Ika 3 Meningitis
44
MENINGITIS dr. Pertiwi Febriana Chandrawati MSc,SpA
-
Upload
azizah-mutiara-rosdiani -
Category
Documents
-
view
236 -
download
3
description
o
Transcript of Ika 3 Meningitis

MENINGITIS dr. Pertiwi Febriana Chandrawati
MSc,SpA

• Meningitis is an infection of the sheaths that cover the brain and spinal cord. Meningitis is usually caused by an infection with a virus, with a
bacterium or even with fungi.


1. acute pyogenic (bacterial) meningitis 2.acute aseptic (viral) meningitis 3.acute focal suppurative infection (brain
abscess,subdural and extradural empyema) 4.chronic bacterial infection (tuberculosis).

To develop bacterial meningitis, the invading organism must gain access to the subarachnoid space. This is usually via hematogenous spread from the upper respiratory tract where the initial colonization has occurred.
Less frequently, there is direct spread from a contiguous focus (eg, sinusitis, mastoiditis, otitis media) or through an injury, such as a skull fracture. ( direct implantation )

The cell walls of both gram-positive and gram-negative bacteria contain potent triggers of the inflammatory response. In the gram-positive bacteria, teichoic acid is considered the major pathogenic component. In gram-negative bacteria, lipopolysaccharide or endotoxin is the major pathogenic component.

The mediators of the inflammatory response include cytokines (tumor necrosis factor, interleukin 1, 6, 8, 10), platelet activating factor, nitric oxide, prostaglandins, and leukotrienes.
These mediators cause disruption of the blood brain barrier, vasodilation, neuronal toxicity, meningeal inflammation, platelet aggregation, and activation of leukocytes. The capillary endothelial cell is the main site of injury in bacterial meningitis

For both meningitis and encephalitis, the greatest occurrence is in children younger than 4 years with a peak incidence in those aged 3-8 months.
Risk factors for bacterial meningitis Age Low family income Attendance at day care Head trauma Splenectomy Chronic disease Children with facial cellulitis, periorbital
cellulitis, sinusitis, and septic arthritis have an increased risk of meningitis.
Maternal infection and pyrexia at the time of delivery are associated with neonatal meningitis.
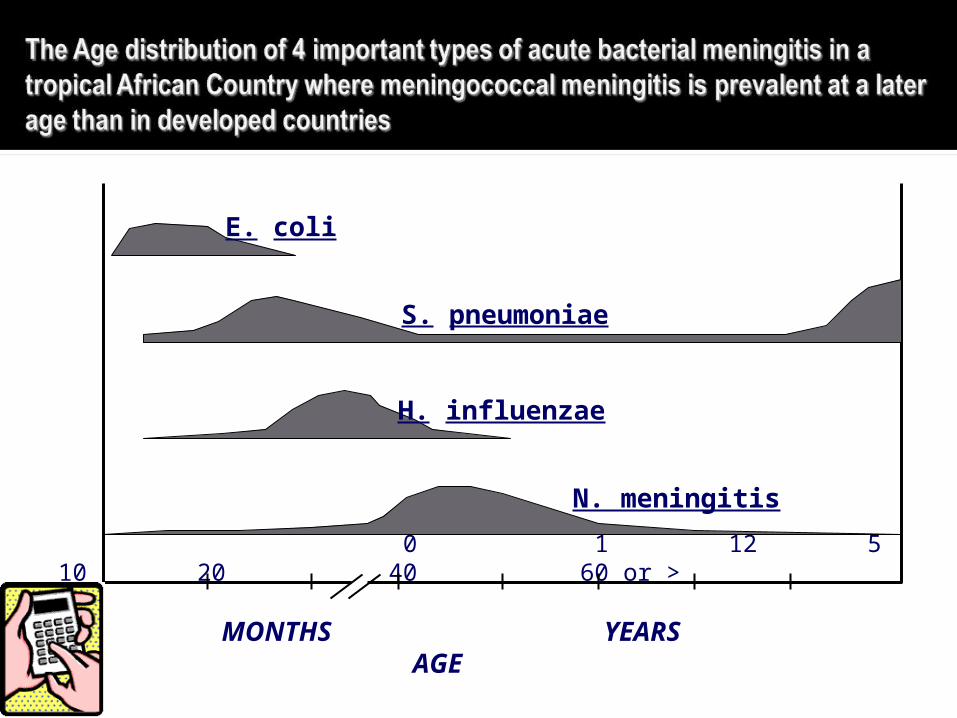
0 1 12 5 10 20 40 60 or >
MONTHS YEARS AGE
E. coli
S. pneumoniae
H. influenzae
N. meningitis


irritability fever sleeping more
than usual poor feeding high-pitched cry
arching back cries when picked
up or being held inconsolable crying bulging fontanelle
(soft spot on an infant's head)
noticeably different temperament

neck and/or back pain
headache sleepiness confusion irritability fever
refusing to eat decreased level of
consciousness seizures photophobia
(sensitivity to light)
nausea and vomiting
neck stiffness




Do not rely on these signs due to low efficacy in pediatrics
Kernig's Sign and Brudzinski's Sign 1. Test Sensitivity: 5% 2. Test Specificity: 95% Nuchal and spinal rigidity 1. Test Sensitivity: 30% 2. Test Specificity: 68% So a high degree of clinical suspicion is
required




White blood cell (WBC) counts over 1000/mm3 usually are caused by bacterial infections.
Gram stain may aid in diagnosis, but the diagnosis may be missed in up to 30% of cases of culture-proven disease.
The protein concentration usually is elevated in bacterial meningitis
Normal CSF glucose should be greater than two-thirds that of the serum glucose. Levels less than 50% of serum are suggestive of bacterial meningitis.

The WBC count in viral meningitis is usually below 500/mm3, with greater than 50% lymphocytes.
The protein may be elevated. The glucose level may be normal or low. Gram stain results are negative.

- Hearing loss is the most encountered sequelae; it occurs * in 30% cases of S. pneumoniae meningitis, * in 20% of H. influenzae meningitis, * in 10% of N. meningitidis meningitis.
- Mental retardation, seizures, delay in language acquisition, visual impairment, behavioural problems and hydrocephalus.
Other serious complications can include:
1. Brain damage
1. Epilepsy
2. Changes in eye sight

Encephalitis is a similar disease of the central nervous system. This disease is an inflammation of brain parenchyma. Often, a viral agent is responsible. Viral entry occurs through hematogenous or neuronal routes.

HSV type 1 and 2 (almost exclusively in neonates), VZV, EBV, measles virus (PIE and SSPE), mumps, and rubella are spread through person-to-person contact.
Mycoplasma speciesRickettsiaToxoplasmosis

Severe headache Sudden fever Drowsiness Vomiting Confusion Seizures

CSF analysis shows pleocytosis (predominantly mononuclear cells) and high levels of protein. A small percentage (3-5%) of samples have normal CSF. Identification of viral antigen or nucleic acid may provide some diagnostic help.


Bacterial meningitis can be treated with a number of effective antibiotics. It is important, however, that treatment be started early in the course of the disease. Appropriate antibiotic treatment of most common types of bacterial meningitis should reduce the risk of dying from meningitis to below reduce the risk of dying from meningitis to below 15%15%, although the risk is higher among the elderly.
Knowing whether meningitis is caused by a virus or a bacterium is important because of differences in the seriousness of the illness and the treatment needed.

1. Antibiotika harus sesuai (2 fase)2. Mempertahankan metabolisme otak3. Pengawasan thd kenaikan tek.
Intrakranial4. Atasi kejang5. Pengelolaan cairan normovolemia
Hipervolemia Dehidrasi
6. Atasi hiperpireksia7. Perawatan meningitis
DIETDIET CAIRCAIR LUNAKLUNAK

1.1. PERAWATAN MENINGITISPERAWATAN MENINGITIS2.2. PENGOBATANPENGOBATAN
a. Homeostasis cairan ivb. Konvulsi / st. konvulsius
Berantas kejang secepatnyaBerantas kejang secepatnyaOksigenasi yang adekuatOksigenasi yang adekuat
c. Kortikosteroidd. Antibiotik

KUMAN OBAT
KOMBINASI
atau
PD. NEONATUS
Ampisilin 200 – 400 mg/kg BB
Kloramfenikol 100 mg/lg BB
Ampisilin 200 – 400 mg/kg BB
Sefurokxim 100 – 200 mg/kg BB
Ampisilin 200 – 400 mg/kg BB
Gentamycin 6 mg/kg BB
I. BELUM ADA HASIL BIAKAN & UJI SENSITIVITAS EMPIRIK

KUMAN OBAT
N. Influensa
S. Pneumonia
N. Meningitis
Gram Negatif
Staphylococus
- Kloramfenikol, ampisilin- Seftriakson, Sefotaksim- Penisilin, Kloramfenikol- Sefuroksim, Seftriakson- Vankomisin- Penisilin, Kloramfenikol- Sefuroksim, Seftriakson- Sebutaksim, Septazidin- Seftriakson, Amikasin- Gentamysin, netilmisin- Nafsilin, Vankomisin- Rifampisin
Arachnoid membraneArachnoid membrane
Choroid plexus epitheliumChoroid plexus epithelium
Endothelial cells dari serebral Endothelial cells dari serebral microvasculaturemicrovasculature
MemisahkanMemisahkan
Intravascular compartment dari otak & cairan Intravascular compartment dari otak & cairan serebro spinalserebro spinal
Akibat pemisahan / peregangan Akibat pemisahan / peregangan intercellular tight junctionsintercellular tight junctions
1. Pada sel endothelial dari cerebral microvasculatur
2. Pada endothel choroid plexus

1.1. Penghambatan sintesis dinding selPenghambatan sintesis dinding sel
Penisilin, Sefalosporin, Vankumisin, Basitrasin, Sikloserin, Penisilin, Sefalosporin, Vankumisin, Basitrasin, Sikloserin, RistosetinRistosetin
2.2. Penghambatan fungsi membran selPenghambatan fungsi membran sel
Amfoterisin B, Kolistin, Polimiksin, Imadazol dllAmfoterisin B, Kolistin, Polimiksin, Imadazol dll3.3. Penghambatan sintesis proteinPenghambatan sintesis protein
Kloram fenikol, Entromisin, Limkomisin, Tetrasiklin, Kloram fenikol, Entromisin, Limkomisin, Tetrasiklin, Aminoglikosid, Amikasin, Neo Strepto, Tobra, NetilmisinAminoglikosid, Amikasin, Neo Strepto, Tobra, Netilmisin
4.4. Penghambatan sintesis asam nukleatPenghambatan sintesis asam nukleat
Asam Nalidiksat, Novobiosin, Rifampin, Sulfonamid, Asam Nalidiksat, Novobiosin, Rifampin, Sulfonamid, TrimetopirinTrimetopirin
1.1. Penghambatan sintesis dinding selPenghambatan sintesis dinding sel
Penisilin, Sefalosporin, Vankumisin, Basitrasin, Sikloserin, Penisilin, Sefalosporin, Vankumisin, Basitrasin, Sikloserin, RistosetinRistosetin
2.2. Penghambatan fungsi membran selPenghambatan fungsi membran sel
Amfoterisin B, Kolistin, Polimiksin, Imadazol dllAmfoterisin B, Kolistin, Polimiksin, Imadazol dll3.3. Penghambatan sintesis proteinPenghambatan sintesis protein
Kloram fenikol, Entromisin, Limkomisin, Tetrasiklin, Kloram fenikol, Entromisin, Limkomisin, Tetrasiklin, Aminoglikosid, Amikasin, Neo Strepto, Tobra, NetilmisinAminoglikosid, Amikasin, Neo Strepto, Tobra, Netilmisin
4.4. Penghambatan sintesis asam nukleatPenghambatan sintesis asam nukleat
Asam Nalidiksat, Novobiosin, Rifampin, Sulfonamid, Asam Nalidiksat, Novobiosin, Rifampin, Sulfonamid, TrimetopirinTrimetopirin

a.a. Pemilihan AB yang tepatPemilihan AB yang tepat
b.b. Cara pemberian & dosisCara pemberian & dosis
Absorbsi, metabolisme, Absorbsi, metabolisme, ekskresiekskresi
a.a. Monitoring & efek sampingMonitoring & efek samping
OUT COMEOUT COME
a.a. Pemilihan AB yang tepatPemilihan AB yang tepat
b.b. Cara pemberian & dosisCara pemberian & dosis
Absorbsi, metabolisme, Absorbsi, metabolisme, ekskresiekskresi
a.a. Monitoring & efek sampingMonitoring & efek samping
OUT COMEOUT COME

TERGANTUNGTERGANTUNG1. Umur2. Jenis kelamin3. Berat ringan infeksi4. Lama sakit seb. Pengobatan5. Kepekaan bakteri thd AB6. Status gizi
SUPORTIFPERAWATAN

Radang selaput otak yang disebabkan oleh Mycobacterium tuberculosis.
Usia 3 bulan sampai 5 tahunMortalitas : 10-20 %
Anamnesis : demam kronis atau akut, penurunan BB, kejang, imunisasi BCG, kontak dengan pasien dewasa.
PD : Stadium I :
gejala gastrointestinal, tanpa kelainan neurologi. apatis, iritabel,nyeri kepala intermiten.
Stadium II : mengantuk,disorientasiRangsang meningeal,refleks tendon meningkat,
abdomen hilang, klonus patela dan pergelangan kaki.N. kranialis VII, IV,VI,III terlibat.
Stadium III :Koma Pupil terfiksasiSpasme kronik
Pernafasan iregulerPeningkatan suhu tubuh Hidrosefalus

CBC LP : - CSF jernih atau xantokrom - sel meningkat 500 sel/mm³ dom
limfosit - Glukosa : menurun PCR ELISA Latex Particle Agglutination CT Scan atau MRI : lesi parenkim dasar otak,
infark, tuberkuloma Ro foto : TB paru.

INH 5-10 mg/kgBB/hari max 300mg/hrRif 10-20 mg/kgBB/hari max 600 mg/hrPZA 20-40 mg/kgBB/hari max 2000
mg/hrEtambutol 15-25 mg/kgBB/hari max
2500mg/hrPrednison 1-2 mg/kgBB/hari, selama 2-
3 mgg, dilanjutkan dg tapp-off.