
IMPACT Guideline
126
Transcript of IMPACT Guideline

IMPACT Third Edition (Version 3.0) 1
Reducing bacterial resistance with IMPACT –
Interhospital Multi-disciplinary Programme on AntimicrobialChemoTherapy
This guideline is available for download at:
HKU Centre of Infection
http://www.hku.hk/hkucoi/impact.pdf
DH Centre for Health Protection
http://www.chp.gov.hk/files/pdf/reducing_bacterial_resistance_with_impact.pdf
HA intranet
http://ha.home/ho/ps/impact.pdf
IMPACT Third Edition (Version 3.0) 2
Editors: PL Ho and SSY Wong
Third Edition 2005
Version 3.0
Second edition: 2001 (ver 2.0), 2002 (ver 2.1), 2003 (ver 2.2)
First edition: 1999
All rights reserved. No part of this publication may be reproduced, stored in a retrieved system, or transmitted, in any form or by any
means, electronic, mechanical, photocopying, and recording or otherwise, without the prior approval from IMPACT
We seek to improve the quality of this document. If you have comments or suggestion on this draft, please email to
[email protected] or [email protected]
NOTICE
This publication contains information relating to general principles of medical care, which should not be
construed as specific instructions for individual patients. Manufacturers' product information and package inserts
should be reviewed for the latest information, including contraindications, dosages and precautions. The editors, the
working group and publisher are not responsible for errors or omissions or for any consequences from the application of the
information in this document and make no warranty, express or implied, with respect to the currency, accuracy, or completeness of the
contents of the publication. Application of this information in a particular situation remains the professional responsibility of the
health care professionals. Readers are reminded that some products may not be available in their instutues.
IMPACT Third Edition (Version 3.0) 3
IMPACT Working Group
Co-chairpersons Dr. Raymond Wai Hung, YUNG
Head, Infection Control Branch, Centre for Health Protection, Department of Health
Dr. Dominic Ngai Chong, TSANG
Consultant Microbiologist, Department of Clinical Pathology Queen Elizabeth Hospital
Members (alphabetical order)
Dr. S Anandaciva Consultant Department of Anaesthesiology and
Intensive Care Unit Tuen Mun Hospital
Dr. Kin Sang, CHAN Chief of Service Department of Pulmonary Medicine Haven of Hope Hospital
Dr. Wai Ming, CHAN Consultant Intensive Care Unit Queen Mary Hospital
Dr. Sik To, LAI Consultant Department of Medicine Princess Margaret Hospital
Dr. Wai Man, LAI Chief of Service Department of Microbiology Prince of Wales Hospital
Dr. Patrick CK, LI Chief of Service Department of Medicine Queen Elizabeth Hospital
Dr. Wei Kwang, LUK Senior Medical Officer Department of Clinical Pathology Tseung Kwan O Hospital
IMPACT Third Edition (Version 3.0) 4
Dr. Tak Keung, NG Consultant Microbiologist Department of Clinical Pathology Princess Margaret Hospital
Dr. Tak Lun, QUE Consultant Microbiologist Department of Clinical Pathology Tuen Mun Hospital
Dr. Loletta KY, SO Senior Medical Officer Department of Medicine Pamela Youde Nethersole Eastern
Hospital
Dr. Wing Kin, TO Senior Medical Officer Department of Clinical Pathology Yan Chai Hospital
Dr. Kwan Keung, WONG Chief of Service Department of Medicine
North District Hospital
Dr. Sai Hung, YEUNG Consultant Department of Orthopaedic Surgery Pamela Youde Nethersole Eastern
Hospital
Dr. Wai Chun, YIP Chief of Service Department of Surgery Kwong Wah Hospital
Mr. Pak Wai, LEE Chief Pharmacist Hospital Authority Head Office
IMPACT Third Edition (Version 3.0) 5
Academic advisors
Professor Robert MT, CHAN Professor of Infectious Diseases Department of Medicine University of British Columbia Vancouver, Canada
Dr. Pak Leung, HO Associate Professor and Honorary Consultant
Division of Infectious Diseases, Department of Microbiology & Centre of Infection
The University of Hong Kong
Professor Margaret IP Professor Department of Microbiology Chinese University of Hong Kong
Professor Allan R. RONALD Distinguished Professor Emeritus (Internal Medicine,Medical Microbiology and Community Health Sciences)
University of Manitoba Canada
Professor Kenneth WT, TSANG Professor and Honorary Consultant Department of Medicine Queen Mary Hospital
Professor Kwok Yung, YUEN Chair Professor in Infectious Diseases Division of Infectious Diseases,
Department of Microbiology & Centre of Infection
The University of Hong Kong
IMPACT Third Edition (Version 3.0) 6
Secretaries
Dr. Cindy WS, TSE Associate Consultant
Department of Clinical Pathology
Kwong Wah Hospital
Dr. Alan KL, WU Medical Officer
Department of Clinical Pathology
Pamela Youde Nethersole Eastern Hospital
Dr. Tak Chiu, WU Associate Consultant
Department of Medicine
Queen Elizabeth Hospital
IMPACT Third Edition (Version 3.0) 7
ContentsList of tables ......................................................................................9Foreword .........................................................................................10Preface.............................................................................................11
Part I: Antibiotic resistance- local scenario ..................................12
Methicillin-resistant Staphylococcus aureus......................................16Vancomycin-resistant enterococci .....................................................17ESBL-producing Enterobacteriaceae .................................................17Enterobacter spp. .............................................................................19
Part II: Antimicrobial stewardship programme .............................21
Antimicrobial stewardship program: summary .................................22Classification of therapy...................................................................34
Part III: Guidelines for selected antimicrobials use ......................37
Vancomycin.....................................................................................38Quinupristin/dalfopristin and linezolid ............................................43Ceftazidime......................................................................................45Imipienem/meropenem/ertapenem..................................................48Once daily aminoglycosides..............................................................50Summary of selected antifungal agents ............................................54
Part IV: Recommendation for the empirical therapy of common
infections .......................................................................................59
Musculoskeletal infections ...............................................................60Skin and soft tissue infections .........................................................61Central nervous system infections....................................................62Intra-abdominal and GI system infections ........................................63Cardiovascular infections.................................................................64Gynaecological infections .................................................................65Head and neck infections .................................................................65Urinary tract infections ....................................................................65Respiratory tract infections ..............................................................66Guidelines on the use and choice of antibiotics in severe acute pancreatitis .....................................................................................71Management of community-acquired pneumonia .............................74General considerations and principles..............................................74
IMPACT Third Edition (Version 3.0) 8
Part V: Guidelines for known pathogen therapy ...........................81
Part VI: Guidelines for surgical prophylaxis..................................88
Antibiotic prophylaxis in clean operations ........................................90Antibiotic prophylaxis in clean-contaminated operations ..................92Antibiotic prophylaxis in contaminated-infected operations ..............94
Part VII: Cost and recommended dosage of commonly-used
antimicrobial agents ......................................................................95
Preparation and recommended dosing regimens for antibiotics.........96Cost comparison of selected IV antibiotics ......................................100Cost comparison of systemic antifungal agents...............................102Dosage of antimicrobial agents for CNS infections ..........................103Intra-peritoneal antibiotic dosing recommendations for patients with CAPD peritonitis ............................................................................104
Reference List ................................................................................105Abbreviations.................................................................................123
IMPACT Third Edition (Version 3.0) 9
List of tables
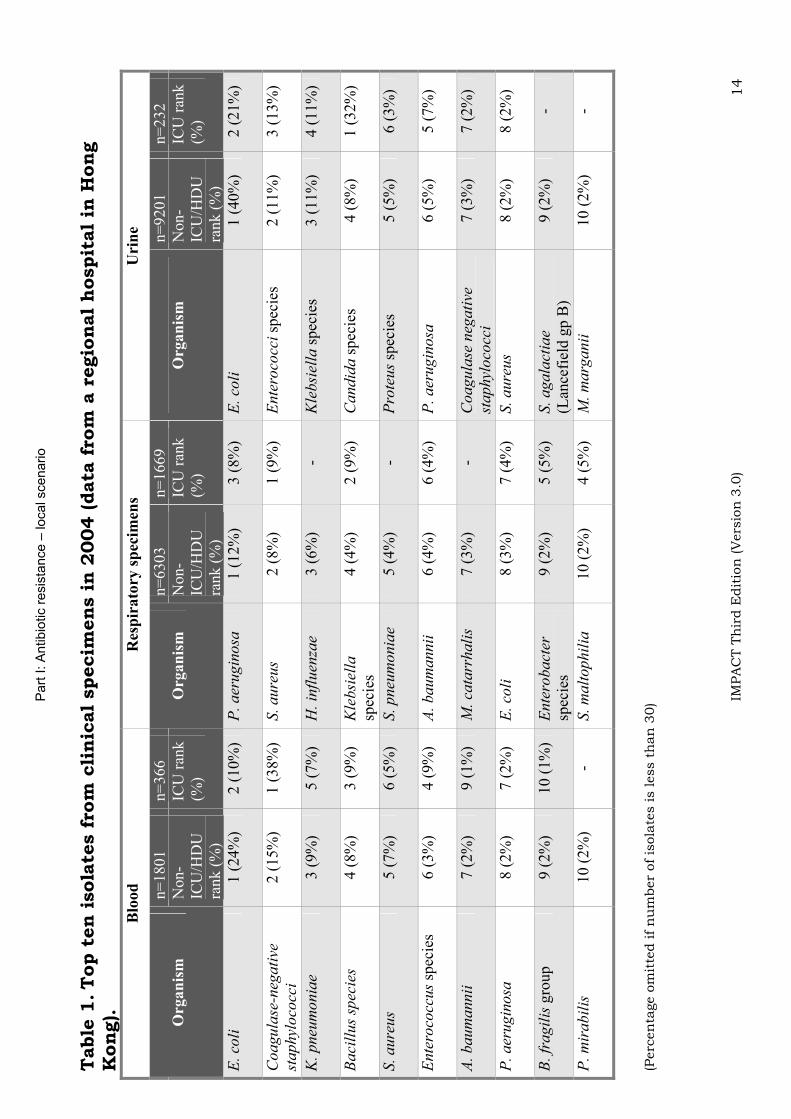
Table 1. Top ten isolates from clinical specimens in 2004 (data from a
regional hospital in Hong Kong). .......................................... 14
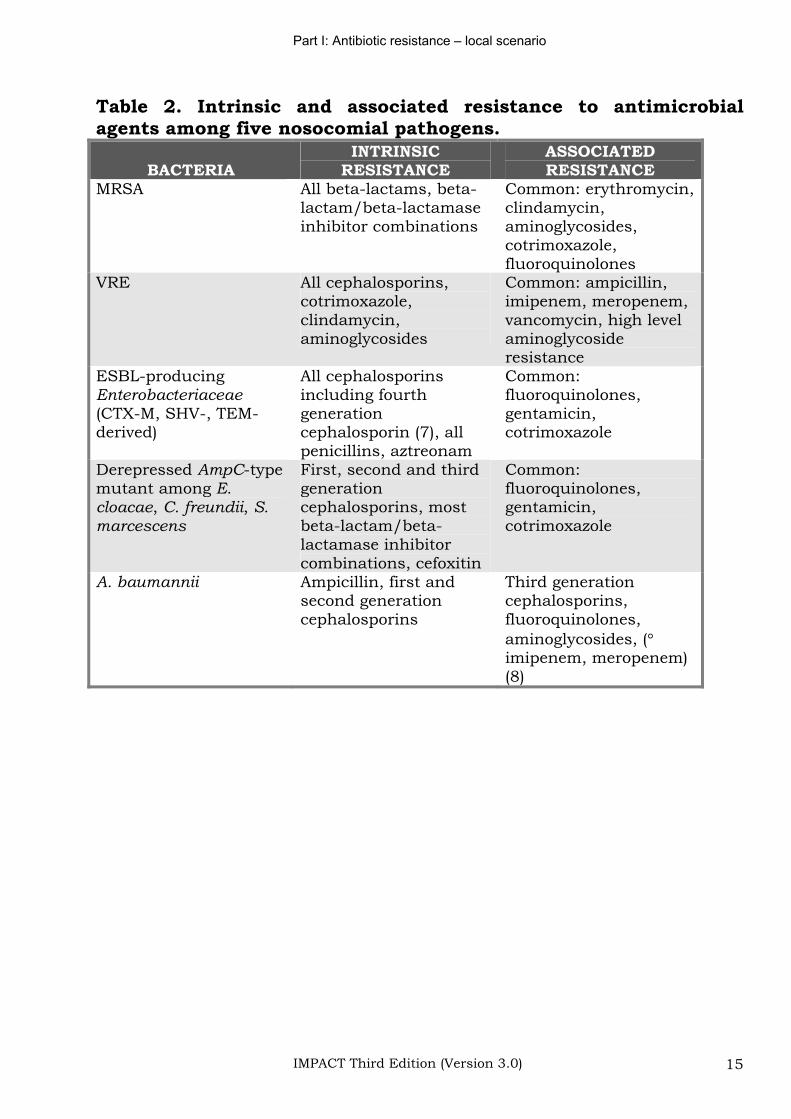
Table 2. Intrinsic and associated resistance to antimicrobial agents
among five nosocomial pathogens. ....................................... 15
Table 3. Methods to implement antimicrobial control......................... 28
Table 4. Potential barriers to reaching the strategic goals .................. 29
Table 5. Summary of published data on antimicrobial strategies as an
intervention to reduce ESBL resistance................................ 33
Table 6. Strategies for optimization of antimicrobial therapy.............. 36
Table 7. Dosage table for vancomycin................................................ 41
Table 8. Calculation of vancomycin dose for morbidly obese patient... 42
Table 9. Comparison of linezolid and quinupristin/dalfopristin.......... 44
Table 10. Hartford Hospital once-daily aminoglycoside normogram for
gentamicin and tobramycin ................................................. 53
Table 11. General patterns of antifungal susceptibility ...................... 54
Table 12. Comparison of susceptibility of selected fungi to the azoles 55
Table 13. Mechanisms of antifungal action........................................ 56
Table 14. Comparison of selected pharmacokinetic parameters for the
azoles and caspofungin ...................................................... 57
Table 15. A suggested scheme for systemic antifungal agents ............ 58
Table 16. Criteria for severity assessment of acute pancreatitis ......... 72
Table 17. Prophylactic use of antibiotic in acute pancreatitis ............. 73
Table 18. Comparative activities of commonly used beta-lactams
against Streptococcus pneumoniae with different levels of
penicillin susceptibility....................................................... 80
IMPACT Third Edition (Version 3.0) 10
Foreword
Antibiotics are one of the essential armaments for management of infections. Antimicrobial resistance results in increased morbidity, mortality, and costs of health care. It is becoming a global problem. Prevention of the emergence of resistance and the spread of resistant microorganisms will reduce these adverse effects and their attendant costs. Promoting appropriate use of antibiotic has shown to be an effective means to control antimicrobial resistance.
In Hong Kong, our long-term battle against antibiotic resistance continues and antimicrobial guideline is an essential tool to promote rational use of antimicrobial agents with better application of existing knowledge and adherence to good practice.
The IMPACT was developed in 1999 as a first step towards better control of the growing problem of antimicrobial resistance in Hong Kong. Developed with a multidisciplinary approach with inputs from different specialties and institutions, the IMPACT took into account the local data on prevalence of different pathogens and antimicrobial resistance patterns.
Now into its third edition, the IMPACT has incorporated constructive comments from clinicians and other colleagues as part of an on-going effort to keep abreast of new antibiotics, changing resistance patterns and literature. This specifically developed guideline for practitioners in Hong Kong provides evidence-based principles focused on situations in which antimicrobial therapy could be curtailed without compromising patient care.
The third edition of the IMPACT is a timely update to coincide with the launching of the Antibiotic Stewardship Programme by the Hospital Authority which includes optimal selection, dose and duration of treatment, as well as control of antibiotic use. The IMPACT constitutes an essential element along with other key elements of education, user-feedback, regular updates, clinical audits and process evaluation in this comprehensive Programme.
I thank the many individuals and organizations who have contributed to the compilation of IMPACT and look forward to your continued support and partnership in our Antibiotic Stewardship Programme.
Dr Cheung Wai-lun DirectorProfessional Services and Operations Hospital Authority
IMPACT Third Edition (Version 3.0) 11
Preface
The “IMPACT” programme is a collaborative effort by recognized authorities in the areas of clinical microbiology and infection, infectious diseases, public health medicine, hospital epidemiology, intensive care medicine, respirology, surgery, orthopaedics and traumatology, and clinical pharmacology. The IMPACT working group recognizes the challenges from drug-resistant organisms and believes that the adverse impact of antimicrobial resistance could be reduced through a better and more judicial use of the existing agents. The document is intended to be of interest and value to colleagues who practise in institutional settings and prescribe or evaluate antimicrobial agents.
This new edition updates and revises all the information in the previous edition. The document is now organized into eight parts. Part 1 and II covers the background information. Part III provides guidelines on the use of six classes of antibiotics. They are discussed separately because they represent new agents (linezolid, quinupristin-dalfopristin), agents in which usage has a strong link to development of multidrug-resistant organisms (glycopeptides, ceftazidime, and carbapenems) or that the dosing and monitoring are complicated (aminoglycosides). Several new sections have been added: antimicrobial stewardship programme, severe acute pancreatitis, antifungal agents, and antibiotic dosing for CAPD peritonitis. The font size and the print-out size have been increased to enhance readability. A full list of tables and a quick reference are added to facilitate the use of this book.
The editors are grateful to the contributions by our experts in the working group. The secretaries are skillful and meticulous in their attention to the compilation of the document. On behalf of the working group, we thank the Infection Control Branch of the Centre for Health Protection for providing administrative support, the Chief Pharmacist Office in the Hospital Authority for the generous support in printing the hard copies and all colleagues who have provided us with their valuable opinions in the preparation of this document.
PL Ho SSY Wong November 2005
Part I: Antibiotic resistance – local scenario
IMPACT Third Edition (Version 3.0) 12
Part I: Antibiotic resistance- local scenario
Part I: Antibiotic resistance – local scenario
IMPACT Third Edition (Version 3.0) 13
Background: the problem of antimicrobial resistance in Hong Kong
1. The emergence of resistance has threatened the successful treatment of patient with infections (1-5).
2. Antimicrobial resistance increases drug costs, length of stay and adversely affects patient’s outcome (6).
3. Resistance to all classes of antibiotics has developed to various extents among the common and important nosocomial pathogens (Tables 1 and 2).
Part
I: A
ntibio
tic r
esis
tance –
local scenario
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 14
Table
1.T
op t
en
isola
tes f
rom
cli
nic
al
specim
en
s i
n 2
004 (data
fro
m a
regio
nal
hospit
al
in H
on
g
Kon
g).
Blo
od
R
esp
irato
ry s
pec
imen
s U
rin
e
n=
1801
n=
366
n=
6303
n=
1669
n=
9201
n=
232
Org
an
ism
Non-
ICU
/HD
U
ran
k (
%)
ICU
ran
k
(%)
Org
an
ism
Non-
ICU
/HD
U
ran
k (
%)
ICU
ran
k
(%)
Org
an
ism
Non-
ICU
/HD
U
ran
k (
%)
ICU
ran
k
(%)
E.
coli
1
(2
4%
) 2
(1
0%
) P
. aer
ugin
osa
1
(1
2%
) 3
(8
%)
E.
coli
1
(4
0%
) 2
(2
1%
)
Co
ag
ula
se-n
ega
tive
sta
ph
ylo
cocc
i
2 (
15
%)
1 (
38
%)
S.
au
reu
s 2
(8
%)
1 (
9%
) E
nte
roco
cci
spec
ies
2 (
11
%)
3 (
13
%)
K. pneu
monia
e 3
(9
%)
5 (
7%
) H
. in
flu
enza
e 3
(6
%)
-K
leb
siel
la s
pec
ies
3 (
11
%)
4 (
11
%)
Ba
cill
us
spec
ies
4 (
8%
) 3
(9
%)
Kle
bsi
ella
spec
ies
4 (
4%
) 2
(9
%)
Candid
a s
pec
ies
4 (
8%
) 1
(3
2%
)
S.
au
reu
s 5
(7
%)
6 (
5%
) S
. p
neu
mo
nia
e 5
(4
%)
-P
rote
us
spec
ies
5 (
5%
) 6
(3
%)
En
tero
cocc
us
spec
ies
6 (
3%
) 4
(9
%)
A.
ba
um
an
nii
6
(4
%)
6 (
4%
) P
. aer
ugin
osa
6
(5
%)
5 (
7%
)
A.
ba
um
an
nii
7
(2
%)
9 (
1%
) M
. ca
tarr
hali
s 7
(3
%)
-C
oa
gu
lase
neg
ati
ve
sta
ph
ylo
cocc
i
7 (
3%
) 7
(2
%)
P. aer
ugin
osa
8
(2
%)
7 (
2%
) E
. co
li
8 (
3%
) 7
(4
%)
S.
au
reu
s 8
(2
%)
8 (
2%
)
B.
fra
gil
is g
roup
9 (
2%
) 1
0 (
1%
) E
nte
robact
ersp
ecie
s
9 (
2%
) 5
(5
%)
S. agala
ctia
e (L
ance
fiel
d g
p B
)
9 (
2%
) -
P. m
irabil
is
10
(2
%)
- S. m
alt
ophil
ia
10
(2
%)
4 (
5%
) M
. m
arg
anii
1
0 (
2%
) -
(Perc
en
tage o
mit
ted if n
um
ber
of is
ola
tes is less t
han
30)
Part I: Antibiotic resistance – local scenario
IMPACT Third Edition (Version 3.0) 15
Table 2. Intrinsic and associated resistance to antimicrobial agents among five nosocomial pathogens.
BACTERIAINTRINSIC
RESISTANCEASSOCIATEDRESISTANCE
MRSA All beta-lactams, beta-lactam/beta-lactamaseinhibitor combinations
Common: erythromycin, clindamycin,aminoglycosides,cotrimoxazole,fluoroquinolones
VRE All cephalosporins, cotrimoxazole,clindamycin,aminoglycosides
Common: ampicillin, imipenem, meropenem, vancomycin, high level aminoglycosideresistance
ESBL-producingEnterobacteriaceae(CTX-M, SHV-, TEM-derived)
All cephalosporins including fourth generationcephalosporin (7), all penicillins, aztreonam
Common:fluoroquinolones,gentamicin,cotrimoxazole
Derepressed AmpC-type mutant among E. cloacae, C. freundii, S.marcescens
First, second and third generationcephalosporins, most beta-lactam/beta-lactamase inhibitor combinations, cefoxitin
Common:fluoroquinolones,gentamicin,cotrimoxazole
A. baumannii Ampicillin, first and second generation cephalosporins
Third generation cephalosporins,fluoroquinolones,aminoglycosides, (imipenem, meropenem) (8)
Part I: Antibiotic resistance – local scenario
IMPACT Third Edition (Version 3.0) 16
Methicillin-resistant Staphylococcus aureus
On the basis of the patient history and epidemiological analysis, Methicillin-Resistant Staphylococcus aureus (MRSA) may be categorized into healthcare-associated or community-associated.
Healthcare-associated MRSA (HA-MRSA)
This type of MRSA is endemic in the local healthcare environment including hospitals, extended care facilities and old age homes since the mid-1980s (3;4;9). The HA-MRSA tends to be isolated in patients who are hospitalized for more than 48 hours. Since MRSA carriage may persist for many months after a previous acquisition, HA-MRSA also include those isolates that are found at admission (or within 48 hours) from patients who possess risk factors for their carriage including hospitalization in the previous 1 year, recent surgery, old age home residence, renal dialysis and exposure to invasive devices and employment in a healthcare institute (10;11).
In Hong Kong, 30-50% of all hospital S. aureus isolates are currently resistant to methicillin. The proportion of MRSA increased to 70-80% among isolates from intensive care units (ICU). In 1999, a study involving ICUs in 11 public hospitals showed 12% of the patients were MRSA carriers at ICU admission and that new acquisition of MRSA occurred in about 12% of the patients who were non-carriers initially (12).
Most HA-MRSA also encode a battery of other resistance genes, theyare thus multiresistant to drugs in other antibiotic classes including aminoglycosides, macrolides, fluoroquinolones and clindamycin (3;12).
Community-associated MRSA (CA-MRSA)
1. Patients infected with CA-MRSA do not have the usual risk factors associated with HA-MRSA. In overseas countries, CA-MRSA were found to be more common among certain populations: children with chronic skin condition, prisoners, military personnel, aboriginals, injection drug users, the homeless and contact sports athletes (13-16); but such associations have not been observed among the CA-MRSA cases in Hong Kong.
Part I: Antibiotic resistance – local scenario
IMPACT Third Edition (Version 3.0) 17
2. This organism often remains susceptible to antibiotic classes other than beta-lactams, including clindamycin, aminoglycosides, tetracyclines and fluoroquinolones.
3. The genotypes of CA-MRSA are different from the local nosocomial strains. Most CA-MRSA strains in Hong Kong represent members in clonal cluster 30, similar to the situation in the Southwest Pacific region (17).
4. CA-MRSA possesses novel types of methicillin-resistance cassette elements: type SCCmec IV or V, which are rare among the HA-MRSA strains.
5. CA-MRSA is more likely to encode the virulence factor, Panton-Valentine leukocidin (PVL) toxin, which is associated with skin/soft tissue infections and severe necrotizing pneumonia (18).
Vancomycin-resistant enterococci
VRE here refers to E. faecium and E. faecalis with resistance to glycopeptides (vancomycin MIC 8 g/mL or teicoplanin MIC 16g/mL). The incidence of VRE in Hong Kong is low at present. The first
isolate of VRE (E. faecium) in Hong Kong was imported in 1997. In the subsequent 3 years, a few sporadic cases were identified in five hospitals including a small cluster recently in TMH. By the end of March 2001, about 10 cases of VRE have been detected, including both vancomycin-resistant E. faecium (vanA and vanB) and E. faecalis (vanA) (19). In a multicentre surveillance of 1600 consecutive patients hospitalized in >10 ICUs in 1999, the prevalence was found to be <0.1%.
ESBL-producing Enterobacteriaceae
1. Extended-Spectrum Beta-Lactamases (ESBLs) are any bacterial enzymes that are capable of inactivation of third generation cephalosporins. The term is most commonly used to refer to a group of bacterial enzymes that are derived from the classical beta-lactamases TEM-1, TEM-2 and SHV-1. In recent years, the “CTX-M” type of ESBL is also emerging in several Asian countries including China and Hong Kong SAR (20-22).
Part I: Antibiotic resistance – local scenario
IMPACT Third Edition (Version 3.0) 18
2. ESBL may lead to therapeutic failures despite apparent susceptiblity to some third generation cephalosporins in conventional antibiotic sensitivity testing methods. The ESBLs confer variable levels of resistance to cefotaxime, ceftazidime, other broad-spectrum cephalosporins, and to monobactams such as aztreonam, but had no detectable activity against the carbapenems (such as imipenem, ertapenem and meropenem).
3. If antibiotic therapy is indicated (colonization do not need any treatment other than infection control), serious infections by ESBL-producers should be regarded as clinically resistant to all the cephalosporins (including cefepime).
4. The ESBLs are usually encoded on genes in plasmids and because of the ready transmissibility of the responsible plasmids, dissemination of the resistance genes to other micro-organisms occur readily. Since genes encoding resistance to multiple antibiotics are often present in the same plasmid, co-transfer of multiple resistance to non-beta-lactam drugs, such as aminoglycosides, cotrimoxazole, chloramphenicol, and tetracycline is common.
5. At present, the prevalence of ESBLs among Enterobacteriaceae isolated in many tertiary hospitals around the world is over 10-15%. In Hong Kong, a survey of four hospitals in 1997/98 (1200 non-duplicate clinical isolates) revealed rates of 6-23% for Klebsiella pneumoniae and 9 -14% for E. coli. (23).
6. Numerous outbreaks due to ESBL-producing bacteria have been reported. Known risk factors for colonization and/or infection with organisms harbouring these enzymes include admission to an intensive care unit, recent surgery, instrumentation, prolonged hospital stay and antibiotic exposure, especially exposure to third generation cephalosporins.
7. Incidence of ESBLs can decrease after changes in antibiotic policy (mainly reducing the use of third generation cephalosporins) and enforcement of barrier precautions (Table 5).
8. Most CTX-M, TEM- and SHV-derived ESBLs are susceptible to inhibition by the beta-lactamase inhibitors and theoretically beta-lactam/beta-lactamase inhibitor combinations should be active against these isolates. It must be remembered that production of ESBL doesn't preclude other mechanisms of resistance. In a recent survey, it was found that 40-70% of the ESBL-producing
Part I: Antibiotic resistance – local scenario
IMPACT Third Edition (Version 3.0) 19
Enterobacteriaceae were resistant to amoxicillin-clavulanate,ampicillin-sulbactam, ticarcillin-clavulanate, piperacillin-tazobactam and cefoperazone-sulbactam (20).
Enterobacter spp.
1. De-repression of AmpC beta-lactamase occurs most frequently among Enterobacter spp. De-repressed mutants are resistant to all the first, second and third generation cephalosporins.
2. AmpC-mediated resistance usually cannot be reversed by the currently available beta-lactamase inhibitors. Hence, most de-repressed mutants are also resistant to ampicillin-sulbactam, amoxicillin-clavulanate, piperacillin-tazobactam, ticarcillin-clavulanate, and cefoperazone-sulbactam.
3. It should be noted that resistance may develop in 20-40% of serious Enterobacter infections during treatment with a second or third generation cephalosporin (refer to Part V for treatment recommendations).
4. In Hong Kong, a recent study found AmpC de-repression in 23% of all Enterobacter spp. (21). It was also found that ESBL of the CTX-M type may be emerging in some Enterobacter spp., such as E. hormaechei. Therefore, laboratories should pay attention to speciation of Enterobacter and be alert to the possibility of ESBL production in this genus.
Multidrug-resistant Pseudomonas aeruginosa
1. Pseudomonas aeruginosa, a saprophyte widely distributed in nature and moist habitats (e.g. sinks, respiratory equipment, antiseptic or detergent solutions found in hospitals), is being increasingly recognized as a nosocomial pathogen, especially among critically ill or immunocompromised patients. Cross transmission or acquisition among patients likely occurs through hands of healthcare workers, or via contaminated fomites.
2. Under increasing antibiotic selection pressure, P. aeruginosa could acquire increasing drug resistance, leading to emergence of multi-drug-resistant phenotype (MRPA). By definition, MRPA isolates exhibit beta-lactam multiresistance (piperacillin, piperacillin-
Part I: Antibiotic resistance – local scenario
IMPACT Third Edition (Version 3.0) 20
tazobactam, ceftazidime, cefepime, carbapenems), along with resistance to aminoglycosides and quinolones (24-26); underlying mechanisms include enhanced production and dissemination of novel beta-lactamases, decreased outer membrane permeability, and presence of drug efflux pumps (27;28).
3. During the past 10 years, there have been numerous reported outbreaks of MRPA worldwide (29-33). According to the recent global SENTRY surveillance conducted in 1997-1999, the rates of MRPA (defined as being resistant to piperacillin, ceftazidime, imipenem, and gentamicin) occurrence were as follows: Latin America, 8.2%; Europe, 4.7%; United States, 1.2%; Asia Pacific, 1.6%; and Canada, 0.9% (34). More recent reports indicate that the overall prevalence of MRPA continues to be on the rise, especially in tertiary care institutions (35;36). The exact prevalence of MRPA in Hong Kong is currently not known.
4. In patients suffering from chronic chest conditions (e.g. cystic fibrosis), MRPA infection occurs after chronic airway colonization (37); other patients appear to acquire the infection after hospitalization. MRPA is predominantly isolated from respiratory samples (35;38). Risk factors for nosocomial MRPA acquisition and infection included: old age; severe underlying disease and / or being bedridden (39); having maxillary sinusitis; high lung injury score and / or need for prolonged mechanical ventilation (40;41); various forms of instrumentation (e.g. urinary catheters and nasogastric feeding tubes (39;39), long dwelling central venous catheters (41). Prolonged use of antipseudomonal antibiotics such as beta-lactams, carbapenems, and fluoroquinolones is also important risk factor (38-41).
5. Treatment of MRPA infections is extremely difficult (42;43), because MRPA can be resistant to all the currently available anti-pseudomonal antibiotics, and may necessitate the use of unlicensed and potentially toxic drugs such as colistin and polymyxin B, or experimental combinations (44-46). Unfortunately, the new antibiotics (such as glycylcyclines and ketolides) in the pipeline are not active against MRPA. In view of this, MRPA infected or colonized patients should be nursed in single rooms whenever feasible and that all attending staff should practise hand hygiene for every patient contact and other necessary standard and contact precautions.
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 21
Part II: Antimicrobial stewardship programme
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 22
Antimicrobial stewardship program: summary
The present summary is based on an article in the Hong Kong Medical Journal (47).
Antimicrobial drug resistance is now an important public health threat because it endangers our ability to effectively treat infections. A multi-faceted approach involving the continuous application of a package of interventions should be implemented at regional and international levels. In healthcare settings, the recommended measures include infection prevention, effective diagnosis and early treatment, using antimicrobials wisely and breaking the chain of transmission (Centers for Disease Control and Prevention, 2003). In the local settings, studies have found that there are rooms for optimization of antimicrobial prescriptions in the hospitals. Research conducted in the recent years further indicates that improvement in the pattern of prescriptions is feasible and can be implemented by means of antimicrobial stewardship programme (ASP) in a safe, scientific and professional manner. As antibiotic-resistant bacteria become more widespread, such initiatives will be assuming increasingly important roles. Therefore, the Scientific Committee on Infection Control in the Centre for Health Protection recently come up with a document on “Optimizing antimicrobial prescriptions in hospitals by antimicrobial stewardship programme in Hong Kong: consensus statement”. The present text summarizes the document under six broad questions:
1. What is the definition for optimal antimicrobial use?
Optimal antimicrobial use (prudent prescribing) has been defined as “the cost-effective use of antimicrobials which maximizes their clinical therapeutic effect, while minimizing both drug-related toxicity and the development of antimicrobial resistance” (48;49). This implies usage in the most appropriate way for the treatment or prevention of human infectious diseases, having regard to the diagnosis, evidence of clinical effectiveness, likely benefits, safety, cost, and propensity for the emergence of resistance. Therefore, optimal antibiotic use means both “less” use (i.e. less unnecessary use), and “appropriate” use (i.e. not only the right antibiotic but also the right dose, route and duration to effect a cure while minimizing side effects and development of resistance according to the up-to-date knowledge).
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 23
2. What is the rationale for optimizing antimicrobial use?
There are growing concerns about antimicrobial resistance. As antimicrobial resistance increases, many previously time-honored, first-line therapies are rapidly losing their efficacies and are becoming obsolete (49). Antimicrobial resistance adds substantially to our already rising healthcare costs, prolongs periods during which individuals are infectious, increases morbidity, increases length of hospital stay, and even mortality.
In developed countries, studies have found that 30-40% of hospitalized patients were treated with antimicrobial agents. When antimicrobial usage was studied, there are large variations in the pattern of usage (50;51) and half of the usage could be classified as suboptimal using recommended quality indicators (52;53). It is clear that suboptimal use not only adversely affects patient outcome (54;55), but also increases the risk of developing antimicrobial resistance (52;53;56;57).
Currently, the issue of antimicrobial resistance is complicated further by an insecure supply of new agents (58-60) and a dwindling number of companies investing in antimicrobial agents (61). Despite the dramatic rise of antimicrobial resistance in the past five years, only two new classes of antibiotics were approved since 2000: oxazolidinones (linezolid) and the cyclic lipopeptides (daptomycin). In 2004, there are few novel antibacterial agents in the pipeline. Thus, improving the use of existing antibiotics by all clinicians is imperative.
3. What is antimicrobial stewardship programme? Who are the advocacies? (Table 3)
The term antimicrobial stewardship is defined as the optimal selection, dosage, and duration of antimicrobial treatment that results in the best clinical outcome for the treatment or prevention of infection, with minimal toxicity to the patient and minimal impact on subsequent resistance (62). In practice, this involves prescribing antimicrobial therapy only when it is beneficial to the patient, targeting therapy to the desired pathogens and using the appropriate drug, dose, and duration. Thus, ASP should not be viewed simply as reduced use or a strategy for cost containment. Instead, by minimizing exposure to drugs, performing dose adjustments, reducing redundant therapy and targeting therapy to
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 24
the likely pathogens, such activities can be viewed as a strategy to enhance patient safety.
ASP involves a multidisciplinary, programmatic, prospective, interventional approach to optimizing the use of antimicrobial agents. The multidisciplinary team typically includes clinical microbiologists, infectious diseases specialists, infection control practitioners, and clinical pharmacists. Having members from other medical specialties, such as surgery and paediatrics, is also recommended. Multiple approaches have been employed to enforce hospital policies to limit or control antimicrobial use (Table 3). Under the auspice of ASP, several behavioural methods have been used successfully to effect changes, including problem-based education, consensus guidelines, peer review, concurrent review, data feedback, computer-based reminders, financial incentives, and the use of opinion leaders (63;64).
Many professional societies and public health guardians including the World Health Organization, Infectious Diseases Society of America (IDSA), Alliance for the Prudent Use of Antibiotics (APUA), Food and Drug Administration (FDA), Centers for Disease Control and Prevention (CDC), National Institutes of Health (NIH) are supportive of programmes that promote optimal antimicrobial use (65;66). A few have even gone a step forward with action plans (48;65-67).
4. Is there evidence that ASP is beneficial? How did people document the benefits of the programme? Is there any evidence that it leads to better and more optimal antibiotic use in the hospital setting?
Most studies found this strategy effective in reducing the usage of targeted antibiotics and in controlling antimicrobial expenditures. In terms of its impact on antimicrobial resistance, programmatic interventions in hospitals have yielded mixed results (68;69). The reason for this is that the factors promoting resistance are complex and multiple. It is clear that strong relationship exists between certain antibiotic classes and multi-drug resistant pathogens such as vancomycin with VRE; third generation cephalosporins with ESBL; and fluoroquinolones with MRSA and MRPA. At an institutional level, programmes designed to limit utilization of agents that exert greater effect on the above were successful in reducing the specific resistance rates.
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 25
Measurement and monitoring is an essential part of the programme.After an initial implementation of a restricted formulary and antimicrobial approval system as part of an antimicrobial control programme, the team should meet regularly to review and update the formulary, assess its effectiveness, provide and coordinate ongoing physician education, and analyze antimicrobial utilization data within the hospital. The programme should be dynamic, and continually reassessed, adding new components or deleting unsuccessful components over time.
To allow for accurate intra- and inter-institutional comparison, confounding differences in expenditure related to acquisition costs and variations in the amount of individual antibiotic used for individual patients should be corrected by appropriate standardization using the defined daily dose (DDD) and rates calculated in terms of DDD per 1,000 admissions and DDD per 1,000 bed-days.
5. Is this the right time for Hong Kong to introduce ASP? Are we too early, or are we too late, and why?
In Hong Kong, few would dispute the threat from antimicrobial resistance and the needless expenditures associated with excessive antimicrobial use (70). Recent surveys show that suboptimal antimicrobial prescriptions may be commonplace in our hospitals (71), and that they could be improved. In the two university hospitals, one prospective study in 2003 found that 76% of antibiotic prescriptions for patients hospitalized for exacerbation of chronic obstructive pulmonary disease were unjustified according to the prevailing Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines (71). In 2004, real-time audit of “big gun” antibiotics in two hospitals have revealed that 20-25% of the prescriptions were not justified or suboptimal. The most common problems include treatment of colonization, narrower and equally effective alternative or less toxic alternatives not being used and inappropriate duration (Seto WH, personal communication). In another prospective study of antibiotic combinations over a six-month period, it was found that one of the agents was redundant in 80% of 200 prescription episodes (71).
More actions are required in areas where the antimicrobial resistance problem is most serious. In Hong Kong, there is evidence that antibiotic resistance in some important nosocomial pathogens
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 26
is worse than in many other parts of the world (72). In the United States, a “Public health action plan to combat antimicrobial resistance-action plan” was developed in 1999. In the United Kingdom, significant progress has been made in optimizing the clinical use of antimicrobials since 2000 in terms of governmental directives, strategy and action plan (67;73). Recently, similar initiatives have been launched in Taiwan and South Korea at a national level. It is, therefore, definitely not premature to introduce such a “universal” and “continuous” programme to the public hospitals in Hong Kong.
Many studies have found that optimization of antibiotics in hospitals was feasible, safe and effective. A diversity of approaches have been reported and the experience accumulated so far indicates a multi-faceted “stewardship” and “immediate concurrent feedback” approach has clear advantages (62;74-81).
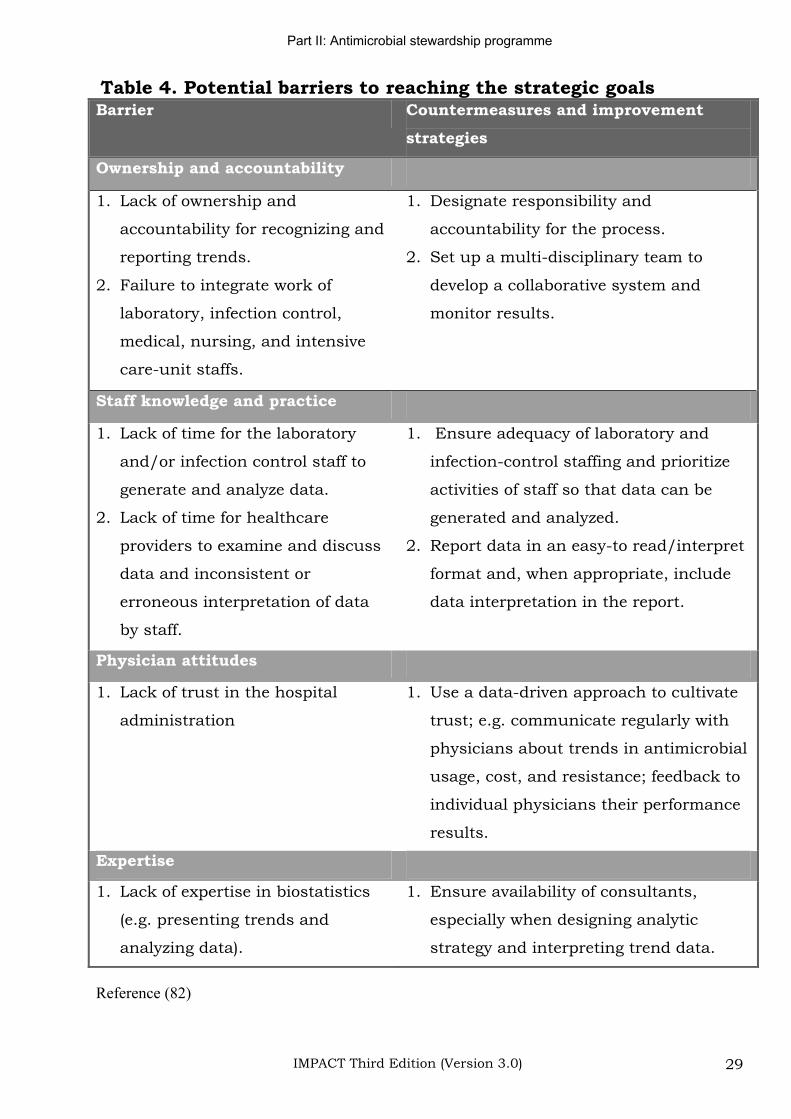
6. What are the disadvantages for having ASP? What problems have been reported? Are there any arguments against having ASP in the literature? Is there a role for an alternative mechanism? (Table 4)
ASP involves proactive monitoring and feedbacks. One alternative approach is “no control” (i.e. only by passive means). Such an approach relies heavily on the distribution of national guidelines. As discussed in detail in an international workshop, such a strategy has not worked in the past (82). Guidelines are seldom studied thoroughly by clinicians, and even if they are read, they rarely are incorporated into everyday practice. On the other hand, there are barriers and concerns to ASP that need to be addressed (Table 4). The perception of “threatened physician autonomy” can be a significant impediment to the effort. Previous studies and local experiences have indicated that this is often an “emotional” response that can be resolved by immediate concurrent feedback, consensus building, involvement of institutional opinion leaders, and attention to process measures (83-85). In fact, similar programmes have been launched successfully in some Hospital Authority hospitals for the other drugs, including the statins, calcium channel blockers and acid suppressive agents.
Another impediment is the incorrect perception that antimicrobial stewardship programmes are solely cost-driven and that patient safety may be at risk. In this regard, recent
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 27
reports have emphasized the inclusion of quality indicators such as time to reception of appropriate empirical antibiotics. Other suggested indicators include: (a) clinical outcomes of bacteraemia due to Gram-negative organisms (86), (b) mortality for all patients, for those treated with antimicrobials, and for those suffering from infections, (c) duration of hospital stay for all patients and for those treated with antimicrobial drugs, and (d) re-hospitalization rate within 30 days after discharge for all patients and those treated with antimicrobial drugs (81). As in any quality improvement programme, a financial incentive is important to secure support by the hospital management. This is no exception for antimicrobial stewardship programme. Good leadership and effective communications are essential to keep members, prescribers and patients to the appropriate focus. This could be enhanced by having a multidisciplinary steering committee, and by regular use of data feedback on the patterns of usages, patient outcomes, and antimicrobial resistance data. In principle, member in the committee should have a strong sense of commitment and cooperation. The composition of the multidisciplinary steering committee may be unique to each institute.
Conclusion
Considering the broader perspective, working targets are needed and the programmes should be regularly evaluated. For a start, each hospital will need to form a steering group and to lay down the institutional priorities. In the literature, programme models are available for optimizing the uses of aminoglycosides, vancomycin, broad-spectrum antibiotics, antibiotic combinations, and for switching therapy from intravenous to oral. It is clear that a multi-faceted approach incorporating immediate concurrent feedback is most likely to be successful. In order to safeguard health care quality, the use of quality indicators and timely feedback of data are essential. Our fight against antimicrobial resistance is going to continue. Hence, a major challenge will be how to keep the programmes viable and sustainable within our system in the longer terms.
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 28
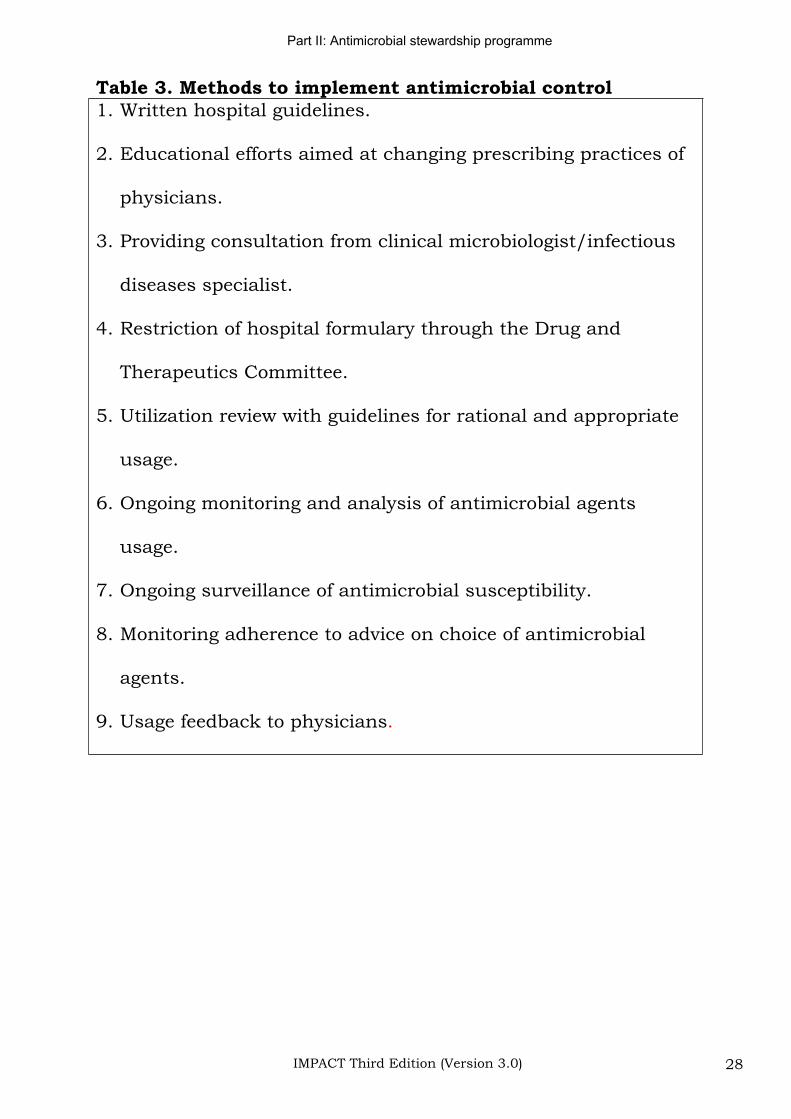
Table 3. Methods to implement antimicrobial control 1. Written hospital guidelines.
2. Educational efforts aimed at changing prescribing practices of
physicians.
3. Providing consultation from clinical microbiologist/infectious
diseases specialist.
4. Restriction of hospital formulary through the Drug and
Therapeutics Committee.
5. Utilization review with guidelines for rational and appropriate
usage.
6. Ongoing monitoring and analysis of antimicrobial agents
usage.
7. Ongoing surveillance of antimicrobial susceptibility.
8. Monitoring adherence to advice on choice of antimicrobial
agents.
9. Usage feedback to physicians.
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 29
Table 4. Potential barriers to reaching the strategic goals Barrier Countermeasures and improvement
strategies
Ownership and accountability
1. Lack of ownership and
accountability for recognizing and
reporting trends.
2. Failure to integrate work of
laboratory, infection control,
medical, nursing, and intensive
care-unit staffs.
1. Designate responsibility and
accountability for the process.
2. Set up a multi-disciplinary team to
develop a collaborative system and
monitor results.
Staff knowledge and practice
1. Lack of time for the laboratory
and/or infection control staff to
generate and analyze data.
2. Lack of time for healthcare
providers to examine and discuss
data and inconsistent or
erroneous interpretation of data
by staff.
1. Ensure adequacy of laboratory and
infection-control staffing and prioritize
activities of staff so that data can be
generated and analyzed.
2. Report data in an easy-to read/interpret
format and, when appropriate, include
data interpretation in the report.
Physician attitudes
1. Lack of trust in the hospital
administration
1. Use a data-driven approach to cultivate
trust; e.g. communicate regularly with
physicians about trends in antimicrobial
usage, cost, and resistance; feedback to
individual physicians their performance
results.
Expertise
1. Lack of expertise in biostatistics
(e.g. presenting trends and
analyzing data).
1. Ensure availability of consultants,
especially when designing analytic
strategy and interpreting trend data.
Reference (82)
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 30
State-of-the art: Limiting antimicrobial resistance
1. US surveys: 22-65% usage of antibiotics in the hospitals is inappropriate.
2. Outbreaks of multi-resistant bacteria, including those that persist despite apparently adequate infection control measures, can be limited effectively by antibiotic programme directed at judicious use of antibiotics.
3. While restriction of an individual antibiotic (such as cefotaxime or ceftazidime) has been reported to be useful in controlling outbreaks of drug-resistant bacteria, the general consensus is that the main focus should be directed at the rational use of all classes of antibiotics rather than merely restricting the use of individual drugs (6;86-96).
Over-prescription of third generation cephalosporins and vancomycin
Experience from several overseas centres suggests that over-prescription of third generation cephalosporins and glycopeptides are closely associated with the selection and dissemination of ESBL-producing Enterobacteriaceae, de-repressed AmpC-type mutant among Enterobacter cloacae, Citrobacter freundii, Serretia marcescens, MRSA, and VRE.
1. Cephalosporin use has been identified as a risk factor for enterococcal colonization and superinfection, as well as for antibiotic-associated diarrhea, the main reason for oral vancomycin (97;98).
2. Significant risk factors for colonization or infection with VRE were prior antibiotic use (p=0.04), the previous use of third-generation cephalosporins (p=0.03), and the previous use of parenteral vancomycin (p=0.002). This data was obtained from 7 hospitals including primary and tertiary care facilities (200-700 beds) (99).
3. In the Cornell University Medical College, New York, it was found that the duration of hospitalization, intrahospital transfer between floors, use of antimicrobials (i.e. vancomycin and third generation cephalosporins), and duration of vancomycin use ( 7
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 31
days) were independently associated with VRE infection or colonization (100).
4. Ten weeks after the introduction of cefotaxime, resistant Enterobacter cloacae could be isolated from stool cultures in an increasing proportion of patients and septicaemia developed in 6 cases (101).
5. In 6 US hospitals, previous administration of third-generation cephalosporins was more likely to be associated with multi-resistant Enterobacter isolates in an initial positive blood culture (69%) than was administration of antibiotics (20%) that did not include a third-generation cephalosporins (p<0.001) (102).
6. Resistance to third generation cephalosporins among Enterobacter spp, Citrobacter freundii, Morganella morganii,Serratia marcescens and Providencia spp. has become widespread both locally within hospitals and nationally. This trend has been shown to correlate closely with the extent of usage of some third generation cephalosporins (1;103).
Decreased antibiotic resistance after changes in antibiotic use
No simple answer exists on the control of multi-drug resistant bacteria. The traditional approach slanted heavily on infection control measures, which are obviously important but can be difficult to implement. When audited, compliance with hand hygiene measures has been consistently low (<40%) (104). Outbreaks of multi-drug resistant bacteria have continued despite apparent adherence to “standard” hygienic measures. In recent years, there has been renewed interest on the strategic use of antibiotics as a measure for prevention or control of antimicrobial resistance (94). In fact, several studies have demonstrated that strategic use of antibiotics (so far, only class restriction of the cephalosporins have been evaluated to a significant extent) can lead to:
1. Less multi-resistant de-repressed AmpC-type Enterobacter spp. An outbreak of infections by multi-resistant Enterobacter spp. disappeared after use of cefotaxime was discontinued in the unit.
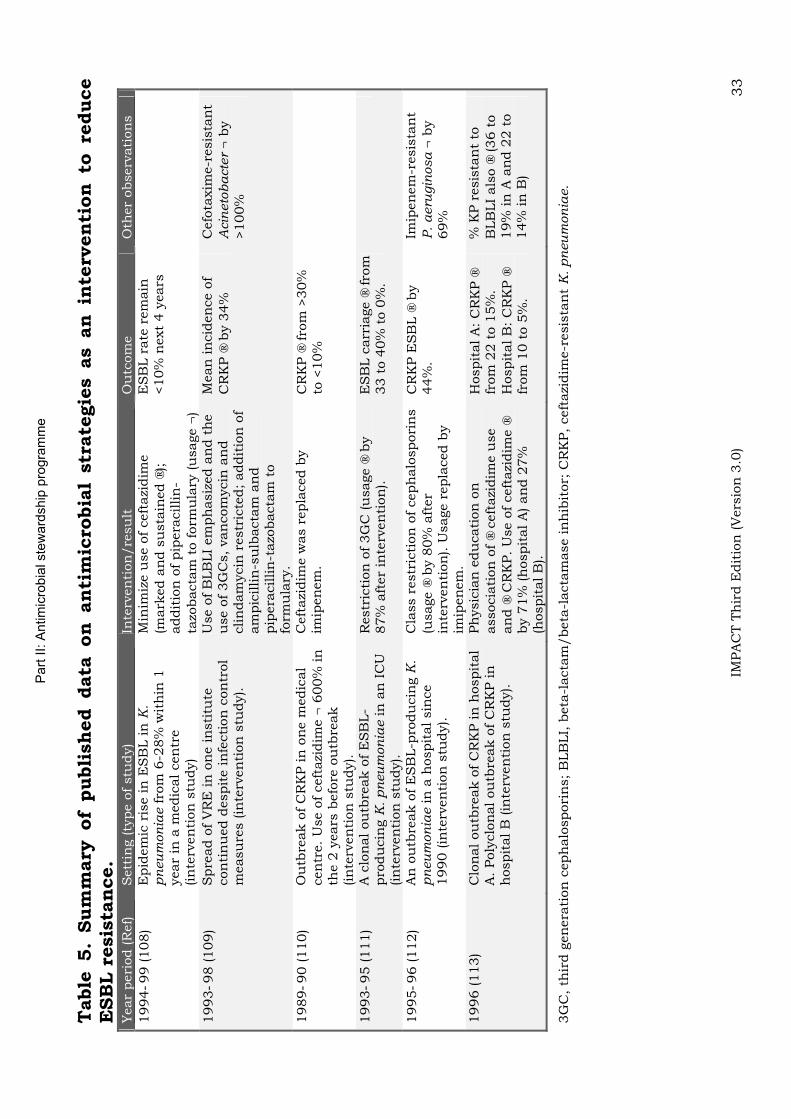
2. Less ESBL-producing Enterobacteriaceae. Literature on antimicrobial strategies as an intervention to reduce ESBL-producing K. pneumoniae was summarized in Table 5. In a case-

Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 32
control study, the use of beta-lactam/beta-lactamase inhibitor combination was shown to be a protective factor (105).
3. Less vancomycin-resistant enterococci. Two studies reported on the successful control of VRE outbreaks by changing antibiotic usage (92;106). In one medical centre (92) , the antibiotic formulary was altered by restricting the use of cefotaxime and vancomycin and adding beta-lactamase inhibitors to replace third-generation cephalosporins. After 6 months, the average monthly use of cefotaxime, ceftazidime, vancomycin, and clindamycin had decreased by 84%, 55%, 34% and 80% respectively (p<0.02). The point prevalence of faecal colonization with VRE decreased from 47-15% (p<0.001). In another haematologic unit (106), acquisition of VRE paralleled the use of ceftazidime as empirical therapy for neutropenic fever. Phase 1: ceftazidime as empirical therapy, VRE carriage rate was 57%. Phase 2: piperacillin-tazobactam replaced ceftazidime as empirical therapy, VRE carriage decreased to 8%. Phase 3: ceftazidime re-introduced as empirical therapy, VRE carriage increased to 36%. Those who are interested in the experimental data that might explained this observed relation between VRE, cephalosporins and BLBLI should refer to a recent review by Rice et al (107).
Part
II: A
ntim
icro
bia
l ste
ward
ship
pro
gra
mm
e
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 33
Table
5.
Sum
mary
of
publi
sh
ed data
on
an
tim
icro
bia
l str
ate
gie
s as an
in
terv
en
tion
to
re
duce
ESB
L r
esis
tan
ce.
Year
peri
od (R
ef)
Sett
ing (ty
pe o
f stu
dy)
Inte
rven
tion
/re
su
lt
Ou
tcom
e
Oth
er
observ
ati
on
s
1994
99 (108)
Epid
em
ic r
ise in
ES
BL in
K.
pn
eu
mon
iae fro
m 6
-28%
wit
hin
1
year
in a
medic
al cen
tre
(in
terv
en
tion
stu
dy)
Min
imiz
e u
se o
f ceft
azi
dim
e
(mark
ed a
nd s
usta
ined
);addit
ion
of pip
era
cillin
-ta
zobacta
m t
o form
ula
ry (u
sage
)
ES
BL r
ate
rem
ain
<10%
next
4 y
ears
1993
98 (109)
Spre
ad o
f V
RE
in
on
e in
sti
tute
con
tin
ued d
espit
e in
fecti
on
con
trol
measu
res (in
terv
en
tion
stu
dy).
Use o
f B
LB
LI
em
ph
asiz
ed a
nd t
he
use o
f 3G
Cs, van
com
ycin
an
d
clin
dam
ycin
restr
icte
d; addit
ion
of
am
pic
illin
-su
lbacta
m a
nd
pip
era
cillin
-tazo
bacta
m t
o
form
ula
ry.
Mean
in
cid
en
ce o
f C
RK
P b
y 3
4%
C
efo
taxim
e-r
esis
tan
t A
cin
eto
ba
cte
r b
y
>100%
1989
90 (110)
Ou
tbre
ak o
f C
RK
P in
on
e m
edic
al
cen
tre. U
se o
f ceft
azi
dim
e
600%
in
th
e 2
years
befo
re o
utb
reak
(in
terv
en
tion
stu
dy).
Ceft
azi
dim
e w
as r
epla
ced b
y
imip
en
em
. C
RK
P fro
m >
30%
to
<10%
1993
95 (111)
A c
lon
al ou
tbre
ak o
f E
SB
L-
pro
du
cin
g K
. pn
eu
mon
iae in
an
IC
U
(in
terv
en
tion
stu
dy).
Restr
icti
on
of 3G
C (u
sage
by
87%
aft
er
inte
rven
tion
).
ES
BL c
arr
iage
fro
m
33 t
o 4
0%
to 0
%.
1995
96 (112)
An
ou
tbre
ak o
f E
SB
L-p
rodu
cin
g K
. p
neu
mon
iae in
a h
ospit
al sin
ce
1990 (in
terv
en
tion
stu
dy).
Cla
ss r
estr
icti
on
of ceph
alo
spori
ns
(usage
by 8
0%
aft
er
inte
rven
tion
). U
sage r
epla
ced b
y
imip
en
em
.
CR
KP E
SB
L
by
44%
.
Imip
en
em
-resis
tan
t P
. a
eru
gin
osa
b
y
69%
1996 (113)
Clo
nal ou
tbre
ak o
f C
RK
P in
hospit
al
A. Poly
clo
nal ou
tbre
ak o
f C
RK
P in
h
ospit
al B
(in
terv
en
tion
stu
dy).
Ph
ysic
ian
edu
cati
on
on
associa
tion
of
ceft
azi
dim
e u
se
an
d C
RK
P. U
se o
f ceft
azi
dim
e
by 7
1%
(h
ospit
al A
) an
d 2
7%
(h
ospit
al B
).
Hospit
al A
: C
RK
P
from
22 t
o 1
5%
. H
ospit
al B
: C
RK
P
from
10 t
o 5
%.
% K
P r
esis
tan
t to
B
LB
LI
als
o
(36 t
o
19%
in
A a
nd 2
2 t
o
14%
in
B)
3G
C, th
ird g
en
era
tion
ceph
alo
spori
ns; B
LB
LI,
beta
-lacta
m/beta
-lacta
mase in
hib
itor;
CR
KP, ceft
azi
dim
e-r
esis
tan
t K
. pn
eu
mon
iae.
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 34
Classification of therapy
Empirical therapy
In the clinical situation of “empirical use”, the antimicrobial(s) is/are used as initial therapy directed to eradicate the most likely pathogens. Before initiation of antimicrobials, appropriate specimens for stains and culture of microorganisms should be obtained. Results of identification and susceptibility of microorganisms are likely to be available in the following 48 to 72 hours. The use of broad-spectrum antibiotics or combination therapy is usually necessary to cover the different organisms capable of causing an infection. In general, the use of agents in this situation should not extend beyond the time required to obtain results of cultures and susceptibility.
Choice of agent(s): based upon adequate coverage of the potential pathogens of the potential infection sites and the anticipated antimicrobial susceptibility patterns of the bacterial isolates. Recommendations of empirical therapy for some common infections are outlined in Part IV.
Known-pathogen therapy
In the clinical situation of known pathogen use, the antimicrobial(s) is /are used when the microbiology laboratory has identified the micro-organism causing the infection and the susceptibility pattern is known. If during empirical use, the patient is started on combination therapy or broad spectrum antibiotics, the antimicrobial spectrum should be narrowed to cover the micro-organisms identified as the aetiologic agent. Streamlining from broad-spectrum to specific, narrow spectrum antimicrobials helps to avoid colonization with resistant organisms and superinfections. In the absence of allergy or other contraindications, the agent (appropriate for the site and type of infection) with the narrowest spectrum in a group or a list of candidate drugs should be used.
It should be noted that the skin and mucous membrane surface of the hospitalized patient are often colonised with nosocomial bacteria (such as MRSA, E. coli, Klebsiella spp, etc.), systemic antimicrobial therapy (both IV and PO) should not be administered in an attempt to eradicate these micro-organisms.
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 35
Switch therapy-conversion from IV to PO
In the clinical situation of switch therapy use, PO antimicrobials replace IV usage for completion of therapy. IV is almost always employed in serious infections to ensure maximal serum/tissue levels. With few exceptions such as meningitis, infective endocarditis, the majority of patients with infections do not require completion of the antimicrobial course with IV therapy. The following criteria have been developed for transition from IV to PO antimicrobial (114;115):
1. Patient with no clinical indication for IV therapy.
2. Patient is afebrile for at least 8 hours.
3. The WBC count is normalizing (falling towards or <10x109/L).
4. Signs & symptoms related to infection are improving.
5. Patient is not neutropenic (neutrophil count >2 x109/L).
6. Patient is able to take drugs by mouth (non-NPO).
7. Patient with no continuous nasogastric suctioning.
8. Patient with no severe nausea or vomiting, diarrhea, gastrointestinal obstruction, motility disorder.
9. Patient with no malabsorption syndrome.
10. Patient with no pancreatitis or active gastrointestinal bleeding or other conditions that contraindicated to the use of oral medications.
Part II: Antimicrobial stewardship programme
IMPACT Third Edition (Version 3.0) 36
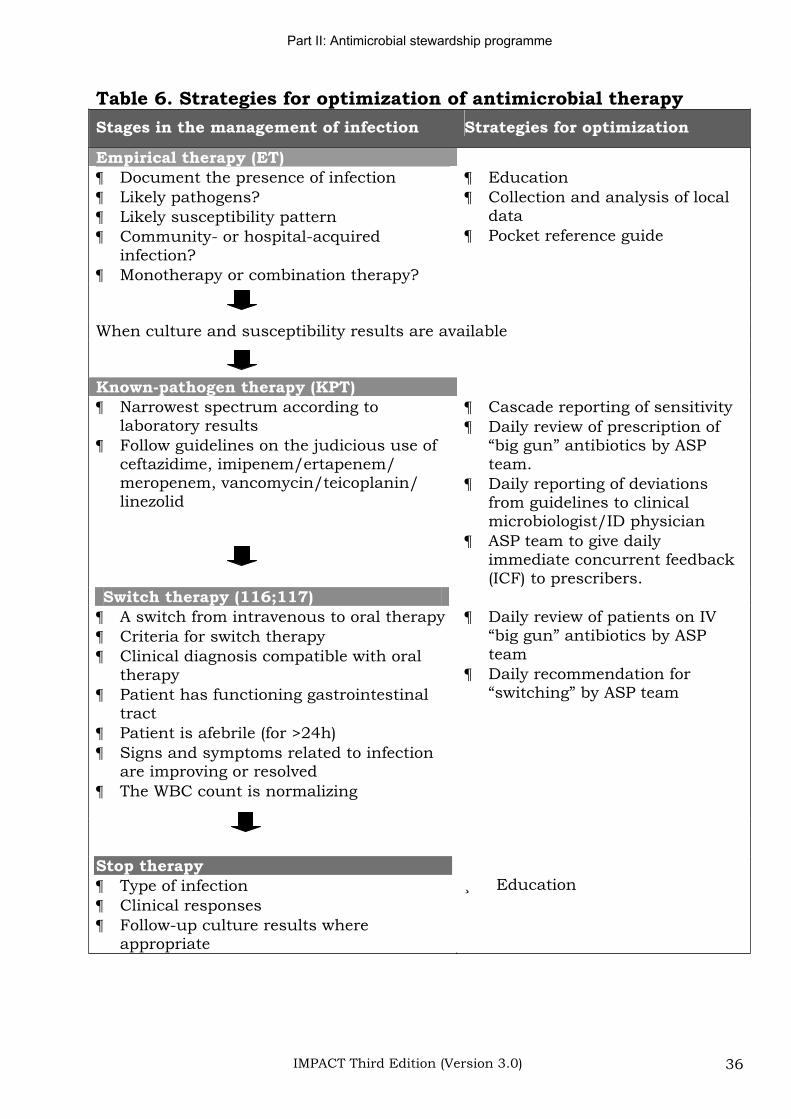
Table 6. Strategies for optimization of antimicrobial therapy
Stages in the management of infection Strategies for optimization
Empirical therapy (ET) Document the presence of infection Likely pathogens? Likely susceptibility pattern Community- or hospital-acquired infection?Monotherapy or combination therapy?
EducationCollection and analysis of local dataPocket reference guide
When culture and susceptibility results are available
Known-pathogen therapy (KPT) Narrowest spectrum according to laboratory results Follow guidelines on the judicious use of ceftazidime, imipenem/ertapenem/ meropenem, vancomycin/teicoplanin/ linezolid
Cascade reporting of sensitivity Daily review of prescription of “big gun” antibiotics by ASP team.Daily reporting of deviations from guidelines to clinical microbiologist/ID physician ASP team to give daily immediate concurrent feedback (ICF) to prescribers.
Switch therapy (116;117) A switch from intravenous to oral therapy Criteria for switch therapy Clinical diagnosis compatible with oral therapyPatient has functioning gastrointestinal tractPatient is afebrile (for >24h) Signs and symptoms related to infection are improving or resolved The WBC count is normalizing
Daily review of patients on IV “big gun” antibiotics by ASP teamDaily recommendation for “switching” by ASP team
Stop therapy Type of infection Clinical responses Follow-up culture results where appropriate
Education

Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 37
Part III: Guidelines for selected antimicrobials use
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 38
Vancomycin
Situations in which the use of vancomycin/teicoplanin is appropriate (6;83)
1. Treatment of serious infections caused by beta-lactam resistant Gram-positive bacteria (e.g. MRSA, coagulase-negative staphylococci).
2. Treatment of infections caused by Gram-positive bacteria in patients who have serious allergies to beta-lactam antimicrobial agents (e.g. anaphylactic reaction, Stevens-Johnson syndrome).
3. When Clostridium difficile colitis fails to respond to metronidazole therapy or is severe and life-threatening.
4. As prophylaxis for endocarditis following certain procedures in-patients at high risk for endocarditis; according to recommendation from the American Heart Association. (e.g. as prophylaxis for genitourinary or gastrointestinal procedures in moderate or high-risk patients allergic to ampicillin/amoxicillin).
5. As prophylaxis for major surgical procedures involving the implantation of prosthetic material or devices in known carriers of MRSA. For elective procedures, daily washing of skin and hair with a suitable antiseptic soap (e.g. 4% chlorhexidine liquid soap) and topical treatment of the anterior nares with nasal mupirocin ointment (for 5 days) are recommended before the procedures. Vancomycin may be less effective in preventing surgical wound infection due to methicillin-sensitive staphylococci (118).
Situations in which the use of vancomycin/teicoplanin are not advised
1. Treatment of MRSA nasal carriage or colonization at other sites such as the isolation of MRSA from
Surface swab of superficial wounds
Surface swab of chronic ulcers
Surface swab of pressure ulcers
2. Routine surgical prophylaxis other than in a patient who has serious allergy to beta-lactam antimicrobial agents.
3. Routine empirical antimicrobial therapy for neutropenic fever (except as recommended by the IDSA 2002 guidelines for the use of antimicrobial agents in neutropenic patients with unexplained fever).
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 39
4. Treatment in response to a single blood culture positive for coagulase-negative staphylococci, if other blood cultures taken during the same time frame are negative.
5. Continued empirical use of presumed infections in patients whose cultures (blood, joint fluid, peritoneal fluid, pus, etc), are negative for beta-lactam-resistant Gram-positive bacteria (e.g. MRSA).
6. Systemic or local (e.g. antibiotic lock) prophylaxis against infection (or colonization) of indwelling (central or peripheral) intravascular catheters.
7. As routine prophylaxis, before insertion of Hickman/Brovac catheter or Tenckhoff catheter.
8. As part of the regimen for selective digestive tract decontamination.
9. Primary treatment of Clostridium difficile colitis, except when it is severe and life-threatening.
10. Routine prophylaxis for patients on continuous ambulatory peritoneal dialysis or haemodialysis.
11. Treatment (e.g. chosen for dosing convenience) of infection caused by beta-lactam-sensitive Gram-positive bacteria in patients who have renal failure.
12. Use of vancomycin solution for topical application (e.g. to burn wound, ulcers) or irrigation (e.g. of T-tube, drains).
Vancomycin dosage in special situations and therapeutic drug monitoring
1. In adults, the standard recommended dose of vancomycin is 30 mg/kg/day (IV 1 g q12h or IV 0.5 g q6h in a normal 70 kg person).
2. Therapeutic drug monitoring (TDM)
Vancomycin exhibits time-dependent killing. Efficacy can usually be assumed if the trough concentration is sufficiently above the MIC of the infecting organism (i.e. best if vancomycin levels at site of infection are maintained above MIC throughout the dose interval). MIC of most susceptible organisms (e.g. MRSA) ranges 1-2 g/mL.
Routine TDM is not indicated in most patients because vancomycin pharmacokinetics are sufficiently predictable that safe and effective vancomycin dosage regimens (giving trough
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 40
levels 5-10 g/mL and peak levels <40 mg/mL) can be constructed on the basis of patient's age, weight and estimated renal function.
Indications for TDM
(a) Renal impairment (rapid change/unstable renal function making it difficult to estimate dose)
(b) ICU patients co-treated with dopamine and/or dobutamine (119)
(c) Severe burn (120)
(d) Morbid obesity (121)
(e) Spinal cord injury (122)
When TDM is indicated, check only trough level. There is no solid data to support the widely referenced trough range of 5-10 g/mL and accordingly, serum concentrations have been selected somewhat arbitrarily, based on pharmacology, retrospective studies, case reports and personal opinions. Due to the poor penetration of vancomycin to certain lung tissues, the 2005 ATS guideline recommend trough levels of 15 20 g/mL for treatment of MRSA hospital-acquired pneumonia (123). Current literature does not support peak concentration measurement (124).
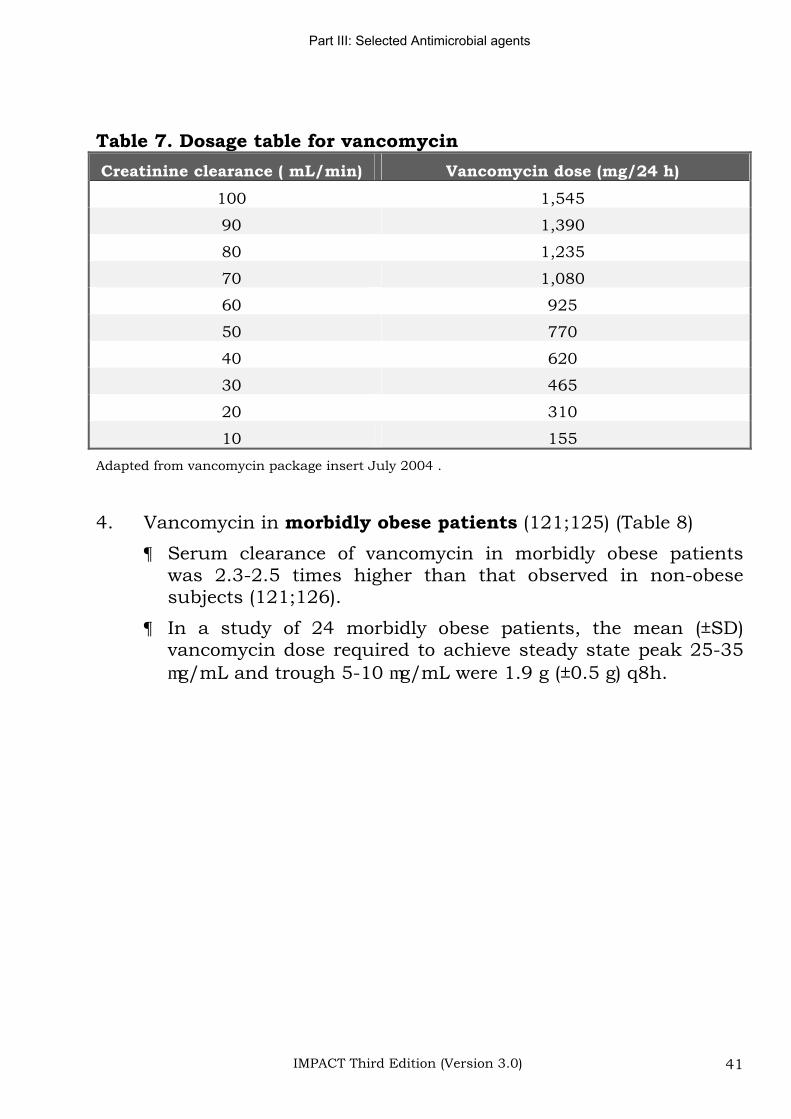
3. Dosage table/nomogram in patients with impaired renal function (Table 7)
An initial single dose of 15 mg/kg should be given to achieve prompt therapeutic serum concentration. Subsequent daily maintenance dose is to be determined according to dosage table/nomogram.
The dosage table/nomogram is not valid for functionally anephric patients on dialysis. For such patients, the dose required to maintain stable concentrations is 1.9 mg/kg/day (~130 mg/day for a 70 kg person).
For patients with marked renal impairment, it may be more convenient to give maintenance doses of 0.25 g to 1 g every 3-7 days.
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 41
Table 7. Dosage table for vancomycin
Creatinine clearance ( mL/min) Vancomycin dose (mg/24 h)
100 1,545
90 1,390
80 1,235
70 1,080
60 925
50 770
40 620
30 465
20 310
10 155
Adapted from vancomycin package insert July 2004 .
4. Vancomycin in morbidly obese patients (121;125) (Table 8)
Serum clearance of vancomycin in morbidly obese patients was 2.3-2.5 times higher than that observed in non-obese subjects (121;126).
In a study of 24 morbidly obese patients, the mean (±SD) vancomycin dose required to achieve steady state peak 25-35 g/mL and trough 5-10 g/mL were 1.9 g (±0.5 g) q8h.
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 42
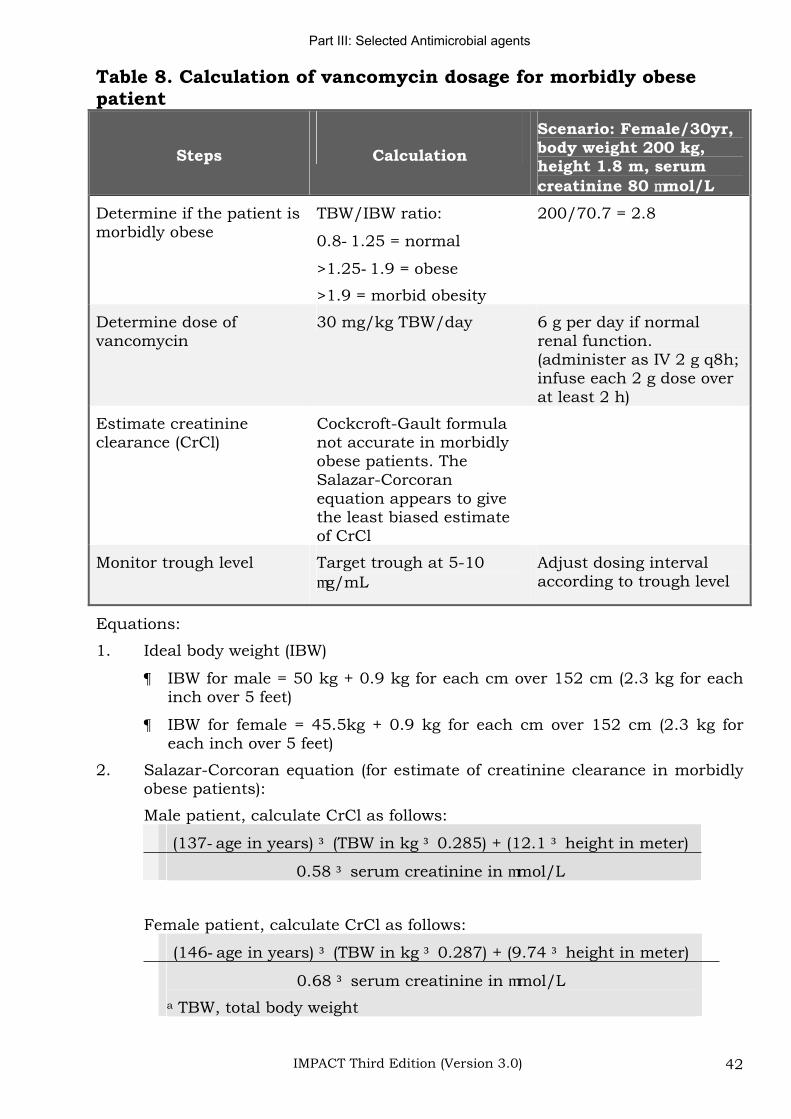
Table 8. Calculation of vancomycin dosage for morbidly obese patient
Steps Calculation
Scenario: Female/30yr, body weight 200 kg, height 1.8 m, serum creatinine 80 mol/L
Determine if the patient is morbidly obese
TBW/IBW ratio:
0.8 1.25 = normal
>1.25 1.9 = obese
>1.9 = morbid obesity
200/70.7 = 2.8
Determine dose of vancomycin
30 mg/kg TBW/day 6 g per day if normal renal function. (administer as IV 2 g q8h; infuse each 2 g dose over at least 2 h)
Estimate creatinine clearance (CrCl)
Cockcroft-Gault formula not accurate in morbidly obese patients. The Salazar-Corcoranequation appears to give the least biased estimate of CrCl
Monitor trough level Target trough at 5-10 g/mL
Adjust dosing interval according to trough level
Equations:
1. Ideal body weight (IBW)
IBW for male = 50 kg + 0.9 kg for each cm over 152 cm (2.3 kg for each inch over 5 feet)
IBW for female = 45.5kg + 0.9 kg for each cm over 152 cm (2.3 kg for each inch over 5 feet)
2. Salazar-Corcoran equation (for estimate of creatinine clearance in morbidly obese patients):
Male patient, calculate CrCl as follows:
(137 age in years) (TBW in kg 0.285) + (12.1 height in meter)
0.58 serum creatinine in mol/L
Female patient, calculate CrCl as follows:
(146 age in years) (TBW in kg 0.287) + (9.74 height in meter)
0.68 serum creatinine in mol/L
a TBW, total body weight
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 43
Quinupristin/dalfopristin and linezolid
1. Indications for linezolid (Zyvox) or quinupristin/dalfopristin (Synercid):
a. Infections by vancomycin-resistant enterococci (VRE) or S.aureus with reduced susceptibility to vancomycin (e.g. VISA)
b. Infections by methicillin-resistant Staphylococcus aureus in the case of vancomycin failure (e.g. unexplained breakthrough bacteraemia) and/or serious allergy. In these complicated circumstances, the opinion of a specialist (microbiologist or ID physician) should be sought.
2. Most VRE (n=11) identified in Hong Kong so far are susceptible to linezolid (both E. faecalis and E. faecium) at 4 g/mL and quinupristin/dalfopristin (E. faecium only, at 1 g/mL) (19).
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 44
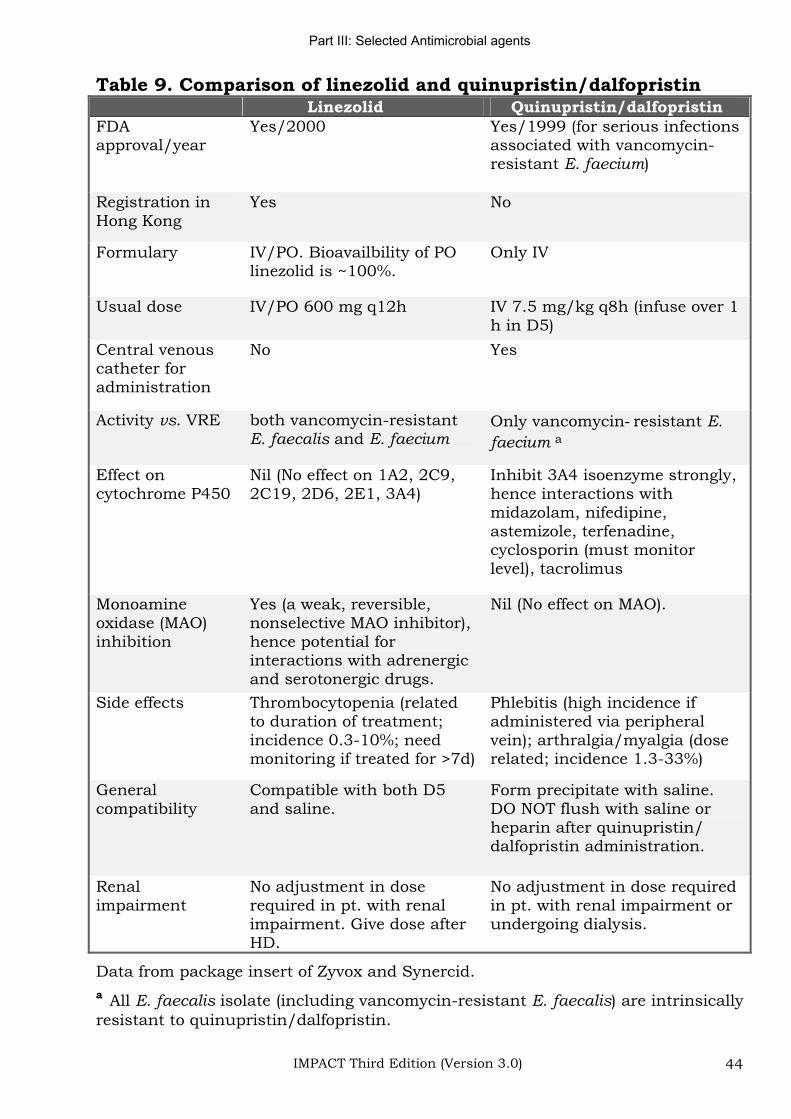
Table 9. Comparison of linezolid and quinupristin/dalfopristin Linezolid Quinupristin/dalfopristin
FDAapproval/year
Yes/2000 Yes/1999 (for serious infections associated with vancomycin-resistant E. faecium)
Registration in Hong Kong
Yes No
Formulary IV/PO. Bioavailbility of PO linezolid is ~100%.
Only IV
Usual dose IV/PO 600 mg q12h IV 7.5 mg/kg q8h (infuse over 1 h in D5)
Central venous catheter for administration
No Yes
Activity vs. VRE both vancomycin-resistant E. faecalis and E. faecium
Only vancomycin resistant E.
faecium a
Effect on cytochrome P450
Nil (No effect on 1A2, 2C9, 2C19, 2D6, 2E1, 3A4)
Inhibit 3A4 isoenzyme strongly, hence interactions with midazolam, nifedipine, astemizole, terfenadine, cyclosporin (must monitor level), tacrolimus
Monoamineoxidase (MAO) inhibition
Yes (a weak, reversible, nonselective MAO inhibitor), hence potential for interactions with adrenergic and serotonergic drugs.
Nil (No effect on MAO).
Side effects Thrombocytopenia (related to duration of treatment; incidence 0.3-10%; need monitoring if treated for >7d)
Phlebitis (high incidence if administered via peripheral vein); arthralgia/myalgia (dose related; incidence 1.3-33%)
Generalcompatibility
Compatible with both D5 and saline.
Form precipitate with saline. DO NOT flush with saline or heparin after quinupristin/ dalfopristin administration.
Renalimpairment
No adjustment in dose required in pt. with renal impairment. Give dose after HD.
No adjustment in dose required in pt. with renal impairment or undergoing dialysis.
Data from package insert of Zyvox and Synercid.
a All E. faecalis isolate (including vancomycin-resistant E. faecalis) are intrinsically resistant to quinupristin/dalfopristin.
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 45
Ceftazidime
Indications for using ceftazidime (Fortum) (127)
1. Empirical therapy of neutropenic fever, either as monotherapy or in combination with an aminoglycoside (128).
2. Therapy of infection by Burkholderia pseudomallei infection (melioidosis).
Probable case (compatible chest X-ray plus a melioidosis titre of 1/640) or definite case (isolation of B. pseudomallei).
3. Known pathogen therapy of documented infection by susceptible Pseudomonas aeruginosaa, such as:
(a) Bacteraemia with isolation of Pseudomonas aeruginosa fromblood culture.
(b) Deep-seated infection with isolation of Pseudomonas aeruginosa from normally sterile body site or fluid (CSF,
peritoneal fluid, pleural fluid, joint fluid, tissue, pus, etc) a.
(c) Nosocomial pneumonia, as defined by CDC guidelines (appendix), with isolation of Pseudomonas aeruginosa in a significant quantity, from a suitably obtained, good quality
respiratory tract specimenb.
Footnotes
a For serious P. aeruginosa infection, an anti-pseudomonal beta-lactam should be given in combination with an aminoglycoside such as gentamicin given once daily for the initial 3 to 5 days to achieve synergistic killing. For susceptible isolates; anti-pseudomonal beta-lactams in decreasing order of preference: piperacillin or piperacillin-tazobactam or ticarcillin-clavulanate > cefoperazone or cefoperazone-sulbactam or cefepime or ceftazidime > imipenem or meropenem.
b Colonization of the respiratory tract by P. aeruginosa, especially in mechanically ventilated patients is common. Antimicrobial therapy of colonization is not indicated. Isolation of P. aeruginosa at the indicated quantity and specimen type is suggestive of infection rather than colonization (in descending order of clinical significance):
1. 102-103CFU/mL or moderate/heavy growth for protected specimen brush.
2. 103-104 CFU/mL or moderate/heavy growth for bronchoalveolar lavage.
3. Moderate/heavy growth for tracheal/endotracheal aspirate specimens with ++ to +++ white cells and absent/scanty epithelial cells.
4. Expectorated sputum (as defined by the American Society for Microbiology) with >25 WBC/low power field and <10 epithelial cells/low power field.
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 46
Situations/conditions in which ceftazidime is not advised
1. Treatment of colonization by Pseudomonas aeruginosa such as the isolation of these organisms from
Surface swab of superficial wounds
Surface swab of chronic ulcers
Surface swab of pressure ulcers
2. Empirical or continued treatment of suspected or confirmed infection by S. pneumoniae including bacteraemia, pneumonia and meningitis.
Infection outside the central nervous system by both penicillin-susceptible and penicillin-non-susceptible (MIC <4 g/mL), the drugs of choice are penicillin G (standard or high dose) or amoxicillin or cefotaxime or ceftriaxone (refer to known-pathogen therapy chart).
3. Empirical or continued treatment of infection by Enterobacteriaceae such as E. coli and Klebsiella spp. susceptible to other antimicrobial agents.
For susceptible isolates the beta-lactam of choice in descending order of preference are as follows: ampicillin or amoxicillin > ampicillin-sulbactam or amoxicillin-clavulanate > cefuroxime > ceftriaxone or cefotaxime.
4. Empirical therapy of community-acquired pneumonia, including patients hospitalized in the ICU for serious pneumonia and patients with structural disease of the lung (adapted from Infectious Disease Society of America 1998).
Other agents with activity vs. P. aeruginosa and S. pneumoniae preferred because ceftazidime (while active vs. P. aeruginosa) is not useful vs. penicillin-non-susceptible S. pneumoniae.
5. Empirical or continued treatment of anaerobic or mixed infection in the head and neck, biliary, pancreatic, gastrointestinal, peritoneal, pelvic or peritoneal regions.
Ceftazidime has virtually no activity against most of the medically important anaerobes.
6. Empirical or continued treatment of patients with colonization or infection by Enterobacteriaceae such as E. coli, Klebsiella spp. and Enterobacter spp. known to produce ESBL.
Applies irrespective of whether ceftazidime was tested or not and also irrespective of the apparent in vitro susceptibility of the isolate to ceftazidime.
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 47
7. Empirical or continued treatment of infection by S. aureus (both MSSA and MRSA).
8. Empirical or continued treatment of infection by all enterococci such as E. faecalis and E. faecium.
9. Empirical treatment for community-acquired meningitis.
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 48
Imipienem/meropenem/ertapenem
Indications for using imipenem/meropenem/ertapenem
1. Therapy of infections attributed to ESBL-producing bacteria (such as E. coli or Klebsiella spp. ) such as:
Bacteraemia with isolation of ESBL-producing bacteria from blood culture.
Deep-seated infection with isolation of ESBL-producing bacteria from normally sterile body site or fluid (CSF, peritoneal fluid, pleural fluid, joint fluid, tissue, pus, etc).
Nosocomial pneumonia, as defined by CDC guidelines, with isolation of ESBL-producing bacteria in a significant quantity, from a suitably obtained, good quality respiratory tract specimensa
2. Empirical therapy of neutropenic fever in high risk patients. (As Ertapenem has no anti-pseudomonal activity, it should not be used as empirical therapy for neutropenic fevers or for treatment of presumed/confirmed infections by the non-fermenters such as Pseudomonas aeruginosa and Acinetobacter.)
Footnotes
a Colonization of the respiratory tract by ESBL-producing bacteria, especially in mechanically ventilated patients is common. Antimicrobial therapy of colonization is not indicated. Isolation of ESBL-producing bacteria at the indicated quantity and specimen type is suggestive of infection rather than colonization (in descending order of clinical significance):
1. 102-103 CFU/mL or moderate/heavy growth for protected specimen brush.
2. 103-104 CFU/mL or moderate/heavy growth for bronchoalveolar lavage.
3. Moderate/heavy growth for tracheal/endotracheal aspirate specimens with ++ to +++ white cells and absent/scanty epithelial cells.
4. Expectorated sputum (as defined by the American Society for Microbiology)
with >25 WBC/low power field and <10 epithelial cells/low power field.
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 49
Situations/conditions in which imipenem/meropenem/ertapenem is not advised
1. Treatment of colonization by ESBL-producing bacteria such as the isolation of these organisms from.
Surface swab of superficial wounds
Surface swab of chronic ulcers
Surface swab of pressure ulcers
2. Empirical therapy of most community-acquired infections including pneumonia, appendicitis, cholecystitis, cholangitis, primary peritonitis, peritonitis secondary to perforation of stomach, duodenum or colon, skin/soft tissue infections, etc.
3. As known-pathogen therapy for infections caused by organisms susceptible to other beta-lactams.
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 50
Once daily aminoglycosides
1. Once daily aminoglycoside (ODA) dosing is as effective as multiple-daily dosing in most clinical settings. The former dosing probably results in a lower risk of nephrotoxicity than the latter. With ODA, any differences in the relative nephrotoxicity of the aminoglycosides are likely to be small. Nonetheless, there is considerable confusion on the dose and how to monitor serum aminoglycoside levels when using ODA dosing.
2. Dosing to be based on actual body weight unless the patient is morbidly obese (i.e. 20% over ideal body weight, IBW).
Aminoglycoside dosing weight for morbidly obsess patient
= ideal body weight + 0.4 (actual body weight - IBW).
Formula for calculation of ideal body weight is as follows:
Ideal body weight for male = 50 kg + 0.9 kg for each cm over 152 cm (2.3 kg for each inch over 5 feet)
Ideal body weight for female = 45.5 kg + 0.9 kg for each cm over 152 cm (2.3 kg for each inch over 5 feet)
3. For patient with impaired renal function, give the first dose according to body weight as above. Subsequent frequency of administration (of the same dose) to be based on the estimated creatinine clearance of the patient according to the following table.
Cockcroft-Gault formula
To estimate creatinine clearance, calculate as follows
Creatine clearance for male patient (mL/min) = (140-age) x 1.2 x ideal body weight (kg) /serum creatinine ( mol/L)
(Female: 0.85 above value)
(Unit conversion for serum creatinine: mg/dL x 88.4 = mol/L)
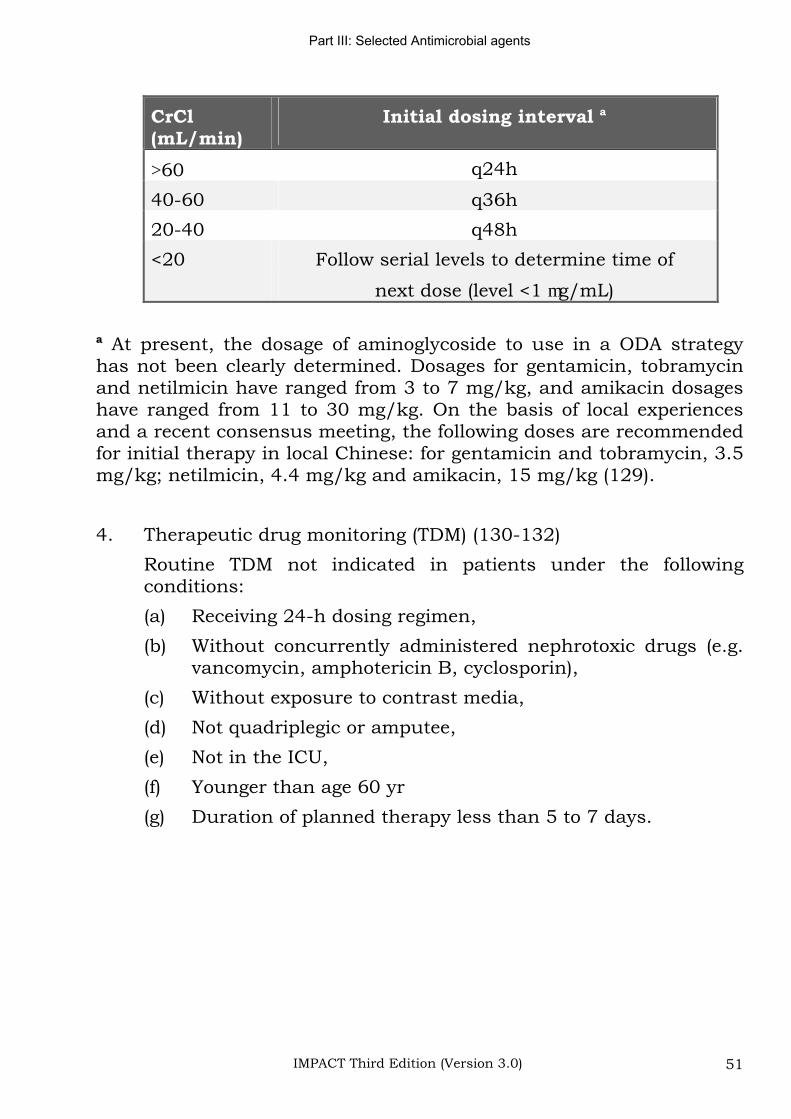
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 51
CrCl (mL/min)
Initial dosing interval a
60 q24h
40-60 q36h
20-40 q48h
<20 Follow serial levels to determine time of
next dose (level <1 g/mL)
a At present, the dosage of aminoglycoside to use in a ODA strategy has not been clearly determined. Dosages for gentamicin, tobramycin and netilmicin have ranged from 3 to 7 mg/kg, and amikacin dosages have ranged from 11 to 30 mg/kg. On the basis of local experiences and a recent consensus meeting, the following doses are recommended for initial therapy in local Chinese: for gentamicin and tobramycin, 3.5 mg/kg; netilmicin, 4.4 mg/kg and amikacin, 15 mg/kg (129).
4. Therapeutic drug monitoring (TDM) (130-132)
Routine TDM not indicated in patients under the following conditions:
(a) Receiving 24-h dosing regimen,
(b) Without concurrently administered nephrotoxic drugs (e.g. vancomycin, amphotericin B, cyclosporin),
(c) Without exposure to contrast media,
(d) Not quadriplegic or amputee,
(e) Not in the ICU,
(f) Younger than age 60 yr
(g) Duration of planned therapy less than 5 to 7 days.
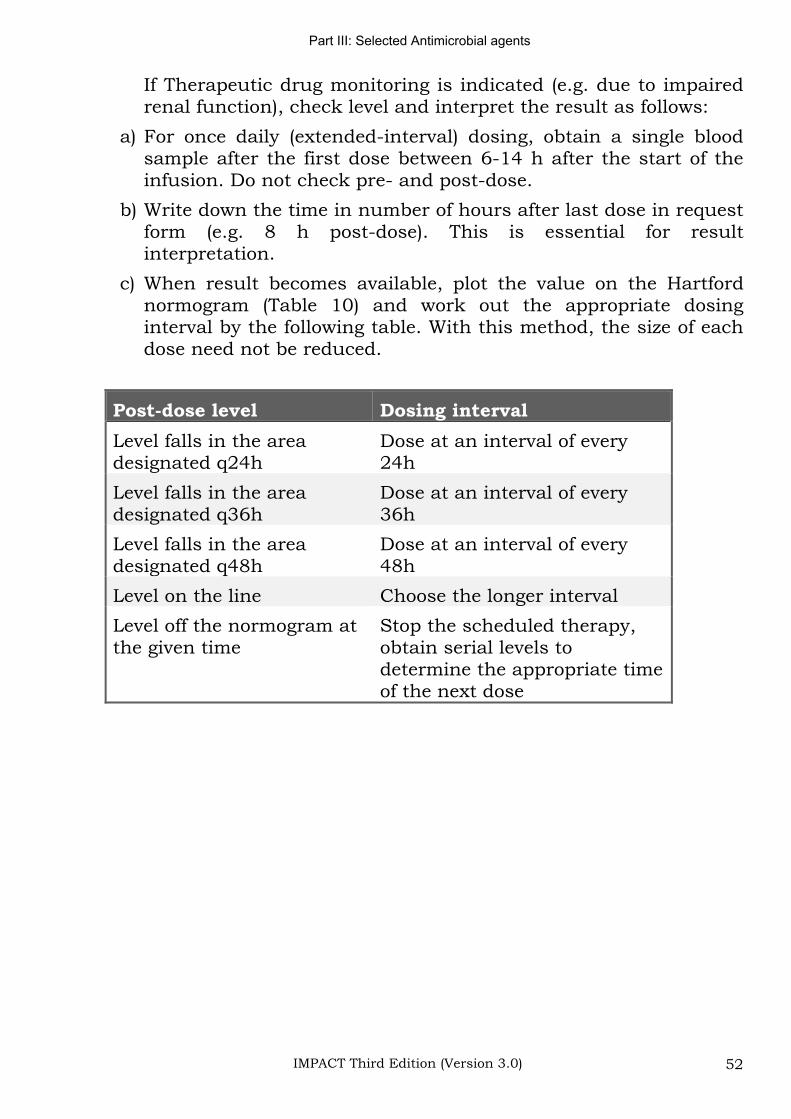
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 52
If Therapeutic drug monitoring is indicated (e.g. due to impaired renal function), check level and interpret the result as follows:
a) For once daily (extended-interval) dosing, obtain a single blood sample after the first dose between 6-14 h after the start of the infusion. Do not check pre- and post-dose.
b) Write down the time in number of hours after last dose in request form (e.g. 8 h post-dose). This is essential for result interpretation.
c) When result becomes available, plot the value on the Hartford normogram (Table 10) and work out the appropriate dosing interval by the following table. With this method, the size of each dose need not be reduced.
Post-dose level Dosing interval
Level falls in the area designated q24h
Dose at an interval of every 24h
Level falls in the area designated q36h
Dose at an interval of every 36h
Level falls in the area designated q48h
Dose at an interval of every 48h
Level on the line Choose the longer interval
Level off the normogram at the given time
Stop the scheduled therapy, obtain serial levels to determine the appropriate time of the next dose
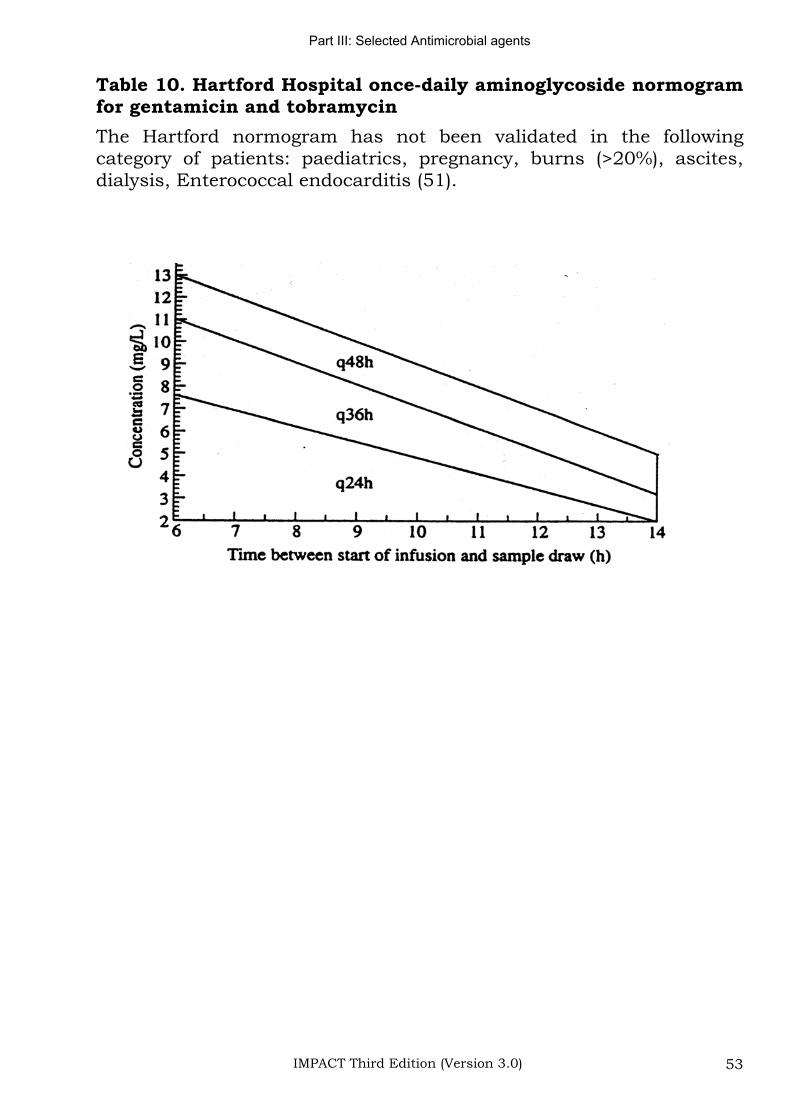
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 53
Table 10. Hartford Hospital once-daily aminoglycoside normogram for gentamicin and tobramycin
The Hartford normogram has not been validated in the following category of patients: paediatrics, pregnancy, burns (>20%), ascites, dialysis, Enterococcal endocarditis (51).
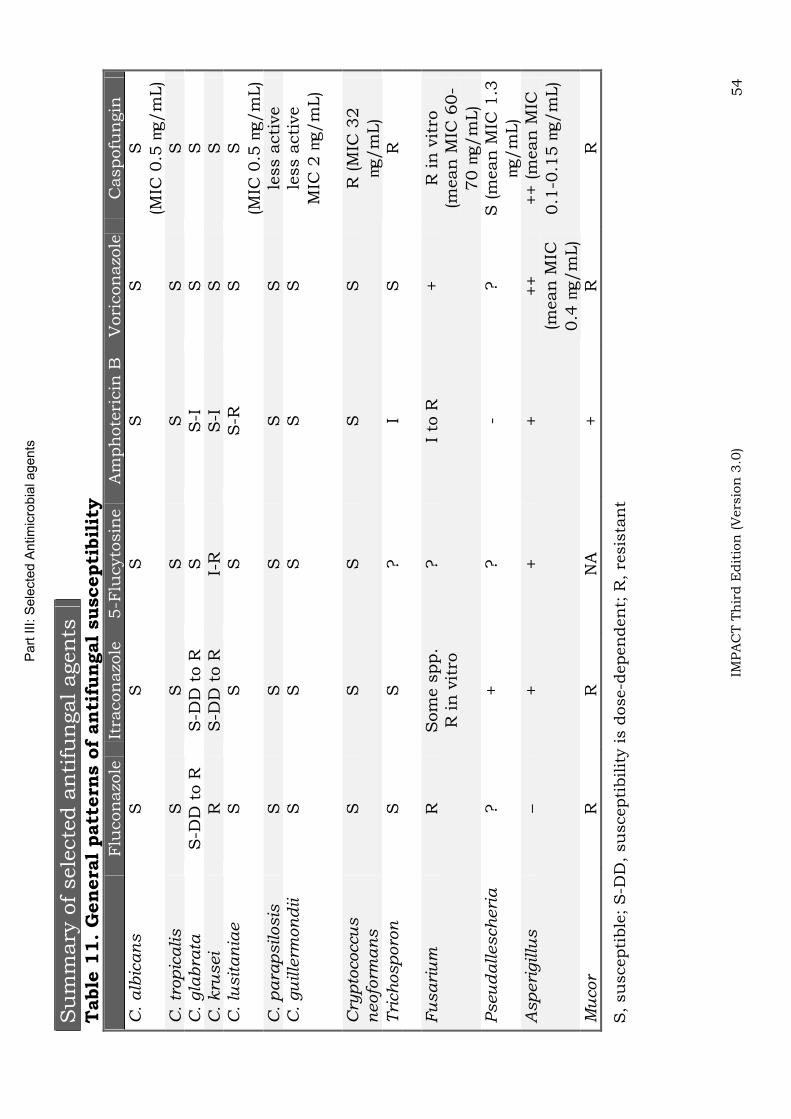
Part
III:
Sele
cte
d A
ntim
icro
bia
l agents
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 54
Su
mm
ary
of sele
cte
d a
nti
fun
gal agen
tsT
able
11.
Gen
era
l patt
ern
s o
f an
tifu
ngal
suscepti
bil
ity
Flu
con
azo
le
Itra
con
azo
le5-F
lucyto
sin
eA
mph
ote
ricin
B
Vori
con
azo
leC
aspofu
ngin
C.
alb
ican
s
S
S
S
S
S
S
(MIC
0.5
g/m
L)
C.
trop
icalis
SS
SS
SS
C.
gla
bra
ta
S-D
D t
o R
S
-DD
to R
S
S
-I
S
S
C. kru
sei
RS
-DD
to R
I-
RS
-IS
SC
. lu
sit
an
iae
S
S
S
S-R
S
S
(M
IC 0
.5
g/m
L)
C. p
ara
psilosis
S
SS
SS
less a
cti
ve
C.
gu
ille
rmon
dii
S
S
S
S
S
less a
cti
ve
MIC
2
g/m
L)
Cry
pto
coccu
s
neofo
rma
ns
SS
SS
SR
(M
IC 3
2
g/m
L)
Tri
ch
osp
oro
n
S
S
?
I S
R
F
usari
um
R
Som
e s
pp.
R in
vit
ro
?I
to R
+
R in
vit
ro
(mean
MIC
60-
70
g/m
L)
Pseu
dallesch
eri
a
?
+
?
- ?
S (m
ean
MIC
1.3
g/m
L)
Asp
eri
gillu
s
–+
++
++
(mean
MIC
0.4
g/m
L)
++ (m
ean
MIC
0.1
-0.1
5g/m
L)
Mu
cor
R
R
NA
+
R
R
S,
su
scepti
ble
; S
-DD
, su
scepti
bilit
y is d
ose-d
epen
den
t; R
, re
sis
tan
t
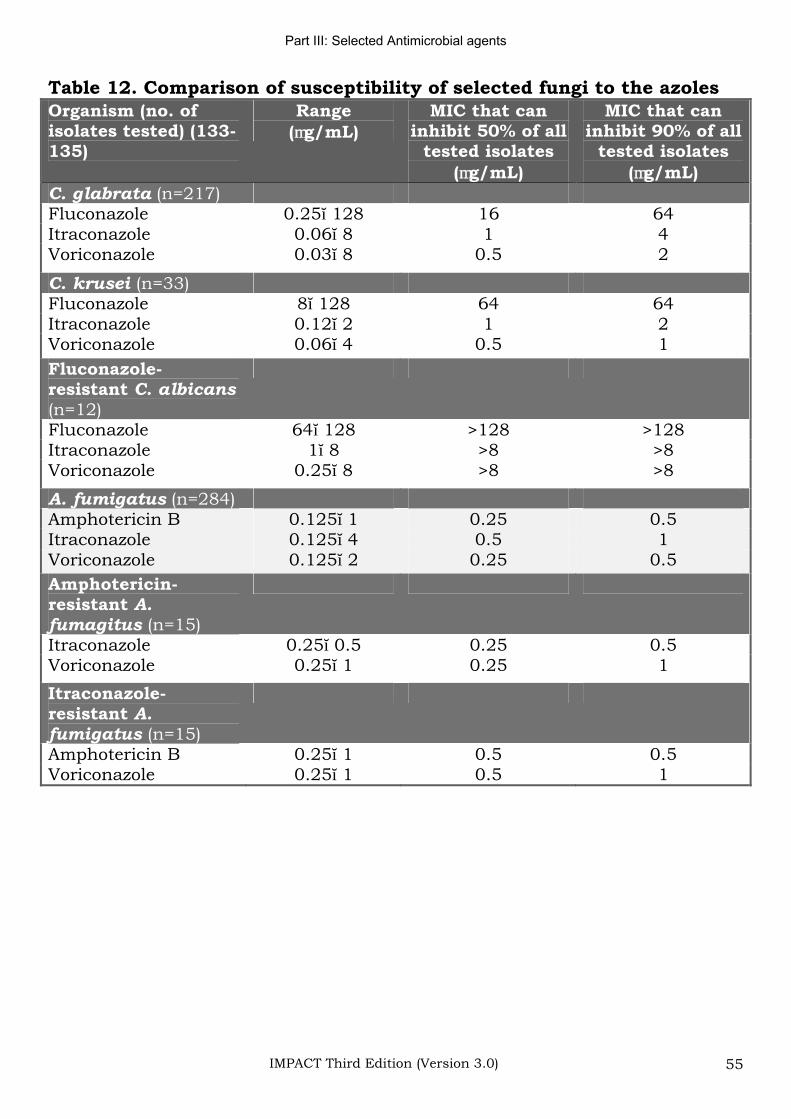
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 55
Table 12. Comparison of susceptibility of selected fungi to the azoles Organism (no. of isolates tested) (133-135)
Range( g/mL)
MIC that can inhibit 50% of all
tested isolates ( g/mL)
MIC that can inhibit 90% of all
tested isolates ( g/mL)
C. glabrata (n=217) Fluconazole 0.25 128 16 64 Itraconazole 0.06 8 1 4 Voriconazole 0.03 8 0.5 2
C. krusei (n=33)Fluconazole 8 128 64 64 Itraconazole 0.12 2 1 2 Voriconazole 0.06 4 0.5 1
Fluconazole-resistant C. albicans (n=12)Fluconazole 64 128 >128 >128 Itraconazole 1 8 >8 >8 Voriconazole 0.25 8 >8 >8
A. fumigatus (n=284) Amphotericin B 0.125 1 0.25 0.5Itraconazole 0.125 4 0.5 1Voriconazole 0.125 2 0.25 0.5
Amphotericin-resistant A. fumagitus (n=15) Itraconazole 0.25 0.5 0.25 0.5 Voriconazole 0.25 1 0.25 1
Itraconazole-resistant A.fumigatus (n=15) Amphotericin B 0.25 1 0.5 0.5 Voriconazole 0.25 1 0.5 1
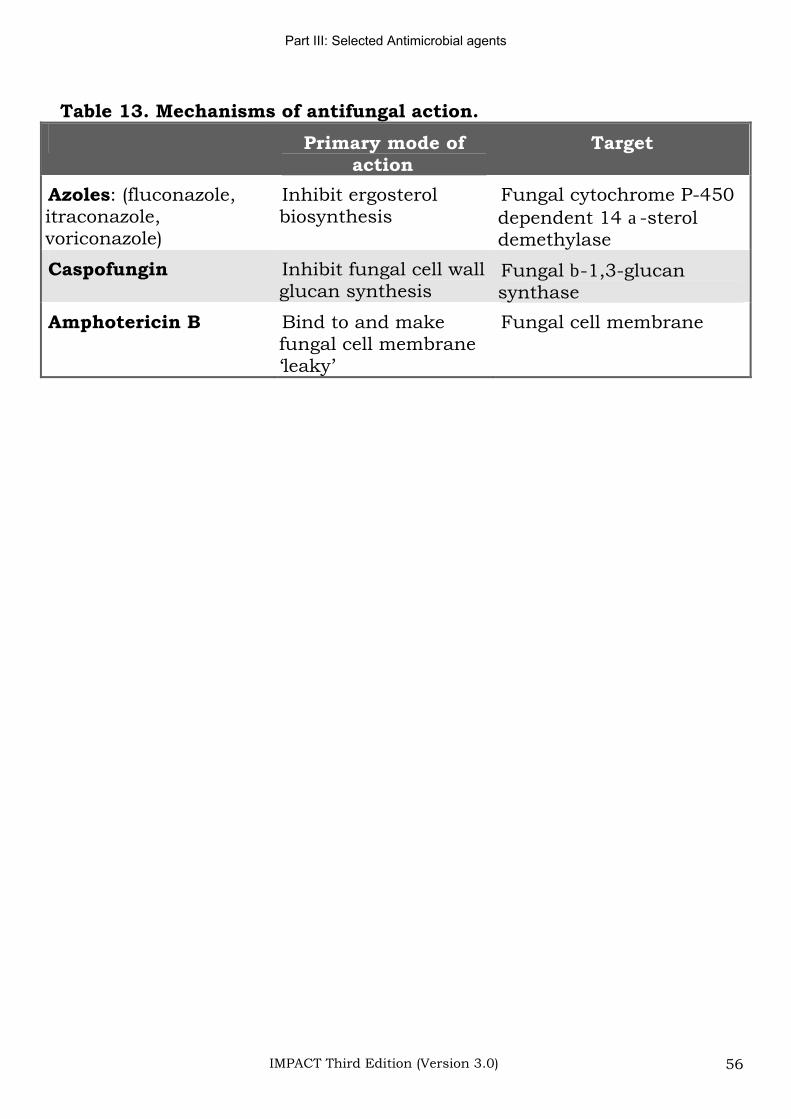
Part III: Selected Antimicrobial agents
IMPACT Third Edition (Version 3.0) 56
Table 13. Mechanisms of antifungal action.
Primary mode of action
Target
Azoles: (fluconazole, itraconazole,voriconazole)
Inhibit ergosterol biosynthesis
Fungal cytochrome P-450 dependent 14 -steroldemethylase
Caspofungin Inhibit fungal cell wall glucan synthesis
Fungal -1,3-glucansynthase
Amphotericin B Bind to and make fungal cell membrane ‘leaky’
Fungal cell membrane
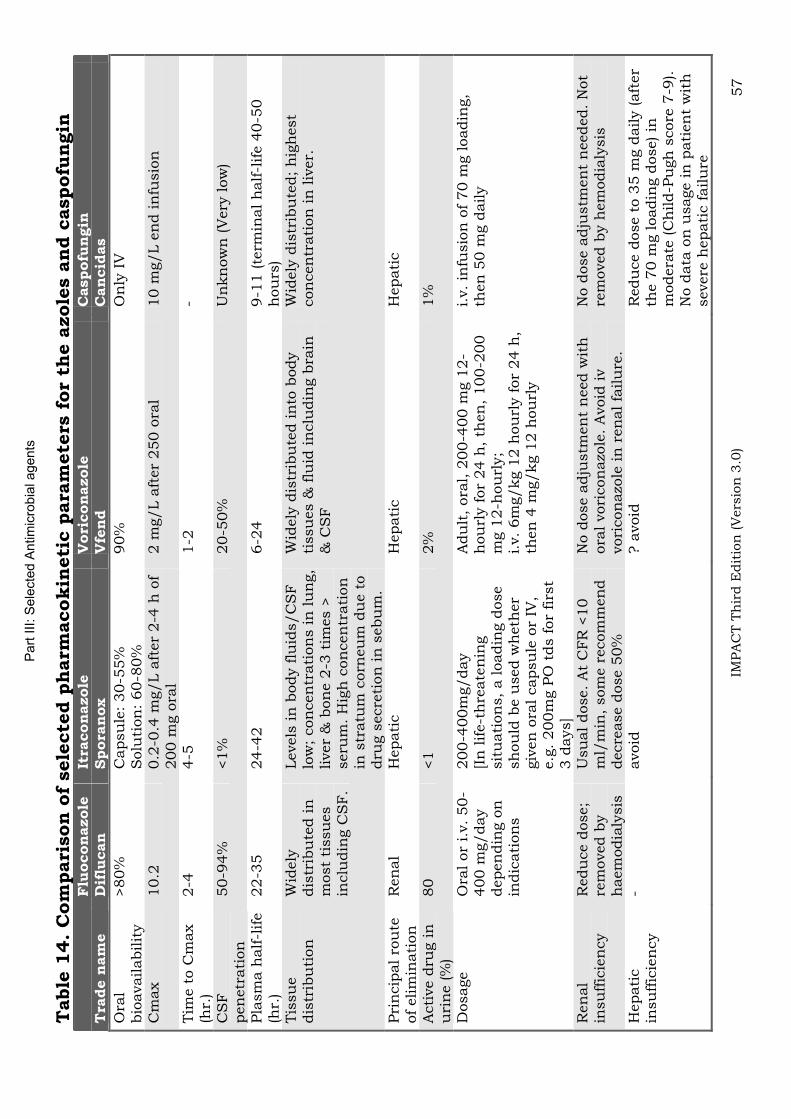
Part
III:
Sele
cte
d A
ntim
icro
bia
l agents
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 57
Table
14.
Com
pari
son
of
sele
cte
d p
harm
acokin
eti
c p
ara
mete
rs f
or
the a
zole
s a
nd c
aspofu
ngin
Flu
oconazole
It
racon
azole
V
ori
con
azole
Caspofu
ngin
T
rade n
am
e
Dif
lucan
Spora
nox
Vfe
nd
Cancid
as
Ora
lbio
availabilit
y
>80%
C
apsu
le:
30-5
5%
S
olu
tion
: 60-8
0%
90%
O
nly
IV
Cm
ax
10.2
0.2
-0.4
mg/L a
fter
2-4
h o
f 200 m
g o
ral
2 m
g/L a
fter
250 o
ral
10 m
g/L e
nd in
fusio
n
Tim
e t
o C
max
(hr.
)2-4
4-5
1-2
-
CS
Fpen
etr
ati
on
50-9
4%
<1%
20-5
0%
U
nkn
ow
n (V
ery
low
)
Pla
sm
a h
alf-l
ife
(hr.
)22-3
5
24-4
2
6-2
4
9-1
1 (te
rmin
al h
alf-l
ife 4
0-5
0
hou
rs)
Tis
su
e
dis
trib
uti
on
W
idely
dis
trib
ute
d in
m
ost
tissu
es
inclu
din
g C
SF
.
Levels
in
body f
luid
s/C
SF
lo
w;
con
cen
trati
on
s in
lu
ng,
liver
& b
on
e 2
-3 t
imes >
seru
m.
Hig
h c
on
cen
trati
on
in
str
atu
m c
orn
eu
m d
ue t
o
dru
g s
ecre
tion
in
sebu
m.
Wid
ely
dis
trib
ute
d in
to b
ody
tissu
es &
flu
id in
clu
din
g b
rain
&
CS
F
Wid
ely
dis
trib
ute
d;
hig
hest
con
cen
trati
on
in
liv
er.
Pri
ncip
al ro
ute
of
elim
inati
on
R
en
al
Hepati
c
Hepati
c
Hepati
c
Acti
ve d
rug in
u
rin
e (%
) 80
<1
2%
1%
Dosage
Ora
l or
i.v. 50-
400 m
g/day
depen
din
g o
n
indic
ati
on
s
200-4
00m
g/day
[In
life-t
hre
ate
nin
g
sit
uati
on
s,
a loadin
g d
ose
sh
ou
ld b
e u
sed w
heth
er
giv
en
ora
l capsu
le o
r IV
, e.g
. 200m
g P
O t
ds f
or
firs
t 3 d
ays]
Adu
lt,
ora
l, 2
00-4
00 m
g 1
2-
hou
rly f
or
24 h
, th
en
, 100-2
00
mg 1
2-h
ou
rly;
i.v.
6m
g/kg 1
2 h
ou
rly f
or
24 h
, th
en
4 m
g/kg 1
2 h
ou
rly
i.v.
infu
sio
n o
f 70 m
g loadin
g,
then
50 m
g d
aily
Ren
al
insu
ffic
ien
cy
Redu
ce d
ose;
rem
oved b
y
haem
odia
lysis
Usu
al dose.
At
CFR
<10
ml/
min
, som
e r
ecom
men
d
decre
ase d
ose 5
0%
No d
ose a
dju
stm
en
t n
eed w
ith
ora
l vori
con
azo
le.
Avoid
iv
vori
con
azo
le in
ren
al fa
ilu
re.
No d
ose a
dju
stm
en
t n
eeded.
Not
rem
oved b
y h
em
odia
lysis
Hepati
c
insu
ffic
ien
cy
- avoid
? a
void
R
edu
ce d
ose t
o 3
5 m
g d
aily (aft
er
the 7
0 m
g loadin
g d
ose) in
m
odera
te (C
hild-P
ugh
score
7-9
).
No d
ata
on
usage in
pati
en
t w
ith
severe
hepati
c f
ailu
re
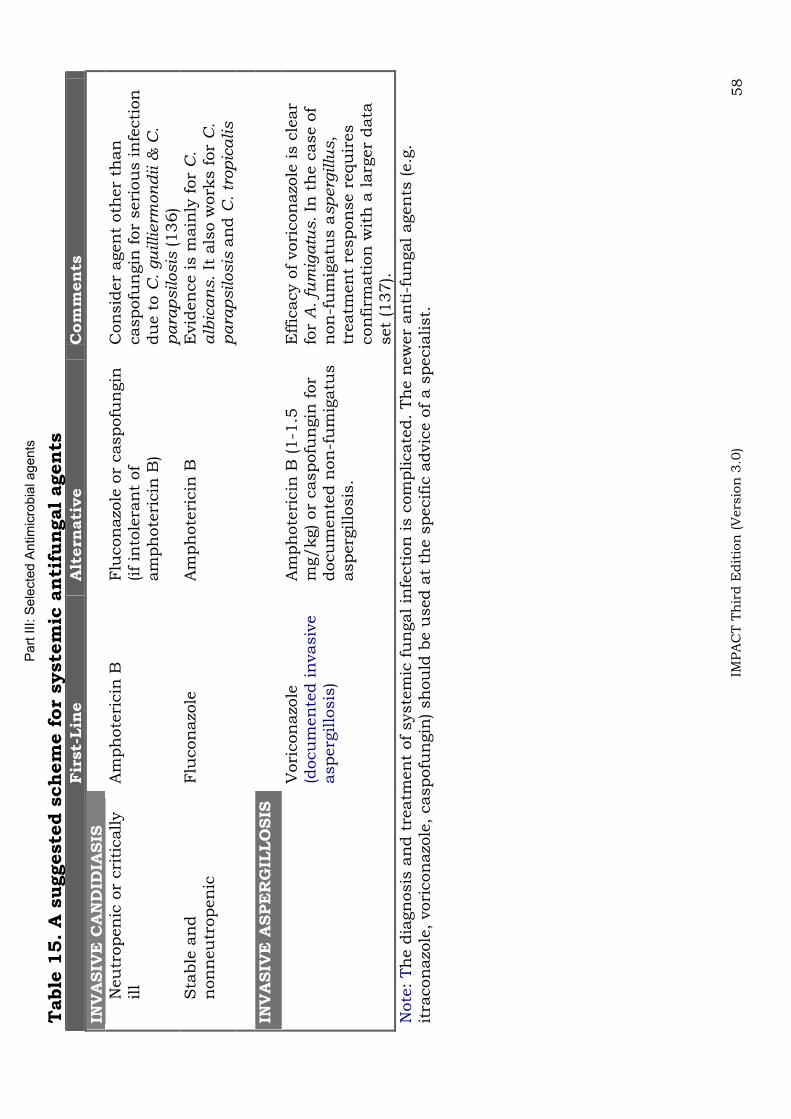
Part
III:
Sele
cte
d A
ntim
icro
bia
l agents
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 58
Table
15.
A s
uggeste
d s
ch
em
e f
or
syste
mic
an
tifu
ngal
agen
ts
Fir
st-
Lin
eA
ltern
ati
ve
Com
men
ts
INV
ASIV
E C
AN
DID
IASIS
Neu
tropen
ic o
r cri
tically
ill
Am
ph
ote
ricin
B
Flu
con
azo
le o
r caspofu
ngin
(if
into
lera
nt
of
am
ph
ote
ricin
B)
Con
sid
er
agen
t oth
er
than
caspofu
ngin
for
seri
ou
s in
fecti
on
du
e t
o C
. gu
illierm
on
dii &
C.
para
psilosis
(136)
Sta
ble
an
d
non
neu
tropen
icFlu
con
azo
le
Am
ph
ote
ricin
B
Evid
en
ce is m
ain
ly f
or
C.
alb
ican
s.
It a
lso w
ork
s f
or
C.
para
psilosis
an
dC
. tr
op
icalis
INV
ASIV
E A
SPE
RG
ILLO
SIS
Vori
con
azo
le(d
ocu
men
ted in
vasiv
e
asperg
illo
sis
)
Am
ph
ote
ricin
B (1-1
.5
mg/kg) or
caspofu
ngin
for
docu
men
ted n
on
-fu
mig
atu
s
asperg
illo
sis
.
Effic
acy o
f vori
con
azo
le is c
lear
for
A. fu
mig
atu
s. In
th
e c
ase o
f n
on
-fu
mig
atu
s a
sp
erg
illu
s,
treatm
en
t re
spon
se r
equ
ires
con
firm
ati
on
wit
h a
larg
er
data
set
(137).
Note
: Th
e d
iagn
osis
an
d t
reatm
en
t of
syste
mic
fu
ngal in
fecti
on
is c
om
plicate
d.
Th
e n
ew
er
an
ti-f
un
gal agen
ts (e.g
. it
racon
azo
le,
vori
con
azo
le,
caspofu
ngin
) sh
ou
ld b
e u
sed a
t th
e s
pecific
advic
e o
f a s
pecia
list.

Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 59
Part IV: Recommendation for the empirical therapy of common infections
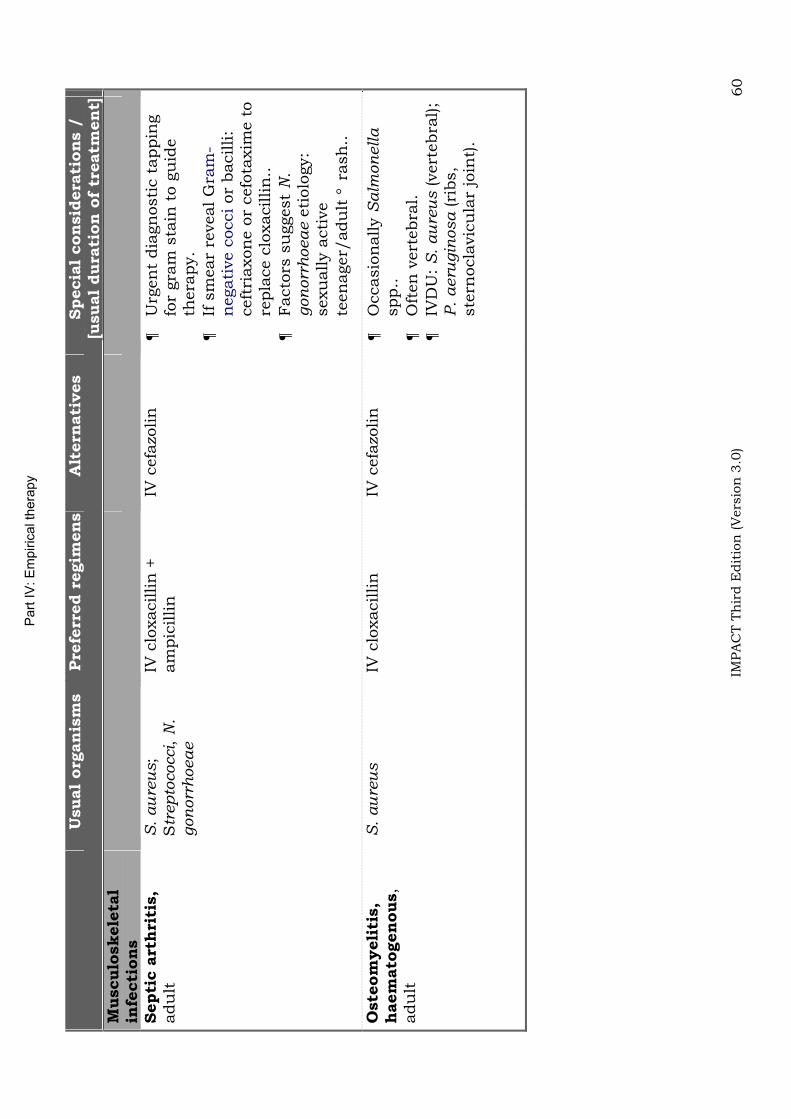
Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 60
Usual
org
an
ism
s
Pre
ferr
ed r
egim
en
sA
ltern
ati
ves
Specia
l con
sid
era
tion
s /
[u
sual
dura
tion
of
treatm
en
t]
Musculo
skele
tal
infe
cti
on
sSepti
c a
rth
riti
s,
adu
ltS
. au
reu
s;
Str
ep
tococci,
N.
gon
orr
hoea
e
IV c
loxacillin
+
am
pic
illin
IV c
efa
zolin
U
rgen
t dia
gn
osti
c t
appin
g
for
gra
m s
tain
to g
uid
e
thera
py.
If s
mear
reveal G
ram
-n
egati
ve c
occi or
bacilli:
ceft
riaxon
e o
r cefo
taxim
e t
o
repla
ce c
loxacillin
..
Facto
rs s
uggest
N.
gon
orr
hoea
e e
tiolo
gy:
sexu
ally a
cti
ve
teen
ager/
adu
lt r
ash
..
Oste
om
yeli
tis,
haem
ato
gen
ous,
adu
lt
S.
au
reu
sIV
clo
xacillin
IV c
efa
zolin
Occasio
nally
Salm
on
ella
spp..
Oft
en
vert
ebra
l.
IVD
U:
S.
au
reu
s (vert
ebra
l);
P.
aeru
gin
osa (ri
bs,
ste
rnocla
vic
ula
r jo
int)
.
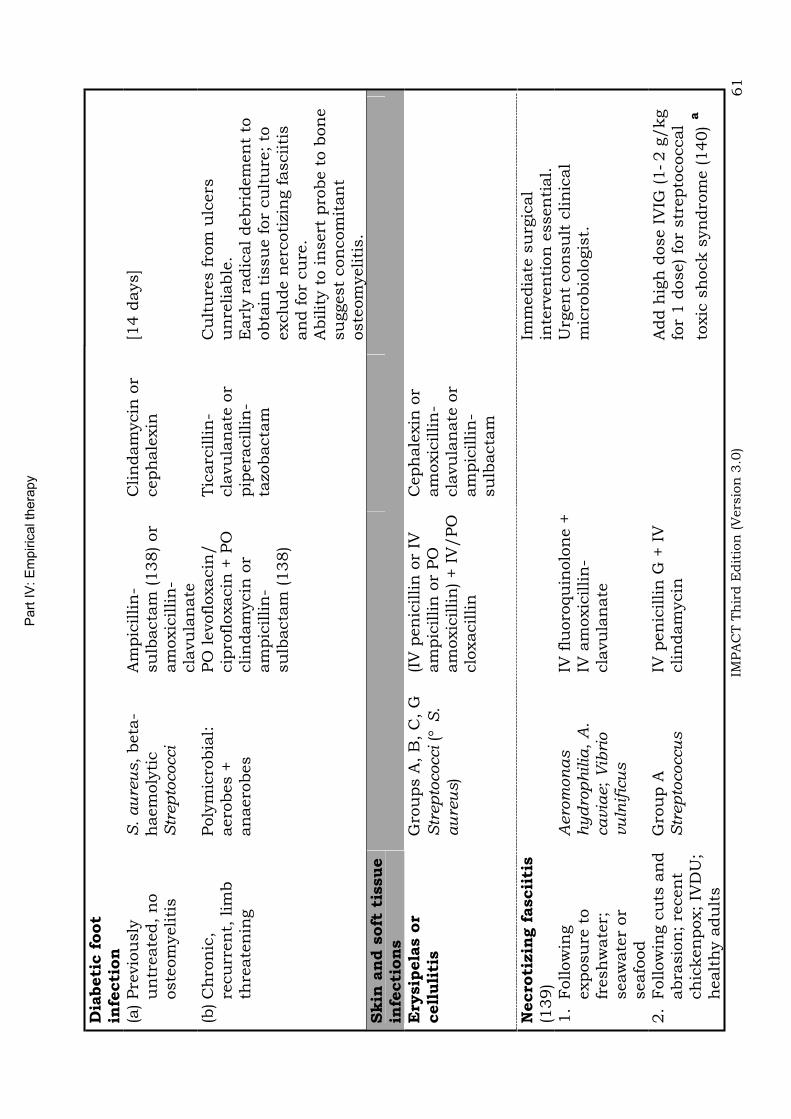
Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 61
Dia
beti
c f
oot
infe
cti
on
(a) Pre
vio
usly
u
ntr
eate
d,
no
oste
om
yeliti
s
S.
au
reu
s,
beta
-h
aem
oly
tic
Str
ep
tococci
Am
pic
illin
-su
lbacta
m (138) or
am
oxic
illin
-cla
vu
lan
ate
Clin
dam
ycin
or
ceph
ale
xin
[14 d
ays]
(b) C
hro
nic
, re
cu
rren
t, lim
b
thre
ate
nin
g
Poly
mic
robia
l:aero
bes +
an
aero
bes
PO
levofloxacin
/
cip
rofloxacin
+ P
O
clin
dam
ycin
or
am
pic
illin
-su
lbacta
m (138)
Tic
arc
illin
-cla
vu
lan
ate
or
pip
era
cillin
-ta
zobacta
m
Cu
ltu
res f
rom
ulc
ers
u
nre
liable
.E
arl
y r
adic
al debri
dem
en
t to
obta
in t
issu
e f
or
cu
ltu
re;
to
exclu
de n
erc
oti
zin
g f
asciiti
s
an
d f
or
cu
re.
Abilit
y t
o in
sert
pro
be t
o b
on
e
su
ggest
con
com
itan
t oste
om
yeliti
s.
Skin
an
d s
oft
tis
sue
infe
cti
on
sE
rysip
ela
s o
r cell
uli
tis
Gro
ups A
, B
, C
, G
S
trep
tococci (
S.
au
reu
s)
(IV
pen
icillin
or
IV
am
pic
illin
or
PO
am
oxic
illin
) + I
V/PO
clo
xacillin
Ceph
ale
xin
or
am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m
Necro
tizin
g f
ascii
tis
(139)
Im
media
te s
urg
ical
inte
rven
tion
essen
tial.
1.
Follow
ing
exposu
re t
o
fresh
wate
r;seaw
ate
r or
seafo
od
Aero
mon
as
hyd
roph
ilia
,A
.cavia
e;
Vib
rio
vu
lnif
icu
s
IV f
luoro
qu
inolo
ne +
IV
am
oxic
illin
-cla
vu
lan
ate
U
rgen
t con
su
lt c
lin
ical
mic
robio
logis
t.
2.
Follow
ing c
uts
an
d
abra
sio
n;
recen
t ch
icken
pox;
IVD
U;
healt
hy a
du
lts
Gro
up A
S
trep
tococcu
sIV
pen
icillin
G +
IV
clin
dam
ycin
Add h
igh
dose I
VIG
(1
2 g
/kg
for
1 d
ose) fo
r str
epto
coccal
toxic
sh
ock s
yn
dro
me (140)
a
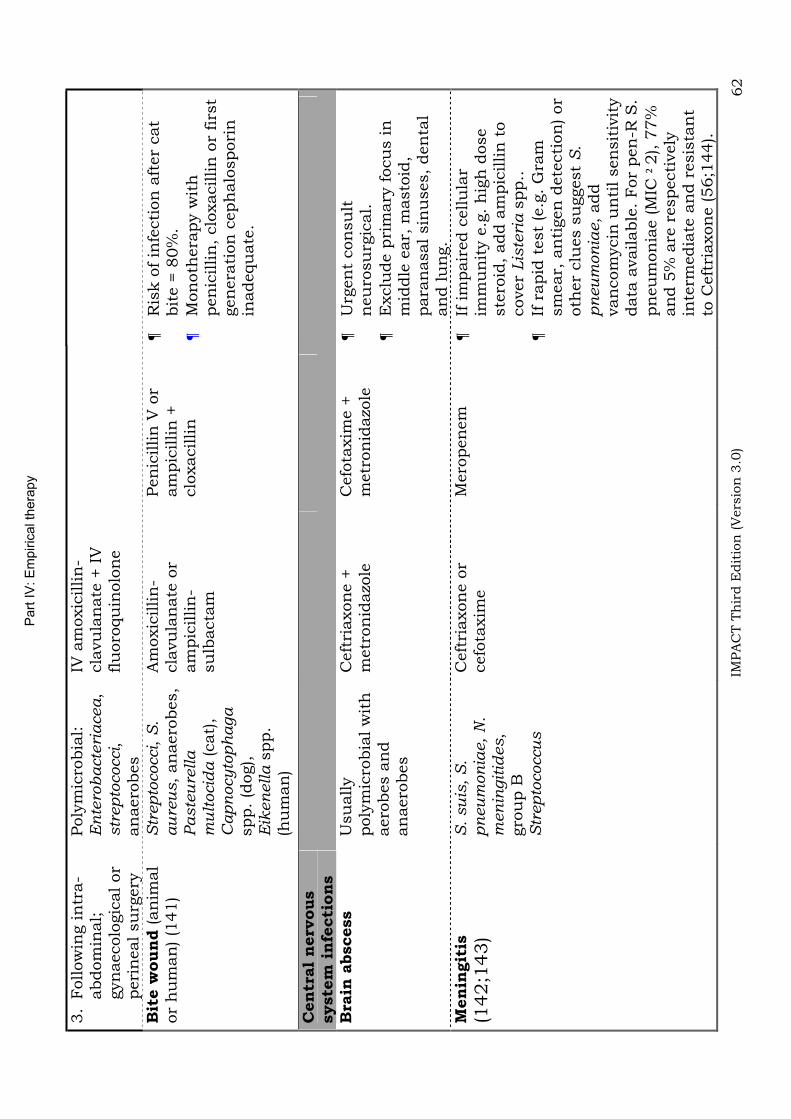
Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 62
3.
Follow
ing in
tra-
abdom
inal;
gyn
aecolo
gic
al or
peri
neal su
rgery
Poly
mic
robia
l:E
nte
rob
acte
riacea,
str
ep
tococci,
an
aero
bes
IV a
moxic
illin
-cla
vu
lan
ate
+ I
V
flu
oro
qu
inolo
ne
Bit
e w
ound
(an
imal
or
hu
man
) (1
41)
Str
ep
tococci,
S.
au
reu
s,
an
aero
bes,
Paste
ure
lla
m
ult
ocid
a (cat)
, C
ap
nocy
top
haga
spp.
(dog),
Eik
en
ella s
pp.
(hu
man
)
Am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m
Pen
icillin
V o
r am
pic
illin
+
clo
xacillin
Ris
k o
f in
fecti
on
aft
er
cat
bit
e =
80%
. M
on
oth
era
py w
ith
pen
icillin
, clo
xacillin
or
firs
t gen
era
tion
ceph
alo
spori
n
inadequ
ate
.
Cen
tral
nerv
ous
syste
m i
nfe
cti
on
s
Bra
in a
bscess
Usu
ally
poly
mic
robia
l w
ith
aero
bes a
nd
an
aero
bes
Ceft
riaxon
e +
m
etr
on
idazo
leC
efo
taxim
e +
m
etr
on
idazo
leU
rgen
t con
su
lt
neu
rosu
rgic
al.
Exclu
de p
rim
ary
focu
s in
m
iddle
ear,
masto
id,
para
nasal sin
uses,
den
tal
an
d lu
ng.
Men
ingit
is
(142;1
43)
S.
su
is,
S.
pn
eu
mon
iae,
N.
men
ingit
ides,
gro
up B
S
trep
tococcu
s
Ceft
riaxon
e o
r cefo
taxim
eM
ero
pen
em
If im
pair
ed c
ellu
lar
imm
un
ity e
.g.
hig
h d
ose
ste
roid
, add a
mpic
illin
to
cover
Lis
teri
a s
pp..
If
rapid
test
(e.g
. G
ram
sm
ear,
an
tigen
dete
cti
on
) or
oth
er
clu
es s
uggest
S.
pn
eu
mon
iae,
add
van
com
ycin
un
til sen
sit
ivit
y
data
available
. For
pen
-R S
. pn
eu
mon
iae (M
IC
2), 7
7%
an
d 5
% a
re r
especti
vely
in
term
edia
te a
nd r
esis
tan
t to
Ceft
riaxon
e (56;1
44).
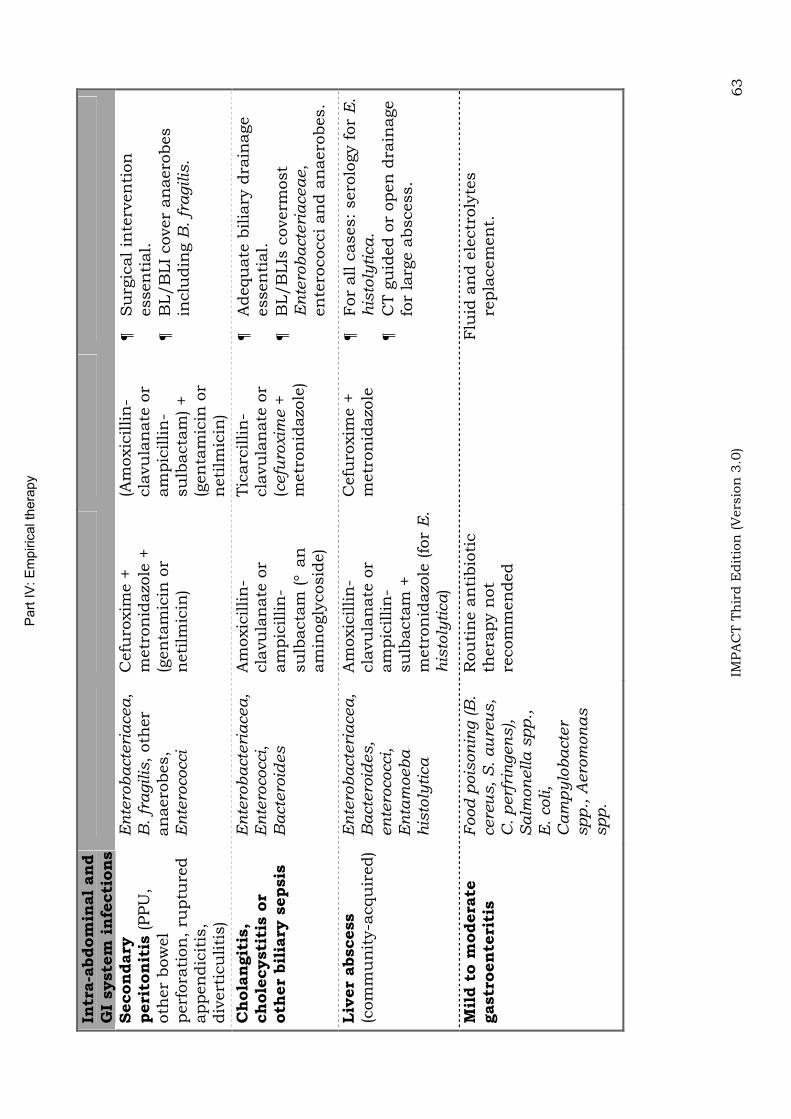
Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 63
Intr
a-a
bdom
inal
an
d
GI
syste
m i
nfe
cti
on
s
Secon
dary
peri
ton
itis
(PPU
, oth
er
bow
el
perf
ora
tion
, ru
ptu
red
appen
dic
itis
,div
ert
icu
liti
s)
En
tero
bacte
riacea,
B. fr
agilis
, oth
er
an
aero
bes,
En
tero
cocci
Cefu
roxim
e +
m
etr
on
idazo
le +
(g
en
tam
icin
or
neti
lmic
in)
(Am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m) +
(gen
tam
icin
or
neti
lmic
in)
Su
rgic
al in
terv
en
tion
essen
tial.
BL/B
LI
cover
an
aero
bes
inclu
din
g B
. fr
agilis
.
Ch
ola
ngit
is,
ch
ole
cysti
tis o
r oth
er
bil
iary
sepsis
En
tero
bacte
riacea,
En
tero
cocci,
Bacte
roid
es
Am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m (
an
am
inogly
cosid
e)
Tic
arc
illin
-cla
vu
lan
ate
or
(cefu
roxim
e +
m
etr
on
idazo
le)
Adequ
ate
bilia
ry d
rain
age
essen
tial.
BL/B
LIs
coverm
ost
En
tero
bacte
riaceae,
en
tero
cocci an
d a
naero
bes.
Liv
er
abscess
(com
mu
nit
y-a
cqu
ired)
En
tero
bacte
riacea,
Bacte
roid
es,
en
tero
cocci,
En
tam
oeb
a
his
toly
tica
Am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m +
m
etr
on
idazo
le (fo
r E
.h
isto
lyti
ca)
Cefu
roxim
e +
m
etr
on
idazo
leFor
all c
ases:
sero
logy f
or
E.
his
toly
tica.
CT g
uid
ed o
r open
dra
inage
for
larg
e a
bscess.
Mil
d t
o m
odera
te
gastr
oen
teri
tis
Food
pois
on
ing (B
. cere
us,
S.
au
reu
s,
C.
perf
rin
gen
s),
Salm
on
ella
sp
p.,
E
. coli,
Cam
py
lob
acte
r sp
p.,
Aero
mon
as
spp.
Rou
tin
e a
nti
bio
tic
thera
py n
ot
recom
men
ded
Flu
id a
nd e
lectr
oly
tes
repla
cem
en
t.
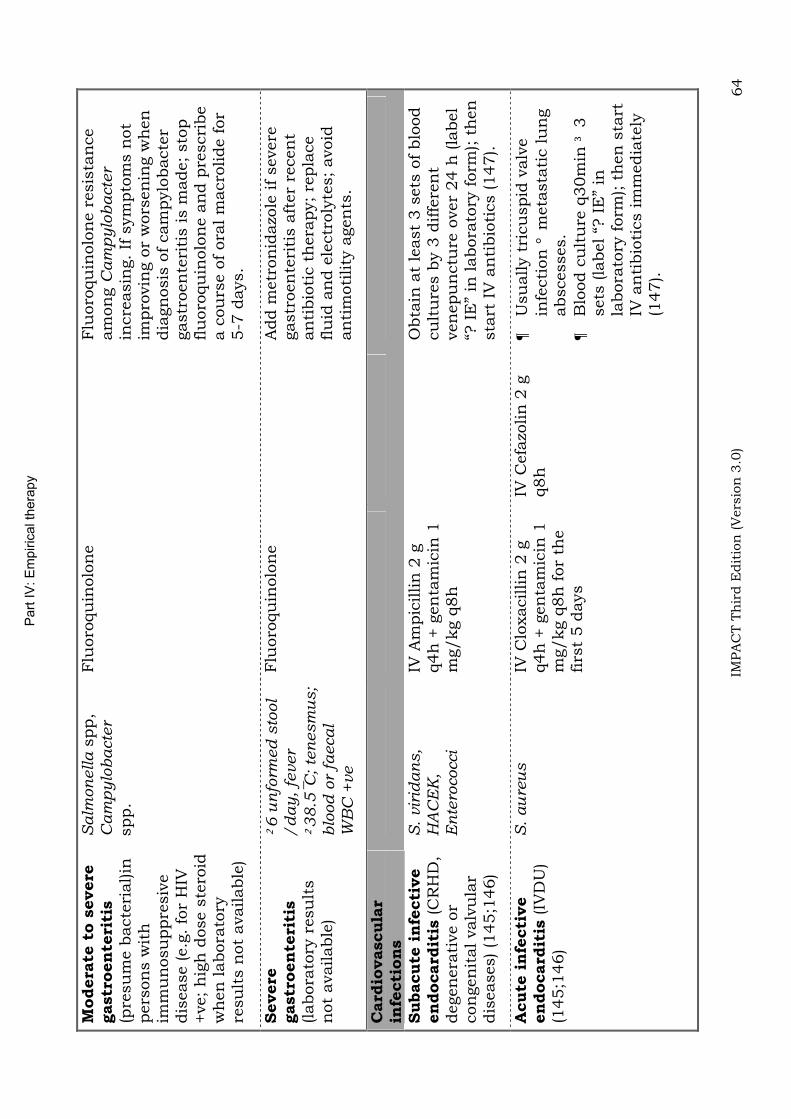
Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 64
Modera
te t
o s
evere
gastr
oen
teri
tis
(pre
su
me b
acte
rial)in
pers
on
s w
ith
im
mu
nosu
ppre
siv
edis
ease (e.g
. fo
r H
IV
+ve;
hig
h d
ose s
tero
id
wh
en
labora
tory
re
su
lts n
ot
available
)
Salm
on
ella s
pp,
Cam
py
lob
acte
rspp.
Flu
oro
qu
inolo
ne
Flu
oro
qu
inolo
ne r
esis
tan
ce
am
on
gC
am
pylo
bacte
rin
cre
asin
g.
If s
ym
pto
ms n
ot
impro
vin
g o
r w
ors
en
ing w
hen
dia
gn
osis
of
cam
pylo
bacte
r gastr
oen
teri
tis is m
ade;
sto
p
flu
oro
qu
inolo
ne a
nd p
rescri
be
a c
ou
rse o
f ora
l m
acro
lide f
or
5-7
days.
Severe
gastr
oen
teri
tis
(labora
tory
resu
lts
not
available
)
6 u
nfo
rmed
sto
ol
/d
ay
, fe
ver
38
.5C
; te
nesm
us;
blo
od
or
faecal
WB
C +
ve
Flu
oro
qu
inolo
ne
A
dd m
etr
on
idazo
le if
severe
gastr
oen
teri
tis a
fter
recen
t an
tibio
tic t
hera
py;
repla
ce
flu
id a
nd e
lectr
oly
tes;
avoid
an
tim
oti
lity
agen
ts.
Card
iovascula
rin
fecti
on
sSubacute
in
fecti
ve
en
docard
itis
(C
RH
D,
degen
era
tive o
r con
gen
ital valv
ula
r dis
eases) (1
45;1
46)
S.
vir
idan
s,
HA
CE
K,
En
tero
cocci
IV A
mpic
illin
2 g
q4h
+ g
en
tam
icin
1
mg/kg q
8h
O
bta
in a
t le
ast
3 s
ets
of
blo
od
cu
ltu
res b
y 3
diffe
ren
t ven
epu
nctu
re o
ver
24 h
(la
bel
“? I
E”
in labora
tory
form
); t
hen
sta
rt I
V a
nti
bio
tics (147).
Acute
in
fecti
ve
en
docard
itis
(IV
DU
) (1
45;1
46)
S.
au
reu
s
IV C
loxacillin
2 g
q4h
+ g
en
tam
icin
1
mg/kg q
8h
for
the
firs
t 5 d
ays
IV C
efa
zolin
2 g
q8h
Usu
ally t
ricu
spid
valv
e
infe
cti
on
meta
sta
tic lu
ng
abscesses.
Blo
od c
ult
ure
q30m
in
3
sets
(la
bel “?
IE
” in
la
bora
tory
form
); t
hen
sta
rt
IV a
nti
bio
tics im
media
tely
(1
47).
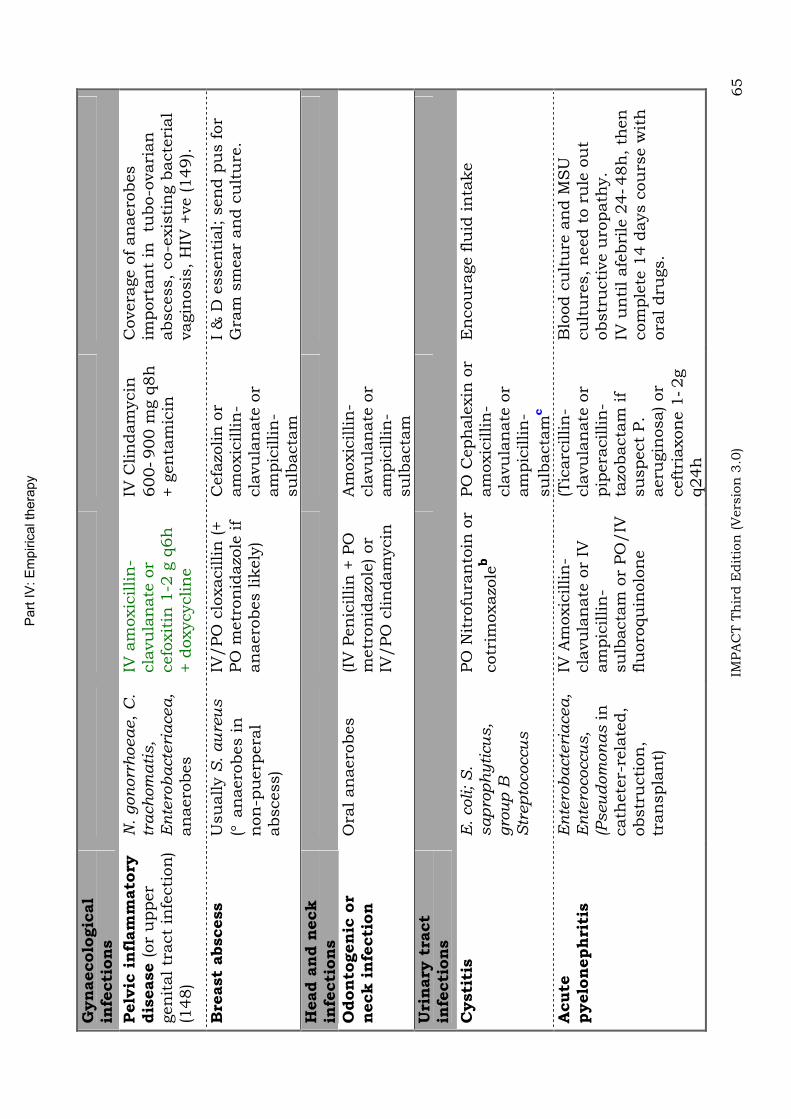
Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 65
Gyn
aecolo
gic
al
infe
cti
on
s
Pelv
ic i
nfl
am
mato
ry
dis
ease
(or
upper
gen
ital tr
act
infe
cti
on
)(1
48)
N.
gon
orr
hoeae,
C.
trach
om
ati
s,
En
tero
bacte
riacea,
an
aero
bes
IV a
moxic
illin
-cla
vu
lan
ate
or
cefo
xit
in 1
-2 g
q6h
+ d
oxycyclin
e
IV C
lin
dam
ycin
600
900 m
g q
8h
+ g
en
tam
icin
Covera
ge o
f an
aero
bes
import
an
t in
tu
bo-o
vari
an
abscess,
co-e
xis
tin
g b
acte
rial
vagin
osis
, H
IV +
ve (149).
Bre
ast
abscess
Usu
ally S
. au
reu
s
( a
naero
bes in
n
on
-pu
erp
era
labscess)
IV/PO
clo
xacillin
(+
PO
metr
on
idazo
le if
an
aero
bes lik
ely
)
Cefa
zolin
or
am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m
I &
D e
ssen
tial; s
en
d p
us f
or
Gra
m s
mear
an
d c
ult
ure
.
Head a
nd n
eck
infe
cti
on
sO
don
togen
ic o
r n
eck i
nfe
cti
on
O
ral an
aero
bes
(IV
Pen
icillin
+ P
O
metr
on
idazo
le) or
IV/PO
clin
dam
ycin
Am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
mU
rin
ary
tra
ct
infe
cti
on
s
Cysti
tis
E.
coli;
S.
sap
rop
hy
ticu
s,
gro
up
B
Str
ep
tococcu
s
PO
Nit
rofu
ran
toin
or
cotr
imoxazo
leb
PO
Ceph
ale
xin
or
am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-
su
lbacta
mc
En
cou
rage f
luid
in
take
Acute
pyelo
neph
riti
sE
nte
rob
acte
riacea,
En
tero
coccu
s,
(Pseu
dom
on
as in
cath
ete
r-re
late
d,
obstr
ucti
on
,tr
an
spla
nt)
IV A
moxic
illin
-cla
vu
lan
ate
or
IV
am
pic
illin
-su
lbacta
m o
r PO
/IV
flu
oro
qu
inolo
ne
(Tic
arc
illin
-cla
vu
lan
ate
or
pip
era
cillin
-ta
zobacta
m if
su
spect
P.
aeru
gin
osa) or
ceft
riaxon
e 1
2g
q24h
Blo
od c
ult
ure
an
d M
SU
cu
ltu
res,
need t
o r
ule
ou
t obstr
ucti
ve u
ropath
y.
IV u
nti
l afe
bri
le 2
448h
, th
en
com
ple
te 1
4 d
ays c
ou
rse w
ith
ora
l dru
gs.

Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 66
Respir
ato
ry t
ract
infe
cti
on
s
Acute
bacte
rial
exacerb
ati
on o
f C
OPD
(A
EC
B) (1
50-
152)
Appro
pri
ate
use o
f an
tibio
tics in
AE
CB
is
impera
tive t
o h
elp
con
trol th
e e
merg
en
ce
of
mu
ltid
rug r
esis
tan
t org
an
ism
s
Respir
ato
ryvir
uses,
S.
pn
eu
mon
iae,
H.
infl
uen
zae,
M.
ca
tarr
halis
d
IV/PO
am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m
Cefo
taxim
e o
r a
new
an
ti-G
ram
posit
ive
flu
oro
qu
inolo
nee
for
mu
lti-
resis
tan
tS
.p
neu
mon
iae w
ith
pen
icillin
MIC
>2
g/m
L)
Late
st
AA
CP/A
CP-A
SIM
re
com
men
dati
on
: an
tibio
tic
is o
nly
in
dic
ate
d w
hen
all 3
card
inal sym
pto
ms a
re
pre
sen
t: s
pu
tum
pu
rule
nce,
spu
tum
volu
me,
dyspn
oea.
Pen
icillin
-in
term
edia
te/re
sis
tan
tS
.
pn
eu
mon
iae (M
IC 0
.12
g/m
L) can
be t
reate
d b
y
hig
h d
ose P
O a
moxic
illin
or
IV p
en
icillin
G (h
igh
dose
Am
oxic
illin
-cla
vu
lan
ate
if
co-i
nfe
cti
on
by a
mpic
illin
-re
sis
tan
tH
. in
flu
en
zae)
(152)
Acute
bacte
rial
exacerb
ati
on o
r pneum
onia
in
pati
en
t w
ith
bro
nch
iecta
sis
P.
aeru
gin
osa
(most)
PO
Levofloxacin
/
cip
rofloxacin
or
IV
ticarc
illin
-cla
vu
lan
ate
or
pip
era
cillin
-ta
zobacta
m a
n
am
inogly
cosid
e
For
P.
aeru
gin
osa,
flu
oro
qu
inolo
ne s
hou
ld b
e
giv
en
at
hig
h d
ose (e.g
. Levofloxacin
PO
500-7
50 m
g
qd;
cip
rofloxacin
500-7
50m
g
bd)(153;1
54)
Aspir
ati
on
pneum
onia
Ora
l an
aero
bes:
Bacte
roid
es,
Pep
tostr
ep
tococci,
Fu
sob
acte
riu
m,
S.
mille
ri
(IV
Pen
icillin
G +
PO
m
etr
on
idazo
le) or
PO
clin
dam
ycin
Am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m
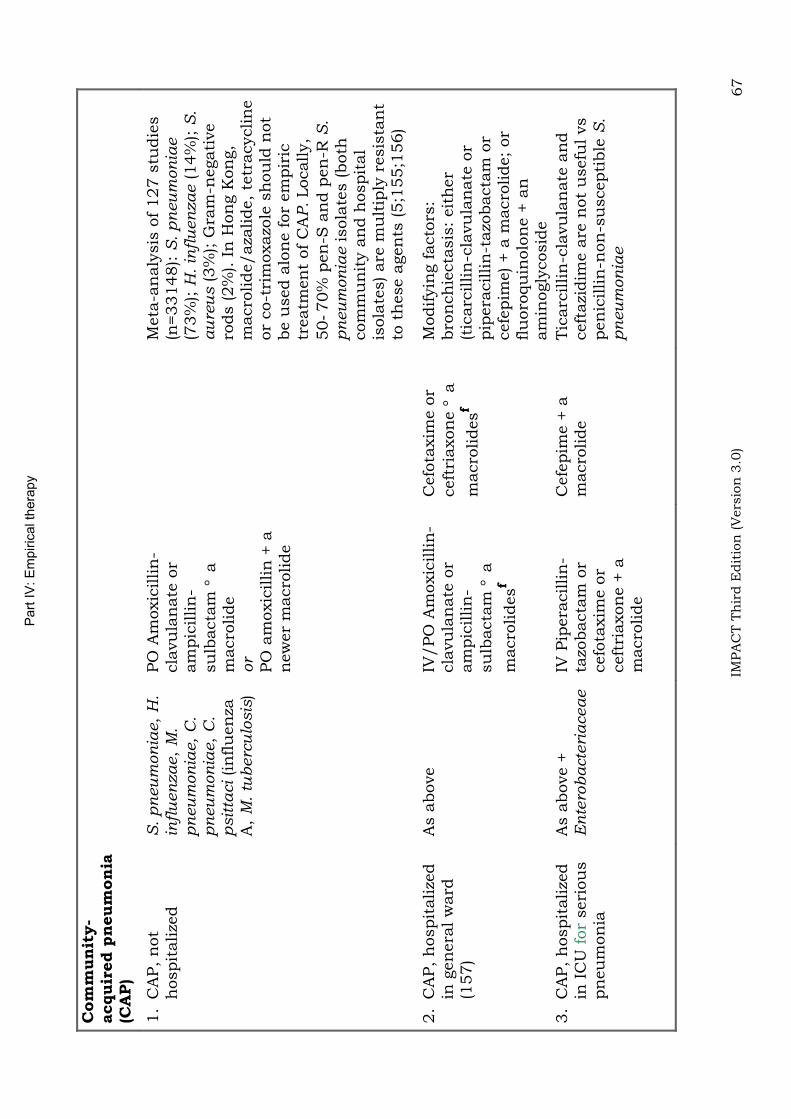
Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 67
Com
mun
ity-
acquir
ed p
neum
on
ia
(CA
P)
1.
CA
P,
not
hospit
alize
dS
. p
neu
mon
iae,
H.
infl
uen
zae,
M.
pn
eu
mon
iae,
C.
pn
eu
mon
iae,
C.
psit
taci (in
flu
en
za
A,
M.
tub
erc
ulo
sis
)
PO
Am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m a
m
acro
lide
or
PO
am
oxic
illin
+ a
n
ew
er
macro
lide
M
eta
-an
aly
sis
of
127 s
tudie
s
(n=33148):
S.
pn
eu
mon
iae
(73%
);H
. in
flu
en
zae (14%
); S
.a
ure
us (3%
); G
ram
-negati
ve
rods (2%
). I
n H
on
g K
on
g,
macro
lide/aza
lide,
tetr
acyclin
e
or
co-t
rim
oxazo
le s
hou
ld n
ot
be u
sed a
lon
e f
or
em
pir
ic
treatm
en
t of
CA
P.Locally,
50
70%
pen
-S a
nd p
en
-R S
.p
neu
mon
iae isola
tes (both
com
mu
nit
y a
nd h
ospit
al
isola
tes) are
mu
ltip
ly r
esis
tan
t to
th
ese a
gen
ts (5;1
55;1
56)
2.
CA
P,
hospit
alize
d
in g
en
era
l w
ard
(1
57)
As a
bove
IV/PO
Am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m a
macro
lidesf
Cefo
taxim
e o
r ceft
riaxon
e a
macro
lidesf
Modifyin
g f
acto
rs:
bro
nch
iecta
sis
: eit
her
(tic
arc
illin
-cla
vu
lan
ate
or
pip
era
cillin
-tazo
bacta
m o
r cefe
pim
e) + a
macro
lide;
or
flu
oro
qu
inolo
ne +
an
am
inogly
cosid
e
3.
CA
P,
hospit
alize
d
in I
CU
for
seri
ou
s
pn
eu
mon
ia
As a
bove +
E
nte
rob
acte
riaceae
IV P
ipera
cillin
-ta
zobacta
m o
r cefo
taxim
e o
r ceft
riaxon
e +
a
macro
lide
Cefe
pim
e +
a
macro
lide
Tic
arc
illin
-cla
vu
lan
ate
an
d
ceft
azi
dim
e a
re n
ot
usefu
l vs
pen
icillin
-non
-su
scepti
ble
S.
pn
eu
mon
iae
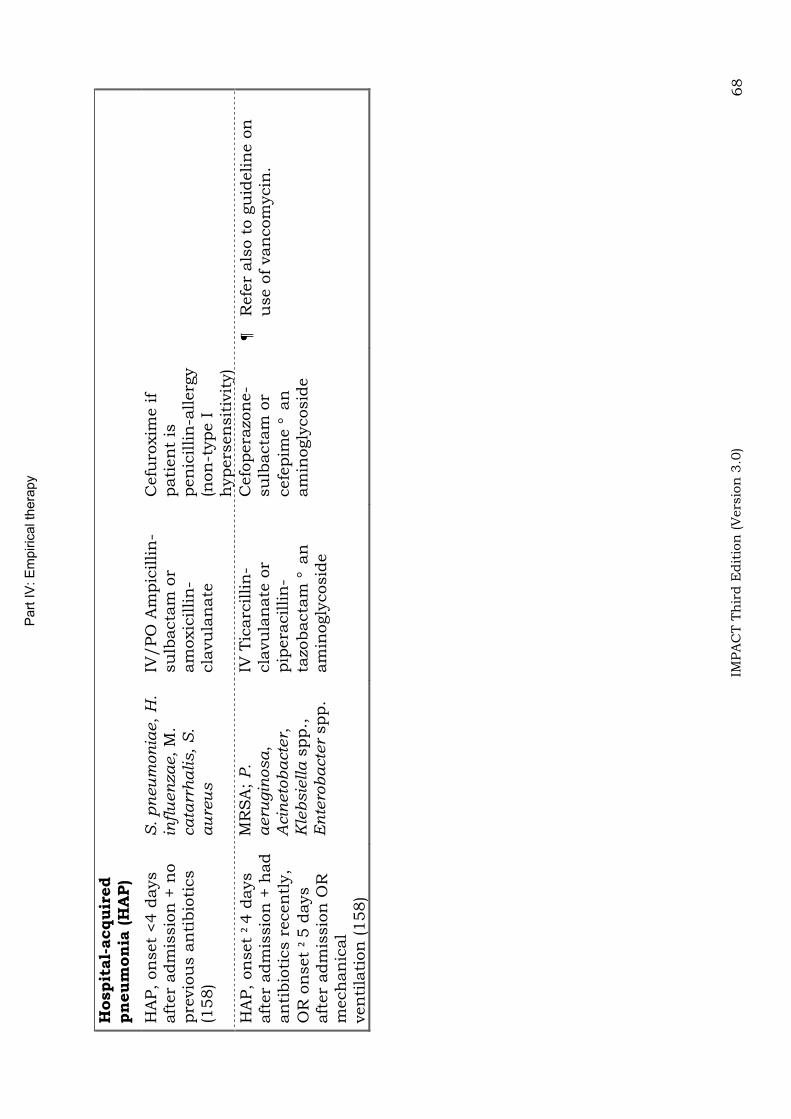
Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 68
Hospit
al-
acquir
ed
pneum
onia
(H
AP)
HA
P,
on
set
<4 d
ays
aft
er
adm
issio
n +
no
pre
vio
us a
nti
bio
tics
(158)
S.
pn
eu
mon
iae,
H.
infl
uen
zae, M
.ca
tarr
halis,
S.
au
reu
s
IV/PO
Am
pic
illin
-su
lbacta
m o
r am
oxic
illin
-cla
vu
lan
ate
Cefu
roxim
e if
pati
en
t is
pen
icillin
-allerg
y(n
on
-type I
h
ypers
en
sit
ivit
y)
HA
P,
on
set
4 d
ays
aft
er
adm
issio
n +
had
an
tibio
tics r
ecen
tly,
OR
on
set
5 d
ays
aft
er
adm
issio
n O
R
mech
an
ical
ven
tila
tion
(158)
MR
SA
;P
.a
eru
gin
osa,
Acin
eto
ba
cte
r,K
lebsie
lla s
pp.,
E
nte
rob
acte
r spp.
IV T
icarc
illin
-cla
vu
lan
ate
or
pip
era
cillin
-ta
zobacta
m a
n
am
inogly
cosid
e
Cefo
pera
zon
e-
su
lbacta
m o
r cefe
pim
e a
n
am
inogly
cosid
e
Refe
r als
o t
o g
uid
elin
e o
n
use o
f van
com
ycin
.
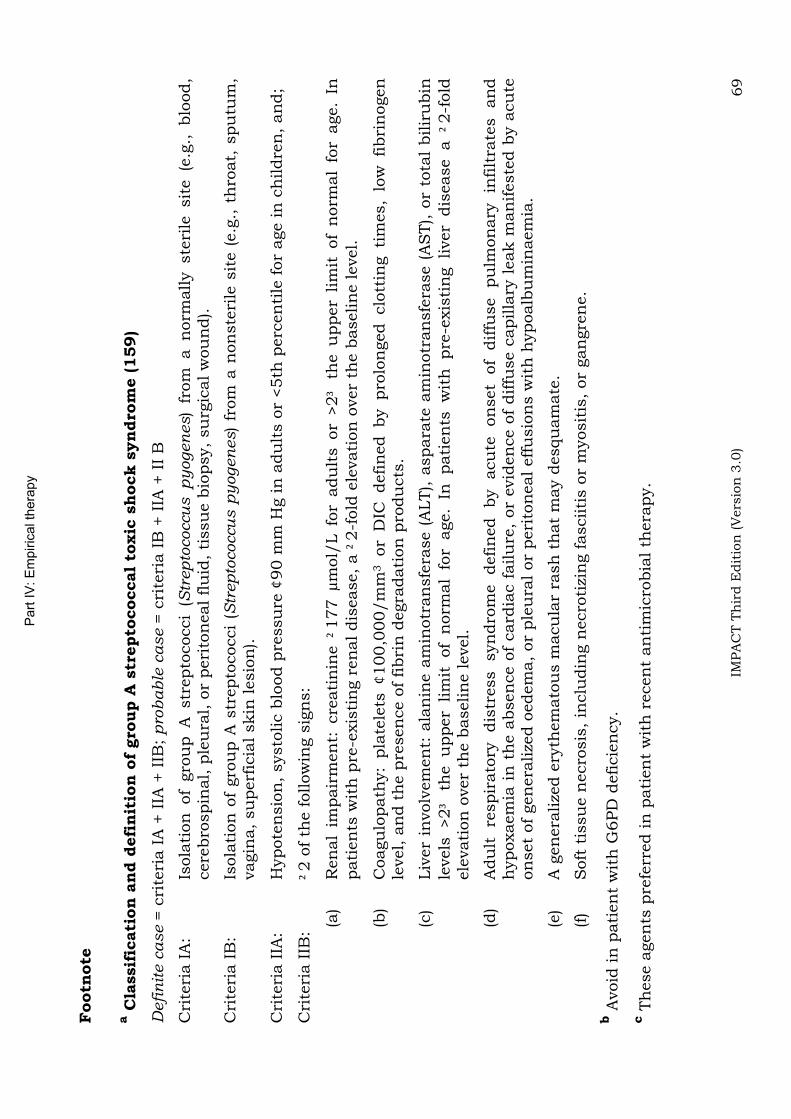
Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 69
Footn
ote
a C
lassif
icati
on
an
d d
efi
nit
ion
of
gro
up A
str
epto
coccal
toxic
shock s
yn
dro
me (159)
Defi
nit
e c
ase =
cri
teri
a I
A +
IIA
+ I
IB;
pro
bab
le c
ase =
cri
teri
a I
B +
IIA
+ I
I B
Cri
teri
a I
A:
Isola
tion
of
gro
up A
str
epto
cocci
(Str
ep
tococcu
s p
yogen
es)
from
a n
orm
ally ste
rile
sit
e (e
.g.,
blo
od,
cere
bro
spin
al, p
leu
ral, o
r peri
ton
eal flu
id,
tissu
e b
iopsy,
su
rgic
al w
ou
nd).
Cri
teri
a I
B:
Isola
tion
of
gro
up A
str
epto
cocci
(Str
ep
tococcu
s p
yogen
es)
from
a n
on
ste
rile
sit
e (
e.g
., t
hro
at,
spu
tum
, vagin
a,
su
perf
icia
l skin
lesio
n).
Cri
teri
a I
IA:
Hypote
nsio
n,
systo
lic b
lood p
ressu
re
90 m
m H
g in
adu
lts o
r <5th
perc
en
tile
for
age in
ch
ildre
n,
an
d;
Cri
teri
a I
IB:
2 o
f th
e f
ollow
ing s
ign
s:
(a)
Ren
al
impair
men
t: c
reati
nin
e
177 µ
mol/
L f
or
adu
lts o
r >2
th
e u
pper
lim
it o
f n
orm
al
for
age.
In
pati
en
ts w
ith
pre
-exis
tin
g r
en
al dis
ease,
a
2-f
old
ele
vati
on
over
the b
aselin
e level.
(b)
Coagu
lopath
y:
pla
tele
ts
100,0
00/m
m3 or
DIC
defin
ed by pro
lon
ged clo
ttin
g ti
mes,
low
fibri
nogen
le
vel, a
nd t
he p
resen
ce o
f fibri
n d
egra
dati
on
pro
du
cts
.
(c)
Liv
er
involv
em
en
t: a
lan
ine a
min
otr
an
sfe
rase (
ALT), a
spara
te a
min
otr
an
sfe
rase (
AS
T), o
r to
tal
bilir
ubin
le
vels
>2
th
e u
pper
lim
it of
norm
al
for
age.
In pati
en
ts w
ith
pre
-exis
tin
g liver
dis
ease a
2-f
old
ele
vati
on
over
the b
aselin
e level.
(d)
Adu
lt re
spir
ato
ry dis
tress syn
dro
me defin
ed by acu
te on
set
of
diffu
se pu
lmon
ary
in
filt
rate
s an
d
hypoxaem
ia i
n t
he a
bsen
ce o
f card
iac f
ailu
re,
or
evid
en
ce o
f diffu
se c
apilla
ry l
eak m
an
ifeste
d b
y a
cu
te
on
set
of
gen
era
lize
d o
edem
a,
or
ple
ura
l or
peri
ton
eal effu
sio
ns w
ith
hypoalb
um
inaem
ia.
(e)
A g
en
era
lize
d e
ryth
em
ato
us m
acu
lar
rash
th
at
may d
esqu
am
ate
.
(f)
Soft
tis
su
e n
ecro
sis
, in
clu
din
g n
ecro
tizi
ng f
asciiti
s o
r m
yosit
is,
or
gan
gre
ne.
b A
void
in
pati
en
t w
ith
G6PD
deficie
ncy.
c T
hese a
gen
ts p
refe
rred in
pati
en
t w
ith
recen
t an
tim
icro
bia
l th
era
py.
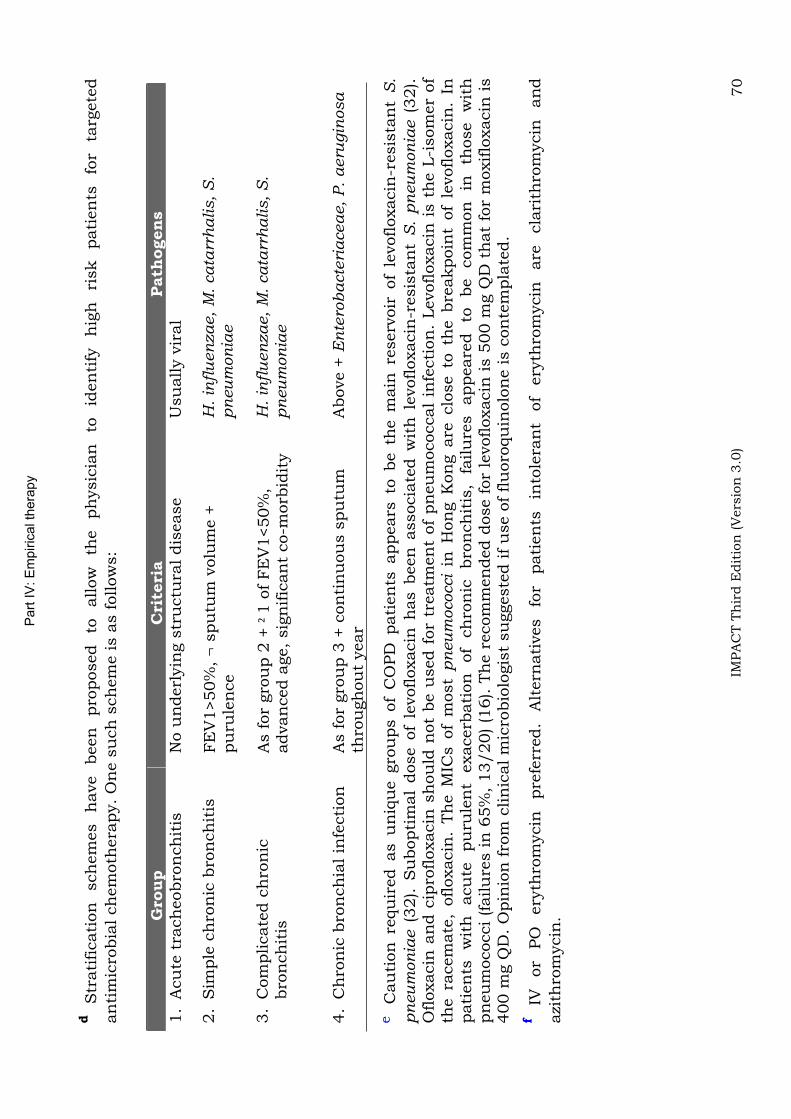
Part
IV
: E
mpir
ical th
era
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 70
d
Str
ati
ficati
on
sch
em
es
have
been
pro
posed
to
allow
th
e
ph
ysic
ian
to
id
en
tify
h
igh
ri
sk
pati
en
ts
for
targ
ete
d
an
tim
icro
bia
l ch
em
oth
era
py.
On
e s
uch
sch
em
e is a
s f
ollow
s:
Gro
up
Cri
teri
aPath
ogens
1.
Acu
te t
rach
eobro
nch
itis
N
o u
nderl
yin
g s
tru
ctu
ral dis
ease
Usu
ally v
iral
2.
Sim
ple
ch
ron
ic b
ron
ch
itis
FE
V1>50%
, s
pu
tum
volu
me +
pu
rule
nce
H.
infl
uen
zae,
M.
ca
tarr
halis,
S.
pn
eu
mon
iae
3.
Com
plicate
d c
hro
nic
bro
nch
itis
As f
or
gro
up 2
+
1 o
f FE
V1<50%
, advan
ced a
ge,
sig
nific
an
t co-m
orb
idit
y
H.
infl
uen
zae,
M.
ca
tarr
halis,
S.
pn
eu
mon
iae
4.
Ch
ron
ic b
ron
ch
ial in
fecti
on
A
s f
or
gro
up 3
+ c
on
tin
uou
s s
pu
tum
th
rou
gh
ou
t year
Above +
En
tero
bacte
riaceae,
P.
aeru
gin
osa
eC
au
tion
requ
ired a
s u
niq
ue g
rou
ps o
f C
OPD
pati
en
ts a
ppears
to b
e t
he m
ain
reserv
oir
of
levofloxacin
-resis
tan
t S
.
pn
eu
mon
iae (
32). S
ubopti
mal
dose o
f le
vofloxacin
has b
een
associa
ted w
ith
levofloxacin
-resis
tan
t S
. p
neu
mon
iae (
32).
Ofloxacin
an
d c
ipro
floxacin
sh
ou
ld n
ot
be u
sed f
or
treatm
en
t of
pn
eu
mococcal
infe
cti
on
. Levofloxacin
is t
he L
-isom
er
of
the r
acem
ate
, ofloxacin
. Th
e M
ICs o
f m
ost
pn
eu
mococci
in H
on
g K
on
g a
re c
lose t
o t
he b
reakpoin
t of
levofloxacin
. In
pati
en
ts
wit
h
acu
te
pu
rule
nt
exacerb
ati
on
of
ch
ron
ic
bro
nch
itis
, fa
ilu
res
appeare
d
to
be
com
mon
in
th
ose
wit
h
pn
eu
mococci (failu
res in
65%
, 13/20) (1
6). T
he r
ecom
men
ded d
ose f
or
levofloxacin
is 5
00 m
g Q
D t
hat
for
moxiflo
xacin
is
400 m
g Q
D.
Opin
ion
fro
m c
lin
ical m
icro
bio
logis
t su
ggeste
d if
use o
f flu
oro
qu
inolo
ne is c
on
tem
pla
ted.
fIV
or
PO
ery
thro
mycin
pre
ferr
ed.
Alt
ern
ati
ves
for
pati
en
ts
into
lera
nt
of
ery
thro
mycin
are
cla
rith
rom
ycin
an
d
azi
thro
mycin
.
Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 71
Guidelines on the use and choice of antibiotics in severe acute pancreatitis
1. Criteria for severity assessment of acute pancreatitis (Table 16).Most acute pancreatitis is mild. Severe acute pancreatitis (SAP) occurs in about 5-13% of all patients. SAP is commonly defined as having any of the following 4 criteria: (a) organ failure; (b) local complication such as necrosis, pseudocyst, or abscess; (c) Ranson score 3; or (d) at least 8 of the APACHE II criteria (160). Of all markers available, CRP is the single most useful parameter in predicting the severity of acute pancreatitis (161).
2. Infection risk. Pancreatic or peripancreatic infection occurs in 30-40% patients who have >30% pancreatic necrosis in CT staging. Infection usually occurs at least 10 days after the onset of SAP. In patients with severe acute pancreatitis, the data suggests that prophylactic antibiotic reduce infection and mortality (162-166).
3. Choice of antibiotics (Table 17): the agents should be able to penetrate into pancreatic tissue. Good pancreatic tissue concentrations have been documented for cefotaxime, piperacillin, imipenem and metronidazole (167). In terms of activity, it seems reasonable to provide coverage for the enteric Gram-negative bacilli and anaerobes. Carbepenem group of antibiotic should be reserved for the most severe form of disease (i.e. SAP with highly suspected or documented pancreatic necrosis)
4. Duration of prophylactic antibiotics: 5 to 14 days depending on disease severity and patient progress (162-169). Excessive and prolonged antibiotic use in this setting is known to cause fungal super-infection and emergence of antibiotic-resistant bacteria, and should be avoided (170;171).
5. Work-up. Consider CT or USS guided-FNA of necrotic area for culture if secondary pancreatic infection is suspected and if fever or leukocytosis persist or develops beyond 7-10 days.
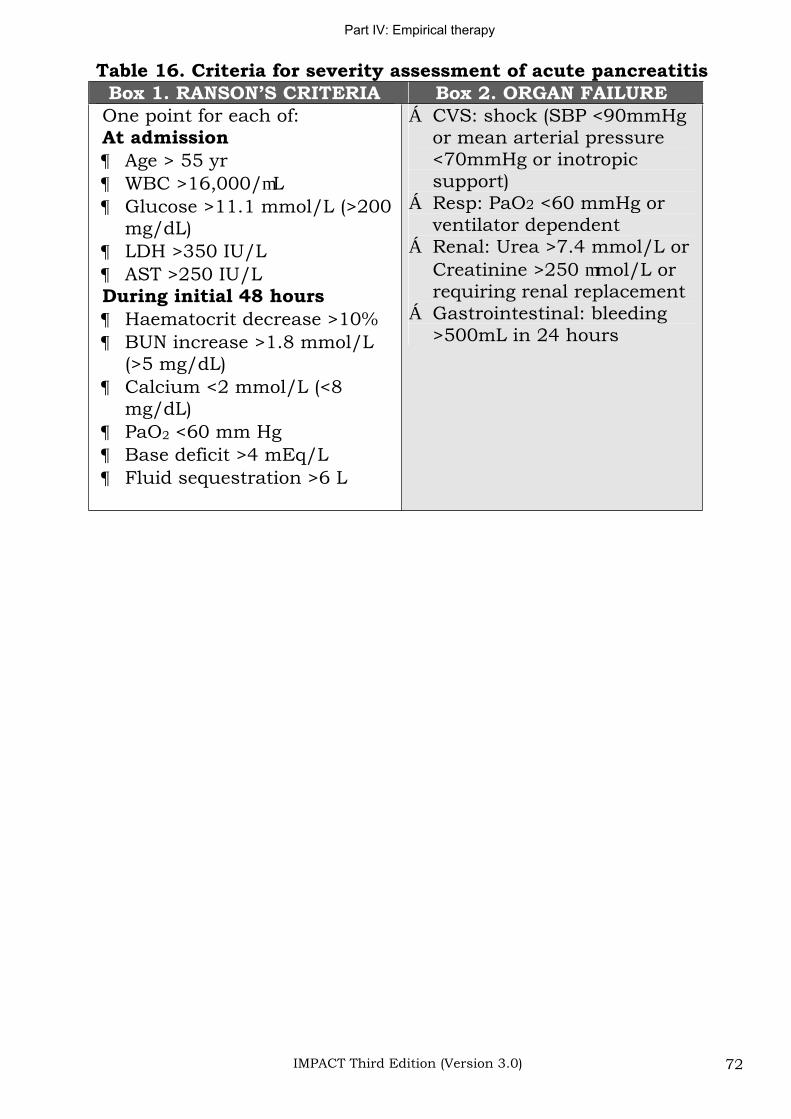
Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 72
Table 16. Criteria for severity assessment of acute pancreatitis Box 1. RANSON’S CRITERIA Box 2. ORGAN FAILURE
One point for each of: At admission
Age > 55 yr WBC >16,000/ LGlucose >11.1 mmol/L (>200 mg/dL)LDH >350 IU/L AST >250 IU/L
During initial 48 hours Haematocrit decrease >10% BUN increase >1.8 mmol/L (>5 mg/dL) Calcium <2 mmol/L (<8 mg/dL)PaO2 <60 mm Hg Base deficit >4 mEq/L Fluid sequestration >6 L
CVS: shock (SBP <90mmHg or mean arterial pressure <70mmHg or inotropic support)Resp: PaO2 <60 mmHg or ventilator dependent Renal: Urea >7.4 mmol/L or Creatinine >250 mol/L or requiring renal replacement Gastrointestinal: bleeding >500mL in 24 hours
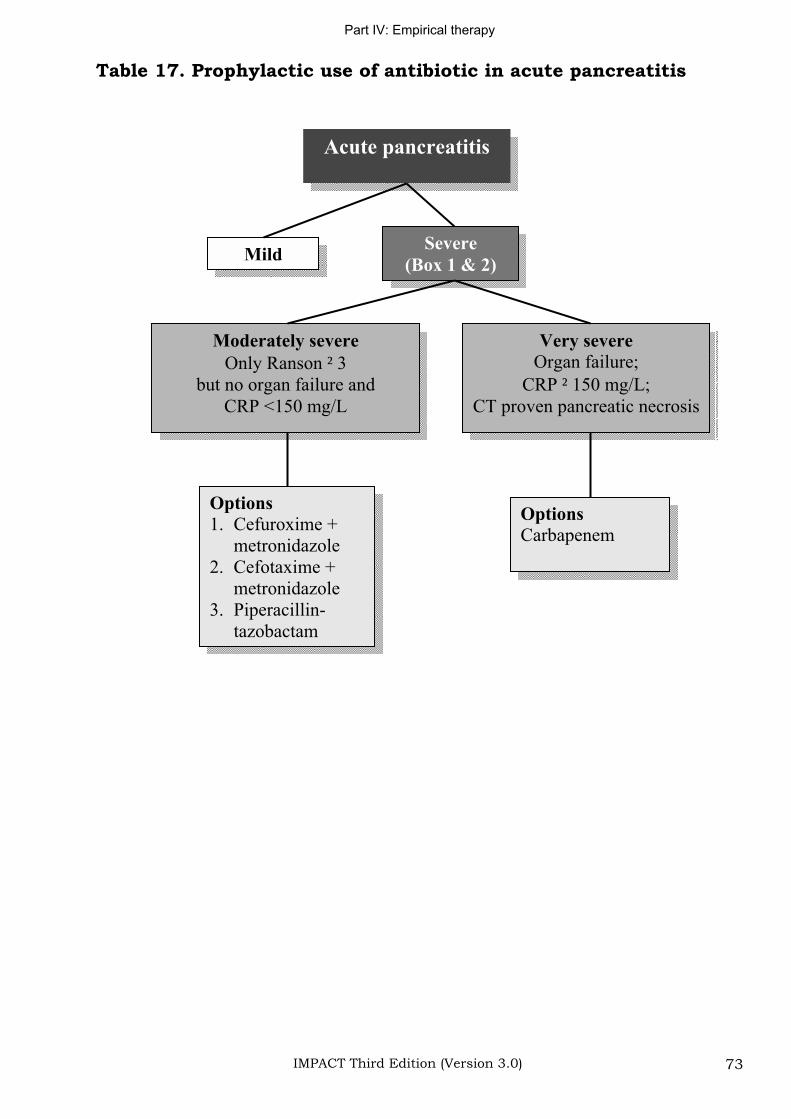
Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 73
Table 17. Prophylactic use of antibiotic in acute pancreatitis
Acute pancreatitis
MildSevere
(Box 1 & 2)
Moderately severe
Only Ranson 3
but no organ failure and
CRP <150 mg/L
Very severe
Organ failure;
CRP 150 mg/L;
CT proven pancreatic necrosis
Options
1. Cefuroxime +
metronidazole
2. Cefotaxime +
metronidazole
3. Piperacillin-
tazobactam
Options
Carbapenem
Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 74
Management of community-acquired pneumonia General considerations and principles
1. A number of guidelines on the management of community-acquired pneumonia (CAP) were released or updated recently. While these guidelines were drawn on the basis of the same set of literature, patient stratification and specific suggestions still vary quite a bit (157;172;173).
2. All agreed that S. pneumoniae is the most common pathogen in CAP including those without an identifiable etiology. Hence, the choice of agents for empirical therapy should consider the regional data on prevalence and risk factors for drug-resistant S. pneumoniae (DRSP).
3. Appropriate antimicrobial therapy should be initiated within 8 hours of hospitalization. Prior studies indicated that compliance with this recommendation is associated with a significant reduction in mortality (174).
4. Factors to be considered in choosing empirical therapy for CAP:
(a) Place of therapy (outpatient, inpatient ward, or intensive care unit).
(b) Role of atypical pathogens (e.g. Chlamydia pneumoniae,Mycoplasma pneumoniae and Legionella spp.) is increasingly being recognized. ATS guidelines even suggested that all patients should be treated for the possibility of atypical pathogen infections (173).
(c) Presence of modifying factors including risk factors for DRSP (e.g. age >65 yr., beta-lactam therapy within past 3 months, alcoholism, multiple medical comorbidities, exposure to a child in a day care centre), enteric Gram- negatives (residence in a nursing home, underlying cardiopulmonary disease, multiple medical comorbidities, recent antibiotic therapy), and P. aeruginosa (e.g. bronchiectasis).
5. Several antibiotics active against P. aeruginosa, including cefepime, imipenem, meropenem, piperacillin, and piperacillin-tazobactam are also highly active against DRSP. They can be used for patients having specific risk factors for P. aeruginosa.
6. If a macrolide is relied upon for coverage of H. influenzae, the newer macrolides (e.g. clarithromycin or azithromycin) should be used instead of erythromycin.
Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 75
7. For most patients, appropriately chosen initial antibiotic therapy should not be changed in the first 72 h, unless there is marked clinical deterioration.
8. Most patients with CAP will have an adequate clinical response within 72 h. After the patient has met appropriate criteria, switch from iv to oral therapy can be made.
Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 76
Management of community-acquired pneumonia in the era of pneumococcal resistance: conclusions from the CDC working group
1. The current CLSI (NCCLS) categories for defining susceptibility concentrations (i.e. penicillin G: sensitive for 0.06 g/mL;intermediate for 0.1-1 g/mL and resistant for 2 g/mL) are not clinically useful for treatment of patients with pneumococcal pneumonia. Comparative studies of adults and children have reported that pneumonia due to penicillin-nonsusceptible pneumococci (most had MIC >0.1-1 g/mL) does not influence the outcome of pneumonia treatment (175;176). At higher level of resistance (penicillin MIC 2-4 g/mL), recent evidence suggests that risk of mortality or suppurative complications were increased (177;178). In one study (179), the observed increase in mortality was confined to patients with pneumococcal isolates with penicillin MIC of 4 g/mL.
2. For S. pneumoniae causing pneumonia (but not otitis media and meningitis), the following revised categorization was suggested: 1 g/mL, sensitive; 2 g/mL, intermediate; 4 g/mL resistant.
By modifying the breakpoints, it is hope that there will be decreased use of broad-spectrum antimicrobial therapy in favour of more narrow-spectrum therapy. Patients with pneumococcal pneumonia caused by strains with penicillin MIC 1 g/mL can be treated appropriately with optimal dosage of IV penicillin and selected other PO/IV beta-lactams. Comparative anti-pneumococcal activities of commonly used beta-lactams is shown in Table 18.
3. Vancomycin is not routinely indicated for treatment of CAP or for pneumonia caused by DRSP.
4. The CDC working group does not advocate the use of newer fluoroquinolones for first line treatment of CAP. The reasons are:
(a) Most penicillin-nonsusceptible S. pneumoniae pneumonia can be appropriately treated with a beta-lactam with good anti-pneumococcal activity at optimal dosage.
(b) Concerns that resistance among pneumococci will rapidly emerge after widespread use of this class of antibiotics.
(c) Their activity against pneumococci with high level penicillin resistance (MIC 4 g/mL) makes it important that they be reserved for selected patients with CAP.
5. Indications for use of fluoroquinolones in CAP

Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 77
(a) Adults for whom one of the first line regimen has already failed.
(b) Allergic to alternative agents.
(c) Documented infection due to pneumococci with high level penicillin resistance (penicillin MIC 4 g/mL).
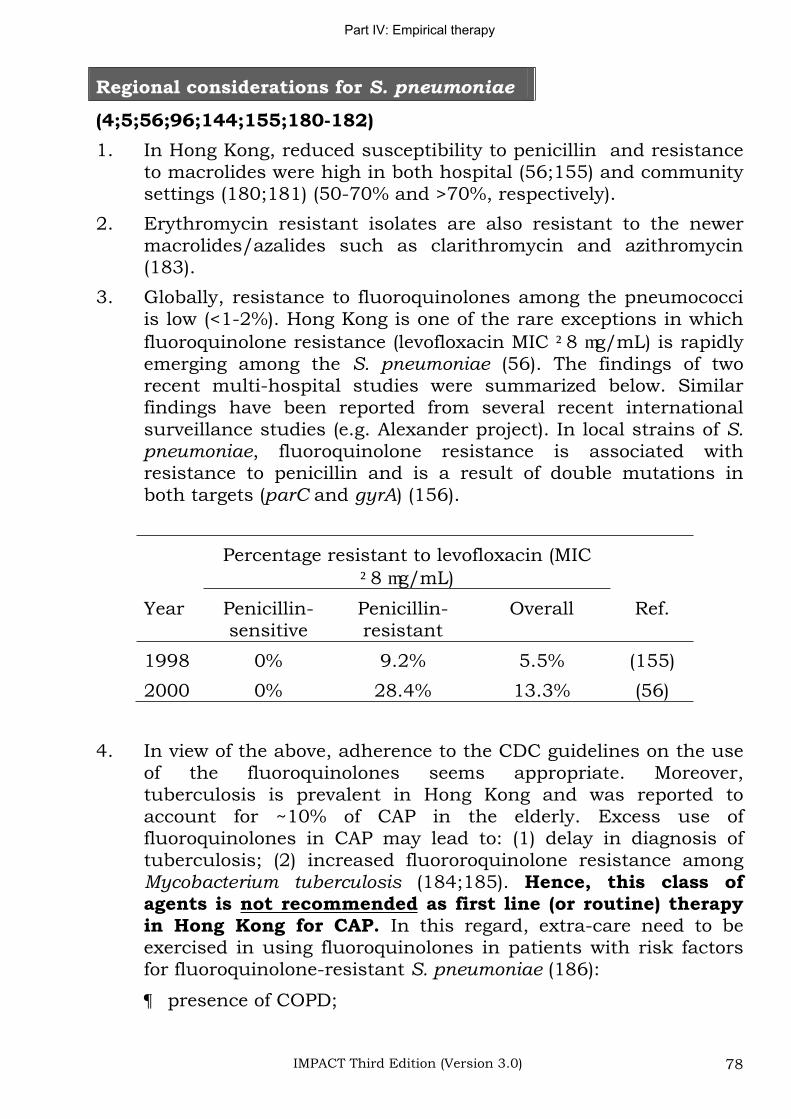
Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 78
Regional considerations for S. pneumoniae
(4;5;56;96;144;155;180-182)
1. In Hong Kong, reduced susceptibility to penicillin and resistance to macrolides were high in both hospital (56;155) and community settings (180;181) (50-70% and >70%, respectively).
2. Erythromycin resistant isolates are also resistant to the newer macrolides/azalides such as clarithromycin and azithromycin (183).
3. Globally, resistance to fluoroquinolones among the pneumococci is low (<1-2%). Hong Kong is one of the rare exceptions in which fluoroquinolone resistance (levofloxacin MIC 8 g/mL) is rapidly emerging among the S. pneumoniae (56). The findings of two recent multi-hospital studies were summarized below. Similar findings have been reported from several recent international surveillance studies (e.g. Alexander project). In local strains of S.pneumoniae, fluoroquinolone resistance is associated with resistance to penicillin and is a result of double mutations in both targets (parC and gyrA) (156).
Percentage resistant to levofloxacin (MIC 8 g/mL)
Year Penicillin-sensitive
Penicillin-resistant
Overall Ref.
1998 0% 9.2% 5.5% (155)
2000 0% 28.4% 13.3% (56)
4. In view of the above, adherence to the CDC guidelines on the use of the fluoroquinolones seems appropriate. Moreover, tuberculosis is prevalent in Hong Kong and was reported to account for ~10% of CAP in the elderly. Excess use of fluoroquinolones in CAP may lead to: (1) delay in diagnosis of tuberculosis; (2) increased fluororoquinolone resistance among Mycobacterium tuberculosis (184;185). Hence, this class of agents is not recommended as first line (or routine) therapy in Hong Kong for CAP. In this regard, extra-care need to be exercised in using fluoroquinolones in patients with risk factors for fluoroquinolone-resistant S. pneumoniae (186):
presence of COPD;
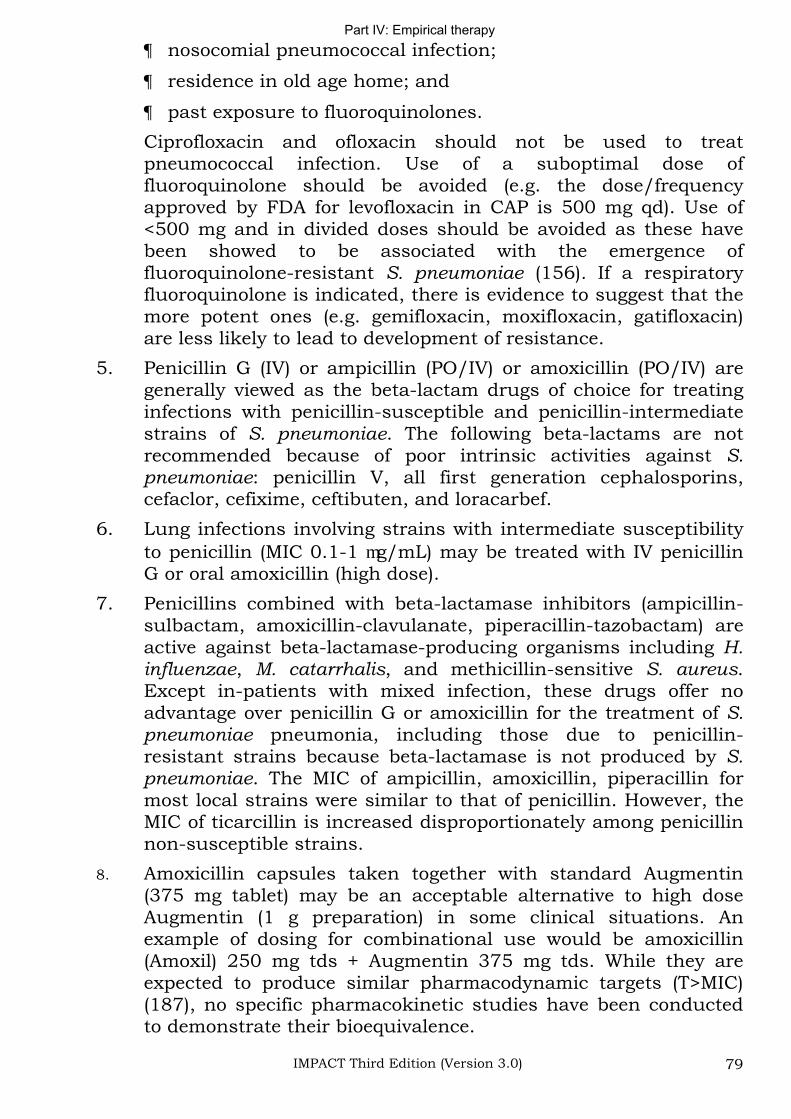
Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 79
nosocomial pneumococcal infection;
residence in old age home; and
past exposure to fluoroquinolones.
Ciprofloxacin and ofloxacin should not be used to treat pneumococcal infection. Use of a suboptimal dose of fluoroquinolone should be avoided (e.g. the dose/frequency approved by FDA for levofloxacin in CAP is 500 mg qd). Use of <500 mg and in divided doses should be avoided as these have been showed to be associated with the emergence of fluoroquinolone-resistant S. pneumoniae (156). If a respiratory fluoroquinolone is indicated, there is evidence to suggest that the more potent ones (e.g. gemifloxacin, moxifloxacin, gatifloxacin) are less likely to lead to development of resistance.
5. Penicillin G (IV) or ampicillin (PO/IV) or amoxicillin (PO/IV) are generally viewed as the beta-lactam drugs of choice for treating infections with penicillin-susceptible and penicillin-intermediate strains of S. pneumoniae. The following beta-lactams are not recommended because of poor intrinsic activities against S.pneumoniae: penicillin V, all first generation cephalosporins, cefaclor, cefixime, ceftibuten, and loracarbef.
6. Lung infections involving strains with intermediate susceptibility to penicillin (MIC 0.1-1 g/mL) may be treated with IV penicillin G or oral amoxicillin (high dose).
7. Penicillins combined with beta-lactamase inhibitors (ampicillin-sulbactam, amoxicillin-clavulanate, piperacillin-tazobactam) are active against beta-lactamase-producing organisms including H. influenzae, M. catarrhalis, and methicillin-sensitive S. aureus.Except in-patients with mixed infection, these drugs offer no advantage over penicillin G or amoxicillin for the treatment of S.pneumoniae pneumonia, including those due to penicillin-resistant strains because beta-lactamase is not produced by S. pneumoniae. The MIC of ampicillin, amoxicillin, piperacillin for most local strains were similar to that of penicillin. However, the MIC of ticarcillin is increased disproportionately among penicillin non-susceptible strains.
8. Amoxicillin capsules taken together with standard Augmentin (375 mg tablet) may be an acceptable alternative to high dose Augmentin (1 g preparation) in some clinical situations. An example of dosing for combinational use would be amoxicillin (Amoxil) 250 mg tds + Augmentin 375 mg tds. While they are expected to produce similar pharmacodynamic targets (T>MIC) (187), no specific pharmacokinetic studies have been conducted to demonstrate their bioequivalence.
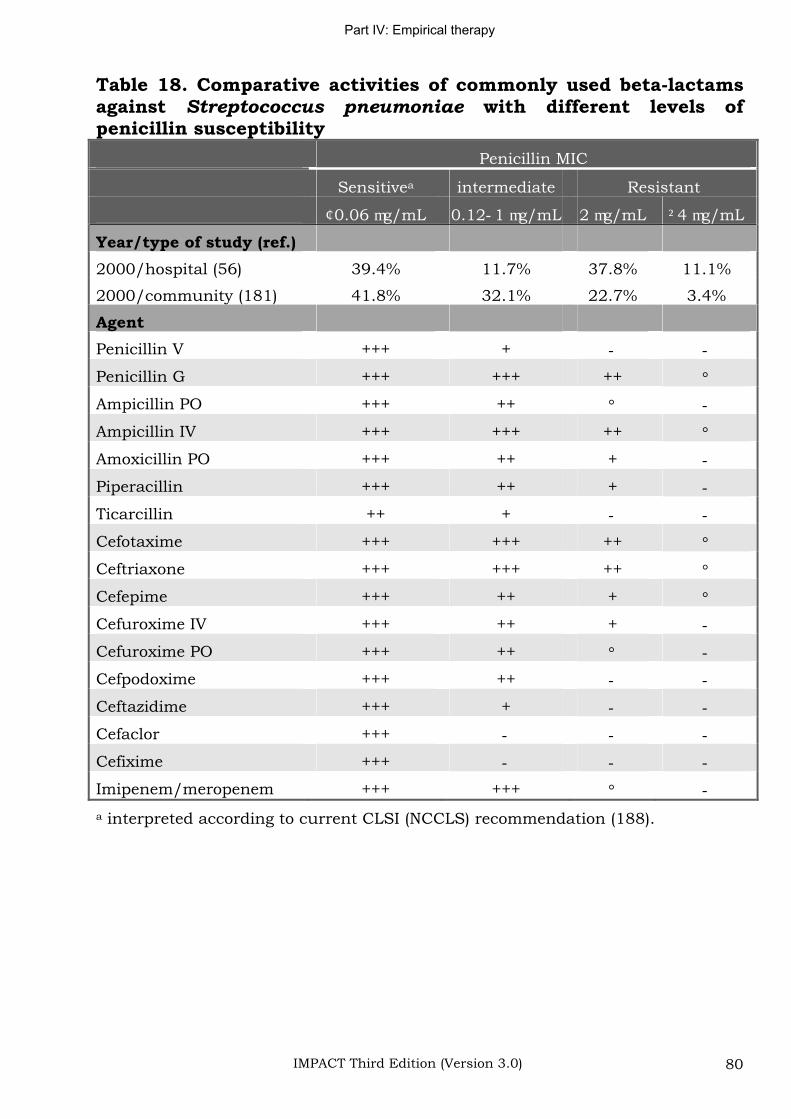
Part IV: Empirical therapy
IMPACT Third Edition (Version 3.0) 80
Table 18. Comparative activities of commonly used beta-lactams against Streptococcus pneumoniae with different levels of penicillin susceptibility
Penicillin MIC
Sensitivea intermediate Resistant
0.06 g/mL 0.12 1 g/mL 2 g/mL 4 g/mL
Year/type of study (ref.)
2000/hospital (56) 39.4% 11.7% 37.8% 11.1%
2000/community (181) 41.8% 32.1% 22.7% 3.4%
Agent
Penicillin V +++ +
Penicillin G +++ +++ ++
Ampicillin PO +++ ++
Ampicillin IV +++ +++ ++
Amoxicillin PO +++ ++ +
Piperacillin +++ ++ +
Ticarcillin ++ +
Cefotaxime +++ +++ ++
Ceftriaxone +++ +++ ++
Cefepime +++ ++ +
Cefuroxime IV +++ ++ +
Cefuroxime PO +++ ++
Cefpodoxime +++ ++
Ceftazidime +++ +
Cefaclor +++
Cefixime +++
Imipenem/meropenem +++ +++
a interpreted according to current CLSI (NCCLS) recommendation (188).

Part V: Known pathogen therapy
IMPACT Third Edition (Version 3.0) 81
Part V: Guidelines for known pathogen therapy
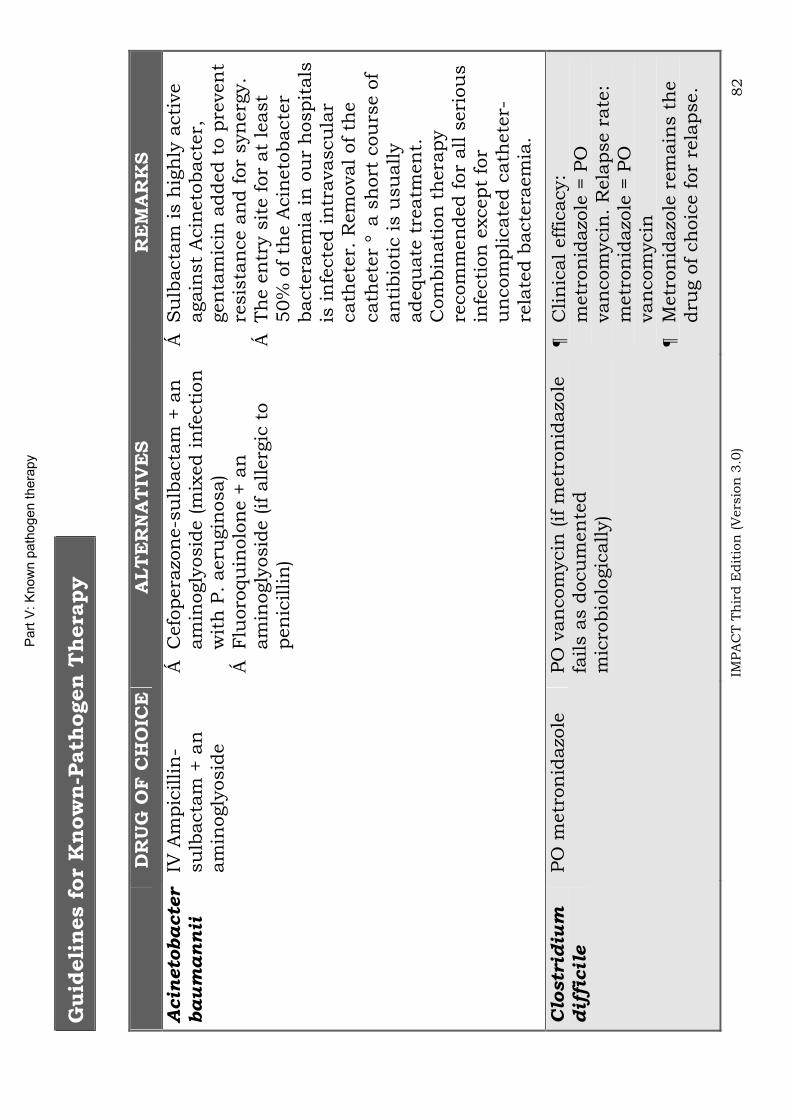
Part
V: K
now
n p
ath
ogen thera
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 82
Guid
eli
nes f
or
Know
n-P
ath
ogen T
hera
py
DR
UG
OF
CH
OIC
E
ALT
ER
NA
TIV
ES
RE
MA
RK
S
Acin
eto
ba
cte
r
ba
um
an
nii
IV
Am
pic
illin
-su
lbacta
m +
an
am
inogly
osid
e
Cefo
pera
zon
e-s
ulb
acta
m +
an
am
inogly
osid
e (m
ixed in
fecti
on
w
ith
P.
aeru
gin
osa)
Flu
oro
qu
inolo
ne +
an
am
inogly
osid
e (if a
llerg
ic t
o
pen
icillin
)
Su
lbacta
m is h
igh
ly a
cti
ve
again
st
Acin
eto
bacte
r,
gen
tam
icin
added t
o p
reven
t re
sis
tan
ce a
nd f
or
syn
erg
y.
Th
e e
ntr
y s
ite f
or
at
least
50%
of
the A
cin
eto
bacte
r bacte
raem
ia in
ou
r h
ospit
als
is
in
fecte
d in
travascu
lar
cath
ete
r. R
em
oval of
the
cath
ete
r a
sh
ort
cou
rse o
f an
tibio
tic is u
su
ally
adequ
ate
tre
atm
en
t.
Com
bin
ati
on
th
era
py
recom
men
ded f
or
all s
eri
ou
s
infe
cti
on
except
for
un
com
plicate
d c
ath
ete
r-re
late
d b
acte
raem
ia.
Clo
str
idiu
md
iffi
cil
ePO
metr
on
idazo
le
PO
van
com
ycin
(if m
etr
on
idazo
le
fails a
s d
ocu
men
ted
mic
robio
logic
ally)
Clin
ical eff
icacy:
metr
on
idazo
le =
PO
van
com
ycin
. R
ela
pse r
ate
: m
etr
on
idazo
le =
PO
van
com
ycin
M
etr
on
idazo
le r
em
ain
s t
he
dru
g o
f ch
oic
e f
or
rela
pse.
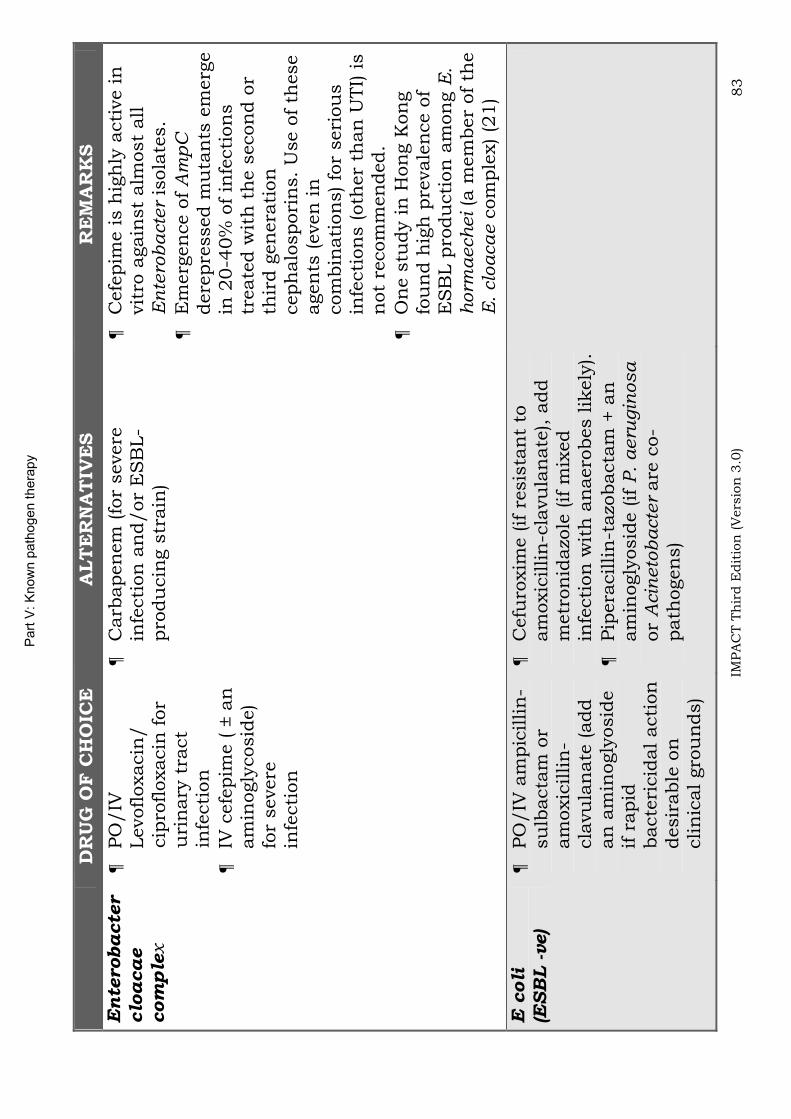
Part
V: K
now
n p
ath
ogen thera
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 83
DR
UG
OF
CH
OIC
E
ALT
ER
NA
TIV
ES
RE
MA
RK
S
Ente
robacte
r
clo
aca
ecom
ple
x
PO
/IV
Levofloxacin
/
cip
rofloxacin
for
uri
nary
tra
ct
infe
cti
on
IV c
efe
pim
e ( ±
an
am
inogly
cosid
e)
for
severe
in
fecti
on
Carb
apen
em
(fo
r severe
in
fecti
on
an
d/or
ES
BL-
pro
du
cin
g s
train
)
Cefe
pim
e is h
igh
ly a
cti
ve in
vit
ro a
gain
st
alm
ost
all
En
tero
ba
cte
r is
ola
tes.
Em
erg
en
ce o
f A
mp
Cdere
pre
ssed m
uta
nts
em
erg
e
in 2
0-4
0%
of
infe
cti
on
s
treate
d w
ith
th
e s
econ
d o
r th
ird g
en
era
tion
ceph
alo
spori
ns.
Use o
f th
ese
agen
ts (even
in
com
bin
ati
on
s) fo
r seri
ou
s
infe
cti
on
s (oth
er
than
UTI)
is
not
recom
men
ded.
On
e s
tudy in
Hon
g K
on
g
fou
nd h
igh
pre
vale
nce o
f E
SB
L p
rodu
cti
on
am
on
g E
.h
orm
aech
ei (a
mem
ber
of
the
E.
clo
aca
e c
om
ple
x) (2
1)
E c
oli
(E
SB
L -ve)
PO
/IV
am
pic
illin
-su
lbacta
m o
r am
oxic
illin
-cla
vu
lan
ate
(add
an
am
inogly
osid
e
if r
apid
bacte
ricid
al acti
on
desir
able
on
clin
ical gro
un
ds)
Cefu
roxim
e (if r
esis
tan
t to
am
oxic
illin
-cla
vu
lan
ate
), a
dd
metr
on
idazo
le (if m
ixed
infe
cti
on
wit
h a
naero
bes lik
ely
).Pip
era
cillin
-tazo
bacta
m +
an
am
inogly
osid
e (if P
. aeru
gin
osa
or
Acin
eto
bacte
r are
co-
path
ogen
s)
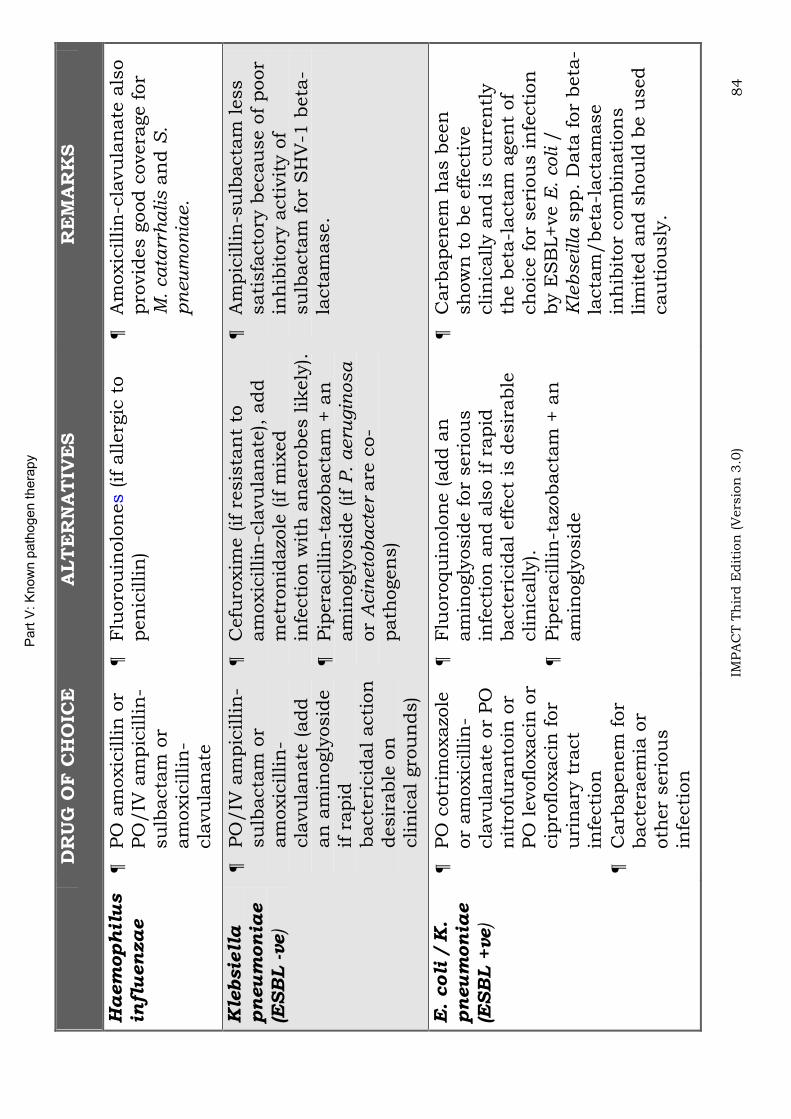
Part
V: K
now
n p
ath
ogen thera
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 84
DR
UG
OF
CH
OIC
E
ALT
ER
NA
TIV
ES
RE
MA
RK
S
Ha
em
oph
ilu
sin
flu
en
za
ePO
am
oxic
illin
or
PO
/IV
am
pic
illin
-su
lbacta
m o
r am
oxic
illin
-cla
vu
lan
ate
Flu
oro
uin
olo
nes
(if
allerg
ic t
o
pen
icillin
)A
moxic
illin
-cla
vu
lan
ate
als
o
pro
vid
es g
ood c
overa
ge f
or
M.
ca
tarr
halis a
nd S
.p
neu
mon
iae.
Kle
bsie
lla
pn
eu
mon
iae
(ES
BL -ve)
PO
/IV
am
pic
illin
-su
lbacta
m o
r am
oxic
illin
-cla
vu
lan
ate
(add
an
am
inogly
osid
e
if r
apid
bacte
ricid
al acti
on
desir
able
on
clin
ical gro
un
ds)
Cefu
roxim
e (if r
esis
tan
t to
am
oxic
illin
-cla
vu
lan
ate
), a
dd
metr
on
idazo
le (if m
ixed
infe
cti
on
wit
h a
naero
bes lik
ely
).Pip
era
cillin
-tazo
bacta
m +
an
am
inogly
osid
e (if P
. aeru
gin
osa
or
Acin
eto
bacte
r are
co-
path
ogen
s)
Am
pic
illin
-su
lbacta
m less
sati
sfa
cto
ry b
ecau
se o
f poor
inh
ibit
ory
acti
vit
y o
f su
lbacta
m f
or
SH
V-1
beta
-la
cta
mase.
E.
coli
/ K
. pn
eu
mon
iae
(ES
BL +
ve)
PO
cotr
imoxazo
le
or
am
oxic
illin
-cla
vu
lan
ate
or
PO
n
itro
fura
nto
in o
r PO
levofloxacin
or
cip
rofloxacin
for
uri
nary
tra
ct
infe
cti
on
Carb
apen
em
for
bacte
raem
ia o
r oth
er
seri
ou
s
infe
cti
on
Flu
oro
qu
inolo
ne (add a
n
am
inogly
osid
e f
or
seri
ou
s
infe
cti
on
an
d a
lso if
rapid
bacte
ricid
al eff
ect
is d
esir
able
clin
ically).
Pip
era
cillin
-tazo
bacta
m +
an
am
inogly
osid
e
Carb
apen
em
has b
een
sh
ow
n t
o b
e e
ffecti
ve
clin
ically a
nd is c
urr
en
tly
the b
eta
-lacta
m a
gen
t of
ch
oic
e f
or
seri
ou
s in
fecti
on
by E
SB
L+ve E
. coli /
Kle
bseilla
spp.
Data
for
beta
-la
cta
m/beta
-lacta
mase
inh
ibit
or
com
bin
ati
on
s
lim
ited a
nd s
hou
ld b
e u
sed
cau
tiou
sly
.
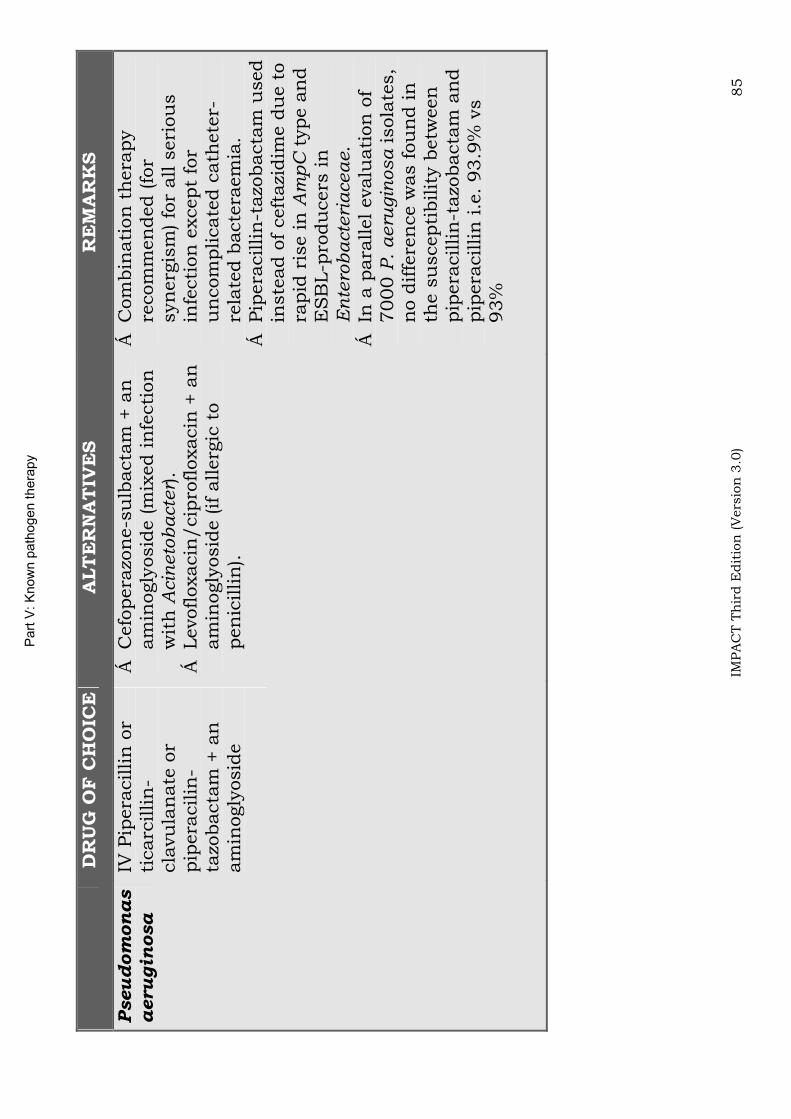
Part
V: K
now
n p
ath
ogen thera
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 85
DR
UG
OF
CH
OIC
E
ALT
ER
NA
TIV
ES
RE
MA
RK
S
Pseudom
onas
aerugin
osa
IV P
ipera
cillin
or
ticarc
illin
-cla
vu
lan
ate
or
pip
era
cilin
-ta
zobacta
m +
an
am
inogly
osid
e
Cefo
pera
zon
e-s
ulb
acta
m +
an
am
inogly
osid
e (m
ixed in
fecti
on
w
ith
Acin
eto
bacte
r).
Levofloxacin
/cip
rofloxacin
+ a
n
am
inogly
osid
e (if a
llerg
ic t
o
pen
icillin
).
Com
bin
ati
on
th
era
py
recom
men
ded (fo
r syn
erg
ism
) fo
r all s
eri
ou
s
infe
cti
on
except
for
un
com
plicate
d c
ath
ete
r-re
late
d b
acte
raem
ia.
Pip
era
cillin
-tazo
bacta
m u
sed
inste
ad o
f ceft
azi
dim
e d
ue t
o
rapid
ris
e in
Am
pC
type a
nd
ES
BL-p
rodu
cers
in
E
nte
rob
acte
ria
cea
e.
In a
para
llel evalu
ati
on
of
7000
P.
aeru
gin
osa isola
tes,
no d
iffe
ren
ce w
as f
ou
nd in
th
e s
uscepti
bilit
y b
etw
een
pip
era
cillin
-tazo
bacta
m a
nd
pip
era
cillin
i.e
. 93.9
% v
s
93%
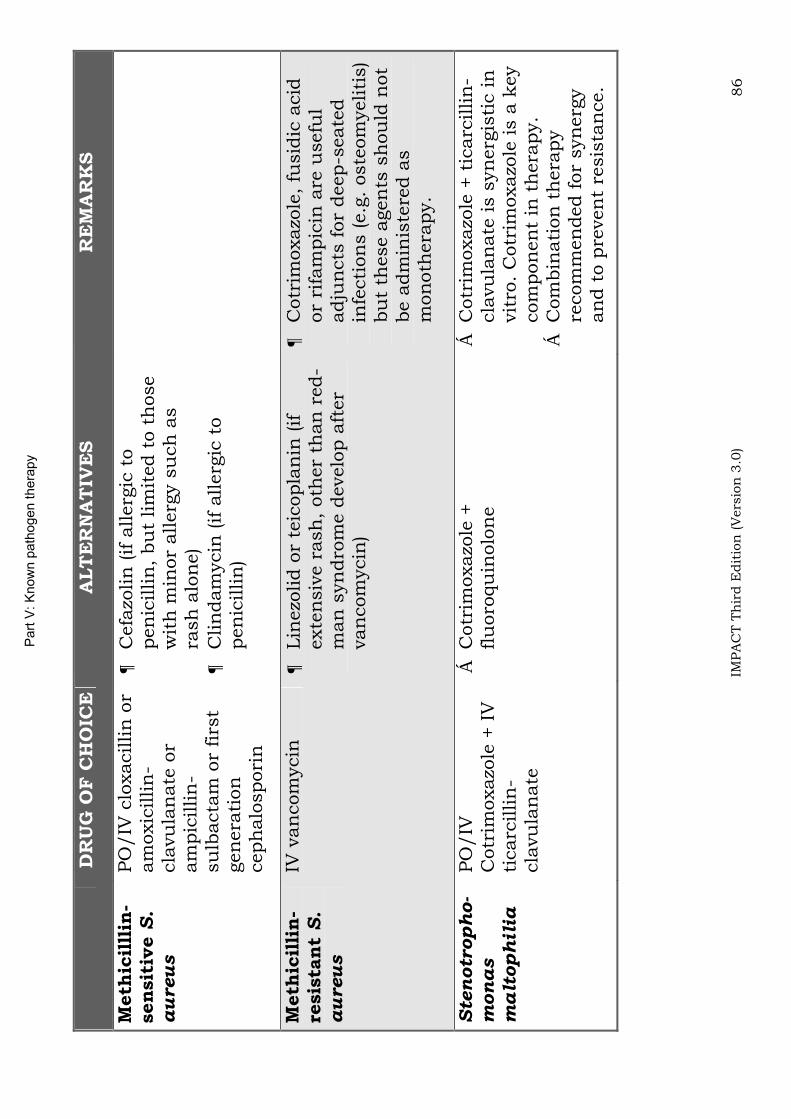
Part
V: K
now
n p
ath
ogen thera
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 86
DR
UG
OF
CH
OIC
E
ALT
ER
NA
TIV
ES
RE
MA
RK
S
Meth
icil
llin
-sen
sit
ive S
.aureus
PO
/IV
clo
xacillin
or
am
oxic
illin
-cla
vu
lan
ate
or
am
pic
illin
-su
lbacta
m o
r firs
t gen
era
tion
ceph
alo
spori
n
Cefa
zolin
(if a
llerg
ic t
o
pen
icillin
, bu
t lim
ited t
o t
hose
wit
h m
inor
allerg
y s
uch
as
rash
alo
ne)
Clin
dam
ycin
(if a
llerg
ic t
o
pen
icillin
)
Meth
icil
lin
-re
sis
tan
tS
.aureus
IV v
an
com
ycin
Lin
ezo
lid o
r te
icopla
nin
(if
exte
nsiv
e r
ash
, oth
er
than
red-
man
syn
dro
me d
evelo
p a
fter
van
com
ycin
)
Cotr
imoxazo
le,
fusid
ic a
cid
or
rifa
mpic
in a
re u
sefu
l adju
ncts
for
deep-s
eate
d
infe
cti
on
s (e.g
. oste
om
yeliti
s)
bu
t th
ese a
gen
ts s
hou
ld n
ot
be a
dm
inis
tere
d a
s
mon
oth
era
py.
Ste
notr
oph
o-
monas
ma
ltoph
ilia
PO
/IV
C
otr
imoxazo
le +
IV
ti
carc
illin
-cla
vu
lan
ate
Cotr
imoxazo
le +
flu
oro
qu
inolo
ne
Cotr
imoxazo
le +
tic
arc
illin
-cla
vu
lan
ate
is s
yn
erg
isti
c in
vit
ro.
Cotr
imoxazo
le is a
key
com
pon
en
t in
th
era
py.
Com
bin
ati
on
th
era
py
recom
men
ded f
or
syn
erg
y
an
d t
o p
reven
t re
sis
tan
ce.
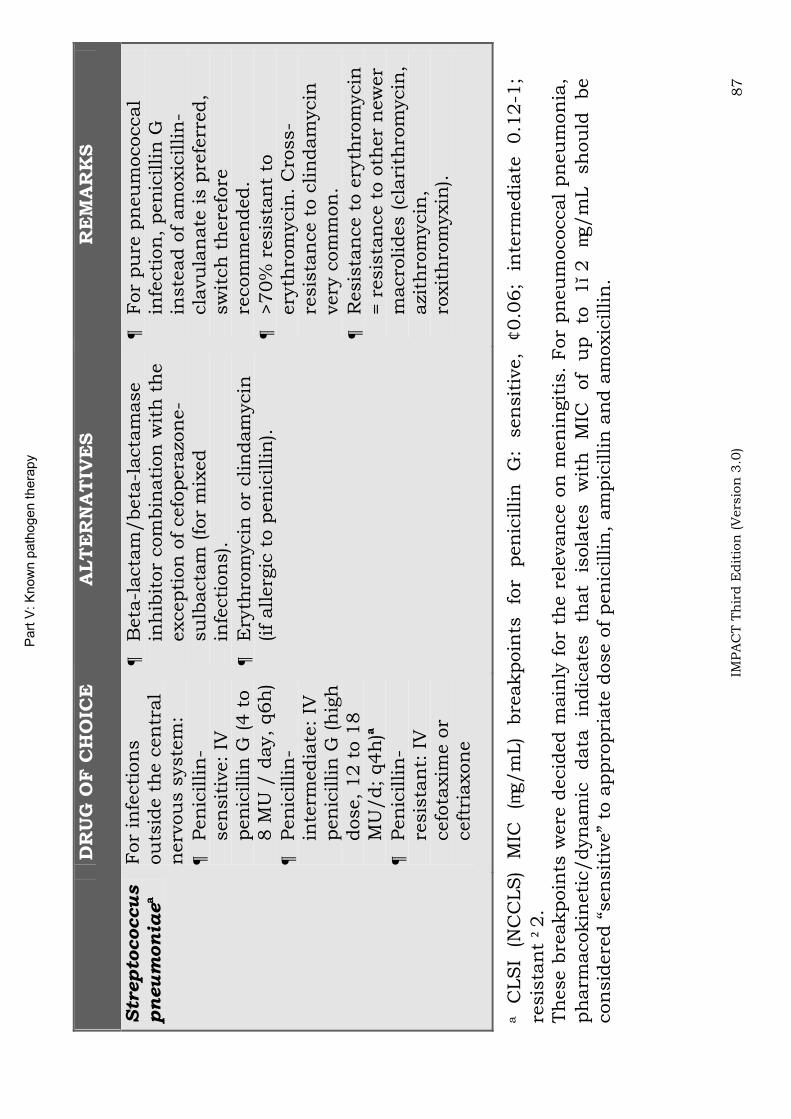
Part
V: K
now
n p
ath
ogen thera
py
IMPA
CT T
hir
d E
dit
ion
(V
ers
ion
3.0
) 87
DR
UG
OF
CH
OIC
E
ALT
ER
NA
TIV
ES
RE
MA
RK
S
Str
epto
coccu
spn
eu
mon
iae
a
For
infe
cti
on
s
ou
tsid
e t
he c
en
tral
nerv
ou
s s
yste
m:
Pen
icillin
-sen
sit
ive:
IV
pen
icillin
G (4 t
o
8 M
U /
day,
q6h
) Pen
icillin
-in
term
edia
te:
IV
pen
icillin
G (h
igh
dose,
12 t
o 1
8
MU
/d;
q4h
)a
Pen
icillin
-re
sis
tan
t: I
V
cefo
taxim
e o
r ceft
riaxon
e
Beta
-lacta
m/beta
-lacta
mase
inh
ibit
or
com
bin
ati
on
wit
h t
he
excepti
on
of
cefo
pera
zon
e-
su
lbacta
m (fo
r m
ixed
infe
cti
on
s).
Ery
thro
mycin
or
clin
dam
ycin
(if
allerg
ic t
o p
en
icillin
).
For
pu
re p
neu
mococcal
infe
cti
on
, pen
icillin
G
inste
ad o
f am
oxic
illin
-cla
vu
lan
ate
is p
refe
rred,
sw
itch
th
ere
fore
re
com
men
ded.
>70%
resis
tan
t to
ery
thro
mycin
. C
ross-
resis
tan
ce t
o c
lin
dam
ycin
very
com
mon
. R
esis
tan
ce t
o e
ryth
rom
ycin
= r
esis
tan
ce t
o o
ther
new
er
macro
lides (cla
rith
rom
ycin
, azi
thro
mycin
,ro
xit
hro
myxin
).
a
CLS
I (N
CC
LS
) M
IC
(g/m
L)
bre
akpoin
ts
for
pen
icillin
G
: sen
sit
ive,
0.0
6;
inte
rmedia
te
0.1
2-1
; re
sis
tan
t2.
Th
ese b
reakpoin
ts w
ere
decid
ed m
ain
ly f
or
the r
ele
van
ce o
n m
en
ingit
is.
For
pn
eu
mococcal
pn
eu
mon
ia,
ph
arm
acokin
eti
c/dyn
am
ic
data
in
dic
ate
s
that
isola
tes
wit
h
MIC
of
up
to
12
g/m
L
sh
ou
ld
be
con
sid
ere
d “
sen
sit
ive”
to a
ppro
pri
ate
dose o
f pen
icillin
, am
pic
illin
an
d a
moxic
illin
.
Part VI: Surgical prophylaxis
IMPACT Third Edition (Version 3.0) 88
Part VI: Guidelines for surgical prophylaxis
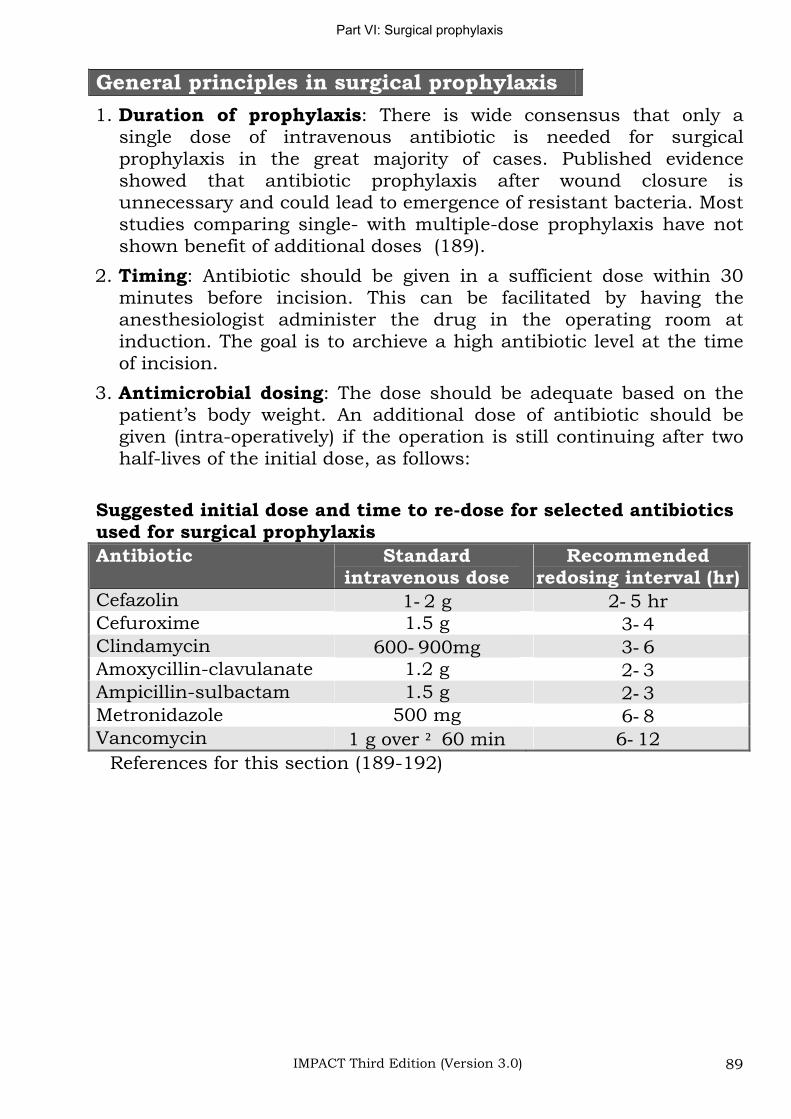
Part VI: Surgical prophylaxis
IMPACT Third Edition (Version 3.0) 89
General principles in surgical prophylaxis
1. Duration of prophylaxis: There is wide consensus that only a single dose of intravenous antibiotic is needed for surgical prophylaxis in the great majority of cases. Published evidence showed that antibiotic prophylaxis after wound closure is unnecessary and could lead to emergence of resistant bacteria. Most studies comparing single- with multiple-dose prophylaxis have not shown benefit of additional doses (189).
2. Timing: Antibiotic should be given in a sufficient dose within 30 minutes before incision. This can be facilitated by having the anesthesiologist administer the drug in the operating room at induction. The goal is to archieve a high antibiotic level at the time of incision.
3. Antimicrobial dosing: The dose should be adequate based on the patient’s body weight. An additional dose of antibiotic should be given (intra-operatively) if the operation is still continuing after two half-lives of the initial dose, as follows:
Suggested initial dose and time to re-dose for selected antibiotics used for surgical prophylaxis
Antibiotic Standardintravenous dose
Recommendedredosing interval (hr)
Cefazolin 1 2 g 2 5 hr Cefuroxime 1.5 g 3 4Clindamycin 600 900mg 3 6Amoxycillin-clavulanate 1.2 g 2 3Ampicillin-sulbactam 1.5 g 2 3Metronidazole 500 mg 6 8Vancomycin 1 g over 60 min 6 12
References for this section (189-192)
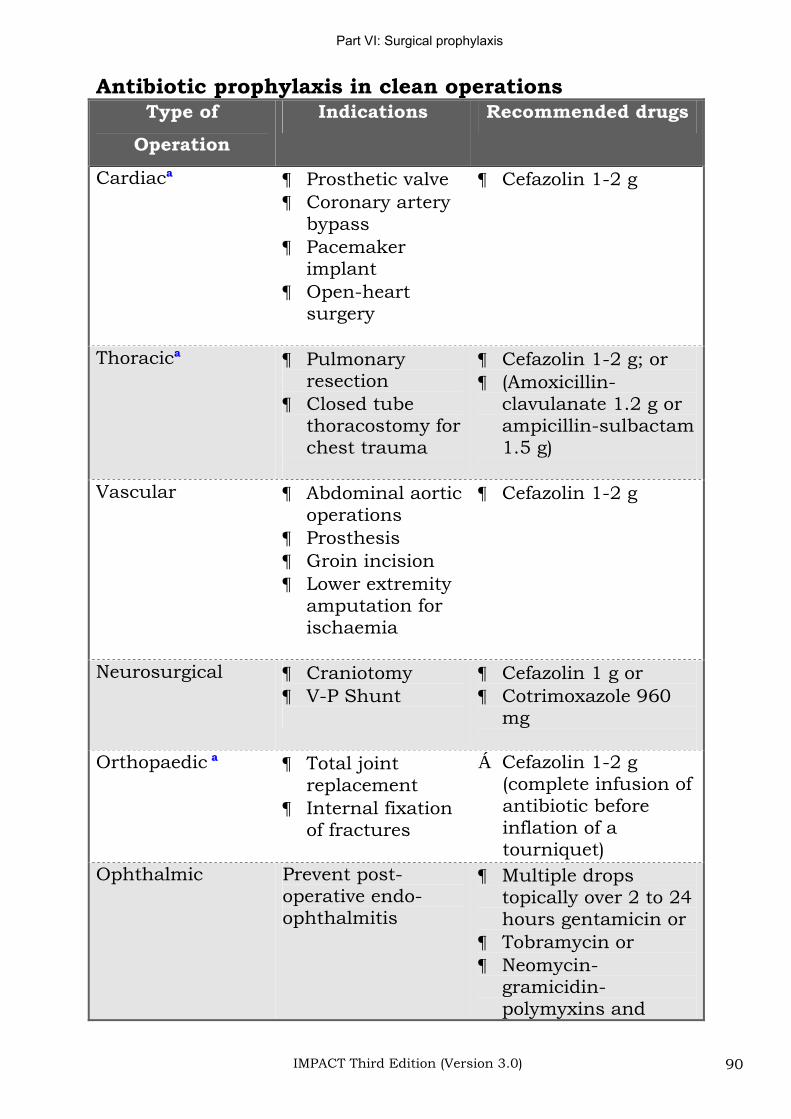
Part VI: Surgical prophylaxis
IMPACT Third Edition (Version 3.0) 90
Antibiotic prophylaxis in clean operations Type of
Operation
Indications Recommended drugs
Cardiaca Prosthetic valve Coronary artery bypassPacemaker implantOpen-heartsurgery
Cefazolin 1-2 g
Thoracica Pulmonary resectionClosed tube thoracostomy for chest trauma
Cefazolin 1-2 g; or (Amoxicillin-clavulanate 1.2 g or ampicillin-sulbactam1.5 g)
Vascular Abdominal aortic operationsProsthesis Groin incision Lower extremity amputation for ischaemia
Cefazolin 1-2 g
Neurosurgical Craniotomy V-P Shunt
Cefazolin 1 g or Cotrimoxazole 960 mg
Orthopaedic a Total joint replacementInternal fixation of fractures
Cefazolin 1-2 g (complete infusion of antibiotic before inflation of a tourniquet)
Ophthalmic Prevent post-operative endo-ophthalmitis
Multiple drops topically over 2 to 24 hours gentamicin or Tobramycin or Neomycin-gramicidin-polymyxins and
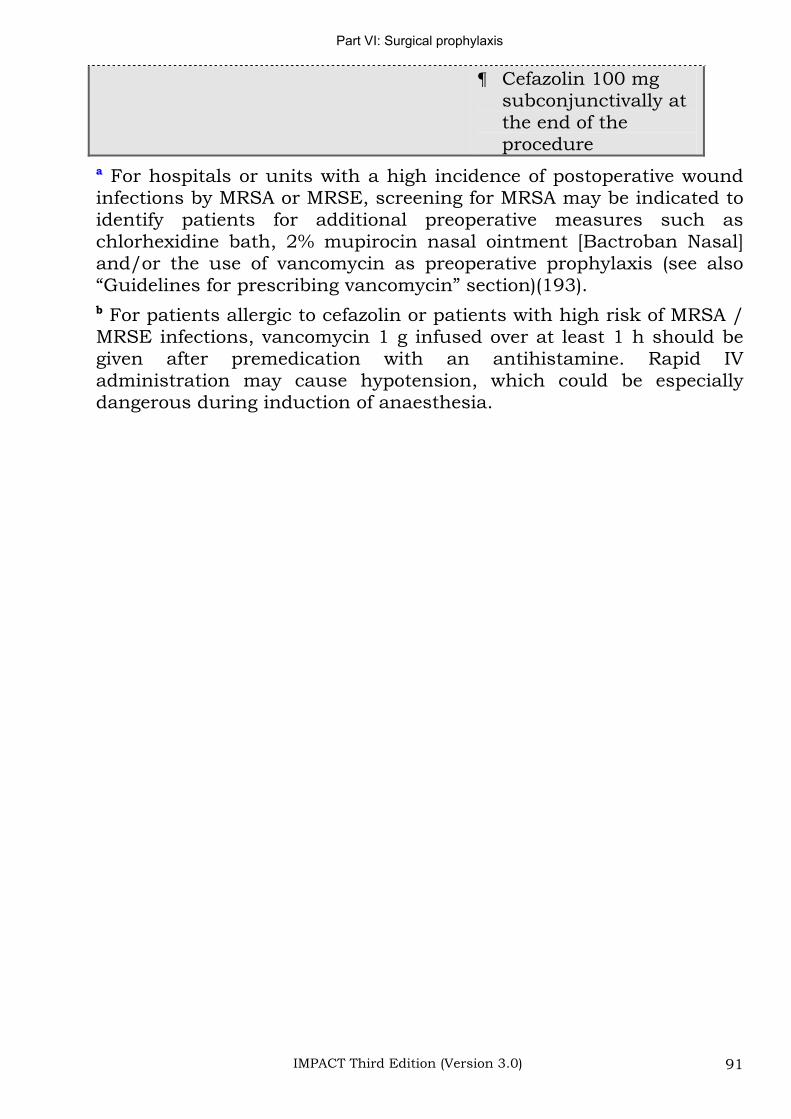
Part VI: Surgical prophylaxis
IMPACT Third Edition (Version 3.0) 91
Cefazolin 100 mg subconjunctivally at the end of the procedure
a For hospitals or units with a high incidence of postoperative wound infections by MRSA or MRSE, screening for MRSA may be indicated to identify patients for additional preoperative measures such as chlorhexidine bath, 2% mupirocin nasal ointment [Bactroban Nasal] and/or the use of vancomycin as preoperative prophylaxis (see also “Guidelines for prescribing vancomycin” section)(193). b For patients allergic to cefazolin or patients with high risk of MRSA / MRSE infections, vancomycin 1 g infused over at least 1 h should be given after premedication with an antihistamine. Rapid IV administration may cause hypotension, which could be especially dangerous during induction of anaesthesia.
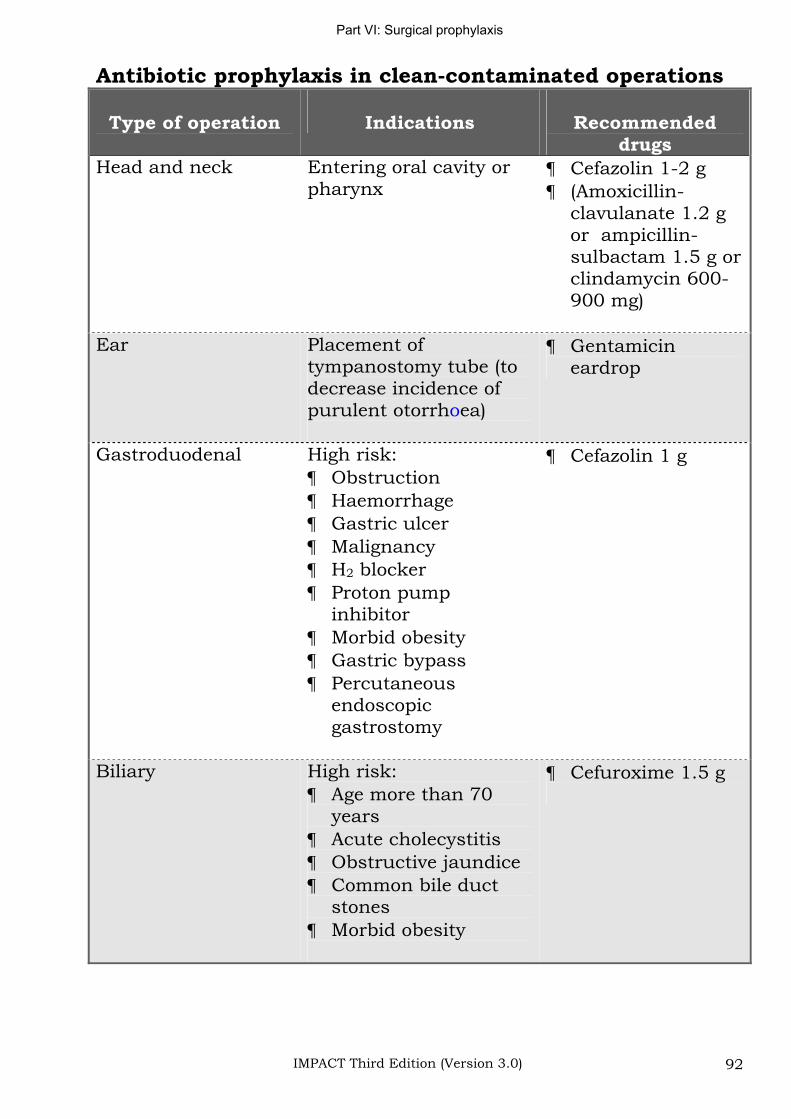
Part VI: Surgical prophylaxis
IMPACT Third Edition (Version 3.0) 92
Antibiotic prophylaxis in clean-contaminated operations
Type of operation Indications Recommendeddrugs
Head and neck Entering oral cavity or pharynx
Cefazolin 1-2 g (Amoxicillin-clavulanate 1.2 g or ampicillin-sulbactam 1.5 g orclindamycin 600-900 mg)
Ear Placement of tympanostomy tube (to decrease incidence of purulent otorrhoea)
Gentamicin eardrop
Gastroduodenal High risk: ObstructionHaemorrhage Gastric ulcer MalignancyH2 blocker Proton pump inhibitor Morbid obesity Gastric bypass Percutaneous endoscopicgastrostomy
Cefazolin 1 g
Biliary High risk: Age more than 70 yearsAcute cholecystitis Obstructive jaundice Common bile duct stonesMorbid obesity
Cefuroxime 1.5 g
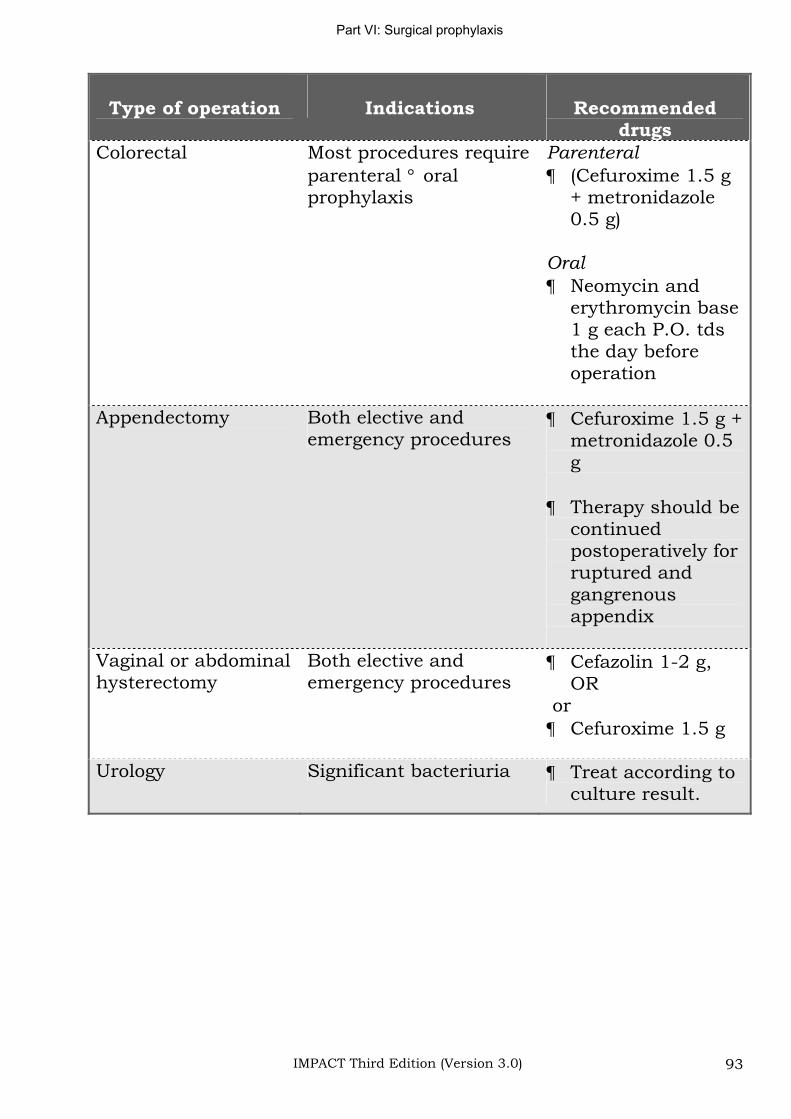
Part VI: Surgical prophylaxis
IMPACT Third Edition (Version 3.0) 93
Type of operation Indications Recommendeddrugs
Colorectal Most procedures require parenteral oral prophylaxis
Parenteral
(Cefuroxime 1.5 g + metronidazole 0.5 g)
Oral
Neomycin and erythromycin base 1 g each P.O. tds the day before operation
Appendectomy Both elective and emergency procedures
Cefuroxime 1.5 g + metronidazole 0.5 g
Therapy should be continuedpostoperatively for ruptured and gangrenousappendix
Vaginal or abdominal hysterectomy
Both elective and emergency procedures
Cefazolin 1-2 g, OR
orCefuroxime 1.5 g
Urology Significant bacteriuria Treat according to culture result.
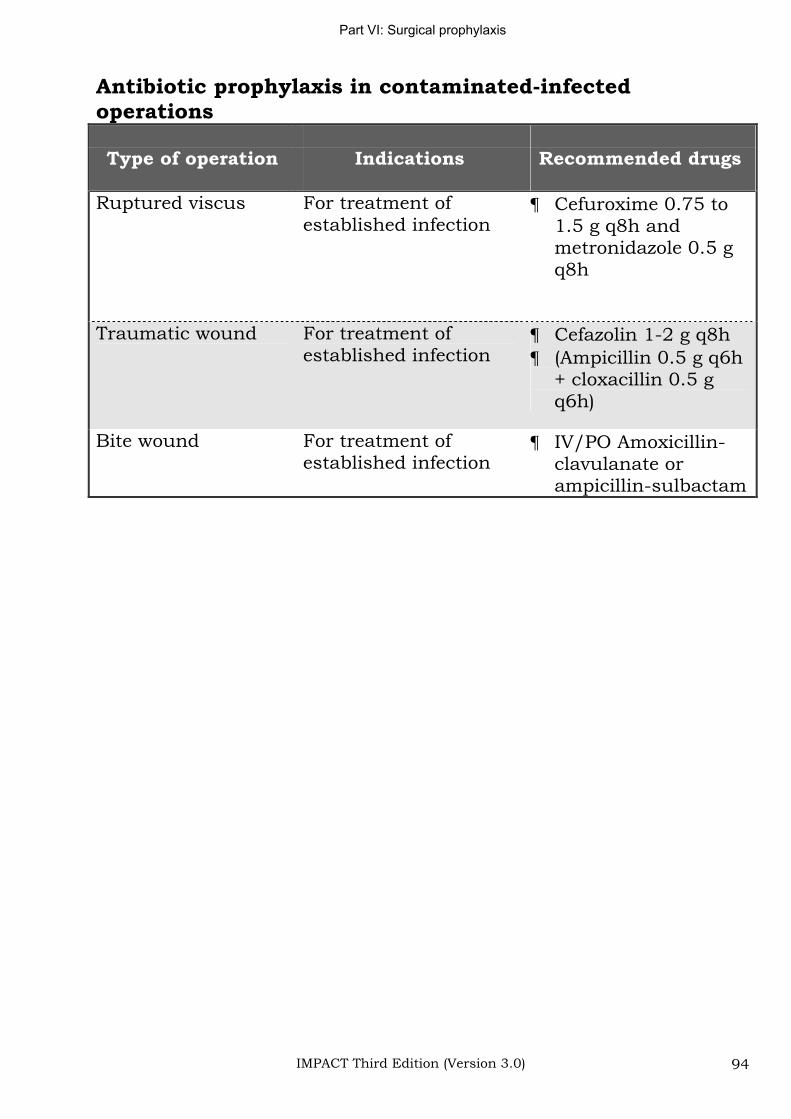
Part VI: Surgical prophylaxis
IMPACT Third Edition (Version 3.0) 94
Antibiotic prophylaxis in contaminated-infected operations
Type of operation Indications Recommended drugs
Ruptured viscus For treatment of established infection
Cefuroxime 0.75 to 1.5 g q8h and metronidazole 0.5 g q8h
Traumatic wound For treatment of established infection
Cefazolin 1-2 g q8h (Ampicillin 0.5 g q6h + cloxacillin 0.5 g q6h)
Bite wound For treatment of established infection
IV/PO Amoxicillin-clavulanate or ampicillin-sulbactam
Cost and dosage
IMPACT Third Edition (Version 3.0) 95
Part VII: Cost and recommended dosage of commonly-used antimicrobial agents
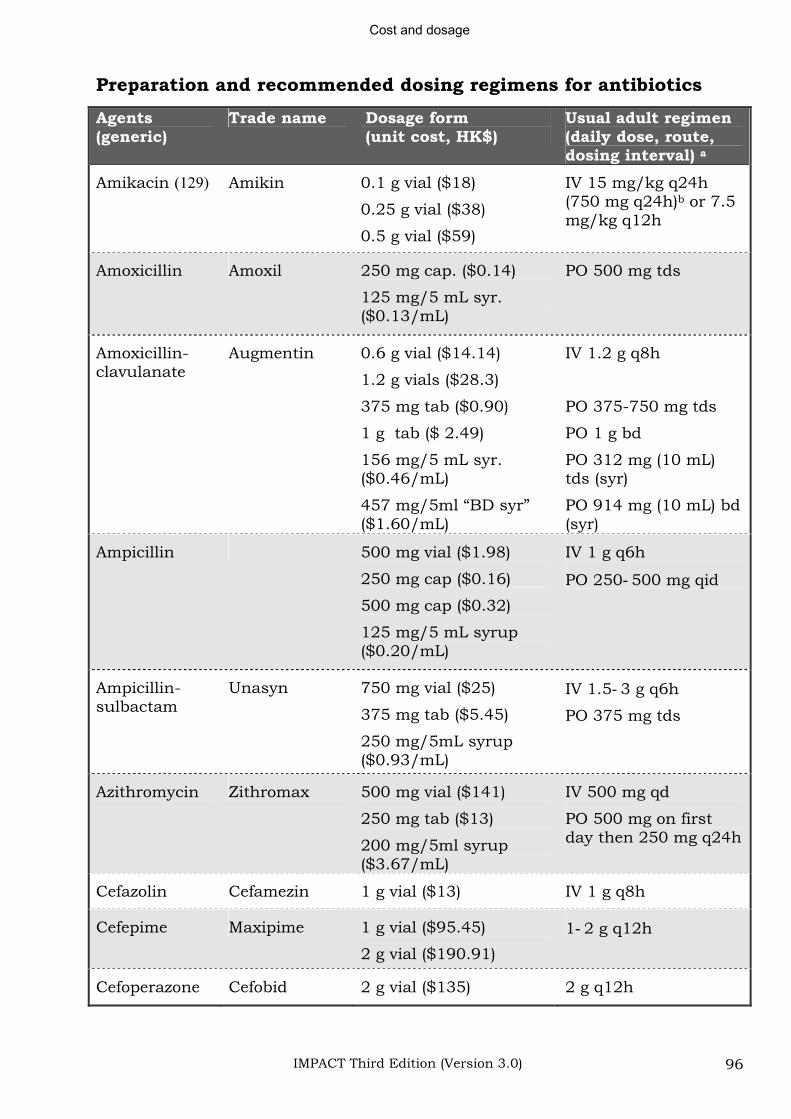
Cost and dosage
IMPACT Third Edition (Version 3.0) 96
Preparation and recommended dosing regimens for antibiotics
Agents(generic)
Trade name Dosage form (unit cost, HK$)
Usual adult regimen (daily dose, route, dosing interval) a
Amikacin (129) Amikin 0.1 g vial ($18)
0.25 g vial ($38)
0.5 g vial ($59)
IV 15 mg/kg q24h (750 mg q24h)b or 7.5 mg/kg q12h
Amoxicillin Amoxil 250 mg cap. ($0.14)
125 mg/5 mL syr. ($0.13/mL)
PO 500 mg tds
Amoxicillin-clavulanate
Augmentin 0.6 g vial ($14.14)
1.2 g vials ($28.3)
375 mg tab ($0.90)
1 g tab ($ 2.49)
156 mg/5 mL syr. ($0.46/mL)
457 mg/5ml “BD syr” ($1.60/mL)
IV 1.2 g q8h
PO 375-750 mg tds
PO 1 g bd
PO 312 mg (10 mL) tds (syr)
PO 914 mg (10 mL) bd (syr)
Ampicillin 500 mg vial ($1.98)
250 mg cap ($0.16)
500 mg cap ($0.32)
125 mg/5 mL syrup ($0.20/mL)
IV 1 g q6h
PO 250 500 mg qid
Ampicillin-sulbactam
Unasyn 750 mg vial ($25)
375 mg tab ($5.45)
250 mg/5mL syrup ($0.93/mL)
IV 1.5 3 g q6h
PO 375 mg tds
Azithromycin Zithromax 500 mg vial ($141)
250 mg tab ($13)
200 mg/5ml syrup ($3.67/mL)
IV 500 mg qd
PO 500 mg on first day then 250 mg q24h
Cefazolin Cefamezin 1 g vial ($13) IV 1 g q8h
Cefepime Maxipime 1 g vial ($95.45)
2 g vial ($190.91)
1 2 g q12h
Cefoperazone Cefobid 2 g vial ($135) 2 g q12h
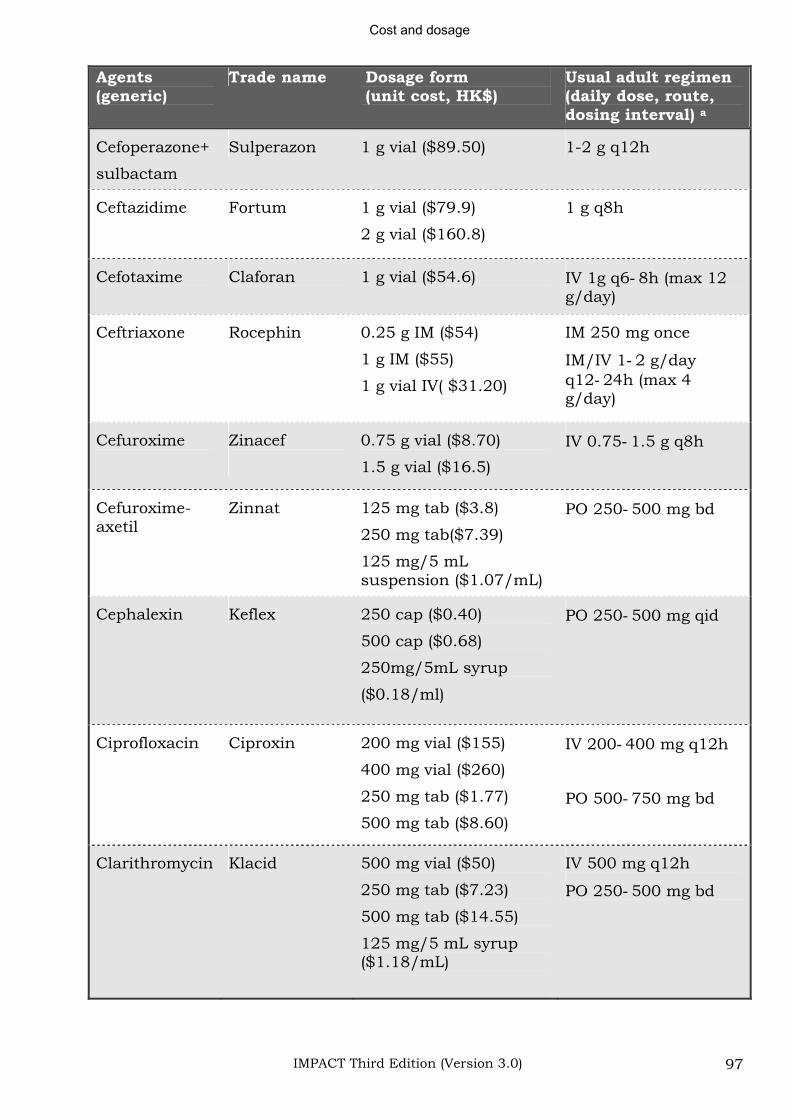
Cost and dosage
IMPACT Third Edition (Version 3.0) 97
Agents(generic)
Trade name Dosage form (unit cost, HK$)
Usual adult regimen (daily dose, route, dosing interval) a
Cefoperazone+
sulbactam
Sulperazon 1 g vial ($89.50) 1-2 g q12h
Ceftazidime Fortum 1 g vial ($79.9)
2 g vial ($160.8)
1 g q8h
Cefotaxime Claforan 1 g vial ($54.6) IV 1g q6 8h (max 12 g/day)
Ceftriaxone Rocephin 0.25 g IM ($54)
1 g IM ($55)
1 g vial IV( $31.20)
IM 250 mg once
IM/IV 1 2 g/day q12 24h (max 4 g/day)
Cefuroxime Zinacef 0.75 g vial ($8.70)
1.5 g vial ($16.5)
IV 0.75 1.5 g q8h
Cefuroxime-axetil
Zinnat 125 mg tab ($3.8)
250 mg tab($7.39)
125 mg/5 mL suspension ($1.07/mL)
PO 250 500 mg bd
Cephalexin Keflex 250 cap ($0.40)
500 cap ($0.68)
250mg/5mL syrup
($0.18/ml)
PO 250 500 mg qid
Ciprofloxacin Ciproxin 200 mg vial ($155)
400 mg vial ($260)
250 mg tab ($1.77)
500 mg tab ($8.60)
IV 200 400 mg q12h
PO 500 750 mg bd
Clarithromycin Klacid 500 mg vial ($50)
250 mg tab ($7.23)
500 mg tab ($14.55)
125 mg/5 mL syrup ($1.18/mL)
IV 500 mg q12h
PO 250 500 mg bd
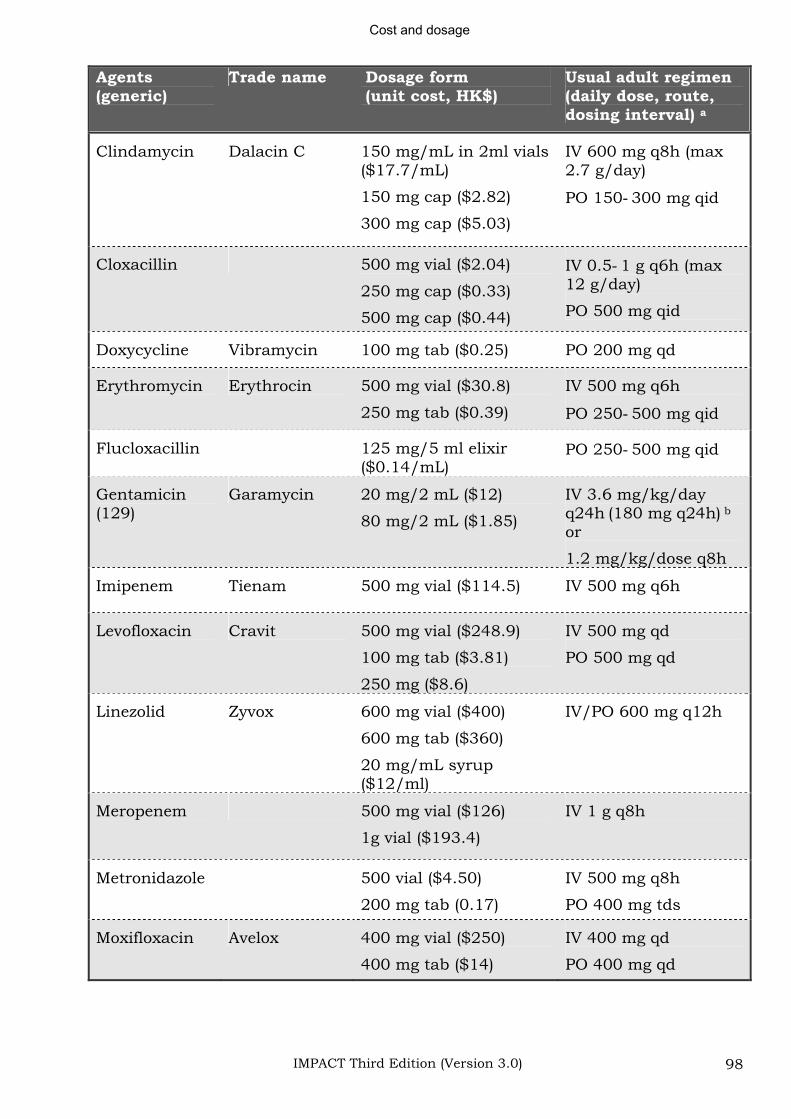
Cost and dosage
IMPACT Third Edition (Version 3.0) 98
Agents(generic)
Trade name Dosage form (unit cost, HK$)
Usual adult regimen (daily dose, route, dosing interval) a
Clindamycin Dalacin C 150 mg/mL in 2ml vials ($17.7/mL)
150 mg cap ($2.82)
300 mg cap ($5.03)
IV 600 mg q8h (max 2.7 g/day)
PO 150 300 mg qid
Cloxacillin 500 mg vial ($2.04)
250 mg cap ($0.33)
500 mg cap ($0.44)
IV 0.5 1 g q6h (max 12 g/day)
PO 500 mg qid
Doxycycline Vibramycin 100 mg tab ($0.25) PO 200 mg qd
Erythromycin Erythrocin 500 mg vial ($30.8)
250 mg tab ($0.39)
IV 500 mg q6h
PO 250 500 mg qid
Flucloxacillin 125 mg/5 ml elixir ($0.14/mL)
PO 250 500 mg qid
Gentamicin(129)
Garamycin 20 mg/2 mL ($12)
80 mg/2 mL ($1.85)
IV 3.6 mg/kg/day q24h (180 mg q24h) b
or
1.2 mg/kg/dose q8h
Imipenem Tienam 500 mg vial ($114.5) IV 500 mg q6h
Levofloxacin Cravit 500 mg vial ($248.9)
100 mg tab ($3.81)
250 mg ($8.6)
IV 500 mg qd
PO 500 mg qd
Linezolid Zyvox 600 mg vial ($400)
600 mg tab ($360)
20 mg/mL syrup ($12/ml)
IV/PO 600 mg q12h
Meropenem 500 mg vial ($126)
1g vial ($193.4)
IV 1 g q8h
Metronidazole 500 vial ($4.50)
200 mg tab (0.17)
IV 500 mg q8h
PO 400 mg tds
Moxifloxacin Avelox 400 mg vial ($250)
400 mg tab ($14)
IV 400 mg qd
PO 400 mg qd
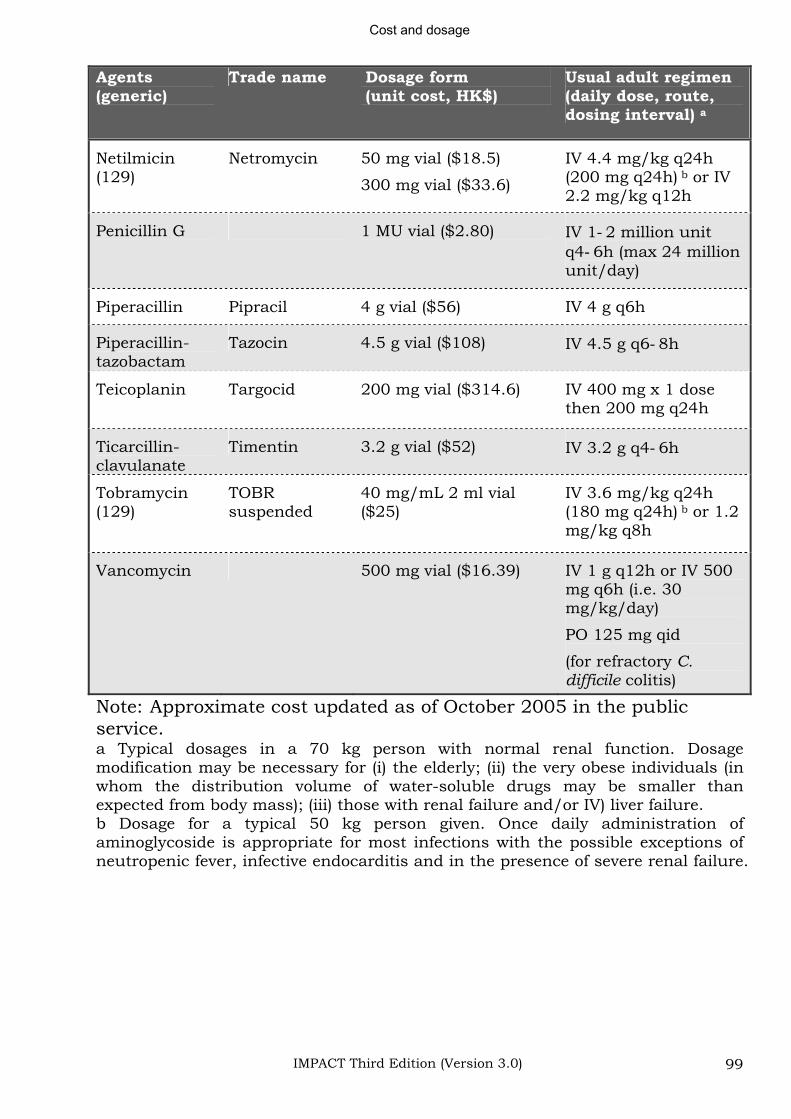
Cost and dosage
IMPACT Third Edition (Version 3.0) 99
Agents(generic)
Trade name Dosage form (unit cost, HK$)
Usual adult regimen (daily dose, route, dosing interval) a
Netilmicin(129)
Netromycin 50 mg vial ($18.5)
300 mg vial ($33.6)
IV 4.4 mg/kg q24h (200 mg q24h) b or IV 2.2 mg/kg q12h
Penicillin G 1 MU vial ($2.80) IV 1 2 million unit q4 6h (max 24 million unit/day)
Piperacillin Pipracil 4 g vial ($56) IV 4 g q6h
Piperacillin-tazobactam
Tazocin 4.5 g vial ($108) IV 4.5 g q6 8h
Teicoplanin Targocid 200 mg vial ($314.6) IV 400 mg x 1 dose then 200 mg q24h
Ticarcillin-clavulanate
Timentin 3.2 g vial ($52) IV 3.2 g q4 6h
Tobramycin (129)
TOBR suspended
40 mg/mL 2 ml vial ($25)
IV 3.6 mg/kg q24h (180 mg q24h) b or 1.2 mg/kg q8h
Vancomycin 500 mg vial ($16.39) IV 1 g q12h or IV 500 mg q6h (i.e. 30 mg/kg/day)
PO 125 mg qid
(for refractory C. difficile colitis)
Note: Approximate cost updated as of October 2005 in the public service.a Typical dosages in a 70 kg person with normal renal function. Dosage modification may be necessary for (i) the elderly; (ii) the very obese individuals (in whom the distribution volume of water-soluble drugs may be smaller than expected from body mass); (iii) those with renal failure and/or IV) liver failure. b Dosage for a typical 50 kg person given. Once daily administration of aminoglycoside is appropriate for most infections with the possible exceptions of neutropenic fever, infective endocarditis and in the presence of severe renal failure.
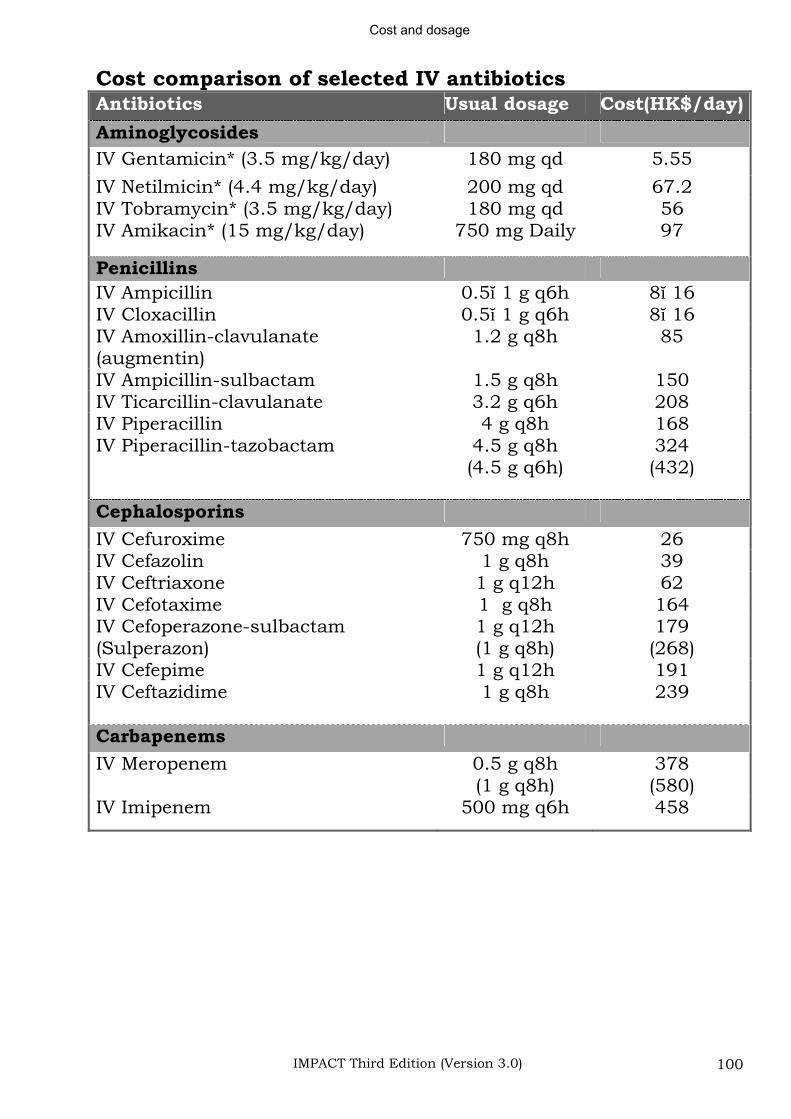
Cost and dosage
IMPACT Third Edition (Version 3.0) 100
Cost comparison of selected IV antibiotics Antibiotics Usual dosage Cost(HK$/day)
Aminoglycosides
IV Gentamicin* (3.5 mg/kg/day) 180 mg qd 5.55
IV Netilmicin* (4.4 mg/kg/day) 200 mg qd 67.2 IV Tobramycin* (3.5 mg/kg/day) 180 mg qd 56 IV Amikacin* (15 mg/kg/day) 750 mg Daily 97
Penicillins
IV Ampicillin 0.5 1 g q6h 8 16IV Cloxacillin 0.5 1 g q6h 8 16IV Amoxillin-clavulanate (augmentin)
1.2 g q8h 85
IV Ampicillin-sulbactam 1.5 g q8h 150 IV Ticarcillin-clavulanate 3.2 g q6h 208 IV Piperacillin 4 g q8h 168 IV Piperacillin-tazobactam 4.5 g q8h
(4.5 g q6h) 324(432)
Cephalosporins
IV Cefuroxime 750 mg q8h 26 IV Cefazolin 1 g q8h 39 IV Ceftriaxone 1 g q12h 62 IV Cefotaxime 1 g q8h 164 IV Cefoperazone-sulbactam (Sulperazon)
1 g q12h (1 g q8h)
179(268)
IV Cefepime 1 g q12h 191 IV Ceftazidime 1 g q8h 239
Carbapenems
IV Meropenem 0.5 g q8h (1 g q8h)
378(580)
IV Imipenem 500 mg q6h 458
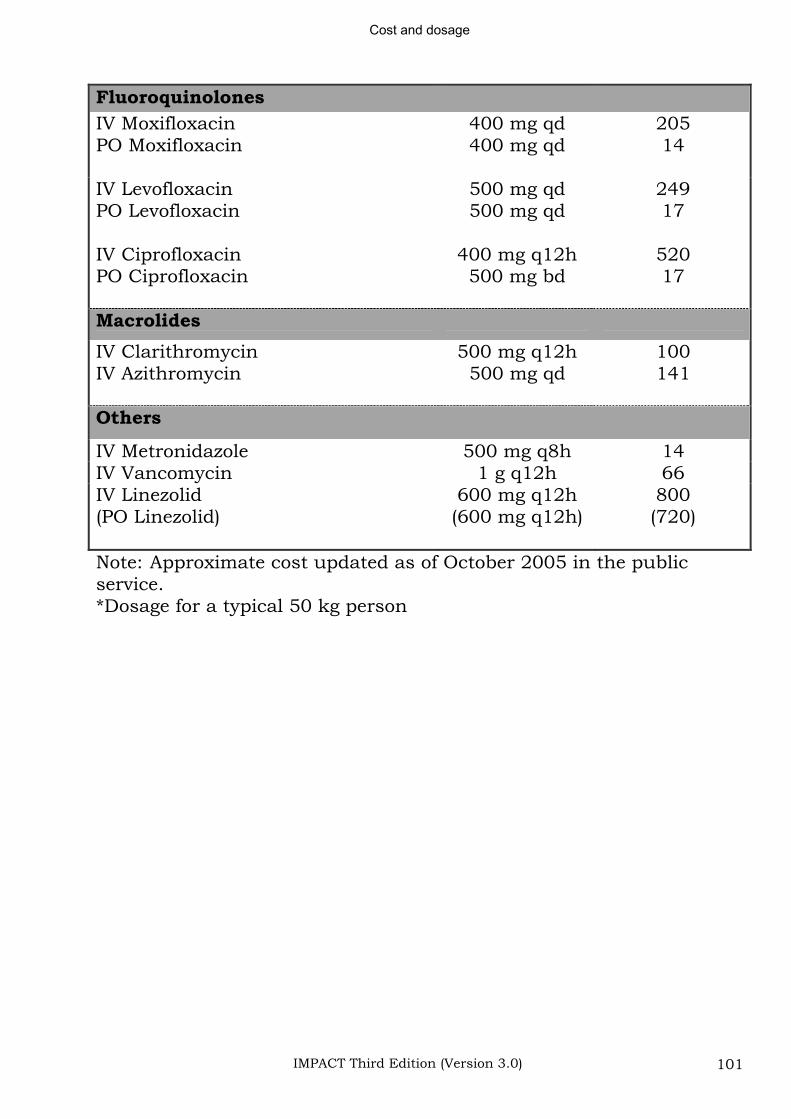
Cost and dosage
IMPACT Third Edition (Version 3.0) 101
Fluoroquinolones
IV Moxifloxacin PO Moxifloxacin
400 mg qd 400 mg qd
20514
IV LevofloxacinPO Levofloxacin
500 mg qd 500 mg qd
24917
IV Ciprofloxacin PO Ciprofloxacin
400 mg q12h 500 mg bd
52017
Macrolides
IV Clarithromycin 500 mg q12h 100 IV Azithromycin 500 mg qd 141
Others
IV Metronidazole 500 mg q8h 14 IV Vancomycin 1 g q12h 66 IV Linezolid(PO Linezolid)
600 mg q12h (600 mg q12h)
800(720)
Note: Approximate cost updated as of October 2005 in the public service. *Dosage for a typical 50 kg person
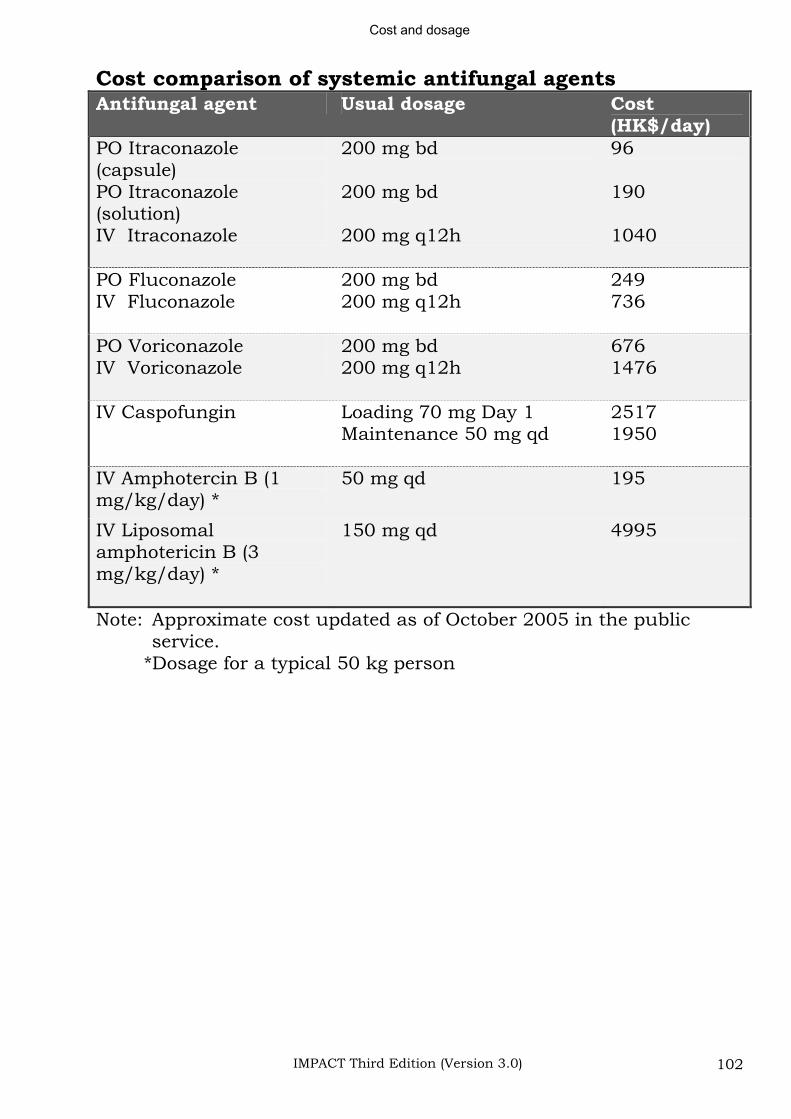
Cost and dosage
IMPACT Third Edition (Version 3.0) 102
Cost comparison of systemic antifungal agents Antifungal agent Usual dosage Cost
(HK$/day)PO Itraconazole(capsule) PO Itraconazole (solution) IV Itraconazole
200 mg bd
200 mg bd
200 mg q12h
96
190
1040
PO Fluconazole IV Fluconazole
200 mg bd 200 mg q12h
249736
PO VoriconazoleIV Voriconazole
200 mg bd 200 mg q12h
6761476
IV Caspofungin Loading 70 mg Day 1 Maintenance 50 mg qd
25171950
IV Amphotercin B (1 mg/kg/day) *
50 mg qd 195
IV Liposomal amphotericin B (3 mg/kg/day) *
150 mg qd 4995
Note: Approximate cost updated as of October 2005 in the public service.
*Dosage for a typical 50 kg person
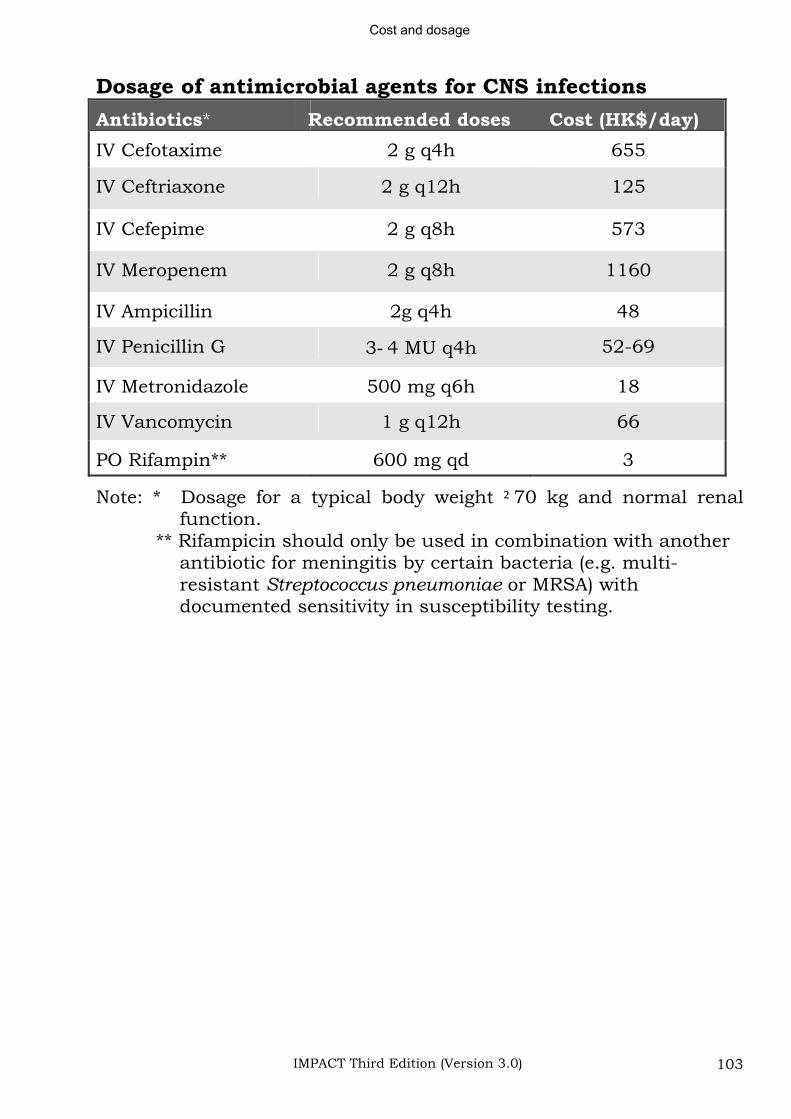
Cost and dosage
IMPACT Third Edition (Version 3.0) 103
Dosage of antimicrobial agents for CNS infections
Antibiotics* Recommended doses Cost (HK$/day)
IV Cefotaxime 2 g q4h 655
IV Ceftriaxone 2 g q12h 125
IV Cefepime 2 g q8h 573
IV Meropenem 2 g q8h 1160
IV Ampicillin 2g q4h 48
IV Penicillin G 3 4 MU q4h 52-69
IV Metronidazole 500 mg q6h 18
IV Vancomycin 1 g q12h 66
PO Rifampin** 600 mg qd 3
Note: * Dosage for a typical body weight 70 kg and normal renal function.
** Rifampicin should only be used in combination with another antibiotic for meningitis by certain bacteria (e.g. multi-resistant Streptococcus pneumoniae or MRSA) with documented sensitivity in susceptibility testing.
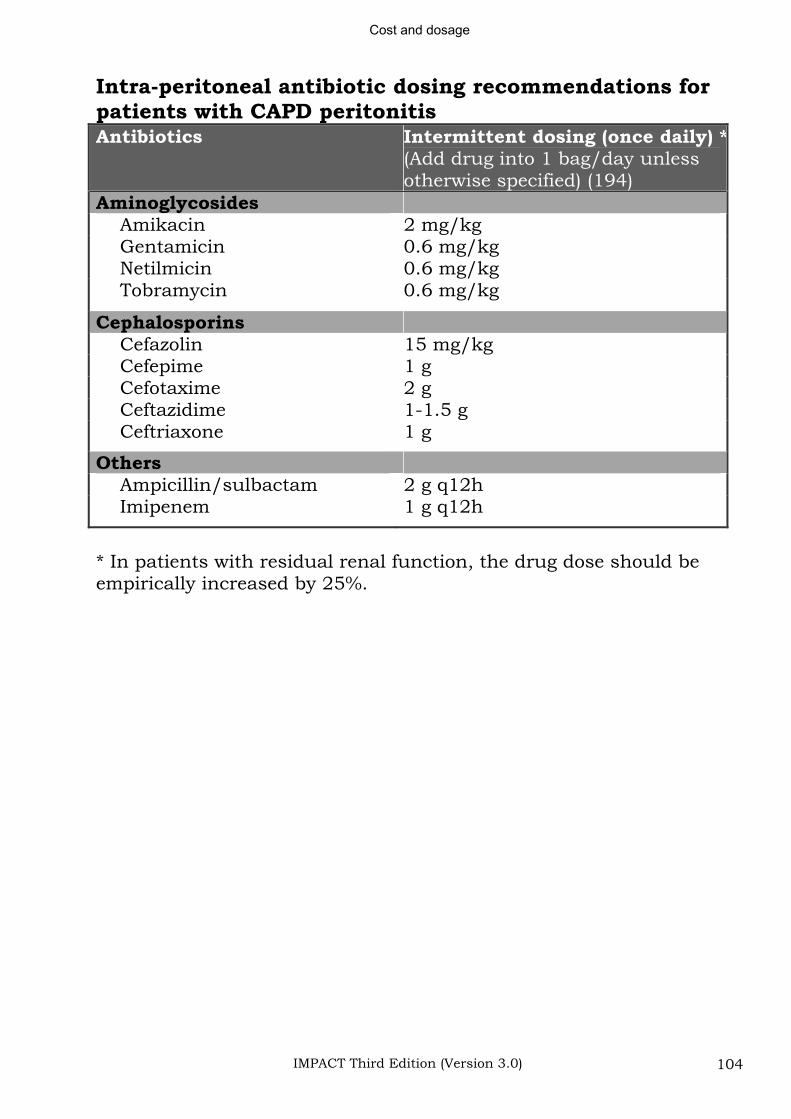
Cost and dosage
IMPACT Third Edition (Version 3.0) 104
Intra-peritoneal antibiotic dosing recommendations for patients with CAPD peritonitisAntibiotics Intermittent dosing (once daily) *
(Add drug into 1 bag/day unless otherwise specified) (194)
Aminoglycosides Amikacin 2 mg/kg Gentamicin 0.6 mg/kg Netilmicin 0.6 mg/kg Tobramycin 0.6 mg/kg
Cephalosporins Cefazolin 15 mg/kg Cefepime 1 g Cefotaxime 2 g Ceftazidime 1-1.5 g Ceftriaxone 1 g
Others Ampicillin/sulbactam 2 g q12h Imipenem 1 g q12h
* In patients with residual renal function, the drug dose should be empirically increased by 25%.
References
IMPACT Third Edition (Version 3.0) 105
Reference List References
(1) Ballow CH, Schentag JJ. Trends in antibiotic utilization and bacterial resistance. Report of the National Nosocomial Resistance Surveillance Group. Diagn Microbiol Infect Dis 1992; 15(2 Suppl):37S-42S.
(2) Cheng AF, French GL. Methicillin-resistant Staphylococcus aureus bacteraemia in Hong Kong. J HOSP INFECT 1988; 12(2):91-101.
(3) French GL, Ling J, Ling T, Hui JW. Susceptibility of Hong Kong isolates of methicillin-resistant Staphylococcus aureus to antimicrobial agents. J Antimicrob Chemother 1988; 21(5):581-588.
(4) Ho PL, Yuen KY, Yam WC, Wong SSY, Luk WK. Changing patterns of susceptibilities of blood, urinary and respiratory pathogens in Hong Kong. Journal of Hospital Infection 1995; 31(4):305-317.
(5) Kam KM, Luey KY, Fung SM, Yiu PP, Harden TJ, Cheung MM. Emergence of multiple-antibiotic-resistant Streptococcus pneumoniaein Hong Kong. Antimicrob Agents Chemother 1995; 39:12-70.
(6) Hierholzer-WJ J, Garner JS, Adams AB, Craven DE, Fleming DW, Forlenza SW et al. Recommendations for preventing the spread of vancomycin resistance: Recommendations of the Hospital Infection Control Practices Advisory Committee (HICPAC). Am J Infect Control 1995; 23(2):87-94.
(7) Song W, Moland ES, Hanson ND, Lewis JS, Jorgensen JH, Thomson KS. Failure of cefepime therapy in treatment of Klebsiella pneumoniae bacteremia. J Clin Microbiol 2005; 43(9):4891-4894.
(8) Chu YW, Afzal-Shah M, Houang ET, Palepou MI, Lyon DJ, Woodford N et al. IMP-4, a novel metallo-beta-lactamase from nosocomial Acinetobacter spp. collected in Hong Kong between 1994 and 1998. Antimicrob Agents Chemother 2001; 45(3):710-714.
(9) Adeyemi-Doro FA, Scheel O, Lyon DJ, Cheng AF. Living with methicillin-resistant Staphylococcus aureus: a 7-year experience with endemic MRSA in a university hospital. Infect Control Hosp Epidemiol 1997; 18(11):765-767.
(10) Ip M, Lyon DJ, Chio F, Enright MC, Cheng AF. Characterization of isolates of methicillin-resistant Staphylococcus aureus from Hong Kong by phage typing, pulsed-field gel electrophoresis, and fluorescent
References
IMPACT Third Edition (Version 3.0) 106
amplified-fragment length polymorphism analysis. J CLIN MICROBIOL 2003; 41(11):4980-4985.
(11) Ip M, Lyon DJ, Chio F, Cheng AF. A longitudinal analysis of methicillin-resistant Staphylococcus aureus in a Hong Kong teaching hospital. Infect Control Hosp Epidemiol 2004; 25(2):126-129.
(12) Ho PL. Carriage of methicillin resistant Staphylococcus aureus,ceftazidime resistant Gram negative bacilli and vancomycin resistant enterococci before and after intensive care units admission. Crit Care Med (in press) 2003.
(13) Zetola N, Francis JS, Nuermberger EL, Bishai WR. Community-acquired meticillin-resistant Staphylococcus aureus: an emerging threat. Lancet Infect Dis 2005; 5(5):275-286.
(14) Palavecino E. Community-acquired methicillin-resistant Staphylococcus aureus infections. Clin Lab Med 2004; 24(2):403-418.
(15) Hidron AI, Kourbatova EV, Halvosa JS, Terrell BJ, McDougal LK, Tenover FC et al. Risk factors for colonization with methicillin-resistant Staphylococcus aureus (MRSA) in patients admitted to an urban hospital: emergence of community-associated MRSA nasal carriage. Clin Infect Dis 2005; 41(2):159-166.
(16) Weber JT. Community-associated methicillin-resistant Staphylococcus aureus. Clin Infect Dis 2005; 41 Suppl 4:S269-S272.
(17) Ho PL, Tse CW, Mak GC, Chow KH, Ng TK. Community-acquired methicillin-resistant Staphylococcus aureus arrives in Hong Kong. J Antimicrob Chemother 2004; 54(4):845-846.
(18) Said-Salim B, Mathema B, Braughton K, Davis S, Sinsimer D, Eisner W et al. Differential distribution and expression of Panton-Valentine leucocidin among community-acquired methicillin-resistant Staphylococcus aureus strains. J CLIN MICROBIOL 2005; 43(7):3373-3379.
(19) Ho PL, Ng TK, Yung RW, Que TL, Yip EK, Tse CW et al. Activity of linezolid against levofloxacin-resistant Streptococcus pneumoniae,methicillin-resistant Staphylococcus aureus and vancomycin- resistant enterococci in Hong Kong. J Antimicrob Chemother 2001; 48(4):590-592.
(20) Ho PL, Chan WM, Tsang KWT, Wong SSY, Young K. Bacteremia caused by Escherichia coli producing extended-spectrum beta-lactamase: a case-control study of risk factors and outcomes. Scandinavian Journal of Infectious Diseases 2002; 34(8):567-573.
References
IMPACT Third Edition (Version 3.0) 107
(21) Ho PL, Shek RH, Chow KH, Duan RS, Mak GC, Lai EL et al. Detection and characterization of extended-spectrum beta-lactamases among bloodstream isolates of Enterobacter spp. in Hong Kong, 2000-2002. J Antimicrob Chemother 2005; 55(3):326-332.
(22) Ho PL, Ho AY, Chow KH, Wong RC, Duan RS, Ho WL et al. Occurrence and molecular analysis of extended-spectrum {beta}-lactamase-producing Proteus mirabilis in Hong Kong, 1999-2002. J Antimicrob Chemother 2005; 55(6):840-845.
(23) Ho PL, Tsang DN, Que TL, Ho M, Yuen KY. Comparison of screening methods for detection of extended-spectrum beta- lactamases and their prevalence among Escherichia coli and Klebsiella species in Hong Kong. APMIS 2000; 108(3):237-240.
(24) Goossens H. Susceptibility of multi-drug-resistant Pseudomonas aeruginosa in intensive care units: results from the European MYSTIC study group. Clin Microbiol Infect 2003; 9(9):980-983.
(25) Jones RN, Kirby JT, Beach ML, Biedenbach DJ, Pfaller MA. Geographic variations in activity of broad-spectrum beta-lactams against Pseudomonas aeruginosa: summary of the worldwide SENTRY Antimicrobial Surveillance Program (1997-2000). Diagn Microbiol Infect Dis 2002; 43(3):239-243.
(26) Fluit AC, Jones ME, Schmitz FJ, Acar J, Gupta R, Verhoef J. Antimicrobial resistance among urinary tract infection (UTI) isolates in Europe: results from the SENTRY Antimicrobial Surveillance Program 1997. Antonie Van Leeuwenhoek 2000; 77(2):147-152.
(27) Livermore DM. Of Pseudomonas, porins, pumps and carbapenems. J Antimicrob Chemother 2001; 47(3):247-250.
(28) Livermore DM. Multiple mechanisms of antimicrobial resistance in Pseudomonas aeruginosa: our worst nightmare? Clin Infect Dis 2002; 34(5):634-640.
(29) Bert F, Maubec E, Bruneau B, Berry P, Lambert-Zechovsky N. Multi-resistant Pseudomonas aeruginosa outbreak associated with contaminated tap water in a neurosurgery intensive care unit. J Hosp Infect 1998; 39(1):53-62.
(30) Douglas MW, Mulholland K, Denyer V, Gottlieb T. Multi-drug resistant Pseudomonas aeruginosa outbreak in a burns unit--an infection control study. Burns 2001; 27(2):131-135.
(31) Luzzaro F, Mantengoli E, Perilli M, Lombardi G, Orlandi V, Orsatti A et al. Dynamics of a nosocomial outbreak of multidrug-
References
IMPACT Third Edition (Version 3.0) 108
resistant Pseudomonas aeruginosa producing the PER-1 extended-spectrum beta-lactamase. J Clin Microbiol 2001; 39(5):1865-1870.
(32) Panzig B, Schroder G, Pitten FA, Grundling M. A large outbreak of multiresistant Pseudomonas aeruginosa strains in north-eastern Germany. J Antimicrob Chemother 1999; 43(3):415-418.
(33) Pellegrino FL, Teixeira LM, Carvalho Md MG, Aranha NS, Pinto DO, Mello Sampaio JL et al. Occurrence of a multidrug-resistant Pseudomonas aeruginosa clone in different hospitals in Rio de Janeiro, Brazil. J Clin Microbiol 2002; 40(7):2420-2424.
(34) Gales AC, Jones RN, Turnidge J, Rennie R, Ramphal R. Characterization of Pseudomonas aeruginosa isolates: occurrence rates, antimicrobial susceptibility patterns, and molecular typing in the global SENTRY Antimicrobial Surveillance Program, 1997-1999. Clin Infect Dis 2001; 32 Suppl 2:S146-S155.
(35) Andrade SS, Jones RN, Gales AC, Sader HS. Increasing prevalence of antimicrobial resistance among Pseudomonas aeruginosa isolates in Latin American medical centres: 5 year report of the SENTRY Antimicrobial Surveillance Program (1997-2001). J Antimicrob Chemother 2003; 52(1):140-141.
(36) Obritsch MD, Fish DN, MacLaren R, Jung R. National surveillance of antimicrobial resistance in Pseudomonas aeruginosa isolates obtained from intensive care unit patients from 1993 to 2002. Antimicrob Agents Chemother 2004; 48(12):4606-4610.
(37) Saiman L, Mehar F, Niu WW, Neu HC, Shaw KJ, Miller G et al. Antibiotic susceptibility of multiply resistant Pseudomonas aeruginosa isolated from patients with cystic fibrosis, including candidates for transplantation. Clin Infect Dis 1996; 23(3):532-537.
(38) Paramythiotou E, Lucet JC, Timsit JF, Vanjak D, Paugam-Burtz C, Trouillet JL et al. Acquisition of multidrug-resistant Pseudomonas aeruginosa in patients in intensive care units: role of antibiotics with antipseudomonal activity. Clin Infect Dis 2004; 38(5):670-677.
(39) Defez C, Fabbro-Peray P, Bouziges N, Gouby A, Mahamat A, Daures JP et al. Risk factors for multidrug-resistant Pseudomonas aeruginosa nosocomial infection. J Hosp Infect 2004; 57(3):209-216.
(40) Cao B, Wang H, Sun H, Zhu Y, Chen M. Risk factors and clinical outcomes of nosocomial multi-drug resistant Pseudomonas aeruginosa infections. J Hosp Infect 2004; 57(2):112-118.
References
IMPACT Third Edition (Version 3.0) 109
(41) Ortega B, Groeneveld AB, Schultsz C. Endemic multidrug-resistant Pseudomonas aeruginosa in critically ill patients. Infect Control Hosp Epidemiol 2004; 25(10):825-831.
(42) Oie S, Uematsu T, Sawa A, Mizuno H, Tomita M, Ishida S et al. In vitro effects of combinations of antipseudomonal agents against seven strains of multidrug-resistant Pseudomonas aeruginosa. J Antimicrob Chemother 2003; 52(6):911-914.
(43) Hamer DH. Treatment of nosocomial pneumonia and tracheobronchitis caused by multidrug-resistant Pseudomonas aeruginosa with aerosolized colistin. Am J Respir Crit Care Med 2000; 162(1):328-330.
(44) Bratu S, Quale J, Cebular S, Heddurshetti R, Landman D. Multidrug-resistant Pseudomonas aeruginosa in Brooklyn, New York: molecular epidemiology and in vitro activity of polymyxin B. Eur J Clin Microbiol Infect Dis 2005; 24(3):196-201.
(45) Falagas ME, Kasiakou SK. Colistin: the revival of polymyxins for the management of multidrug-resistant gram-negative bacterial infections. Clin Infect Dis 2005; 40(9):1333-1341.
(46) Tascini C, Gemignani G, Ferranti S, Tagliaferri E, Leonildi A, Lucarini A et al. Microbiological activity and clinical efficacy of a colistin and rifampin combination in multidrug-resistant Pseudomonas aeruginosa infections. J Chemother 2004; 16(3):282-287.
(47) Ho PL, Cheng JCF, Ching PTY, Kwan JKC, Lim WWL, Tong WCY et al. Optimizing antimicrobial prescription in hospitals by introducing an antimicrobial stewardship program in Hong Kong: consensus statement. 2005. Hong Kong Med J (in press).
(48) Simonsen GS, Tapsall JW, Allegranzi B, Talbot EA, Lazzari S. The antimicrobial resistance containment and surveillance approach-a public health tool. Bull World Health Organ 2004; 82(12):928-934.
(49) Smith RD, Coast J. Antimicrobial resistance: a global response. Bull World Health Organ 2002; 80(2):126-133.
(50) Carling PC, Fung T, Coldiron JS. Parenteral antibiotic use in acute-care hospitals: A standardized analysis of fourteen institutions. Clin Infect Dis 1999; 29(5):1189-1196.
(51) Lesch CA, Itokazu GS, Danziger LH, Weinstein RA. Multi-hospital analysis of antimicrobial usage and resistance trends. Diagn Microbiol Infect Dis 2001; 41(3):149-154.
References
IMPACT Third Edition (Version 3.0) 110
(52) Kumarasamy Y, Cadwgan T, Gillanders IA, Jappy B, Laing R, Gould IM. Optimizing antibiotic therapy-the Aberdeen experience. Clin Microbiol Infect 2003; 9(5):406-411.
(53) Kunin CM, Tupasi T, Craig WA. Use of antibiotics. A brief exposition of the problem and some tentative solutions. Ann Intern Med 1973; 79(4):555-560.
(54) Brown RB, Iannini P, Gross P, Kunkel M. Impact of initial antibiotic choice on clinical outcomes in community-acquired pneumonia: analysis of a hospital claims-made database. Chest 2003; 123(5):1503-1511.
(55) Fowler RA, Flavin KE, Barr J, Weinacker AB, Parsonnet J, Gould MK. Variability in antibiotic prescribing patterns and outcomes in patients with clinically suspected ventilator-associated pneumonia. Chest 2003; 123(3):835-844.
(56) Ho PL, Yung RWH, Tsang DN, Que TL, Ho M, Seto WH et al. Increasing resistance of Streptococcus pneumoniae to fluoroquinolones: results of a Hong Kong multi-centre study in 2000. J Antimicrob Chemother 2001.
(57) Thomas JK, Forrest A, Bhavnani SM, Hyatt JM, Cheng A, Ballow CH et al. Pharmacodynamic evaluation of factors associated with the development of bacterial resistance in acutely ill patients during therapy. Antimicrob Agents Chemother 1998; 42(3):521-527.
(58) James JS. Empty antibiotic pipeline critically endangers public: IDSA report. AIDS Treat News 2004;(404):7.
(59) Nelson R. Antibiotic development pipeline runs dry. New drugs to fight resistant organisms are not being developed, experts say. Lancet 2003; 362(9397):1726-1727.
(60) Wenzel RP. The antibiotic pipeline-challenges, costs, and values. N Engl J Med 2004; 351(6):523-526.
(61) Projan SJ. Why is big Pharma getting out of antibacterial drug discovery? Curr Opin Microbiol 2003; 6(5):427-430.
(62) Gerding DN. The search for good antimicrobial stewardship. Joint Commission J Qual Improv 2001; 27:403-404.
(63) Cauffman JG, Forsyth RA, Clark VA, Foster JP, Martin KJ, Lapsys FX et al. Randomized controlled trials of continuing medical education: what makes them most effective? J Contin Educ Health Prof 2002; 22(4):214-221.
References
IMPACT Third Edition (Version 3.0) 111
(64) Thomson O'Brien MA, Oxman AD, Davis DA, Haynes RB, Freemantle N, Harvey EL. Audit and feedback: effects on professional practice and health care outcomes. Cochrane Database Syst Rev 2000;(2):CD000259.
(65) Bell DM. Promoting appropriate antimicrobial drug use: perspective from the Centers for Disease Control and Prevention. Clin Infect Dis 2001; 33 Suppl 3:S245-S250.
(66) Bell DM. Development of the public health action plan to combat antimicrobial resistance and the CDC activities related to its implementation. In: Knobler SL, Lemon SM, Najafi M, Burroughs T, editors. The Resistance Phenomenon in Microbes and Infectious Diseases Vectors: Implications for Human Health and Stretegies for Containment:Workshop Summary. Washington, DC: National Academy Press, 2003: 198-206.
(67) Department of Health. Hospital pharmacy initiative for promoting prudent use of antibiotics in hospitals. 2003. London, Department of Health.
(68) Burke JP. Antibiotic resistance-squeezing the balloon? JAMA 1998; 280(14):1270-1271.
(69) Livermore D. Can better prescribing turn the tide of resistance? Nat Rev Microbiol 2004; 2(1):73-78.
(70) IMPACT working group. Reducing bacterial resistance with IMPACT: Interhospital Multi-disciplinary Programme on Antimicrobial ChemoTherapy. 2nd ed. Centre of Infection, The University of Hong Kong, 2003.
(71) Ho PL. Antibiotic guidelines and optimization programme. In: Yuen KY, Wong SY, editors. Infectious diseases update: course 6. Centre of Infection, University of Hong Kong, 2004: 1-110.
(72) Wang TKF, Ho PL. The challenge of antibiotic resistance in Asia: problems and solutions. Medical Progress 2003; 30:41-48.
(73) Department of Health. Winning ways: working together to reduce healthcare associated infection in England. Report from the chief medical officer. 2003. London, Department of Health.
(74) Bantar C, Sartori B, Vesco E, Heft C, Saul M, Salamone F et al. A hospitalwide intervention program to optimize the quality of antibiotic use: impact on prescribing practice, antibiotic consumption, cost savings, and bacterial resistance. Clin Infect Dis 2003; 37(2):180-186.
References
IMPACT Third Edition (Version 3.0) 112
(75) Carling P, Fung T, Killion A, Terrin N, Barza M. Favorable impact of a multidisciplinary antibiotic management program conducted during 7 years. Infect Control Hosp Epidemiol 2003; 24(9):699-706.
(76) Gould IM. Stewardship of antibiotic use and resistance surveillance: the international scene. J Hosp Infect 1999; 43 Suppl:S253-S260.
(77) Gross R, Morgan AS, Kinky DE, Weiner M, Gibson GA, Fishman NO. Impact of a hospital-based antimicrobial management program on clinical and economic outcomes. Clin Infect Dis 2001; 33(3):289-295.
(78) Keuleyan E, Gould M. Key issues in developing antibiotic policies: from an institutional level to Europe-wide. European Study Group on Antibiotic Policy (ESGAP), Subgroup III. Clin Microbiol Infect 2001; 7 Suppl 6:16-21.
(79) Masterson RG. Antibiotic policies and the role of strategic hospital leadership. J Hosp Infect 1999; 43 Suppl:S261-S264.
(80) Owens RC, Jr., Fraser GL, Stogsdill P. Antimicrobial stewardship programs as a means to optimize antimicrobial use. Insights from the Society of Infectious Diseases Pharmacists. Pharmacotherapy 2004; 24(7):896-908.
(81) Ruttimann S, Keck B, Hartmeier C, Maetzel A, Bucher HC. Long-term antibiotic cost savings from a comprehensive intervention program in a medical department of a university-affiliated teaching hospital. Clin Infect Dis 2004; 38(3):348-356.
(82) Goldmann DA. Resistance movement: the antibiotic crisis in hospitals. Health Syst Rev 1997; 30(1):20-24.
(83) Kumana CR, Ching TY, Kong Y, Ma EC, Kou M, Lee RA et al. Curtailing unnecessary vancomycin usage in a hospital with high rates of methicillin resistant Staphylococcus aureus infections. Br J Clin Pharmacol 2001; 52(4):427-432.
(84) LaRocco A, Jr. Concurrent antibiotic review programs--a role for infectious diseases specialists at small community hospitals. Clin Infect Dis 2003; 37(5):742-743.
(85) McGowan JE, Jr. Minimizing antimicrobial resistance: the key role of the infectious diseases physician. Clin Infect Dis 2004; 38(7):939-942.
(86) White-AC J, Atmar RL, Wilson J, Cate TR, Stager CE, Greenberg SB. Effects of requiring prior authorization for selected antimicrobials:
References
IMPACT Third Edition (Version 3.0) 113
expenditures, susceptibilities, and clinical outcomes. Clin Infect Dis 1997; 25(2):230-239.
(87) Anglim AM, Klym B, Byers KE, Scheld WM, Farr BM. Effect of a vancomycin restriction policy on ordering practices during an outbreak of vancomycin-resistant Enterococcus faecium. Arch Intern Med 1997; 157(10):1132-1136.
(88) Bradley JS. Antibiotic restriction in the pediatric intensive care unit: now worthless? Crit Care Med 1998; 26(11):1790-1791.
(89) Conly J, Shafran S. Antimicrobial stewardship. Can J Infect Dis 1997;(6):315-316.
(90) Conly J. State of the art in antimicrobial stewardship in Canadian acute institutions. Can J Infect Dis 1998; 9 (Suppl C):4-6.
(91) Gross PA. The potential for clinical guidelines to impact appropriate antimicrobial agent use. Infectious Disease Clinics of North America 1997; 11(4):803-&.
(92) Quale J, Landman D, Saurina G, Atwood E, DiTore V, Patel K. Manipulation of a hospital antimicrobial formulary to control an outbreak of vancomycin-resistant enterococci. Clin Infect Dis 1996; 23(5):1020-1025.
(93) Record KE, Dickens GR, Amerson AB, Rapp RP. Implementation of a criteria-based antimicrobial formulary system. Am J Health Syst Pharm 1995; 52(6 Suppl 2):S34-S38.
(94) Shlaes DM, Gerding DN, John-JF J, Craig WA, Bornstein DL, Duncan RA et al. Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the Prevention of Antimicrobial Resistance: guidelines for the prevention of antimicrobial resistance in hospitals. Clin Infect Dis 1997; 25(3):584-599.
(95) White-AC J, Atmar RL, Cate TR, Greenberg SR. Enforcing antimicrobial restrictions. Am J Health Syst Pharm 1996; 53(7):796-797.
(96) Wong SS, Woo PC, Ho PL, Cheng CC, Yuen KY. Emergence of Streptococcus pneumoniae with high level resistance to cefotaxime in Hong Kong. Hong Kong Med J 1999; 5:406-409.
(97) George RC, Uttley AH. Susceptibility of enterococci and epidemiology of enterococcal infection in the 1980s. Epidemiol Infect 1989; 103(3):403-413.
References
IMPACT Third Edition (Version 3.0) 114
(98) Golledge CL, McKenzie T, Riley TV. Extended spectrum cephalosporins and Clostridium difficile. J Antimicrob Chemother 1989; 23(6):929-931.
(99) Moreno F, Grota P, Crisp C, Magnon K, Melcher GP, Jorgensen JH et al. Clinical and molecular epidemiology of vancomycin-resistant Enterococcus faecium during its emergence in a city in southern Texas. Clin Infect Dis 1995; 21(5):1234-1237.
(100) Tornieporth NG, Roberts RB, John J, Hafner A, Riley LW. Risk factors associated with vancomycin-resistant Enterococcus faecium infection or colonization in 145 matched case patients and control patients. Clin Infect Dis 1996; 23(4):767-772.
(101) Follath F, Costa E, Thommen A, Frei R, Burdeska A, Meyer J. Clinical consequences of development of resistance to third generation cephalosporins. Eur J Clin Microbiol 1987; 6(4):446-450.
(102) Chow JW, Fine MJ, Shlaes DM, Quinn JP, Hooper DC, Johnson MP et al. Enterobacter bacteremia: clinical features and emergence of antibiotic resistance during therapy. Ann Intern Med 1991; 115(8):585-590.
(103) Jones RN, et a. Inducible beta-lactamase-mediated resistance to third-generation cephalosporins. Clin Microbiol Infect 1997; 3 (S1):S7-S20.
(104) Widmer AF. Replace hand washing with use of a waterless alcohol hand rub? Clin Infect Dis 2000; 31(1):136-143.
(105) Piroth L, Aube H, Doise JM, Vincent MM. Spread of extended-spectrum beta-lactamase-producing Klebsiella pneumoniae: are beta-lactamase inhibitors of therapeutic value? Clin Infect Dis 1998; 27(1):76-80.
(106) Bradley SJ, Wilson AL, Allen MC, Sher HA, Goldstone AH, Scott GM. The control of hyperendemic glycopeptide-resistant Enterococcus spp. on a haematology unit by changing antibiotic usage. J Antimicrob Chemother 1999; 43(2):261-266.
(107) Rice LB. Emergence of vancomycin-resistant enterococci. Emerg Infect Dis 2001; 7(2):183-187.
(108) Rice LB, Eckstein EC, DeVente J, Shlaes DM. Ceftazidime-resistant Klebsiella pneumoniae isolates recovered at the Cleveland Department of Veterans Affairs Medical Center. Clin Infect Dis 1996; 23(1):118-124.
References
IMPACT Third Edition (Version 3.0) 115
(109) Landman D, Chockalingam M, Quale JM. Reduction in the incidence of methicillin-resistant Staphylococcus aureus and ceftazidime-resistant Klebsiella pneumoniae following changes in a hospital antibiotic formulary. Clin Infect Dis 1999; 28(5):1062-1066.
(110) Meyer KS, Urban C, Eagan JA, Berger BJ, Rahal JJ. Nosocomial outbreak of Klebsiella infection resistant to late- generation cephalosporins. Ann Intern Med 1993; 119(5):353-358.
(111) Pena C, Pujol M, Ardanuy C, Ricart A, Pallares R, Linares J et al. Epidemiology and successful control of a large outbreak due to Klebsiella pneumoniae producing extended-spectrum beta-lactamases. Antimicrob Agents Chemother 1998; 42(1):53-58.
(112) Rahal JJ, Urban C, Horn D, Freeman K, Segal MS, Maurer J et al. Class restriction of cephalosporin use to control total cephalosporin resistance in nosocomial Klebsiella . JAMA 1998; 280(14):1233-1237.
(113) Patterson JE, Hardin TC, Kelly CA, Garcia RC, Jorgensen JH. Association of antibiotic utilization measures and control of multiple- drug resistance in Klebsiella pneumoniae. Infect Control Hosp Epidemiol 2000; 21(7):455-458.
(114) Ahkee S, Smith S, Newman D, Ritter W, Burke J, Ramirez JA. Early switch from intravenous to oral antibiotics in hospitalized patients with infections: a 6-month prospective study. Pharmacotherapy 1997; 17(3):569-575.
(115) Ramirez JA, Bordon J. Early switch from intravenous to oral antibiotics in hospitalized patients with bacteremic community-acquired Streptococcus pneumoniae pneumonia. Arch Intern Med 2001; 161(6):848-850.
(116) Ramirez JA, Srinath L, Ahkee S, Huang A, Raff MJ. Early switch from intravenous to oral cephalosporins in the treatment of hospitalized patients with community-acquired pneumonia. Arch Intern Med 1995; 155(12):1273-1276.
(117) Ramirez JA. Switch therapy with beta-lactam/beta-lactamase inhibitors in patients with community-acquired pneumonia. Ann Pharmacother 1998; 32(1):S22-S26.
(118) Finkelstein R, Rabino G, Mashiah T, Bar-El Y, Adler Z, Kertzman V et al. Vancomycin versus cefazolin prophylaxis for cardiac surgery in the setting of a high prevalence of methicillin-resistant staphylococcal infections. J Thorac Cardiovasc Surg 2002; 123(2):326-332.
References
IMPACT Third Edition (Version 3.0) 116
(119) Pea F, Porreca L, Baraldo M, Furlanut M. High vancomycin dosage regimens required by intensive care unit patients cotreated with drugs to improve haemodynamics following cardiac surgical procedures. J Antimicrob Chemother 2000; 45(3):329-335.
(120) Rice TL. Simplified dosing and monitoring of vancomycin for the burn care clinician. Burns 1992; 18(5):355-361.
(121) Bauer LA, Black DJ, Lill JS. Vancomycin dosing in morbidly obese patients. Eur J Clin Pharmacol 1998; 54(8):621-625.
(122) Griver AR, Prince RA, Darouiche RO. A simple method for administering vancomycin in the spinal cord injured population. Arch Phys Med Rehabil 1997; 78(5):459-462.
(123) American Thoracic Society. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 2005; 171(4):388-416.
(124) Begg EJ, Barclay ML, Kirkpatrick CJ. The therapeutic monitoring of antimicrobial agents. Br J Clin Pharmacol 1999; 47(1):23-30.
(125) Bearden DT, Rodvold KA. Dosage adjustments for antibacterials in obese patients: applying clinical pharmacokinetics. Clin Pharmacokinet 2000; 38(5):415-426.
(126) Blouin RA, Bauer LA, Miller DD, Record KE, Griffen WO, Jr. Vancomycin pharmacokinetics in normal and morbidly obese subjects. Antimicrob Agents Chemother 1982; 21(4):575-580.
(127) Kumana CR, Chau PY, French GL. Antibiotic guidelines. 1st ed. Science press, 1999.
(128) Hughes WT, Armstrong D, Bodey GP, Bow EJ, Brown AE, Calandra T et al. 2002 guidelines for the use of antimicrobial agents in neutropenic patients with cancer. Clin Infect Dis 2002; 34(6):730-751.
(129) Kumana CR, Yuen KY. Parenteral aminoglycoside therapy. Selection, administration and monitoring. Drugs 1994; 47(6):902-913.
(130) Nicolau DP, Freeman CD, Belliveau PP, Nightingale CH, Ross JW, Quintiliani R. Experience with A Once-Daily Aminoglycoside Program Administered to 2,184 Adult Patients. Antimicrob Agents Chemother 1995; 39(3):650-655.
(131) Nicolau DP, Wu AH, Finocchiaro S, Udeh E, Chow MS, Quintiliani R et al. Once-daily aminoglycoside dosing: impact on
References
IMPACT Third Edition (Version 3.0) 117
requests and costs for therapeutic drug monitoring. Ther Drug Monit 1996; 18(3):263-266.
(132) Paterson DL, Robson JM, Wagener MM, Peters M. Monitoring of serum aminoglycoside levels with once-daily dosing. Pathology 1998; 30(3):289-294.
(133) Espinel-Ingroff A, Boyle K, Sheehan DJ. In vitro antifungal activities of voriconazole and reference agents as determined by NCCLS methods: review of the literature. Mycopathologia 2001; 150(3):101-115.
(134) Pfaller MA, Messer SA, Hollis RJ, Jones RN, Doern GV, Brandt ME et al. In vitro susceptibilities of Candida bloodstream isolates to the new triazole antifungal agents BMS-207147, Sch 56592, and voriconazole. Antimicrob Agents Chemother 1998; 42(12):3242-3244.
(135) Pfaller MA, Messer SA, Gee S, Joly S, Pujol C, Sullivan DJ et al. In vitro susceptibilities of Candida dubliniensis isolates tested against the new triazole and echinocandin antifungal agents. J Clin Microbiol 1999; 37(3):870-872.
(136) Mora-Duarte J, Betts R, Rotstein C, Colombo AL, Thompson-Moya L, Smietana J et al. Comparison of caspofungin and amphotericin B for invasive candidiasis. N Engl J Med 2002; 347(25):2020-2029.
(137) Herbrecht R, Denning DW, Patterson TF, Bennett JE, Greene RE, Oestmann JW et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med 2002; 347(6):408-415.
(138) Grayson ML, Gibbons GW, Habershaw GM, Freeman DV, Pomposelli FB, Rosenblum BI et al. Use of ampicillin/sulbactam versus imipenem/cilastatin in the treatment of limb-threatening foot infections in diabetic patients. Clin Infect Dis 1994; 18(5):683-693.
(139) Tang WM, Ho PL, Fung KK, Yuen KY, Leong JC. Necrotising fasciitis of a limb. J Bone Joint Surg Br 2001; 83(5):709-714.
(140) Kaul R, McGeer A, Norrby-Teglund A, Kotb M, Schwartz B, O'Rourke K et al. Intravenous immunoglobulin therapy for streptococcal toxic shock syndrome--a comparative observational study. The Canadian Streptococcal Study Group. Clin Infect Dis 1999; 28(4):800-807.
(141) Fleisher GR. The management of bite wounds. N Engl J Med 1999; 340(2):138-140.
References
IMPACT Third Edition (Version 3.0) 118
(142) de Gans J, van de BD. Dexamethasone in adults with bacterial meningitis. N Engl J Med 2002; 347(20):1549-1556.
(143) Tunkel AR, Hartman BJ, Kaplan SL, Kaufman BA, Roos KL, Scheld WM et al. Practice guidelines for the management of bacterial meningitis. Clin Infect Dis 2004; 39(9):1267-1284.
(144) Ip M, Lyon DJ, Yung RWH, Chan C, Cheng AF. Evidence of clonal dssemination of multidrug-resistant Streptococcus pneumoniaein Hong Kong. J Clin Microbiol 1999; 37:2834-2839.
(145) Baddour LM, Wilson WR, Bayer AS, Fowler VG, Jr., Bolger AF, Levison ME et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the committee on rheumatic Fever, endocarditis, and kawasaki disease, council on cardiovascular disease in the young, and the councils on clinical cardiology, stroke, and cardiovascular surgery and anesthesia, american heart association--executive summary: endorsed by the infectious diseases society of america. Circulation 2005; 111(23):3167-3184.
(146) Berbari EF, Cockerill FR, III, Steckelberg JM. Infective endocarditis due to unusual or fastidious microorganisms. Mayo Clin Proc 1997; 72(6):532-542.
(147) Sande MA, Kartalija M, Anderson JL. Infective endocarditis. In: Fuster V, editor. Hurst's the heart. McGraw-Haill Medical Publishing, 2001: 2087-2128.
(148) Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2002. MMWR Recomm Rep 2002; 51(RR-6):1-78.
(149) Walker CK, Workowski KA, Washington AE, Soper D, Sweet RL. Anaerobes in pelvic inflammatory disease: implications for the Centers for Disease Control and Prevention's guidelines for treatment of sexually transmitted diseases. Clin Infect Dis 1999; 28 Suppl 1S29-36 *LHM:Click.
(150) Grossman RF. Guidelines for the treatment of acute exacerbations of chronic bronchitis. Chest 1997; 112(6 Suppl):310S-313S.
(151) McCrory DC, Brown C, Gelfand SE, Bach PB. Management of acute exacerbations of COPD: a summary and appraisal of published evidence. Chest 2001; 119(4):1190-1209.
References
IMPACT Third Edition (Version 3.0) 119
(152) Schentag JJ, Tillotson GS. Antibiotic selection and dosing for the treatment of acute exacerbations of COPD. Chest 1997; 112(6 Suppl):314S-319S.
(153) Tsang KW, Chan WM, Ho PL, Chan K, Lam WK, Ip MS. A comparative study on the efficacy of levofloxacin and ceftazidime in acute exacerbation of bronchiectasis. Eur Respir J 1999; 14(5):1206-1209.
(154) Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 2005; 171(4):388-416.
(155) Ho PL, Que TL, Tsang DN, Ng TK, Chow KH, Seto WH. Emergence of fluoroquinolone resistance among multiply resistant strains of Streptococcus pneumoniae in Hong Kong. Antimicrob Agents Chemother 1999; 43(5):1310-1313.
(156) Ho PL, Yam WC, Que TL, Tsang DN, Seto WH, Ng TK et al. Target site modifications and efflux phenotype in clinical isolates of Streptococcus pneumoniae from Hong Kong with reduced susceptibility to fluoroquinolones. J Antimicrob Chemother 2001; 47(5):655-658.
(157) Bartlett JG, Dowell SF, Mandell LA, File Jr TM, Musher DM, Fine MJ. Practice guidelines for the management of community-acquired pneumonia in adults. Infectious Diseases Society of America. Clin Infect Dis 2000; 31(2):347-382.
(158) Brown EM. Empirical antimicrobial therapy of mechanically ventilated patients with nosocomial pneumonia. J Antimicrob Chemother 1997; 40(4):463-468.
(159) Defining the group A streptococcal toxic shock syndrome. Rationale and consensus definition. The Working Group on Severe Streptococcal Infections. JAMA 1993; 269(3):390-391.
(160) Bradley EL, III. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993; 128(5):586-590.
(161) Papachristou GI, Whitcomb DC. Inflammatory markers of disease severity in acute pancreatitis. Clin Lab Med 2005; 25(1):17-37.
(162) Dervenis C, Johnson CD, Bassi C, Bradley E, Imrie CW, McMahon MJ et al. Diagnosis, objective assessment of severity, and management of acute pancreatitis. Santorini consensus conference. Int J Pancreatol 1999; 25(3):195-210.
References
IMPACT Third Edition (Version 3.0) 120
(163) Golub R, Siddiqi F, Pohl D. Role of antibiotics in acute pancreatitis: A meta-analysis. J Gastrointest Surg 1998; 2(6):496-503.
(164) Sharma VK, Howden CW. Prophylactic antibiotic administration reduces sepsis and mortality in acute necrotizing pancreatitis: a meta-analysis. Pancreas 2001; 22(1):28-31.
(165) Toouli J, Brooke-Smith M, Bassi C, Carr-Locke D, Telford J, Freeny P et al. Guidelines for the management of acute pancreatitis. J Gastroenterol Hepatol 2002; 17 Suppl:S15-S39.
(166) Uhl W, Warshaw A, Imrie C, Bassi C, McKay CJ, Lankisch PG et al. IAP Guidelines for the Surgical Management of Acute Pancreatitis. Pancreatology 2002; 2(6):565-573.
(167) Barie PS. A critical review of antibiotic prophylaxis in severe acute pancreatitis. Am J Surg 1996; 172(6A):38S-43S.
(168) Bassi C, Larvin M, Villatoro E. Antibiotic therapy for prophylaxis against infection of pancreatic necrosis in acute pancreatitis. Cochrane Database Syst Rev 2003;(4):CD002941.
(169) Swaroop VS, Chari ST, Clain JE. Severe acute pancreatitis. JAMA 2004; 291(23):2865-2868.
(170) De Waele JJ, Vogelaers D, Hoste E, Blot S, Colardyn F. Emergence of antibiotic resistance in infected pancreatic necrosis. Arch Surg 2004; 139(12):1371-1375.
(171) Yousaf M, McCallion K, Diamond T. Management of severe acute pancreatitis. Br J Surg 2003; 90(4):407-420.
(172) Mandell LA, Marrie TJ, Grossman RF, Chow AW, Hyland RH. Canadian guidelines for the initial management of community-acquired pneumonia: an evidence-based update by the Canadian Infectious Diseases Society and the Canadian Thoracic Society. The Canadian Community- Acquired Pneumonia Working Group. Clin Infect Dis 2000; 31(2):383-421.
(173) Niederman MS, Mandell LA, Anzueto A, Bass JB, Broughton WA, Campbell GD et al. Guidelines for the Management of Adults with Community-acquired Pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med 2001; 163(7):1730-1754.
(174) Meehan TP, Fine MJ, Krumholz HM, Scinto JD, Galusha DH, Mockalis JT et al. Quality of care, process, and outcomes in elderly patients with pneumonia. JAMA 1997; 278(23):2080-2084.
References
IMPACT Third Edition (Version 3.0) 121
(175) Friedland IR. Comparison of the response to antimicrobial therapy of penicillin-resistant and penicillin-susceptible pneumococcal disease. Pediatr Infect Dis J 1995; 14(10):885-890.
(176) Pallares R, Linares J, Vadillo M, Cabellos C, Manresa F, Viladrich PF et al. Resistance to penicillin and cephalosporin and mortality from severe pneumococcal pneumonia in Barcelona, Spain [see comments] [published erratum appears in N Engl J Med 1995 Dec 14;333(24):1655]. N Engl J Med 1995; 333(8):474-480.
(177) Metlay JP, Hofmann J, Cetron MS, Fine MJ, Farley MM, Whitney C et al. Impact of penicillin susceptibility on medical outcomes for adult patients with bacteremic pneumococcal pneumonia. Clin Infect Dis 2000; 30(3):520-528.
(178) Turett GS, Blum S, Fazal BA, Justman JE, Telzak EE. Penicillin resistance and other predictors of mortality in pneumococcal bacteremia in a population with high human immunodeficiency virus seroprevalence. Clin Infect Dis 1999; 29(2):321-327.
(179) Feikin DR, Schuchat A, Kolczak M, Barrett NL, Harrison LH, Lefkowitz L et al. Mortality from invasive pneumococcal pneumonia in the era of antibiotic resistance, 1995-1997. Am J Public Health 2000; 90(2):223-229.
(180) Boost MV, O'Donoghue MM, Dooley JS. Prevalence of carriage of antimicrobial resistant strains of Streptococcus pneumoniae in primary school children in Hong Kong. Epidemiol Infect 2001; 127(1):49-55.
(181) Chiu SS, Ho PL, Chow FKH, Yuen KY, Lau YL. Nasopharyngeal carriage of antimicrobial-resistant Streptococcus pneumoniae among young children attending 79 kindergartens and day care centers in Hong Kong. Antimicrob Agents Chemother 2001; 45(10):2765-2770.
(182) Lyon DJ, Scheel O, Fung KS, Cheng AF, Henrichsen J. Rapid emergence of penicillin-resistant pneumococci in Hong Kong. Scand J Infect Dis 1996; 28(4):375-376.
(183) Clincal and Laboratory Standard Institute (National Committee for Clinical Laboratory Standards). Performance standards for antimicrobial susceptibility testing: fifteen informational supplement. Wayne, Pa, National Committee for Clinical Laboratory Standards, 2005.
References
IMPACT Third Edition (Version 3.0) 122
(184) Sterling TR. The WHO/IUATLD diagnostic algorithm for tuberculosis and empiric fluoroquinolone use: potential pitfalls. Int J Tuberc Lung Dis 2004; 8(12):1396-1400.
(185) Dooley KE, Golub J, Goes FS, Merz WG, Sterling TR. Empiric treatment of community-acquired pneumonia with fluoroquinolones, and delays in the treatment of tuberculosis. Clin Infect Dis 2002; 34(12):1607-1612.
(186) Ho PL, Tse WS, Tsang KW, Kwok TK, Ng TK, Cheng VC et al. Risk Factors for Acquisition of Levofloxacin-Resistant Streptococcus pneumoniae: A Case-Control Study. Clin Infect Dis 2001; 32(5):701-707.
(187) Odenholt I, Cars O, Lowdin E. Pharmacodynamic studies of amoxicillin against Streptococcus pneumoniae: comparison of a new pharmacokinetically enhanced formulation (2000 mg twice daily) with standard dosage regimens. J Antimicrob Chemother 2004; 54(6):1062-1066.
(188) National Committee for Clinical Laboratory Standards. Performance standards for antimicrobial susceptibility testing: eleventh informational supplement. Wayne, Pa: National Committee for Clinical Laboratory Standards, 2001.
(189) Bratzler DW, Houck PM. Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. Am J Surg 2005; 189(4):395-404.
(190) Anonymous. ASHP Therapeutic Guidelines on Antimicrobial Prophylaxis in Surgery. American Society of Health-System Pharmacists. Am J Health Syst Pharm 1999; 56(18):1839-1888.
(191) Anonymous. Antimicrobial prophylaxis in surgery. Med Lett Drugs Ther 2001; 43(1116-1117):92-97.
(192) Bratzler DW, Houck PM. Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. Clin Infect Dis 2004; 38(12):1706-1715.
(193) Muto CA, Jernigan JA, Ostrowsky BE, Richet HM, Jarvis WR, Boyce JM et al. SHEA guideline for preventing nosocomial transmission of multidrug-resistant strains of Staphylococcus aureus and enterococcus. Infect Control Hosp Epidemiol 2003; 24(5):362-386.
(194) Piraino B, Bailie GR, Bernardini J, Boeschoten E, Gupta A, Holmes C et al. Peritoneal dialysis-related infections recommendations: 2005 update. Perit Dial Int 2005; 25(2):107-131.
Abbreviations
IMPACT Third Edition (Version 3.0) 123
Abbreviations
3GC Third generation cephalosporins
AACP American Association of Colleges of Pharmacy
ACP-ASIM American College of Physicians- American Society of Internal Medicine
AECB Acute exacerbation of chronic bronchitis
APUA Alliance for the Prudent Use of Antibiotics
ASP Antimicrobial stewardship programme
bd Twice daily
BLBLI Beta-lactam/beta-lactamase inhibitor
CA-MRSA Community acquired methicillin resistant Staphylococcal aureus
CAP Community acquired pneumonia
cap/caps Capsule/capsules
CDC Centers for Disease Control and Prevention
CLIS Clinical and Labortory Standards Institute
COPD Chronic obstructive pulmonary disease
CRHD Chronic rheumatic heart disease
CRKP Ceftazidime-resistant Klebsiella pneumoniae
CT Computerised tomography
D5 5% dextrose solution
DDD Defined daily dose
DRSP Drug resistant Streptococcus pneumoniae
ESBL Extended-spectrum beta lactamase
ET Empirical therapy
FDA Food and Drug Administration
FNA Fine needle aspiration
HA-MRSA Healthcare associated methicillin resistant Staphylococcus aureu
HACEK Hemophilus parainfluenzae, H. aphropilus, Actinobacillus, Cardiobacterium, Eikenella,
Abbreviations
IMPACT Third Edition (Version 3.0) 124
Kingella IBW Ideal body weight
IDSA Infectious Diseases Society of America
IE Infective endocarditis
IM Intramuscular
IV Intravenous
IVDA Intravenous drug abuser
KPT Known-pathogen therapy
MIC Minimal inhibitory concentration
MRPA Multiply-resistant Pseudomonas aeruginosa
MRSA Methicillin resistant Staphylococcus aureus
MSSA Methicillin sensitive Staphylococcus aureus
NCCLS National Committee for Laboratory Standards
NIH National Institues of Health
ODA Once daily aminoglycerides
PO Oral
PPU Perforated peptic ulcer
PVL Panton-Valentine leukocidin
qd Daily
qid Four times per day
syr Syrup
tab/tabs Tablet/tablets
TBW Total body weight
TDM Therapeutic drug monitoring
tds Three times per day
USS Ultrasound
VRE Vancomycin resistant Enterococcus
WHO World Health Organisation
Soft copy of this document is available at the following web links. http://www.hku.hk/hkucoi/impact.pdfhttp://www.chp.gov.hk/files/pdf/reducing_bacterial_resistance_with_impact.pdfhttp://ha.home/ho/ps/impact.pdf
Part I: Antibiotic resistance-local scenario 12
Part II: Antimicrobial stewardship programme 21
Part III: Guidelines for selected antimicrobial use 37
Part IV: Empirical therapy of common infections 59
Part V: Known-pathogen therapy 81
Part VI: Guidelines for surgical prophylaxis 88
Part VII: Cost and dosage of antimicrobial agents 95
QU
ICK
RE
FE
RE
NC
E















![Guideline on Environmental Impact Assessment for Veterinar… · Environmental Impact Assessment (EIAs) For Veterinary Medicinal Products - Phase I. [2] published in 2000; CVMP Guideline](https://static.fdocuments.us/doc/165x107/5fbbf87c4c2ff92c182f3904/guideline-on-environmental-impact-assessment-for-veterinar-environmental-impact.jpg)
![Impact Assessments Director’s Guideline [DGL 22/20]](https://static.fdocuments.us/doc/165x107/6169d5cf11a7b741a34be531/impact-assessments-directors-guideline-dgl-2220.jpg)

