
Identification and transport of sick neonate
37
Identification And Transport Of Sick Neonate L S DESHMUKH DM(NEONATOLOGY) PROFESSOR, GMCH, AURANGABAD
-
Upload
laxmikant-deshmukh -
Category
Healthcare
-
view
104 -
download
0
Transcript of Identification and transport of sick neonate

Identification And Transport
Of Sick NeonateL S DESHMUKH
DM(NEONATOLOGY)
PROFESSOR,
GMCH, AURANGABAD
Signs of Good Health at Birth
Objective measures
Breathing
Heart rate above
100 beats/minute
Subjective measures
Vigorous cry
Pink skin
Good muscular tone
Good reactions to
stimulus
•Most important measure is whether newborn is breathing
• Assessing all of above delays resuscitation, if it is necessary.
Sick newborn
Early detection,
prompt treatment and
referral (if required)
necessary to prevent high mortality

Problems in early diagnosis of
sick newborn
Many NBs referred unnecessarily
Non-specific signs
Difficulties in preterm and LBW babies

Identifying Sick New born – Danger
Signs

Danger signs
Lethargy
Hypothermia
Respiratory distress
Cyanosis
Convulsion
Abd. distension
Bleeding
Yellow palms/
soles
Excessive wt. loss
Vomiting
Diarrhea

Lethargy and poor sucking
In a term baby who was feeding earlier
indicates neonatal illness
(as perceived by mother)
In a preterm baby needs careful
assessment because it may be due to cold
stress or immaturity

Capillary refill time (CRT)
Indicates tissue perfusion
Normal CRT < 3 seconds
Prolonged CRT > 3 seconds *
Use 10ml/kg normal saline bolus
* Hypotension, hypothermia, acidosis
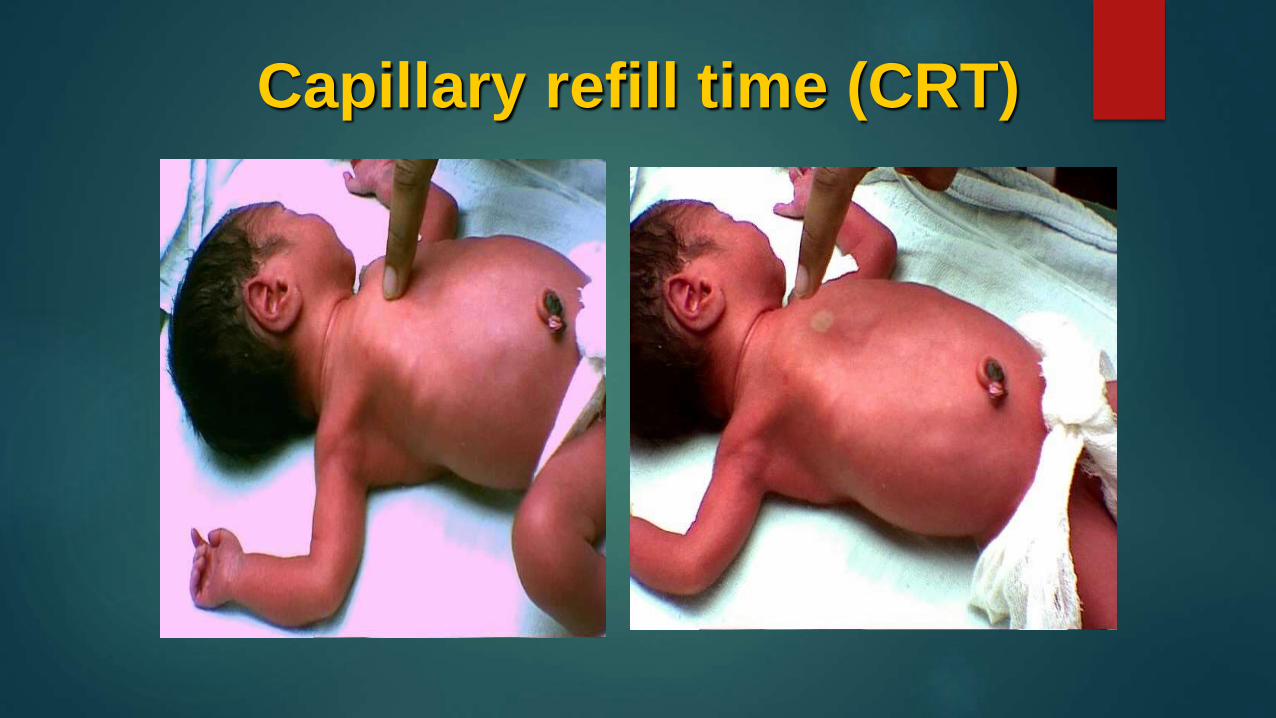
Capillary refill time (CRT)

Respiratory problems
RR > 60 / min*
Retractions
Grunt
Central cyanosis
Apnea
*Rate should be counted in a quiet state
and not immediately after feed

R
E
T
R
A
C
T
I
O
N
S
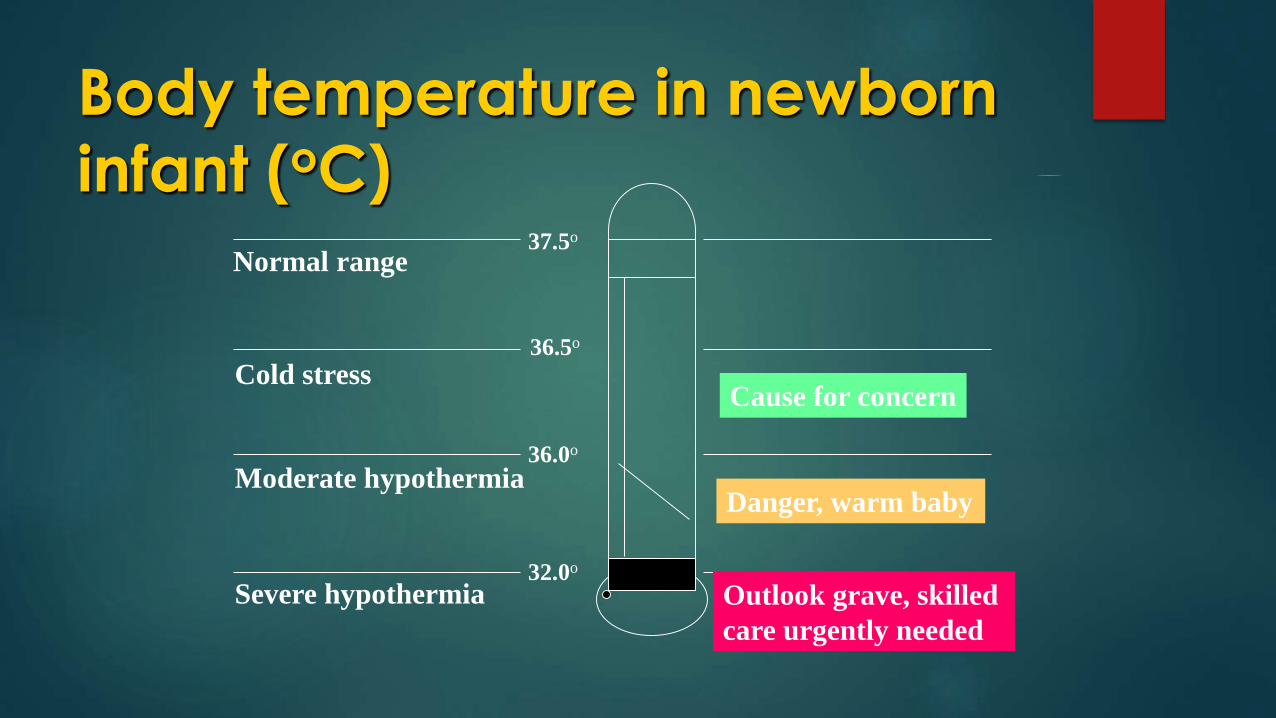
Body temperature in newborn
infant (oC)
Normal range
Cold stress
Moderate hypothermia
Severe hypothermia Outlook grave, skilled
care urgently needed
Danger, warm baby
Cause for concern
37.5o
36.5o
36.0o
32.0o
Failure to pass meconium and
urineFailure to pass meconium
Majority pass within 24 hrs Delayed passage May have passed in –utero Don’t miss Imperforate Anus Suspect obstruction PolyhydramniosFailure to pass urine
Majority pass within 48 hrs Many pass in LR Delayed passage Exclude obstructive uropathy or renal agenesis Oligohydamnios

Causes of vomiting*
Commonly Amniotic fluid gastritis
Systemic illness
CCF
Raised ICP – IVH, asphyxia
Metabolic disorders (CAH, galactosemia)
• Persistent, projectile or bile stained –
r / o intestinal obstruction
Causes of diarrhea Infective diarrhea* (often non breast fed
baby)
Maternal ingestion of drugs (ampicillin,
laxatives)
Metabolic disorders
Thyrotoxicosis
Maternal drug addiction
*Infective diarrhea needs treatment with
systemic antibiotics

Cyanosis
Peripheral
Normal at birth
Seen in extremities due to cold
Central
Always needs appropriate referral
Seen on Tongue (Mucosa)
Indicates cardiac or pulmonary disease

Peripheral cyanosis

Central cyanosis

Yellow staining of soles

Yellow Palms & Soles

Tracheo-esophageal fistula
Excessive drooling; choking; cyanosis
during feeds; respiratory distress
Failure to pass red rubber catheter
beyond 8 to 10 cm from mouth
Polyhydramnios
Look for other anomalies

Tracheo-esophageal fistula
Suspect cardiac disease
Cyanosis
Tachycardia
Murmur
Hepatomegaly
Shock
Cardiomegaly

Abnormal weight loss pattern
> 10 percent of birth weight in term
> 15 percent in preterm
> 5 percent acute weight loss

Danger signs
Lethargy
Hypothermia
Respiratory distress
Cyanosis
Convulsion
Abd. distension
Bleeding
Yellow palms/
soles
Excessive wt. loss
Vomiting
Diarrhea

Importance of Looking at Feet
• Temp
• Hb
• O2 Saturations
• BP
• Jaundice
• Maturity
• Deformity
Neonatal Transport - Goal
Taking Right New born at the Right
Time , By Right Personnel, to the
Right Place, By the Right form of
Transport, and receive the Right
Care Throughout .

Neonatal Transport - Practical constraints Facilities are scarce and not easily available
Families have poor resources
Organized transport services are not available.
No health provider is available to accompany the
baby
Mostly self-transport (Taxi/Rickshaw/public transport)
Facilities are not fully geared up to receive sick
neonates
Communication systems are non existent or inefficient

Neonatal Transport - Practical
constraintsSpecialized Transport – 108 ETS
Transport team imp
“Organised transport reduces
morbidity and mortality”

Prepare well before transport
Assess – necessity
Correct Hypothermia
Write a Note
Encourage mother to accompany
Arrange a care provider to accompany
Pre-transport stabilization:
STABLE:
Sugar,
Temperature,
Artificial breathing,
Blood pressure, (CRT)
Laboratory work,
Emotional support.

Care during transport
Ensure warm feet
Ensure an open airway
Check breathing
Provide feeds
[NB: Intravenous fluid administration during transport is best avoided]

Ensure warm transport
Skin to skin care (Kangaroo Mother Care)
Cover the baby
Transport incubator
Improvised containers

Neonatal Transport - Equipments
Communication
Explain the condition,
the prognosis
the reasons for referral of the baby to the
family.
Explain where to go and indicate whom to
contact.
Inform the referral facility beforehand, if
possible.
THANK YOU















![Jaundice in Neonate[1]](https://static.fdocuments.us/doc/165x107/577cdf6d1a28ab9e78b136c3/jaundice-in-neonate1.jpg)