Identification and Management of Twin-Twin Transfusion · Identification and Management of ... –...
49
Kenneth J. Moise, Jr., M.D. Professor of Obstetrics and Gynecology Professor of Pediatric Surgery McGovern Medical School – UT Health Co-Director The Fetal Center Children’s Memorial Hermann Hospital Identification and Management of Twin-Twin Transfusion
-
Upload
dangkhuong -
Category
Documents
-
view
220 -
download
0
Transcript of Identification and Management of Twin-Twin Transfusion · Identification and Management of ... –...

Kenneth J. Moise, Jr., M.D.Professor of Obstetrics and GynecologyProfessor of Pediatric SurgeryMcGovern Medical School – UT Health Co-DirectorThe Fetal CenterChildren’s Memorial Hermann Hospital
Identification and Management ofTwin-Twin Transfusion

• Royalties for multiple chapters on red cell alloimmunization in UpToDate®
• Consultant to LFB Biotechnologies in development of synthetic Rhesus immune globulin
• Consultant to Momenta Pharmaceuticals in the development of immunomodulation for the treatment of HDFN
Disclaimers

• Describe the proper timing of determining the chorionicity of a twin gestation
• Describe the risks and benefits of laser therapy for the treatment of twin-twin transfusion syndrome.
Twin-Twin TransfusionObjectives
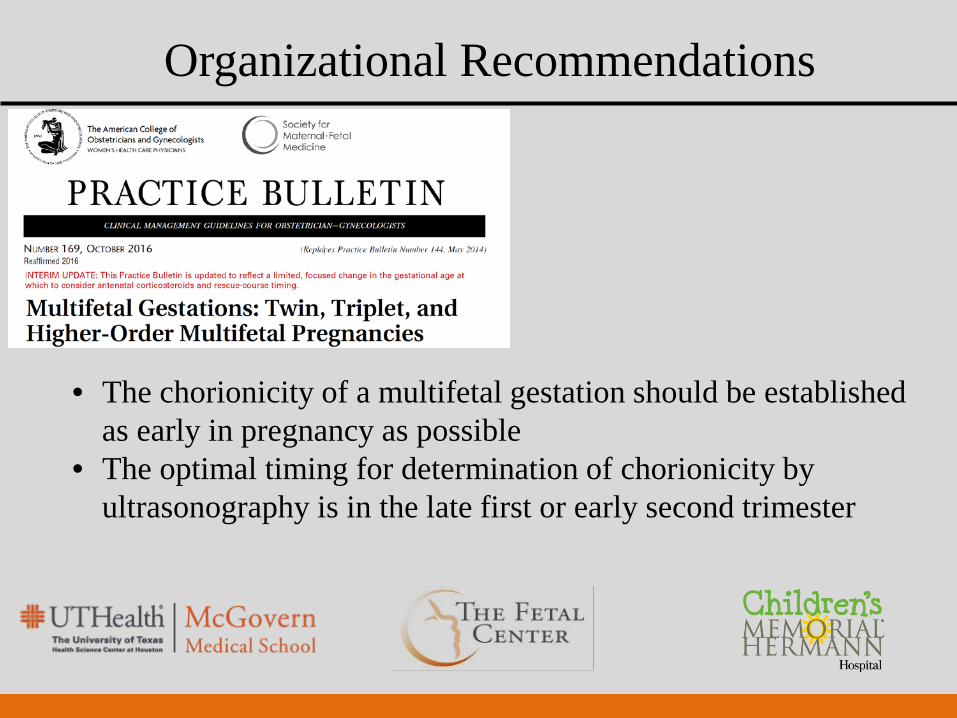
Organizational Recommendations
• The chorionicity of a multifetal gestation should be established as early in pregnancy as possible
• The optimal timing for determination of chorionicity by ultrasonography is in the late first or early second trimester

Diagnosis of Chorionicity
T sign
MonochorionicPlacenta
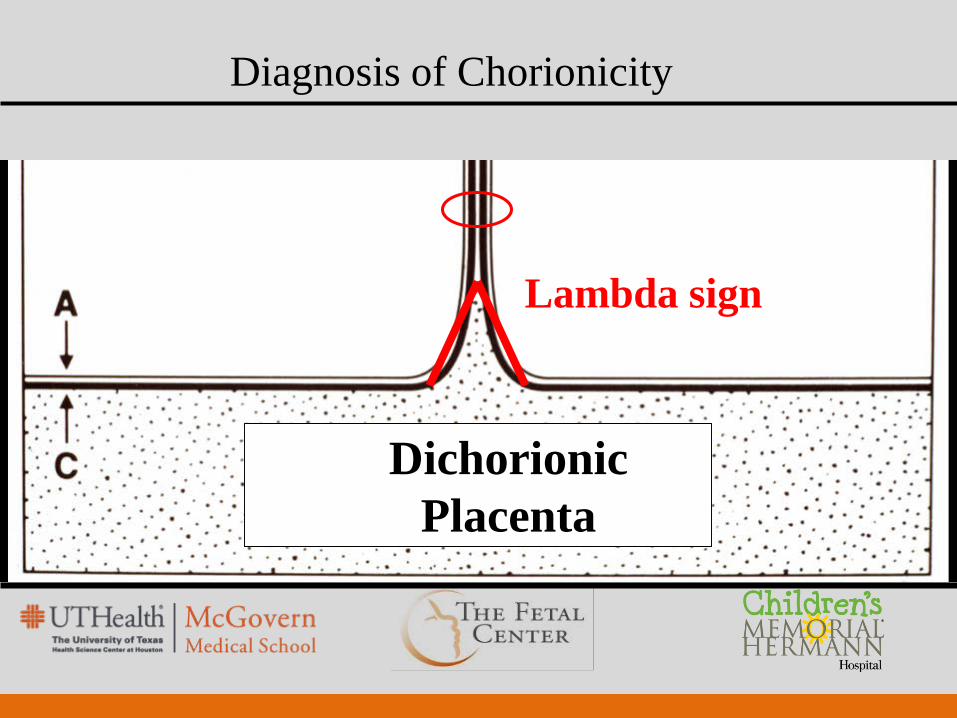
Lambda sign
DichorionicPlacenta
Diagnosis of Chorionicity
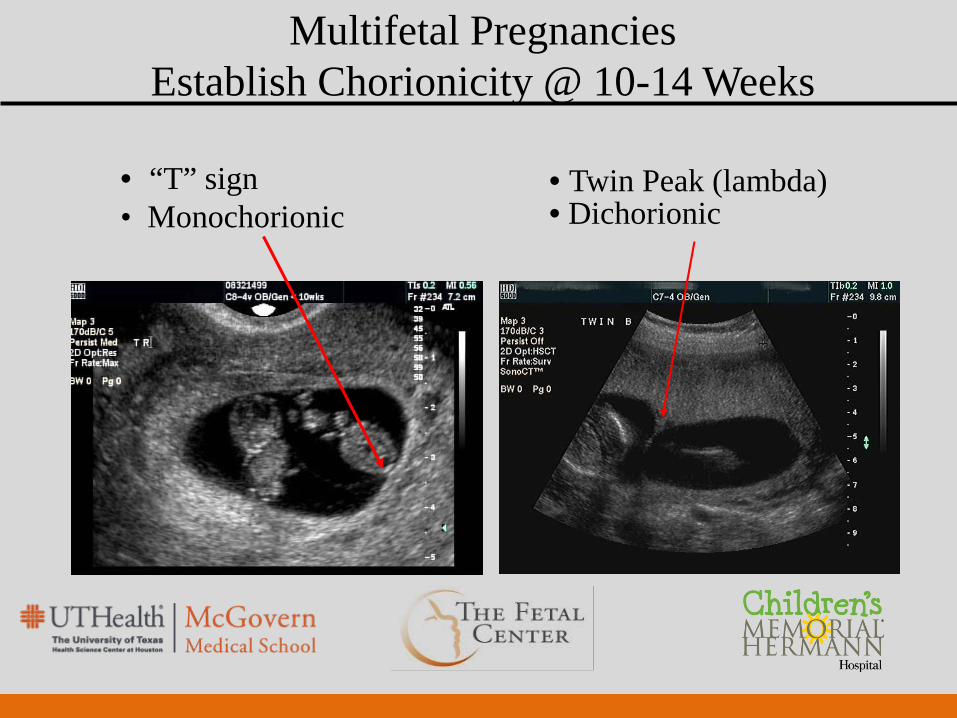
Multifetal Pregnancies Establish Chorionicity @ 10-14 Weeks
• “T” sign • Monochorionic
• Twin Peak (lambda) • Dichorionic

Take-home Message
There is NO diagnosis of twins

Monochorionic TwinsSurveillance
• Start at 16 weeks gestation• Evaluate MVP in both sacs and fetal bladders every
2 weeks • Anatomy scan at 20 weeks• Fetal echocardiogram
SMFM, Simpson. Am J Obstet Gynecol 2013;208:3-28
Monochorionic TwinsComplications
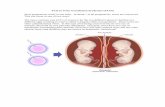
• Increased risk of anomalies (2.7X increased over dichorionic twins; 82% discordant)
• Death of a single twin (?)• Twin-twin transfusion (10 – 15%)• Selective IUGR (10 – 15%)• Twin anemia-polycythemia sequence (3 – 5%)• Acardiac twinning (TRAP sequence) (1%)

Risk of Death of a Monochorionic Twin

Monochorionic TwinsRisk of Single Demise
– Old theory of “bad humors” crossing to the live twin discounted– Acute hemodynamic changes the more likely etiology– No benefit from acute delivery
– 15% of cases associated with IUFD of co-twin• ↑ 5X over dichorionic twins
– 26% of survivors with neurologic sequelae• ↑ 5X over dichorionic twins
12
Risk of in-utero death of affected twin
Fusi et al. Obstet Gynecol 1991;78:517-20Hillman et al. Obstet Gynecol 2011;118:928-40


↓ BP ↓ BP
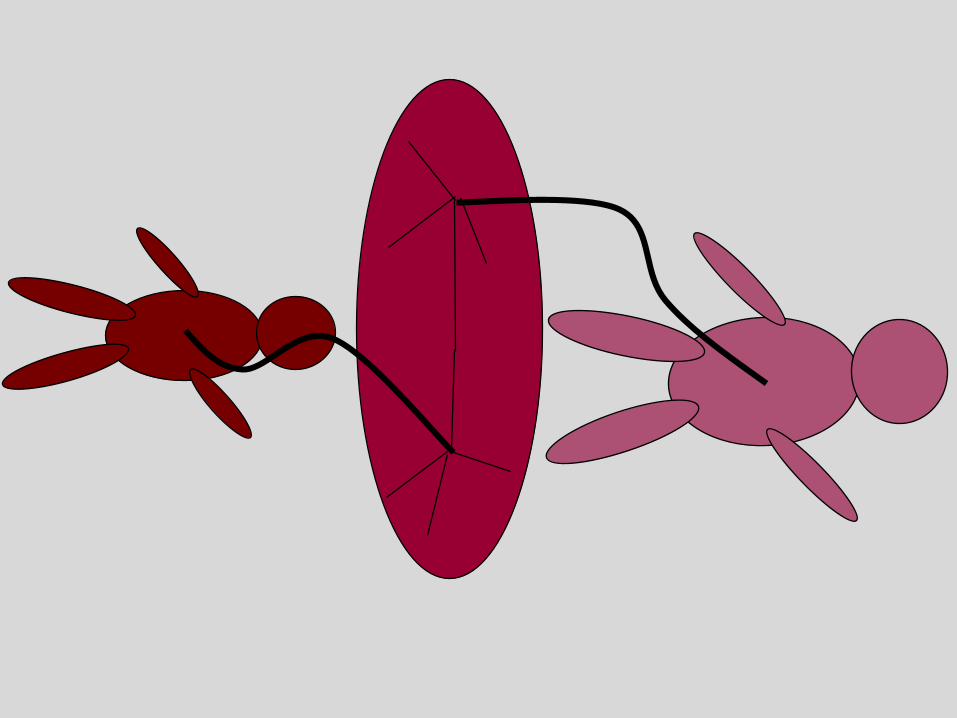

SelectiveIUGR

Monochorionic TwinsSelective IUGR

Monochorionic TwinsSelective IUGR
• One twin with normal growth and amniotic fluid
• Second twin with IUGR (< 10% EFW with > 20% discordance in growth between twins) and oligo
• Related to unequal placental sharing

Monochorionic TwinsSelective IUGR
• Type 1: Normal diastolic UA flow (29%)
• Type II: Persistent AREDV (22%)
• Type III: iAEDV (49%)
134 cases (< 10% EFW)
Gratacos et al. Ultrasound Obstet Gynecol 2007:30:28-34

Monochorionic TwinsSelective IUGR
Gratacos et al. Ultrasound Obstet Gynecol 2007:30:28-34
Parameter Type 1 Type II Type IIIGest Age @ delivery 35.4 30.7 31.6Unexpected death
Larger twin 2.6% 0% 6.2%
Smaller twin 2.6% 0% 15.4%
Parenchymal damage
Larger twin 0% 3.3% 19.7%
Smaller twin 0% 14.3% 2.0%
Twin-twinTransfusionSyndrome

Monochorionic TwinsEpidemiology of TTTS
Dickinson et al. Am J Obstet Gynecol 2000;182:706-12Saunders et al. Am J Obstet Gynecol 1992;166:820-4
• Complicates 10% of monochorionic twins
• One in 58 twin pregnancies
• One in 4,170 pregnancies
• Presentation @ <25-26 weeks associated with a 90% perinatal mortality

Monochorionic TwinsDiagnostic Criteria
• Same sex• Single placenta• Thin dividing membrane (or “T” sign documented
in the first trimester)• Massive hydramnios/oligohydramnios> 8 cm vertical pocket @ <20 wks; >10 cm >20 wks< 2 cm vertical pocket in second sac
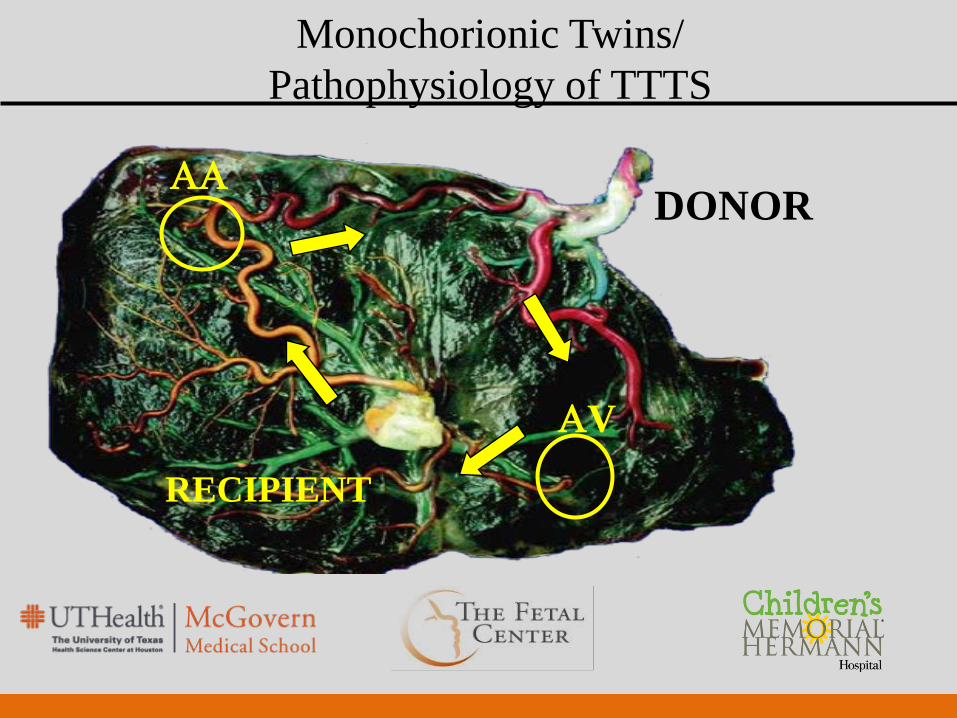
Monochorionic Twins/Pathophysiology of TTTS
ΑΑ
ΑV
DONOR
RECIPIENT

Monochorionic Twins/Pathophysiology of TTTS

Monochorionic Twins/TTTS Staging
Stage 1Donor MVP <2 cm;Recipient MVP >8-10 cm
Stage 2Absent bladder in donor twin; normal Doppler studies
14cm

Monochorionic Twins/TTTS Staging Stage 3
Normal
Umbilical Artery
Ductus Venosus
Umbilical Vein
Middle CerebralArtery
Abnormal
Recipient
Donor

Monochorionic Twins/TTTS Staging
Stage 5One or both fetuses have died
Stage 4

Monochorionic TwinsLaser for TTTS
• First performed by DeLia
• 3 cases at 18.5, 22 and 22.5 weeks’ gestation
• Delivery at 27 and 34 weeks for PPROM; third case delivered at 29 weeks due to pre-eclampsia
• 4/6 infants survived DeLia et al. Obstet Gynecol 1990;75:1046-53

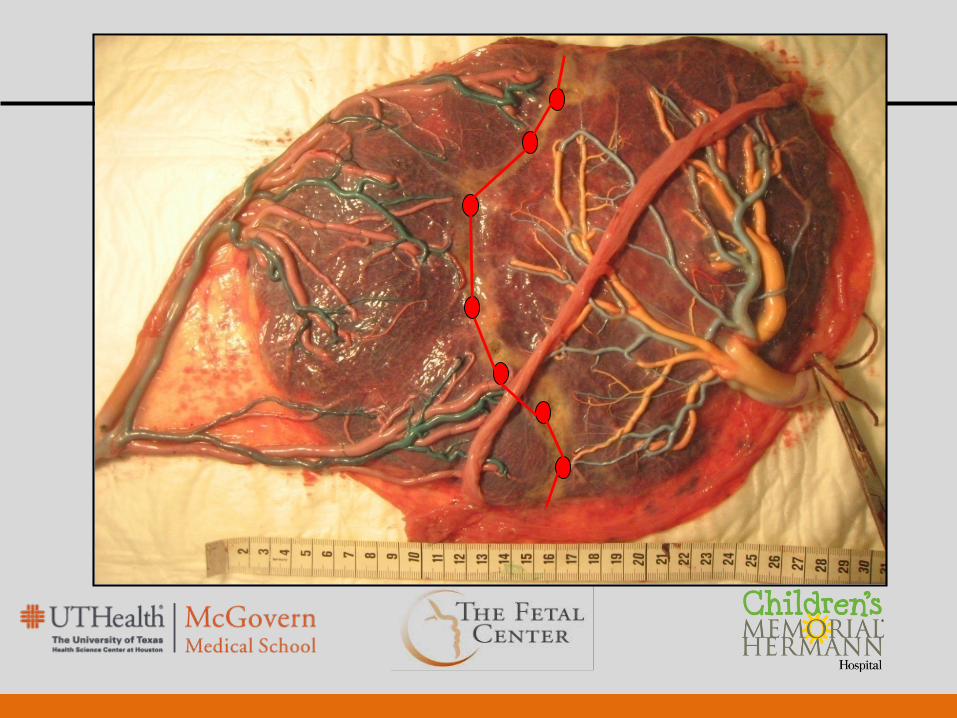
Laser Photocoagulation
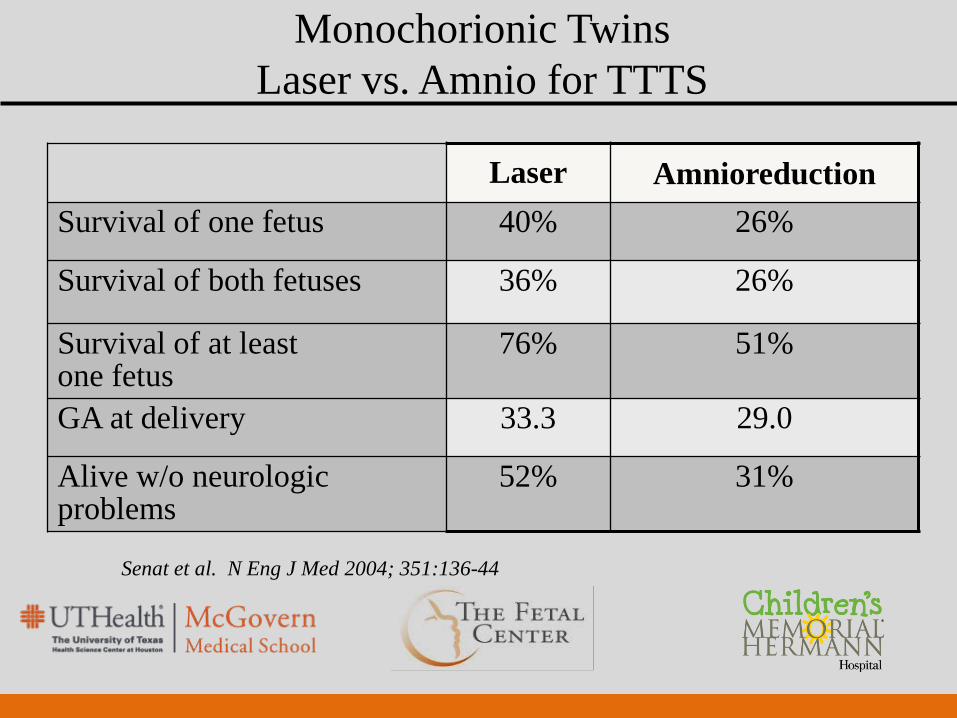
Monochorionic TwinsLaser vs. Amnio for TTTS
Laser AmnioreductionSurvival of one fetus 40% 26%
Survival of both fetuses 36% 26%
Survival of at least one fetus
76% 51%
GA at delivery 33.3 29.0
Alive w/o neurologic problems
52% 31%
Senat et al. N Eng J Med 2004; 351:136-44
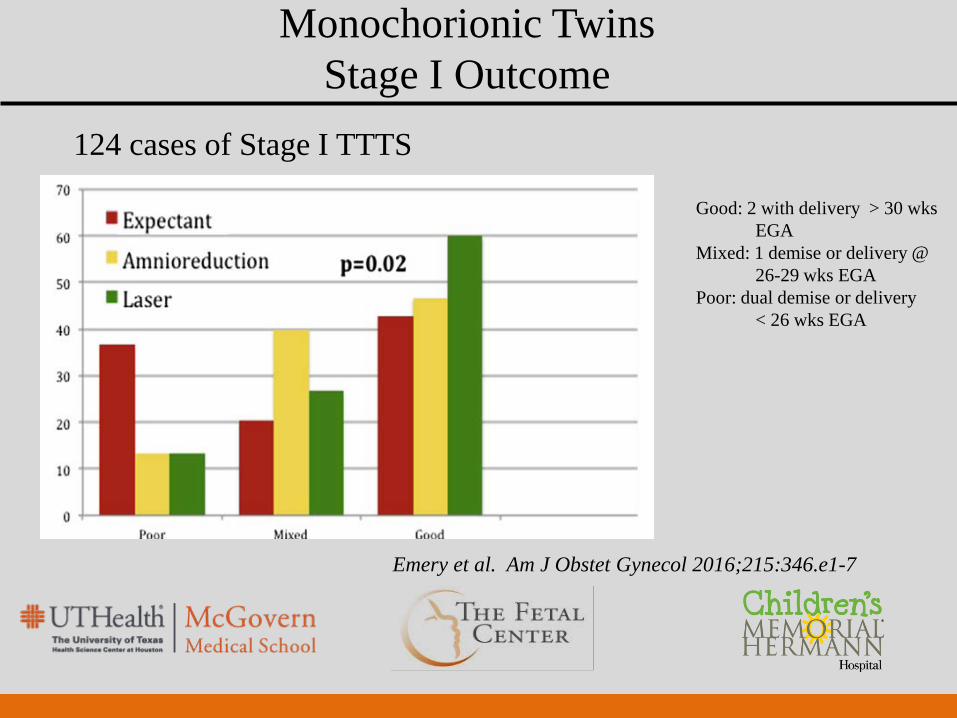
Monochorionic TwinsStage I Outcome
Emery et al. Am J Obstet Gynecol 2016;215:346.e1-7
124 cases of Stage I TTTS
Good: 2 with delivery > 30 wks EGA
Mixed: 1 demise or delivery @ 26-29 wks EGA
Poor: dual demise or delivery < 26 wks EGA

Monochorionic TwinsCandidates for Laser for TTTS
• Stage II – IV TTTS• Stage I with one of the following Severe maternal discomfort due to polyhydramnios Short cervix Amnioreduction for travel onlyo Septostomy – unable to perform laser

Monochorionic TwinsLearning Curve of Laser
Papanna et al. Am J Obstet Gynecol 2011;204:218 e1-4

Laser Photocoagulation Outcome

Laser Photocoagulation Outcome
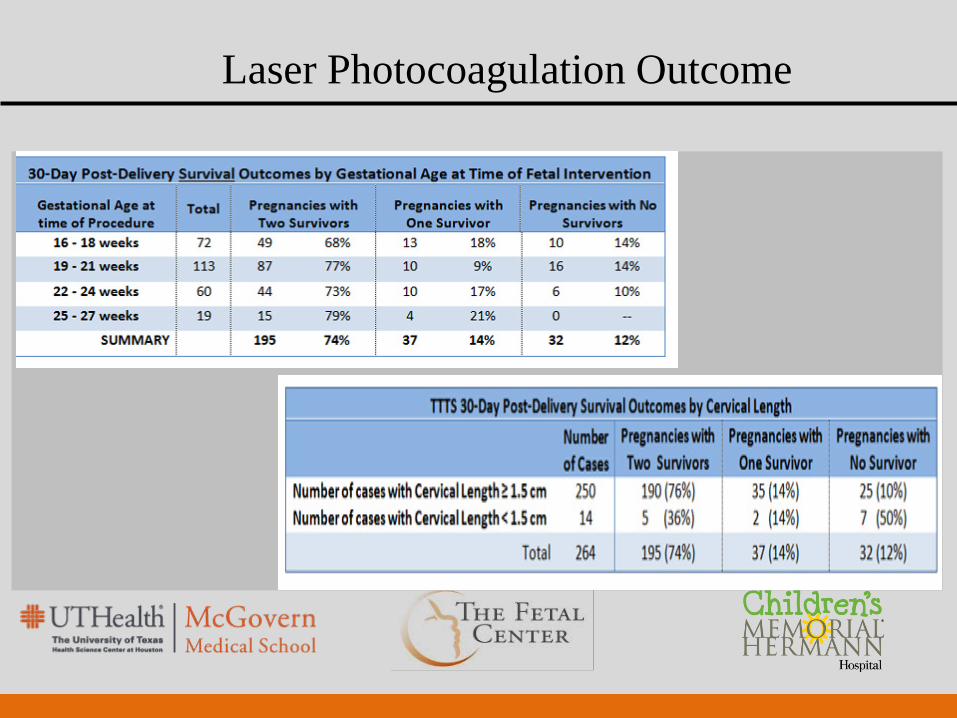
Laser Photocoagulation Outcome
Monochorionic TwinsComplications After Laser for TTTS
• Twin-anemia polycythemia sequence
• Reversed TTTS
• IUGR (typically the “donor”)
• Chorion-amnion separation
• Septostomy with tangled cords

Complications of TTTS
40

Monochorionic TwinsTwin Anemia-Polycythemia Sequence
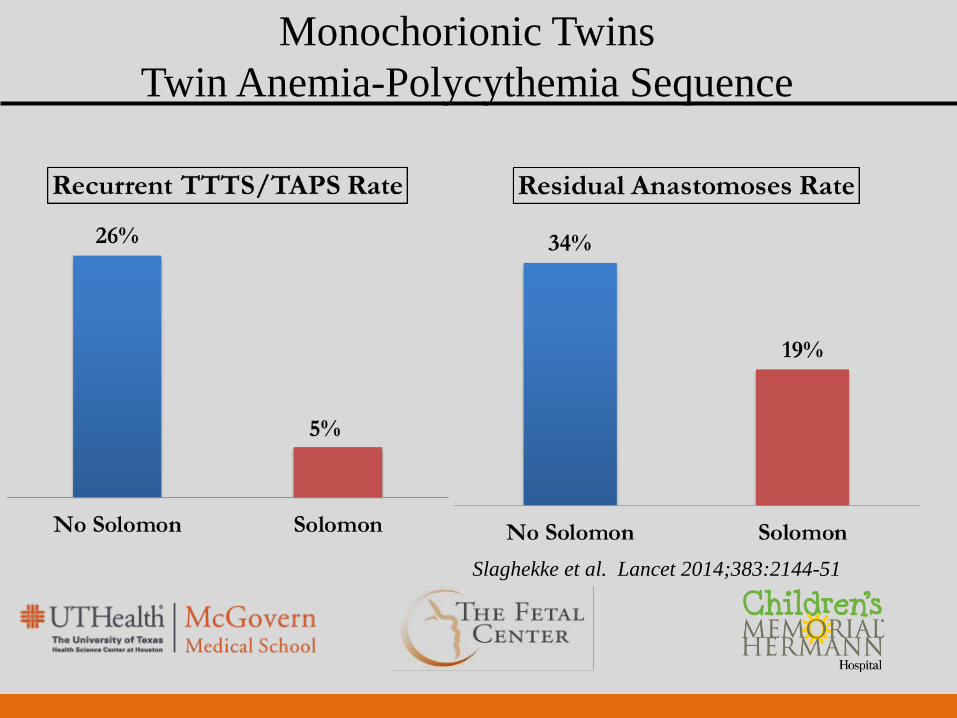
Monochorionic TwinsTwin Anemia-Polycythemia Sequence
Slaghekke et al. Lancet 2014;383:2144-51
Monochorionic TwinsTwin Anemia-Polycythemia Sequence
• Direct intravascular transfusion of anemic donor
• Direct intravascular transfusion of anemic donor w/ exchange transfusion of plethoric recipient
• Intraperitoneal transfusion of anemic donor
Genova et al. Fetal Diag Ther 2013;34:121-126

Monochorionic TwinsTwin Anemia-Polycythemia Sequence
Herway et al. Ultrasound Obstet Gynecol 2009;33:592-4

Monochorionic TwinsSurveillance After Laser for TTTS
• Ultrasounds weekly with Dopplers including MCA’s
Complications usually noted in first few weeks
• Delivery at 35 – 37 weeks

48