
Immediate Placement of Endosseous Implants in Extraction Sites - A Case Report
4
IMMEDIATE PLACEMENT OF ENDOSSEOUS IMPLANTS IN EXTRACTION SITES - A CASE REPORT Rajesh*, Singh VakiI**, Singh B.P.***, Bansal Monika**** Due to the tremendous success of end osseous dental implants, these are being p referred over conventional fixed and removable prosthesis. This success has lead to the extractio n and replaceme nt of teet h with guarded prognosis. A 24 years old male patient, reported with pain in upper cent ral incisor, which had undergone trauma four months earlier. Due to trauma, he lost his right lateral incisor & suffered from fracture of the central incisor. The prognosis of the fractured central incisor was poor bec ause this was located in the middle ofthe root. Hence, the tooth was extracted and two implants were placed. Th e restora- tion was executed with two metal ceramic crowns which were splinted to each other. The pros thesis is successfully function ing for last 5 years. KEY WORDS: Immediate placement, endosseous dental implant, delayed implant placement, bone fill. Dental implants are customarily done only after complete bone healing following extraction of teeth . Recent studies have shown 50% bone loss in bucco- lingual direction within first 6 week of extraction. Hence, the immediate placement of implants become very important as it prevents the tissues from col- lapsing. Implants should be placed in sites which are not infected. Well confiued puthulugy such cyst and granulomas can be removed and implant can be plueod 11 thouo urc nul accondurily infected. Pres- once of infection oontruindicatca the proce dure and should be delayed by 6-8 weeks. I ,2J Studi es ha ve sho wn that placement of endosseous implants in fresh extraction sites can re- sult in integration as determined by histological evi- dence of bone closely adapted to implant's surface and lack of cllnlcal mobility CASEREPORT A 24 ycara old male patient reported with com - plaint of pain ill his upper fiuut lu ulh since lust une "Lecturer, ***ProJessor. ****Senior Resident Faculty of Dental Sciences. Instillite oj Medical Sciences. B.H. u. Varanasi. **ProJessor Department oj Metallurgical Engineering, lnstitute of Tech- nology, BHU, Varanasi. 36 JPFA , Vol. 23. March. 2009 week which increases at night and gets relieved on taking pain killers. The patient got an accident by a motor bike 4 months back during which he lost his maxillary left lateral incisor ami traumati zed central incisor (Fig. I & 2). Radiographic examination revealed that there was a fracture in the middle root portion of 21 and the corona l fragm ent was mobil e The latera l incisor was missing and there was a good amount of hon o fill in the socket. As the prognosis of the ce ntra l incisor was guarded, the extraction of the tooth was planned and performed atraumatically, keeping the labial plat e in. tact. The socket was flushed with normal saline and betadine. (Fig. 3). 3-4 mill uf bouc wus available above root apex, which was used for stability of implant along with the walls of extraction socket. Two cp titanium, root form, indigenous val implants were placed: one in21 and another In 22 positions. The procedure was done under local infiltration anesthesia and la- bial side flap was not reflected to avoid the thin labial cortical plate from getting deprived of periost eal blood supp ly (Fig . 4). Interrupted sutures were placed and routine post-operative instructions were given. Sutures were removed after 8 days and the im- plants were slightly recontoured for paral1elism of abutments. An extra layer of die spacer was applied
Transcript of Immediate Placement of Endosseous Implants in Extraction Sites - A Case Report

IMMEDIATE PLACEMENT OF ENDOSSEOUS IMPLANTS INEXTRACTION SITES - A CASE REPORT
Rajesh*, Singh VakiI**, Singh B.P.***, Bansal Monika****
Due to the tremendous success of end osseous dental implants, these are being preferred over conventionalfixed and removable prosthesis. This success has lead to the extraction and replacement of teeth withguarded prognosis. A 24 years old male patient, r epor ted with pain in upper central incisor, which hadundergone trauma four months earlier. Due to trauma, he lost his right lateral incisor & suffered fromfracture of the central incisor. The prognosis of the fractured central incisor was poor bec ause this waslocated in the middle ofthe root. Hence , the tooth was extracted and two implants were placed. The restoration was executed with two metal ceramic crowns which were splinted to each other. The prosthesis issuccessfully functioning for last 5 years.
KEY WORDS: Immediate placement, endosseous dental implant, delayed implant placement, bone fill.
Dental implants are customarily done only aftercomplete bone healing following extraction ofteeth .Recent studies have shown 50% bone loss in buccolingual direction within first 6 week of extraction.Hence, the immediate placement ofimplants becomevery important as it prevents the tissues from collapsing. Implants should be placed in sites which arenot infected. Well confiued puthulugy such U~ cystand granulomas can be remo ved and implant can beplueod 11 thouo urc nul accondurily infected. Presonce of infection oontruindicatca the procedure andshould be delayed by 6-8 weeks.I,2J
Studies ha ve shown that placement ofendosseous implants in fresh extraction sites can result in integration as determined by histological evidence of bone closely adapted to implant's surfaceand lack ofcllnlcal mobilityp.~.M.l
CASEREPORT
A 24 ycara old male pati ent reported with complaint of pain ill his upper fiuut luulh since lust une
"Lecturer, ***ProJessor. ****Senior Resident
Faculty of Dental Sci ences. Instillite oj Medical Sciences.B.H.u. Varanasi.
**ProJessor
Department oj Metallurgical Engineering, lnstitute of Technology, BHU, Varanasi.
36 JPFA, Vol. 23. March. 2009
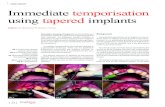
week wh ich increases at night and gets relieved ontaking pain killers. The patient got an accident by amotor bike 4 months back during which he lost hismaxillary left lateral incisor ami traumatized centralincisor (Fig. I & 2).
Radiographic examination revealed that there wasa fracture in the middle root portion of 21 and thecorona l fragm ent was mobil e The latera l incisor wasmissing and there was a good amount of hon o fill inthe socket.
As th e prognosis of the central incisor wasguarded, the extraction of the tooth was planned andperformed atraumatically, keeping the labial plat e in.tact. The socket was flushed with normal salin e andbetadine. (Fig. 3).
3-4 mill uf bouc wus ava ilable above root apex,which was used for stabili ty of implant along withthe walls ofextraction socket. Two cp titanium, rootform, indigenous llall~gillgival implants were placed:one in 21and another In 22 positions. The procedurewas done under local infiltration anesthesia and labial side flap was not reflected to avoid the thin labialcortical plate from getting deprived ofperiosteal bloodsupp ly (Fig . 4) . Interrupted sutures were placed androutine post-operative instructions were given.
Sutu res were removed after 8 days and the implants were slightly recontoured for paral1elism ofabutments. An extra layer of die spacer was applied

Fig. 1: Preoperative facial view.
Fig. 3: Extracted tooth slwll';lI[;[mcture ;11 thomiddle ofroot.
FiK. 5: Intra oral view with filial prosthesiscemented.
Fig. 6: Facial view with filial prosthesiscemellted.
JPFA, Vo!' 23, March 2009 37

e1"\tic~c:J '17
(Chlorhexidine gluconate 0.2% wtv)
~ Broad Spectrum of activity against Gram negative,Gram positive, vegetative bacteria, yeasts ,dermatophyte, fungi & lipophilic viruses
~ Binds strongly to mucosa
• prevents plaque in absence of brushingprevents & treats gtnglv iUs
• aids in the treatment of mouth& throat infections
~ ,fittCPA HEALTH PRODUCTS LTD.E-mail : [email protected]

REFERENCESI. Mentag PJ, Koinski TF, Sowinski LL: Dental implant
reconstruction after endodontic failure: Report of case.J. Am. Dent. Assoc.1990; 121: 24 1-244.
2. Yukna RA: Clinical comparison of hydroxyapatitecoated titanium dental implants placed in fresh extraction sockets and healed sites. J. Periodonta1.l991; 62:468-472.
3. Yukna RA: Placement of hydroxylapatite-coated implants into fresh or recent extraction sites. Dent. ClinNorth Am.1992; 36: 97-116.
4. Barz ilny I, Graser G, Irnnpour R. Notiel1o. J. ProskinH:Histologicand clinical assessmentof implantsplacedin cxtrnction sockets (obstruct 1452). J. Dent. Res.1990; 69, (spec iss): 290.
5. Block MS, Kent IN : Placementof endosseous implantsinto tuuLh oxtruetion uitcu, J. Owl. Muxillufuu, Surg,1991; 49: 1269-1276.
G. Nail OA, 3t"ill 3, Kului, M, Wai L" DE. Ev.tluaLiull ufendosseous implants placed in fresh extraction site indogs (abstract 1906). J. Dent. Res. 1982; 60 (spec iss):379-418, 1982.
7. Niznlck GA: The Core-Vent implant system. .I. Oral ,Implantol.19R2; 10: 379-41R.
8. Ashman A: An immediate tooth root replacement: Animplant cylinder and synthetic bone combination. J.Oral. Implantol.1990; 16:28-38.
9. Mcntog PJ, Kosinski T: Hydroxyapatite-augmentedsites as receptors for replacement implants, J. OralImplantol1989; 15: 114-123.
CONCLUSION
It appears magical to replace a troublesome too thwith the help of an immediate implant to both thedent ist and patient bu t it should be perfo rmed cautiously in se lec ted cas es because greed can lead tofrustrating fa ilures. Immediate implantation is an additio n to various modalities available to sol ve themissing tooth problem and no t the replace ment ofdelayed implant pla cement which will continue to beused for main stream cases.
Fig. 7: Radiographshowing two
endosseous dentalimplants with metalceramic restorations.
DISCUSSION
Immediate placementof implants can be successfully used in cases oftraumatic tooth loss without significant bone loss andsites without cellulitis or purulent exudate ; this issupported by various histological studies showi ngbone formation against implant surface.1.8.9
to ensure the passive fitof prosthesis. The prosthesis was cemented inplace after 3 months. Theprosthesis was relieved incentric occlusion so as toavoid the occlusal contactand reduce the force impact. (Fig. 5 & 6) Patientwas recalled after 1, 3 and6 months in first year andthe implants are workingsuccessfully after 5 years.
Tooth loss due to carie s or periodontitis, withoutpu rul ent exudate, adequate soft tissue health andquantity to achieve primary closure ami bo ne available above socket for adequate initial sta bi lity areother situat ions where this modality can be used sueces stully. Stili the case select ion should be very strictand wherever doubt exists, we should not hesitate topel iUl111 delaved imp lant placement.l-" ~
Mo st common sites for immediate implant placement are the incisors and canines. The bon e defectsdue to trauma, endo-perio lesions or inadvert ent cortical plate fracture during tooth extraction may needrepair. Small defects can be augment ed by alloplasticgraft (e.g. HA).~ Large detects need autogenous graftalone or combined with allogenous grafts. Implantscan be placed along with grafts , on ly iftheir mechanical stability is obtained by engaging the patient'sbasal bone.
JPFA, Vol. 23, March, 2009 39














![Cronicon · technique. Endosseous implant markets are growing very rapidly world-wide [2-4]. Endosseous implants are used to support and retain all kinds of prostheses in Dentistry](https://static.fdocuments.us/doc/165x107/5f46559ae33ada56f64703b0/cronicon-technique-endosseous-implant-markets-are-growing-very-rapidly-world-wide.jpg)


