Immunohistochemical findings in cranial arteritis
5
75 IMMUNOHISTOCHEMICAL FINDINGS IN CRANIAL ARTERITIS PATRICK GALLAGHER and KAREN JONES The cause of cranial arteritis is unknown, but the demonstration of immunoglobulin and complement in temporal artery biopsies by immunofluorescence sug- gests that it may be a disease of disordered immunity. Because of the inevitable problems of histologic inter- pretation associated with the fluorescent technique, 15 temporal artery biopsies from patients with active arter- itis were examined by an immunoperoxidase method. Varying amounts of IgA, IgG, and IgM were identified in plasma cells and macrophages. Extracellular IgG was identified in 1 case, but there was no staining for complement. These findings provide no support for the concept of cranial arteritis as a form of immune complex vasculitis. The etiology of temporal arteritis remains un- known 90 years after its first description by Hutchin- son (1). Because of the close histologic association of mononuclear and giant cells with disrupted fragments of the elastic lamellae (2), an allergic cellular response to some component of the arterial wall may be impor- tant in the pathogenesis of cranial arteritis. In support of this concept, there are several reports (3-5) of the immunofluorescent identification of complement and immunoglobulin in the arterial walls of affected pa- tients. The immunofluorescent technique has several inherent disadvantages. Frozen sections must be used, From the Department of Pathology, Southampton Universi- ty General Hospital, Southampton, England. Patrick J. Gallagher, MD, PhD: Karen Jones, BSc. Address reprint requests to Patrick J. Gallagher, MD, Department of Pathology, Southampton University General Hospi- tal, Southampton, SO9 4XY, England. Submitted for publication April 9, 1981: accepted in revised form June 18, 1981. the reaction product is unstable, and the preparations can be examined only with a fluorescent microscope (6). Recent refinements of the immunoperoxidase method (7,8) now permit a variety of antigens and antibodies to be accurately and sensitively localized in permanent, counterstained paraffin sections. In this report, we describe the immunohistochemical findings in 15 cases of temporal arteritis examined by this technique. PATIENTS AND METHODS Patients. The clinical records and temporal artery histology of 12 women and 3 men (mean age 70, range 55-78 years) with biopsy-proven cranial arteritis were reviewed. Thirteen of the patients had a history of persistent headache or visual disturbance. In all but 1 case, a woman with polycythemia, the erythrocyte sedimentation rate (ESR) was raised (mean 98, range 36-147). Every patient responded symptomatically to steroid treatment, most with a reduction in ESR. In each case, the histologic features were typical of giant cell arteritis (9). There was marked intimal thickening, disruption of the internal elastic lamella, and a dense infil- trate of mononuclear and giant cells, often centered around fragments of elastica. The material from 3 patients with negative temporal artery biopsies was also studied. One showed arteriosclero- sis (MU, clinical diagnosis: hypertension), 1 early athero- sclerosis (F64, no final clinical diagnosis), and 1 was normal histologically (F40, clinical diagnosis: migraine). Immunohistochemical methods. All biopsies had been fixed in 10% neutral buffered formol saline; then they were processed into paraffin and cut at 5p thickness. They were then treated with a freshly prepared solution of trypsin (7) at 37°C. The effects of varying the incubation time between 20 and 40 minutes were investigated at trypsin concentrations of 0.05 and 0.1%. In most cases, optimal results were obtained with 0.05% trypsin for 30 minutes. The sections were then stained by a modification (7,8) of the unlabeled antibody-peroxidase-antiperoxidase Arthritis and Rheumatism, Vol. 25, No. 1 (January 1982)
-
Upload
patrick-gallagher -
Category
Documents
-
view
212 -
download
0
Transcript of Immunohistochemical findings in cranial arteritis

75
IMMUNOHISTOCHEMICAL FINDINGS IN CRANIAL ARTERITIS
PATRICK GALLAGHER and KAREN JONES
The cause of cranial arteritis is unknown, but the demonstration of immunoglobulin and complement in temporal artery biopsies by immunofluorescence sug- gests that it may be a disease of disordered immunity. Because of the inevitable problems of histologic inter- pretation associated with the fluorescent technique, 15 temporal artery biopsies from patients with active arter- itis were examined by an immunoperoxidase method. Varying amounts of IgA, IgG, and IgM were identified in plasma cells and macrophages. Extracellular IgG was identified in 1 case, but there was no staining for complement. These findings provide no support for the concept of cranial arteritis as a form of immune complex vasculitis.
The etiology of temporal arteritis remains un- known 90 years after its first description by Hutchin- son (1). Because of the close histologic association of mononuclear and giant cells with disrupted fragments of the elastic lamellae (2), an allergic cellular response to some component of the arterial wall may be impor- tant in the pathogenesis of cranial arteritis. In support of this concept, there are several reports (3-5) of the immunofluorescent identification of complement and immunoglobulin in the arterial walls of affected pa- tients.
The immunofluorescent technique has several inherent disadvantages. Frozen sections must be used,
From the Department of Pathology, Southampton Universi- ty General Hospital, Southampton, England.
Patrick J. Gallagher, MD, PhD: Karen Jones, BSc. Address reprint requests to Patrick J. Gallagher, MD,
Department of Pathology, Southampton University General Hospi- tal, Southampton, SO9 4XY, England.
Submitted for publication April 9, 1981: accepted in revised form June 18, 1981.
the reaction product is unstable, and the preparations can be examined only with a fluorescent microscope (6). Recent refinements of the immunoperoxidase method (7,8) now permit a variety of antigens and antibodies to be accurately and sensitively localized in permanent, counterstained paraffin sections. In this report, we describe the immunohistochemical findings in 15 cases of temporal arteritis examined by this technique.
PATIENTS AND METHODS Patients. The clinical records and temporal artery
histology of 12 women and 3 men (mean age 70, range 55-78 years) with biopsy-proven cranial arteritis were reviewed. Thirteen of the patients had a history of persistent headache or visual disturbance. In all but 1 case, a woman with polycythemia, the erythrocyte sedimentation rate (ESR) was raised (mean 98, range 36-147). Every patient responded symptomatically to steroid treatment, most with a reduction in ESR. In each case, the histologic features were typical of giant cell arteritis (9). There was marked intimal thickening, disruption of the internal elastic lamella, and a dense infil- trate of mononuclear and giant cells, often centered around fragments of elastica.
The material from 3 patients with negative temporal artery biopsies was also studied. One showed arteriosclero- sis ( M U , clinical diagnosis: hypertension), 1 early athero- sclerosis (F64, no final clinical diagnosis), and 1 was normal histologically (F40, clinical diagnosis: migraine).
Immunohistochemical methods. All biopsies had been fixed in 10% neutral buffered formol saline; then they were processed into paraffin and cut at 5p thickness. They were then treated with a freshly prepared solution of trypsin (7) at 37°C. The effects of varying the incubation time between 20 and 40 minutes were investigated at trypsin concentrations of 0.05 and 0.1%. In most cases, optimal results were obtained with 0.05% trypsin for 30 minutes.
The sections were then stained by a modification (7,8) of the unlabeled antibody-peroxidase-antiperoxidase
Arthritis and Rheumatism, Vol. 25, No. 1 (January 1982)

76 GALLAGHER AND JONES
(PAP) method of Sternberger (10). All biopsies were exam- ined with antisera raised in rabbits to the heavy chains of IgA, IgG, and IgM, and Clq and C3 fractions of comple- ment. In representative cases, the staining produced by antisera to C4, albumin, fibrin, kappa and lambda immuno- globulin light chains, a1 antitrypsin, and the lysosomal enzyme muramidase was also studied.
The most appropriate dilutions of the primary rabbit anti-human antibodies, the swine anti-rabbit immunoglob- ulin bridge, and the peroxidase antiperoxidase reagent were determined by titration. In most cases immunoglobulin heavy chain antisera were used at 1:1,000 or 1:2,000, complement antisera at 1 :400 or 1 :800, swine anti-rabbit IgG at 1 :80, and PAP at 1 :200. All sections were counterstained with hematoxylin to permit full histologic orientation. In each of the 15 patients with cranial arteritis, there was evidence of inflammation in all of the sections stained by the immunoperoxidase technique.
As a negative control, whole rabbit serum was sub- stituted for the rabbit anti-human primary antiserum in 1 slide from every set of sections. In four instances slides of human renal biopsies were stained alongside the sections of temporal artery. C3 and extracellular IgG had been pre- viously demonstrated in these biopsies by an immunofluo- rescent technique, and in each case this was confirmed by the immunoperoxidase method.
In 2 patients the specificity of the staining for IgG and IgM was investigated by a blocking technique (11). Sections were stained in parallel with I ) the normal primary (1 : 1 ,OOO) rabbit antibody and 2) an equal mixture of concen-
or IgM. By virtue of its higher concentration, the goat antibody binds preferentially to tissue antigens, but cannot subsequently react with the swine anti-rabbit immunoglob- ulin bridge. On each occasion a marked reduction in staining intensity was observed with the mixture of antibodies, confirming the specificity of the original reaction.
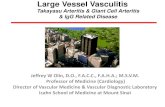
Figure 1. IgM, woman, age 55. Occasional macrophages stain Positively (arrows). (Magnification x600.)
trated (1:s) goat and dilute (1: 1,000) rabbit anti-human IgG lesser extent in the vascular lumen itself. This pattern was ascribed to a reaction with plasma immunoglob-
Complement components. No significant intra-
preparations examined. Even when the trypsin incuba- or extracellular complement was detected in any of the
RESULTS Immunoglobulin antisera. Some intracellular
immunoglobulin was identified in plasma cells, macro- phages, and giant cells in all cases of cranial arteritis (Figures 1-3). In plasma cells the pattern of cytoplas- mic staining was more uniform than in macrophages and giant cells, in which granular deposits were occa- sionally seen. The intensity of staining was greatest with IgG, but in all but 4 cases some intracellular IgA and IgM was also present. There was no difference between the staining with kappa and lambda light chain antisera.
In a 64-year-old man, small amounts of extra- cellular IgG were seen in the outer intima and inner media (Figure 3 ) . The specificity of this reaction was confirmed by a blocking technique. No other extracel- Mar immunoglobulin staining was seen. In some arter- ies a thin rim of IgG or IgM was present on the endothelial surface, in the innermost intima, and to a
tion time and concentration were adjusted to produce optimal staining for C3 in the positive control sections of renal biopsies, no appreciable reaction was ob- tained.
Other immunoproteins. Fibrin was identified in the intima or media of 7 of 12 biopsies. In 4 cases extensive deposits were present (Figure 4). Much smaller amounts of albumin were seen in 3 of 6 cases. In all ten cases stained with antisera to the lysosomal enzyme muramidase, a prominent cytoplasmic reac- tion was noted in macrophages and giant cells (Figure 5). Much of the staining in macrophages was granular, but a lighter more diffuse pattern was seen in giant cells. In some parts of several sections a patchy, but apparently genuine, staining of the elastic lamellae was obtained with antibodies to muramidase. A slight granular reaction was seen in the cytoplasm of occa- sional macrophages stained with a1 antitrypsin anti- sera.
In the atherosclerotic temporal artery, small

IMMUNOHISTOCHEMICAL FINDINGS IN CRANIAL ARTERITIS 77
absent. In contrast, Liang, Simkin, and Mannik (3) reported a variety of staining patterns with immuno- globulin antisera, including extracellular deposits close to elastic lamellae and both diffuse and granular cytoplasmic staining. Complement was also identified, chiefly in the cytoplasm of inflammatory cells. Broad- ly similar results were described by Plouvier and his colleagues (5).
Detailed histologic structure is often difficult to distinguish under fluorescent light, and this is un- doubtedly one of the major disadvantages of the immunofluorescent technique. We find it surprising that Park and Hazleman were able to report a consistent pattern of extracellular staining, but no intracellular reaction for immunoglobulin. A certain number of plasma cells are invariably found in active giant cell arteritis, and should these not stain with immunoglobulin antisera, the sensitivity and specific- ity of the reaction should be questioned. We had no difficulty in detecting cytoplasmic immunoglobulins in
Figure 2. IgG, woman, age 77. Moderate numbers of positively stained cells (thin arrows), including a plasma cell (thicker arrow). (Magnification ~ 5 0 0 . )
amounts of extracellular fibrin and albumin were iden- tified in the intima, and some IgG was seen in the cytoplasm of adventitial chronic inflammatory cells. No significant staining was present in either the arte- riosclerotic or the normal temporal artery.
DISCUSSION The results of this study indicate that a variety
of intracellular immunoglobulins can be detected in the inflammatory infiltrates in cranial arteritis. With one exception there was no appreciable extracellular immunoglobulin, nor was there any staining for com- plement.
Because there are no other accounts of tempo- ral artery biopsies studied by the immunoperoxidase method, our results can be compared only with studies that used the immunofluorescent technique. In the most recent of these, Park and Hazleman (4) described a consistent pattern Of extracellular staining with antisera to IgA, IgG, and IgM, and c3 , but carefully stated that cytoplasmic (i.e. intracellular) staining was
Figure 3. IgG, man, age 64. Small amounts of extracellular (short arrow) and cytoplasmic (Long arrows) staining, (m) arterial media. (Magnification ~ 6 0 0 . )

78 GALLAGHER AND JONES
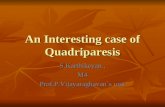
Figure 4. Fibrin, man, age 67. Abundant dark staining in both intima (i) and media (m). (Magnification ~ 2 5 0 . )
both plasma cells and macrophages and confirmed the staining specificity with blocking techniques.
In view of the results of prevous immunofluo- rescent studies, the absence of complement staining with the immunoperoxidase method was surprising. Nonspecific background staining of connective tissue is a recurrent problem when arterial tissue is stained by the immunoperoxidase technique. This can be virtually eliminated by dilution of the primary antise- rum, and this may have reduced the sensitivity of complement staining. Nevertheless our staining meth- od was intentionally adjusted to favor the demonstra- tion of extracellular immunoproteins, and sections of renal biopsies stained simultaneously for complement were consistently positive.
Our findings provide no additional support for the concept of cranial arteritis as an immune complex disorder. The pattern of intracytoplasmic staining for immunoglobulins would be anticipated in any chronic inflammatory reaction. In the absence of complement the small amount of extracellular IgG seen in one case is of no particular importance. Fibrin and albumin can be detected in a wide variety of arterial diseases, and the presence of lysosomal enzyme (muramidase) only
confirms that mononuclear and giant cells are derived from the monocyte-macrophage series.
Even if we disregard the results of immunohis- tochemical studies, other evidence suggests a role for disordered immunity in cranial arteritis. Elevations of serum IgG and complement have been reported in temporal arteritis (12), and the numbers of circulating immunoblasts are increased in polymyalgia rheuma- tics (13). Hazleman, Maclennan, and Esiri (14) studied the behavior of peripheral blood lymphocytes exposed in vitro to human arterial and muscular antigens. The rate of proliferation was increased in patients with polymyalgia rheumatica, perhaps suggesting a modi- fied cellular immune response. However, these find- ings were not confirmed in a subsequent detailed study reported by Papaioannou, Hunder, and McDuffie (15).
Further immunohistochemical studies may help to clarify the part that disordered immunity plays in cranial arteritis. In future immunofluorescent investi- gations, a wider range of antisera to complement com- ponents should be used, and the specificity of any positive reactions should be tested by blocking tech- niques. Antisera are now available to a variety of lymphocyte subsets, such as helper or suppressor T
Figure 5. Fibrin, man, age 67. Intense staining in many macrophages (short arrow) and to a lesser extent giant cells (g). Note unexplained staining of elastic lamella (long arrow). (Muramidase, magnification X225 .)

IMMUNOHISTOCHEMICAL FINDINGS IN CRANIAL ARTERITIS 79
cells. These may allow the functional nature of the Edited by RC Nairn. London, Churchill Livingstone,
7. Mepham BL, Frater W, Mitchell BS: The use of proteo- lytic enzymes to improve immunoglobulin staining by
lymphoid infiltrates to be defined in cranial arteritis. 1976, pp 68-108
ACKNOWLEDGMENTS the PAP technique. Histochem J 11:345-357, 1979
8. MacIver AG, Giddings J, Mepham BL: Demonstration of extracellular immunoproteins in formalin fixed renal biopsy specimens. Kidnev Int 16:632-636, 1979
We thank Mr. Brian Mepham for his advice On technical aspects of this work and Miss Margaret Harris for typing the manuscript.
1.
2.
3.
4.
5 .
6.
REFERENCES Hutchinson J: Diseases of the arteries. Arch Surg 1:325- 326, 1890 Parker F, Healey LA, Wieske KR, Odland GF: Light and electron microscopic studies on human temporal arteries with special reference to alterations related to senescence, atherosclerosis, and giant cell arteritis. Am J Pathol 7957-80, 1975 Liang GC, Simkin PA, Mannik M: Immunoglobulins in temporal arteries: an immunofluorescent study. Ann Intern Med 81:19-24, 1974 Park JR, Hazleman BL: Immunological and histological study of temporal arteries. Ann Rheum Dis 37:238-243, 1978 Plouvier B, Francois M, Wattre P, Francois P, Devulder B: Examen en immunofluorescence directe de coupes d'artere temporale: interet et limites. Nouv Presse Med
Nairn RC: Fluorescence microscopy and photomicrog- raphy, Fluorescent Protein Tracing. Fourth edition.
7:1719-1721, 1978
9. Allsop CJ, Gallagher PJ: Temporal artery biopsy in cranial arteritis: a reappraisal. Am J Surg Pathol 5:317- 323, 1981
10. Sternberger LA: Immunocytochemistry. Second edi- tion. New York, John Wiley & Sons Inc, 1979, pp 104- 169
1 1 . Goldman M: Fluorescent Antibody Methods. New York, Academic Press, 1968, pp 155-162
12. Malmvall BE, Bengtzzon B-A, Kaijser B, Nilsson LA, Alestig K: Serum levels of immunoglobulin and comple- ment in giant cell arteritis. JAMA 236:1876-1878, 1976
13. Eghtedari AA, Esselinckx W, Bacon PA: Circulating immunoblasts in polymyalgia rheumatica. Ann Rheum Dis 35: 158-162, 1976
14. Hazleman BL, Maclennan ICM, Esiri MM: Lympho- cyte proliferation to artery antigen as a positive diagnos- tic test in polymyalgia rheumatica. Ann Rheum Dis 34: 122-127, 1975
15. Papaioannou CC, Hunder GG, McDuffie FC: Cellular immunity in polymyalgia rheumatica and giant cell arter- itis: lack of response to muscle or artery homogenates. Arthritis Rheum 22:740-745, 1979