
Imaging of Brain Metastases From Melanoma
42
Imaging of Melanoma Metastases in the Brain Jessica J. Kim, HMS III & Dr. Gillian Lieberman, M.D. Harvard Medical School Beth-Israel Deaconess Medical Center May 21, 2010
-
Upload
carlos-manuel-constain -
Category
Documents
-
view
231 -
download
0
description
mri imagingbrain metastases melanoma
Transcript of Imaging of Brain Metastases From Melanoma
Imaging of Melanoma Metastases in the Brain
Jessica J. Kim, HMS III & Dr. Gillian Lieberman, M.D. Harvard Medical School
Beth-Israel Deaconess Medical CenterMay 21, 2010

Overview
•
Melanoma–
Background–
Brain metastases: Epidemiology, Symptoms, Treatment
•
Menu of imaging modalities in brain melanoma
•
Case presentation–
Patient AC clinical history and imaging by MRI–
Variety of appearances of brain melanoma on MRI
•
Utility of alternative imaging modalities (CT, FDG-PET)

Let’s discuss why we want to learn about diagnostic imaging of metastatic melanoma in the brain
Melanoma•
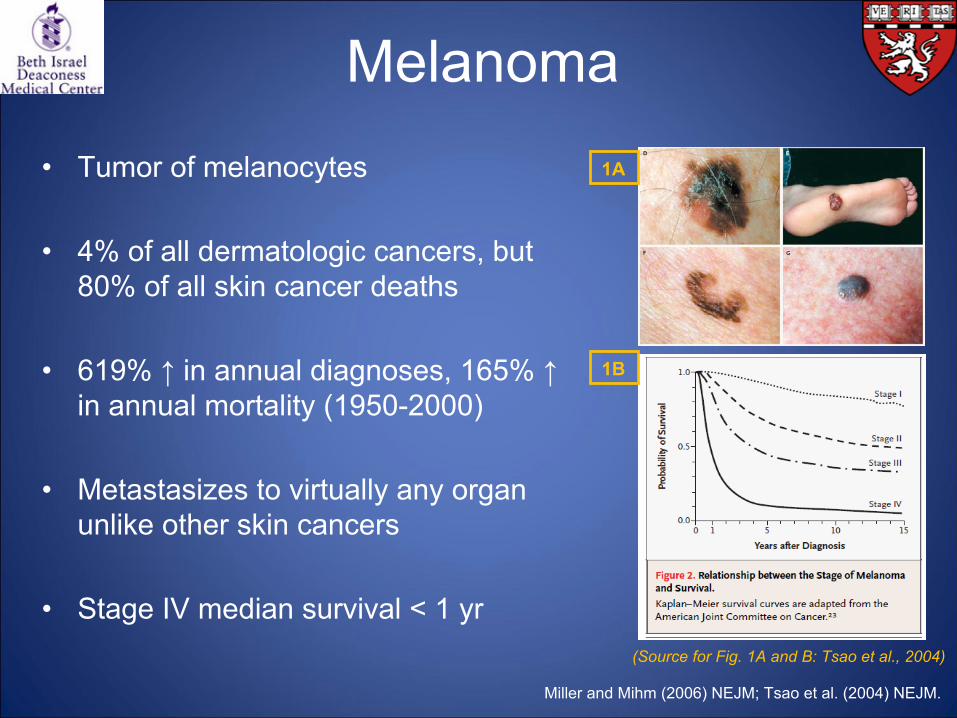
Tumor of melanocytes
•
4% of all dermatologic cancers, but 80% of all skin cancer deaths
•
619% ↑
in annual diagnoses, 165% ↑ in annual mortality (1950-2000)
•
Metastasizes to virtually any organ unlike other skin cancers
•
Stage IV median survival < 1 yr (Source for Fig. 1A and B: Tsao
et al., 2004)
Miller and Mihm
(2006) NEJM; Tsao
et al. (2004) NEJM.
1A
1B
Melanoma: Metastasis
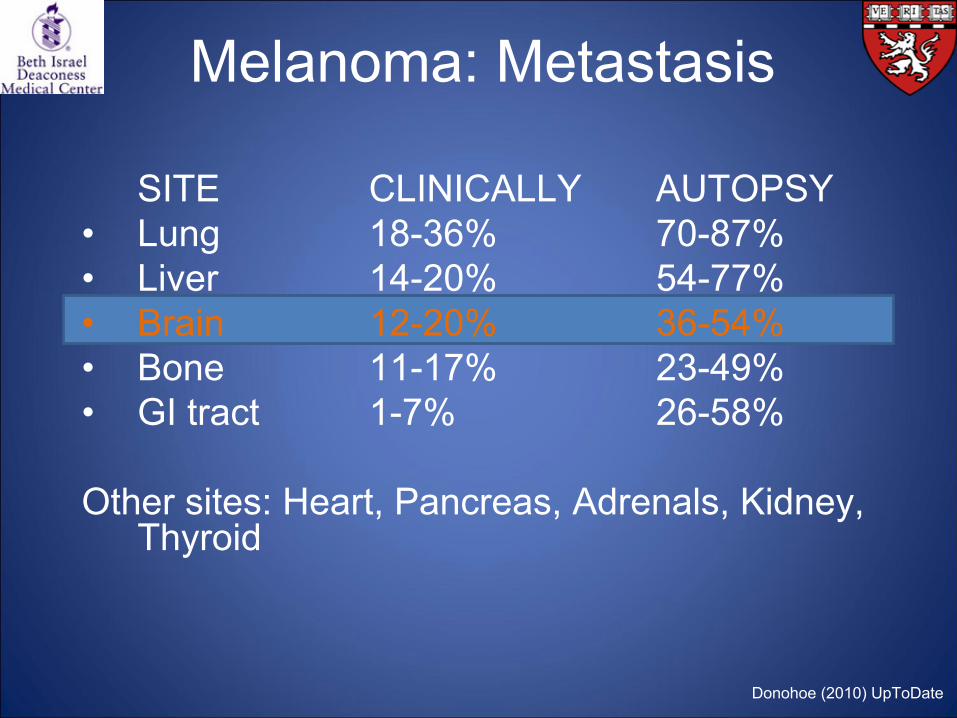
SITE
CLINICALLY
AUTOPSY•
Lung 18-36% 70-87%
• Liver 14-20% 54-77%
• Brain 12-20% 36-54%
• Bone 11-17% 23-49%
• GI tract 1-7% 26-58%
Other sites: Heart, Pancreas, Adrenals, Kidney, Thyroid
Donohoe
(2010) UpToDate
Melanoma: Metastasis
Sloan et al. (2009) Cancer Control; Eichler
and Loeffler
(2007) Oncologist; Testori
et al. (2009) Ann Oncol
•
3rd most common cause of brain metastases
•
Highest propensity to metastasize to the brain of all primary tumors in adults
•
Clinical features:–
Headaches & symptoms from increased pressure–
Focal neurologic deficits–
Seizures; cognitive impairment
“Given the recognized neurotropism of melanoma, neurological symptoms in a melanoma patient should prompt diagnostic imaging studies.” (Sloan et al., 2009)
Let’s preview the menu of tests and their use in brain melanoma imaging
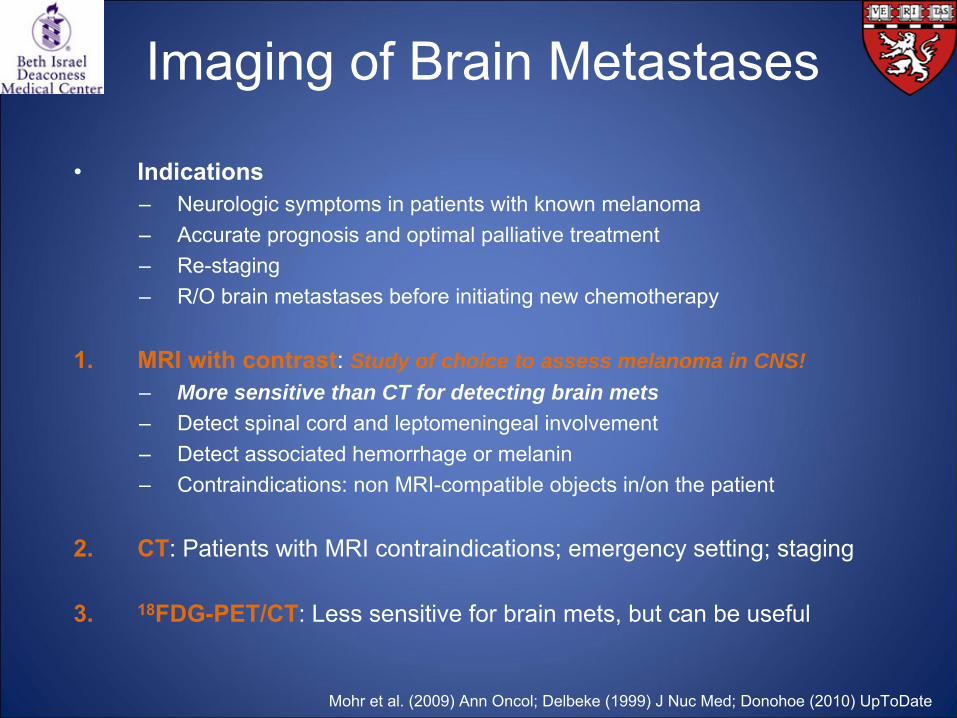
Imaging of Brain Metastases
Mohr et al. (2009) Ann Oncol; Delbeke
(1999) J Nuc
Med; Donohoe
(2010) UpToDate
•
Indications –
Neurologic symptoms in patients with known melanoma–
Accurate prognosis and optimal palliative treatment –
Re-staging–
R/O brain metastases before initiating new chemotherapy
1.
MRI with contrast: Study of choice to assess melanoma in CNS!–
More sensitive than CT for detecting brain mets–
Detect spinal cord and leptomeningeal
involvement–
Detect associated hemorrhage or melanin –
Contraindications: non MRI-compatible objects in/on the patient
2.
CT: Patients with MRI contraindications; emergency setting; staging
3.
18FDG-PET/CT: Less sensitive for brain mets, but can be useful
Before we proceed, let’s get our eyes used to the normal brain anatomy on a few MRI images
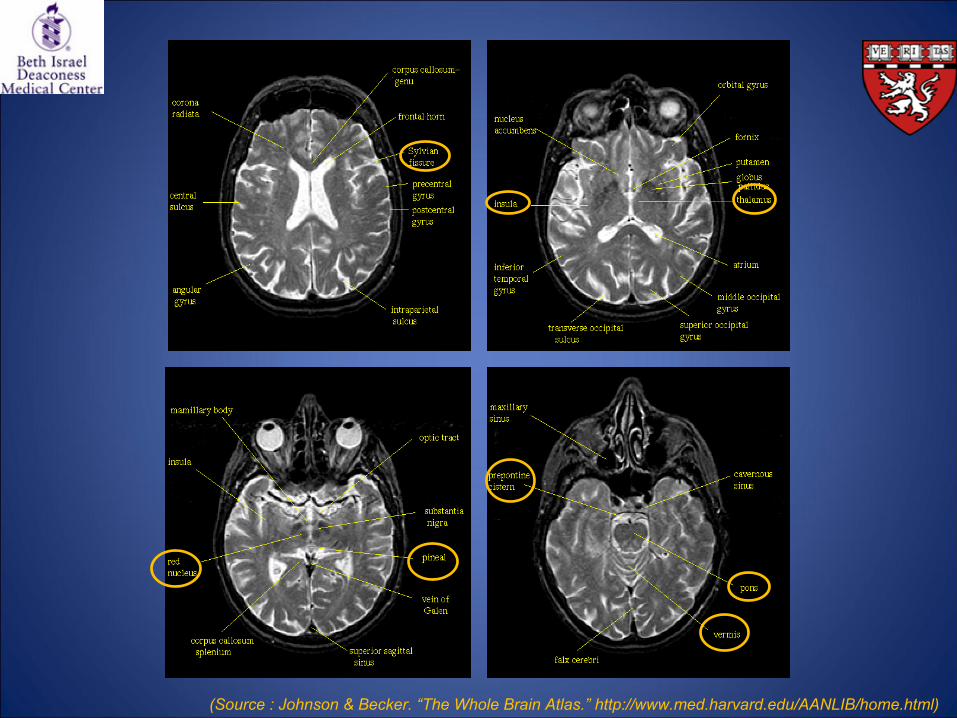
(Source : Johnson & Becker. “The Whole Brain Atlas.”
http://www.med.harvard.edu/AANLIB/home.html)
We have:
1) Learned why diagnostic imaging of metastatic melanoma in the brain is important
2) Reviewed the menu of tests relevant for our discussion
3) Familiarized ourselves with a bit of normal brain anatomy
We are now ready to apply and expand our knowledge…
Interim Summary 1
Case Presentation Patient AC and Her Intractable
Melanoma Brain Mets
Patient AC
42 yo
female with history of metastatic melanoma, presented to ED in 3/07 with headache
2/07: Diagnosed with the first brain mets
from melanoma after experiencing severe headaches; underwent whole brain radiation; dexamethasone
wean to begin TMZ
1d prior to admission: Onset of “slight”
bifrontal
headaches
Day of admission: Worse headaches, pain 5-6/10
Neurologic ROS unremarkable
Patient AC
As the patient presented to the ED with acute headache, CT was first ordered to r/o
bleed
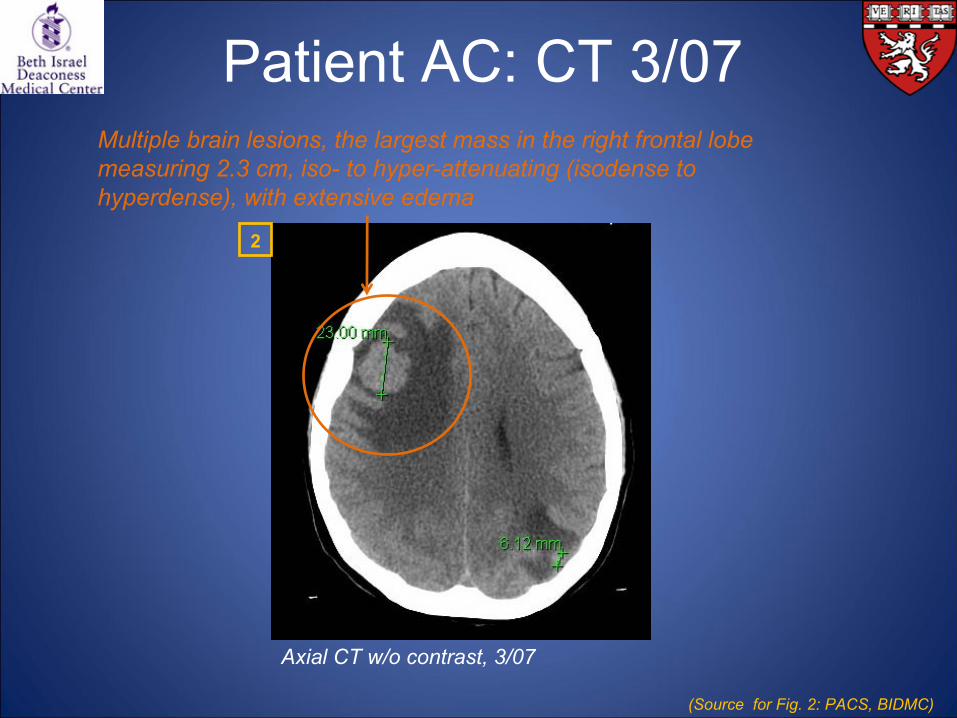
Patient AC: CT 3/07
Axial CT w/o contrast, 3/07
Multiple brain lesions, the largest mass in the right frontal lobe measuring 2.3 cm, iso-
to hyper-attenuating (isodense
to hyperdense), with extensive edema
(Source for Fig. 2: PACS, BIDMC)
2
Patient AC
MRI was recommended for further evaluation of intracranial masses
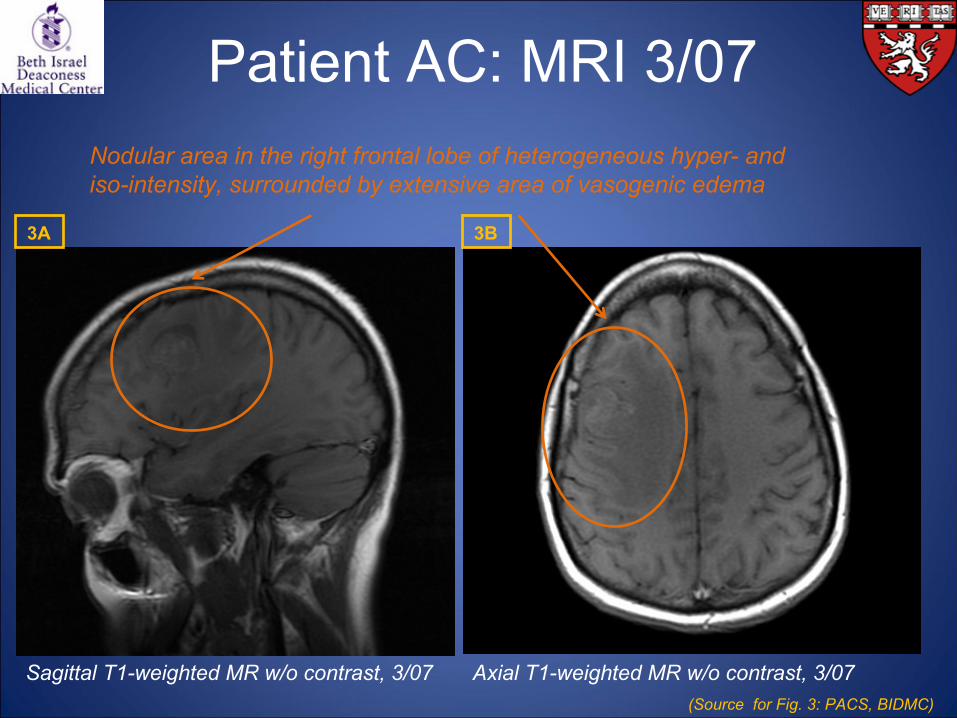
Patient AC: MRI 3/07
Sagittal
T1-weighted MR w/o contrast, 3/07 Axial T1-weighted MR w/o contrast, 3/07
Nodular area in the right frontal lobe of heterogeneous hyper-
and iso-intensity, surrounded by extensive area of vasogenic
edema
(Source for Fig. 3: PACS, BIDMC)
3A 3B
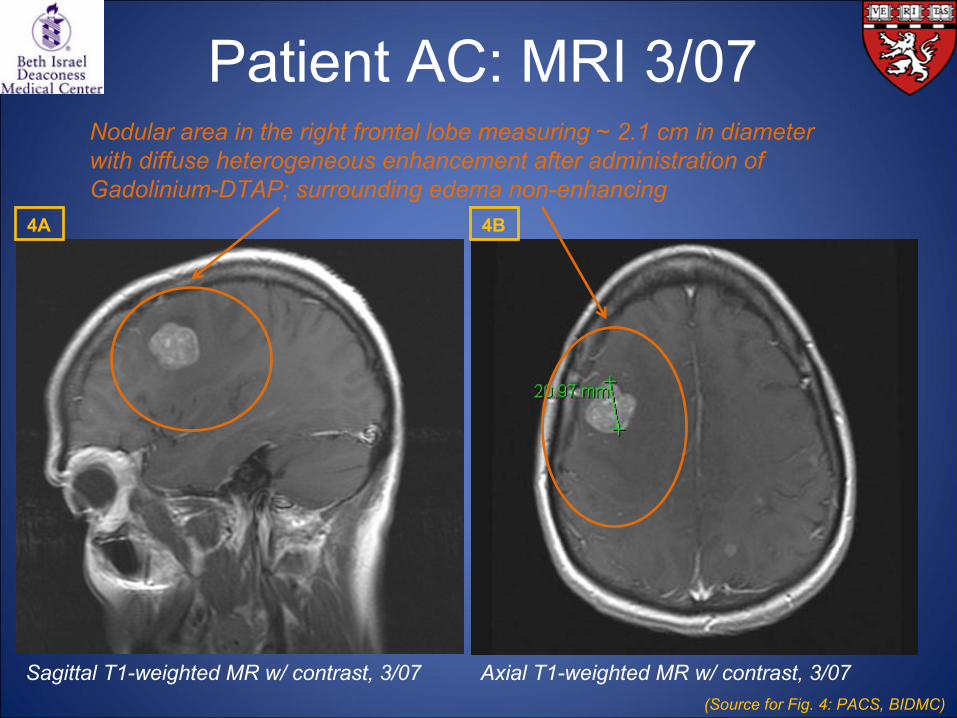
Patient AC: MRI 3/07
Sagittal
T1-weighted MR w/ contrast, 3/07 Axial T1-weighted MR w/ contrast, 3/07
Nodular area in the right frontal lobe measuring ~ 2.1 cm in diameter with diffuse heterogeneous enhancement after administration of Gadolinium-DTAP; surrounding edema non-enhancing
(Source for Fig. 4: PACS, BIDMC)
4A 4B
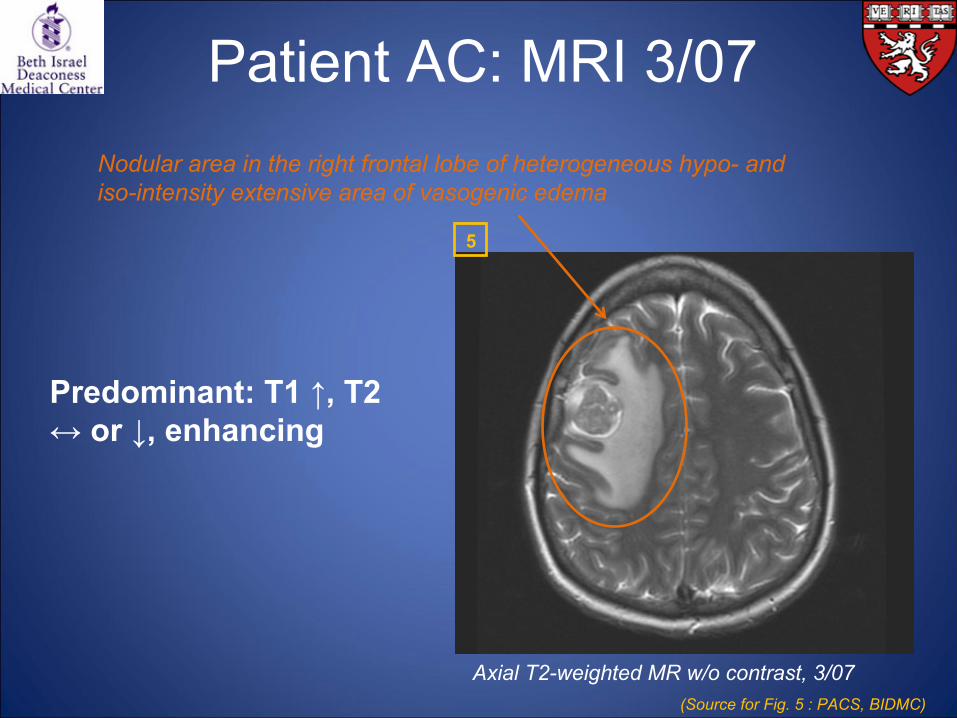
Patient AC: MRI 3/07
Axial T2-weighted MR w/o contrast, 3/07
Nodular area in the right frontal lobe of heterogeneous hypo-
and iso-intensity extensive area of vasogenic
edema
Predominant: T1 ↑, T2 ↔ or ↓, enhancing
(Source for Fig. 5 : PACS, BIDMC)
5

What do we make of these findings?
Let’s study how melanoma brain mets
should appear on MRI
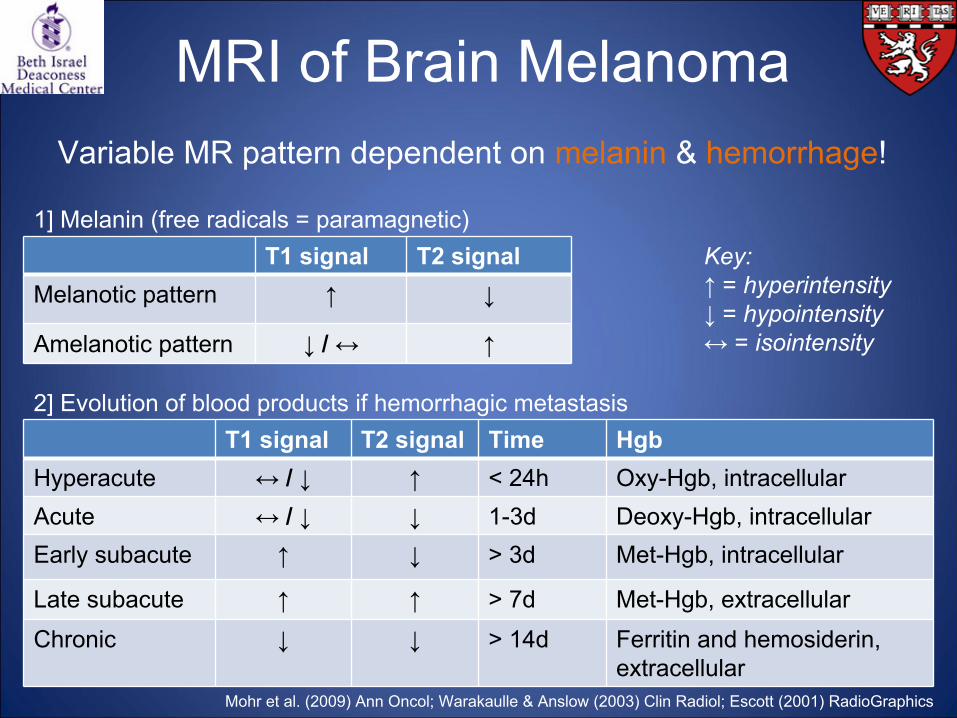
MRI of Brain Melanoma
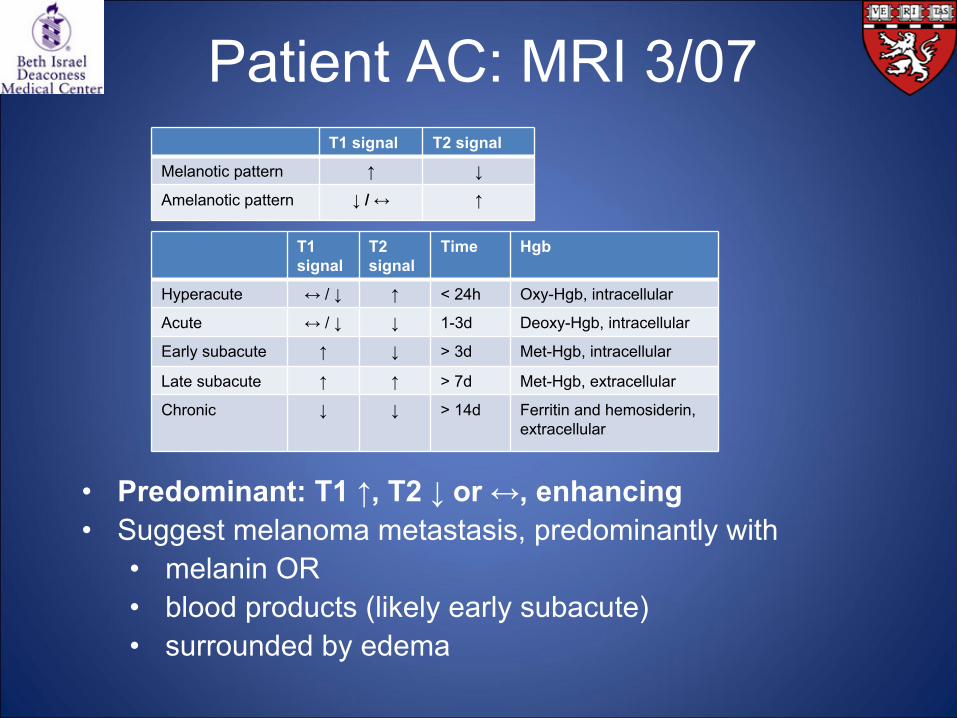
T1 signal T2 signalMelanotic
pattern ↑ ↓
Amelanotic
pattern ↓
/ ↔ ↑
1] Melanin (free radicals = paramagnetic)
2] Evolution of blood products if hemorrhagic metastasisT1 signal T2 signal Time Hgb
Hyperacute ↔ / ↓ ↑ < 24h Oxy-Hgb, intracellularAcute ↔ / ↓ ↓ 1-3d Deoxy-Hgb, intracellularEarly subacute ↑ ↓ > 3d Met-Hgb, intracellular
Late subacute ↑ ↑ > 7d Met-Hgb, extracellular
Chronic ↓ ↓ > 14d Ferritin
and hemosiderin, extracellular
Key:↑
= hyperintensity↓
= hypointensity↔ = isointensity
Mohr et al. (2009) Ann Oncol; Warakaulle
& Anslow
(2003) Clin
Radiol; Escott
(2001) RadioGraphics
Variable MR pattern dependent on melanin & hemorrhage!
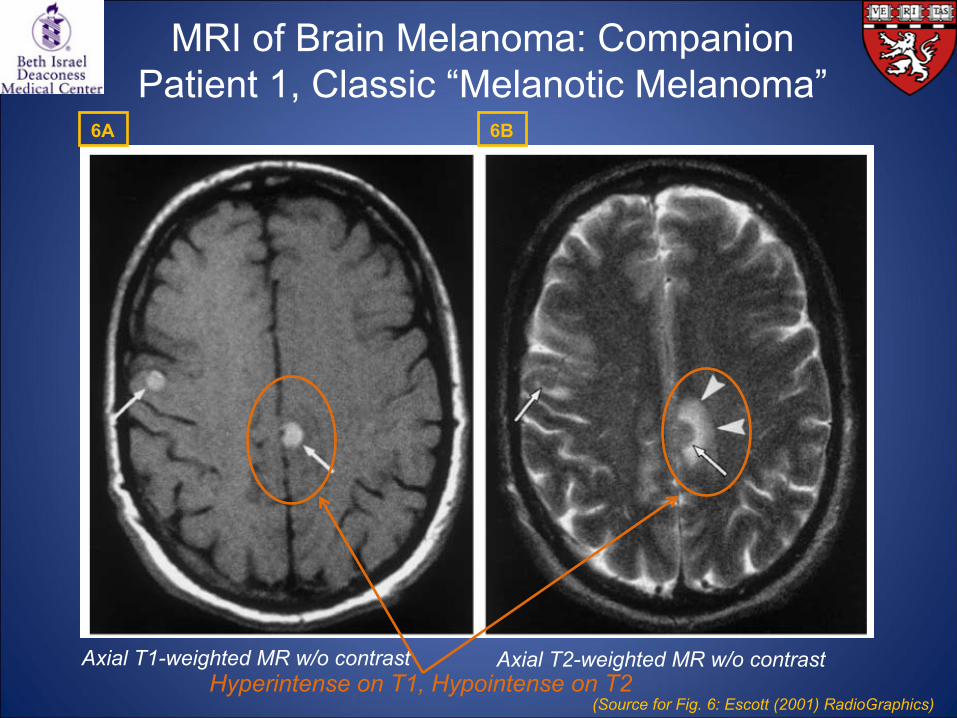
MRI of Brain Melanoma: Companion Patient 1, Classic “Melanotic
Melanoma”
Axial T1-weighted MR w/o contrast Axial T2-weighted MR w/o contrastHyperintense
on T1, Hypointense
on T2(Source for Fig. 6: Escott
(2001) RadioGraphics)
6A 6B

MRI of Brain Melanoma: Companion Patient 2, Classic “Amelanotic
Melanoma”
Axial T1-weighted MR w/o contrast Axial T2-weighted MR w/o contrast
Hypointense
(or isointense) on T1, Hyper-
or iso-intense on T2(Source for Fig. 7: Escott
(2001) RadioGraphics)
7A 7B
Armed with this knowledge, we can now go back to our
Patient AC…
•
Predominant: T1 ↑, T2 ↓
or ↔, enhancing•
Suggest melanoma metastasis, predominantly with •
melanin OR
•
blood products (likely early subacute)•
surrounded by edema
Patient AC: MRI 3/07T1 signal T2 signal
Melanotic
pattern ↑ ↓
Amelanotic
pattern ↓
/ ↔ ↑
T1 signal
T2 signal
Time Hgb
Hyperacute ↔ /
↓ ↑ < 24h Oxy-Hgb, intracellular
Acute ↔ /
↓ ↓ 1-3d Deoxy-Hgb, intracellular
Early subacute ↑ ↓ > 3d Met-Hgb, intracellular
Late subacute ↑ ↑ > 7d Met-Hgb, extracellular
Chronic ↓ ↓ > 14d Ferritin
and hemosiderin, extracellular

•
Hemorrhagic lesions–
Infarcts–
Infections–
Intraparenchymal
hematoma–
Cortical contusions–
Diffuse axonal injuries–
Subarachnoid hemorrhage–
Vascular malformations and aneurysms associated with hemorrhage and/or thrombosis
–
Hemorrhagic primary tumors–
Hemorrhagic metastases•
Melanoma•
Renal cell carcinoma•
Choriocarcinoma•
Bronchogenic
carcinoma•
Thyroid carcinoma
•
Protein-containing lesions–
Colloid cyst of third ventricle–
Craniopharyngioma–
Rathke’s
cleft cyst–
Atypical epidermoid
DDx
of Intracranial Lesions with Increased Signal on T1
•
Fatty lesions–
Lipoma–
Dermoid–
Lipomatous
meningioma
•
Calcified/ossified lesions–
Endocrine-metabolic disorders–
Calcified neoplasms–
Infections–
Dural osteomas
•
Lesions with other mineral accumulation–
Acquired hepatocerebral
degeneration–
Wilson’s disease
•
Melanin-containing lesions–
Melanoma metastases–
Leptomeningeal
melanosis
•
Miscellaneous–
Ectopic neurohypophysis–
Multiple sclerosis (chronic stage)–
Neurofibromatosis type I
Cakirer
et al. (2003) Curr
Probl
Diagn
Radiol

Patient AC: MRI 4/10
4/07 –
4/10: Progressing brain mets; multiple radiosurgeries, radiotherapy, and chemotherapy
4/10•
45 yo, presents with severe bilateral “sharp”
headaches
•
Similar to headaches from prior metastatic disease•
Associated nausea
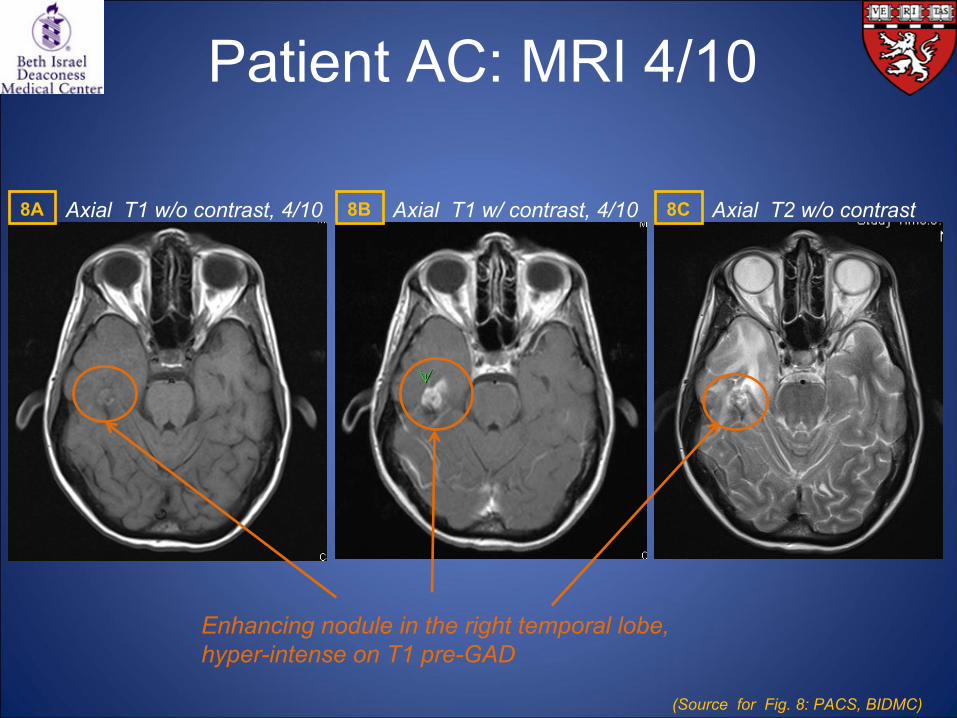
Patient AC: MRI 4/10
Axial T1 w/o contrast, 4/10 Axial T1 w/ contrast, 4/10 Axial T2 w/o contrast
Enhancing nodule in the right temporal lobe, hyper-intense on T1 pre-GAD
(Source for Fig. 8: PACS, BIDMC)
8A 8B 8C
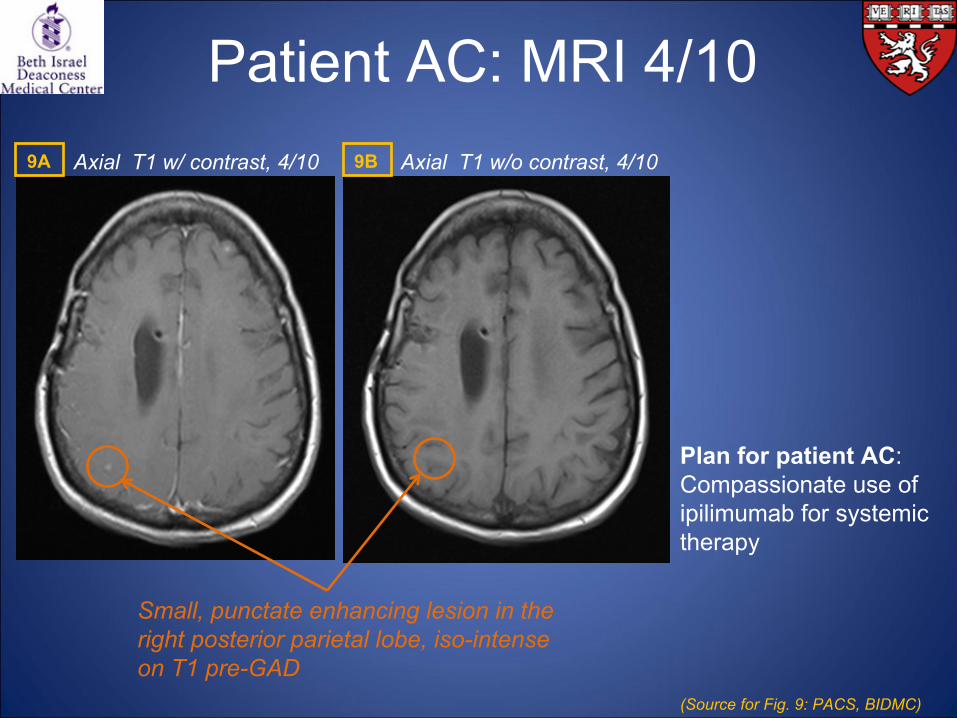
Patient AC: MRI 4/10Axial T1 w/ contrast, 4/10 Axial T1 w/o contrast, 4/10
Small, punctate
enhancing lesion in the right posterior parietal lobe, iso-intense on T1 pre-GAD
Plan for patient AC: Compassionate use of ipilimumab
for systemic therapy
(Source for Fig. 9: PACS, BIDMC)
9A 9B
As we have learned from the multiple MR images, beware of atypical and various appearances of melanoma mets!
1) They can adhere to OR deviate from the typical “melanotic
and amelanotic”
patterns.
2) They can be subtle and small OR easily discernible.
3) They may or may not hemorrhage.
4) They can be stable OR rapidly growing!
Interim Summary 2

What about imaging modalities other than MRI?
Let’s briefly discuss our patients PG and MO…
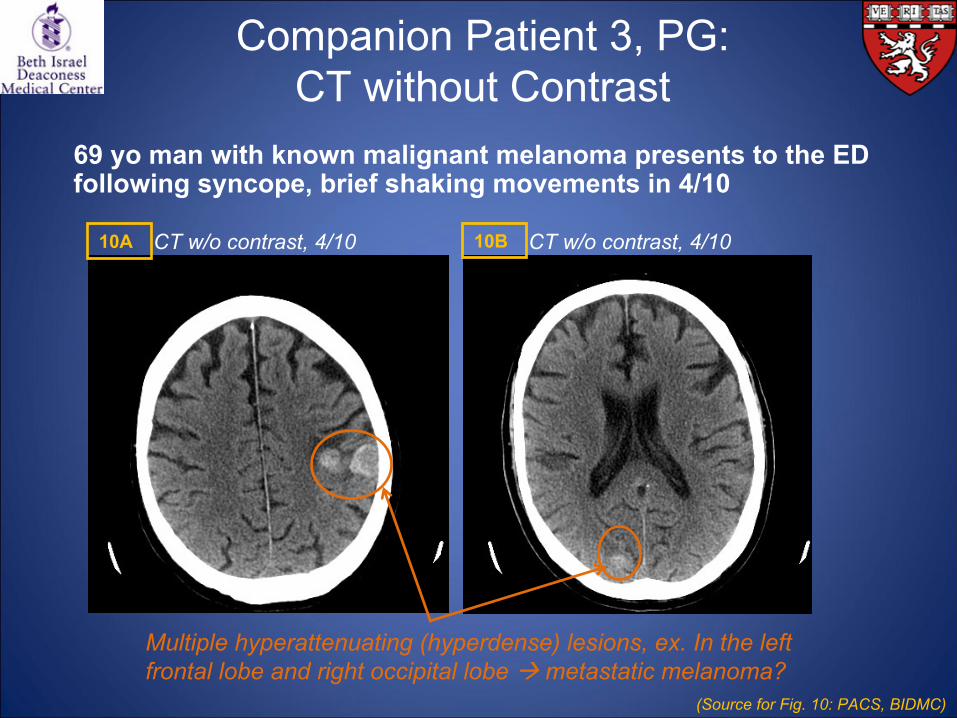
Companion Patient 3, PG: CT without Contrast
Multiple hyperattenuating
(hyperdense) lesions, ex. In the left frontal lobe and right occipital lobe metastatic melanoma?
(Source for Fig. 10: PACS, BIDMC)
10A 10BCT w/o contrast, 4/10 CT w/o contrast, 4/10
69 yo
man with known malignant melanoma presents to the ED following syncope, brief shaking movements in 4/10
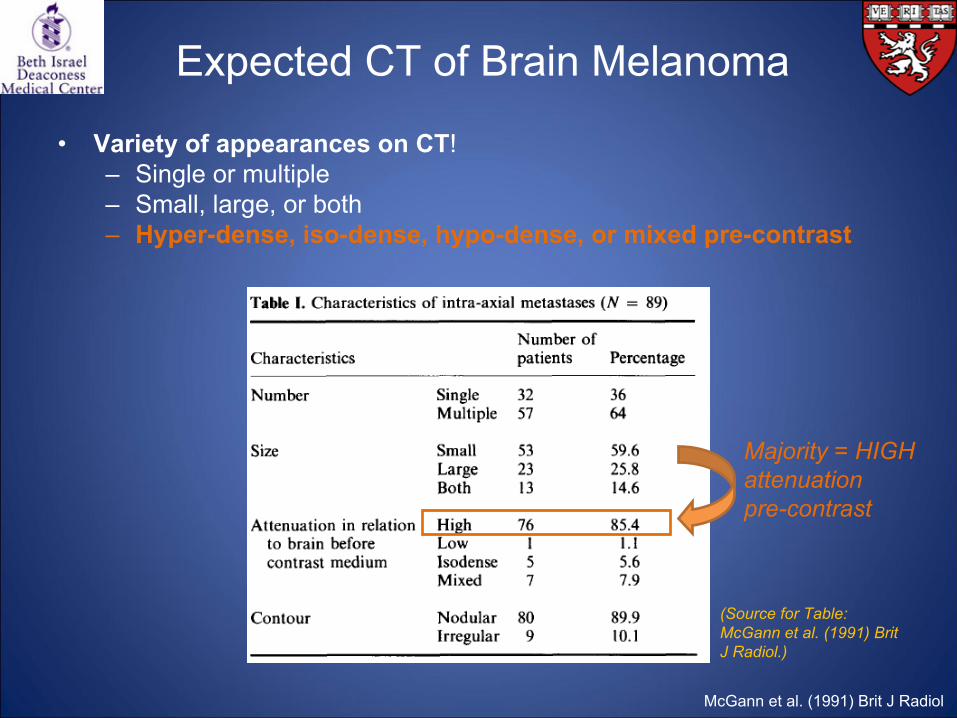
Expected CT of Brain Melanoma
•
Variety of appearances on CT! –
Single or multiple–
Small, large, or both–
Hyper-dense, iso-dense, hypo-dense, or mixed pre-contrast
McGann
et al. (1991) Brit J Radiol
(Source for Table: McGann
et al. (1991) Brit J Radiol.)
Majority = HIGH attenuationpre-contrast
•
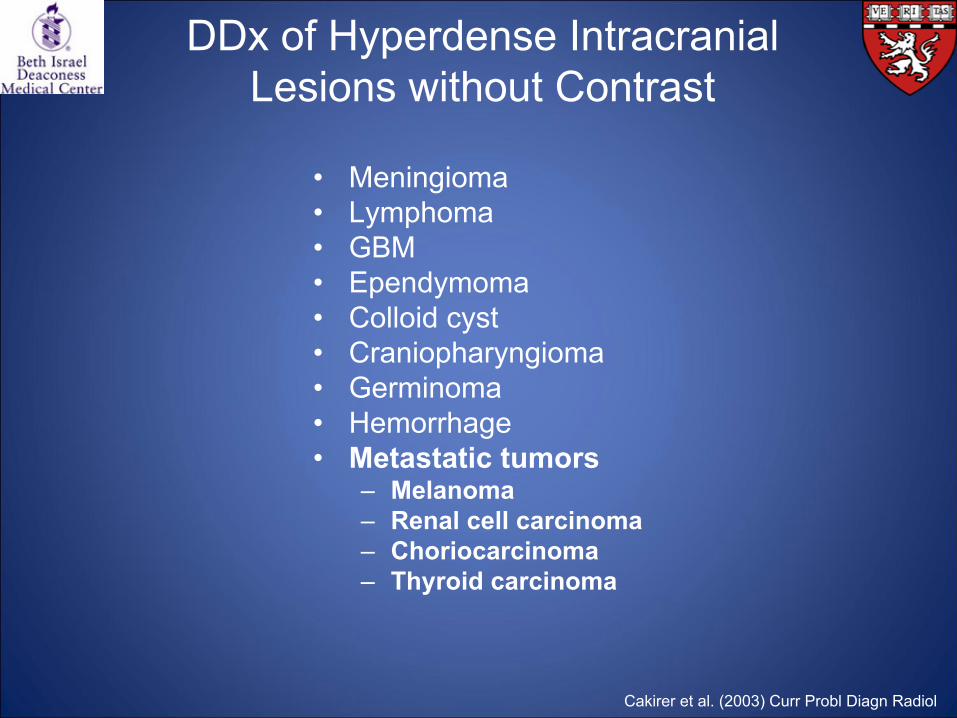
Meningioma•
Lymphoma
•
GBM•
Ependymoma
•
Colloid cyst•
Craniopharyngioma
•
Germinoma•
Hemorrhage
•
Metastatic tumors–
Melanoma–
Renal cell carcinoma–
Choriocarcinoma–
Thyroid carcinoma
DDx
of Hyperdense
Intracranial Lesions without Contrast
Cakirer
et al. (2003) Curr
Probl
Diagn
Radiol
Companion Patient 3, PG: CT without Contrast
•
Patient PG has a pacemaker + renal insufficiency no f/u
on MRI or CT C+
•
Patient PG was scheduled for whole brain cranial irradiation
•
Remember, CT w/o contrast offers only limited evaluation for melanoma brain mets
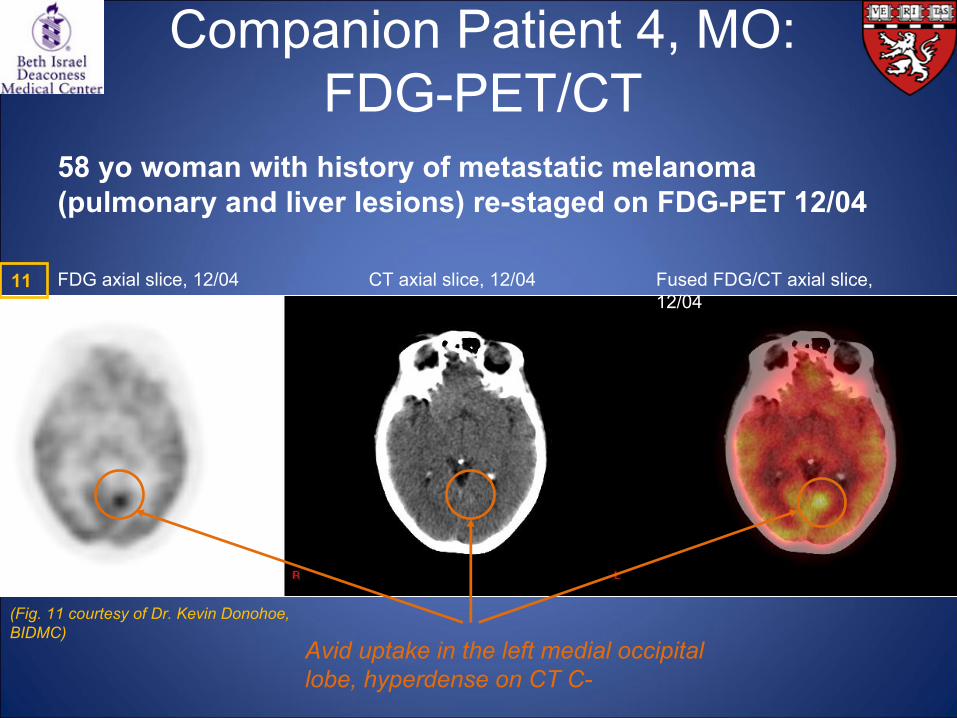
Companion Patient 4, MO: FDG-PET/CT
58 yo
woman with history of metastatic melanoma (pulmonary and liver lesions) re-staged on FDG-PET 12/04
Avid uptake in the left medial occipital lobe, hyperdense
on CT C-
FDG axial slice, 12/04 Fused FDG/CT axial slice, 12/04
CT axial slice, 12/04
(Fig. 11 courtesy of Dr. Kevin Donohoe, BIDMC)
11
Companion Patient 4, MO: DDx
for Increased Signal on PET
•
Infection•
Inflammation
•
Neoplasm•
Beware of physiologic uptake (brain, myocardium, exercising muscle, thymus in children and post-chemo patients, thyroid in patients with thyroid disease, etc)
Delbeke
(1999) J Nucl
Med
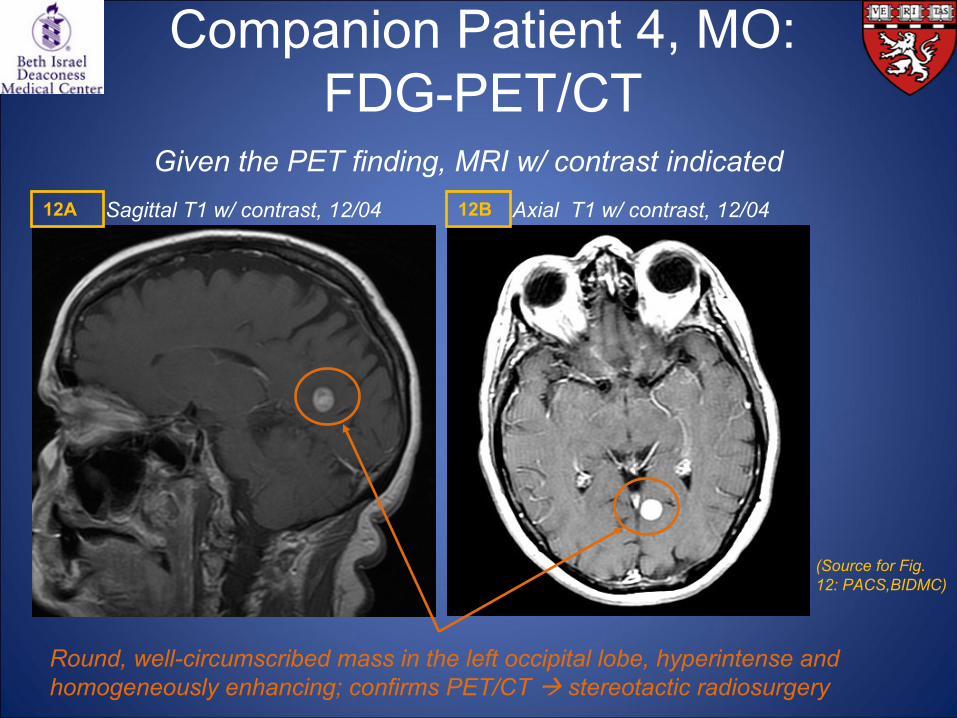
Companion Patient 4, MO: FDG-PET/CT
Given the PET finding, MRI w/ contrast indicated
Round, well-circumscribed mass in the left occipital lobe, hyperintense
and homogeneously enhancing; confirms PET/CT stereotactic radiosurgery
(Source for Fig. 12: PACS,BIDMC)
Sagittal
T1 w/ contrast, 12/04 Axial T1 w/ contrast, 12/0412A 12B
FDG-PET for Brain Melanoma Mets
•
Less sensitive for detection of mets
in the brain due to high background FDG accumulation in the cortex
•
CAN detect new metabolically active lesions: f/u
using conventional imaging methods
•
CAN be useful to w/u
lesions identified in MRI: Recurrence (avid) versus radiation necrosis effects (non-avid)
Delbeke
(1999) J Nucl
Med; Kumar & Alavi
(2005) Curr
Opin
Oncol
Summary
1.
Radiologic imaging of melanoma metastases to the brain is clinically important
2.
MRI with contrast enhancement is the imaging modality of choice for brain metastases of melanoma, and we saw multiple examples in our patient AC
3.
Metastatic melanoma lesions in the brain have a variety of appearances due to hemorrhage and melanin: Beware!
4.
While MRI is the preferred test, CT and FDG-PET/CT have their uses in melanoma imaging in the brain: Remember when and why these imaging modalities can be useful

Acknowledgements
•
Gillian Lieberman, MD•
Kevin Donohoe, MD
•
Neel Madan, MD•
Johannes Roedl, MD
•
Maria Levantakis
References1)
Cakirer
S, Karaarslan
E & Arslan
A (2003). Spontaneously T1-hyperintense lesions of the brain on MRI: a pictorial review. Curr
Probl
Diagn
Radiol
32: 194-217.2)
Delbeke
D (1999). Oncological
applications of FDG PET imaging: brain tumors, colorectal cancer lymphoma and melanoma. J Nuc
Med 40: 591-603.3)
Donohoe
K. Imaging studies in melanoma.
In: UpToDate, Basow
DS (Ed), UpToDate, Waltham, MA, 2010. Viewed May 17, 2010.
4)
Eichler
AF & Loeffler
JS (2007). Multidisciplinary management of brain metastases. Oncologist 12: 884-98. 5)
Escott
EJ (2001). A variety of appearances of malignant melanoma in the head: a review. RadioGraphics
21: 625-39.6)
Jayashankar
A, Sabourin
SM & Mullins ME (2008). AJR teaching file: acute onset headache.
AJR Am J Roentgenol
191(3 suppl): S25-7.7)
Johnson KA & Becker JA. The whole brain atlas. [http://www.med.harvard.edu/AANLIB/home.html]. Viewed May 17, 2010.
8)
Kumar R & Alavi
A (2005). Clinical applications of fluorodeoxyglucose-positron emission tomography in the management of malignant melanoma. Curr
Opin
Oncol
17: 154-9.9)
McGann
GM & Platts
A (1991). Computed tomography of cranial metastatic malignant melanoma: features, early detection, and unusual cases. Brit J Radiol
64: 310-313.10)
McWilliams RR, Brown PD, Buckner JC, Link MJ & Markovic
SN (2003). Treatment of brain metastases from melanoma. Mayo Clin
Proc 78: 1529-36.11)
Miller AJ & Mihm
MC Jr
(2006). Melanoma. N Engl
J Med
355: 51-65.12)
Mohr P, Eggermont
AMM, Hauschild
A & Buzaid
A (2009). Staging of cutaneous
melanoma. Ann Oncol
20 Suppl
6: vi14-21.
13)
Sloan AE, Nock CJ & Einstein DB (2009). Diagnosis and treatment of melanoma brain metastasis: a literature review. Cancer Control 16: 248-55.
14)
Testori
A, Rutkowski
P, Marsden J, Bastholt
L, Chiarion-Sileni
V, Hauschild
A & Eggermont
AMM (2009). Surgery and radiotherapy in the treatment of cutaneous
melanoma. Ann Oncol
20 Suppl
6: vi22-29.15)
Tsao
H, Atkins MB & Sober AJ (2004). Management of cutaneous
melanoma. N Engl
J Med 351: 998-1012.16)
Warakaulle
DR & Anslow
P (2003). Differential diagnosis of intracranial lesions with high signal on T1 or low signal on T2-weighted MRI. Clin
Radiol
58: 922-33.


















