
IMAGING FINDINGS IN INFERTILE FEMALE …ihi.eprints.org/1024/1/muhas25.pdf · ii imaging findings...
52
i IMAGING FINDINGS IN INFERTILE FEMALE PATIENTS WHO UNDERWENT HYSTEROSALPINGOGRAPHY INVESTIGATION AT MUHIMBILI NATIONAL HOSPITAL Ramadhan Bihindi Kabala,MD MMED (Radiology) Dissertation Muhimbili University of Health and Allied Sciences April 2011
Transcript of IMAGING FINDINGS IN INFERTILE FEMALE …ihi.eprints.org/1024/1/muhas25.pdf · ii imaging findings...

i
IMAGING FINDINGS IN INFERTILE FEMALE PATIENTS WHO
UNDERWENT HYSTEROSALPINGOGRAPHY INVESTIGATION
AT MUHIMBILI NATIONAL HOSPITAL
Ramadhan Bihindi Kabala,MD
MMED (Radiology) Dissertation
Muhimbili University of Health and Allied Sciences
April 2011

ii
IMAGING FINDINGS IN INFERTILE FEMALE PATIENTS WHO
UNDERWENT HYSTEROSALPINGOGRAPHY INVESTIGATION AT MUHIMBILI NATIONAL HOSPITAL
By
Ramadhan Bihindi Kabala,MD
A dissertation/Thesis Submitted in Partial Fulfilment of the Requirements for the Degree of Master of Medicine (Radiology) of
Muhimbili University of Health and Allied Sciences
Muhimbili University of Health and Allied Sciences April 2011

iii
CERTIFICATION
The undersigned certify that he has read and hereby recommend for examination the dissertation entitled “Imaging findings in infertile female patients who underwent hysterosalpingography investigation at Muhimbili National hospital” in fulfilment of the requirements for the degree of Master of Medicine (Radiology) of
Muhimbili University of Health and Allied Sciences.
_______________________________ Dr Kazema RR
(Supervisor)
Date: ___________________________

iv
DECRALATION AND COPYRIGHT
I, Ramadhan B Kabala, declare that this dissertation entitled “Imaging findings in infertile
female patients who underwent hysterosalpingography investigation at Muhimbili
National hospital ” is my own original work and that it has not been presented and will not
be presented to any other university for a similar or any other degree award.
Signature………………………………………. Date………………..
This dissertation is a copyright material protected under the Berne Convention, the Copyright
Act 1999 and other international and national enactments, in that behalf, on intellectual
property. It may not be reproduced by any means, in full or in part, except for short extracts in
fair dealing, for research or private study, critical scholarly review or discourse with an
acknowledgement, without the written permission of the Directorate of Postgraduate Studies,
on behalf of both the author and the Muhimbili University of Health and Allied Sciences.

v
ABSTRACT
Background
Fallopian tube and uterine defects are responsible for infertility in more than 30% of infertile
couples. Hysterosalpingography (HSG) is a safe and less invasive method of detecting both
the tubal and uterine defects.
Objectives
To describe hysterosalpingography (HSG) imaging findings in infertile female patients
investigated at Muhimbili National Hospital (MNH)/Radiology department from July to
December,2010
Material and methods
This descriptive cross-sectional study, involved 130 women participants with infertility who
attended MNH Radiology department for HSG examination between July to December 2010.
Demographic data and radiological findings were reviewed and the obtained data analysed
with SPSS version 15. Statistical level of significance was set at p < 0.05.
Results
The participants mean age was 30 years and mean duration for infertility was 5 years.
Secondary infertility was slightly commoner than primary infertility. Majority (70%) of
patients were aged 16-30 years. Abnormal findings at HSG were found in 60% of the patients.
Most of these abnormal findings were found in those patients with older age between 31 and
45 years and those with long duration of infertility for more than 5 years. The commonest
finding was tubal blockage accounting 41% of cases and the least was uterine congenital
abnormality (3.8%). Uterine fibroid was the commonest uterine pathology accounting for
10% of all cases.
Conclusion
Generally, high proportion of patients in this study showed presence of uterine and fallopian
tubes pathology. Fallopian tubal blockage was the most diagnosed tubal structural
abnormality while the uterine leiomyoma was the highest uterine pathology. There was no

vi
significant difference in the presence of pathology between patients with primary and
secondary infertility. However, older age above 30 years were significantly associated with
presence of structural abnormality in both uterus and fallopian tubes
Recommendation
HSG is recommended for initial routine work-up of infertile women.
Further studies are needed to establish the aetiologies of these abnormalities.
.

vii
TABLE OF CONTENTS CERTIFICATION .....................................................................................................................iii DECRALATION AND COPYRIGHT...................................................................................... iv ABSTRACT................................................................................................................................ v ACRONYMS............................................................................................................................. ix LIST OF TABLES ...................................................................................................................... x LIST OF FIGURES ................................................................................................................... xi DEDICATION ..........................................................................................................................xii ACKNOWLEDGEMENTS.....................................................................................................xiii 1.0 INTRODUCTION AND LITERATURE REVIEW............................................................ 1
1.1 Prevalence of infertility..................................................................................................... 1 1.2 Radiological investigations of infertility........................................................................... 2 1.3 HSG Findings.................................................................................................................... 4
2.0 PROBLEM STATEMENT ................................................................................................... 7 3.0 STUDY RATIONALE.......................................................................................................... 8 4.0 OBJECTIVES ..................................................................................................................... 10
4.1 Broad Objectives............................................................................................................. 10 4.2 Specific Objectives......................................................................................................... 10
5.0 METHODOLOGY.............................................................................................................. 11 5.1 Study design and period ............................................................................................. 11 5.2 Study setting ............................................................................................................... 12 5.3 Study population......................................................................................................... 12 5.4 Exclusion criteria........................................................................................................ 12 5.5 Sample size Estimation .............................................................................................. 12 5.6 Sampling technique .................................................................................................... 12 5.7 Data collection............................................................................................................ 12
5.8 Data analysis..............................................................................................................13 5.9 Ethical consideration.................................................................................................. 13
6.0 RESULTS ........................................................................................................................... 14 6.1 Demographic and clinical data........................................................................................ 14 6.2 Hysterosalpingography findings ..................................................................................... 15
6.2.1 HSG findings by demographic characteristicts and fertility status.......................... 15 6.2.2 Pattern of uterine and fallopian tubes abnormalities................................................ 17 6.2.3 HSG uterine findings ............................................................................................. 187 6.2.4 HSG fallopian tubes findings................................................................................... 18
7.0 DISCUSSION .................................................................................................................... 21 8.0 STUDY LIMITATION....................................................................................................... 27 9.0 CONCLUSION................................................................................................................... 27 10.0 RECOMMENDATIONS.................................................................................................. 28 11.0 REFERENCES.................................................................................................................. 29 APPENDEX:I. DATA COLLECTION SHEET....................................................................... 34

viii
APPENDEX: II. Consent: English version............................................................................... 36 APPENDEX: III. Consent: Swahili version.............................................................................. 38
ix
ACRONYMS
CI; Confidence interval
HSG; Hysterosalpingography
IRB; Institutional Review Board
LMP; Last Menstrual period
MNH; Muhimbili National Hospital
MRI; Magnetic Resonance Imaging
MUHAS; Muhimbili University Of Health and Allied Sciences
PID; Pelvic inflammatory disease
S.d; Standard deviation
SPSS; Statistical Package for Social Science
UK; United kingdom

x
LIST OF TABLES Page
Table 1: Descriptive statistics ...............................................................................................12
Table 2: Age distribution by type of infertility......................................................................13
Table 3: HSG findings by demographic characteristics and fertility status...........................14
Table 4: Summary of HSG uterine findings...........................................................................15
Table 5: Summary of HSG fallopian tubes findings..............................................................16

xi
LIST OF FIGURES Page
Figure 1: Histogram showing age distribution of patients...............................................12
Figure 2: Distribution of uterotubal abnormalities..........................................................14
Figure 3: HSG images showing bicornuate uterus..........................................................15
Figure 4: HSG images showing a filling defect due to fibroid........................................16
Figure 5: HSG image showing hydrosalpinx..................................................................17
Figure 6: Normal HSG images.......................................................................................18

xii
DEDICATION I dedicate this dissertation to my mother, Asha Ramadhan, my wife Rahma Lugoye Antony and our children Hashim and Aisha.

xiii
ACKNOW LEDGEMENTS
My sincere gratitude and appreciation to the Ministry of Health and Social Welfare for
sponsoring my course and this dissertation. I’m greatly indebted to my supervisor Dr. Kazema
R R for his valuable advice and support throughout the study period. His tireless efforts,
encouragement and constructive inputs made this work a success. Sincere appreciations to the
Head of Muhimbili National Hospital Radiology Department and members of the department
for their tireless assistance and advice during the period of preparation of this dissertation.
Special thanks to Dr.Hokororo J, Dr. Akoko L and Dr. Mwanga A for their support during
data analysis. I am also indebted to my family and friends for their tireless moral and material
support.

1
1.0 INTRODUCTION AND LITERATURE REVIEW
1.1 Prevalence of infertility
The problem of infertility in our setting is common in day to day practice. Infertility is
defined as the inability of a couple to achieve conception after 12 months doing
unprotected coitus. Primary infertility describes couples who have never been able to
become pregnant after at least 1 year of unprotected sexual intercourse. Secondary
infertility describes couples who have been pregnant at least once, but have not been able
to become pregnant again. It is estimated that 8 to 15% of all women experience primary
or secondary infertility at one point in time in their reproductive life. In tropical Africa,
infertility rate is between 10% to 20%, although the prevalence in Congo was reported to
be high between 30% to 50% (1, 2, 3, 4). In Tanzania national demographic and health
survey conducted in 1999 showed that 2.5% of women had primary infertility while 18%
had secondary infertility. The prevalence of infertility was 8.1% in previous study
conducted in Moshi northern part of Tanzania with secondary infertility being more
common than primary infertility (5).
Primary infertility is relatively low and it exceeds 3% in most African countries (5).
Several studies showed that secondary infertility is more common than primary infertility
(6, 7, 8). Secondary infertility for women aged 20-44 ranges from 5% in Togo to 23% in
Central Africa Republic (5). Some studies done in Turkey and Iran found out that
primary infertility was more common, when compared to secondary infertility (9,10).
Women with secondary infertility have a higher likelihood of having structural
abnormalities in both uterus and fallopian tubes in comparison to those with primary
infertility (11,12).

2
1.2 Radiological investigations of infertility
Hysterosalpingography (HSG) is readily available investigation in our settings, as such
is one among the investigations used for evaluation of infertility. It is the best first line
anatomic imaging investigation for the basic infertility work. HSG evaluates the cervical
canal, uterus, fallopian tubes and the pelvic cavity (13,14).
Hysterosalpingography (HSG) demonstrates the morphology and patency of both the
uterine canal and fallopian tubes (15,16). HSG is performed by injecting contrast
medium into the uterus and the fallopian tubes and following its flow using fluoroscopy.
Uterine abnormalities are outlined by the contrast medium and fallopian tubal
obstruction is noted by the absence of free spill into the peritoneal cavity (13,17). In
addition to the diagnostic value, HSG may also be used for therapeutic purposes to
unblock the blocked fallopian tubes (18,19).
The size of the uterine cavity varies with parity. The endocervical canal is of cylindrical
shape with length of 3 to 4cm and width of 1 to 3cm (1). The uterine cavity is sharply
defined by HSG having a triangular shape with mild concavity at the fundus. The
normal fallopian tube has a length between 10 to 12 cm extending from cornua of the
uterus. Its lumen is threadlike with width of 1 to 2mm until reaches ampulla where it
expands to 5 and up to 10mm with visible rugal folds.
Although HSG has a lot of advantages as outlined above, but there are some
disadvantages accompanying it. These are the possibility of allergic reaction to iodine,
pelvic infection, bleeding spots, endometriosis secondary to carriage of endometrial
tissue onto extra uterine sites and tubal rupture due to contrast material given under
pressure in patient with hydrosalpinx.
Other techniques for assessing structural causes of female infertility such as ultrasound,
sonohysterography (Hycospy), laparoscopy, magnetic resonance imaging (MRI) and
hysteroscopy are increasingly used elsewhere. HSG is not reliable test for evaluation of
extrinsic tubal pathology such as peritubal adhesions compared to other techniques

3
(20,21,22). However it has the advantage over other techniques by giving a clear tubal
resolution and definition (2,15).
In hysteroscopic procedure the scope is used to visualize the inside of the uterus
including the openings of fallopian tubes and can be used for treatment of intrauterine
pathology. However the procedure may complicate rarely with perforation of the uterus,
infection and reaction to anaesthetic agents.
Laparoscopy examination provides accurate information about extrinsic tubal pathology
but is poor in diagnosing intrinsic tubal pathology. Laparoscopy is performed under
general anaesthesia during the follicular phase of the menstrual cycle. After making
pneumoperitoneum, a thorough inspection of pelvis and pelvic organs is performed. This
is followed by testing the patency of fallopian tubes using methylene blue. A dilute
solution of methylene blue is injected through the cervix via a cannula. The evaluation of
adhesions, structural abnormalities of the uterus, endometriosis and fallopian tubes
occlusion are sought for.
Laparoscopy also has the advantage of allowing treatment of abdominal pathology such
as endometriosis and peritubular adhesions. Moreover, both laparoscopy and
hysteroscopy procedures are invasive with related risk of surgical complications, high
cost as well as high expertise. They are not able to give detailed information on the
uterine, making them disadvantageous over HSG. A study done in India revealed that
Hysterosalpingography and Laparoscopy are complimentary rather than competitive
procedures (23). Both hysteroscopy and laparoscopy should therefore be reserved for
confirmation and treatment of the intrauterine and fallopian tubes abnormalities (24,25).

4
Ultrasound has a great role in diagnostic as well as therapeutic management of infertility.
It can confirm the normal anatomy of the pelvis, assessing ovarian morphology and look
for uterotubal and pelvic pathology such as fibroids, hydrosalpinx and endometriosis.
Ultrasound is also used in monitoring menstrual cycle so that ovulation can be confirmed
in both natural cycles and due to induction agent like clomifene. However ultrasound is
poor in confirming the patency of fallopian tubes (26,27).
In experienced hands sonohysterography is safe, well tolerated and easy to assess
intrauterine structures more superior than HSG (28,29). In this procedure the cervix is
inspected through vaginal speculum and cleansed with antiseptic solution. A
polyethylene cannula is introduced and the speculum removed. Then a sterile sheathed
vaginal ultrasound probe is introduced. Lastly, an infusion of normal saline is
commenced gradually with a slow and sustained flow while scanning the endometrial
cavity and myometrium. Several studies showed that sonohysterography (Hycospy) is
similar to HSG as regards to the appearance of endometrial cavity but is inferior to it for
evaluation of tubal factor (30-34).
Magnetic resonance imaging (MRI) is the study of choice in infertile women with
suspected uterine anomalies because of its high accuracy and detailed elaboration of
uterovaginal anatomy. It is superior in diagnosing uterine anomalies, but is poor to
diagnose intrauterine adhesions and peritubal adhesion as compared to HSG (35).
1.3 HSG Findings
The normal HSG findings in infertile women was found to be low, 16.6% in Uganda
and 18.2% in South Africa(2,6), whilst in UK and Nigeria studies showed high
proportion of infertile women with abnormality, 51.5% and 60% respectively (3,15).

5
Almost one quarter of women with congenital or acquired structural uterine
abnormalities experience difficult in conception, accounting for up to 10% of infertility
cases (2). HSG has been found to be an invaluable procedure for the assessment of intra-
uterine lesions(18,36,37).The uterine abnormalities using HSG were present in 25% of
South African black patients with half of them having fibroids and only 2.5% of cases
had congenital abnormalities(6). However in a study conducted in UK only 15.2% of
cases had uterine abnormalities, in which 5.8% presented with congenital abnormalities
and 5.5% of the cases presented with fibroids with rest being polyps, Asherman
syndrome and post-caesarean scar(15). The congenital uterine abnormalities among
Nepalese women with primary infertility are 3.2% whilst those with secondary infertility
are 2% (47).
HSG is widely used as a first line approach to assess the patency of fallopian tubes in
routine fertility work-up (15,16).Tubal factor remain a cause of infertility which accounts
for 35% to 40% of cases of infertility(3,7,23). Previous studies revealed that tubal
pathology is significantly associated with secondary infertility(8) .In a study which was
done in South Africa among infertile black patients, 81.8% of cases had fallopian tube
abnormalities(6). In that study 5% of cases had peritoneal adhesions while the tubal
blockage was present in 27.4% of cases and the most common abnormality was the
terminal hydrosalpinx(6). Bilateral tubal occlusion was noted in 20% of infertile women
in a study done in Kenya. In several studies hydrosalpinx was the most common tubal
abnormality (3,6,15). Similarly, series done in Nigeria showed that hydrosalpinx was the
most common tubal abnormality which was present in 23.3% of patients. In this study
patients with bilateral tubal blockage were 7.5% while 13.3% of cases had unilateral
tubal blockage (3).
Tubal blockage was present as the most common tubal abnormality, 37.7% in a study
done in Birmingham, UK with hydrosalpinx accounting for 20.6% of cases(15).

6
In a study done in Turkey, 21% of infertile women had one sided tubal occlusion and
12% had bilateral tubal occlusion. Features for adnexal adhesion were seen among 12%
of infertile women in Turkey (9).
Therefore, assessment of the structural integrity of the reproductive tract is essential to
fertility evaluation and necessary for all female patients presenting with infertility. Thus
HSG still remains a more accurate and efficient method for the diagnosis of intrinsic
tubal and uterine pathology.

7
2.0 PROBLEM STATEMENT
Infertility is a global problem, but the highest prevalence is in low resources areas,
particularly Sub-Saharan Africa where infection-related tubal damage is the commonest
cause (38). The prevalence of uterotubal structural abnormalities by HSG ranges from
about half among women with infertility in Nigeria to three quarter in Uganda and South
Africa (2,3,6).
Currently in Tanzania little is known about the magnitude of the problem in terms of
common etiological factors; what is the most common cause of infertility, is it ovulatory
dysfunction, or is it structural abnormalities or is it hormonal infertility.
Observation of patients attending Radiology department at MNH reveals significant
number of women with infertility coming for evaluation of structural abnormalities.
In view of above arguments there is a need to conduct an investigation that is reliable and
which is readily available for screening possible structural abnormalities in reproductive
anatomy.
This can easily be done by hysterosalpingography (HSG) which is widely available in all
regions in Tanzania. It is affordable, readily available and yields reliable findings.
Therefore, this study looks into clinically reliability and usefulness of HSG in evaluation
of structural pathology in uterus, fallopian tubes and pelvis.
8
3.0 STUDY RATIONALE
The prevention of infertility in a population requires an active surveillance mechanism to
be in place. Previous studies done in other parts of Sub-Saharan Africa showed that the
major underlying cause for the high levels of infertility is the tubal blockage which is a
sequel of pelvic infection. These infections follow mismanaged deliveries, abortion and
sexually transmitted infections.
This calls for a study that is cheap, available and sensitive to document the pattern of
uterine and fallopian tubes diseases that are the culprit of infertility among women in our
setting.
In developing countries like Tanzania where resources are still limited, widely available
fluoroscopy units can be wisely used to investigate and even manage the women with
infertility.
Therefore, the results of this study will reveal the prevalence of uterotubal structural
abnormalities that will be used for comparison with other studies elsewhere and assist in
planning of future research areas on infertility.
Use of HSG investigation in infertile women may provide important information useful
to the Gynaecologist during treatment planning. It will also provide useful information on
pattern and proportion of uterine and tubal abnormalities necessary for formulating
various strategies for prevention of infertility, as almost all causes of tubal blockage are
preventable.

9
Therefore by knowing these underlying causes, various strategies can be put in place
through improving prevention, diagnosis and treatment of infertility at all levels of health
care delivery. Hence, this study is significant in the sense that the findings contained
herein will contribute to knowledge concerning the role of uterotubal structural
abnormalities as the cause of infertility in women.

10
4.0 OBJECTIVES
4.1 Broad Objectives
To describe imaging findings in infertile female patients who underwent
Hysterosalpingography investigation at Muhimbili National Hospital (MNH), Radiology
department, July to December, 2010.
4.2 Specific Objectives
1. To determine the proportion of women with congenital uterine anomalies.
2. To determine the proportion of women with tubal blockage.
3. To determine the pattern of uterotubal abnormalities in infertile female patients.
4. To determine association between the type of infertility and diagnosis of abnormal
HSG findings.

11
5.0 METHODOLOGY
5.1 Study Design and Period;
This was a descriptive cross sectional study conducted between July to December, 2010.
5.2 Study setting;
5.2.1 The study was conducted at Muhimbili National Hospital, Radiology department.
Patients were referred from gynaecology clinic of MNH by a gynaecologist. HSG
procedure was performed by an investigator supervised by a radiologist on duty. The
findings were interpreted by the investigator and discussed with the senior radiologist
before handled to patients.
5.2.2 Hysterosalpingography Procedure; There was no specific patient preparation
required and the examination was scheduled during days 7-12 of the menstrual cycle.
The endometrium is thin during this proliferative phase, a fact that facilitates image
interpretation and should also ensure that there is no pregnancy. The patient instructed
to abstain from sexual intercourse from the time menstrual bleeding ended until the
day of the study to avoid a potential pregnancy. The patient placed on the fluoroscopy
table in the lithotomy or modified lithotomy. The perineum cleaned with savlon and
draped with sterile towels. A speculum was inserted in the vagina and the cervix
localized and cleansed with savlon. Then a cannula positioned in the cervical canal. A
scout radiograph of the pelvis then taken with cannula in place. Water soluble contrast
(Ultravisit) about 10-30 ml slowly instilled with fluoroscopic images obtained
intermittently to evaluate the uterus and fallopian tubes. The first image obtained
during early filling of the uterus and used to evaluate any filling defects or contour
abnormality. The second image was taken with uterus fully distended, the shape of the

12
uterus is best evaluated at this stage. The third image was obtained to demonstrate and
evaluate the fallopian tubes and free intraperitoneal spillage of contrast material
5.3 Study Population; The study involved women who were evaluated at the Radiology
department due to infertility between July and December, 2010.
5.4 Exclusion criteria; The study did not involve women patients with acute infection of the
vagina or cervix and also women with active vaginal bleeding. Other groups of patients
that were also excluded from the study were those with sub fertility complaints lasting
less than a year.
5.5 Sample size Estimation; Considering the study power of 95%, a random likely error is
estimated to be 5%.The sample size of 113 patients were to be studied estimated basing
on the general population prevalence of 8.1% of infertile women in Tanzania(5). The
standard sample size estimation formula(Kish and Leslie) is N = z2p (1-p) ÷ E2 where
Z – is the point of normal distribution corresponding to the significant level of 1.96; p-
prevalence from the general population of infertile women which is 0.08; E – Maximum
likely error which is 0.05. Therefore the sample size is calculated as follows N=
(1.96)2*0.0.8(1-0.08) ÷ 0.052 =113
5.6 Sampling technique; a consecutive sampling method was used, due to limited time and
difficult in defining sampling frame as there is no specific clinic for infertility. Hence all
patients referred to the Radiology department for hysterosalpingography examination
were included after considering inclusion and exclusion criteria till the sample size
reached.
5.7 Data collection; Data collection in this study involved interviewing the patients to obtain
the demographic particulars. The special designed clinical surveillance forms (Appendix
I) used to collect both demographic and HSG findings. Data collections from each day
were done on the same day and then the obtained data were recorded in sheets and

13
transferred to the analysis program. To minimize the observer bias the report included the
documentation from the investigator and certification from a senior radiologist. The
findings were then communicated to the patients through the gynaecology clinic as they
continued to be followed up.
5.8 Data analysis;
The identification number was labelled in each of the filled clinical surveillance form and
screened before entering into the statistical package for social science (SPSS). Quantitative
data were then tabulated, analyzed and interpreted according to the result obtained. Then all
variables summarized and printed out for careful study and a cross tabulation done for defined
independent variables in order to obtain table of results. Data entry, filter and analysis was
done using SPSS version 15 analysis program. Chi- square statistical test was done to check
for statistical significance p<0.05.
5.9 Ethical consideration
Research protocol was submitted to the MUHAS Higher Degrees Research and Publications
Committee for review, approval and ethical clearance processing. Ethical clearance letter was
obtained before commencing the study. The aim of the study as well as potential risks and
benefits were clearly explained to all participants and a written informed consent in Swahili
language was signed by each participant (Appendix II). A participant had the right and
freedom to join or leave the study unconditionally. A patient who did not consent for the
study but entitled was attended as usual. Confidentiality was observed during performing the
HSG procedures as well as during conversation. A written report of findings was given to
patient and sent to gynaecologist.
14
6.0 RESULTS
6.1 Demographic and clinical data
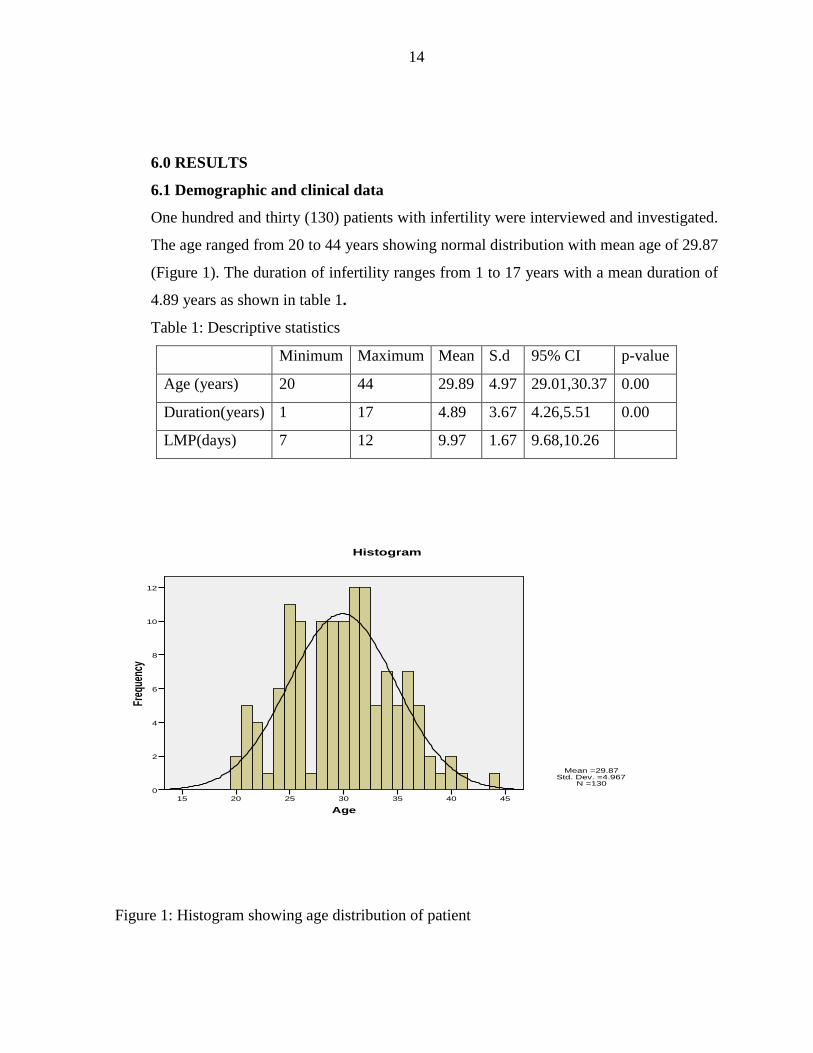
One hundred and thirty (130) patients with infertility were interviewed and investigated.
The age ranged from 20 to 44 years showing normal distribution with mean age of 29.87
(Figure 1). The duration of infertility ranges from 1 to 17 years with a mean duration of
4.89 years as shown in table 1.
Table 1: Descriptive statistics
Minimum Maximum Mean S.d 95% CI p-value
Age (years) 20 44 29.89 4.97 29.01,30.37 0.00
Duration(years) 1 17 4.89 3.67 4.26,5.51 0.00
LMP(days) 7 12 9.97 1.67 9.68,10.26
Age45403530252015
Freq
uenc
y
12
10
8
6
4
2
0
Histogram
Mean =29.87�Std. Dev. =4.967�
N =130
Figure 1: Histogram showing age distribution of patient

15
Table 2 shows that more participants had secondary infertility 68 (52.3%). More patients
70(53.8%) aged 16-30 years . The young aged group 16-30 years had a high proportion of
primary infertile participants(67.7%) while more secondary infertile patients,58.8% were in
age 31-45 years which was statistically significant (p= 0.002).
Table 2: Age distribution by type of infertility
Type of infertility
Age groups Primary % Secondary % Total %
16-30 42 67.7 28 41.2 70 53.8
31-45 20 32.3 40 58.8 60 46.2
Total 62 47.7 68 52.3 130 100
Pearson Chi-square,x2=9.209, df=1, p-value=0.002
6.2 Hysterosalpingography findings
6.2.1 HSG findings by demographic characteristic and fertility status of women. Table 3 shows that patients who aged 31-45 years had more abnormal HSG findings (71.7%)
than those of aged 16-30 years. The difference seen is statistcally significant (p-value=0.012).
However patients with secondary infertility had slightly more abnormal HSG findings
(60.3%) than those with primary infertility (59.7%). This difference is not statistically
significant (p-value=0.943). More patients had duration of infertility of 1-5 years (63%) and
those with long duration (5-17 years) had more abnormal HSG findings (73%) compared to
those with short duration(52%). This difference is statistically significant(p-value=0.021).

16
Table 3 . HSG findings by demographic characteristic and fertility status(N=130)
HSG Findings Statistics Normal Abnormal p-value Age groups 16-30 35(50%) 35(50%) 0.012p 31-45 17(28.3%) 43(71.7%) Type of infertility Primary 25(40.3%) 37(59.7%) 0.943p Secondary 27(39.7%) 41(60.3%) Duration of infertility(years)
1-5 39(48%) 43(52%) 0.021p >5 13(27%) 35(73%) P= Pearson chi square 6.2.2 Pattern of uterine and fallopian tubes abnormalities
The study revealed that fallopian tubal blockage was the highest abnormality affecting
53(41%) infertile women followed by 25(19%) women with uterine abnormality, 23(18%)
women with pelvic adhesion and 17 (13%) women with hydrosalpinx as shown in figure 2.
0
10
20
30
40
50
Uterin
e ab
norm
ality
Tubal
block
age
Hydro
salpi
nx
Pelvic
adhe
sion
Pattern of uterotubal abnormalities
Pattern of uterotubalabnormalities
Figure 2. Distribution of uterotubal abnormalities

17
6.2.3 HSG uterine findings
Table 4 shows that uterine filling defect due to fibroids was the most common abnormality
seen accounting for 10% of all patients(figure 4), the irregular uterine cavity which may be
due to endometritis or synechiae was seen in 5.4% while patients with congenital abnormality
was 3.8% (figure 3).
Table 4: Summary of HSG uterine findings
Characteristics Frequency %
Unicornuate 2 1.5
Bicornuate 1 0.8
Arcuate 2 1.5
Irregular uterine cavity 7 5.4
Fibroids 13 10
Normal 105 80.8
Total 130 100
Figure 3: HSG images showing bicornuate uterus.

18
Figure 4: HSG showing filling defect(A) in early image and deformed uterus (B) in late
image due to fibroid
6.2.4 HSG fallopian tubes findings
Unilateral tubal blockage either the right or left tube, was the most tubal abnormality observed
in 28 patients (21.5%), bilateral tubal blockage was noted in 25 patients (19.2%). Unilateral
hydrosalpinx (figure 5) was noted in 11 patients (8.5%) while bilateral hydrosalpinx was seen
in 6 patients (4.6%). Tubal adhesions were found in both sides in 11 patients (8.5%) and
unilaterally in 12 patients (9.2%). This is shown in table 5
Table 5: Summary of HSG fallopian tubes findings (N=130)
Characteristics Frequency %
Bilateral blockage 25 19.2
Unilateral blockage 28 21.5
Bilateral hydrosalpinx 6 14.6
Unilateral hydrosalpinx 11 8.5
Bilateral adhesion 11 8.5
Unilateral adhesion 12 9.2
N 130

19
Figure 5. HSG Showing left hydrosalpinx and irregularity in lower uterine cavity

20
Figure 6. Normal HSG shows filling of uterus and both fallopian tubes in (a) and peritoneal
spillage in (b)
a
b

21
7.0 DISCUSSION
This cross-sectional study analysed the findings in HSG as observed in infertile women
attended Radiology department at MNH in Dar-es-Salaam. A consecutive sampling method
was used due to limited data collection time, accessibility to target group and shortage of
resources. The study was also for partial fulfilment of masters of medicine in Radiology.
The sample in this study may not be a true representation of Dar-es-Salaam women
inhabitants with infertility as it included only those patients who attended MNH radiology
department with infertility. However the sample size was reasonable enough and the age
distribution of patients followed a normal distribution curve that gives a confidence in the
results obtained. Despite these limitations, the findings discussed below may be useful in
planning a more large scale study in the topic of infertility and HSG in general.
Infertility in women is the main indication to undergo hysterosalpingography examination.
About 40-45% of infertility is attributed by female factor including cervical factors,
endometrial-uterine factors, ovarian factors and peritoneal factors. Male factors attribute for
about 25-40% while both male and female factors account for 10% and the remaining 10% is
due to unexplained factors. Therefore infertility workup is incomplete without an initial
hysterosalpingography examination that will depict abnormality in uterus and fallopian tubes.
In this study more patients had secondary infertility than those with primary infertility which
is similar to other previous studies (2,3,6,7,8). However this differs from other studies where
it was found that primary infertility is commoner (9,10). This higher rate of patients with
secondary infertility compared to the primary infertility can be used as a crude indicator of the
possible effects of pelvic inflammatory infections in our setting (3,41).

22
The participants included in this study were of mean age of 29.89 years which was similar to
the mean age of infertile women in Uganda and Nigeria (2,3) and lower than those in Turkey
(9) and higher than those in Iran (10).
The mean duration of infertility was 4.26 years which is similar to other studies done in
Nigeria and Turkey (3,9). The mean duration of infertility is reported low in other previous
studies conducted in Nepal and India (14,37). Most of patients in this study had 1- 5 years of
infertility but majority of patients who had long duration of infertility, between 6-17 years,
showed significant maximum number of abnormalities (73%). This long duration could be
due to hesitancy of patients in seeking early advice fearing for marital disharmony. Another
reason that could contribute to this long duration of infertility may be due to unawareness of
the importance of early treatment among the infertile couple. The presence of enormous local
tradition healing practices as well as other alternative medicine practices could be an
important contributory factor for the delay in coming earlier to health facilities.
In the present study of 130 patients, 52 cases (40%) had normal HSG findings. 78 patients had
abnormal findings accounted for about 60% of total cases. The reason behind this could be
due to the fact that MNH being the tertiary level hospital receiving referrals from periphery
health facilities where initial evaluation of infertility causes has been done. Also most of these
patients have already seen and evaluated in MNH Gynaecology clinic for other causes of
infertility and found normal, hence more likely to have structural abnormalities.
Hysteroscopy is the best technique for the diagnosis of uterine endometrial pathology because
small submucosa myoma and polyps can be missed by hysterosalpingography. However no
case of abnormal HSG findings will have normal finding in hysteroscopy, meaning false
positive rate of HSG is close to zero. In comparison to hysteroscopy the accuracy rate of
HSG in diagnosing endometrial pathology ranges from 75% to 90% (4,34). Therefore in this

23
study there is possibility that few patients who had normal finding could have small
submucosa myoma and polyps which were not picked up by HSG.
Congenital abnormalities of the uterine shape are the result of abnormal fusion of Mullerian
ducts during the early weeks of gestation. The most common anomaly is the arcuate uterus
which has no impact on fertility. In this study it was demonstrated that arcuate, unicornuate
and bicornuate uteri were common congenital abnormalities of the uterus encountered 3.8%.
This is also quoted in previous studies (1,6,36,42). The common uterine pathology in this
study was the presence of fibroids (10%). Fibroids which project in the uterine cavity such as
those of submucosa will cause the actual filling defects which can be detected by the HSG.
Uterine cavity may be distorted in its shape when the uterus has a large myoma. So HSG is of
great value in evaluation of uterine cavity and fallopian tubes patency when planning for the
myomectomy.
Irregular uterine cavity which is a sign of infection was present in 5.4%. This may be due to
endometritis or synechiae following PID, post abortal or post partum infections (3,41). This
distortion of uterine cavity due to both congenital and acquired causes result in infertility due
to failure of embryo implantation or spontaneous abortion. Preterm labour, malposition of the
foetus and obstructed labour may be another sequel of the uterine cavity distortion.
Previous studies that compared HSG and laparoscopy showed that ,HSG has a high specificity
of 80% and low sensitivity of 65% for detecting tubal patency (6,9,15,21). Another study
showed that HSG is as accurate as laparoscopy in the diagnosis of tubal patency or blockage
(22). Therefore due to its high specificity, making HSG a useful test for ruling out tubal
obstruction. When patency is demonstrated in HSG, there is little chance that the tube to be
actually occluded.

24
Most patients in this study (41%) were found to have tubal blockage which is similar to what
was reported in Uganda, Nigeria and Pakistan (2,8,36). Other previous studies reported that
tubal blockage accounted for less than 41% (3,10,14,15), whilst in South Africa reported to be
higher accounting for more than 67.2% (6,7). The main reason for this high proportion of
patients with tubal blockage is more likely due to high prevalence of pelvic inflammatory
diseases among women in our environment (2,6). Majority of patients with secondary
infertility showed higher proportion of tubal blockage which is similar with some previous
studies (8,24). In a study done in Nepal revealed the same incidence of tubal blockage in both
primary and secondary infertility (47).
However in HSG a common pitfall is non opacification of fallopian tube due to spasm.
Though antispasmodic was not used routinely in this study, its use would not have reduced
the number of patients with tubal blockage significantly as very few patients show tubal
spasm. Another false negative result occurs when there is inadequate wedging of cervical
cannula allowing leakage of contrast material into the vagina, thus interfering with generation
of sufficient intracavitary pressure and leading to misdiagnosis of tubal blockage. During this
study senior radiologist was called upon whenever the procedure was difficult and suspicious
of tubal spasm. Contrast intravasation into uterine and ovarian veins can sometimes be
mistaken for tubal filling, therefore is important to remember the anatomical locations of
these vessels. In order to minimise the chance for contrast intravasation patients were
scheduled during menstrual proliferative phase between 7th to 12th day when the endometrium
is thin and not fragile.
In our study majority of patients with tubal blockage were of older age (31-45years) in both
types of infertility (53.3%). This same result was reported in the literature previously in
Nigeria and India (8,24). This could be due to the increased risk of acquiring pelvic infection
with age.
25
Hydrosalpinx which is not detected by pelvic examination can be diagnosed by HSG.
Hydrosalpinx is seen as a dilated convoluted tubular structure on HSG which gradually
increase in size due to distal tubal occlusion. It is a result of fallopian tubes inflammation
following infections like gonococcal, chlamydial or tuberculosis of the genital tract. The
fimbrial ends are eventually occluded due to adhesions leading to collection of the secretions
in the lumen with gradual distension of the fallopian tube.
In this study 17(13%) patients had hydrosalpinx either unilateral or bilateral which was
similar with that reported in previous study done in Uganda (2) and higher than those reported
in Iran and Kathmandu (10,14).
Peritubal adhesions occur secondary to previous surgery or inflammation similar to the cause
of tubal occlusion. Adhesions around the fallopian tube results in loculation of contrast
material that has spilled from the fallopian tubes. Patients with features of pelvic adhesions
accounted for 18% of all infertile patients in this study. A study conducted previously in
Uganda showed that the peritubular adhesion was high (28%) while that done in Pakistan was
low, 7% of all patients (2,36)
This high incidence of tubal related pathology may be due to the following reasons. The first
is PID which is reported to be the most common gynaecological disease affecting many
African women (2,6,43). The second reason is that, in this group may be non compliance to
PID treatment that may lead to sub acute or chronic PID with deleterious effects on the
fallopian tubes. This indicates that pelvic inflammatory disease (PID) is still common in our
set up and makes it a common cause of infertility.

26
In this study it was observed that equal proportion of participants in both primary and
secondary infertility had utero-fallopian tubes pathology in general. This is different from
previous studies which showed the secondary infertile patients to have higher proportion of
pathology than primary infertile patients (8,24). A larger sample size would have been
appropriate in this study in order to get similar results, because there is slightly higher
proportion of patients with abnormality in secondary compared to primary infertility (60.3%
vs 59.7%). And also most pathologies are also higher among secondary than primary
infertility when considering individual uterotubal abnormalities.

27
8.0 STUDY LIMITATION
Limitation in design of study was the greatest set back in this study. This was due to time
limitations that could not be avoided, hence a non random sampling method was used instead
of random sampling method. Also there was no special clinic for infertility at MNH rather
patients were seen in usual general gynaecology clinic made it difficult to define sampling
frame, hence a consecutive sampling method could not be avoided.
However consecutive sampling method results in more representative sample in comparison
to convenient sampling method.
9.0 CONCLUSION
Generally, high proportion of patients in this study showed presence of uterine and fallopian
tube pathology. Fallopian tubal blockage was the highest observed tubal structural
abnormality while fibroid was the highest uterine pathology. There was no significant
difference in the presence of pathology between patients with primary and secondary
infertility. Older age above 30 years was more associated with presence of structural
abnormality in both uterus and fallopian tubes.

28
10.0 RECOMMENDATIONS
More than half of patients investigated in this study had uterotubal abnormalities, thus making
HSG being effective method for initial work-up of infertile women. Equipment and
consumables associated with this investigation should be readily available.
Further studies are needed to investigate the etiologies of these abnormalities at the earliest ,
this could be a measure to bring down the occurrence of such conditions.
There is a need of more studies on HSG findings using much bigger sample sizes to be
conducted in Tanzania.
There is a need to raise public awareness on causes and risk habits leading to infertility.
A large combined study with gynaecologist to find causes of infertility among the remaining
40% infertile women with normal HSG findings is recommended.

29
11.0 REFERENCES
1) Brant WE, Helmes CA. Genital tract Radiographic imaging and MR .In: Fundamentals of
Diagnostic Radiology. 3rd Edition. Philadephia .Lippincott Williams& Wilkins,2007, pg
909-911
2) Malwadde EK ,Byanyima RK .Structural findings at hysterosalpingography in patients
with infertility at two private clinics in Kampala, Uganda; African Health Sciences
2004;4(3):178-181
3) Bello TO. Pattern of tubal pathology in infertile women on hysterosalpingography in
Ilorin, Nigeria. Annals of African Medicine Vol.3,No.2;2004:77-79
4) Shakya B .Hysterosalpingography Vs Hysteroscopy in the detection of the intrauterine
pathology in infertility. Journal of Nepal Health Res Counc, 2009,April;7(14):6-9
5) Larsen U . Primary and secondary infertility in Tanzania. Journal of Health and
Population in developing countries, July 2003(ISN 1095-8940)
6) Blumenthal NJ, Hertzanu Y ,Ferreira MMV, Mendelsohn DB, Godberger S.
Hysterosalpingography in the assessment of infertility in black patients. South African
Medical Journal,1984;65:854-856
7) Adebiyi GA, Ameh CA, Eka A. Hysterosalpingography tubal abnormalities and HIV
infection among black women with infertility in Subsaharan Africa. Gynecol Obstet
Invest 2008:66:119-122
8) Bello TO. Tubal abnormalities on hysterosalpingography in primary and secondary
infertility. West Afr J Med .2006 ,Apr-Jun:25(2):130-133

30
9) Gokhan G, Gamze Y, Oznur G, Isin K, Lale W, Birol D . Hysterosalpingography ,
laparascopy or both in the diagnosis of tubal disease in infertility. World Journal of
Laparascopic Surgery,May-August,2008:1(2):23-26
10) Mesbazri S, Pourissa M, Refahi S, Tabarraei Y, Dehgha MH. Hysterosalpingographic
abnormalities in infertile women. Research Journal of Biological Sciences, 4(4):430-432,
2009
11) Kasby CB. Hysterosalpingography ; an appraisal of current indications. British Journal of
Radiology, 53, 279-282, 1980.
12) Lash MM,Yaghamee A, Strohsinitter W, Lalwani S. Association between secondary
infertility and fallopian tube obstruction on hysterosalpingography. J Reprod Med ,2008
Sep:53(9):677-680
13) Crofton M .Gnaecological imaging. In :Sutton D, London. Elsevier Churchill
Livingstone.Textbook of Radiology and Imaging 7th Edition.Vol.2 pg.1084-1090 ,
14) Poonam. The role of hysterosalpingography in case of subfertility. Kathmandu
University Medical Journal ,vol.5,No.4, (20):456-60. 2007.
15) Rajah R, McHuggo JM, Obhrai M. The role of hysterosalpiongography in modern
gynaecological practice .The British Journal of Radiology,1992;65:849-851
16) Perquin PAM, Dorr PJ, de Craen AJM, Helmerhost FM . Routine use of
hysterosalpingography prior to laparascopy in the fertility work up: multicenter
randomized controlled trial. Human Reprod 2006;21:1227-31
17) Chapman S, Nakienly R. Reproductive system. In: A guide to Radiological procedures.
Saunders publishers. London. 4th Edition, 2001, pg. 175-178.

31
18) Salle B, Sergeant P, Gaucherand P, IGwimont I, de Saint Hillaire P, Rudigoz RC.
Transvaginal hysterosonographic evaluation. Human Reproduction 1996,Vol.11, 5:1004-
1007
19) Rasmussen F, Justesen P , DNielsen DT. Therapeutic value of hysterosalpingography
with lipiodol ultra fluid. Acta Radiologica,1987 vol.28, No.3, pg.319-322
20) Sakar MN, Gul T, Atay AE, Celik Y. Comparison of hysterosalpingography and
laparascopy in the evaluation of infertile women. Saudi Med J 2008 Sep:29(9):1315-1318
21) Swart P, Mol BW, Van der Veen F, van Beurden M, Redekup WK, Bossuvt PM. The
accuracy of hysterosalpingography in the diagnosis of tubal pathology: a meta analysis .
Fertil Steril .1995 Sep:64(3):486-491
22) Fayez JA, Mutie G, Schneider PJ. The diagnostic value of hysterosalpingography and
laparascopy in infertility investigation . Int J Fertil 1988 Mar-Apr:33(2):98-101
23) Kanal P, Sharma S. Study of primary infertility in females by diagnostic laparascopy.
Internet Journal Of Medical Update,vol.1 No.2, July-Dec,2006
24) Fayez JA, Mutie G, Schneider PJ. The diagnostic value of hysterosalpingography and
hysteroscopy in infertility investigation. AM Journal Of Obstetric and Gynecology
,1987,March; 156(3): 558-560
25) Boudhraa K, Jellouli MA, Kassaoui O, Ben AN, et al. Role of the hysteroscopy and
laparascopy in management of female infertility. Tunis Medical Journal,2009 Jan:
87(1):55-60
26) Ragni G, Diaferia D, Vegetti W, Colombo M, Arnold M, Crosignani PG. Effectiveness
of sonohysterography in infertile patients work-up:A comparison with transvaginal
ultrasonography and hysteroscopy. Gynecology Obstetric Investigation J. 2005: 59:184-
188

32
27) Kaspa T, Gal M, Hartman M, Hartman J, Hartman A. A prospective evaluation of
uterine abnormalities by saline infusion sonohysterography in 1,009 women with
infertility or abnormal uterine bleeding .Fertility and Sterility.Vol.86;6: 1731-1735
28) Case AM, Pierson RA. Clinical use of sonohysterography in the evaluation of infertility.
J Obstet Gynecol Can. 2003 Aug: 25(8): 641-648
29) Salehpour S, Taheripanah R, Soltan L .An assessment of sonohysterography as a
diagnostic tool for uterine cavity defect and tubal patency. Journal of Reproduction and
Infertility, 2000. Vol.1:1(1)
30) Alatas G, Aksoy E, Akarsu C, Yakin K, Akson S, Hayran M. Evaluation of intrauterine
abnormalities in infertile patients by sonohysterography. Human Reprod vol.12 ,1997;
3:487-490
31) Strandell A, Bourne T, Bergh C, Grandberg S, Asztey M, Thorburn J. The assessment of
endometrial pathology and tubal patency: a comparison between the use of
ultrasonography and x-ray hysterosalpingography for the investigation of infertility
patients. Ultrasound Obstet Gynecol. 1999 Sept:14(3):200-204
32) Oguntoyibnbo AE, Amok AOD, Komolafe OF. Sonographic assessment of fallopian tube
patency in the investigation of female infertility in Ilorin ,Nigeria. African Journal of
Reproduction Health,vol.5 No.1, August,2001 pg.100-105
33) Darwish AM, Youseff AA. Screening sonohysterography in infertility. Gynecol Obstet
Invest ,1999:48(1):43-47
34) Bonilla-Mosoles F, Simon C, Serra V, Sampaio M, Pellicer A. An assessment of
hysterosalpingosonography(HSSG) as a diagnostic tool for uterine cavity defects and
tubal patency. J Clin Ultrasound 1992,Mar-Apr:20(3):175-181

33
35) Malek KA, Hassan M, Soliman A, El-sawah H, Azab AO. A prospective comparative
study to assess the accuracy of MRI versus HSG in tubouterine causes of infertility.
Middle East Fertility Society Journal,vol.10,No.3,2005. 250-257
36) Naula U. Hysterosalpingography .Professional Med J, Dec 2005;12(4):386-391
37) Kumar S, Neelangi G. Assessment of uterine factor in infertile women :
Hysterosalpingography vs Hysteroscopy. MJAFI,2004,Vol.60 No.1: 39-41
38) Sharma S, Mittal S, Aggarwal P. Management of infertility in low resource countries. B
JOG,2009 Oct:116(1):77-83
39) Tvarijonavicene E, Nadisauskiane RJ. The value of hysterosalpingography in the
diagnosis of tubal pathology among infertile patients .
Medicina(Kaunas).2008:44(6):439-448
40) Mencaglia L, Colafranceschi M, Gordon AG, Lindemann H, et al . Is hysteroscopy of
value in the investigation of female infertility? Acta Eur Fertil 1988 Jul Aug:19(4):239-
241
41) Besley .WHO Report: The epidemiology of infertility .A review with particular reference
in Subsaharan Africa. Bull WHO 1976;54:319-345
42) Shrivastava VR ,Rijal B, Shrestha A, Shrestha HK,Tuladhar AS. Detection of tubal
abnormalities by hysterosalpingography in Nepalese sub fertile women .Nepal Med Coll
J 2009;11(1):42-45
43) Favot I, Ngalula J, Mgalla Z , Klokke AH, et al. HIV infection and sexual behaviour
among women with infertility in Tanzania: A Hospital-Based study. International Journal
of Epidemiology 1997;26:2:414-419.

34
APPENDEX:I. DATA COLLECTION SHEET Part I. Demographic data
AGE Last
Menstrual
Period(LMP)
Type of
infertility
Duration of infertility
Part II. Clinical data
1. What are HSG findings?
a) Normal
b) Abnormal
2. Uterine abnormalities noted in 1 b) above
a) Yes
b)No
3. If yes in 2 above, which type
a) Unicornuate uterus
b) Bicornuate uterus
c) Septate
d) Irregular uterine cavity
e) Filling defects/fibroids
4. Fallopian tubes abnormalities noted in 1b?
a) Yes
b) No
5. I f the answer is Yes in 4 above, which type?
a) Right unilateral blockage
b) Left unilateral blockage
c) Bilateral blockage

35
6. Are there extrauterine abnormalities noted?
a) Yes
b) No
7. If the answer is Yes in 6 above, which type?
a) Adhesion
b) Mass
c) Other ,mention…………………..

36
APPENDEX: II. Consent: English version Informed Consent Form
Greetings!
I am Dr .Ramadhan Bihindi Kabala, a postgraduate student at Muhimbili University of
Health and Allied Sciences (MUHAS), investigating on the structural abnormalities of
the uterus an fallopian tubes as the causes of infertility among the patients who attend the
Gynecology clinic at Muhimbili National Hospital(MNH) using
Hysterosalpingography(HSG) investigation.
The main objectives of this study is to assess the usefulness and ability of the HSG
investigation to detect the abnormalities that cause the failure to conceive the pregnancy
which will help the Gynaecologist in treatment plan of the patient.
I f you agree to participate in this study ,you will be asked some questions and being
investigated for the patency of your fallopian tubes and uterus using HSG by introducing
the contrast media through the vagina and then x-ray images will be taken for
interpretation.
The HSG results and all information collected will be entered in the computer without
your name, but just using the identification number. We expect no harm to happen to you
during the course of this study but you will experience some pain during the procedure
and bleeding spots after the procedure. The study participation is completely voluntary
and refusal to participate or withdrawal will not involve penalty or loss of any benefits to
which you are entitled. You will be treated as per usual Hospital protocol for all patients
with infertility.
It is our expectation that information that will be gained from this study will be of
benefit for many infertile couples and the community at large..
In case you will have any other questions regarding this study, please feel free to contact
the investigator, Dr. Ramadhan Bihindi Kabala ,P.o.Box 65001, MUHAS, Dar es slaam.
Mobile phone ; 0713 682 405
If you have any questions concerning your rights as a participant, you may contact Prof.
E.F. Lyamuya, Chairman of the college research and publication committee, P.O. Box

37
65001, Dar es Salaam. Telephone: 2150302/6. Do you agree to participate? (Tick the
response) ...........YES ……….NO.
I, ………………………………………………………………………..have read the
consent form and my questions have been answered and I agree to participate in this
study.
Signature of Participant…………………………………………………………..
Signature of Investigator………………………………………………………….
Date of signed consent…………………………………………………………….

38
APPENDEX: III. Consent: Swahili version FOMU YA RIDHAA YA KUSHIRIKI UTAFITI
Salaam!
Ruhusa ya Kushiriki Utafiti Kuhusu “ uwezo wa kipimo cha HSG kuonyesha
magonjwa yaletayo ugumba kwa wanawake katika chumba cha uzazi na mirija ya
kupitisha mbegu”
Mimi naitwa Dr. Ramadhan Bihindi Kabala, ni mwanafunzi wa udhamili chuo kikuu cha
tiba Muhimbili. Ninachunguza sababu zinazosababisha ugumba kwa kutumia kipimo
kinaitwa HSG kwa wagonjwa wenye matatizo ya kupata mimba wanaotibiwa katika
kliniki ya magonjwa ya wanawake ya hospitali ya taifa Muhimbili(MNH). Dhumuni la
utafiti huu ni kuonyesha uwezo wa kipimo cha HSG kuonyesha magonjwa mbalimbali
katika chumba cha uzazi na mirija ya kupitisha mbegu za uzazi ambayo yanasababisha
tatizo hili la ugumba na ili matokeo yake yaweze kutumika kumuongoza Mganga katika
matibabu ya mgonjwa mbeleni.
Kama unakubali kushiriki kwenye utafiti huu, utaulizwa maswali, utapimwa chumba cha
uzazi na mirija ya kupitisha mbegu za uzazi kwa kuingiza dawa ukeni na kasha kupiga
picha kwa kutumia mionzi ya inayoitwa x-rays. Majibu ya picha zako yataingizwa
kwenye kompyuta na nambari ya utambulisho; jina lako halitatumika kwenye maelezo ya
utafiti. Tunategemea kwamba hakuna madhara yoyote makubwa yatokanayo na utafiti
huu, zaidi ya kusikia maumivu kiasi wakati wa kufanya kipimo na matone kidogo ya
damu baada ya kumaliza kipimo. Kipimo hiki hakina athari yoyote kwa afya yako
Kushiriki kwenye utafiti huu ni kwa hiari na kutokubali kushiriki au ukijitoa
hautaadhibiwa au kupoteza haki yako ya matibabu. Utatibiwa na kuendelea kufuatiliwa
kama taratibu za hospitali zinavyoelekeza kwa mtu mwenye matatizo ya kupata uzazi.
Tunatumaini kwamba taarifa zitakazopatikana zitawanufaisha wengine pia. Kama una
maswali au maelezo kuhusu utafiti huu, uwe tayari kuwasiliana na mtafiti, Dr. Ramadhan
Bihindi Kabala, MUHAS, P.O. Box 65216, Dar es Salaam. 0713 682 405.

39
Kama una maswali kuhusu haki yako kama mshiriki wasiliana na Prof. E. Lyamuya,
Mwenyekiti wa kamati ya utafiti, P.O. Box 65001, DSM. Simu 2150302/6. Je,
umekubali kushiriki? ........NDIYO, .......HAPANA
Mimi………………………………………………………..nimesoma maelezo na
maswali yangu yamejibiwa na nimekubali kushiriki kwenye utafiti huu.
Sahihi ya Mshiriki………………………………………………………………


















