Immune Mediated Renal Diseases
4
Immune Mediated Renal Diseases Definition Renal Diseases (damage to Glomeruli, Tubules, Interstitial Tissue) Glomeruli – Most due to Immunological Mechanism Tubules, Interstitium – Some Degree Nephritis Antibodies with Complement , Polymorph (↑ Important than Cellular Mechanism in Pathogenesis) Antibodies Induce Damage (2 ways) React Directly with Glomerular, Tubular Basement Membrane Antibody forms Immune Complexes with Circulating Antigen (Deposited in Kidney) Immunologic Tests Diagnose Renal Diseases Clinical Syndromes Acute Nephritis Sudden onset of Haematuria, Proteinuria, Hypertension, Oliguria Following Streptococcal Infection (of Throat, Skin in Children) Nephrotic Syndrome Hypoalbuminaemia, Edema Resulting from Proteinuria (common presentation of GN) Persistent Proteinuria Protein < 300 mg/day Protein > 300 mg/day Normally Present in Urine Pathologic (Most All Renal Disease) Recurrent Haematuria (1 st Manifestation of Renal/ Extrarenal Disease) Micro, Macroscopic Upper, Lower Urinary Tract Renal Failure Acute Chronic Sudden onset with Severe Impairment of Renal Function End- Result of any Disorder Destroys Renal Architecture Inflammatory Origin Poor Correlation (between Clinical Picture, Underlying Morphology) Diagnosis by Renal Biopsy Histological Classification of Glomerulonephritis Glomeruli Composed of Mesangial, Endothelial, Epithelial Cells Glomerulonephritis (by defining Types of Cells, Parts or All Parts Damaged) Classification based on LM, EM, Direct Immunohistology (IF)
description
Immune Mediated Renal Diseases
Transcript of Immune Mediated Renal Diseases

Immune Mediated Renal Diseases
Definition
Renal Diseases (damage to Glomeruli, Tubules, Interstitial Tissue)
Glomeruli – Most due to Immunological Mechanism
Tubules, Interstitium – Some Degree
Nephritis
Antibodies with Complement, Polymorph
(↑ Important than Cellular Mechanism in Pathogenesis)
Antibodies Induce Damage (2 ways) React Directly with Glomerular, Tubular Basement Membrane
Antibody forms Immune Comple xes with Circulating Antigen
(Deposited in Kidney)
Immunologic Tests
Diagnose Renal Diseases
Clinical Syndromes
Acute Nephritis
Sudden onset of Haematuria, Proteinuria, Hypertension, Oliguria
Following Streptococcal Infection (of Throat, Skin in Children)
Nephrotic Syndrome
Hypoalbuminaemia, Edema
Resulting from Proteinuria (common presentation of GN)
Persistent Proteinuria
Protein < 300 mg/day Protein > 300 mg/day
Normally Present in Urine Pathologic (Most All Renal Disease)
Recurrent Haematuria (1st
Manifestation of Renal/ Extrarenal Disease)
Micro, Macroscopic
Upper, Lower Urinary Tract
Renal Failure
Acute Chronic
Sudden onset with Severe
Impairment of Renal Function
End-Result of any Disorder
Destroys Renal Architecture
Inflammatory Origin
Poor Correlation (between Clinical Picture, Underlying Morphology)
Diagnosis by Renal Biopsy
Histological Classification of Glomerulonephritis
Glomeruli
Compose d of Mesangial, Endothelial, Epithelial Cells
Glomerulonephritis (by defini ng Types of Cells, Parts or All Parts Damaged)
Classification based on LM, EM, Direct Immunohistology (IF)
jslum.com | Medicine
Acute Immune-Complex Nephritis (Serum Sickness)
Occurs when Amount of Circulating Antigen is still in excess of Antibody
Immune Complexes Forme d, Soluble, Trapped in Capillary Membranes
IF
Irregular
Granular (Lumpy-Bumpy) Deposition
Renal Injury (due to Accumulation of Macrophages in Glomeruli, Release of
Inflammatory Mediators)
Transient with Complete Healing
Example
Post-Streptococcal GN
Acute Post-Streptococcal GN
Preceded by Streptococcal Infection of Throat, Skin (90% of Cases)
Acute Nephritis 10-12 days after Throat Infection
3 weeks after Skin Infection
Diagnosis
History of Sore Throat
Throat Culture
↑ Titres of Streptococcal Antibodies
(Anti-Streptolysin, Anti-DNAse B, Anti-Hyaluronidase)
↓ Serum C3 Level
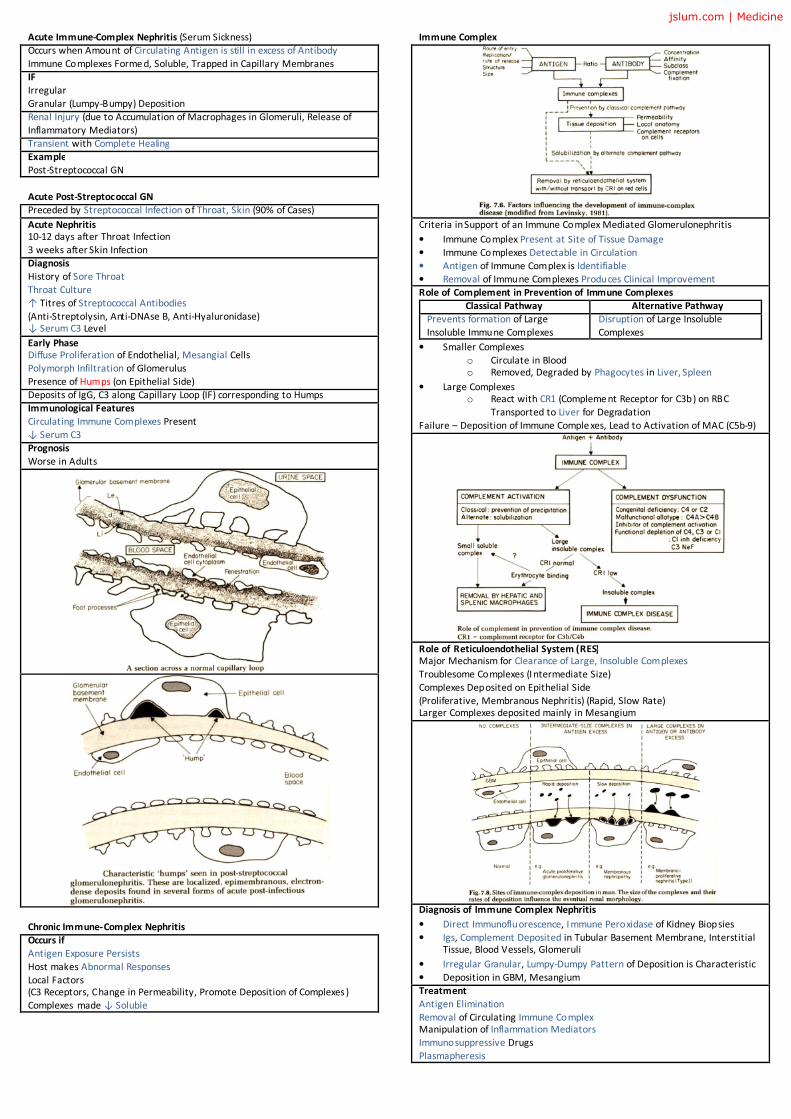
Early Phase Diffuse Proliferation of Endothelial, Mesangial Cells
Polymorph Infiltration of Glomerulus
Presence of Humps (on Epithelial Side)
Deposits of IgG, C3 along Capillary Loop (IF) corresponding to Humps
Immunological Features
Circulating Immune Complexes Present
↓ Serum C3
Prognosis
Worse in Adults
Chronic Immune-Complex Nephritis
Occurs if
Antigen Exposure Persists
Host makes Abnormal Responses
Local Factors
(C3 Receptors, Change in Permeability, Promote Deposition of Complexes)
Complexes made ↓ Soluble
Immune Complex
Criteria in Support of an Immune Complex Mediated Glomerulonephritis
• Immune Complex Present at Site of Tissue Damage
• Immune Complexes Detectable in Circulation
• Antigen of Immune Complex is Identifiable
• Removal of Immune Complexes Produces Clinical Improvement
Role of Complement in Prevention of Immune Complexes
Classical Pathway Alternative Pathway
Prevents formation of Large
Insoluble Immune Complexes
Disruption of Large Insoluble
Complexes
• Smaller Complexes
o Circulate in Blood
o Removed, Degraded by Phagocytes in Liver, Spleen
• Large Complexes
o React with CR1 (Compleme nt Receptor for C3b) on RBC
Transported to Liver for Degradation
Failure – Deposition of Immune Comple xes, Lead to Activation of MAC (C5b-9)
Role of Reticuloendothelial System (RES) Major Mechanism for Clearance of Large, Insoluble Complexes
Troublesome Complexes (I ntermediate Size)
Complexes Deposited on Epithelial Side
(Proliferative, Membranous Nephritis) (Rapid, Slow Rate)
Larger Complexes deposited mainly in Mesangium
Diagnosis of Immune Complex Nephritis
• Direct Immunofluorescence, I mmune Peroxidase of Kidney Biopsies
• Igs, Complement Deposited in Tubular Basement Membrane, Interstitial
Tissue, Blood Vessels, Glomeruli
• Irregular Granular, Lumpy-Dumpy Pattern of Deposition is Characteristic
• Deposition in GBM, Mesangium
Treatment
Antigen Elimination
Removal of Circulating Immune Complex
Manipulation of Inflammation Mediators
Immunosuppressive Drugs
Plasmapheresis
jslum.com | Medicine
Membranous Glomerulonephritis
Present with Florid Nephrotic Syndrome (80%)
Proteinuria, Microscopic Haematuria
30 – 50 y/o (Peak Age)
Characteristic Thickening of GBM without Proliferation of Cells
Types
Idiopathic Secondary
Causal Antigen Never Found Drugs
Complexes Accumulated only on Epithelial Side of GBM
(Serum Comple ment Normal)
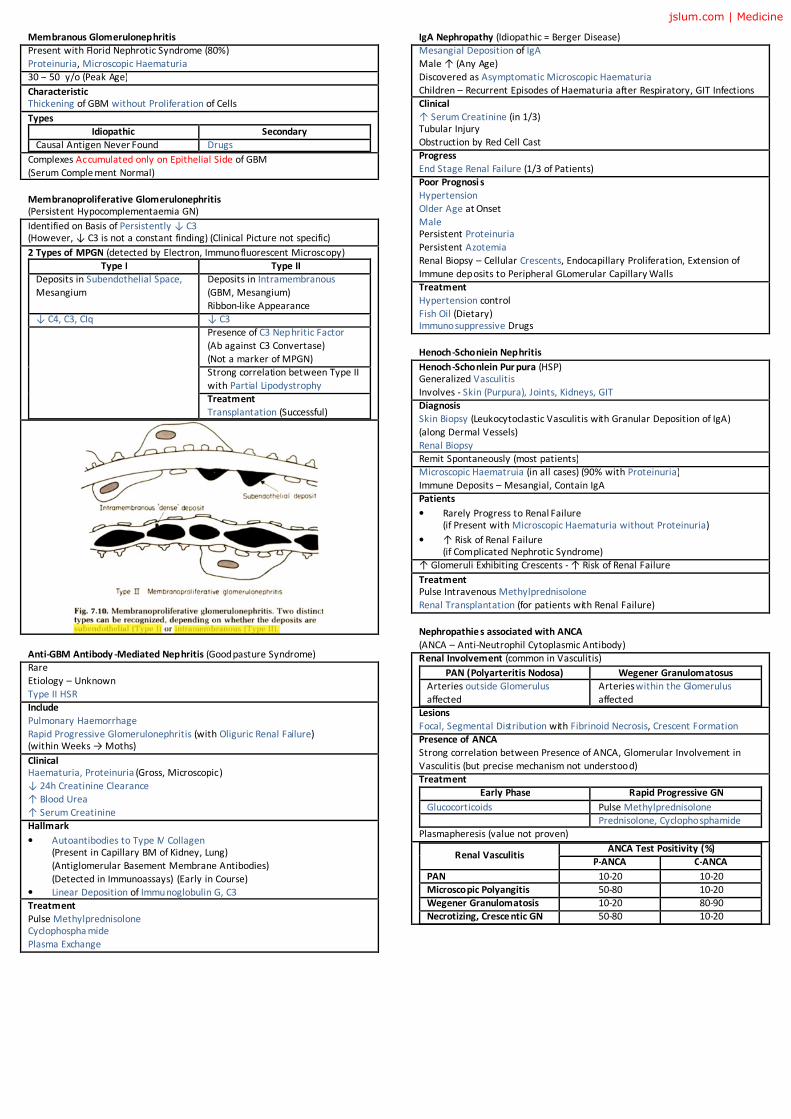
Membranoproliferative Glomerulonephritis (Persistent Hypocomplementaemia GN)
Identified on Basis of Persistently ↓ C3
(However, ↓ C3 is not a constant finding) (Clinical Picture not specific)
2 Types of MPGN (detected by Electron, Immunofluorescent Microscopy)
Type I Type II
Deposits in Subendothelial Space,
Mesangium
Deposits in Intramembranous
(GBM, Mesangium)
Ribbon-like Appearance
↓ C4, C3, CIq ↓ C3
Presence of C3 Nephritic Factor
(Ab against C3 Convertase)
(Not a marker of MPGN)
Strong correlation between Type II
with Partial Lipodystrophy
Treatment
Transplantation (Successful)
Anti-GBM Antibody -Mediated Nephritis (Goodpasture Syndrome)
Rare
Etiology – Unknown
Type II HSR
Include
Pulmonary Haemorrhage
Rapid Progressive Glomerulonephritis (with Oliguric Renal Failure)
(within Weeks → Moths)
Clinical Haematuria, Proteinuria (Gross, Microscopic)
↓ 24h Creatinine Clearance
↑ Blood Urea
↑ Serum Creatinine
Hallmark
• Autoantibodies to Type IV Collagen
(Present in Capillary BM of Kidney, Lung)
(Antiglomerular Basement Membrane Antibodies)
(Detected in Immunoassays) (Early in Course)
• Linear Deposition of Immunoglobulin G, C3
Treatment
Pulse Methylprednisolone
Cyclophospha mide
Plasma Exchange
IgA Nephropathy (Idiopathic = Berger Disease)
Mesangial Deposition of IgA
Male ↑ (Any Age)
Discovered as Asymptomatic Microscopic Haematuria
Children – Recurrent Episodes of Haematuria after Respiratory, GIT Infections
Clinical
↑ Serum Creatinine (in 1/3)
Tubular Injury
Obstruction by Red Cell Cast
Progress
End Stage Renal Failure (1/3 of Patients)
Poor Prognosi s
Hypertension
Older Age at Onset
Male
Persistent Proteinuria
Persistent Azotemia
Renal Biopsy – Cellular Crescents, Endocapillary Proliferation, Extension of
Immune deposits to Peripheral GLomerular Capillary Walls
Treatment
Hypertension control
Fish Oil (Dietary)
Immunosuppressive Drugs
Henoch-Schoniein Nephritis
Henoch-Schonlein Pur pura (HSP)
Generalized Vasculitis
Involves - Skin (Purpura), Joints, Kidneys, GIT
Diagnosis
Skin Biopsy (Leukocytoclastic Vasculitis with Granular Deposition of IgA)
(along Dermal Vessels)
Renal Biopsy
Remit Spontaneously (most patients)
Microscopic Haematruia (in all cases) (90% with Proteinuria)
Immune Deposits – Mesangial, Contain IgA
Patients
• Rarely Progress to Renal Failure
(if Present with Microscopic Haematuria without Proteinuria)
• ↑ Risk of Renal Failure
(if Complicated Nephrotic Syndrome)
↑ Glomeruli Exhibiting Crescents - ↑ Risk of Renal Failure
Treatment Pulse Intravenous Methylprednisolone
Renal Transplantation (for patients with Renal Failure)
Nephropathie s associated with ANCA
(ANCA – Anti-Neutrophil Cytoplasmic Antibody)
Renal Involvement (common in Vasculitis)
PAN (Polyarteritis Nodosa) Wegener Granulomatosus
Arteries outside Glomerulus
affected
Arteries within the Glomerulus
affected
Lesions
Focal, Segmental Distribution with Fibrinoid Necrosis, Crescent Formation
Presence of ANCA
Strong correlation between Presence of ANCA, Glomerular Involvement in
Vasculitis (but precise mechanism not understood)
Treatment
Early Phase Rapid Progressive GN
Glucocorticoids Pulse Methylprednisolone
Prednisolone, Cyclophosphamide
Plasmapheresis (value not proven)
Renal Vasculitis ANCA Test Positivity (%)
P-ANCA C-ANCA
PAN 10-20 10-20
Microscopic Polyangitis 50-80 10-20
Wegener Granulomatosis 10-20 80-90
Necrotizing, Cresce ntic GN 50-80 10-20
jslum.com | Medicine
Renal Involvement (Systemic Connective Tissue Disease)
Lupus Nephritis
Renal Involement (affects most of SLE patients)
Nephritis (Major cause of Morbidity, Mortality)
DNA, anti-DNA Antibodies (Glomerular Deposits in Subepithelial)
(Central Role in Pathogenesis of Proliferative LN)
Proliferative LN Rapid Progressive LN
Symptomatic Haematruia Cellular Crescents
Proteinuria
Hypertension
Azotaemia
Hypocompleme ntaemia
↑ Titre of Anti-DNA Antibodies
Diagnosis
• Serum Complement - ↓ Level Indicate Flares
• Antibodies Detection
• Renal Biopsy
Other Conne ctive Tissue Diseases
Scleroderma (Diffuse Form)
Sjogren Syndrome
Rheumatoid Arthritis
jslum.com | Medicine