
iGuide in Conducting an Implementation Review of the ...
69
Transcript of iGuide in Conducting an Implementation Review of the ...

i Guide in Conducting an Implementation Review of the Community Health Service Record System

ii Guide in Conducting an Implementation Review of the Community Health Service Record System
This Guide was made possible by the generous support of the American People through the United States Agency for International Development (USAID). The contents of this Guide are the sole responsibility of RTI International and do not necessarily reflect the views of USAID or the United States Government.
iii Guide in Conducting an Implementation Review of the Community Health Service Record System

iv Guide in Conducting an Implementation Review of the Community Health Service Record System

v Guide in Conducting an Implementation Review of the Community Health Service Record System
Table of Contents
Acknowledgments ..................................................................................................................... vii
List of Acronyms ........................................................................................................................ ix
About This Guide ........................................................................................................................ x
I. Background ....................................................................................................................... 1
II. The Community Health Service Record Implementation Review Process and Tool .......... 3
A. Clarifying the Roles and Tasks of Government Agencies and Partner Nongovernment
Organizations/Community Health Volunteer Groups ............................................................... 3
B. Conduct of Preparatory Activities ..................................................................................... 4
C. Developing/Modifying the CHSR Implementation Review Tools ....................................... 5
D. Actual Conduct of the CHSR Implementation Review Workshop ..................................... 7
III. Next Steps .......................................................................................................................27
References ...............................................................................................................................29
ANNEXES .................................................................................................................................31
Annex A: Sample Activity Design ..............................................................................................33
Annex B: Table of Gaps and Challenges in the CHSR Process and Actions
Taken/Recommendations .........................................................................................................39
Annex C: CHSR Summary Discussion Forum ...........................................................................41
Annex D: CHSR Referral Percentage Contribution Worksheet ..................................................43
Annex E: Good Practice Writing Guide .....................................................................................45
Annex F: Sample Presentation of a Good CHSR Practice - 2016 .............................................47

vi Guide in Conducting an Implementation Review of the Community Health Service Record System

vii Guide in Conducting an Implementation Review of the Community Health Service Record System
Acknowledgments
Sincere gratitude is extended to the following individuals for their invaluable contribution in the development and review of this Guide in Conducting an Implementation Review of the CHSR System and all the tools contained therein: 1. , Regional Director, DOH Regional Office III
2. , Regional Director, DOH Regional Office IV
3. , former Regional Director, DOH Regional Office IV
4. , OIC Regional Director, DOH Regional Office V
5. Head, Family Health Cluster, DOH Regional Office V
6. , Regional FP Nurse Coordinator, DOH Regional Office III
7. , Development Management Officer IV, Provincial DOH Office, Albay
8. , Regional MNCHN Coordinator, DOH-Regional Office IV
9. , Provincial Health Officer II, Nueva Ecija
10. , Provincial Health Officer I, Nueva Ecija
11. , Provincial Health Officer, Tarlac
12. , Provincial Health Officer, Bulacan
13. , Provincial Health Officer, Albay
14. , Provincial BHW Coordinator, Provincial Health Office, Tarlac
15. , City Health Officer, Sta. Rosa CHO I, Sta. Rosa City
16. , City Health Officer, San Carlos City
17. , Municipal Health Officer, San Manuel, Pangasinan

viii Guide in Conducting an Implementation Review of the Community Health Service Record System

ix Guide in Conducting an Implementation Review of the Community Health Service Record System
List of Acronyms
ANC Antenatal Care BHS Barangay Health Station BHW Barangay Health Worker CHD City Health Department CHO City Health Office CHSR Community Health Service Record CHT Community Health Team CHW Community Health Volunteer CPR Contraceptive Prevalence Rate CU Current Users DOH Department of Health DOHRO Department of Health Regional Office DSWD Department of Social Welfare and Development EBF Exclusive Breastfeeding EPI Expanded Program on Immunization FAQs Frequently Asked Questions FBD Facility-Based Delivery FHSIS Field Health Service Information System FIC Fully Immunized Child FP Family Planning HSP Health Service Provider HUP Health Use Plan ICV Informed Choice and Voluntarism IPC Interpersonal Communication IPCC Interpersonal Communication and Counseling KP Kalusugan Pangkalahatan LCE Local Chief Executive LuzonHealth Integrated Maternal, Neonatal, Child Health and Nutrition/Family Planning in the
Philippines MNCHN Maternal, Newborn, Child Health and Nutrition NA New Acceptors NDP Nurse Deployment Project NHTS National Household Targeting System PHN Public Health Nurse PHO Provincial Health Office PIR Program Implementation Review PDO Provincial DOH Office RHM Rural Health Midwife RHU Rural Health Unit RHU-MHC Rural Health Unit Main Health Center RPRH Responsible Parenthood and Reproductive Health SBA Skilled Birth Attendance TB Tuberculosis TCL Target Client List UHC Universal Health Care USAID United States Agency for International Development

x Guide in Conducting an Implementation Review of the Community Health Service Record System

xi Guide in Conducting an Implementation Review of the Community Health Service Record System
About This Guide
This Guide in Conducting an Implementation Review of the Community Health Service Record System describes the workshop process and tools used during a review of the implementation of the Community Health Service Record (CHSR) System. The two-day implementation review workshop aims to assess the status of the implementation of the CHSR System in data collection, recording and reporting by the Community Health Team (CHT) partners/barangay health workers (BWHs). This activity serves as the venue for discussing the contributions, gaps, and sustainability of CHSR in collecting/gathering data from the National Household Targeting System (NHTS)/non-NHTS families to provide quality health services to those found with unmet need for family planning, maternal, newborn, child health and nutrition, and TB (FP/MNCHN/TB). Through house-to-house profiling of household members, all those found with unmet need are identified and immediately referred for utilization of appropriate health services, thus, significantly reducing unmet health needs and resulting in achievement of higher-level health outcomes. For FP, this strategic activity continues to be important at this time when the Department of Health Regional Offices (DOHROs) and Provincial/City Health Offices (P/CHOs) are scaling up FP strategies and activities in response to Executive Order No. 12 (Attaining and Sustaining Zero Unmet Need for Modern FP) issued in January 2017; and to DOH Administrative Order No. 2017-0005 entitled “Achieving the Desired Family Size through Accelerated and Sustained Reduction in Unmet Need for Modern Family Planning Methods.” This guide is intended for the use of the BHW coordinators of the DOHROs and P/CHOs in assessing the use of the CHSR, in coordination with the Regional/Provincial/City/Municipal Program Managers/Coordinators for FP/MNCHN/TB Programs. For health program managers, there is a need for them to provide oversight in ensuring continuous quality improvement in the implementation of health programs; and for the CHSR System, in particular, regular conduct of an Implementation Review is essential to institutionalize a periodic evaluation system to determine the status of demand generation, community referral system, and quality of community-generated data vis-a-vis referral data entries in the Target Client Lists (TCLs) as a support mechanism for improving the implementation of FP/MNCHN/TB Programs. The conduct of this CHSR System Implementation Review had been introduced in 2015 and 2016 by the United States Agency for International Development (USAID) LuzonHealth Project in selected sites that were implementing CHSR, particularly in San Carlos City, San Manuel Municipality in Pangasinan, Santa Rosa City in Laguna, and in the provinces of Tarlac, Nueva Ecija, Bulacan and Albay.. In the conduct of the review, the use of the CHSR Summary and Discussion Form and the CHSR Referral Percentage Contribution Worksheet was introduced. The CHSR Summary and Discussion Form is used during the review of the CHSR notebooks of the BHWs in a barangay health station (BHS) catchment area and the Rural Health Midwives’ (RHMs’) Target Client Lists or Tuberculosis (TB) Registry for the different health conditions (pregnant, postpartum, FP user, under-one year old, TB patients). For a particular recording and reporting period, the Rural Health Unit (RHU) Team checks if the referred patients/FP clients listed in the CHSR notebooks actually went for consultation and received the appropriate services by checking the RHM’s Field Health Service Information System (FHSIS) TCLs for that recording and reporting period.

xii Guide in Conducting an Implementation Review of the Community Health Service Record System
The CHSR Referral Percentage Contribution Worksheet, on the other hand, is used to check the percentage contribution of community health volunteer referrals to the accomplishments for the key FP/MNCHN intermediate indicators – FP current users/new acceptors (CU/NA), ≥4 antenatal care (ANC), skilled birth attendance (SBA), facility-based deliveries (FBD), and fully immunized child (FIC) – at the barangay level, by counting the aggregated referrals made by the community health volunteers from the list of patients/FP clients in the corresponding TCLs of the RHM they refer to. The Program Implementation Review (PIR) workshop results in the different provinces showed a range of percentage contribution of CHT referrals in the FP/MNCHN accomplishments. These two forms were adopted in the conduct of the CHSR Evaluation Study in Tarlac, where all the 18 LGUs (17 municipalities and one city) are implementing the CHSR.
It is hoped that this guide in conducting a CHSR System Implementation Review will be applied periodically in areas where the BHWs continue to use the CHSR as a recording tool for health information, as they profile household members, identify those with unmet need for FP/MNCHN/TB services, and refer and follow them up to access the needed health and FP services.

1 Guide in Conducting an Implementation Review of the Community Health Service Record System
I. Background In 2010, the Aquino Administration launched its Health Sector Reform Agenda called Universal Health Care/Kalusugan Pangkalahatan (UHC/KP) through Department of Health (DOH) Order No. 2010-0036, with focus on poor families. The UHC/KP had three thrusts: financial risk protection for the poor through the expansion of National Health Insurance Program (NHIP) enrollment and benefit delivery; improved access to quality hospitals and health care facilities; and attainment of the health-related Millennium Development Goals (MDGs). The Community Health Team (CHT) System was developed as a critical component of the local implementation of these three UHC/KP thrusts. In each barangay, the CHT was made up of the Management Group that included the barangay captain and the midwife, and its members called the CHT Partners. The CHT Partner may be a barangay health worker (BHW) or a parent leader. In reference to the three UHC/KP three thrusts, the CHTs were expected to: (1) facilitate enrolment to PhilHealth and availment of its benefits; (2) link families to health providers; and (3) transform health needs to effective demand. In 2011, the DOH trained regional teams on the UHC/KP-CHT System. These teams then rolled out the training in the different provinces down to the municipal level nationwide, where CHTs were organized and likewise trained. The CHTs were trained to: look for the poorest families as listed by the Department of Social Welfare and Development (DSWD) through its National Household Targeting System (NHTS); profile the household members to identify those who have unmet need for family planning (FP), maternal, newborn, and child health and nutrition (MNCHN), and TB services; and refer them to nearby health facilities for appropriate health/FP services. Part of the training of the CHT Partners was on the use of the Health Use Plans (HUPs) and the CHT monitoring logbook, for the recording and reporting of health information gathered from the NHTS household members. However, an assessment of CHT operations by the DOH revealed some issues regarding the use of the HUP. For example, the HUPs consisted of too many loose forms that got lost during referrals, and these were costly to reproduce. Also, the key steps taught during training were oftentimes not done completely, specifically the development of HUPs and the follow-up of the referred family members if they actually went back for checkup. In addition, messages were not adequately delivered as taught, the updating of the HUPs and CHT monitoring logbook was not done in some areas, and CHTs were not closely supervised by the rural health midwives (RHMs) in some areas. In 2012, in partnership with the Pangasinan Provincial Health Office, the USAID HealthGov Project introduced the use of the Columnar Notebook in San Carlos City and the municipality of San Manuel in Pangasinan. The use of the Columnar Notebook, an alternative recording tool in place of the HUPs and CHT monitoring logbook, aimed to simplify the recording system for community health volunteers including the CHT Partners and BHWs. During the training, the CHT Partners/BHWs were guided in preparing their own Columnar Notebooks. They were taught how to record health information generated through the profiling of household members in their respective barangays in the household health profile section of the Columnar Notebook, and to accomplish/update the Summary Sheets for the different conditions – prenatal, postpartum, newborn, infant, child, FP current users (CUs), FP non-users, with cough, chronic disease, elderly, adolescent, and others. The instructions on how to fill up the Columnar Notebook are described in detail in the USAID HealthGov Project’s manual, Health Profiling, Recording and Reporting in the CHT System Using the Columnar Notebook: Guide.

2 Guide in Conducting an Implementation Review of the Community Health Service Record System
Starting in 2013, the USAID LuzonHealth Project took over in providing technical assistance on the use of the Columnar Notebook, per request of selected Department of Health Regional Offices (DOHROs), particularly DOHROs III, IV-A and V. By this time, the Columnar Notebook was already called the Community Health Service Record (CHSR). DOHROs III, IV-A and V provided funding for the CHSR region-wide implementation, which included the LuzonHealth provincial project sites. In 2015 and 2016, the provinces of Tarlac, Bulacan and Nueva Ecija in Region III and Albay in Region V, and later the CaLaBaRZon provinces (Region IV), trained their CHT Partners. By this time, the CHT Program had ended, so these provinces shifted to training BHWs on the CHSR. The CHSR has been found to be a useful tool for the BHWs in profiling not only the priority population of NHTS households, but also non-NHTS households, to identify household members with unmet need for FP/MNCHN services and refer them to appropriate health facilities/health service providers for more information, counseling and needed clinical services. In the Province of Tarlac, right from the start, the Provincial Health Office (PHO) decided that all households, NHTS and non-NHTS, would be profiled and visited regularly by the BHWs. From 2015 to 2016, the CHSR became the source of community health information for the DOH-CHT Reporting using the DOH-prescribed reporting forms for Regions IV and V, but there were also areas where the CHSR was just used as a recording tool, as in San Carlos City and San Manuel Municipality in Pangasinan and in Tarlac Province. After two years of CHSR implementation, LuzonHealth provided technical assistance to the PHOs of Pangasinan, Tarlac, Bulacan, Nueva Ecija and Albay and to the CHO of Sta. Rosa City in Laguna in the conduct of a series of CHSR System Implementation Reviews. The activity was designed to review the health information gathered by the BHWs using the CHSR tool and to determine its contribution in improving health service coverage. It also aimed to strengthen the participants’ appreciation of CHSR data and encourage them to utilize the generated information as basis for future actions in improving health service delivery as well as demand-generation strategies. The series of CHSR Implementation reviews conducted surfaced the need for the RHU staff to continue the regular conduct of supportive supervision and monthly meetings to support the BHWs in updating family profiles in the CHSR notebooks for easy tracking of patients/FP clients, including defaulters for the different health services. Also, for the CHSR system to be sustainable, the LGUs need to include in their annual health plans a budget item for the procurement of columnar notebooks with printed headings. During a CHSR Implementation Review conducted for the province of Tarlac in 2016, the
Provincial Health Officer, , shared that the use of the CHSR tool has helped
increase the province’s contraceptive prevalence rate (CPR) from 25 percent to 30 percent and
she attributed this increase to the use of the CHSR in tracking women with unmet need for FP.
3 Guide in Conducting an Implementation Review of the Community Health Service Record System
II. The Community Health Service Record Implementation
Review Process and Tool The CHSR Implementation Review process consists of the following: 1. Clarifying the roles and tasks of government agencies, nongovernment organizations and
community health volunteer groups 2. Conduct of preparatory activities 3. Developing/Modifying the CHSR Implementation Review Tools 4. Actual conduct of the CHSR Implementation Review Workshop
Lecture-presentations
Workshop proper: Group work using the CHSR Implementation Review Tools
Action planning
Synthesis and agreements; next steps for the province/city
A. Clarifying the Roles and Tasks of Government Agencies and Partner
Nongovernment Organizations/Community Health Volunteer Groups Collaboration and support of government agencies, partner nongovernment organizations (NGOs), and the community health volunteer groups (composed of the BHWs) are important factors in the successful implementation of the CHSR System. The agencies and partners involved, along with their roles, are described below. Department of Health Regional Offices
The DOHROs provide oversight in the implementation of the DOH health programs, including the FP/MNCHN Programs. A Regional BHW Coordinator is also assigned to provide regional oversight in the training and organization of community health volunteers including BHWs. The DOHROs are mandated to ensure quality of health services in public health facilities down to the level of the barangay health stations (BHSs), and see to it that BHWs play a vital role in demand generation for patients/FP clients to access and utilize health services. The DOHROs continue to provide oversight to the PHOs/CHOs in the conduct of training and organizing of community health volunteers, including BHWs. The BHW Training Course includes recording and reporting of the BHW accomplishments, and one of the recording tools being used by the BHWs in selected provinces is the CHSR. In 2015 and 2016, DOHROs III, IV and V funded and led the conduct of a Trainers’ Training Course on CHSR Use for their respective PHOs/CHOs with technical assistance from the USAID LuzonHealth Project. DOHRO III procured columnar notebooks for the initial use of the trained CHT Partners/BHWs region-wide. DOHRO IV had the CHSR with its column headings printed in a bigger notebook (15x13 inches) with bigger spaces for the BHWs to write on for all the CaLaBaRZon provinces. DOHRO V adopted this CHSR version and likewise printed copies for all the Bicol provinces. After implementing the use of the CHSR for a few years, DOHROs/Provincial DOH Offices (PDOs) assisted the PHOs/CHOs in selected provinces/cities in the conduct of a CHSR Implementation Review in order to assess the health information gathered by the BHWs using the CHSR tool, and determine its contribution in improving health service coverage.

4 Guide in Conducting an Implementation Review of the Community Health Service Record System
Local Government Units: Provincial/City Health Offices and Rural Health Units The Provincial/City BHW Coordinators provide oversight in the actual training and organization of BHWs by the RHU staff whom they have trained earlier in CHSR use. These Provincial/City BHW Coordinators coordinate closely with the FP/MNCHN Coordinators in tracking health program accomplishments and as a technical team, they conduct monitoring and supportive supervision of health service providers down to the RHU Main Health Center (MHC)/BHS level. At the RHU-MHC/BHS level, they assist the Public Health Nurses (PHNs) and RHMs in identifying and resolving issues and concerns related to demand generation, which include the profiling and follow-up of household members by the BHWs using the CHSR. Hence it is usually the technical team from the PHO/CHO that is in the position to identify the need and readiness of the RHUs to conduct a province-wide or citywide CHSR Implementation Review. Nongovernment Organizations and Community Health Volunteers NGOs can also be tapped to provide technical assistance in the conduct of the CHSR System Implementation Review. On the other hand, the BHW Federation presidents can assist the RHU staff in ensuring that all the active BHWs participate as community health volunteers in the CHSR training and in the CHSR System Implementation Review Workshops.
B. Conduct of Preparatory Activities As mentioned, the PHO/CHO technical staff are the ones who usually determine the need to conduct a CHSR System Implementation Review, considering that they work closely with the RHUs in implementing the different health programs. Once the need to conduct a CHSR Implementation Review has been determined, the Provincial/City BHW Coordinator, together with the Provincial/City FP/MNCHN Program Coordinators, then form themselves into a Team of Facilitators to plan out the conduct of the two-day CHSR Implementation Review Workshop. They can also ask for technical assistance from the DOHRO/PDO. During the team’s initial meeting, they can identify the preparatory activities that have to be done, and spell out the roles and responsibilities or task assignments among themselves, to include the following: 1. Review the CHSR Implementation Review tools that had been developed by the LuzonHealth
Project as a technical assistance to its LGU partners, and decide if there is a need to make modifications on the tools based on their needs for such revisions.
2. Identify the FP/MNCHN indicators that they think should be included in the review of CHSR
and Target Client Lists (TCLs) during the CHSR Implementation Review Workshop. The Senior PHN from each of the RHUs will be requested to prepare and bring with him/her to the workshop the needed FHSIS data, particularly for the selected BHS/barangay for the current and previous year, disaggregated by quarter/month. This request should be included in the invitation letter to the Municipal Mayor/Municipal Health Officer.
3. Identify the participants to the CHSR Implementation Review Workshop. The Team of
Facilitators shall have to decide if they will just invite one team composed of the MHO/Senior PHN, the FP/MNCHN Nurse Coordinator, one RHM, one Nurse Deployment Program (NDP)

5 Guide in Conducting an Implementation Review of the Community Health Service Record System
nurse, and two BHWs from one BHS per municipality; or if they will conduct the workshop in two batches to accommodate more participants from one municipality per batch. It is important to request the RHM and NDP nurse of the selected BHS to bring with them their TCLs for FP, prenatal care, postpartum care, and EPI/nutrition, and TB registry for the current and previous year; while the BHWs should bring with them their CHSR notebooks for the current and previous years. The RHM will also be requested to bring with her the CHSR notebooks of the rest of the BHWs in her BHS catchment area for the current and previous year, for their RHU team to generate the overall CHSR referral contribution for their selected BHS catchment area.
Because of time constraints during the workshop, the team may decide to just assign the RHUs by district what to bring with them when they attend the workshop. For example, the RHUs in District 1 will be assigned to bring TCLs for FP while the RHUs in District 2 will have to bring TCLs for prenatal care and postpartum care, and so on. All these instructions should be included in the invitation letters.
4. Prepare the Activity Design and Program for the two-day CHSR Implementation Review
Workshop. (Refer to Annex A for a sample Activity Design.) 5. Compute the needed budget, including sources (DOHRO, P/CHO, Municipal LGU, NGO) 6. Identify the dates of the activity and the workshop venue. 7. Arrange for the venue, accommodations, and meals/snacks. 8. Prepare and send out the invitation letters. 9. Prepare the needed workshop materials. The Facilitators’ Team should conduct at least two meetings as necessary to work on the preparatory tasks listed here, starting about a month prior to the workshop, to ensure that the invited participants are available during the scheduled dates of the activity. The last meeting should be conducted at least one week prior to the scheduled dates of the workshop, to give the Facilitators’ Team the opportunity to check if all the preparatory tasks have been accomplished. By this time the invitation letters with instructions on what to bring to the workshop should have all been sent out and the participants asked to confirm their participation. The Activity Design, the CHSR Implementation Review tools, and the slide presentations for the workshop inputs should have been finalized. Arrangements with the venue and accommodations should have likewise been completed and workshop materials ready for the activity. The Facilitators’ Team should then go over the final Program of Activities, for their roles and assignments during the actual conduct of the workshop.
C. Developing/Modifying the CHSR Implementation Review Tools
The CHSR Implementation Review tools had been developed by LuzonHealth, and were presented for review and discussion to the PHO/CHO technical team during the Facilitators’ Meeting prior to the conduct of the CHSR Implementation Review Workshops in the provinces and cities implementing CHSR use. The Team of Facilitators may decide to do modifications on these tools as they deem necessary when they conduct the activity.

6 Guide in Conducting an Implementation Review of the Community Health Service Record System
These tools include the following: 1. Table of Gaps and Challenges in the CHSR Process and Actions Taken/
Recommendations – A copy of this table is sent out to the Senior PHN together with the invitation letter so that he/she can already share it with the RHU team (including the BHWS) for them to discuss the gaps and challenges that they have encountered in the implementation of the CHSR, as well as the actions they have taken, or recommendations that they would like to take up to further improve the CHSR System implementation in their municipality. Having them discuss these and fill up the table beforehand would cut short the time spent filling up this table during the actual workshop. (Refer to Annex B for a copy of this table.)
2. CHSR Summary Discussion Form – This form is used by the RHM and the BHWs
assigned in her catchment area to review the names of referred patients/FP clients in the CHSR notebooks for the different health conditions (pregnant, postpartum, FP user, under-one year of age) for a particular reporting period. They will verify if the patients/FP clients actually went for consultation and received the appropriate services by checking against the FHSIS Target Client Lists of the RHM for that reporting period, and record the findings in the appropriate column of the CHSR Summary Discussion Form. The names of clients needing follow-up are also noted down in the CHSR notebooks of the community health volunteers. (Refer to Annex C for a copy of the CHSR Summary Discussion Form.)
This process when adopted by the RHU Teams during the monthly meetings among the RHM, NDP Nurses and BHWs helps ensure that those identified with unmet need for FP and MNCHN services and were referred to health service providers are actually provided with the needed services, or are followed up by the BHWs in their homes to remind them to go back to the health facility for the needed services. This process also helps ensure that the TCLs of the RHM and the CHSRs of the BHWs are regularly updated. The process likewise contributes to improving the quality of the reported FHSIS data from the BHS level.
3. CHSR Referral Percentage Contribution Worksheet – This worksheet is used to check
the percentage contribution of community health volunteer referrals to the accomplishments for the key FP/MNCHN intermediate indicators – FP current users/new acceptors (CU/NA), ≥4 antenatal care (ANC), skilled birth attendance (SBA), facility-based deliveries (FBD), and fully immunized child (FIC) – at the barangay level, by counting the aggregated referrals made by the community health volunteers from the list of patients/FP clients in the corresponding TCLs of the RHM they refer to. During the Program Implementation Review (PIR) Workshop that LuzonHealth conducted in the provinces and cities using CHSR, trends in the FP/MNCHN accomplishments relative to CHSR referral contribution were also analyzed. The results in the different provinces showed a range of percentage contribution of CHT referrals in the FP/MNCHN accomplishments. (Refer to Annex D for a copy of the CHSR Referral Percentage Contribution Worksheet.)
4. Good Practice Writing Guide – In a group work, the RHU Teams are asked to choose
one of their CHSR good practices and write a brief description on Manila paper, following the Good Practice Writing Guide. (Refer to Annex E for a copy of the Good Practice Writing Guide.)

7 Guide in Conducting an Implementation Review of the Community Health Service Record System
D. Actual Conduct of the CHSR Implementation Review Workshop The general objective of the activity is to review the health information gathered by the BHWs using the CHSR tools and how these contributed to improving health service delivery among the NHTS and non-NHTS population. The activity processes are expected to strengthen the appreciation of the CHSR data and assist local health implementers in using the health information generated from the CHSR as the basis for next actions in improving health service delivery to NHTS and non-NHTS families. Specifically, the activity aims to:
a. Identify the gaps and challenges at every step of the CHSR process. b. Review data generated from the CHSR tools. c. Discuss BHW action points and validate the content of the CHSR records with the TCLs. d. Present the contributions of BHW deployment and CHSR data in improving health
service delivery to NHTS families; present as well as the contributions of BHWs using the CHSR in improving health service delivery to non-NHTS families.
e. Identify gains and gaps in the implementation of CHSR. f. Develop Provincial/City/Municipal Action Plans to strengthen the CHSR implementation.
The following are the expected outputs:
a. List of gaps and challenges, including actions taken and/or recommendations made to address these.
b. CHSR records and reports validated with the TCLs. c. List of contributions of BHW participation and CHSR data in improving health service
delivery to NHTS and non-NHTS families. d. P/CHO and RHU/BHS Action Plans on CHSR based on the identified gains and gaps.
Different methodologies will be employed during the activity, including: workshops, small group discussion, gallery and plenary presentations.
1. Lecture Presentations
After the preliminary activities on the first day, the participants are oriented on the workshop activities for them to have an idea of what to expect during the two-day activity. This can be done through a brief slide presentation and a walk-through the Program of Activities. Other slide presentations provided during the morning session include the following:
Presentation of Status of CHSR Implementation in the Province/City – The Provincial/City BHW Coordinator is usually asked to present and discuss this topic.
Monitoring and Supportive Supervision for CHSR – This is a discussion of the definitions of monitoring and supportive supervision, and who are responsible for conducting these at the RHU-MHC and BHS level, particularly for the BHWs at the community level on the CHSR System.
Ensuring Quality Data for the CHSR System at the Barangay Level – This is a discussion of the desirable attributes of health data – which include completeness, accuracy, reliability/consistency, and timeliness of recording and reporting of health data

8 Guide in Conducting an Implementation Review of the Community Health Service Record System
– and how these attributes are applied to health data/information generated by the BHWs and are recorded in their CHSR notebooks and reported to the RHM.
Orientation on Informed Choice and Voluntarism (ICV) – Since the BHWs are tasked to
profile and refer women of reproductive age identified to have unmet need for FP, then it is important that they are also aware of the principles of ICV.
2. Workshop Proper: Group Work Using the CHSR System Implementation
Review Tools Workshop Introduction – In the afternoon of the first day of the CHSR System Implementation Review, the workshop proper is introduced by one of the facilitators through a brief review of the CHSR implementation process. (See Figure 1 below.)
Figure 1. Improving the BHW Recording System through the CHSR (Adapted from the 2013 LuzonHealth Project CHT process presentation).
The assigned facilitator for Workshop 1 then explains the objective of the workshop, which is the refinement and enhancement of the pre-workshop output conducted at the RHU/BHS/community level to identify gaps and challenges as well as actions/recommendations. It has been mentioned in Part II Section B (Conduct of Preparatory Activities) above that a copy of this table is sent out to the Senior PHN prior to the workshop so that the RHU team can already accomplish it before they attend the workshop. (Refer to Annex B for a copy of this table.) During the actual workshop, the participants group themselves by RHU Teams, and each group are tasked to review and enhance their respective table outputs. The results are then written on Manila paper and presented by the team’s reporter in a gallery setup. The reporters are requested not to repeat anymore issues and concerns that have already been reported by the

9 Guide in Conducting an Implementation Review of the Community Health Service Record System
other groups, but they may still present the actions they have taken or recommendations they have formulated in response to those issues, so that the other groups may consider adopting them. At the end of the presentations and discussions, the different RHU Teams are advised to make use of their respective Workshop 1 outputs as their reference when they prepare their CHSR Action Plans in the afternoon of Day 2. The Workshop 1 outputs are then summarized by the facilitators, as shown in the sample accomplished Table 1 below. Table 1. Sample Accomplished Form: Summary of Gaps and Challenges of CHSR Implementation
in San Carlos City, Pangasinan
CHSR Task Gaps and Challenges Encountered by Action
Taken/Recommendation
1. Preparation of the CHSR Notebook
Identification and numbering of HHs
Group 1 List catchment NHTS (sorting) by purok
Unavailability/lack/delayed arrival of materials/supplies, e.g. heading, stickers, scissors, paste, art paper, plastic cover
1, 2 Availability, resourcefulness and creativity
Delayed arrival of the tools 1, 2 Shoulder own expenses in providing necessary supplies for CHSR tool
Preparation of the headings is tedious and time-consuming
3 Printed heading on the CHSR
Labeling 4 Familiarity with the different labels
Narrow spaces on the columnar
4 Improvement of the columnar
Provide bigger and better CHSR tool
Inadequate supplies (e.g., headings, notebook)
5 Provided through Xerox copy; hand written
Provision of columnar for NHTS and non-NHTS and key messages
2. Conducting the Profiling
2.1 Locating NHTS HHs
Long walking distance 1 Clustering per purok
NPA 2 Proper endorsement
Scattered purok catchment; Distance from one house to another; The target NHTS are not located on the same purok as where the CHT partner resides; Distant from CHT partner
2, 3, 5 Team work
Assign the CHT to their own purok
Provide fixed schedule, get contact number and other social network
Not familiar with some catchment facilities
4 House to house
Transferred to another place 5 Communicate with neighborhood
No person around; 1, 2, 3 Revisit, inform immediate

10 Guide in Conducting an Implementation Review of the Community Health Service Record System
CHSR Task Gaps and Challenges Encountered by Action
Taken/Recommendation
2.2 Conducting the Interviews
Availability of family during HH visit; Parents/adult guardians are not present during interview
relatives
Set an appointment with the parent
Respondent not familiar with birthdays (personal data)
1 Validation
Some mothers are hesitant to answer truthfully
2
Lack of understanding regarding questions given
4 Further explanation
Conflict in schedule 5 Set the interview for next schedule
2.3 Recording of Information in CHSR
Computation of age/month 1 Use of calculator
Wrong information on birthdates; Inconsistency of data gathered; Incomplete and inaccurate data
2, 4, 5 Ask for birth certificates
Validation
Inadequate space for some data/information
3 Additional paper/notebook
2.4 Delivering of Key Health Messages
Difficulty in convincing client to seek health services (FP, EPI, prenatal, etc.)
1 Explained the importance of the health services and programs
Clients are inattentive during the delivery of key health services
3 Set time when client is available and ready to listen
Some facilities are doubting the capacity of the CHT in delivering the health messages
4 Continue on convincing them by presenting more information
Lack of knowledge and skills on some programs
5 Set up meeting
3. Consolidating the different conditions
Availability of information needed; Inadequate information; CHT is not available; Incomplete data
1, 3, 5 Collect sufficient data
Revisit and validation of information
Data quality check (TCL)
Availability of the partner 4 Planning ahead of time
4. Referring Clients
For patients with cough for more than 2 weeks, “social stigma”; Stereotype
1, 4 Reassurance
Accompany them to RHU
Assurance of confidentiality
Denial of clients health condition
2 Proper information dissemination
Embarrassment of client; Hesitation, uncomfortable
2, 5 Build rapport and trust
Clients referred to a health facility do not go/seek consultation, giving different alibis (e.g.,. no time, no money); No feedback mechanism
3 Accompany clients to the health facility
Follow up/revisit
Home visit

11 Guide in Conducting an Implementation Review of the Community Health Service Record System
CHSR Task Gaps and Challenges Encountered by Action
Taken/Recommendation
5. Following up of Clients
5.1 Who have not consulted HSP
Attitude of clients; Hard-headed and lazy clients (low health seeking behavior); Attitude towards health services
1, 3, 4 Health education/encouragement
Home visit together with midwife and NDP
Give extra time and effort
Informed clients pero nakakalimutan na (attitude problem)
1 Home visit
Availability of time/conflict in schedule
5 Explain to them the possible untoward signs and symptoms
5.2 Given health services
Unable to come back on scheduled visit (e.g., AP, FP, EPI, NTP, PP); Failure to return on the scheduled follow-up/checkup
1, 3, 4 Home visit together with midwife and NDP;
Follow-up/home visit
Depends on their beliefs Explain the benefits of the services
6. Reporting to the Midwife
6.1 Validation of CHSR data
Trans-in/out patients 1 Close monitoring/follow-up
Lack of data of reports; Incomplete data
2, 3, 5 Reported upon schedule
CART; timely and accurate;
Completion of data before reporting to RHM
Follow-up
Not updated data/CHSR; Inadequate data and inconsistency of reports
3, 4, 5 Early monitoring
Gather reports through text gathering the reports during their duty
Proper validation and consolidation
Sometimes other CHTs are not around during reporting period
4 Constant reminder through text or during their duty
7. Reporting to the PHN and P/CHO
Some data are not updated 1 CART
Late submission of reports 3 Giving early reminder setting deadline
Accuracy and reliability on time reporting
4 Setting time for submission and checking reports with CHT’s
Early detection of RHM rather than CHTs
5 Close monitoring and follow-up
8. Reporting to the DOH (NDPs/DMOs)
Insufficient data gathered (some CHT partners not around)
1 Follow-up
Validation
Late reporting 3, 5 Setting of early deadline
9. Other tasks

12 Guide in Conducting an Implementation Review of the Community Health Service Record System
For Workshop 2, the facilitator assigned to handle the session also explains the objective of the workshop, and the workshop process and steps. This involves the review of health indicators by condition generated from the CHSR notebook using the CHSR Summary and Discussion Form. (Refer to Annex C for a copy of the CHSR Summary Discussion Form.) The facilitator instructs the participants to group themselves again by RHU Teams and presents the CHSR Summary and Discussion Form when everyone has been given a copy. The facilitator explains that in the invitation letter to the participants, they had been requested to bring with them the BHWs’ CHSRs for a barangay or for an entire BHS, along with the RHM’s TCLs for the assigned health condition (pregnant, postpartum, FP user, under-one year of age, and suspected TB patient). This means that, due to time constraints, during this workshop, one RHU Team works on just one assigned health condition instead of conducting the records review for all the FP/MNCHN indicators. The participants also decide on the time coverage of the review (e.g., the past four quarters or the past 12 months) depending on the available updated health data in the CHSRs and TCLs the RHU Teams brought with them. If an RHU Team has BHW representatives from just one barangay who have with them all the CHSRs of all the BHWs assigned in their area, then the RHU Team will have to review all the CHSR notebooks of all the BHWs assigned in this barangay, and the corresponding TCL of the RHM for this barangay, for the health condition assigned to the RHU Team to review. If the BHS has two or more barangays represented in the workshop, then the CHSR notebooks of all the BHWs in these barangays are likewise reviewed along with the RHM’s corresponding TCLs for these barangays for the condition assigned to them. The CHSRs of the BHWs in the barangay/s who are not present should be included in the review, for each RHU Team to generate a more complete CHSR referral picture for their selected barangay/BHS. One can recall that in the preparation of the invitation letters for this activity, the RHM from the selected BHS was asked to also bring with her the CHSR notebooks of the BHWs not participating in the workshop. The next instruction to the participants is on what to review in the CHSRs and TCLs. Using the CHSR Summary and Discussion Form, the RHU Team reviews the names of referred patients/FP clients in the CHSR notebooks for the different health conditions (pregnant, postpartum, FP user, under-one year of age) for a particular reporting period, and verifies if those referred actually went for consultation and received the appropriate services. This is done by checking the TCLs of the RHM for that reporting period. The findings are then recorded in the appropriate column of the CHSR Summary Discussion Form. The number of patients/FP clients needing follow-up is then recorded in the CHSR Summary Discussion Form, but the names of these clients are written in the CHSR notebooks of the BHWs for their actual follow-up. A records review for just one health condition for the past four recording quarters takes just about 10 to 15 minutes per RHU Team to complete for each health indicator during Workshop 2. So, the take-home message for the participants is that it is very feasible to conduct such a records review using the same tool during the monthly meetings among the RHM, NDP Nurse, and BHWs – such a small amount of time to help ensure that their CHSR notebooks and TCLs are regularly updated, contributing to improved quality of the reported health data from the BHS level. More importantly, those identified with unmet need for FP and MNCHN services who were referred to health service providers are actually provided with the needed services, or are followed up by the BHWs in their homes to be reminded to go back to the health facility for the needed services.

13 Guide in Conducting an Implementation Review of the Community Health Service Record System
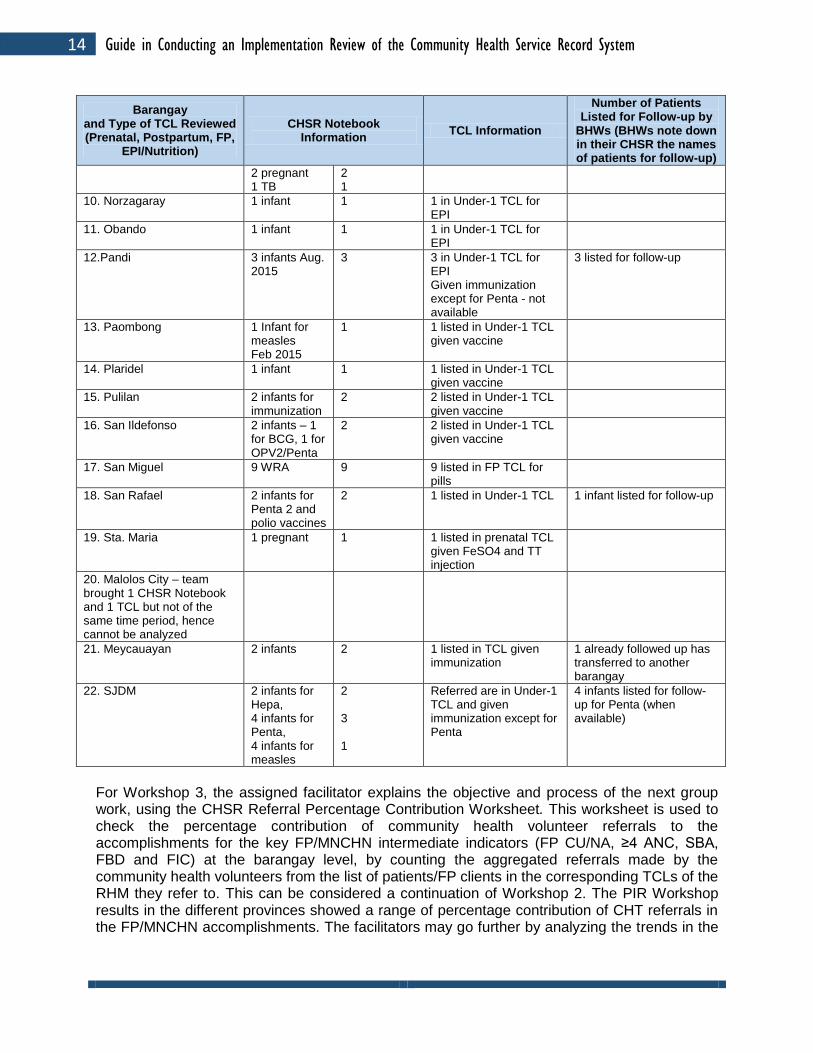
The workshop process gives the participants a feel of how feasible it is to conduct the review process in their respective areas. The RHU Team can refer again to Annex C for a copy of the CHSR Summary Discussion Form that they can use for the monthly meetings of the RHM, NDP Nurses and the BHWs to review their records. A sample accomplished CHSR Summary Discussion Form, consolidated for the participating municipalities of Bulacan, is shown in Table 2. For the one-hour workshop for Bulacan, the CHSR of one BHW from one barangay and the RHM’s TCL were reviewed for one health condition per municipality.
Table 2. Sample Accomplished CHSR Summary Discussion Form, Consolidated for Bulacan Province
Community Health Team/Community Health Service Record (CHSR) System
Name of Facility (BHS): Consolidation for Bulacan Province Address: _________________________ Name of RHM: _______________________________ Date of Activity: _________________________ Names of BHWs/Barangay: ______________________________________________________________ _____________________________________________________________________________________ Note: Use 1 form for each type of TCL reviewed. DISCUSSION RESULTS COMPARING CHSR DATA WITH TCL ENTRIES USING THE CHSR SUMMARY AND DISCUSSION TOOL:
Barangay and Type of TCL Reviewed (Prenatal, Postpartum, FP,
EPI/Nutrition)
CHSR Notebook Information
TCL Information
Number of Patients Listed for Follow-up by
BHWs (BHWs note down in their CHSR the names of patients for follow-up)
Note: The CHSR of 1 BHW from 1 barangay and the RHM’s TCL were reviewed for 1 health condition per municipality.
Seen Referred Number of Referred and Given Services and Recorded in TCL of services given
1. Angat 2 PP (postpartum)
2 PP 2 in PP TCL 0
2. Balagtas 2 NB (newborn) Sept. 2014
2 NB 2 in Under-1 TCL 2 for scheduled follow-up
3. Bocaue 1 PP Aug. 2015
1 PP 1 in PP TCL
4. Baliwag 5 suspect TB 5; 2 patients refused consultation
3 examined, 2 positive; now in TB Registry
2 for follow-up for referral
5. Bustos 1 infant 1 infant 1 in Under-1 TCL for EPI
6. Calumpit 1 infant out of 13
1 1 in Under-1 TCL
7. Guguinto 1 infant 1 1 in Under-1 TCL for EPI
For scheduled follow-up
8. Hagonoy (Best RHU) 1 infant for Penta 3 and OPV - July 2015
1 1 in Under-1 TCL for EPI
9. Marilao 4 NB for BCG; 4 infants, 4 of 18 children for MMR;
4 4 4
All in TCLs
14 Guide in Conducting an Implementation Review of the Community Health Service Record System
Barangay and Type of TCL Reviewed (Prenatal, Postpartum, FP,
EPI/Nutrition)
CHSR Notebook Information
TCL Information
Number of Patients Listed for Follow-up by
BHWs (BHWs note down in their CHSR the names of patients for follow-up)
2 pregnant 1 TB
2 1
10. Norzagaray 1 infant 1 1 in Under-1 TCL for EPI
11. Obando 1 infant 1 1 in Under-1 TCL for EPI
12.Pandi 3 infants Aug. 2015
3 3 in Under-1 TCL for EPI Given immunization except for Penta - not available
3 listed for follow-up
13. Paombong 1 Infant for measles Feb 2015
1 1 listed in Under-1 TCL given vaccine
14. Plaridel 1 infant 1 1 listed in Under-1 TCL given vaccine
15. Pulilan 2 infants for immunization
2 2 listed in Under-1 TCL given vaccine
16. San Ildefonso 2 infants – 1 for BCG, 1 for OPV2/Penta
2 2 listed in Under-1 TCL given vaccine
17. San Miguel 9 WRA 9 9 listed in FP TCL for pills
18. San Rafael 2 infants for Penta 2 and polio vaccines
2 1 listed in Under-1 TCL 1 infant listed for follow-up
19. Sta. Maria 1 pregnant 1 1 listed in prenatal TCL given FeSO4 and TT injection
20. Malolos City – team brought 1 CHSR Notebook and 1 TCL but not of the same time period, hence cannot be analyzed
21. Meycauayan 2 infants 2 1 listed in TCL given immunization
1 already followed up has transferred to another barangay
22. SJDM 2 infants for Hepa, 4 infants for Penta, 4 infants for measles
2 3 1
Referred are in Under-1 TCL and given immunization except for Penta
4 infants listed for follow-up for Penta (when available)
For Workshop 3, the assigned facilitator explains the objective and process of the next group work, using the CHSR Referral Percentage Contribution Worksheet. This worksheet is used to check the percentage contribution of community health volunteer referrals to the accomplishments for the key FP/MNCHN intermediate indicators (FP CU/NA, ≥4 ANC, SBA, FBD and FIC) at the barangay level, by counting the aggregated referrals made by the community health volunteers from the list of patients/FP clients in the corresponding TCLs of the RHM they refer to. This can be considered a continuation of Workshop 2. The PIR Workshop results in the different provinces showed a range of percentage contribution of CHT referrals in the FP/MNCHN accomplishments. The facilitators may go further by analyzing the trends in the

15 Guide in Conducting an Implementation Review of the Community Health Service Record System
FP/MNCHN accomplishments relative to CHSR referral contribution. (Refer to Annex D for a copy of the CHSR Referral Percentage Contribution Worksheet.) A sample consolidation of the accomplished CHSR Referral Percentage Contribution Worksheets for the participating municipalities of Tarlac is presented in Table 3. An RHU Team was assigned to work on one FP/MNCHN indicator. The numerators are the number of patients/FP clients who were profiled and referred by the BHWs to the BHS using their CHSR notebooks, while the denominators represent the total number of patients/FP clients counted from the TCLs of the RHM. Most of the RHU Teams got a rating of “very significant”, which means at least 30% of the BHS accomplishments were referrals from the BHWs using the CHSR.

16 Guide in Conducting an Implementation Review of the Community Health Service Record System
Table 3. Consolidated CHSR Implementation Review Workshop Results Using the CHSR Referral Percentage Contribution Worksheet, for 1 Midwife CHSR Team, by City/Municipality for 2015
Tarlac Province
City/Municipality/Barangay
Documents Reviewed by the Midwife CHSR
Team (TCLs and CHSRs)
% Contribution of CHSR Referrals to Service
Delivery Accomplishments for Key FP/MNCHN Indicators
RATING 1. Very Significant (VS) = 30% or more; 2. Significant (S) = 10 to 29% 3. Needs Improvement = <10%
Jan-March 2015
April-June 2015
July-Sept. 2015
Oct-Dec. 2015
1. Tarlac City Quarterly FPNA Accomplishments 2015
120 / 132 (91%)
60 / 143 (42%)
40 / 158 (25%)
10 / 170 (6%)
NI / S / VS
2. Pura RHU – Barangays Linao and Sinat
Quarterly SBA and FBD Accomplishments 2015
9/14 (64%)
9/9 (100%)
9/20 (45%)
9/14 (64%)
VS
3. La Paz RHU – Barangay San Roque
Quarterly FPCU Accomplishments 2015
117 / 263 (44%)
104 / 232 (45%)
117 / 261 (45%)
127 / 276 (46%)
VS
4. Santa Ignacia RHU – Barangays Poblacion East, Poblacion West, Pilipili, Nambalan, Diego Cecilio
Quarterly FIC Accomplishments 2015
38 / 44 (86%)
50 / 56 (89%)
48 / 53 (90%)
74 / 78 (95%)
VS
5. Moncada RHU – Barangays San Julian and Sta. Maria
Quarterly FIC Accomplishments 2015
7 / 7 (100%)
7 / 7 (100%)
5 / 5 (100%)
5 / 5 (100%)
VS
6. Gerona RHU – Barangay Abagon Quarterly SBA Accomplishments 2015
12 / 12 (100%)
15 / 16 (93%)
24 / 26% (92%)
19 /21 (90%)
VS
7.Victoria RHU – Barangay Canarem Quarterly SBA and FBD Accomplishments 2015
11/ 14 (79%)
4 / 6 (66%)
12 / 13 (92%)
7 / 8 (88%)
VS
8. Paniqui RHU – Barangay Aduas Quarterly 4ANC Accomplishments 2015
9 / 9 (100%
8 / 8 (100%)
10 / 15 (67%)
9 / 9
(100%)
VS
9. Ramos RHU – Barangay Guiteb Quarterly 4ANC 7 / 9 6 / 7 21 / 23 16 / 17 VS

17 Guide in Conducting an Implementation Review of the Community Health Service Record System
Accomplishments 2015
(78%) (86%) (91%) (94%)
10. San Jose RHU – Barangay Sula Quarterly EBF Accomplishments 2015
19 / 25 (75%)
19 / 25 (75%)
19 / 25 (75%)
19 / 25 (75%)
VS
Quarterly FIC Accomplishments 2015
46 / 61 (75%)
46 / 61 (75%)
46 / 61 (75%)
46 / 61 (75%)
VS
12. Concepcion RHU – Barangay San Jose
Quarterly SBA Accomplishments 2015
28 / 65 (43%)
0 / 58 (0%)
7 / 64 (11%)
28 / 69 (40%)
S
Quarterly FBD Accomplishments 2015
28 / 58 (48%)
0 / 53 (0%)
7 / 58 (12%)
28 / 63 (44%)
S
13. Bamban RHU – Barangay San Nicolas
Quarterly 4ANC Accomplishments 2015
8 / 14 (57%)
8 / 7 (114%)
8 / 14 (57%)
10 / 9 (113%)
VS
15. Capas RHU – Barangay Cristo Rey
Quarterly FPCU Accomplishments 2015
76 / 1473 (5%)
125 / 1623 (8%)
85 / 1695 (5%)
121 / 1815 (7%)
S
16. Anao RHU – Barangay San Juan Quarterly 4ANC Accomplishments 2015
2 / 2 (100%)
1 / 1 (100%)
0 1 / 1
(100%) VS
17. San Clemente RHU Quarterly EBF Accomplishments 2015
31 (9%) 26 (7%) 46 (13%) 48 (14%) S
Quarterly FIC Accomplishments 2015
59 (17%) 71 (20%) 68 (19) 48 (14%) S
18. Mayantoc RHU – Mamonit BHS and Pedro L. Quines
Quarterly SBA and FBD Accomplishments 2015
3 / 5 (60%
6 / 6 (100%)
9 / 9 (100%)
3 / 4 (75%)
VS

18 Guide in Conducting an Implementation Review of the Community Health Service Record System
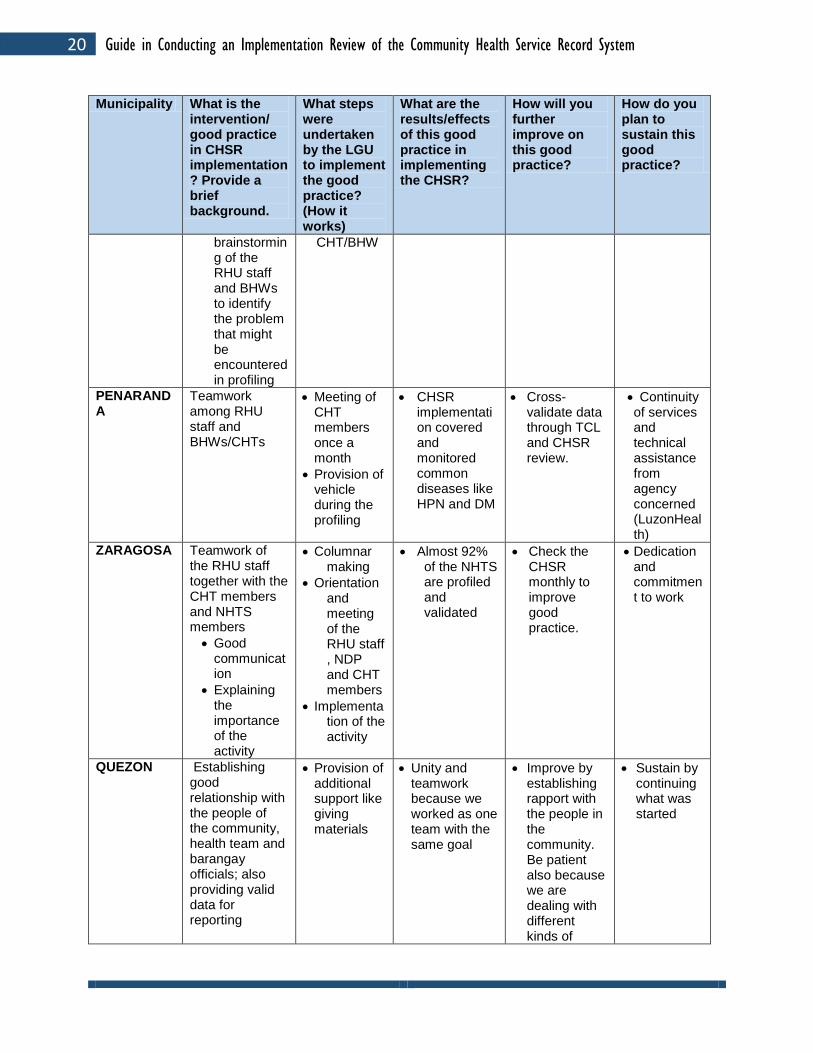
In Workshop 4, the RHU Teams are asked to choose one of their CHSR good practices on data generation that facilitates utilization of services at the BHS/barangay level towards improving program performance. They are further asked to write a brief description of their chosen good practice on Manila paper, following the Good Practice Guide prepared for this activity. Their outputs are then presented in plenary so that the other RHU Teams can learn from their experiences in the use of the CHSR. (Refer to Annex E for a copy of the Good Practice Writing Guide.)
Table 4 is a sample consolidation of CHSR good practices as reported by the RHU Teams of Nueva Ecija during the conduct of their province-wide CHSR System Implementation Review in March 2016. (Refer to Annex F for a Sample Presentation of a Good CHSR Practice in Legazpi City, Albay that was presented during the conduct of a CHSR Study Tour by the DOHRO IV-A Team in Albay Province on November 24-25, 2015.) Table 4. Consolidated CHSR Good Practices by Municipality in Nueva Ecija, March 2016
GOOD PRACTICES IN IMPLEMENTING THE CHSR IN NUEVA ECIJA
CHSR System Implementation Review March 29-30, 2016
Municipality What is the intervention/ good practice in CHSR implementation? Provide a brief background.
What steps were undertaken by the LGU to implement the good practice? (How it works)
What are the results/effects of this good practice in implementing the CHSR?
How will you further improve on this good practice?
How do you plan to sustain this good practice?
LICAB Teaming up with the NDP/CHT/BHW for house-to-house visits
Headings for the columnar notebook columns funded by LGU
It was implemented well that NHTS families in the community were given the services they needed.
Establish rapport with the community people in order for us to gain their trust.
Regular home visits for us to know the patients’/clients’ condition and attend to their needs immediately
TALUGTUG Weekly evaluation/supervision and coaching of the BHW/CHT on the first month of implementation for proper encoding of data, and then monthly monitoring for
Validation of data by NDPs and midwives on a monthly basis to ensure correct encoding and updated information
Accurate reporting
Monitoring of NHTS families made easier and handy for BHWs/CHTs
Continue implementing CHSR.
Provision of CHSR tool
Training of BHW/CHT on CHSR technology
Continue implementing CHSR.

19 Guide in Conducting an Implementation Review of the Community Health Service Record System
Municipality What is the intervention/ good practice in CHSR implementation? Provide a brief background.
What steps were undertaken by the LGU to implement the good practice? (How it works)
What are the results/effects of this good practice in implementing the CHSR?
How will you further improve on this good practice?
How do you plan to sustain this good practice?
the following months
SAN LEONARDO
Unity among health providers for a common goal
Time allowance, medical mission and community assembly
Improvement of accomplished CHSR since implemented
Continue and prioritize.
Conduct evaluation and PIR.
Assistance from LuzonHealth, PHO, LGU and DOH and dedication of health workers and BHWs
CARRANGLAN
Regular monthly meetings
Implemented since 2014 to the present
Initiated by the RHU staff and NDPs
RHU, NDPs and BHWs as the persons responsible
Unique feature: Increase compliance
LGU provided venue
Increased compliance
Increased accomplishments
Identified unmet needs of the target clients
Orient barangay council/community on the benefits.
Promote it as contributing to good health: “Health is Wealth”
Stir everybody’s interest to participate.
Regular evaluation/ monitoring of the implementation of CHSR
Sustenance of the needed logistics
GENERAL MAMERTO NATIVIDAD
Good relationship with the people of the community and monthly validation of CHSR
Continuous financial support from the LGU by sustaining the logistics needed by the CHT
Good rapport made the work easier for the CHT
Maintain the good relationship within the community.
To be patient and understanding
Always update the CHSR
GUIMBA Regular updating of CHSR and validation of data between RHM, NDP and CHT/BHW
Meeting and
Coordination with barangay officials
Meeting and rollout of program to the
Systematic, organized and accurate collection of data
Time management
Have good relationship with all personnel.
Using all the resources available
20 Guide in Conducting an Implementation Review of the Community Health Service Record System
Municipality What is the intervention/ good practice in CHSR implementation? Provide a brief background.
What steps were undertaken by the LGU to implement the good practice? (How it works)
What are the results/effects of this good practice in implementing the CHSR?
How will you further improve on this good practice?
How do you plan to sustain this good practice?
brainstorming of the RHU staff and BHWs to identify the problem that might be encountered in profiling
CHT/BHW
PENARANDA
Teamwork among RHU staff and BHWs/CHTs
Meeting of CHT members once a month
Provision of vehicle during the profiling
CHSR implementation covered and monitored common diseases like HPN and DM
Cross-validate data through TCL and CHSR review.
Continuity of services and technical assistance from agency concerned (LuzonHealth)
ZARAGOSA Teamwork of the RHU staff together with the CHT members and NHTS members
Good communication
Explaining the importance of the activity
Columnar making
Orientation and meeting of the RHU staff , NDP and CHT members
Implementation of the activity
Almost 92% of the NHTS are profiled and validated
Check the CHSR monthly to improve good practice.
Dedication and commitment to work
QUEZON Establishing good relationship with the people of the community, health team and barangay officials; also providing valid data for reporting
Provision of additional support like giving materials
Unity and teamwork because we worked as one team with the same goal
Improve by establishing rapport with the people in the community. Be patient also because we are dealing with different kinds of
Sustain by continuing what was started

21 Guide in Conducting an Implementation Review of the Community Health Service Record System
Municipality What is the intervention/ good practice in CHSR implementation? Provide a brief background.
What steps were undertaken by the LGU to implement the good practice? (How it works)
What are the results/effects of this good practice in implementing the CHSR?
How will you further improve on this good practice?
How do you plan to sustain this good practice?
people.
SCIENCE CITY OF MUNOZ
RHU staff monitoring the BHWs’ activities
Once-a-week RHU staffs visits to BHW
Monthly submission of their accomplishment
BHW monthly meetings
Coordination with the barangay official using ambulance for field purposes
Increase in accomplishments
Have good teamwork.
Good communication of the RHU staff with the BHW
SAN JOSE CITY
Support of the LGU/Barangay Council
Provision of vehicle in conducting home visits and follow-up
Fast delivery of services/resources needed by the NHTS families especially those in hard-to-reach areas
Coordinate health workers
Continuing what was started
NAMPICUAN
Regular meeting of the CHTs and the RHU staff for validation, updating and evaluation of data
Frequent meeting of the RHU staff to identify the programs that need to be improved
Quarterly PIR and initiating
Increase in the accomplishments, early detection and prevention of complications, and people’s awareness of the health services
Maintain close coordination of the RHU staffs with the BHWs/CHTs and NHTS members.
Continuation of the activity started

22 Guide in Conducting an Implementation Review of the Community Health Service Record System
Municipality What is the intervention/ good practice in CHSR implementation? Provide a brief background.
What steps were undertaken by the LGU to implement the good practice? (How it works)
What are the results/effects of this good practice in implementing the CHSR?
How will you further improve on this good practice?
How do you plan to sustain this good practice?
new programs in order to increase accomplishments in different indicators
offered at the RHU
PALAYAN CITY
Coordination of the barangay officials and support of the LCE
All barangays provided with health personnel who were very active in providing health services
All the NHTS families were provided health services for free.
Practice time management for updating.
Validate records.
Frequent monitoring of the BHWs with the supervision of the RHMs
LLANERA
Implementation of CHSR
Monthly monitoring of households that needed health services
Monthly meeting of BHW with RHM
The households that need health services go directly to health facility without hesitation.
Conduct monthly updating and monitoring of CHSR by RHM and NDP.
Have good teamwork among BHWs, RHMs and NDPs.
Regular monitoring/ updating CHSR
3. Action Planning After the conduct of the workshop proper, the RHU Teams are asked to prepare their respective Action Plans to address topic areas previously identified for improvement in Workshop 1. Table 5 shows a sample Action Plan for the continuing implementation of CHSR.

23 Guide in Conducting an Implementation Review of the Community Health Service Record System
Table 5. Sample Action Plan Municipality/RHU: Zaragosa Date: 03/30/2016 Objective: To address identified gaps and challenges in profiling, identifying those with unmet need for FP/MNCHN, and referring them to health facilities to access the needed health services.
Identified Gaps and Challenges
Activities
Time Frame
Resource Requirement
Person Responsible
Budget for printing Meeting with the LCE regarding the budget allocation
April 11, 2016 Columnar printing/bond paper, ball pen and glue
MHO RHP Nurse RHM
Some NHTS family members not cooperative
Continuous follow-up of NHTS family members who were not yet profiled
April 13-15, 2016
Transportation BHW RHM
Lack of consolidation forms
PHO or LGU to reproduce/provide consolidation forms
April 13, 2016 Bond paper, ink for the copier
Nurse
No money for transportation expenses of BHWs
Coordinate with barangay captain for assistance in the transportation of the clients
April 18, 2016 Additional budget for gasoline
MHO Nurse Barangay captain
Patients do not have enough money going to the hospitals for treatment
Lobby with the LCE to request the use of the ambulance in referring patients to the hospital.
April 11, 2016 Gasoline, ambulance
MHO Nurses
4. Synthesis and Agreements/Next Steps for the Province/City The last session is on the presentation of the workshop synthesis and agreements, including the next steps for the PHO/CHO. This is usually presented by the Provincial Health Officer/City Health Officer or his/her representative. Table 6 is an example of this output that is presented in a plenary session.
Table 6. Synthesis, Agreements and Next Steps in the CHSR Implementation in Tarlac Province
Item / Concern Synthesis, Agreements and Next Steps
1. Development of a CHSR version for the use of BHWs in Tarlac based on the province’s needs
In 2014, the PHO, , led her technical staff in developing their own version of the CHSR, including the modification of the columnar headings/indicators and the formatting of the cell entries/codes in the columnar notebook to come up with a simplified version for the use of the BHWs.
2. Coverage of use of the CHSR The BHW maintains a CHSR for NHTS HHs, and a separate CHSR for the rest of the population, as prescribed by the DOH-

24 Guide in Conducting an Implementation Review of the Community Health Service Record System
Item / Concern Synthesis, Agreements and Next Steps
CHT System. However, Dr. Lazatin is recommending that there be just one CHSR tool per BHW, and that NHTS family members listed in the CHSR be simply identified by putting an asterisk in the remarks column.
3. Supply of Columnar Notebooks > Initial supply > Concern: Lack of Columnar Notebooks for continuing use in some municipalities as identified in Workshop 1, especially for the general population
Initially the DOHRO III provided columnar notebooks for the use of the CHT Partners, who were mostly BHWs. The Tarlac Provincial Government also procured columnar notebooks (2,800 pieces) for the use of BHWs. The BHWs were asked to shell out 10 pesos per person to shoulder the cost of the photocopying of the Columnar Headings.
Those municipalities which reported lack of columnar logbooks for continuing use were advised to advocate for support from the municipal/barangay local chief executives (LCEs) to procure columnar notebooks.
4. In Workshop 1, some municipalities reported the lack of a reporting form to use from the barangay level to the PHN.
It was emphasized throughout the activity that the use of the CHSR is primarily for BHWs to identify those with unmet needs for FP/MNCHN/TB and refer them to the HSPs/health facilities for the appropriate health services. Hence, Dr. Lazatin pointed out the importance of the conduct of monthly meetings among the RHM, the NDP assigned in the area, and the BHWs to verify the CHSR data with the RHM’s TCL entries for the different health conditions. The names of patients/FP clients who did not yet seek consultation or need follow-up are then listed down or marked in the CHSR for the concerned BHW to follow up. This will help the RHM check and ensure that all those provided with health services are recorded in her TCLs, improving the quality of the RHU’s FHSIS data. There is no need to report the CHSR data to the level of the MHO/PHN.
5. Some RHUs reported in Workshop 1 that CHSR tools in their areas were not updated or not properly filled up.
It is important to perform regular monitoring and supportive supervision through coaching and mentoring by the RHMs and NDP nurses.
Include in the discussion the need for BHWs to cross out the names of patients/FP clients listed in one health condition who were transferred to another section of the CHSR for another health condition (e.g., pregnant to postpartum, newborn to infant, dropped from the list of FP current users), using a highlighter or shading with a pencil.
6. Also in Workshop 1, some RHUs commented on the need to fill up a column for date of birth repeatedly on the CHSR pages for the Newborn, Infant and Child sections; and that the CHSR spaces are too small to write on.
It was explained that it is important to repeatedly write the date of birth because the giving of the different vaccines is dependent on the age of the child at a given time.
The small spaces in the CHSR are meant to be filled up only with a check or a cross mark, or with Y or N, or other letter codes. The CHSR is meant only to record information on those with unmet needs for FP/MNCHN/TB for referral purposes, and that detailed information should be collected by the RHM for recording in her TCLs when the client avails of the needed services.
Dr. Lazatin also informed the participants that her technical staff will sit down to update the CHSR, particularly the Expanded Program on Immunization (EPI) headings.

25 Guide in Conducting an Implementation Review of the Community Health Service Record System
Item / Concern Synthesis, Agreements and Next Steps
7. Some BHWs reportedly lack knowledge and skills in giving key health messages.
The BHWs were advised to simply read from the CHSR tool the appropriate messages for their patients/FP clients.
Review the key health messages for better understanding of the BHWs during their monthly meetings with the RHM and NDP nurse. The BHWs should be advised to just discuss the health messages applicable/appropriate for the condition of the patient they are talking to. Additional messages and explanations can be given by the midwife during consultation.
PHN and RHMs trained in __________ (IPCC) can provide inputs/tips on __________ (IPC) skills for the CHT Partners to make them more confident in giving health messages.
The RHU staff were advised to recommend for retirement the quite old BHWs who already have difficulty reading/performing tasks.
8. The RHUs reported that the DOH requires the health volunteers to conduct 100% house-to-house visits for NHTS families to profile and identify those with unmet needs for FP/MNCHN.
emphasized that health is the responsibility of each person, and that health education/teaching should be intensified for the community to access available health services that they need, instead of the HSPs/BHWs doing house-to-house visits for them.
9. Results of Workshop 2 on the exercise on verifying CHSR data with the TCL entries using the CHSR Summary and Discussion Tool
The results of Workshop 2 showed that the task of verifying CHSR data with the TCL entries for a monthly period is very doable, as it took the participants only about 10 to 15 minutes in checking the data in the CHSR for a given health program against the entries in the corresponding TCL. This can easily be done by the RHM, NDP nurse, and the BHWs during their monthly meetings.
10. Results of Workshop 3 on the Accomplishments for Key FP/MNCHN Indicators Relative to CHSR Contribution
The results of Workshop 3 showed that almost all of the municipalities (16 of 18) that were able to bring their FHSIS data for the key FP/MNCHN got a score in the range of 25% to 100% CHSR contribution in referrals. This means that 30% or more (very significant) of the accomplishments for their assigned health program for the municipality/barangay were seen and referred to the HSPs by the BHWs using the CHSR for the given reporting periods. The two municipalities also brought their TCLs and CHSR tools, but these did not belong to partner RHM and BHW; hence, the data entries cannot be verified.
It was also shared that the use of the CHSR tool has helped increase the province’s contraceptive prevalence rate (CPR) from 25% to 30% for the past year (an increase of 5% points). Dr. Lazatin attributed this increase to the use of the CHSR in looking for women with unmet need for FP.
11. Presentation of good practices in CHSR
The different RHUs also shared their good practices in the use of the CHSR in a plenary session. Several municipalities reported the support they get from the barangay LCEs who provide columnar notebooks. Some reported that the midwife and NDPs had been conducting monthly meetings to check the CHSRs and mentor the BHWs in correctly filling these up.
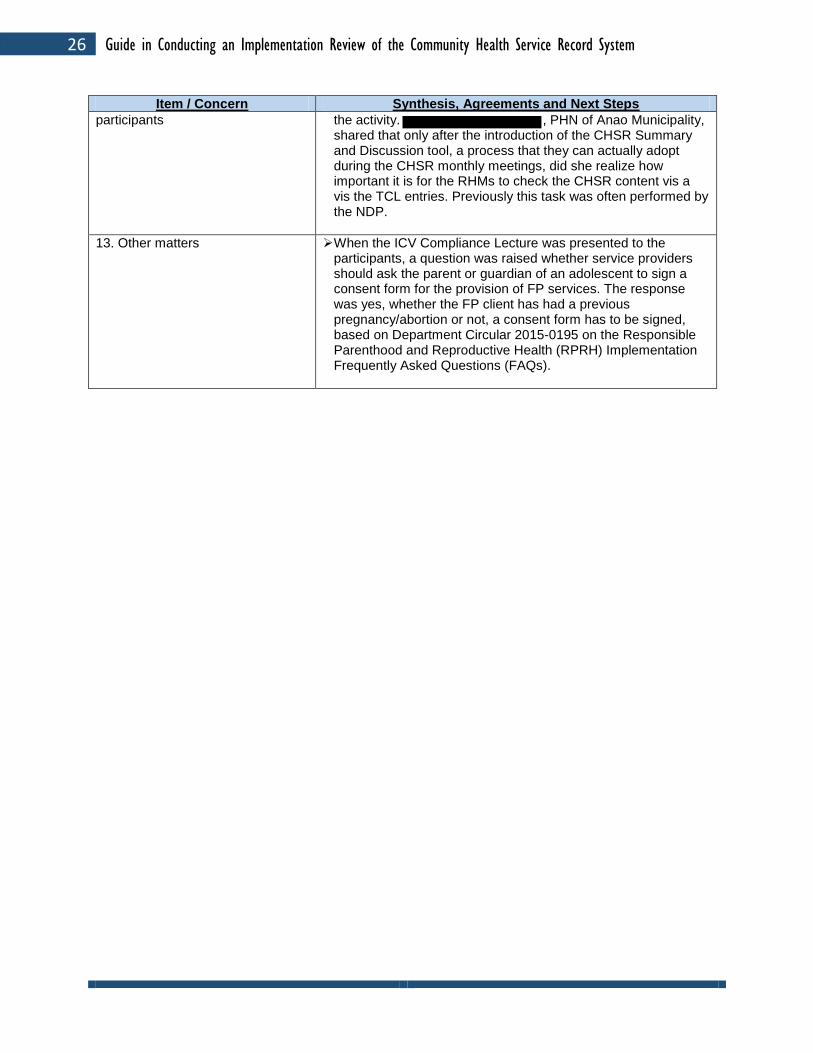
12. Impressions from the A few participants were asked to share their impressions about
26 Guide in Conducting an Implementation Review of the Community Health Service Record System
Item / Concern Synthesis, Agreements and Next Steps
participants the activity. , PHN of Anao Municipality, shared that only after the introduction of the CHSR Summary and Discussion tool, a process that they can actually adopt during the CHSR monthly meetings, did she realize how important it is for the RHMs to check the CHSR content vis a vis the TCL entries. Previously this task was often performed by the NDP.
13. Other matters When the ICV Compliance Lecture was presented to the participants, a question was raised whether service providers should ask the parent or guardian of an adolescent to sign a consent form for the provision of FP services. The response was yes, whether the FP client has had a previous pregnancy/abortion or not, a consent form has to be signed, based on Department Circular 2015-0195 on the Responsible Parenthood and Reproductive Health (RPRH) Implementation Frequently Asked Questions (FAQs).

27 Guide in Conducting an Implementation Review of the Community Health Service Record System
III. Next Steps The results of the CHSR System Implementation Reviews conducted in the different participating provinces and cities had been helpful to the P/CHO and RHU program coordinators in identifying gaps and challenges in the use of the CHSR. This enabled them to address these issues and improve the use of the CHSR not simply as a recording tool for BHWs, but more importantly to profile and refer those with unmet need for FP/MNCHN/TB services to health facilities, so that they can be provided with the needed services. The following are the common agreements made during the conduct of the CHSR System Implementation Review in the participating provinces/cities:
1. To expand the use of the CHSR, not only for NHTS households, but also to include non-NHTS households;
2. For the RHU staff to continue the regular conduct of supportive supervision and monthly meetings to support the BHWs in updating family profiles in the CHSR notebooks for easy tracking of patients/FP clients, including defaulters for the different health services;
3. To include in their annual health plans a budget item for the procurement of columnar notebooks with printed headings;
4. To request the DOHRO and LCEs to provide printed copies of the CHSR; and 5. Some of the provinces and cities have also set the schedule for their next CHSR
Implementation Review, as a periodic assessment of the status of implementation of CHSR use.
Since this exercise was done for only one program indicator per RHU Team during the conduct of the CHSR Implementation Reviews, the results are not sufficient to show the real picture of the referral contribution of community health volunteers in increasing FP/MNCHN service utilization through the use of the CHSR. As one of the next steps, therefore, the USAID-LuzonHealth Project collaborated with the Tarlac PHO to conduct a more focused CHSR Evaluation Study that will cover all the program indicators. The study will entail conducting the same process of checking the percentage contribution of referrals of all the community health volunteers to the accomplishments in the TCLs of the RHM in selected health facilities from the study sites, using the tools developed for the CHSR Implementation Review. Tarlac Province was selected as the study site because the community health volunteers in this area, who are all BHWs, cover not only NHTS households, but all households. It is hoped that the use of this CHSR System Implementation Review Guide will be helpful for the provinces and cities that continue to implement the use of the CHSR, as well as for those areas that will adopt the CHSR use in the future.

28 Guide in Conducting an Implementation Review of the Community Health Service Record System

29 Guide in Conducting an Implementation Review of the Community Health Service Record System
References
1. Department of Health. Community Health Team Guidebook for CHT Partners. 2011. 2. Department of Health. Management and Supervision of Community Health Team (CHT)
Operations. August 2014. 3. Global Health Workforce Alliance/World Health Organization. Global Experience of
Community Health Workers for Delivery of Health-Related Millennium Development Goals: A Systematic Review, Country Case Studies, and Recommendations for Integration into National Health Systems. 2010.
4. USAID-LuzonHealth. CHSR Briefer. July 14, 2014.
5. USAID-LuzonHealth Project. Draft: An Evaluation Study to Determine the Referral Contribution of Community Health Volunteers Towards Increasing FP/EPI Service Utilization Through the Use of the Community Health Service Record (CHSR) in Four Municipalities in Tarlac Province. 2017.
6. USAID-HealthGov Project. Health Profiling, Recording and Reporting in the CHT System
Using the Columnar Notebook: Guide. December 2012. 7. USAID-LuzonHealth Project. Stories from the Field, Volume 1. October 2017. 8. USAID-LuzonHealth Project. Strategy Paper (Collecting, Recording and Reporting
Household-Based Information among NHTS-PR Households Using the Community Health and Service Record). February 21, 2014.

30 Guide in Conducting an Implementation Review of the Community Health Service Record System

31 Guide in Conducting an Implementation Review of the Community Health Service Record System
ANNEXES

32 Guide in Conducting an Implementation Review of the Community Health Service Record System
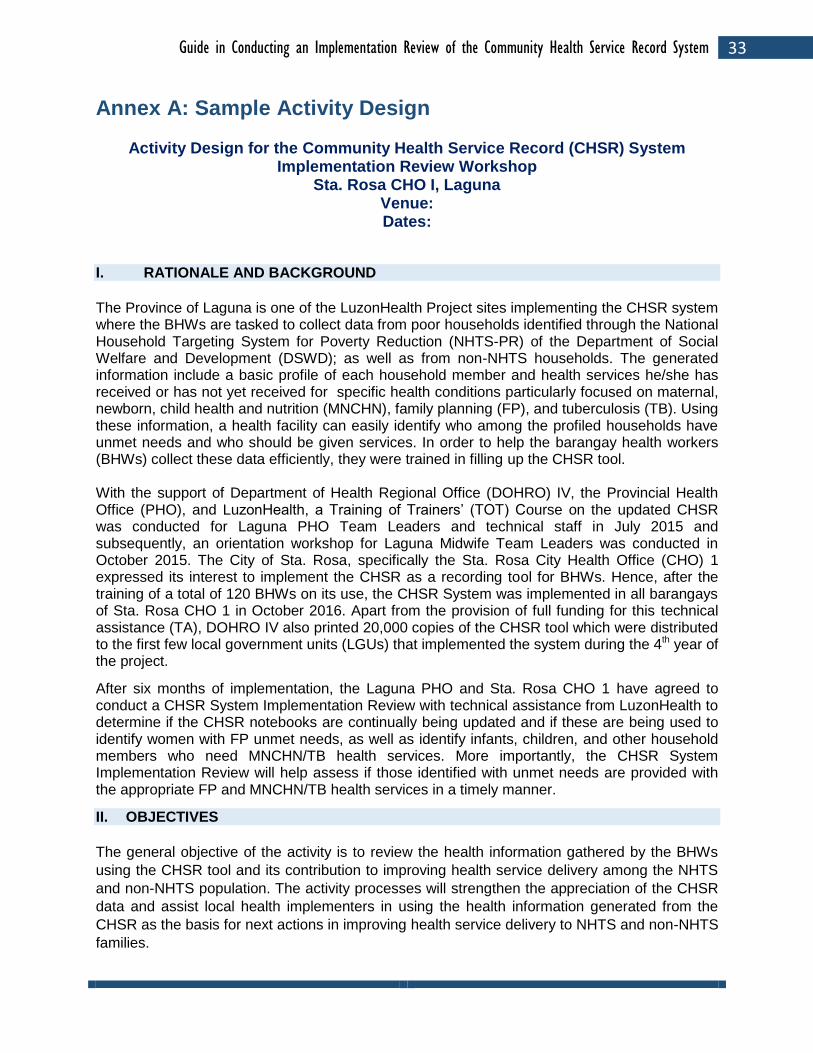
33 Guide in Conducting an Implementation Review of the Community Health Service Record System
Annex A: Sample Activity Design
Activity Design for the Community Health Service Record (CHSR) System Implementation Review Workshop
Sta. Rosa CHO I, Laguna Venue: Dates:
I. RATIONALE AND BACKGROUND
The Province of Laguna is one of the LuzonHealth Project sites implementing the CHSR system where the BHWs are tasked to collect data from poor households identified through the National Household Targeting System for Poverty Reduction (NHTS-PR) of the Department of Social Welfare and Development (DSWD); as well as from non-NHTS households. The generated information include a basic profile of each household member and health services he/she has received or has not yet received for specific health conditions particularly focused on maternal, newborn, child health and nutrition (MNCHN), family planning (FP), and tuberculosis (TB). Using these information, a health facility can easily identify who among the profiled households have unmet needs and who should be given services. In order to help the barangay health workers (BHWs) collect these data efficiently, they were trained in filling up the CHSR tool. With the support of Department of Health Regional Office (DOHRO) IV, the Provincial Health Office (PHO), and LuzonHealth, a Training of Trainers’ (TOT) Course on the updated CHSR was conducted for Laguna PHO Team Leaders and technical staff in July 2015 and subsequently, an orientation workshop for Laguna Midwife Team Leaders was conducted in October 2015. The City of Sta. Rosa, specifically the Sta. Rosa City Health Office (CHO) 1 expressed its interest to implement the CHSR as a recording tool for BHWs. Hence, after the training of a total of 120 BHWs on its use, the CHSR System was implemented in all barangays of Sta. Rosa CHO 1 in October 2016. Apart from the provision of full funding for this technical assistance (TA), DOHRO IV also printed 20,000 copies of the CHSR tool which were distributed to the first few local government units (LGUs) that implemented the system during the 4th year of the project.
After six months of implementation, the Laguna PHO and Sta. Rosa CHO 1 have agreed to conduct a CHSR System Implementation Review with technical assistance from LuzonHealth to determine if the CHSR notebooks are continually being updated and if these are being used to identify women with FP unmet needs, as well as identify infants, children, and other household members who need MNCHN/TB health services. More importantly, the CHSR System Implementation Review will help assess if those identified with unmet needs are provided with the appropriate FP and MNCHN/TB health services in a timely manner.
II. OBJECTIVES
The general objective of the activity is to review the health information gathered by the BHWs
using the CHSR tool and its contribution to improving health service delivery among the NHTS
and non-NHTS population. The activity processes will strengthen the appreciation of the CHSR
data and assist local health implementers in using the health information generated from the
CHSR as the basis for next actions in improving health service delivery to NHTS and non-NHTS
families.
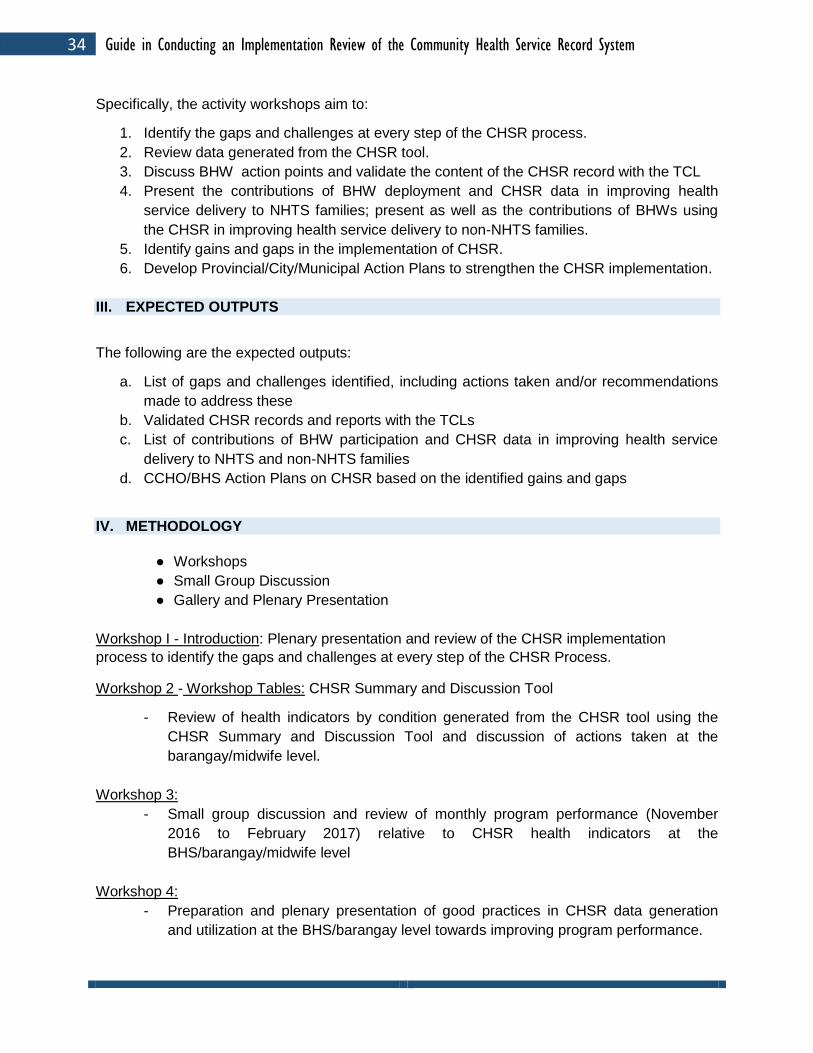
34 Guide in Conducting an Implementation Review of the Community Health Service Record System
Specifically, the activity workshops aim to:
1. Identify the gaps and challenges at every step of the CHSR process.
2. Review data generated from the CHSR tool.
3. Discuss BHW action points and validate the content of the CHSR record with the TCL
4. Present the contributions of BHW deployment and CHSR data in improving health
service delivery to NHTS families; present as well as the contributions of BHWs using
the CHSR in improving health service delivery to non-NHTS families.
5. Identify gains and gaps in the implementation of CHSR.
6. Develop Provincial/City/Municipal Action Plans to strengthen the CHSR implementation.
III. EXPECTED OUTPUTS
The following are the expected outputs:
a. List of gaps and challenges identified, including actions taken and/or recommendations
made to address these
b. Validated CHSR records and reports with the TCLs
c. List of contributions of BHW participation and CHSR data in improving health service
delivery to NHTS and non-NHTS families
d. CCHO/BHS Action Plans on CHSR based on the identified gains and gaps
IV. METHODOLOGY
● Workshops
● Small Group Discussion
● Gallery and Plenary Presentation
Workshop I - Introduction: Plenary presentation and review of the CHSR implementation
process to identify the gaps and challenges at every step of the CHSR Process.
Workshop 2 - Workshop Tables: CHSR Summary and Discussion Tool
- Review of health indicators by condition generated from the CHSR tool using the
CHSR Summary and Discussion Tool and discussion of actions taken at the
barangay/midwife level.
Workshop 3:
- Small group discussion and review of monthly program performance (November
2016 to February 2017) relative to CHSR health indicators at the
BHS/barangay/midwife level
Workshop 4:
- Preparation and plenary presentation of good practices in CHSR data generation
and utilization at the BHS/barangay level towards improving program performance.

35 Guide in Conducting an Implementation Review of the Community Health Service Record System
- Action planning (to address areas identified for improvement)
V. EXPECTED PARTICIPANTS AND ROLES
Participants and Number
Roles Office/Total Pax
LGU: 60 - Participate in the review and provide data from the CHSR
and TCLs. CHO 2
PHN 6
RHM 13
NDP 6
BHW
3 BHWs per
Barangay Health
Station
3 x11 = 33 BHWs
PDO: 2 - Facilitate in the conduct of CHSR System Implementation
Review.
- Assist the participants in identifying the gaps and
recommendations for the continuous implementation of CHSR.
- Monitor CHSR implementation in their respective areas of
assignment.
BHW
Coordinator
and Assistant
2
PHO: 2
PHO Staff
(BHW
Coordinator,
FP/MNCHN
Coordinators
3
LuzonHealth/Partner NGO: 3 - Facilitate the conduct of CHSR System Implementation
Review.
- Document the CHSR IR activity.
- Assist the DOHRO and PHO in the monitoring of CHSR
implementation.
1.
2.
3.

36 Guide in Conducting an Implementation Review of the Community Health Service Record System
VI. VENUE & SCHEDULE
The two-day CHSR Implementation Review will be held at the Conference Hall, Sta. Rosa CHO
1, Sta. Rosa City, Laguna on April 25-26 2017.
VII. PROPOSED ACTIVITY DESIGN
Date/Time Activity Person
Responsible
Day 1
8:00 – 9:00AM Registration Laguna PHO/Sta. Rosa
CHO1/LuzonHealth
9:00 -9:30AM
Preliminaries
● Opening ● Invocation ● National Anthem ● Welcome message ● Introduction of participants ● Leveling of expectation
Laguna PHO/Sta. Rosa
CHO1
9:30 – 9:50AM SESSION 1
Objectives and Overview of the Activity
PDO/PHO
9:50 – 10:15AM
SESSION 2
Presentation of Status of CHSR
implementation in Sta. Rosa CHO 1
Sta. Rosa CHO 1
10:15 – 11:15AM
SESSION 3
Monitoring and Supportive Supervision for
CHSR
PHO
11:15 – 12:00NN
SESSION 4
Ensuring Quality Data for the CHSR System
at the Barangay Level
LuzonHealth
12:00 – 1:00PM LUNCH
1:00 – 2:15PM
SESSION 5
Workshop Introduction: Plenary
presentation and review of the CHSR
implementation process
LuzonHealth/PHO/PDO/ CHO1

37 Guide in Conducting an Implementation Review of the Community Health Service Record System
Workshop 1: Refinement and enhancement
of the pre-workshop output conducted at the
barangay/midwife level to identify gaps and
challenges including
actions/recommendations
2:15 – 3:15PM SESSION 6 (con’t)
Plenary presentation of Workshop 1 outputs
3:15 – 3:45PM SESSION 7
The CHSR Summary and Discussion Tool
LuzonHealth
3:45 – 4:45PM
SESSION 8
(Using the CHSR Summary and Discussion
tool)
Workshop 2: (Activity to be done at the
BHS/Barangay/Midwife level in groups)
1. Review of health indicators by condition
generated from the CHSR tool using
workshop tables and discussion of actions
taken at the barangay/midwife level
LuzonHealth/PHO/PDO/
CHO1
4:45 – 5:00PM Wrap-up for Day 1 PHO
Day 2
8:00 – 8:30AM Recap Participants
8:30 – 9:30AM Workshop 2: (con’t)
Plenary presentation of Workshop 2 outputs PHO
9:30 – 11:00AM
SESSION 9
Workshop 3:
Small group discussion and review of
program performance relative to CHSR
contribution at the BHS/barangay level using
the CHSR. Selected groups to present in
plenary.
PHO/PDO/CHO1
11:00- 12:00NN
Workshop 4:
Group work and plenary presentation of good
practices in CHSR data generation and
utilization at the BHS/barangay level towards
PHO/PDO/CHO1

38 Guide in Conducting an Implementation Review of the Community Health Service Record System
improving program performance
12:00 – 1:00PM LUNCH
1:00 – 3:00PM
Session 10
Action planning (to address areas identified
for improvement)
PHO/PDO/CHO1
3:00- 4:00PM Plenary Presentation of Action Plans PHO
4:15 – 4:30PM Synthesis and Next Steps PHO/CHO1
4:30 – 4:45PM Closing Program PHO/CHO1
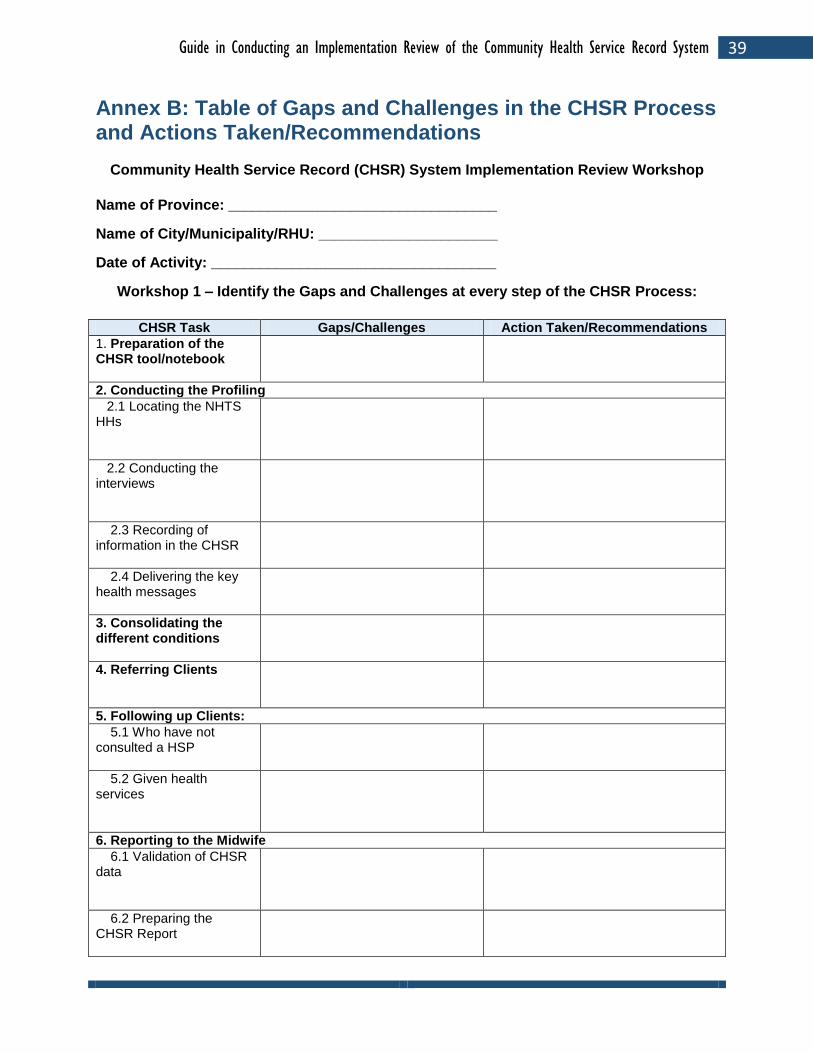
39 Guide in Conducting an Implementation Review of the Community Health Service Record System
Annex B: Table of Gaps and Challenges in the CHSR Process and Actions Taken/Recommendations
Community Health Service Record (CHSR) System Implementation Review Workshop
Name of Province: _________________________________
Name of City/Municipality/RHU: ______________________
Date of Activity: ___________________________________
Workshop 1 – Identify the Gaps and Challenges at every step of the CHSR Process:
CHSR Task Gaps/Challenges Action Taken/Recommendations
1. Preparation of the CHSR tool/notebook
2. Conducting the Profiling
2.1 Locating the NHTS HHs
2.2 Conducting the interviews
2.3 Recording of information in the CHSR
2.4 Delivering the key health messages
3. Consolidating the different conditions
4. Referring Clients
5. Following up Clients:
5.1 Who have not consulted a HSP
5.2 Given health services
6. Reporting to the Midwife
6.1 Validation of CHSR data
6.2 Preparing the CHSR Report

40 Guide in Conducting an Implementation Review of the Community Health Service Record System
7. Reporting to the PHN and P/CHO
8. Reporting to the DOH (NDPs/DMOs)
9. Other Tasks

41 Guide in Conducting an Implementation Review of the Community Health Service Record System
Annex C: CHSR Summary Discussion Forum
Community Health Team / Community Health Service Record (CHSR) System
Name of Facility (BHS): ______________________ Address: ________________________________
Name of RHM: ______________________________ Date of Activity: __________________________
Names of BHWs/Barangay: ____________________________________________________________
____________________________________________________________________________________
Note: Use 1 Form for each Type of TCL reviewed.
DISCUSSION RESULTS COMPARING CHSR DATA WITH TCL ENTRIES USING THE CHSR
SUMMARY AND DISCUSSION TOOL:
Barangay and Type of TCL Reviewed (Prenatal, Postpartum, FP, EPI/Nutrition)
CHSR Notebook Information
TCL Information Number of Patients Listed for Follow-up by BHWs (BHWs notes down in her CHSR the names of patients for follow-up)
Example: FP TCL of RHM for each of 3 barangays in her BHS
Seen Referred Number of Referred Given Services and Recorded in TCL; List services given
1. Barangay Gana:
BHW1
BHW2
BHW3
TOTAL for Barangay
2. Barangay Las-ud
BHW4
BHW5
TOTAL for Barangay
3. Barangay Sobredillo
BHW6
OVERALL TOTAL for BHS

42 Guide in Conducting an Implementation Review of the Community Health Service Record System

43 Guide in Conducting an Implementation Review of the Community Health Service Record System
Annex D: CHSR Referral Percentage Contribution Worksheet
Community Health Service Record (CHSR) System Implementation Review Workshop BHS/ Barangay: ___________________________ City/Municipality: ____________________________________________
INDICATOR April-June
2015 July-Sept.
2015 Oct-Dec.
2015 Jan.-March
2016 Remarks
Estimated PROPORTION (%) of the Accomplishments REFERRED by CHT Partners/BHWs implementing the CHSR Formula: Number of Patients/FP Clients REFERRED by CHT Partners/BHWs divided by the Total Number of Patients/FP Clients Listed in the Corresponding TCL of the Midwife for the same period. This represents the % referral contribution of CHT Partners/BHWs using the CHSR in the total accomplishments for a given period, by health indicator.
1. FP-CU
2. 4ANC
3. SBA
4. FBD
5. EBF
6. FIC

44 Guide in Conducting an Implementation Review of the Community Health Service Record System

45 Guide in Conducting an Implementation Review of the Community Health Service Record System
Annex E: Good Practice Writing Guide
GOOD PRACTICE IN IMPLEMENTING THE CHSR
Name of City/Municipality/Barangay: ____________________________________________
____________________________________________________________________________
Office/Unit/Facility: ___________________________________________________________
Start of CHSR Implementation: _____________________
1. What is the Intervention/Good Practice in CHSR implementation? Provide a brief
background, highlighting the following, among others:
Length of time that the good practice has been in place/implemented
How the good practice came about (who initiated/conceptualized and what were the circumstances or problems encountered that led to the adoption of the good practice)
Person/office primarily responsible for implementing the good practice
Estimate of resources (time, manpower, financial) required to implement the good practice
Unique features of the good practice
2. What steps were undertaken by the LGU to implement the good practice? (How it works)
Enumerate and discuss the specific steps involved in implementing the good practice
and identify the specific persons/units involved in each step.
3. What are the results/effects of this good practice in implementing the CHSR?
Give an account of the observable impact of the good practice on various aspects of
CHSR implementation as well as on the beneficiaries (including client satisfaction) and
program implementers.
Describe the lessons learned from the introduction of the good practice in CHSR
implementation.
4. How will you further improve on this good practice?
5. How do you plan to sustain this good practice?

46 Guide in Conducting an Implementation Review of the Community Health Service Record System

47 Guide in Conducting an Implementation Review of the Community Health Service Record System
Annex F: Sample Presentation of a Good CHSR Practice -
2016

48 Guide in Conducting an Implementation Review of the Community Health Service Record System
CHSR and the CHT Partners August,2012 – Pilot training of CHT Partners in Legazpi
City
Year 2013- Columnar Technology was implemented by the CHT Partners for the following health conditions: Newborn, Infant, Child, Pregnant, Postpartum, FP Current User, not using FP, Elderly, PWD and Chronic Diseases
November and December, 2014- Introduced the CHSR with additional health conditions: Adolescent, TB Adult, TB among children, Dengue, Malaria, Rabies, Senior Citizen and Death Cases
3

49 Guide in Conducting an Implementation Review of the Community Health Service Record System
Adapting the CHSR for BHWs of Dita BHC (1)
• The RHM assigned in Dita BHC made a strategy to facilitate the early submission of reports from BHWs
• She adopted the idea of CHSR / Columnar Notebook being used by the CHT partners in her Barangays and modified it according to the program implementation needs
• She encouraged the BHWs to adopt the modified CHSR / Columnar Notebook for the non – NHTS HH
5
Adapting the CHSR for BHWs of Dita BHC (2)
• New data and information gathered by the BHWs in the barangays are all entered in the modified CHSR notebook / Columnar Notebook
• the RHM upon monthly collection of reports, validates the data in the Columnar Notebooks of the BHWs with the entries in her Target Client Lists (TCLs) for patients that she has given health services, thus facilitating an organized and easier generation of data from the BHWs
6
50 Guide in Conducting an Implementation Review of the Community Health Service Record System
Unique Features of the Good Practice (1)• Cost of columnar notebook is only ₽ 23.00 per piece
• Columnar notebook may be used for 3 years
• The BHW Columnar Notebook contains the following Health Conditions as Column Headings:• Pregnancy tracking
• PostPartum
• Newborn and EPI Schedules ( includes listing of defaulters and follow-up)
• Mortality and Morbidity
• The RHM and the non-CHT BHWs practice one-on-one consultation and validation of records and reports every month based on the Columnar Notebook and TCLs
7
Steps in Developing the Good Practice (1)• To address the issue about double reporting and to
ensure efficient masterlisting and record- keeping, the RHM of Dita BHC adopted a strategy on how to comprehensively implement the needed health services in the barangay level
• She proposed to the BHWs during their meeting to adopt a more systematic way of keeping records by introducing the modified CHSR/Columnar Notebook
• The health indicators that are needed to be monitored and followed-up became the headings of the 14-column BHW Columnar Notebook
8

51 Guide in Conducting an Implementation Review of the Community Health Service Record System
• Thus, besides the CHT partners, the non-CHT BHWs assigned in all puroks and sitios in their barangays are also asked to bring their modified CHSR / Columnar Notebooks with them during monthly meetings to be validated by their Supervisor (RHM) with the assistance of the NDP Nurse
• This way not only NHTS families are thoroughly monitored for their health conditions but non-NHTS families will have the same opportunity of being covered and listed in the modified CHSR / Columnar Notebook
Steps in Developing the Good Practice (2)
9
Good results and effects of this practice
Program Implementors Beneficiaries
• The use of too many loose forms is minimized and the BHWs have intact records for their assigned areas
• All the data for the needed health indicators are in one columnar notebook, thus, reports are easily extracted
• Double reporting is avoided
• The modified CHSR/Columnar Notebook is handy and light
• EPI defaulters are easy to follow-up
• Maternal Tracking among pregnant mothers is facilitated especially in identifying pregnant mothers during their first trimester
10

52 Guide in Conducting an Implementation Review of the Community Health Service Record System
Learnings
• The implementation of the FP/MNCHN/TB Programs require commitment, passion ,patience and hard work on the part of the not only of CHT Partners but also of BHWs who follow-up patients for all programs in the community
• Some of the BHWs are also members of CHTs that is why the use of a more comprehensive and organized system of record keeping like the modified CHSR/Columnar Notebook is more advantageous on their part
11
How to further improve this Good Practice
• The Nursing Service of the City Health Office is in the process of introducing to the other RHMs in LegazpiCity this good practice of encouraging the BHWs to use the modified CHSR/Columnar Notebook for recording the information they get from the households in their areas of assignment
• The CHO staff will monitor the use of this tool and provide supportive supervision at the barangay level once its use is implemented
12

53 Guide in Conducting an Implementation Review of the Community Health Service Record System
How to sustain this good practice• The Nursing Service Division of Legazpi City Health
Office with the leadership of the City Health Officer is planning to make a proposal to the City Council and Barangay Councils for them to fund the procurement of Columnar Notebooks to be used by the CHT Partners and BHWs for them to be able to continue to serve the community better using this tool
• The NDP Nurses will be requested to facilitate re-training and re-orientation activities on the FP/MNCHN Programs for the CHTs/BHWs so that they will better understand the use of the modified CHSR / Columnar Notebook
13
CHSR Roll-out Training Nov-Dec., 2014
14

54 Guide in Conducting an Implementation Review of the Community Health Service Record System
CHTs in action
15
Community Health Service Record
(CHSR)BHW Columnar Record Book
16

55 Guide in Conducting an Implementation Review of the Community Health Service Record System
Thank You!
17

56 Guide in Conducting an Implementation Review of the Community Health Service Record System

57 Guide in Conducting an Implementation Review of the Community Health Service Record System


















