010), the lesser developed states like Orissa, Bihar, Uttar Pradesh and Assam spend
higher proportion of total health expenditure on purchase of drugs (79 per cent to 80 per cent). It
has been observed that the poorer wealth quintile is spending a larger amount on purchase of
drugs and medicines in comparison to the rich which shows a greater burden on the lower
income strata.
3.2 Utilization of health care services for non-hospitalized treatment among the rural
population of Assam:
The share of population depending on government health facilities for non-hospitalized treatment
was 83 per cent in 1987-88 in Assam. The percentage declined to 74 per cent in 1995-96 and it
remained constant for 2004 (74 per cent) (Table 2). Although the dependence on government
health facilities is very high for hospitalization cases but the rate of utilization has declined in
Assam. The dependence is high because of low cost in government hospitals as compared to the
private hospitals. For the state as a whole the percentage was 57 per cent, 45 per cent and 35 per
cent during 1987-88, 1995-96 and 2004 respectively. This shows that there is a significant
decline in the dependence on public health facilities for inpatient care for the state as a whole
after initiation of health reform measures in India.
The cost of inpatient and outpatient care has increased over the years in both government and
private health facilities, the increase being higher in private health sector. The dependence on
private sector for hospitalization cases has been increasing in the rural areas as well. Cost of care
on health also increased after privatization of 1990‟s. In comparison to the mid 1980‟s, the
average cost on both inpatient cares increased in India. Based upon the NSSO 42nd
, 52nd
and 60th
round results, Mukherjee and Levesque (2010) show that in India access of the poor to
government medical facilities are declining, with simultaneous increases in costs of inpatient
care. They also argue that the average costs of inpatient care in government hospitals has
increased across states in India, so much so that it has exceeded the prices of essential food items
resulting in net welfare losses to the poor. In other words, accessibility of government health
facilities has also become difficult due to higher charges. There was also a fall in public sector
utilization of healthcare facilities in poorer states such as Assam, Orissa and Madhya Pradesh
(ibid, 2010).

ISSN: 2249-2496 Impact Factor: 7.081
826 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
Moreover higher dependence on private health facilities for both outpatient and inpatient care
has resulted in increase in the catastrophic health expenditure among the poor and rural
population. The rich benefit from having access to both better quality health services in the
private sector, and to subsidized services from the government sector. The poorer sections are
heavily taxed on account of low quality of public healthcare as well as non-affordability of
private healthcare services (Kumar and Prakash, 2011). A large numbers of households are also
pushed below poverty line because of catastrophic OOP payments. Ghosh (2010) estimates show
that in India OOP payment has resulted in increase in the poverty headcount by 4 percent in
1993-94 to 4.4 percent in 2004-05. In order to protect the households from financial catastrophe
the scheme of health insurance was initiated which is another form of privatization that has been
openly embraced in the post reforms period. However, evidences shows that the health insurance
schemes have been successful in some the specific stares only (see Ahuja, 2004; Acharya and
Ranson, 2005; Mudgal et al., 2005; Hasio, 2013; Selvaraj and Karan, 2012; Fan et al., 2012;
Desai, 2009, Rao, 2004; Ellis et al., 2000).
4. Choice of healthcare facility (a pooled regression analysis) based on cross section
data
In order to statistically test the choice of healthcare facility among residents in the study areas, a
pooled logistic regression analysis was carried out.2 The analysis is restricted to only those who
have sought care in health facilities (either government of private) thus excluding treatment
through home remedial measures, self-prescribed medicines or traditional healers. The dependent
variable in this model is “whether the resident visited a government or private health facility” if
yes the variable will take value 1, or 0 otherwise. For the model fit we have considered nine
variables keeping in mind the composition of households and data gathered during the household
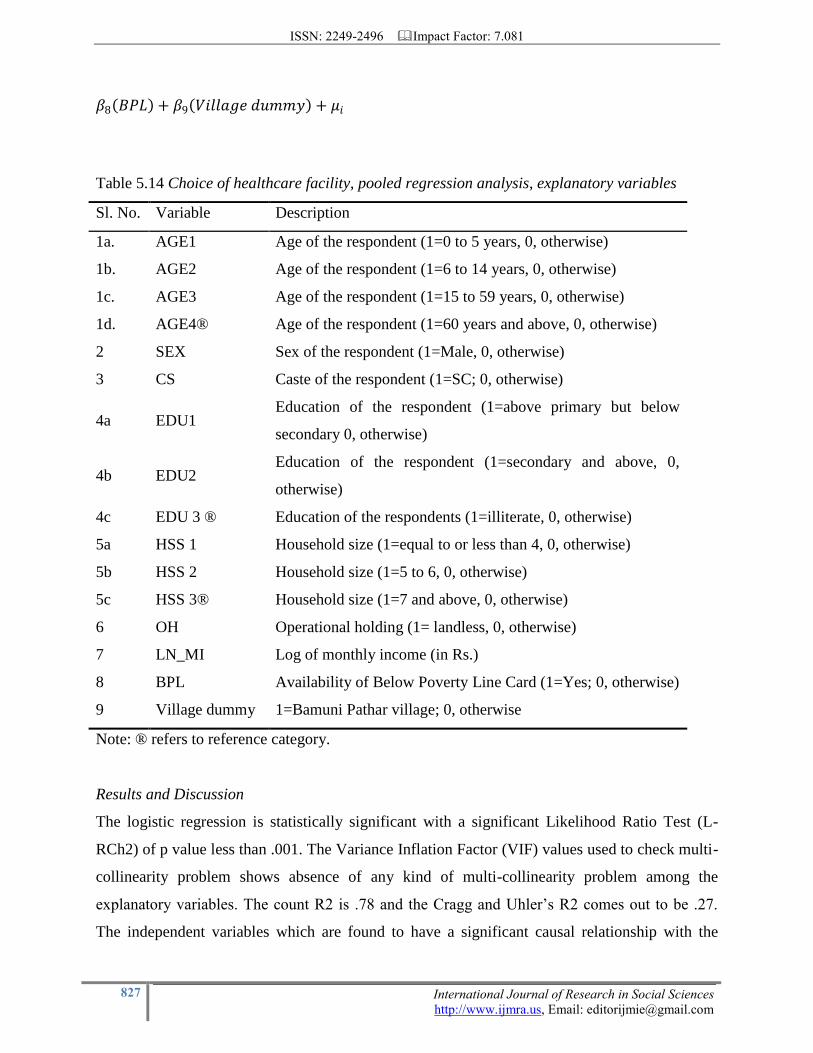
survey. The explanatory variables used in the model are described in Table 5.14. The functional
form of the logistic regression model is:
𝑍𝑖 =∝ +𝛽1 𝐴𝐺𝐸 + 𝛽2 𝑆𝐸𝑋 + 𝛽3 𝐶𝑆 + 𝛽4 𝐸𝐷𝑈 + 𝛽5 𝐻𝑆𝑆 + 𝛽6 𝑂𝐻 + 𝛽7 𝐿𝑁_𝑀𝐼 +
2 Separate regression has not been carried out for both the villages because the dependence on private health facility is
very low in Bamuni Pahtar village (8 percent). This will not represent the appropriate picture and the logistic regression will not be representative.
ISSN: 2249-2496 Impact Factor: 7.081
827 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
𝛽8 𝐵𝑃𝐿 + 𝛽9 𝑉𝑖𝑙𝑙𝑎𝑔𝑒 𝑑𝑢𝑚𝑚𝑦 + 𝜇𝑖
Results and Discussion
The logistic regression is statistically significant with a significant Likelihood Ratio Test (L-
RCh2) of p value less than .001. The Variance Inflation Factor (VIF) values used to check multi-
collinearity problem shows absence of any kind of multi-collinearity problem among the
explanatory variables. The count R2 is .78 and the Cragg and Uhler‟s R2 comes out to be .27.
The independent variables which are found to have a significant causal relationship with the
Table 5.14 Choice of healthcare facility, pooled regression analysis, explanatory variables
Sl. No. Variable Description
1a. AGE1 Age of the respondent (1=0 to 5 years, 0, otherwise)
1b. AGE2 Age of the respondent (1=6 to 14 years, 0, otherwise)
1c. AGE3 Age of the respondent (1=15 to 59 years, 0, otherwise)
1d. AGE4® Age of the respondent (1=60 years and above, 0, otherwise)
2 SEX Sex of the respondent (1=Male, 0, otherwise)
3 CS Caste of the respondent (1=SC; 0, otherwise)
4a EDU1 Education of the respondent (1=above primary but below
secondary 0, otherwise)
4b EDU2 Education of the respondent (1=secondary and above, 0,
otherwise)
4c EDU 3 ® Education of the respondents (1=illiterate, 0, otherwise)
5a HSS 1 Household size (1=equal to or less than 4, 0, otherwise)
5b HSS 2 Household size (1=5 to 6, 0, otherwise)
5c HSS 3® Household size (1=7 and above, 0, otherwise)
6 OH Operational holding (1= landless, 0, otherwise)
7 LN_MI Log of monthly income (in Rs.)
8 BPL Availability of Below Poverty Line Card (1=Yes; 0, otherwise)
9 Village dummy 1=Bamuni Pathar village; 0, otherwise
Note: ® refers to reference category.
ISSN: 2249-2496 Impact Factor: 7.081
828 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
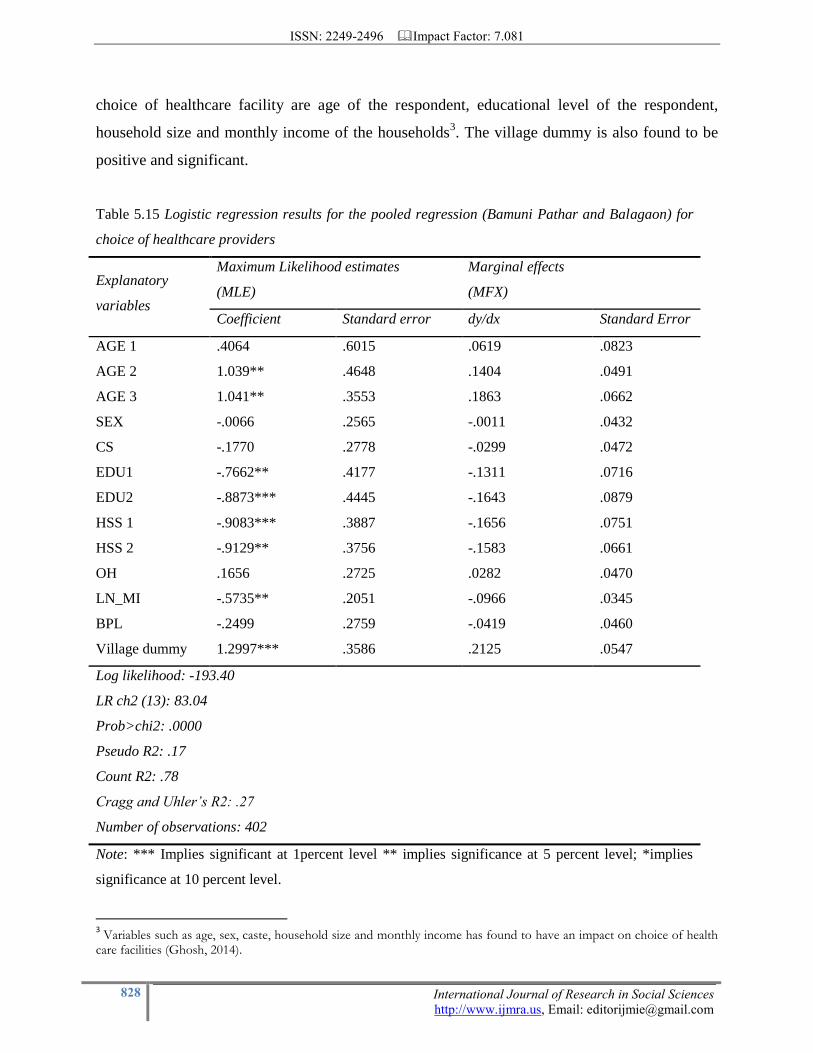
choice of healthcare facility are age of the respondent, educational level of the respondent,
household size and monthly income of the households3. The village dummy is also found to be
positive and significant.
Table 5.15 Logistic regression results for the pooled regression (Bamuni Pathar and Balagaon) for
choice of healthcare providers
Explanatory
variables
Maximum Likelihood estimates
(MLE)
Marginal effects
(MFX)
Coefficient Standard error dy/dx Standard Error
AGE 1 .4064 .6015 .0619 .0823
AGE 2 1.039** .4648 .1404 .0491
AGE 3 1.041** .3553 .1863 .0662
SEX -.0066 .2565 -.0011 .0432
CS -.1770 .2778 -.0299 .0472
EDU1 -.7662** .4177 -.1311 .0716
EDU2 -.8873*** .4445 -.1643 .0879
HSS 1 -.9083*** .3887 -.1656 .0751
HSS 2 -.9129** .3756 -.1583 .0661
OH .1656 .2725 .0282 .0470
LN_MI -.5735** .2051 -.0966 .0345
BPL -.2499 .2759 -.0419 .0460
Village dummy 1.2997*** .3586 .2125 .0547
Log likelihood: -193.40
LR ch2 (13): 83.04
Prob>chi2: .0000
Pseudo R2: .17
Count R2: .78
Cragg and Uhler’s R2: .27
Number of observations: 402
Note: *** Implies significant at 1percent level ** implies significance at 5 percent level; *implies
significance at 10 percent level.
3 Variables such as age, sex, caste, household size and monthly income has found to have an impact on choice of health
care facilities (Ghosh, 2014).

ISSN: 2249-2496 Impact Factor: 7.081
829 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
The analysis shows a significant effect of age on choice of healthcare facility. β2 co-efficient
(AGE) is found to have a positive and significant relationship with choice of healthcare facility.
The result shows that there is a positive and significant relationship between the respondents
with 0 to14 years of age and 16 to 59 years of age. This implies that the probability of use of
government healthcare facility is higher among these age groups compared to the elders above
60 years of age. In case of elders it is observed that most of the residents are suffering from
chronic diseases and therefore had to visit private hospital as the required healthcare facilities are
not available in the nearby government health facilities. The partial probability of the variables
implies that if the age of the respondent is 0-14 years and 16-59 years the probability of visiting a
government health facility increases by .14 and .18 points other things remaining the same. The
β4 co-efficient (EDU) indicates that there is a negative and significant relationship between
educational level and choice of healthcare facility. This implies that higher the educational level
of the respondent lower is the probability of visiting a government health facility for treatment.
The education variable indicates that the choice for a government healthcare facility is lower for
those who have educational level higher than primary level and above secondary in comparison
to those who are illiterate. The partial probability of the variables indicate that if the resident has
educational level higher than primary or secondary, the probability of using government health
facility decreases by .13 and .16 points, other things remaining the same. The β5 co-efficient
(HSS) has a statistically significant and negative relationship with visit to a government health
facility. It implies that those households having household members equal to 4 or 5-6 have
higher probability of visiting a private health care facility compared to households with more
than 7 members. The partial probability of the variables indicates that the probability of visiting a
government health facility decreases by .16 points and .15 points if the household has 4 or 5 to 6
member. β7 coefficient (LN_MI) has a significant and negative relationship with choice of
healthcare facility. Higher the monthly income of the household, lower is the probability of visit
to a government health facility. Respondents with higher income generally visit private
healthcare facilities because they can afford treatment in the private healthcare facilities which is
not true in case of the lower income strata. The partial probability of the variable implies that
with increase in income the probability of the household visiting a government health facility
decreases by .96 points. The β9 co-efficient (village dummy) is found to have a statistically
significant and positive relationship with choice of a healthcare facility. It implies that the

ISSN: 2249-2496 Impact Factor: 7.081
830 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
residents of Bamuni Pathar village have a higher probability of visiting a government healthcare
facility in comparison to the resident of Balagaon which has been already been discussed in the
early part of this section.
5. Results:
The analysis imply that the utilization of public health care services for outpatient care has
declined drastically in Assam since the period from 1987-88 to 2004. The decline in the rate of
utilization of government health facilities is mainly due to low quality of care in the government
hospitals. However, the gradient is not so sharp in case of inpatient care. In case of inpatient care
the dependence on government health facilities is very high but the rate of utilization has
declined after the initiation of the economic reform measures. The decline in utilization of
government health facilities on one hand and increase in utilization of private health facilities on
the other hand has resulted in catastrophic health expenses mainly among the poor section of
population. A high proportion of catastrophic health expenses have also resulted in increase in
the proportion of population below the poverty line. The rural poor are deprived of quality care
in the government hospitals and are compelled to visit the private hospitals although unwillingly.
Lack of financial protection in the form of health insurance further deteriorates the situation. The
results of the binary logistic regression model indicate that the non-poor, highly educated people
have greater likelihood of using private health facilities than their counterparts.
To improve the situation the state requires greater public investment for improving the quality of
care in the government health facilities. Moreover, there is a need to regulate the private health
care market as majority of the rural population depends on public hospitals for treatment. The
government should also focus on providing proper financial risk protection measures with
viability.
References:
1. Achraya, A. and Ranson M. K., „Healthcare Financing for the Poor: Community Based
Health Insurance Schemes in Gujarat, Economic and Political Weekly, vol. 40, no. 38, 2005, pp.
4141-4150.

ISSN: 2249-2496 Impact Factor: 7.081
831 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
2. Ahuja, R., „Health Insurance for the Poor‟, Economic and Political Weekly, vol. 39. no.
28, 2004, pp. 3171-3178.
3. Baru, R., Acharya, A., Acharya, S., Kumar, S. A., and Nagaraja, K., „Inequities in Access
to Health Care Services in India:Caste, Class and Religion‟, Economic and Political Weekly,
2010, vol. 45, no. 38, pp. 49-58
4. Barua, J., „On Identification of Backward Blocks‟, Research Paper Series (04), Omeo
Kumar Institute of Social Change and Development (OKDISCD), Guwahati, 2012.
5. Choudhury, M., Nath, H.K.A. and Dutta, P. H., „Health Expenditure by Central
Government in India: State level Distributions‟, National Institute of Public Finance and Policy,
2011.
6. Desai, S., „Keeping the „Health‟ in Health Insurance‟, Economic and Political Weekly‟,
vol. 44, no. 38, 2009, pp.18-21.
7. Duggal, R. and Gangoli, L. V., „Introduction to Review of Healthcare in India‟ L. V.
Gangoli, R. Duggal and A. Shukla (ed.) in Review of healthcare in India, Centre for Enquiry into
Health and Allied Themes, 2005.
8. Ellis, R. P., Alam, M. and Gupta, I., „Health Insurance in India: Prognosis and Prospects‟
Economic and Political Weekly, vol.35, no.4, 2000, pp. 204-217.
9. Fan, V. Y., Karan, A. and Mahal, A., „State health insurance and out-of-pocket health
expenditures in Andhra Pradesh, India, International Journal of Healthcare Finance Economics,
DOI 10.1007/s10754-012-9110-5, vol.12, no. 22, 2012, pp. 189-215.
10. Garg, C. and Karan, A., „Reducing out-of-pocket Expenditures to Reduce Poverty: a
Disaggregated Analysis at Rural-Urban and State Level in India‟. Health Policy and Planning,
vol. 24, no. 2, 2008, pp. 116–28.
11. Garg, C.C. and Karan, A.K., „Health and Millennium Development Goal 1: Reducing out
of Pocket Expenditure to Reduce Income Poverty: Evidences from India‟, Equitap Project,
working paper 15, 2005.
12. Ghosh Soumitra (2010): Catastrophic Payments and Impoverishment Due to Out-of-
Pocket Health Spending: The effects of Recent Health Sector Reforms in India, Asia Health
Policy Program, Working Paper.
ISSN: 2249-2496 Impact Factor: 7.081
832 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
13. Ghosh, S., „Health Sector Reforms and changes in prevalence of untreated morbidity,
choice of healthcare providers among the poor and rural population in India‟, International
Journal of Heath Policy and Management, vol. 2, no.3, 2014, pp.125-130.
14. Ghosh, S., „Health Sector Reforms and changes in prevalence of untreated morbidity,
choice of healthcare providers among the poor and rural population in India‟, International
Journal of Heath Policy and Management, vol. 2, no.3, 2014, pp.125-130.
15. Ghosh, S., „The utilization of Healthcare Services in India: Do Education and income
Matter?, a paper presented in the conference of Indian Association for Social Sciences and
Health, 2009.
16. Guhan, S., „Health in India during a Period of Structural Adjustment‟, S. Subranium (ed.)
in India’s Development Experience, Oxford University Press, 2001.
17. Hooda, S.K., Changing Pattern of Public Expenditure on Health in India: Issues and
Challenges, Institute for Studies in Industrial Development (ISID) and Public Health Foundation
of India Collaborative Research Programme, Working Paper Series 01, 2013.
18. Hsiao, W.C., „Why is a Systematic View of Health Financing Necessary? Health Affairs,
vol. 26. no. 4, 2007, pp. 950-961.Available at
http://content.healthaffairs.org/content/26/4/950.full
19. Kumar, C. and Prakesh, R., „Public-Private Dichotomy in Utilization of Health Care
Services in India‟. The Journal of Sustainable Development , vol.5, no.1, 2011, pp. 25-52.
20. Mudgal, J., Sarkar, S. and Sharma, T., „Health Insurance in Rural India‟ Economic and
Political Weekly, vol. 40.no. 43, 2005, pp. 4640-4646.
21. Mukherjee, S. and Levesque, J. F., „Changing Inequalities in Utilization of Inpatient Care
in Rural India: Evidence from the National Sample Survey (NSS)‟, Economic and Political
Weekly, vol. 45, no. 46, 2010, pp. 84-91.
22. Peter, D.H., Sujatha K.R. and Fryatt, R., „Lumping and Splitting: the health policy
agenda in India‟, Health Policy Plan, vol. 18, no. 3, 2003, pp. 249-260.
23. Ram, F. and Shekhar, C., „Ranking and Mapping of Districts Based on Socio-economic
and Demographic Indicators‟ International Institute of Population Sciences, Ministry of Health
and Family Welfare, Government of India (2006)
24. Rao, S., „Health Insurance: Concepts Issues and Challenges‟, Economic and Political
Weekly, vol.39, no.34, 2004, pp. 3835-3844.

ISSN: 2249-2496 Impact Factor: 7.081
833 International Journal of Research in Social Sciences
http://www.ijmra.us, Email: [email protected]
25. Sarma, S., “Public Investment in Primary Healthcare”, Mittal Publication, New Delhi, pp.
41-47.
26. Selvaraj, S. and Karan, A.K., „Why Publicly Financed Health Insurance Schemes are
Ineffective in Providing Financial Risk Protection‟, Economic and Political Weekly, vol. 47, no.
18, 2012, pp. 60-68.
27. Selvaraju, V. and Annigeri, V.B., Trends in Public Spending in Health in India,
Background Paper for Commission on Macroeconomics and Health (India Study) Indian Council
for Research on International Economic Relations, 2001.
28. Tulashidhar, V.B., „Compression and Health Sector Outlays‟ Economic and Political
Weekly, vol. 28, no. 45, 1993, pp. 2473-2477.


















