
ILMU BEDAH
125
Copyright2010@edi ahsani 06 Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
-
Upload
tammie-young -
Category
Documents
-
view
75 -
download
1
description
sip
Transcript of ILMU BEDAH

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
CLEFT PALATE Dr. Mgs. Roni Saleh, SpB-SpBP(K)
I. Normal Anatomy
A. Hard palate 1. Primary (anterior) hard palate: Formed by fusion of the
bilateral palatine processes of the maxilla. 2. Secondary (posterior) hard palate: Formed by fusion of the
bilateral horizontal plates of the palatine bone. 3. Incisive foramen: Separates the primary from the secondary
hard palate. 4. Premaxilla: The maxilla anterior to the incisive foramen,
including the anterior hard palate and alveolus. B. Soft palate (velum): contains the muscles involved in
velopharyngeal closure. 1. Levator veli palatini. 2. Tendon of the tensor veli palatini. 3. Palatopharyngeus. 4. Uvulate.
C. Vascular and nerve supply 1. Hard palate: The greater palatine artery and nerves, through
the greater platine foramen in the posterior lateral hard palate.
2. Soft palate: The lesser palatine artery and nerves. II. Cleft Anatomy
A. Clefts of the secondary palate 1. A variable degree of clefting can be seen.
a. Bifid uvula. b. Submucous cleft palate triad.
1) Bifid uvula. 2) Hard palate notching (palpable). 3) Zona pellucida: Midline white line, due to the
anomalous insertion of the palatal musculature. c. Cleft velum d. Cleft of the entire secondary palate
2. Anomalous inseretion of the tensor veli palatini. a. The normal bilateral tensor veli palatini muscles
interdigitate and insert transversely in the posterior part of the velum

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
b. With clefting, the tensor veli palatini muscles course anteriorly and insert onto the posterior edge of the hard palate.
c. In this position, their ability to lift the soft palate is significantly impaired
B. Clefts of the primary palate. 1. The lip, nostril sill, alveouls, and primary palate are all
considered derivatives of the primary palate. 2. Clefts of the primary palate can involve the lip alone, extend
into or through the alveolus and primary palate, or extend through the secondary palate.
C. Kernahan’s striped Y serves as a shorthand for recording cleft palate extent.
III. Facial Embryology
A. Five facial prominences (develop during week 4 of gestation) 1. Midline frontonasal prominence: Mesenchyme ventral the
forebrain, not a branchial arch. 2. Bilateral maxillary prominences: First branchial arch. 3. Bilateral mandibular prominences: First branchial arch.
B. Bilateral nasal placodes 1. Appear on the inferior frontonasal prominence, late in week
4. 2. The medial and lateral nasal prominences emerge on each
side of the nasal placodes. C. Fusion: week 5
1. The lateral nasal prominence fuses with the maxillary prominence, connecting the nose to the cheek.
2. The medial nasal prominence fuse. 3. The medial nasal prominence fuses with the maxillary
prominence, connecting the nose and lip. Failure of the fusion results in a cleft lip.
IV. Palatal embryology
A. Primary palate and premaxilla 1. The medial nasal proceses fuse to form the median palatine
process in week 5. 2. The median palatine process becomes the premaxilla.
B. Secondary palate: weeks 5 to 12 1. The bilateral lateral palatine processes develop from the
medial portion of the maxillary process. 2. The lateral palatine processes hang vertically, and then lift
horizontally as the tongue drops.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
3. Fusion stars at the incisive foramen and moves posteriorly, forming the secondary palate.
V. Epidemiology
A. Racial distribution 1. Isolated cleft palate
a. Incidence of about 0.5 per 1,000 births. b. Does not vary with race.
2. Cleft lip with or without cleft palate a. Asians: 2 per 1,000 births. b. Whites: 1 per 1,000 births c. Blacks: 0.4 per 1,000 births
B. Gender distribution 1. Isolated cleft palate is more common in females. 2. Cleft lip with cleft palate is more
C. Familial distribution 1. Cleft lip with or without cleft palate and isolated cleft palate
appear to be genetically different 2. Isolated cleft palate is more common in relatives of cleft
palate patients. 3. Cleft lip/palate is more common in relatives of cleft lip /
palate patients Table 24-1. Probability of subsequent children with isolated cleft palate or cleft lip with / without cleft palate Family members with Probability of subsequent Probability of subsequent Cleft Palate Child with cleft palate (%) Child with cleft lip +/- Cleft Palate (%) One affected child only 2 4 One affected parent only 2-4 2-4 One affected child and a Positive family history 7-0 7 ( with normal parents ) One affected parent and One affected child 15 14-17 VI. Etiology
A. Genetics 1. An isolated cleft palate is probabaly a single major gene
autosomal recessive trait with other minor genes contributing 2. Cleft lip/palate is probably polygenic with multiple major
and minor genes contributing

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
B. Environment 1. The exact role of anny environment factor is not clear 2. Alcohol has not been conclusively shown to cause isolated
cleft palate 3. Smoking : Data are not conclusive 4. Many teratogens ( including alcohol, isotretinoin and others )
are known to cause multiple congenital malformations, which may include cleft palate as part of a series of malformations
5. Folic acid and vitamn B6 intake during pregnancy may reduce cleft lp / palate
VII. Surgical goals
A. Closure of the cleft 1. Closure of the cleft palate separates the oral and nasal
cavities 2. This prevents aerophagia and reflux of oral contens into the
nasal cavity B. Speech and hearing
1. Cleft palate repair must be performed early in life to prevent irreparable speech defects
2. However,”early” palate surgery is associated with impaired facial growth
3. Because facial structures can be surgically repaired later in life, whereas speech patterns cannot, most surgeons feel that normal speech development is more important than normal facial growth and therefore favor early repair.
C. Otitis and Hearing 1. Otitis media
A. Secondary to eustachian tube dysfunction A. The levator veli palatini ( LVP) originates along
the eustachian tube B. An abnormal LVP insertion is thought to
decrease ‘ milking “ action and therefore lead to poor venting of the middle ear.
B. Occurs in almost all patients with cleft palate, and can lead to permanently impaired hearing
2. Hearling in cleft palte patients generally improves after myringotomy
3. The earliner the myringotomy is performed the greather the improvement is hearing. Normal hearing is usually achieved with early bilateral tympanostomy.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
4. it is not clear whether repair of cleft palate or repair of velopharyngeal inincompetence (VPI) reduce otitis media or improves hearing
D. Facial growth 1. Early palate surgery can adversely affect maxillary growth 2. Repair of the primary palate and alveolus has more
significant effects on maxillary growth than repair of the secondary palate alone
3. Facial growth is less affected if palatoplasty is delayed until 1 year of age.
4. For rhese reasons, some surgeons close the soft palate early ( around 3 months ) and the hard palate later ( ranging from 9 to 18 months )
5. Each case must be approached individually, carefully considering facial growth and speech devetlopment.
VIII. Surgical repair
A. Hard palate clefts 1. Von langenbeck repair
a. Bilateral, bipidicled mucoperiosteal flaps. b. Lateral relaxing incisions are made bilaterally c. The flaps are closed at the mdline, nasal mucosa first
and oral mucosa d. Many modifications exist e. This repair may result in a short palate and contribute
to VPI 2. V-Y pushback ( Veau-Wardill-Kilner)
a. Bilateral mucoperiosteal flaps, unipedicled posteriorly b. V-Y advancement posteriorly is performed c. Anterior exposed areas are left open to granulate and
mucosalize. d. Improves velopharyngeal closure by lengthening the
palate, may improved speech

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
B. Soft palate clefts 1. Straight-line repair : Separate nasal and oral mucosal flaps
are raised and approximated 2. Double Z-plasty ( Furlow )
a. Z-plasty flaps of oral and nasal mucosa ( with LVP muscle included) are used in opposing directions.
b. Z-plasties are performed in layers, with nasal mucosal flaps transposed and closed, followed by transposition and closure of oral mucosal flaps
c. Lengthents the soft palate d. Reorients the levator veli palatini muscles e. Can be used along with hard palate closure in one
operation, or as veloplasty to be followed later by hard palate closure ( see above )
C. Vomer flap 1. Flaps may be based inferiorly or superiorly and may be
unilateral or bilateral 2. Helps provide tissue for closure of wide clefts 3. Superiorly based flaps are used more commonly 4. Inferiorly based flaps are useful for wider clefts 5. May or may not impair maxillary growth ( controversial)
D. Alveolar repair 1. Mucoperiosteal flaps are raised and inset as advancement
flaps 2. Bone grafting is fermormed if necessary 3. Some perform grafting early ( primarilly), although most
prefer secondary bone grafting before the permanent cleft canine emerges, during the period of early mixed dentition, arround 8 yeasrs of age
4. For primary grafting a mucosal flap is raised in the vestibule of the lip anterior to the cleft, and a rib graft is commonly used
5. For secondary grafting, gingival mucoperiosteal flaps are raised on both sides of the cleft, with the incision at the gingival sulcus of the teeth, and cancellous bone from the ilium is used
IX. Complications
A. Fistulae 1. Occur in up to 50% of procedures depending on the
preoperative anatomy and the repair technique 2. More common in wide or bilateral clefts 3. Most occur in the hard palate, posterior to the alveolus

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
4. More common with a single-layer closure B. Midfacial growth problems
1. Multifactorial 2. Cleft palate patients have inherent facial growth impairment 3. Lip and alveolar repair significantly affect facial growth 4. The extent and timing of palate repair can affect facial
growth ( see above ) C. Airway obstruction
1. Maya occur secondary to postoperative bleeding 2. More common in operations that include pharyngeal flaps 3. Patients should be monitored closedly postoperatively
X. Velopharyngeal incompetence
A. Definition : Inappropriate incomplete closure of the velum against the posterior pharynx during speech
B. Etiology 1. In cleft palate patients, the levator veli palatini inserts
anteriorly on to the hard palate, and loses its ability to lift the soft palate to achieve velopharyngeal closure
2. Approximately 20% of patients acquire clinical VPI following palate repair
3. Some cleft palate operations greatly improve palate length and levator orientatin, whereas others do so a lesser extent.
a. The Von Langenbeck procedure tends to cause a short palate because no length is added in the procedure
b. The V-Y pushback techniiques improve palate length c. The Furlow double Z-plasty soft palate repair
lengthens the palate and corrects muscle insertion on the palate.
C. Speech and velopharyngeal insufficiency 1. Air escapes from the oropharynx up through the
nasopharynx 2. This results in hypernasal speech and escape of excess air
from the nose during speech ( nasal emission ) causing difficulty with consonants
3. The patient adjusts to these problems by developing alternative methods for creating certain vocal sounds ( pharyngeal fricatives and glottal stops).Plosives : /p/,/b/,/t/,/d/,/k/,/g/; fricatives : /f/,/v/,/th/,/s/,/z/,/sh/,/zh/.
D. Treatment of VPI 1. Pharyngeal flaps

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
a. Best for patients with adequate lateral pharyngeal wall movement ( good medial excursion ) based on nasal endoscopy or videofluoroscopy
b. A myomucosal flap from the posterior pharyngeal wall is elevated
c. The flap contains mucosa and pharyngeal constrictor muscle, exposing the prevertebral fascia
d. May be based superiorly or inferiorly e. The flaps is then sutured to the posterior soft palate f. This creates a tissue bridge betwwn the soft palate and
the posterior pharynx, alowing the lateral pharyngeal walls to close in and cause velopharyngeal closure
g. This is a statis repair ( the flap does not move to cause port closure ).
h. The diffuculty is in adjusting the port / opening size correctly ; too wide an opening leaves the patien hypernasal, whereas limiting air flow too much induces a state of hyponasality
2. Pharyngoplasty ( dynamic sphincter pharyngoplasty ) a. Best for patients with inadequate lateral phartngeal wall
medial excursion b. Superiorly based bilateral flaps that include the posterior
tonsillar pillars and the palatopharyngeus muscles are elevated and are set in overlapping positions into a horizontal incision in the posterior pharyngeal wall
c. This is a potentially dynamic repair. The sphincter created may have some mevement to help achieve port closure
3. Complications a. Airway obstruction in the acute postoperative period can be
life threatening and patients hould have apnea monintors b. Obstructive sleep apnea is not uncommon in the early
postoperative period c. Dehiscence, bleedingg and infection are other comlications d. Patients with velocardifacial syndrome the risk of carotid
injury during flap elevation. Consider preoperative angiogram and / or magnetic resonance angiogram. Palate intraoperatively for medialized carotid pulsations.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Cleft Lip Dr.Mgs. Roni Saleh,
I. Embryology
A. The critical developmental period of the lip and primary palate occurs during weeks 4 to 6 of gestation.
B. Failure of complete union of the medial nasal prominence and the maxillary prominence leads to a variable extent of clefting of the primary palate, invoiving the upper lip, alveolus, and anterior hard palate to the incisive foramen.
C. Cleft lip alone (CL) and cleft lip and palate (CLP) are considered to be the same entity along a morphologic continuum. Clef palate alone (CF), on the other hand, has different demographics.
II. Epidemiology and Genetics A. Incidence of cleft lip and of cleft lip and palate
1. The overall incidence is 1 in 1,000 live births 2. White ancestry: 1 in 750 live births 3. Asian ancestry: 1 in 500 live births. 4. African ancestry: 1 in 2,000 lilve births.
B. Demographics 1. Male-to-female ratio of 2:! 2. The ratio of left (L) to right ® to bilateral (B) clefts (L:R:B):
6:3:1 3. The ratio of CLPmto CL is 2:1 4. Three percent are syndromic. 1. Risk factors
a. Medications: Phenytoin, methylprednisolone (Solo-Medrol), steroids, phenobarbital, diazepam, and isotretinoin.
b. Smoking c. Parental age, especially father’s age, or both mother
and father over 30 years old. d. Family history (see “Genetics”)
C. Genetics
1. The risk of having a child with CLP a. If parents have one child with CLP: 4% b. If one parent has CLP: 2% to 4% c. If parents have two children with CLP:9% d. If one child and one parent have CLP: 14% to 17%.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
1. Most cases are sporadic(and multifactorial), but may be X-linked, autosomal dominant (Van der Woude’s syndrome) of familial (see “Syndromes Associatied with Cleft Lip and Palate,” later in this chapter).
III. Anatomy A. Normal lip anatomy
1. Topographic landmarks a. Nasal alae. b. Columella c. Philtral columns. d. White roll: Well-defined mucocutaneus or vermilion-
cutaneous border. e. Vermilion: Red portion of lip. f. Tuberle. g. Cupid’s bow h. Wet-dry border: The vermilion-mucosa junction is the
border between keratinized and nonkeratinized mucosa.
2. Musculature a. Orbicularis oris
A. Fibers cross (decussate) in the midline and create the opposite philtral columns.
B. Functions as a sphincters (deep fibers) and for speech (superficial fibers).
b. Levator labli superioris. A. Inserts into the dermis at the vermilion vorder
and the lower edge of the philtral columns. B. Elevates the upper lip.
c. Nasalis or depressor septi nasi muscle: The fibers run from the alveolar bone into the medial crural footplates, skin of the columelia and the tip of the nose, and into the opposite philtral columns.
3. Normal measurements. a. Vertical length (height) of the upper lip
A. Newborn: 10 mm. B. Age 3 months: 13 mm. C. Adult: 17 mm
b. The distance between the peaks of Cupid’s bow: Aprroximately 3 mm at 3 months
4. Arterial blood supply: The labial artery, bilaterally. 5. Sensory Innervation: the trigeminal nerve, cranial nerve
(CN) V, maxillary division (V2).

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
6. Motor Innervation: the facial nerve, CN VII, zygomatic and buccal branches.
B. Cleft lip anatomy 1. Alterations in the orbicularis oris, levator labii, and nasalis
result in disruption of continuity, orientation, and quality of the muscless.
a. Fibers are disoriented and run parallel to the cleft margin.
b. Fibers insert into the alar base on the cleft (lateral) segment and into the columella in the non cleft (medial)segment, as well as intradermally.
c. Incomplete clefts. A. Simonart’s band consist of a skin bridge across
the nasal sill. It does not usually contain any significant muscle mass.
B. Some fibers may cross the cleft, if the cleft is less than two-thirds of lip height.
d. Bilateral complete clefts: No muscle tissue is present in the pro-labium.
2. Vertical lip length is decreased: Cupid’s bow and the lip are rotated cephalad on both the lateral, cleft side as well as the medial side.
3. Disrupted Cupid’s bow. 4. The alveolus and nostril floor are open in a complete cleft
lip. 5. The premaxilla is rotated and protruding, especially in
bilateral cleft lip, often with collapase of the lateral segment of the cleft side(s).
6. Associated cleft lip nasal abnormalities a. Hypoplastic, flattened alar dome on the affected side. b. Lack of upper lateral cartilage overlap of lower lateral
cartilage. c. Subluxed lower lateral cartilage with alar base
displaced cephalad and posteriorly. d. Hypoplastic bony foundation (maxilla). e. The caudal septum is pulled toward the noncleft side. f. Flattening of the nasal bones. g. Shortened columella, especially in bilateral cases.
IV. Classification A. Extent of the cleft: Complete versus incomplete
1. Complete cleft lip a. Complete disruption of the soft tissues
to the nasar floor.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
b. Tends to be wider than incomplete celfts, with greater nasal deformities.
2. Incomplete cleft lilp a. Disruption of the soft tissues to varying degrees. b. The alveolus is usually intact, with less of a tendency
for the premaxilla to protrude. c. Forme fruste: A very mild cleft.
1) May be difficult to detect 2) May appear as vermilion notching or a scarlike
line or depression B. Location of the cleft: Unilateral versus bilateral
1. Unilateral cleft lip 2. Bilateral cleft lip
a. May have complete or incomplete cleft on both sides,or a combination b. More likely to be complete clefts and are often wide c. The premaxillary segment may include tooth buds. d. In bilateral complete clefts, the prolabium lacks
muscle tissue, and therefore lacks philtral columns. C. Alveolar segments
2. Narrow versus wide cleft 3. Collapse versus no collapse
Syndromes associated with cleft lip and palate
A. Van der Woude’s syndrome 1. Autosomal dominant, with variable penetrance. 2. Associated with CLP or CP (40%-50% penetrance). 3. Associated with lip pits (accessory salivary glands, 70%-
80% penetrance). 4. May also have absent second molar, syndactyly, abnormal
genitalia, and popliteal pterygia. B. Waardenburg’s syndrome
1. A group of anomalies arising from abnormal development and migration of neural crest cells.
2. Features may include cleft lip, cleft plate. C. Down syndrome (trysomy 21) D. Trisome 13 E. Stickler’s syndrome
1. A group of anomalies caused by connective tissue dysplasia. 2. Typical features: Cleft palate, progressive joint degeneration,
and various ocular abnormalities that may lead to blindness. 3. Autosomal dominant inheritance.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
4. Other anomalies: Cardiac, sensorineural, and learning disorders or mental retardation.
F. Pierre Robin sequence (Note: A sequence is a group of anomalies that result from a single disrupted event)
1. Micrognathia or retrognathia prevents normal descent of the tongue. The tongue then interferes with fusionof the palatal shelves. As a result, typical features include micrognathia or retrognathia, glossoptosis (tongue falls back into the pharynx, causing airway obstruction), and a U-shaped cleft palate.
2. May be a part of multiple different syndromes or may be an isolated finding.
3. Treatment. A. Prone positioning to help move the tongue out of the
aierway, the most conservative approach. B. Supplemental oxygen. C. Tongue-lip adhesion. D. Mandibular distraction osteogeneisi E. Intubation/tracheostomy
4. Patients may show catch-up mandibular growth, depending on their syndromic association.
5. Palysomnogram: Necessary to evaluate for desaturations as well as apneic events
G. Velocardiofacial syndrome 1. Autosomal dominant inheritance: Fluorescent in situ
hybridization (FISH) may show an abnormality in chromosome 22.
2. Characteristic feature include the following. A. Cleft palate. B. Congenital heart disease. C. Broad nasal dorsum and elongated face. D. Narrow, down-slanting palpebral fissures. E. Velopharyngeal insufficiency is common, even with a
submucous cleft palate. F. The carotid arteries may be displaced medially,
placing them at high risk of injury during pharyngeal flap surgery or dynamic sphincter pharyngoplasty. Always palpate the posterior pharynx prior to making an incision; consider obtaining a preoperative angiogram.
H. Median cleft lip 1. Rare

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
2. A different entity from the typical cleft lip; more accureately considered a median craniofacial cleft (Tessier type zero).
3. Associated with a group of syndromes (median cerebral facial dysgenesis) that involve more severe deformities of midline CNS and facial structures.
4. Further workup is needed, including a formal CNS evaluation.
5. May be associated with holoprosencephaly, pituitary problems, and a limited lifespan.
VI. Staging of intervention
A. Initial evaluation 1. Reassure the parents and family that they are not to blame. 2. Explain the stages and operations that should be expected
throughout the child’s lifetime 3. Evaluate for associated anomalies. 4. Consultations
a. Genetics, for evaluation and possible counseling b. Social works c. Feeding/nutrition
1) The child may need special nipples or bottles (e.g., cross-cut nipple)
2) Monitor for appropriate weight gain d. Otolaryngology: Children with cleft lip and palate
have a high incidence of eustachian tube dysfunction, and therefore otitis media, requiring close follow-up.
1) The child may need myringotomy tubes. 2) If unreated, repeat otitis may affect hearing and
speech development. B. Wide clefts (> 1 cm)
1. Goal : Bring the segments closer together to facilitate a tension-free repair.
a. Has not been shown to chanbe skeletal development in the anteroposterior direction.
b. Does not seem to prevent future crossbite. 2. Passive: Preoperative taping
a. Steri-Strip tapes applied across both segments of the lip.
b. Requires reliable parents who can reapply the tape and keep it on at all times
3. Passive: Lip adhesion operation a. Suturing the edges of the cleft together is performed
under anesthesia.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
b. The definitive lip repair is performed once the segments have moved closer together.
c. Variable success. 4. Active: Latham-type device
a. An orthodontic appliance that must be placed onto the palatal segments under anesthesia.
b. Parents turn a screw daily, which slowly brings the palatal segments into better alignment.
c. Removed at the time of definitive lip repair. 2. Repair
1. Timing (controversia) a. Repair at 3 months is generally accepted. b. Some argue for earlier repair in order to produce better
scars. 2. Rule of tens: For increased anesthetic safety, an infant
should a. Be 10 weeks old b. Weigh 10 pounds. c. Have a hemoglobin level of at least 10 mg/dL.
3. Cleft palate repair and secondary alveolar frafting 4. May also choose to address the cleft, nasal deformity at time
of lip repair. VII. Intraoperative considerations
A. Landmarks 1. Tattooed with methylene blue, using a hypodermic needle or
a quill pen. a. Alar bases. b. Columella. c. Philtral columns. d. D. Peak of Cupid’s bow midline on the medial
segment. Measure the anticipated distance for the new Cupid’s bow (approximately 3-4 mm).
e. Peak of Cupid’s bow on the lateral segment. 2. Account for distortion from the uncountered pull of the
orbicularis on the medial segment. The philtral columns are usually slightly C-shaped.
B. Mark lines for expected repair type. C. Only after marks are completed, infiltrate tissue with local
anesthetic to avoid distortion of anatomy and measurements. D. Goals of repair
1. Reconstitute Cupid’s bow 2. Minimize scarring

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
3. Produce a slight pout of the tubercle. 4. Produce functional continuity of the muscles 5. Recreate symmetry.
VIII. Types or repair
A. Straight-line repair 1. Historically, the first cleft lip repairs relied on freshening the
edges of the cleft and suturing them together. These have been largely replace by various Z-plasty-base techniques.
2. Rose-Thompson repair a. Modified straight-line repair that can be used for
minor clefts with lip length nearly equal on both sides of cleft (e.g. forme fruste)
b. Fusiform excision with straight-line closure. B. Quadrangular flap
1. Proposed by LeMesurier and Hagedorn. 2. Cupid’s bow is derived from the lateral lip. 3. 90-degree Z-plasty. 4. Violates Cupid’s bow and the philtral dimple. 5. May also have problem with a long lip.
C. Triangular flap 1. Proposed by Tennison and Randall
a. The Z-plasty is place at the vermilion border. b. Produces an natural appearing Cupid’s bow c. May be used for clefts of all widths. d. Violates Cupid’s bow and the philtral dimple. e. Has a tendency to produce a long lip.
2. Skoog repair a. Consists of two Z-plasties b. Violates Cupid’s bow and the philtral dimple.
D. Rotation advancement 1. Popularized by Millard
a. Likely the most commonly used repair. Often described as the “cut-as-you-go” technique.
b. The medial lip is rotated downward to fill the cleft defet.
c. A small pennant-shaped C-flap can either be rotated to create the nasal sill or used to lengthen the columella.
d. Does not violate Cupid’s bow or the philtral dimple____
e. Difficult for wider clefts. f. Common fitfall is inadequate flaprotation leading to
nothing and in-adequate vertical lip length.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
1) Repeat advancement or a small Z-plasty at the vermilion border can be performed.
2) Better results are obtained if adequate rotation is permormed at the time of the original operation.
2. Poople repair b. Preserves the integrity
of the aesthetic unit at the columellar-labial junction.
c. Allows lengthening of the lip woithout extending the advancement flap up on the ala or encroaching on horizontal lip length.
c. Bilateral cleft lip repair 1. The premaxillary segment is often a greater problem than in
a unilateral cleft lip. 2. Consider taping, lip adhesion, or presurgical orthodontics 3. Most common techniques
b. Dissect the prolabium to maintain a central skin flap to resemble the philtrum.
c. Deepithelialize the remainder of the prolabium d. Use the prolabial vermilion to create a labial sulcus,
not for the final lip the lateral lip segments, not from the prolabium.
e. Columellar lengthening may be performed at the time of lip repair or as a secondary procedure.
IX. Postoperative care A. Orders
1. Arm restraints (“no-no’s”) for 3 weeks to prevent disruption of repair.
2. Specialized nipple/bottle to decrease sucking effort when bottle-feeding.
B. Leave Steri-Strips in place over the incision for reinforcement. C. Follow up in 1 week for suture removal if nonabsorbable skin
sutures were used. Pearls Preoperative
1. Practice lip markings and cuts on foam first 2. Do not forget to assess for an adequate bony platform and the need
for orthogmatic surgery when assessing cleft nasal deformities.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Intraoperative 1. Mark several times, cut once. 2. Beaver scalpel blades are helpful. 3. Line up the white roll first, placing a stitch above and below the
white roll, then reapproximate the wet dry border. 4. Bilateral cleft: Do not use the “vermilion” of the premaxillary
segment in the final vermilion. It tends to look like an abnormal, dry patch postoperatively.
Postoperative 1. Instruct the parents to hold off feeding prior to the clinic
appointment. In the clinic, the baby will stay quet during feeding usually just long enough for suture removal.
2. Keep a Steri-Srip tape in place for 1 to 2 weeks for support.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
GRAFT & FLAP Dr. Mgs. Roni Saleh, SpBP
Departemen Bedah RSMH Palembang
GRAFT & FLAP Kulit melindungi tubuh dari invasi luar dan mencegah kehilangan
cairan, elektrolit, protein dll. Kehilangan kulit harus diganti baik dengan epitelisasi spontan atau graft maupun flap
I. Skin Graft Satu segmen kulit yang diambil secara komplit dari suatu daerah (donor site) dan ditransplantasikan ke daerah lain (recipient site) Klasifikasi 1. Berdasarkan species
a. Autograft : graft dari satu tempat ke tempat lain pada individu yang sama b. Allograft (homograft) graft dari satu individu ke individu lain yang satu species c. Xenograft (heterograft) graft dari satu individu ke lain species
2. Berdasarkan ketebalan a. Split Thickness
1. Seluruh epidermis dan sebagian dermis 2. Sebagian dermal skin appendiges (glandula sebacea, glandula
sudorifera,follicle rambut) masih ada didonor site dan akan sembuh dg epitelisasi
3. Ketebalan a. makin tipis kemungkinan “take” lebih besar b. makin tipis graft makin besar akan terjadinya engkerutan 4. Pemakaian a. Penutupan suatu daerah yang kehilangan kulit yang luas b. Penutupan jaringan granulasi
5. Metode a. Free hand (dengan pisau khusus atau dengan pisau lain) b. Dermatome (drum atau dengan power driven “hair clipper” type machine) 6. Donor Site a. Sembuh dengan epitelisasi tepi luka dan skin appendige b. Diperlukan perawatan untuk mencegah infeksi

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
b. Full Thickness 1. Seluruh ketebalan epidermis &
dermis 2. Sebagai penutup luka yang lokal
tetapi tidak semudah STSG “take”nya karena vascularisasi yang lambat
3. Daerah donor harus ditutup primer atau STSG
4. Pemakaian a. untuk wajah color match b. jari – jari tdk terjadi kontraktur c. dimana saja diharapkan kontraksi dari graft minimal B. Seleksi Donor Site
1. Ditentukan berapa banyak kulit diperlukan
2. Diambil dari daerah yang tersembunyi mis. lateral utk STSG atau lipat paha untuk FTSG
3. Color match penting terutama untuk
graft di wajah. Donor site : Supra clavicular Palpebra superior
C. Graft Survival
1. Graft mendapat inhibisi dari cairan pada bed 2. Dalam minggu berikutnya pembuluh darah pada bed tumbuh ke
dalam graft terjadi neovaskularisasi 3. STSG dan FTSG harus di daerah yang perdarahannya baik dengan
jumlah bakteri sedikit untuk menjamin “take” 4. Graft harus diimobilisasi cegah pergeseran graft dengan bed,
hematom mengganggu neovaskularisasi 5. Kontra Indikasi
- daerah yang miskin vaskularisasi seperti : - tendo yaitu telanjang

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
- cortex tulang tanpa periostium - daerah yang mendapat radiasi yang masif - luka yang terinfeksi, dll II. Skin Flap
Kulit & jaringan subkutan,kadang-kadang dapat dengan otot dan tulang yang ditransfer dari satu tempat ke tempat lain dengan mempertahankan vascularisasinya. “Pedicle” adalah dimana pembuluh darah dipertahankan. A. Klasifikasi 1. Dg Vascular Pedicle a. Flap dg pedicle yg intact 1. Cutaneous (random flap) Perdarahan dari pleksus dermal dan subdermal 2. Arterial (axial flap) Perdarahan dari direct cutaneous arteri 2.1. Peninsular kulit danpembuluh darah intact 2.2. Island hanya pembuluh darah intact 2.3. Musculocutaneus flap a. Kulit, subcutan dan otot otot sekitarnya b. perdarahan kulit dari pembuluh darah yang menembus otot dibawahnya dan berasal dari arteri segmentalis, pembuluh darah longitudinal dari dalam otot c. dapat peninsular atau island
b. Free Flap Suatu arterial flap dimana pembuluh darahnya dipotong, kemudian flap dipindahkan ke lokasi lain dan pembuluh darah direanastomosis dengan tehnik micro surgery dengan pembuluh darah dari recipient site

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
B. Penggunaan 1. Menggantikan jaringan yang hilang akibat trauma atau
akibat operasi 2. Dapat sebagai penutup kulit segera setelah operasi 3. Sebagai bantalan jaringan diatas tulang yang menonjol 4. Memberikan pendarahan yang baik pada bed yang
pendarahannya buruk 5. Meningkatkan sensasi pada suatu area (nerve pada flap skin
intact) 6. Dapat memakai jaringan lain seperti tulang untuk
rekonstruksi
III. Graft Lain
A. Tendon 1. Dipakai pada penggantian tendo yang hilang 2. Donor site : palmaris dan plantaris
B. Tulang 1. Dipakai pada defek yang rigid seperti tulang wajah, tengkorak, tulang panjang 2. Donor site : os iliaca, costa
C. Kartilago 1. Untuk pembentukan daun telinga, hidung, dagu 2. Donor site : kartilago costa, telinga, septum nasi
D. Fascia 1. Dipakai pada dermal defek dan sling pd paralise n.fasialis 2. Donor site : fascia lata, fascia temporalis
E. Dermis 1. Untuk restorasi contour spt parut yang cekung 2. Jaringan fat dg dermis dipakai sebagai pengisi 3. Donor site : dimana kulit yang tebal: bokong
F. Otot Biasanya free graft dari otot-otot juga mempertahankan perdarahan, graft gracillis atau gastrocnemous muscle graft
G. Syaraf Dipakai bila ada nerve gap, terutama pada 1. N. medianus, n. ulnaris, digital & facial nerve 2. Donor site : n. suralis & n. cutaneus humeri & ante brachi
H. Pembuluh darah 1. Bila ada, vascular gap 2. Banyak dipakai pada replantasi pada free graft transfer 3. Donor site : vena lengan atas & vena saphena

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
HYPOSPADIAS Dr. Mgs. Roni Saleh, SpB-SpBP(K) Bagian Bedah FK. UNSRI/ RSMH
Palembang I. Biology and development
A. The urethra normally coalesces at the raphe in the midline, from proximal to distal ( from perineum to glans ). Hypospadias result form failure of the urethral folds to fuse completely. This leaves themeatus located along the ventral aspect of thepenis.
B. Testosterone influences the development of the genitals by induction of virilization of indifferent external genetalia.
C. Potential causes of hypospadias. 1. Abnormal androgen production 2. Varying degrees of androgen receptor sensitivity in partinent
tissues (e.g.,the genital tubercle ) 3. Environment estrogens ( controversial )
II. Characterization A. Incidence ; 1 in 300 live births B. Common triad : Hypospadias, chordee, and a dorsal hood.
1.Chordee a. Ventral curvature of the penis b. Historically was thought to be due to a band of fibrous tissue along the course of the urethral plate, the dorsal half of the hypoplastic urethra. c. The true etiology is currently unclear d. The artificial erection test ( see “ Pertinent Principles in Hypospadias Repairs”) is useful to gauge the severity of the curvature and to measure the adequacy of correction.
2. Dorsal hood : in the presence of hypospadias, the dorsal foreskin is termed the dorsal hood, and is often quite noticeable due to the relative absence of ventral tissue.
C. Associated congenital anomalies 1. Other urinary tract anomalies are not typically associated
with isolated hypospadias. Therefore, reserve urinary tract imaging for those patients with other congenital anomalies ( e.g. imperforate anus )
2. Enlarged prostatic utricle ( Mullerian remnant ) : Present in 10% to 15% of hypospadias patients ; can lead to difficult urethral catheterization.
3. Cryptorchidism : Present in 9%; may be associated with intersex ( ambiguous genitalia ).

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
4. Intersex conditions ; More likely to be associated with proximal (e.g.’ perineal ) hypospadias or cryptorchidism.
a. Reserve intensive evaluation (e.g.,karyotyping ) for such patients
b. Mixed gonadal dysgenesis is the most common intersex variant in thin population.
D. Location of meatus 1. Determines the type of repair to some degree ; may be
related to degree and timing of the androgen insult 2. Incidence according to the location after the correction of
chordee a. Anterior hypospadias ( 50% ) : Granular, coronal and subcoronal b. Middle hypospadias ( 30 % ) : Distal penile, midshaft, and proximal Penile c. Posterior hypospadias ( 20 % ) : Penoscrotal. Scorotal and perineal III. Surgical repair A. Best performed between 6 and 18 months of age.
1. Minimizes anesthetic risk ( after 3 months of age ) 2. Limits psychological impact of surgery 3. Avoids feeling of being “ different “ (e.g. sitting to urinate ) 4. Limits the potential impact on toilet training
B. Goals of repair 1. Create a functionnally straight phallus : Verified by the
artificial erection test 2. Establish a functional urethra : Allows for a directed stream
and mixturation while standing ; can be objectively followed by uroflowmetry.
3. Pri\ovide a normal apperance : critical goal. One-third of adult patients are dissatisfield with their cosmetic result due to scarring, redudant skin ( from preserving skin for possible secondary procedures ) and reduced penile lenght ( a consequence of dorsal plication )
C. Pertinent principles in hypospadias repair 1. Optical magnification ( 2,5 x to 3,5 x operating loupes ) 2. Subcutaneous injection of epinephrine along planned
incision lines facilitates hemostasis. 3. Correct the chordee first. Use the artificial erection test :
Insert a smallgauge butterfly needle into the corpora through the glans ( to avoid penetrating Buck”s fascia ) and inject saline while having a tourniquet ( e.g.,a. Rubber drain) around the base of the penis to prevent outflow

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
D. Types of repair 1. Chordee correction
a. Excision of the urethral plate b. Dorsal plication of the corpora
1. Plication stiches are placed laterally to avoid the neurovascular bundles in the dorsal midline
2. It is unclear if early repair predisposes to recurrence during puberty, the period of ciorporal growth.
3. Potential exists for penile shortening c. Elevation of the urethral plate d. Recurrence rates are variable ( up to 40 % )
2. Meatal advancement and glansplasty ( MAGPI ) a. Initially described in 1981 b. Indicated for glanular and coronal variants only; result
are largely dependent on patient selection c. Meatal regression, the most troublesome
complication, may be minimized by careful approximation of the glans ventrally
d. Urinary diversion with a ctheter is not necessary e. Complication rate : 1 %
3. Parameatal – based flap ( e.g., Mathieu ) a. For slightly more proximal variants b. Flap cannot contain hair – bearing skin c. Complications : 6 %
4. Onlay island flap a. Flap from the inner preputial skin of the dorsal hood b. Useful for midshaft variants c. Onlay on to the urethral plate ; must tailor to the
appropriate size to prevent formation of a urethral diverticulum
d. Complications : 6% 5. Tubularized flap ( e.g., transverse preputial island flap )
a. Same flap as an only island flap, except completely tubularized
b. Intended for longer gaps; can use event if the urethral plate has been excised
c. There is potential for stricture formation at the proximal anastomosis
d. Complications : 10% to 15% 6. Tubularized incised plate ( e.g.,Snodgrass repair )
a. Useful for most variants

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
b. Has essentially supplanted other techniques as the procedure of choice for “middle” hypospadias variants and possibly others
c. Direct incision and subsequent tubularization of the urethral plate.
7. Grafts ( e.g.,buccal mucosa, bladdermucosa ) can be performed as onlay or tubular grafts E. Staged repairs
1. Generally reserved for more proximal ( osterior ) variants or very small phallused ( to allow for growth )
2. Second stage is usually performed 6 to 12 months after the initial procedur
IV. Outcomes
A. The more proximal the meatus, the more likely are complications B. Potential complications of hypospadias reconstruction
1. Urethrocutaneous fistula : Occurs in 5 % to 10 % of one – stage repairs. Excision and closure of the fistula can be performed at 6 months, provided nodistal obstruction is present
2. Other complications include meatal stenosis ( which may lead to urethrocutaneous fistula ), urethral stricture, inadvertent tranfes of hair – bearing skin, recurrent chordee, and urethral diverticula.
Pearls 1. Correct the chordee first. Once the penis is adequately straight, the
best technique for hypospadias repair can be detrmined 2. Do not rush to fix fistula. Wait at least 6 months and make surethat
there is no distal urethral obstruction 3. Proximal/posterior hypospadias and any variant associated with
undescended testes warrant an interesex evaluation. 4. Never use skin that will eventually be hair-bearing 5. Most successful repairs have multilayer flap coverage.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Anatomi Traktus Genito Urinarius Dr. Arizal Agoes, Sp.B, Sp.U
Ginjal
Pembuluh darah ginjal
Pembuluh vena ginjal

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Pembuluh limfe ginjal
Nephron

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Calyx dan pelvis renalis
Ureter
Ureter, pembuluh darah, saraf dan lymphatik

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Kandung kemih
Kandung kemih, pembuluh darah, saraf dan lymphatik
Urethra pada pria

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Prostat
Vesicula seminalis

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Penis
Penis, pembuluh darah, saraf dan lymphatik

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Scrotum dan testis
Epididimis dan Vas deferen
Urethra pada wanita

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Pemeriksaan ginjal
Pemeriksaan kandung kemih
Pemeriksaan Rectal Toucher

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
UROLOGI Dr. Arizal Agoes, SpB, SpU
Dept. Bedah RSMH Palembang WHAT IS UROLOGY The science of diseases of the urogenital organs, except for the female genital tract PENYAKIT ORGAN UROGENITAL?
Menguasai anatomi & fisiologi T.U.G Memahami patofisiologi dari problem urologi
PROBLEM2 UROLOGI, APA SAJA ?
I. Problem gangguan kontrol B.A.K II. Problem gangguan “volding” (pancaran)
III. Benjolan atau nyeri pinggang atau perut IV. Pembengkakan scrotum V. Urethral Discharge
VI. Disfungsi seksual/impotensi VII. Intertility I. GANGGUAN KONTROL
1. Kencing normal tapi pakaian dalam kadang-kadang basah * Urgensi - sistitis - hipertrofi otot detrussor - neurogenic bladdar (UMN) - anxious woman * Stress Incontinence Peningkatan tek Intra abd & intra vesical yang mendadak seperti batuk, bersin, naik tangga. Urin dalam jumlah kecil akan keluar Penyebab : Kelemahan Sphincter ext Prolaps Genitalia * Overflow Incontinence Buli tidak pernah kosong = Residual urine ?? Akibat frekwensi dan voiding volume sedikit Patologi : Dekompensasi otot detrussor (BPH lanjut) Flaccio Bladder/Neurogenic Bladder Tipe L.M.N

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
* Enuresis = Bed wetting = ngompol Normal usia < 4 th > 5 th 50-80% (-) 2. Bak normal tapi pakaian dalam selalu basah - Wanita dengan ectopic ureter - Kerusakan sphincter operasi prostatectomy - Uretero vaginal fistula cedera ureter saat operasi histerektomi 3. Bak sedikit/tidak sama sekali Pakaian dalam selalu basah = True Incontinence Patologi kerusakan total sphincter mis : tur prostat malignancy (wanita) radioterapi (wanita) * Fistula vesicavaginal Partus kasep Operasi vagina Radiasi II. Problem Voiding Urine
1. Nyeri saat kencing = dysuria nyeri dapat dirasakan buli2, urethra atau perineum nyeri timbul sebelum, saat atau sesudah kencing 2. Pancaran Abnormal - lemah = weak stream (Q max > 20 cc/dt Q ave 8 -10 cc/dt) - menetes - hesitansi - intermittent - tidak lampias - bercabang / kecil 3. Frequency - interval/jarak antara kencing makin pendek - voiding volume = sedikit - Dibedakan dengan polyuria kencing sering & voiding volume banyak Penyakit : DM, DI, Peny. Ginjal chronis, atau banyak minum/cuaca dingin - day time frequency nervous origin Psikogenik

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
- night time frequency nocturnal frekwensi * obat diuretika * peny. Jantung Kongestif Frequency
Sehari-hari sering dijumpai Keadaan patologi buli-buli
Inflamasi Tumor buli B a t u Prostat hipertrofi (BPH) Iritasi mukosa (pH sangat asam/alkali)
Kapasitas buli kecil (normal 300-450 ml) mis.
TBC buli, radiasi buli Partial sistektomi Sistitis Intersitialis
Patologi diluar buli Tumor Gynecologis Fibrosis Peri Vesical Gravid (normal)
4. Hematuria (microscopic atau gross) Terdapat darah (erithrosit) dalam urine dd/ urin berwarna merah
Anthocyanin (bats) Phenolpthaline (obat pencahar) Urate Porphyria Seratia marcestens (infeksi pada bayi)
Hematuria disertai nyeri = pain hematuria Colic renal Colic ureter batu Sakit daerah supra pubic
Tumor buli Inflamasi T r a u m a
Hematuria tanpa nyeri = painless hematuria Initial : asal urethra Durante/selama kencing : asal ginjal sampai buli Terminal – bladder tumor

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
III. BENJOLAN PADA PINGGANG/ABDOMEN DISERTAI NYERI Disertai nyeri
Hydronefrosis/pyonefrosis Retro peritonial hematoma Tumor ginjal (malignancy)
Tanpa nyeri Hydronefrosis Tumor ginjal jinak
Nyeri pinggang/abdomen (antero lateral) Nyeri renal Lokasi = CVA ipsilateral Akibat regangan kapsul ginjal mis = - destruksi pyelum/ureter - inflamasi parenchym ginjal Refered pain ke anterior, ABD atas dan umbilicus Nyeri inflamasi menetap Nyeri obstruksi intensitas berfluktuasi kdg2 disertai symtoms git Dd/ = asal intra peritonial
Pancreatitis Perforasi ulcus duodenum
= neurogen nyeri radiculer T10-12 (iritasi N. intercostalis) Nyeri ureter = ureter colic Sifat nyeri
Akut, kolik Spasme dan interperistaltic otot ureter Ada fluktuasi / bergelombang
Penyebab Sumbatan ureter - b a t u - bekuan darah Obstruksi atas = nyeri regio cva Obstruksi tengah = nyeri abdomen bawah -sampai scrotum/labia majora Obstruksi bawah = iritasi buli-buli - frekwensi - urgensi nyeri supra pubis

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Nyeri asal testis Akut
Torsio testis keadaan emergensi, nyeri awal regio abd bawah ipsilateral
T r a u m a Epididymitis akut
Kronis Hidrocele Varicocele
IV. PEMBENGKAKAN DAERAH SCROTUM Cancer Inf Hernia HydrocelTorsio Varicocel
Onset akut
- + - - + -
Nyeri ? - + - - ++ -
Trauma ? - + - - - -
Hub. Sex - + - - - -
Discharge - -/+ - - - -
Perubahan (size)
- - ++ +/- - +
V. URETHRAL DISCHARGE
Kekentalan = encer = clamydia/NGU Warna discharge, purulent = GO Hub sex = veneral disease Trauma = blood
VI. DISFUNGSI SEXUAL “ Male sexual dysfunction “ Klasifikasi
Disorders of desire Hyperactivity Hypoactivity = adrogen menurun Sexual aversion
Disorders of erection Erectile dysfunction Prolonged erection (priapism) Erectile deformity

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Disorders of ejaculation Premature E emotional disorders Delayed E An E Denervasi simpatis Retrograde E prostatectomy
Disorders of orgasm An O psyciatric disorders Delayed O
Disorder of sensation Hyposensitivity Hypersensitivity Sexual pain disorders
CLINICAL DIAGNOSIS Clinical diagnosis dibuat berdasarkan :
I. History of the presenting illness II. Physical examinations
III. Performance of special tests I. History = riwayat = anamnesa dimulai dengan keluhan/problems yang menjadi alasan pasien mencari pertolongan, keluhan dicatat secara kronologis Contoh :
Laki-laki, 64 tahun datang dengan keluhan pancaran kencing melemah
Sejak 2 tahun yang lalu Pancaran mulai melemah Hesistensi, mengedan Terminal dribling Frekwensi siang 1-2 jam Nocturia 4 x
Sejak 6 bulan Urgensi Pakaian dalam sering basah Sering ke toilet Malam tidur terganggu Perut bagian bawah terasa penuh
Anamnesa diatas mengarahkan ke suatu keadaan retensio chronis
Tanya hal yang berhub dengan fungsi ginjal mis : anoreksia, nausea, vomitting
Tanya hal yang mungkin berhubungan dengan obstruksi

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Infeksi = dysuria, frekwensi, urgensi Hematuria = BPH malignancy Veneral disease = stricture urethra Hasil anamnesa operasi ? Perlu ditanya keadaan
Kardiorespiratori Perokok, batuk kronis MCI Gangguan pembekuan darah Obat-obat yang dikonsumsi Allergy ???
Anamnesa oleh dokter yang berpengalaman Masalah mudah diketahui Terarah / tidak bertele-tele Mengurangi/menghindari test-test yang tidak perlu Dapat menilai apakah diperlukan tindakan emergensi (tampak
sesak, sianosis) A. KEADAAN UMUM = STATUS GENERALIS KESAN UMUM :
Status Gizi : - Cachexia - Obesity
Edema Gynecomastia limfadenopati Kulit : - Pucat
- Icterus - Dehidrasi B. STATUS UROLOGI 1. Ginjal
pemeriksaan : Inspeksi, palpasi, perkusi, auskultasi, transilluminasi
Daerah sudut costovertebra, abdomen quadran atas kanan/kiri
2. Vesica urinaria= buli-buli=bladder Normal : Volume < 150 cc palpasi (-) Volume 500 cc distensi terlihat/inspeksi (+) Perkusi lebih informatif dibanding palpasi 3. PENIS Inspeksi :
Sirkumsisi/tidak

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Kulit ditarik kebelakang : Inflamasi = balanoposthitis Tumor
Meatus Urethra : - posisi : -hipospadia -epispadia
Kulit Penis : - Ulkus - Condyloma/warts Palpasi :
Corpus cavernosa fibrotik Nyeri +/-
4.SCROTUM + TESTIS Abnormalitas kulit scrotum : - Infeksi
- Kista sebasea Palpasi testis : - ukuran
- bagian yang keras/tumor - UDT +/-
Transiluminasi Palpasi : - epididymis
- vas deferens 5. COLOK DUBUR = RT = DRE
Rutin untuk laki laki > 40 th TSA Prostat Buli Faeces - darah?
KEADAAN ABNORMAL YG SERING DITEMUKAN PADA SAAT PEMERIKSAAN FISIK Ginjal
Tumor = kistik : hydronefrosis poli - multi = Malignancy :
Wilm’s tumor Neuroblastoma Grawitz tumor
Scrotum dan Isinya : torsio hydrocele varicocele
Penis : phimosis paraphimosis peyronie’s Priapismus

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Hypospadia Epispadia Carsinoma
Prostat : prostatitis BPH prostat cancer
III. PEMERIKSAAN PENUNJANG = TEST KHUSUS 1. URINALISA
Pada wanita : midstream Pada laki-laki : void I urethra
void II Bladder void III prostat washing
Mikroskopik sedimen : eritrosit : normal (-) atau < 3 /LPB lekosit : normal < 5 /LPB pada wanita
<2 /LPB pada laki-laki cast : - hyalin
- granular - lekosit - eritrosit
kristal : Calcium Oxalat Calcium Phosphat Calcium amonium magnesium phosphat Uric acid Cystinuria
• Kultur Urin • Cytology
2. TEST FUNGSI GINJAL : - Ureum - Creatinin - C.C.T. 3. URORADIOLOGI
BNO-IVP - Arteriografi Urethrografi - Limfografi Cystografi - CT Scan Tomografi - MRI RPG - Caversonografi APG

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Pemeriksaan Dasar UROLOGI URO + LOGOS UROLOGI: TRAKTUS URINARIUS PRIA & WANITA DAN TRAKTUS REPRODUKSI PRIA (UROLOGI & ANDROLOGI) General Urology Pediatric Urology Endourology Oncologic Urology Female Urology Neuro Urology Andrology Male Infertility
Pemeriksaan dasar Urologi Anamnesa / Keluhan (symptoms) Pemeriksaan fisik Laboratorik Radiologik
Anamnesa / Keluhan (symptoms)
keluhan utama riwayat penyakit dahulu riwayat penyakit keluarga
keluhan utama harap diingat oleh dokter durasi, beratnya, akut/kronik, periodik, derajat gangguan dan hal2 penting (demam, BB turun, lemah) apa yang mengganggu saat ini
Symptoms GU tracts Systemic manifestations
Fever & weight loss Unexplained attacks of fever General malaise
Local & referred pain LOCAL : Involved organ:
kidney (T10-12, L1) testicle
REFERRED : From diseased organ:
ureteral colic ipsilateral testicle (T11-12)

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
I.Ureter 1/3 proximal
2\
II.Ureter 1/3 tengah
III.Ureter 1/3 distal
Urologic organ (common nerve supply) GI Gynec.
KELUHAN (Symptoms) Nyeri Hematuria LUTS (lower urinary tract
symptoms) Disfungsi seksual Hematospermia Pneumaturia Discharge urethra Demam & menggigil Nyeri
nyeri ginjal (renal pain) nyeri ureter (ureteral pain) nyeri vesika (vesical pain) nyeri prostat (prostatic pain nyeri penis (penile pain) nyeri testis (testicular pain) nyeri ginjal (renal pain)
tumpul & menetap (dull pain) keradangan kolik (colicky pain) obstruksi DD: pseudorenal pain (radikulitis)
--lokal --dari tempat lain (referred pain)
nyeri ureter (ureteral pain) akut, kolik, (obstruksi) referred pain (= lokasi) ureter distal: frekuensi, urgensi
DD: divertikulitis (kiri) adnexitis (ki/ka) appendisitis (kanan) kolik tr.digestivus

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Anamnesa / Keluhan (symptoms) • Nyeri
– nyeri vesikal (vesical pain) • Menetap / konstan: retensi urin • Intermiten : inflamasi (suprapubic discomfort)
mis: sististis bakterial atau sistitis interstisialis – nyeri prostat (prostatic pain)
• sekunder o.k. inflamasi dan distensi kapsul prostat – nyeri penis (penile pain)
• kausa: priapismus, Peyronie’s, parafimosis, inflamasi buli2 & uretra (BBB)
– nyeri testis (testicular pain) • dari testis: orko-epididimitis, torsio testis, torsio
apendiks testis • kemeng: hidrokel, varikokel • referred: dari ginjal, ureter
• Hematuria • makros (gross) / mikros ? Sedimen: eri > 3 hpf • inisal / terminal / total • nyeri / tidak • bekuan (clots) & bentuk
‘selalu curiga keganasan sampai terbukti sebaliknya’ • LUTS (lower urinary tract symptoms)
– keluhan iritatif: – keluhan obstruktif – inkontinensia – enuresis – keluhan iritatif (STORAGE):
• frekuensi / nokturia / urgensi / disuria – keluhan obstruktif (VOIDING):
• pancaran melemah • hesitansi • intermitensi • menetes • retensi urin
– Inkontinensia • continue (true) • stress • overflow • urge
– Enuresis • diurnal • nocturnal

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
– Disfungsi seksual – libido menurun – impotensi – gagal ejakulasi – anorgasmus – ejakulasi prematur
• Hematospermia – sering sembuh sendiri – jarang ada patologi – o.k.inflamasi non spesifik uretra prostat, ves.seminalis
• Pneumaturia • Discharge urethra • Demam & menggigil
Riwayat penyakit dahulu
– penyakit dahulu dg sequelae urologik : keluar batu, DM, neurologik, dll
– obat-obatan – pembedahan y.l. – merokok dan alkohol – alergi
Riwayat penyakit keluarga – kanker – BSK
Pemeriksaan fisik • kesan umum:
– cachexia – striae – jaundice – hiperpigmentasi – ginekomastia – edema – uremic frost – anemia – septic
Pemeriksaan fisik • Inspeksi • Palpasi • Auskultasi

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Pemeriksaan fisik • ginjal • buli-buli • penis • skrotum & isi • rektal & pem. prostat (laki2) • pem. pelvis (perempuan) • ginjal
– dewasa: sulit teraba (bimanual) – palpasi bimanual
• Bila teraba : permukaan, konsistensi, nyeri tekan • K.p. : perkusi, transilluminasi
• buli-buli – teraba bila terisi 150 ml – palpasi (bimanual) – perkusi – mobilitas
– penis – bila tdk circ., tarik preputium – kulit – meatus urethrae – palpasi indurasi, batu – fimosis – Peyronie’s disease – priapismus – Hipospadia (+ chordee) – karsinoma
– skrotum & isi – kulit – testis (ganas) – epididimis, vas (jinak) – transiluminasi – kanalis inguinalis (HIL)
• pem. rektal & prostat pd. pria (CD/RT/DRE) – semua pria dg . keluhan urologik – semua pria diatas 40 th

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
• pem. pelvis pd. perempuan – pemeriksa pria didampingi dr./prw. perempuan – inspeksi teliti dlm posisi litotomi – VT atau RT (+ palpasi bimanual)
Pemeriksaan fisik ----- abnormal: • skrotum dan isi
– tumor testis (hampir selalu ganas) – tumor para testikular (hampir selalu jinak)
hidrokel, spermatokel, kista epididimis, – varikokel – torsio testis – epididimitis – orkitis / orko-epididimitis
– prostat – prostatitis akuta – benign prostate hyperplasia (BPH) – karsinoma prostat
Laboratorik
– urinalisis – pd semua pend urologi – UL: kimiawi & mikroskopik – cara koleksi:
– pria: arus tengah (midstream) – perempuan: bersihkan & arus tengah atau urin dg
kateter – neonatus dan bayi: spp (supra pubic puncture /
aspiration) – pem. fisik urin: warna, kekeruhan, BJ, pH – pem. kimiawi:
– urine dipsticks: darah, protein, glukosa, keton, urobilinogen & bilirubin, leukosit
– hematuria & DD – proteinuria – glukosa & keton – bilirubin & urobilinogen – test nitirit
– pem. mikroskopik: sel, silinder (cast), kristal, bakteria, ragi, parasit
– biakan dan test kepekaan AB

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
• sekresi prostat (expressed prostatic secretion) • darah:
• DL: Hb, leuko, diff, PCV, LED • faal ginjal: BUN, kreatinin serum, as.urat • k/p: elektrolit
• Radiologik – USG – foto polos abdomen (BOF, BNO,KUB) – IVP / IVU (intravenous pyelo/uro-graphy)
• Diagnosis – Primer – Sekunder – Komplikasi
• DD (differential diagnosis=diagnosis banding) • Diagnosis kerja • Diagnosis klinik • Diagnosis patologik

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
UROLITHIASIS defenisi “UROLITHIASIS or urinary calculi or urinary stone disease (USD) or batu saluran kemih (Indonesia) is the accurence of stones WITHIN the urinary tract” Human suffered urolithiasis since the beginning of recorded history. It was found by archeologist in the egyptian mummys that estimated to be over 7000 years old. Over the last decade the incidence has significantly increased. EPIDEMIOLIGY Incidence : 2 – 4 % of population The average lifetime risk of stone formation range from 5 – 10 % In the USA stone diseases hospitalization account for more than
400.000 annually The peak incidence : 3rd – 5th decades of life Males are affected 3 times as female Recurrence rates : 15 % in 3 years
30 – 50 % in 15 years In the developing countries the incidence has significantly
increased over the last decades
The development of USD is a complex, still poorly understood and multifactorial process
The theories of stone formation :
1
I. CRYSTALLIZATION THEORY
SUPERSATURATED SOLUTION
CRYSTAL NIDUS
CRYSTALGROWTH (AGGREGATION)
STONE
Solute
pH
temperature
- Inhibitors : • Magnesium • Citrate • Pyrophoshate • Peptides • Heavy Metals

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Prerenal
◦ Exogenous : Dietary Immobilization Medication : vit D over dosage
vit C more 4 g/day ◦ Endogenous :
Hyperpara thyroidism Uric acid diasthesis Malabsorbsi
Renal ◦ Glomerular ◦ Tubular : RTA
Idiopathic hypercalciuria Post renal
◦ Epithelial lesion ◦ Obstruction ◦ infection
II. COLLOID/MATRIX THEORY :
Kidney excrete organic compound
Muco Protein (MATRIX)
STONE
Crystal deposition

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
I. GENETICS/heredity :
• Cystinuria • Renal tubular acidosis • Medullarry sponge kidney
II. GEOGRAPHY : • High temperature • High humidity
III. DIET : • Increase intake of
Calcium Oxalat
IV. OCCUPATION • Scdentary job
Composition Freq
(%) Effect of pH On solubility
Rö density
Calcium : – oxalat – phosphate – oxalat &
phosphate
80 35 10 35
Little effect
0,50 1,0
Struvit 10 At pH < 5,5 0,2 Uric acid 8 At pH > 6,8 0,05 Cystine 1 At pH > 7,5 0,15 Other 1 0,05

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Type of stone Etiologic Factors Calcium oxalate Calcium phosphate Calcium carbonate Uric acid Cystine Struvit Matrix
Supersaturation of urine with calcium from : a. Renal leak b. Intestinal absorption c. Bone resorption hyperoxaluria Hyperuricosuria Constantly low urine pH Cystinuria Alkaline urine caused by ure splitting organism As above (idem dito)
I. UPPER TRACT USD :
◦ Renal Calculi : Asymtomatic until : Causes obstruction or Infection
◦ Obstruction : Acute
Colicky pain, may be radiate to : Groin Testis Tip of the penis
Hematuria, negative in 15 % Nausea, vomiting
Chronic : asymtomatic ◦ Infection : Fever and chills
Pain in the costovertebral angle

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Blood examination : WBC
creatinine Urine analysis and culture Plain abdominal film (KUB) USG if available • Spiral / helical CT Scan • IVU : recently is infrequenly used
I. Acute Treatment A. Ureteric Colic adequate pain relief
Parenteral narcotics : Morphine sulfat Pethidine HCL
Nonsteroid anti inflamatory drugs (NSAID) Ketonoloc tromethamine Acetaminophen Ibuprofen : 600 – 8– mg/8 hours Nifedipine XR : 30 mg/once/day Cox-2 inhibitor : Parecoxib : i.v. 40 mg
Anti emetic drugs B. Immediate intervention
The form of intervention : Ureteral stenting Percutaneous/open nephrostomy tube
Indications : A solitary functioning kidney Elevated creatinine Pre existing renal insufficiency Fever of unclear etiology/suspected UTI Intractable pain/colick Pyonephrosis
II. Definitive treatment of upper tract USD 1. Expectant treatment/non surgical treatment
Indications : a. Small opaque stone ( < 5 mm ) b. Minimal hidronephrosis c. No UTI d. Stone in the lower third ureter e. asymptomatic

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Methods : a. Oral hydration drink copious quantities of
water b. Drugs : Kalkurenal, enatin, 1 blocker c. Jump around d. Save for analysis any stone passaged out e. Weekly plain abdominal film f. Expectative time : 4 – 6 weeks
Result : a. 90% of 4 mm stone pass spontaneously b. 20% of stone > 6 mm pass spontaneously
2. ESWL Indications :
a. Renal stone with size of 1,5 cm – 2 cm b. Ureter proximal stone < 8 mm or after pushed
up and stenting c. Distal ureteral stone
3. Endoscopic Treatment :
A. Ureteroscopic : Rigid /semirigid ureteroscope Flexible ureteroscope
Usage of ureteroscope : Stone extruction :
Grasped forcep Stone basket
Stone fragmentation (lithotripsy) using : Ultrasound Electrohydraulic Pneumatic Laser (Holmium-YAG)

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Pushing stone upward Succes rate : up to 95%
B. Percutaneous Nephrolithotripsy (PCNL) :
Indications : Stone size > 2 cm Staghorn calculi
(multistage treatment) Succes rate : up to 85%
4. Laparoscopic Surgery : Indication : proximal large ( > 2 cm ) ureteral stone
5. Open Surgery : Pyelolithotomy Nephrolithotomy Bivalve/anatrophic Ureterolithotomy
I. Bladder Stone : A. Predisposing factors :
Bladder outlet obstruction Foreign bodies Passing of ureteral stone nidus in the bladder Hyperuricosuria Diverticle
B. Clinical Presentation Pain :
Hypogastrium area Referred pain to the penis
Hematuria Dysuria Intermittent stream Recurrent UTI
C. Diagnosis : KUB photo USG cystoscopy
D. Treatment : 1. Lithotripsy :
Mechanical Electrohydraulic

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Laser ESWL Pneumatic
2. Vesicolithotomy
Most of the small bladder stones will pass spontaneously A small amounts of urethral stone entrappe and impacted in the
urethra i.e in the verumontanum and in the fossa naviculare
Gently posterior lubrication Dorsal meatolithotomy Pushing endoscopycally into the bladder and lithotripsy
USD : ◦ 90% of patients USD accosiated with metabolic,
environmental and life style etiology ◦ Up to 80% will recure after first episode of USD ◦ Prevention of recurrent USD is utmost important
Normal value of substances in 24 hr urine Substance Male (mg) Female (mg) Calcium Uric acid Oxalate Citrate
< 300 < 800 < 50 450 - 600
< 250 < 750 < 50 650 - 800
Baseline evaluation for USD Determination of :
◦ Serum Ca, phosphorus, and uric acid ◦ 24 hour excretion in the urine of :
Ca, P, uric acid, oxalate and creatinine If any abnormality found should a more extensive evaluation
performed

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Causes : ◦ Hyperparathyroidsm
Bone resorption ◦ Renal leak ◦ Hyperabsorption from g i tract
Metabolic evaluation : 1. Baseline studies :
Regular diet Collect 24 hours urine for :
Creatinine Calcium P Uric acid Oxalat Citrate
Metabolic evaluation : 2. Dietary Restriction :
Diet limited to 400 mg Ca 100 m Eq Na/day 1 week Urine 24 hours examination as foremention
1. Calcium loading :
Overnight fasting First voided urine discarded 2 hours urine collection examination Receive 1 g Ca gluconate 4 hours urine collection
and examination Classification Hypercalciuria
Type Serum Ca Urine Calsium
Fasting After Loading Resorptive Absorptive Renal Leak
Up N N
Up N Up
Up Up Up

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
ETIOLOGY :
1. Hyperparathyroidsm 2. Bone metastatic Cancer 3. Multiple myeloma 4. Immobilization 5. Cushing’s syndrome 6. Hyperthyroidism
Treatment : ◦ Treat the etiology
Found in > 50% of patients USD After loading test positive Hyperabsorption of ingested Ca Treatment :
1. Diet and hydration – Restructed Calcium to 400 mg Ca/day and Na 100 m
Eq/day – Drink 3 – 4 L water daily
2. Cellulose phosphate 3 x 5 g/day need : Magnesium supplement and lowering oxalate diet
3. Orthophosphate 3 – 6 g daily
Accounts for appreoxmately 10% patients with hypercalciuria Pathogenese : innability of the tubulus to resorb calcium Treatment :
1. Thiazide diuretics : – Increase resorption in the tubulus – Dosis : 2 x 50 mg a day – Pottasium supplement is necessary
2. Orthophosphates
Pure uric acid stones : 10% of USD Uric acid insoluble in pH < 5,8 Etiology : - gout disease in 25%
- others unknown Risk factors : - constantly
- low urine output Treatment :
1. Hydration : > 3 L/day

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
2. Alkalinization of urine : sodium bicarbonate orally 650 mg (2tablets) every six hours
3. Low purine diet Low protein diet, 90 g/day
4. Allupurinol : 200 – 600 mg daily
Oxalic acid :
◦ Extremely insoluble ◦ End product of metabolism (mostly) ◦ 10% is absorbed from g.l. tract
Hyperoxaluria divided in : 1. Primary 2. Enteric 3. Exogenous
1. Primary Hyperoxaluria :
• An autosomal recessive disorder • Urinary oxalate > 100 mg/day • Early onset of nephrocalcmiosis • R/ - pyridoxine 100 – 400 mg daily
- hydration - low oxalate diet
2. Enteric hyperoxaluria : • Malabsorption (increase) of oxalat
due : inflamatory bowel disease small bowel by pass ◦ R/ - low oxalate/fat diet
- calcium supplement - cholestyramine
3. Exogenous hyperoxaluria • Ascorbic acid > 5 g/day • methoxyflurane
Found in up to 50% pts with Ca stones check rutinly urinary citrate R/ Potassium citrate

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Are composed of : magnesium ammonium phosphate and carbonate apatite
= triple-phosphte strued Need : - markedly elevated urine pH
- high concentration in the urine of : ammonia, bicarbonate and carbonate - produce by urea splitting organisms The urea splitter : Protein ( > 75% )
Klebsiella Pseudomonas Providenced Staphylococcus Ureaplasma urealyficum Female 2 x male Occurred in 10% of praplegic pts
Urinary infection with high urine pH Relative radiolucent big stone in the PCS
Treatment :
1. Anatrophic nephrolithotomy 2. P N L 3. P N L & ESWL (sandwich technique) 4. Chemolysis :
10% Hemiacidrin salution (Renacidin) (pH = 4,0) is dilevered via nephrostomy tube or ureteral catheter

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Benign Prostatic Hyperplasia (BPH)
Anatomi prostat: • Kel.prostat: kel.seks
asesorius pria • Normal sebesar buah kenari
dikelilingi kapsul fibrous dan mengelilingi uretra
• Pada waktu ejakulasi memproduksi cairan prostat
yang bersama dengan produk dari testis, ves.seminalis & kel.bulbouretral membentuk semen Prostat & buli2 normal Letak anatomik prostat Perubahan patologik pada prostat juga berakibat pada buli2 Perubahan pada buli2 bisa berakibat perubahan pada traktus
urinarius bagian atas (ureter dan ginjal) Pembesran prostat jinak Lobus medius menonjol ke dasar buli2 Uretra pars prostatika menyempit Terjadi trabekulasi dari dinding buli2
Akibat dari BPH o Penebalan dinding buli2 o Hematuria berulang o Terbentuk divertikel buli2 o Infeksi saluran kemih o Terbentuk batu buli2 o Dilatasi bgaian atas Diketahui sejak 1500 S.M. 1000 tahun kemudian
didiskusikan oleh Hippocrates Insidensi: 50% (klinis) pria 60-
69 tahun, k.l. 100% pada umur 80 tahun (mikroskopik sejak umur 35 tahun)
BPH - DM S 2002 3
Anatomikelenjar prostat
Uretra parsprostatika Prostat
Muara duktusejakulatorius
Sfingter uretraeksterna

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Patogenesis BPH Syarat terjadinya BPH : * Testis yg memproduksi androgen * Ketuaan ( ? )
BPH 2000 - DMS
Cinical prevalence in the Baltimore Longitudinal Study of Ageing (based on history andPhysical examination, n = 1,057)
Clinical prevalence in the Baltimore Longitudinal Study of Ageing (based on rectal examination, n= 1,057)
27
51
69
80
9
42
57
27
0 20 40 60 80 100
40-49
50-59
60-69
70-79
Age
(yea
rs)
Prevalence (%)
0 20 40 60 80 100
Age-specific prevalence of BPH

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
13
TheoryDihydrotestosteronhypothesis
Oestrogen-testosteronimbalance
Stromal-epithelialinteractions
Reduced cell death
Stem cell theory
Theories for the cause of BPHCause 5- reductase and androgen receptors
Oestrogens Testosteron
Epidermal growthfactor/fibroblastgrowth factor Transforming growthfactor
Oestrogens
Stem cells
EffectEpithelial and stromalhyperplasia
Stromal hyperplasia
Epithelial and stromalhyperplasia
Longevity of stromaand epithelium
Proliferation of transitcells
Simptomagenesis Prostatisme Sindroma Prostatisme LUTS (lower urinary tract symptoms) Fungsi unit Vesiko Urethral 1. Penyimpanan (STORAGE) 2. Mengeluarkan urin periodik (VOIDING) BPH LUTS keluhan obstruktif: 1. Hesitansi 2. Pancaran lemah 3. Mengejan 4. Kencing lama 5. Terasa tak habis 6. Retensi urin 7. Overflow Incontinence (ischuria paradoxa) BPH LUTS keluhan iritatif -1.Urgensi Urge incontinence -2.Frekuensi (pollakisuria) -3.Nokturia

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
International Prostate Symptom Score (I-PSS) Dalam 1 bulan terakhir:
• 1. Terasa sisa kencing 0 1 2 3 4 5 • 2. Sering kencing 0 1 2 3 4 5 • 3. Terputus-putus 0 1 2 3 4 5 • 4. Tidak bisa menunda 0 1 2 3 4 5 • 5. Pancaran lemah 0 1 2 3 4 5 • 6. Mengejan 0 1 2 3 4 5 • 7. Kencing malam 0 1 2 3 4 5
Total ……. Total IPSS score: 0-7: ringan, 8-18 : sedang, 19-35 : berat Provokator Retensi Urine Akuta 1. Minum alkohol Stimulan simpatetik Tonus Prostat & otot polos bladder outlet 2. Bepergian jauh 3. Masukan cairan banyak 4. Konstipasi 5. Agen anti cholinergik DRE (digital rectal examination) = RT = CD Ukuran Konsistensi: padatkenyal/keras/nodul Mobilitas Batas2 anatomik: atas, lateral, sulkus
PSA interpretation Kadar PSA 0.5 - 4 ng/ml 4 - 10 ng/ml > 10 ng/ml kenaikan > 20% / tahun Uroflowmetri Max.flow rate (ml/sec) > 15 ml/sec 10 - 15 ml/sec
Interpretasi
Normal
20% kemungkinan Ca
50% kemungkinan Ca
Perlu biopsi
Interpretation
Normal
Mild obstructed
Obstructed

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
< 10 ml/sec TRUS (Transrectal ultrasound) Accurate measurement of the prostate Hypoechoic focus Prostatic biopsy (if indicated)
Diagnosa BPH Anamnesa:
I-PSS Pem.fisik:
buli-buli CD / RT
Pem.tambahan: lab: UL,DL,RFT,PSA pencitraan: USG/BOF/TRUS/IVP
Terapi BPH Konservatif: observasi (watchful waiting) 0 - 7 Medikamentosa (Tx medik) 8 - 18 Pembedahan: 19 - 35
terbuka endoskopik: TURP, TUIP
Invasif minimal: balloon dilatation stent microwave (thermotherapy) radiofrequency laser ablation
Kontra-indikasi Tx medik BPH Retensi urin (akut atau kronik) Insufisiensi renal Dilatasi traktus atas Hematuria berulang ISK berulang Batu buli-buli / divertikel
Terapi medik BPH Alpha blocker
terazosin prazosin tamsulosin, dll
Supresi Androgen 5 alfa-reduktase inhibitor
Fitoterapi Morfometri BPH Rasio of epithelium terhadap stroma:

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Efikasi vs. risiko terapi BPHefikasi
risiko
OPEN PROSTATECTOMY
OPEN PROSTATECTOMY
TURPTURP
TUNATUNA
THERMOTHERAPYTHERMOTHERAPY
ALPHA BLOCKERSALPHA BLOCKERS5-ALPHA REDUCTASE INHIBITORS
5-ALPHA REDUCTASE INHIBITORS
PHYTOTHERAPYPHYTOTHERAPY
epith : stroma = 21.6 - 50 % : 60 - 78 % BPH simtomatik: proporsi stroma lebih tinggi Respons terhadap Tx: predominan otot polos : alpha blocker predominan epithel : supresi androgen predominan fibrosis : bedah
Rasional penggunaan alpha blocker Kontraksi otot polos prostat dimediasi oleh : stimulasi simpatis
reseptor alpha Kontraksi otot polos (kapsul, adenoma, leher buli) : merupakan
40% dari penyebab obstruksi saluran keluar Alpha blocker :
relaksasi otot polos prostat mengurangi simtom memperbaiki pancaran kencing
Agen fitoterapi untuk BPH Pygeum africanum (African plum) Urtica spp. (stinging nettle) Sabal serrulatum (Dwarf palm) Serenoa repens B (American dwarf palm) Cucurbita pepo (Pumpkin seed) Populus tremula (Aspen) Echinaceapurpurea (Purple coneflower) Secale cerelea (Rye)
Intervensi urologis di Surabaya Balloon
dilatation Prostatic stent Thermotherapy TUIP
(transurethral incision of the prostate)
TURP (transurethral resection of the p.)
Laser TURP Open
prostatectomy

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Prostatektomi terbuka Retropubik (Millin) atau Suprapubik (Freyer) Indikasi: Prostat yang besar (>40-60 mg) BPH + BBB besar Kelainan sendi coxae (tak bisa litotomi) RS yang tak ada alat TURP
TURP (transurethral resection of the prostate) Memakai alat resektoskop Dengan atau tanpa endokamera (video) Indikasi:
Gold standard terapi operatif BPH Harus dilakukan oleh dokter spesialis urologi
Paramedis harus terlatih, di OK maupun ruangan TURP (transurethral resection of the prostate) Penyulit intra bedah:
Perforasi buli2 Perforasi kapsul prostat (sinus terbuka) Perdarahan Lesi sfingter uretra eksterna Sindroma TUR
Penyulit pasca bedah dini: Sindroma TUR Perdarahan Retensi bekuan darah Urosepsis Retensi urin pasca lepas kateter
Penyulit pasca bedah lanjut: Hematuria berulang Infeksi saluran kemih Orko-epididimitis Ejakulasi retrograd Inkontinensia urin Striktura uretra Stenosis leher buli2

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Prostat Hipertrofi Pembesaran jinak prostat BPH = Benign Prostate Hyperplasia Definisi :
Suatu keadaan terjadinya pertumbuhan yang berlebihan dari komponen stroma dan epitel gld. Prostat Berdasarkan PA yang terjadi sebenarnya hiperplasia
kelenjar periurethral yang kemudian mendesak jaringan prostat yang asli ke perifer menjadi kapsul = surgical capsule
Prevalensi
Data di indonesia belum ada Berry dkk ( 1984 )
hasil autopsi tentang hubungan usia dengan besarnya prostat : 41 – 50 th 23% 51 – 60 th 42% 61 – 70 th 71% 71 – 80 th 82% 81 - 90 th 88%
Watanabe (1984)

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
37% laki-laki jepang ≥ 55 tahun BPH berdasarkan skriningUSG
Glynn ( 1985 ) Angka prostatektomi per 1000 pria/tahun 40 – 49 thn 0,9% 50 – 59 thn 4,1% 60 – 69 thn 12,1% 70 – 80 thn 19,4% Insiden di RSUP palembang
I. Batu saluran kencing II. Prostat hipertrofi III.Striktur IV. Trauma V. Keganasan Etiologi
Belum jelas benar Beberapa teori :
Teori stem cell Teori reawakening Teori hypothalamic-pituitary gonade axis = DHT Teori groeth factors
Terdapat hubungan antara usia dengan faktor hormonal Teori Stem Cell ( Isaac 1987, Cohey 1990 )
Normal : sel tumbuh sebanding dengan sel mati = steady cell BPH : pembentukan sel baru lebih banyak dibanding sel mati Berry, 1987 :
pengaruh estrogen memperlambat kematian sel prostat Stem Cell proliferasi/sel baru sebanding dgn sel mati - usia - ggn keseimbangan hormonal Teori Reawakening ( Mc Neal 1978 )
Proses hiperplasia prostat merupakan interaksi antara elemen stroma dan elemen epitel
Pada kehidupan embrional elemen stroma menginduksi pertumbuhan epitel
Pengulangan proses ini = reawakening mungkin merupakan mekanisme pembentukan BPH
Estrogen turut mempengaruhi perkembangan stroma dan DHT mempengaruhi komponen epitel

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Teori Growth Factors adanya interaksi antara unsur stroma dan unsur epitel ternyata dipengaruhi oleh faktor faktor pertumbuhan seperti ;
EGF = epidermal growth factor KGF = keratinocyte growth factor IGF = insuline like growth factor TGFβ = Transforming growth factor
• Skema antara stimulasi – inhibisi factor
androgen( DHT)
- KGF- EGF TGFβ- IGF
proliferasi sel sel mati
seimbangprostat normal
androgen( DHT )
Agonistic antagonisticKGF
EGF TGF βIGF
sel mati
Proliferasi selprostat hiperplasia

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
• Patologi prostat hiperplasia – Lowsley : 5 lobus – Mc Neal (1972) : Zona perifer
Zona sentral Zona transisional Zona pre prostatik sfinkter Zona segmen anterior
• Daerah predileksi tersering terbentuknya nodule hiperplasia yaitu zona transisi dan zona preprostatik spinkter
• Gejala prostat hypertrofi – Tidak ada korelasi antara besar prostat dengan beratnya
gejala – Boyarsky ( 1977) : gejala gangguan miksi sebab pembesaran
prostat 1. gejala Obstruksi = statik
• Pancaran melemah = menetes • Intermitten = terputus • Driblling terminal • Hesitansi
2. gejala iritatif = dinamik • Frekwensi, nocturia • Urgency • Dysuria • Tidak lampias = sisa kencing
• Gejala Umum : – nyeri pinggang – Mual muntah ggn fungsi ginjal – somnolen disorientasi – lemah ,BB menurun azotemia
• Patofisiologi Gejala
– timbulnya manifestasi obstruksi di tentukan oleh : • volume kelenjar • elastisitas leher vesika, otot polos prostat dan kapsul • kekuatan kontraksi detrusor
– gejala iritatif oleh karena faktor : • gangguan tonus otot buli o.k. hipertrofi detrusor • infeksi • residual urin
– acut retensi • infeksi • pemberian cairan >> • obat obat anti cholinergik, sympatomimetik

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
– hematuria • Pelebaran vena prostat ruptur • Infeksi • Batu • Keganasan
DIAGNOSTIK Rekomendasi WHO/ICC For BPH : I. 1. Menggunakan symptom score untuk penderita BPH 2. Menggunakan kriteria Quality of Life Assesment ( QOL ) II. Rekomendasi “diagnostic Work-up” terhadap laki-laki ≥ 50 th dengan simtom LUTS dan kecurigaan B.O.O. 1. Highly Recommended Diagnostic Test a. History = anamnesa meliputi :
– Tractus urogenital – Operasi sebelumnya – Kesehatan umum – Obat yang dikonsumsi – Kondisi ( fitness ) untuk kemungkinan tindakan operasi
b. Quantification of symptom ( penghitungan scor simtom )
– I-PSS 0 - 35 – QOL 0 - 6
c. Voiding Diary meliputi frekwensi dan volume miksi sepanjang hari ( 24 jam ) membedakan dengan ;
– DM – Penyakit Jantung Kongestif – Banyak minum – Penyakit ginjal
d. Pemeriksaan fisik dan RT difokuskan untuk meng”assess” :
– Regio suprapubik tanda-tanda distensi buli – Tonus spinkter – Bulbo cavernosus refleks – status neurologis ekst. Inf.
R T mengevaluasi Gld. Prostat – perkiraan ukuran – konsistensi – bentuk

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
– kecurigaan cancer prostat e. Urinalisa
– hematuria – proteinuria – pyuria – Keadaan patologis lain misal : krystal, glukosa, bilirubin,dll
f. Assesment Fungsi Ginjal – serum creatinin - ureum
g. Serum Prostate Spesific Antigen ( PSA ) terutama :
– perkiraan usia > 10 thn lagi = life expectancy – diagnostik Ca.prostat – PSA meningkat - setelah ejakulasi
- inflamasi = infeksi prostat - ischemic = infark prostat - BPH - PIN - Prostat Ca
– PSA Menurun - pengurangan ukuran prostat - stimulus androgen : - LNRH Analog - Castrasi - Estrogen - 5 alfa reduktase inhibitors
– PSA density = nilai PSA/Vol Prostat – PSA Velocity= perubahan PSA/ml/thn – Normal ( Cut off Level ) PSA = 4,0 ng/ml
2. Recommended Diagnostic Test Bila : LUTS (+) tapi BOO tidak spesifik a. Flow Rate alat ; Uroflowmeter satuan ; ml/dtk = cc/dtk Qmax = max.urinary flow rate Qave = average urinary flow rate b. Residual urine cara : - cateterisasi post void - USG / TRUS 3. Optional a. Pressure flow studies b. Imaging :
• TAUS atau TRUS PSA • saluran kencing atas = U U T dengan USG atau
IVP - riwayat infeksi UUT

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
- hematuria - riwayat urolithiasis - pernah operasi TUG - renal insufisiensi DIFFERENTIAL DIAGNOSE Ca. prostat Prostatitis Ca. Vesika Tumor ekstra Vesika Obstruksi leher vesika ( Fibrosis, Kontraktur ) Obstruksi urethra ( striktur, Batu ) NMeurogenic Bladder = spinchter dyssinergia
TERAPI BPH 1. Watchful waiting BPH dengan simptom minimal 2. Medical therapy a. Alfa adrenergic rec. antagonist ( Alfa Blockade )
• Terazosin = Hytrin • Prazosin = minipress
b. 5 alfa reduktase inhibitor • proscar
c. Phytoterapi • epi prostat • tandenan
3. Non Surgical invasive therapy – Ballon dilatation
– Urethral stents – Thermo therapy = hyperthermia

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
4. Surgery – TUR - P – TUI - P – Open prostatectomy – Laser prostatectomy – Electrovaporization
Prostatectomy terbuka Cara : 1. Freyer : trans vesica
2. Terrence millin : retro pubic Indikasi :
perkiraan berat prostat > 60 gram disertai : batu buli, divertikel
Kelemahan/kerugian morbiditas tinggi 10 - 25 % mortalitas 1 - 4 % nyeri pasca operasi ++ ada luka sayatan di kulit
Keuntungan mudah/sederhana, tanpa alat mahal dapat dikerjakan ahli bedah umum
T U R - P merupakan pengobatan terpilih, gold standard
pada prostat hipertrofi morbiditas 8 - 10 % mortalitas 0,2 - 1 % Nyeri pasca bedah minimal tanpa luka sayat operasi pada kulit Kelemahan :
perlu alat khusus hanya dapat dikerjakan oleh ahli urologi

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
ORTHOPAEDIC SURGERY Dr. MUZAKKIE, SpB, SpOT.
NICOLAS ANDRY 1741 ORTHOS = LURUS PAIS = PAEDOS = ANAK Orthopaedic Definition ( Salter ) Art & Science
• Investigation • Diagnosis • Treatment • Prevention
Disorder & Injury of musculoskeletal system by medical surgical & physical study. Physiology, pathology & basic science ORTHOPAEDIC - TRAUMA - DISORDERS
• TRAUMA FRACTURE & DISLOCATION
• DEGENERATIF • SCOLIOSIS • OSTEOPOROSIS • ARTHROSCOPY • RHEUMATOID • TUMOR • C P
BONE : STRUKTUR 1. FRAME WORK 2. LEVERS 3. PROTECTION
ORGAN 4. HEMOPOETIC 5. STORAGE EMBRYONIC MESENCHYMAL MOD. CARTILAGE MOD. CO PERISOTEUM 5th WEEK 6 th WEEK 6 BLN 9 BLN

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
GROWTH • LENGTH :
1. ARTICULAR CARTILAGO 2. EPIPHYSEAL PLATE CARTILAGO
• WIDTH : PERIOSTEUM REMODELING WOLF LAW (Julius Wolf 1872)
• DEPOSIT – STRESS (+) CONCAF • RESORBSI – STRESS (-) CONVEX
PROSTHESIS PARTIAL AUSTIN MOORE THOMSON TOTAL -> Calcar Femorale SENDI SYNDESMOSIS → IV DISC SYNCHONDROSIS → EPIPH. PLATE SYNOSTOSIS → SKULL SYMPHYSIS → SYMP. PUBIS SYNOVIAL JOINT MOVE ABDUCTION – ADDUCTION FLEXI – EXTENSI INTERNAL ROTATION – EXTERNAL ROTATION PRONASI – SUPINASI EVERSI – INVERSI DEVIASI : - RADIAL DEVIASI - ULNAR DEVIASI DEFORMITAS
• CALCANEUS >< EQUINUS • CAVUS >< PLANUS • VARUS >< VALGUS • ANGULASI = BOWING DEFORMITY
PEMERIKSAAN LOOK - INSPEKSI FEEL - PALPASI MOVE - ROM SYMETRISITAS RADIOLOGI

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
TEST HIP : - THOMAS TEST - TRENDELENBERG - BARLOW ORTOLANI ORTHOPAEDIC DISORDERS VARIASI NORMAL
• JOINT LAXITY - PES PLANUS - GENU VALGUM
• INTERNAL TORSION - FEMORAL TORSION - TIBIAL
• EXTERNAL TORSION - FEMORAL - TIBIAL
• GENU VARUM • KYPHOSIS
CONGENITAL APLASIA/ HYPOPLASIA DISPLASIA HIPERTROPHY : LOCAL GIGANTISM DUPLICATION : • POLYDACTYLY → THUMB : WASSEL TYPE→ 7 TYPE CONGENITAL SPESIFIC FOOT : * METATARSUS PRIMUS VARUS → HALLUX VALGUS * METATARSUS ADDUCTUS ( VARUS) CTEV (congenital talipes equino varus) CLUB FOOT
• ♂ > ♀ • INSIDENS , 2 ‰ • DEFORMITAS
• MIDTARSAL JOINT FOREFOOT ADD & SUP • SUBTALAR JOINT HEEL VARUS • ANKLE JOINT EQUINUS • NECK OF TALUS ANGULATION FOOT DEVIATION

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
TH/ - SERIAL CAST - DENIS BROWNE SPLINT - OUT FLARE SHOES - SURGICAL • RIGID • NEGLECTED • PES CALCANEOVALGUS • TARSAL COALITION = RIGID VALGUS FOOT • ACESSORY TARSAL NAVICULAR (OS TIBIALE EXTERNA)
• LONG BONE PSEUDO ARTHROSIS OF TIBIA
• KNEE : DISCOID MENISCUS • HIP : COXA VARA
CDH – BARLOW ORTOLANI Th/ FREJKA PILLOW PAVLIC HARNESS
• POLYDACTYLY / MIRROR FINGER • TRIGGER THUMB • HIPOPLASIA OF RADIUS • SPINA BIFIDA • SCOLIOSIS • TORTICOLLIS • OSTEOGENESIS IMFERFECTA • ACHONDROPLASIA • ARACHNODACTYLY • MULTIPLE EXOSTOSIS • AMYOTONIA CONGENITAL =
FLOPY CHILD • AMYOPLASIA CONGENITAL =
ATHROGRYPOSIS MULTIPLEX CONGENITA. PENYAKIT METABOLIC ORTHOPAEDIC RICKETS - DEF VIT D →↓CALCIFIC MATRIX - RACHIITIC ROSARY OSTEOMALACIA - DEWASA RICKETS - PSEUDO FRAKTUR - MILKMAN’S SYNDROME SCURY - AVITAMINOSIS C - MATRIX ↓ - PSEUDOPARALYSIS

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
OSTEOPOROSIS - OSTEOPLASTIC → MATRIX (↓) - OSTEOPENI - HORMONAL IMBALANCE - DISUSE - POST MENOPAUSAL & SENILE OSTEITIS FIBROSA CYSTICA = HYPERPARATHYROIDISM OSTEOCLASTIC RESORBSI ↑ - OSTEOLYTIC LESION = BROWN TUMOR - PATHOLOGIC FRACTURE HYPERPITUITARISM = - GIGANTISM → FEMORAL EPIP SLIP (COXA VARA) - AEROMEGALY ( ADULT ) CUSHING SYNDROME - HYPER ADRENOCORTICISM HIPOPITUITARISM HORMON ↓ - DWARFISM - FROLIC SYNDROMW
• POLYOSTOTIC FIBROUS DYSPLASIA • PATHOLOGIC FRACTURE • ALBRIGHT’S SYNDROME - ♀ , SEX PRECOC
• OSTEITIS DEFORMANS (PAGET’S DISEASE) - UMUR TUA → BOWING PROGRESIF & SAKIT TULANG PANJANG SKELETAL RETICULOSIS - NON LIPID RETICULOSIS (HISTIOCYTOSIS X) 1. LETTERES SIWE’S 2. HAND SCHULLER- CHRISTIAN DIS 3. EOSINOPHYLIC GRANULOMA - LIPID RETICULOSIS : GAUCHERS’S - LIPID KERASIN

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
PENYAKIT INFLAMASI ORTHOPAEDI I. PYOGENIC BACTERIAL
II. GRANULOMATOUS BACTERIAL III. NON SPESIFIC INFLAMATORY DISORDER I.1. OSTEOMYELITIS AKUT - HEMATOGENOUS → METAPHYSIS - STAPHLOCOCCUS * FOCUS → REAKSI PERIOSTEAL => UBCUTAN ABSES - BONE NECROSIS => SEQUESTER → CLOACA - NEW BONE FORMATION =>INVOLUCRUM - SEPTIC ARTHRITIS KOMPLIKASI : ACUTE : - † - ABCESS > LATE : - CHRONIC - FRAKTUR PATOLOGIS - KONTRAKTUR 2. OSTEOMYELITIS KRONIK - SEQUESTRUM - INVOLUCRUM * ONCE OSTEOMYLITIS FOR EVER OSTEOMYELITIS 3. ACUTE SEPTIC ARTHRITIS DALAM PERSENDIAN 4. OSTEOMYELITIS OF THE SPINE - STAPHYLOCOCCUS, E.COLI 5. JARI-JARI - PARONICHIA, FELON II. GRANULOMATOUS BACTERIAL INFECTION CAUSA : - TB - SYPHYLIS - FUNGI : ACTINOMYCOSIS TUBERCULOSIS OSTEOMYELITIS OF THE SPINE - BATSON PLEXUS - ANTERIOR PART DARI CORPUS VERT → PUS - KIPOSIS → KOMPLIKASI PARAPLEGIC III. NON SPECIFIC RHEUMATOID ARTHRITIS ANKYLOSING SPONDYLITIS HEMOPHYLIC ARTHRITIS TB SPINE → ANTERIOR SPINAL FUSION

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
PENYAKIT DEGENERASI • HNP = PID • SPINAL STENOSIS • NON ARTICULAR RHEUMATISM
* CALCIFIC SUPRASPINATUS TENDINITIS - PAINFULL ARCH SYNDROME * ADHESIVE CAPSULITIS - FROZEN SHOULDER
• TENNIS ELBOW : EPICONDYLITIS • DE QUERVAIN’S : APL & EPB • TRIGGER FINGER : CAPSUL & TENDON SHEATHS OF THE
PALM • POPLITEAL CYST (BAKER’S CYST)
- KNEE JOINT (SPT GANGLION)
• BURSITIS - BUNION - MP I - HOUSEMAID’S KNEE – PREPATELLA - WEAVER’S BUTTON – RADIAL - STUDENT ELBOW - OLECRANON NEUROMUSCULAR DISORDER Cerebral Palsy - SPASTIC
- ATAXIC - ATHETOID * SCISSOR GAIT * EQUINUS DEFORMITY * THUMB CLUTCHED * POLIOMYLITIS - RESIDUAL DEFORMITY → ADL NERVE ENTRAPMENT
- CARPAL TUNNEL SYNDROME (CTS) - ULNAR TARDY PALSY - SCALENUS SYNDROME * BRACHIAL PLEXUS pd THORAX OUT LET - MORTON : METATARSALGIA
• BRACHIAL PLEXUS INJURY ( OBSTETRICAL) → UPPER ARM TYPE * ERBS PALSY (C5-6) → LOWER ARM TYPE * KLUMPKES PALSY (C7-8) * MUSCLE DYSTROPY (DMP) → GOWER SIGN

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
ORTHOPAEDIC disorder congenital Dr. MUZAKKIE, SpB, SpOT.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Neglected CTEV
Matatarsus primus varus halux valgus Genu varum Congenital constriction band
Congenital constriction bands are partial or complete annular skin depressions seen at birth. The cause is unknown. The incidence in Malays is estimated to be 1 in 3500 births-about 5 times that of Chinese and Indians. In severe constriction, gangrene may occur distally.
The constriction band was excised and the skin closed by Z-plasty in a two-stage procedure.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Habitual patella dislocation Amyoplasia congenital
Congenital Dislocation of the Hip
The Ortolani’s test to assess hip stability is done by abducting and flexing the hip to reduce a dislocated hip.
The Barlow’s test the reverse of the Ortolani’s. An unstable hip is dislocated by adducting the hip and gently pushing it posteriorly. Excessive force must not be used and the baby should be calm.
Syndactyly polylydacty
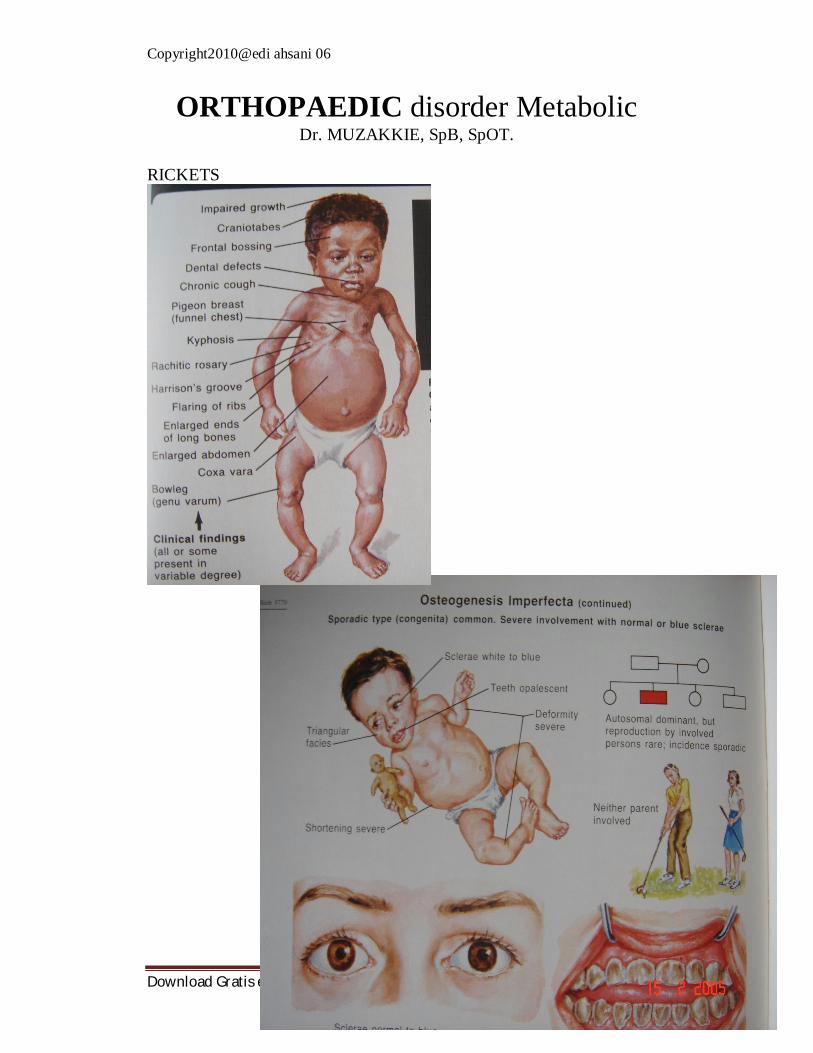
Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
ORTHOPAEDIC disorder Metabolic Dr. MUZAKKIE, SpB, SpOT.
RICKETS

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Sofield osteotomy = cis kebab

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Ehler Danlos Syndrome

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Senile osteoporosis

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Trendelenburg’s test
true length – apparent length

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Perthes’ diseasae
Bryant’s triangle

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Heberden,s nodes

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Swan neck deformity

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Musculo Skeletal Tumors ( MST )
FKUI / RSCM 1995 – 1999 Prof Dr Errol U Hutagalung
Incidence MST : 1.2 % Malignant : 1.3 % Benign : 1 %
Dept. of Pathology FKUI 13.160 cases of neoplasm : 8.718 cases of malignant tumor 4.442 cases of benign tumor .154 cases of MST : .111 cases (72%) malignant . 43 cases (28%) benign January 1995 – December 2004 (10 years periods) FKUI .455 cases - Malignant : 72% ( 327 cases ) - Benign : 28% ( 128 cases ) Mayo Clinic 11.087 cases - Malignant : 77 % - Benign : 23 % USA : 93.000 new cases of Lung Ca /year 88.000 new cases of Breast Ca /year Only 1.500 new cases of Bone Sa WHO (2002) : MST only 0.2% of overall human tumor burden On a numeric basis, Musculo Skeletal Tumors (MST) are uncommon and unimportant. However, many of bone tumor affect young children and are associated with radical surgery, extensive and painful chemotherapy

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
It is universally accepted that the management of patients with MST needs a “TEAM APPROACH” consisted of Orthopedic Surgeon, Pathologist and Radiologist. that works in close cooperation, good communication, Orthopedic Surgeon Pathologist Radiologist. These 3 specialist considered as
the “THREE PILLARS” of the team the setting it is called
the Clinico Pathological Conference ( “CPC” ) of Musculo Skeletal Tumor ( MST ) Diagnosis established in Clinico Pathological Conference (CPC)
Surgical Staging Tumor detected Surgical staging studies Information from clinical and radiological studies surgical staging Surgical Staging SystemEnneking WF Enneking Surgical Staging Benign : Stage 1 : Latent Stage 2 : Active Stage 3 : Aggressive Malignant : Stage I : Low grade A : Intracomp. Stage II : High grade B : Extracomp. Stage III : Meta (+) Procedure FKUI : FNAB as first procedure Literature : accuracy in bone lesions : 70 – 95% FKUI : 79.7% accuracy in Osteosarcoma : 80 – 95% FKUI : 93% FNAB if inconclusive, discrepancy with clinical, radiological studies open biopsy Final diagnosis : C.P.C.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Benign Tumors Accepted treatment methods for benign tumor 1. Curettage : w/wo bone grafting for lesion with cavitary formation such as in GCT, enchondroma, etc. 2. Resection only : osteochondroma; Bone Tumor in expendable bones 3. Resection + reconstruction : GCT stage 2 or 3 4. Sometimes amputation is necessary : GCT stage 3 ++ Osteochondroma
Complain (+) Resection

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Giant Cell Tumor GCT of Bone : 8 years period (1990 – 1997) : 32 cases Demography : Surgical Treatment
Curettage + autograft, allograft, w/wo bone cement
Resection in expendable bones Resection + Reconstruction such as fibular
autograft, allograft, arthrodesis or prosthesis replacement
O+ 31 YEARS Currently : for contaminated surgery in stage 3 post operative adjuvant radiotherapy Literature : - Megavoltage range 40-70 Gy - Follow up average 10 years : recurrences (-), malignant deg. (-)
FFKKUUII.. WWeesstteerrnn SSuunngg LLiitteerraattuurree RRaass CChhiinnaa
SStt 22 3311 %% 7700--8800%% MMaajjoorriittyy
SStt 33 6699 %% 1100--2200%% 77%%
SSeexx MMaallee FFeemmaallee MMaallee

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
PRIMARY MALIGNANT GCT

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Dem ography of D em ograph y o f O steoOsteo Sarcom aS arcom a
FKUIF KUI Literatu reL ite ra ture(M ayo C lin ic)(Ma yo Clin ic)
S exSe x M aleM a le M aleM ale
A geAg e M os tlyM os tly M os tlyM os tlysec on d dec ad es ec ond d ec ade s ec ond d eca desec on d dec ad e
L oc aliza tio nLoc a l iz at ion M os tly a ro und M os tly arou nd M o stly a ro und M os tly arou nd t he k neethe k nee the k neeth e k nee
F req uenc yF reque nc y 31 % 3 1 % 1 9% 19%
S tag eSt age 90 % in S t I I B90 % in S t II B ??10 % in S t I II B10 % in S t III B
Malignant Tumor � Most common : Osteo Sarcoma � 10 years period (1995 – 2004) : 102 cases
OSTEOSARKOMA
Procedure : Clinical, Radiological Fine Needle Aspiration Biopsy (FNAB)
Advantage of FNAB : - Avoid complication of open biopsy - Immediate neoadjuvant therapy
Final diagnosis CPC Surgical Treatment :
Limb ablation for large tumors Limb salvage : - Arthrodesis
- Resection only - Resection + Reconstruction Reconstruction using : - Autograft / Allograft - Prosthesis /Megaprosthesis - Composite Autograft : As alternative due to unavailability of allograft or megaprosthesis For osteoblastic tumors
Technique - Autoclaved - Extracorporeal irradiation (ECI) Autoclaved 1200C – 20’ 1350C – 10’

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
ECI : - Range : 50 – 300 Gy - FKUI / RSCM cases : 100-150 Gy at BATAN (National Atomic Energy) Problems Diagnostic: small number of cases limited experience difficulties in tissue diagnosisunder or over diagnosis Late presentationbenign : stage 3 or 3+ malignant: stage II B or II B+ Funding / education: chemotherapy in complete drop out or refused treatmentalternative Diagnostic CPC can make or break (make a new diagnosis)
Funding / Education: chemotherapy in complete drop out or refused treatment alternative
THREE PILLARS setting of the Clinico Pathological Conference ( CPC ) of MST

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Spinal Cord lesions Anatomy Spinal cord lies within protective covering of vertebral column. Begins just below foramen magnum of the skull. Ends opposite 2nd lumbar vertebra. Below L2 continue as a leash of nerve roots known as cauda
equina. Prolongation of the pia matter forms filum terminale.
Tumors Tumors are classified into 3 types according to their site:
-extradural ( between the meninges and spine bones) -intradural extramedullary (within meninges) -intramedullary ( inside the cord) Spinal tumors Most spinal tumors are extradural – about 85% They may be primary tumors originating in the spine, or secondary
tumors that are the result of the spread of cancer from other locations primarily the lung, breast, prostate, kidney, or thyroid gland.
Any type of tumor may occur in the spine, including lymphoma, leukemic tumors, myeloma, and others. A small percentage of spinal tumors occur within the nerves of the spinal cord itself, most often consisting of ependymomas and other gliomas.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Symptoms of spinal tumors Pain (in 90% of patients), numbness or sensory changes, motor
problems and loss of muscle control. Pain can feel as if it is coming from various parts of the body. Numbness or sensory changes can include decreased skin
sensitivity to temperature and progressive numbness or a loss of sensation, particularly in the legs.
Motor problems and loss of muscle control can include muscle weakness, spasticity (in which the muscles stay stiffly contracted), and impaired bladder and/or bowel control.
17% have Multiple level involvement. Metastatic lesion mostly found in Thoracic spine. Myelopathy develops over days to weeks. Acute SCC does occur if tumor enlarges very rapidly due to
hemorrhage or if a vertebral body suddenly collapses. Extradural tumors The most common spinal tumor – 85% mostly metastatic. Arise from osseous element of spinal column. Grow rapidly. Primary ; Lung, Breast, prostate and kidney. Compress the spinal cord by Growing in epidural space
Causing collapse of vertebrae, distortion and narrowing. e.g. lymphoma, hemangioma and neuroblastoma. Intradural extramedullary tumors Inside the dura but outside the spinal cord. e.g. Meningioma, Neurinoma. Arise from the dural sheath around the cord or showann cell sheath
around the spinal root. Multiple tumors in Pt. with neurofibromatosis. Can grow extradurally into retropleural or retroperitoneal through
intervertebral foramen. Intradural intramedullary tumors Inside the spinal cord
Examples: Glioma, ependymoma, astrocytoma Arise from glial elements of spinal cord or trapped ectodermal
elements. More common in children. Astrocytoma of spinal cord is the most common intramedullary
tumor of childhood.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Ependymoma of spinal cord is the most common intramedullary tumor of adulthood. Arise from ependyma of central canal. Well demarcated.
Investigations Plain X-rays. Myelography “contrast material is injected into the thecal sac fluid
surrounding the spinal cord and nerve root within the spinal canal” CT. MRI ( study of choice ).
Rx spinal tumors The goal of treatment is to reduce or prevent nerve damage from compression of the spinal cord, relieve pain and maintain the function. - Surgical excision is the treatment for extramedullary tumors. - Radiation therapy for intramedullary tumors. The traditional treatment of intramedullary gliomas has been biopsy followed by radiation therapy. Radiotherapy is clearly of value in metastatic lesions. - Chemotherapy can be considered in patients with progression of disease after radiation therapy. Clinical presentation Symptoms vary depending on the cause of the compression, its location, severity, extent and rate of development but can include: - Back pain at the spinal site of compression. - Pain or burning in other parts of the body. - Difficulty breathing. - Weakness in the arms, legs, or both. - Numbness or tingling in the neck, shoulder, arms, hands, or legs. - Loss of coordination or difficulty walking. - Loss of fine motor skills. - Loss of sexual function. - Loss of bladder or bowel control. - Paralysis. - Cervical spine disease produce Quadriplegia. - Thoracic spine disease produce paraplegia. - TENDON REFLEXES
Increase; below level of compression Absent; at the level of compression Normal; above the level of compression

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
- Sphincter disturbances are late feature of cervical and thoracic cord compression. Cauda equina syndrome;
is a serious condition caused by compression of the nerves in the lower portion of the spinal canal . is considered a surgical emergency because if left untreated it can lead to permanent loss of bowel and bladder control and paralysis of the legs. Investigation X ray. CT scan. MRI. Myelogram. Biopsy. Bone scan. Blood and spinal fluid studies.

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Evaluation and Management of Head and Spinal Injuries
Welcome to Trauma! • First and Foremost………ABC’s
airway breathing circulation disability exposure Head Injuries:
• Account for about one half of all trauma deaths • Survivors range from baseline function to severe morbidity • Even “minor” head injury can have severe impact • As with most trauma, broken down into blunt and penetrating
Anatomy for Head Injuries • Scalp
– may result in significant bleeding • Skull
– well placed fractures place vessels and nerves at risk for injury
– protective, but a rigid, fixed space • Dura
– Falx separates hemispheres – Tentorium separates cerebrum
• Brain – Direct (Primary) – Indirect (secondary)
Direct (Primary) Brain Injuries • Direct damage done to brain parenchyma • Damage is already done • Irreversible • Damage control (debridement)
Indirect (Secondary) Brain Injury • Damage that occurs after the initial insult • Expanding mass lesions, swelling or bleeding quickly overwhelm
buffers • End result is increased intracranial pressure (ICP) and/or herniation • Diagnosis and treatments target minimizing the effects of these
indirect insults

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Intracranial Pressure (ICP) • Intracranial space essentially full of brain, blood vessels, and a
little CSF • In response to an insult, small amount of CSF can be displaced, can
decrease blood volume, then increase ICP • At higher ICP, loss of autoregulation occurs • Cerebral perfusion pressure = (MAP-ICP) • Ischemia and neuronal death
Herniation • Other possible result of insult is to displace brain parenchyma itself • Damage to brain from trauma against the dura itself as well as
producing ischemia as well • Uncal herniation classic, but may see others as well
Categories of Brain Injuries • Diffuse
– Concussion (movement to TBI!) – Diffuse Axonal Injury
• Focal – Laceration (blunt) and penetrating – Contusions – Intracerebral hematomas
• Epidural and subdural – Subarachnoid hemorrhage
Diffuse Brain Injuries • Concussion
– “Mild traumatic brain injury” – No significant imaging findings – Does not mean no injury
• Diffuse Axonal Injury – Severe injury globally caused by sheering of axons – Often neurologically devastated
Focal Brain Injuries • Penetrating injuries often intuitively obvious • Contusions (including contrecoup) • Hematomas
– Epidural – Subdural
• Subarachnoid hemorrhage Contusions
• Focal areas of hemorrhage within the parenchyma • Contrecoup injuries occur from a “whiplash” effect of the brain
against the skull on the opposite side of the initial point of impact or injury

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Epidural Hematomas • Blood between inner table of the
skull and the dura • Usually a tear of the MMA • Lens shaped hematomas that do
not cross suture lines on CT • Rare in elderly
Subdural Hematomas
• Blood beneath the dura, overlying the brain and arachnoid, resulting from tears to bridging vessels
• Crescent shaped density that may run length of skull
• Very common in the elderly Subarachnoid hemorrhage
• Subarachnoid blood vessels ruptured • May be the most common finding on moderate to severe brain
injuries Penetrating Brain Injury (GSW) Contusions

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Prehospital Care of Head Injured Patient • Historically, most patients were hyperventilated (bad!) • ABC’s • Spinal immobilization • Initial resuscitation • Rapid transport
Head Injury Management • Management overall goal is to prevent or minimize secondary
injuries to the brain – Prevent hypoxia – Prevent hypotension – Prevent hemorrhage (anemia) – Prevent or limit increasing pressure
ED Assessment of Head Injured Patient • ABC’s (again) • History (think alternate sources) • Clues to brain injury (examples: Cushing’s reflex, raccoon eyes,
etc) • Physical exam – treat prioritized life threats first • The “D” of the ABC’s (neuro exam)
Glasgow Coma Scale (GCS) MOTOR VERBAL EYES
6 follow commands 5 conversant + oriented
4 open spontaneously
5 localizes 4 conversant + disoriented
3 open to command
4 flexion/withdrawal 3 inappropriate words 2 open to pain
3 decorticate post 2 incomprehensible sounds
1 doesn’t open
2 decerebrate post 1 no sounds
1 no movement
GCS 13-15 Mild head injury GCS 9-12 Moderate head injury GCS < 8 Severe head injury

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Management Principles • ABC’s (Get used to it) • Protect spine as well (C spine injury assumed until proved
otherwise) • Stop blood loss elsewhere • Maintain perfusion (why hyperventilation is detrimental!) • Rapid imaging for definitive diagnosis
• Assumes a patient stable enough to go to CT • Early, rapid specialty care
• Neurosurgeons, trauma centers • Temporizing measures
• Hyperventilation • Mannitol • Burr holes
Delayed Problems in Head Injured Patients • Postconcussive Syndrome • Delayed CSF leak • Delayed Seizure
Future of Traumatic Brain Injury • Ongoing efforts at UF and elsewhere to investigate approaches to
minimize damage • Have already debunked what not long ago was good care
(hyperventilation) • Free radical scavengers
C Spine Injuries • Varied mechanisms of injury (flexion, extension, rotation,
distraction, compression, lateral flexion, combination of forces) • Mostly blunt, some penetrating • Spinal cord injury obviously feared, particularly for cervical spine • Range from unstable injuries (ruptured transverse atlantal
ligament) to stable (Clay shoveler’s fracture) Evaluation of C Spine Trauma
• ABC’s (get it yet!) • History • Palpation • Neuro exam
– GCS – Motor – Sensory – Reflexes and tone
Complete vs Incomplete Spinal Cord Injuries • Complete is the total loss of movement and sensation below the
level of injury

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
• Incomplete spares some function • 3 incomplete cord syndromes
– Anterior cord syyndrome – Central cord syndrome – Brown-Sequard syndrome
C Spine Imaging • NEXUS study provided evidence to forego unnecessary x rays • Cross table lateral most useful • Run the “4 lines” of the lateral film • Look for other evidence of injury • Flexion and extension views assess for ligamentous injuries
CT Scan for C spine Injuries • Data shows that x rays miss a significant number of serious injuries • CT is beginning to become the study of choice in many trauma
centers and emergency departments ED Management of C Spine Injuries
• Immobilization • Early neurosurgical of orthopaedic consultation • Steroid protocol for cord injury
– Solumedrol 30 mg/kg bolus followed by infusion 5.4 mg/kg over next 23 hours
– Controversy exists Thoracic and Lumbar Injuries
• Believe it or not, not much more to add beyond C spine discussion in terms of ED care (immobilization, neuro exam, imaging, appropriate consultation, solumedrol protocol for neurologic compromise
• Backboard are a transport device, not definitive immobilization devices (ie, get them off the backboards ASAP)
Neck Trauma • Numerous structures packed in tight space • Blunt vs Penetrating Injuries • Innocuous appearing injuries may quickly become dangerous or
lethal with both blunt and penetrating injuries Death from Neck Trauma
• 1. Associated CNS injury • 2. Hemorrhage • 3. Airway compromise
Blunt Neck Trauma • Difficult to assess • Airway protection a concern for various causes:
– Intrinsic bleeding – Extrinsic bleeding

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
– Tracheal or pharyngeal injury – Aspiration
Blunt Trauma Assessment and Management • Airway protection • CT scan evaluation • Esophagram • Esophagoscopy • Trauma surgeon experience with management
Penetrating Neck Trauma • Old school
– Neck divided into 3 zones – Zone 1 – base of neck to cricoid – Zone 2 - cricoid to angle of mandible – Zone 3 - above angle – If zone 2 and violated platysma, take to OR for exploration;
others get CT, angiography, esophagram, etc • New school
Selective management with imaging rather than OR with zone 2 injuries Take home points
• As always with trauma, ABC’s • Early recognition of injuries, stabilization, and rapid initiation of
definitive treatment will minimize morbidity and reduce mortality • Must rapidly involve or transfer to appropriate trauma surgeons
and or neurosurgeons • Life threats dealt with first

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
COMPLAINTS OF HEADACHE INTRACRANIAL NEOPLASM
• Epidemiology • Risk Factors • Pathophysiology • Classification • Clinical Presentation • Syndromes
Patient concerns…
• How serious are brain tumors? • What can I expect? • How long do I have?
Epidemiology
• Incidence: • 19.1 per 100,000 persons per year
• 11.8/100,000 - symptomatic • 7.3/100,000 – asymptomatic
• Central Brain Tumor Registry of the United States • annual rate: 11.5/100,000
• Primary Brain Tumors: • Astrocytoma 45-50%
» Most common primary intra-axial brain tumor
• Meningioma 15-20% • Pituitary Adenoma 10% • Acoustic Neuroma 8%
• Secondary/Metastatic Brain Tumors: 25-30% of all intracranial tumors
Risk Factors • Ionizing radiation
• only unequivocal risk factor identified for glial and meningeal neoplasms
• Cranial Irradiation (even low doses) – incidence of meningiomas: factor of 10 – incidence of glial tumors: factor of 3 to 7
• latency period: 10 years to >20 years after exposure

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
• No other environmental exposure or behavior has been clearly identified as a risk factor
• conflicting and unconvincing data: • cellular telephones • exposure to high-tension wires • hair dyes • head trauma • dietary exposure to N-nitrosourea compounds or other
nutritional factors • all reported to increase the risk of brain tumors
Clinical Presentation Focal or generalized neurologic symptoms Generalized symptoms/signs
reflect raised ICP include:
1. headache when the illness is severe:
2. Nausea 3. Vomiting 4. CN VI (Abducens) palsy
Focal symptoms/signs reflect intracranial tumor location include:
1. Hemiparesis 2. Aphasia 3. Seizures
the most common presentation of brain tumors is progressive neurologic deficit - 68%
usually motor weakness - 45% rapidly evolving hemiparesis is more typical of a high-grade than a
low-grade glioma Symptom frequency and duration vary with tumor type
Symptoms of Brain Tumors

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Tumor Headache • occurs in about half of all patients with brain tumors • typically diffuse
• can accurately indicate the hemisphere in which the tumor is located
• occasionally unilateral and throbbing • generally more noticeable on awakening in the morning • even without treatment, dissipates within a few hours • can mimic migraine or cluster headaches • often exacerbated by coughing, straining, bending forward • associated nausea and vomiting frequently • Etiologies: • 1. Increased ICP:
• Tumor, hydro, edema, hemorrhage • 2. Invasion or compression of pain sensitive structures
• Dura, vessels, periosteum • 3. Secondary to difficulty with vision • 4. Extreme Hypertension • 5. Psychogenic
Intracranial Pressure • Monroe Kellie Hypothesis:limited space for expansion whitin the
skull • Skull= Brain tissue+Blood+CSF • Increase in any volume IncICP • Compensation (shifting of CSF, increased CSF
absorption,decreased cerebral blood volume) Increased ICP
• Reduced cerebral blood flowischemia • Systemic Response: increased Blood Pressure, slowing pulse,
respiratory irregularity (+ decreases consciousnessCushing Response)
Management of IICP • Prevent hipoxia, ischemia (ABCs), increase intrathoracal( smooth
sucktion) and abdominal pressure (NGT,Urine cathether) • Prevent high metabolic( fever, pain, seizures) • Controlled edema( steroid) • Osmotic diuresis
Seizures • occur at presentation in 15-95% of patients with brain tumors,
depending on tumor type • Typically:

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
• Focal seizures • may become generalized and cause loss of
consciousness • Postictal hemiparesis or aphasia (Todd's phenomenon) may
indicate tumor location Other Symptoms
• Other symptoms that reflect tumor location such as: • Hemiparesis • Aphasia • (when not associated with seizures)
• Typically • subacute onset • progressive
• Exception: Visual-field deficit • may develop progressively • often goes unnoticed by the patient until it contributes
to an accident (frequently an automobile accident) Diagnosis
• MRI – central to the workup of a brain tumor is cranial magnetic resonance imaging
• Computed tomography (CT) • can miss structural lesions • particularly in the posterior fossa, or nonenhancing
tumors such as low-grade gliomas • if a brain tumor is a diagnostic consideration, MRI with gadolinium
enhancement = test of choice • a normal contrast-enhanced MRI scan essentially rules out the
possibility of a brain tumor. Tumors of the Nervous System - Classification
• 1. WHO Classification • 2. Age • 3. Location – Supratentorial, Infratentorial • 4. Cell Type/Histology • 5. Primary vs. Secondary • 6. Benign vs. Malignant • Neoplasms may be classified according to localization and
histological features

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
• Histological classification can be sub-divided according to whether the cells are:
1. Normally present within the cranial or spinal cavity 2. Derived from the skull or spine 3. Represent cells that are not normal components of the central
nervous system, usually representing embryonal components 4. Metastatic from elsewhere in the body
WHO Classification Tumors of the Nervous System • 1. Tumors of Neuroepithelial Tissue • 2. Tumors of Peripheral Nerves • 3. Tumors of the Meninges • 4. Lymphomas and Haemopoietic Neoplasms • 5. Germ Cell Tumors • 6. Tumors of the Sellar Region • 7. Metastatic Tumors
Tumors of Neuroepithelial Tissue WHO GRADING OF ASTROCYTOMAS
n HISTOLOGICAL CRITERIA (4) – anaplasia – increased mitoses – vascular proliferation – tumour necrosis
4 HISTOLOGIC GRADES OF MALIGNANCY Grades I - II : BENIGN Grades III - IV : ANAPLASTIC/MALIGNANT Tumors of Peripheral Nerves WHO Classification Tumors of Peripheral Nerves
• Schwannoma (Neurilemmoma,Neurinoma) • Neurofibroma • Malignant peripheral nerve sheath tumour
Tumors of the Meninges MENINGIOMAS
• Benigns tumor • Meningothelial • Fibrous • Transtitional • Psammomatous • Angiomatous

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
Lymphomas and Haemopoietic Neoplasms • Malignant lymphomas • Plasmacytoma • Granulocytic sarcoma
Germ Cell Tumors • 1. Teratoma • 2. Choriocarcinoma
Tumors of the Sellar Region • 1. Craniopharyngioma Adamantinomatous Papillary • 2. Granular cell tumour • 3. Pituitary adenoma
Metastatic Tumors 25-30% of all intracranial tumours Lung, breast commonest primary sites PEDIATRIC INTRACRANIAL NEOPLASM
• Second most common malignancy • Epidemiology :inc 2-5/100.000 • No sex predominance • Metastatic are very rare
Clinical feature • Often have different patterns of clinical presentations, often a
function of location • I.posterior fossa tumor • II.low grade hemispheric tumord • III.sellar region
Posterior fossa tumors • Signs and symptoms • Headache (morning), nausea, projectile vomiting, drowsiness and
lethargy, diplopia, ataxia, papiledema • Medulloblastoma (25-30%) • Cerebellar astrocytoma (25%)
Management • Similar to adults intracranial neoplasm

Copyright2010@edi ahsani 06
Download Gratis ebook kedokteran, visit http://noteskedokteran.blogspot.com
"Bagaimana Meningkatkan Kehandalan Bahasa Inggris Anda tanpa menghambur-hamburkan rumus Grammar, tanpa Melalui Kursus Yang Mahal dan Membuang Waktu Berharga Anda?"
Download MATERI TANTANGAN GRATIS Full Conversation (audio) + Ebook Kunjungi http://caramudah.net/teguhhandoko/ atau http://klikdisini.com/studyenglish


















