
IC 56: Distal Radius Gone Wrong- Management of the Malunion
48
All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH. No statement or presentation made is to be regarded as dedicated to the public domain. IC 56: Distal Radius Gone Wrong- Management of the Malunion Moderator(s): Jerry I. Huang, MD Faculty: Jerry I. Huang, MD, James M. Saucedo, MD, MBA, Alexander Lauder, MD, Robert J. Medoff, MD, Karl-Josef Prommersberger, MD, Prof Session Handouts Saturday, September 07, 2019 74TH ANNUAL MEETING OF THE ASSH SEPTEMBER 5 – 7, 2019 LAS VEGAS, NV 822 West Washington Blvd Chicago, IL 60607 Phone: (312) 880-1900 Web: www.assh.org Email: [email protected]
Transcript of IC 56: Distal Radius Gone Wrong- Management of the Malunion

All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH. No statement or presentation made is to be regarded as dedicated to the public domain.
IC 56: Distal Radius Gone Wrong-
Management of the Malunion
Moderator(s): Jerry I. Huang, MD
Faculty: Jerry I. Huang, MD, James M. Saucedo, MD, MBA, Alexander Lauder, MD,
Robert J. Medoff, MD, Karl-Josef Prommersberger, MD, Prof
Session Handouts
Saturday, September 07, 2019
74TH ANNUAL MEETING OF THE ASSH
SEPTEMBER 5 – 7, 2019
LAS VEGAS, NV
822 West Washington Blvd
Chicago, IL 60607
Phone: (312) 880-1900
Web: www.assh.org
Email: [email protected]

8/18/19
1
Distal'Radius'Gone'Wrong2Management'of'the'Malunion
Jerry'I.'Huang,'MDJames Saucedo,'MDAlexander Lauder, MD
Rob'Medoff,'MDKarl'Prommersberger,'MD
Malpractice*in*Hand*and*Wrist• Wrist fractures (48%)*and carpal tunnel (22%)*most common (Khan*and Giddins 2010)• Malunion/Nonunion the most commonadverse event in*UE*claims (Matsen et*al*2014)• Usually simple'fracturesw/*inadequate clinicalfollowGup and radiographs

8/18/19
2
Unacceptable*! Malunion??
• Change*of 20° in*volar*tilt! 10° dorsal*tilt or 25° volar*tilt• Radial*shortening >*5*mm• Articular stepoff >*2*mm• DRUJ*instability
Articular)Congruity)+)Concentricity
Extra&ArticularDistal.Radius.Malunion
Jerry.I..Huang,.MDAssociate.Processor
Dept of.Orthopaedics and.Sports.MedUniversity.of.Washington.Medical.Center
ASSH.2019.ICL

8/18/19
3
• Load%on%ulnocarpal joint increase18%to%42%%w/%2.5%mm%shortening
• Increased wrist pain withshortening >%4? 5mm
• Pain w/ extension + limited rotation
Extra?Articular%Malunions
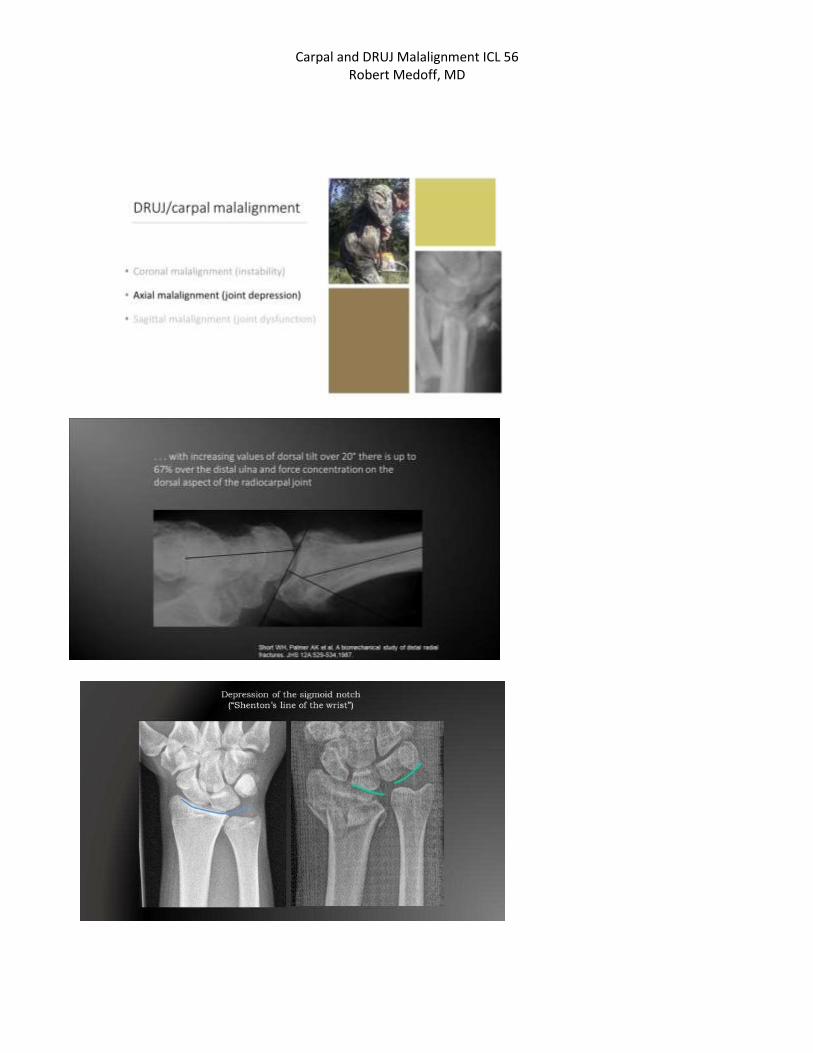
• 30º$dorsal$angulation• 50% load on the ulna (Short)• Increased strain DRUJ
(Hirahara 2003;$Kihara 1996)• Volar tilt > 20º$ ! Decreased
supination (Nishiwaki 2015)
VolarJDorsal$Tilt
Indications for Osteotomy
1) Ulnocarpal Abutment
2)9Radiocarpal subluxation3) Loss9of forearm rotation(supination)
Extra@Articular9Malunions
8/18/19
4
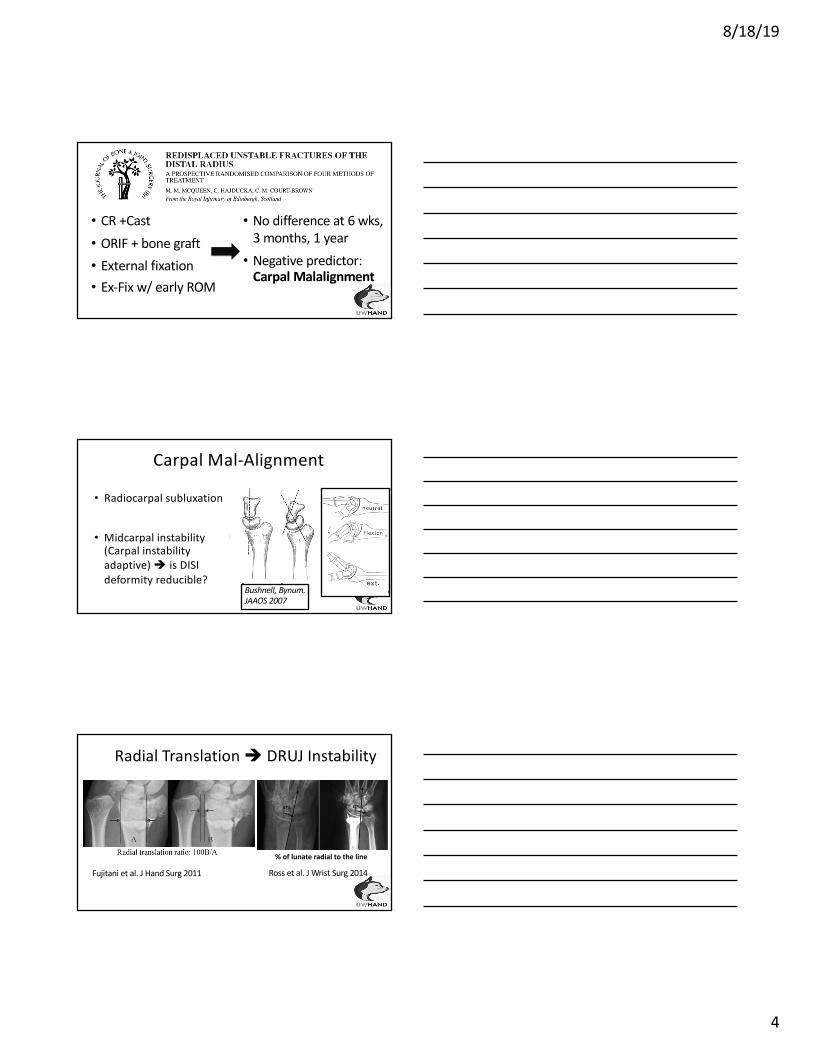
• CR#+Cast• ORIF#+#bone graft• External fixation• Ex6Fix#w/#early ROM
• No difference at 6#wks,#3#months,#1#year• Negative#predictor:#Carpal Malalignment
• Radiocarpal subluxation
• Midcarpal instability(Carpal instabilityadaptive)7! is DISI7deformity reducible?7
Bushnell,)Bynum.)JAAOS)2007
Carpal7Mal>Alignment
Radial&Translation&! DRUJ&Instability
%"of"lunate"radial"to"the"line
Fujitani et&al.&J&Hand&Surg&2011 Ross&et&al.&J&Wrist&Surg&2014&
8/18/19
5
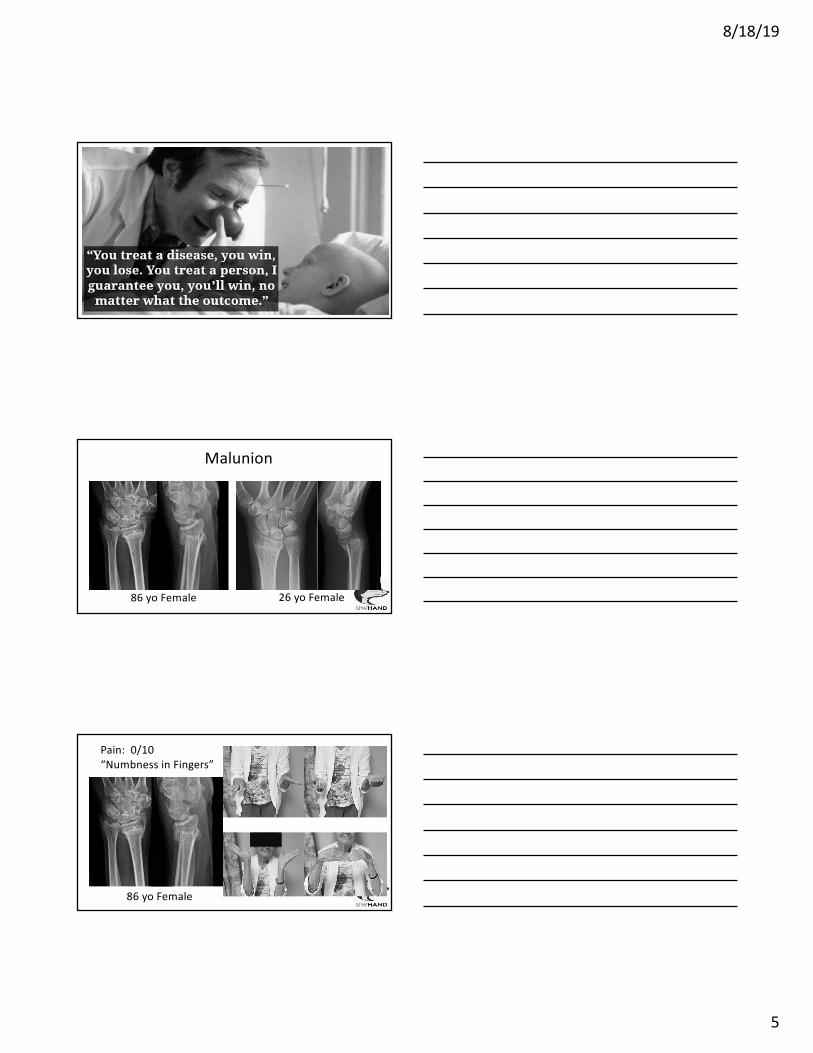
Malunion
86*yo Female 26*yo Female
86#yo Female
Pain:##0/10“Numbness#in#Fingers”

8/18/19
6
Functional*Outcomes*in*Pts >*70
ORIF*vs.*Cast*(Arora et*al*JOT*2008)
• Loss*of reduction in*Cast*group! dorsal*
tilt 1° vs.*24°,*height 1.5*mm*vs.*4.0*mm
• No difference in*Wrist FlexionNExtension*or PronationNSupination
• No difference in*DASH*+*PRWE*+*Pain
Oken U3298879+ Volar1Malunion
• 261yo female s/p181weeks of casttreatment• WF160/1WE160• Pronation160• Supination 20
Volar&Malunion
• Pain 1/10&at 6&wks• WF/WE:&60/60• Pronation&80• Supination 60

8/18/19
7
Extra&Articular,Malunion
• Closing vs.,OpeningWedge Osteotomy
• Surgical Approach:,Volar,vs.,Dorsal
• Bone Grafting?• Role of Ulnar Shortening Osteotomy
• Timing,of Surgery
Closing(Wedge(Osteotomy:(Biplanar
Bushnell,)Bynum.)JAAOS)2007• Easy,(direct bone contact• Radius(shortened
Opening'Wedge:'Most'Common
• Osteotomy parallel'to joint line (coronal +sagittal)• Restore tilt +'inclination +'HEIGHT

8/18/19
8
Volar&vs.&Dorsal&Osteotomy
• Anatomic volar,locking plates• Improved stability• Reduce bone to plate• Less soft,tissue irritation• Structural vs.,Cancellous:,nodifference (Ring,et,al.,2002)
Miyake,et,al,CORR,2011
Volar,vs.,Dorsal,Osteotomy
Autograft vs.,Allograft
• Ozer et,al,2011:,14,pts with nograft vs.,14,pts with allograft• Tarallo et,al,2014:,20,pts withvolar,plating w/,no bone grafting• With no bone grafting:,All,healedw/o,loss of correction

8/18/19
9
Variations:*Opening*Wedge
Bushnell,)Bynum.)JAAOS)2007(Thiavaios and)McKee)JOT)2003)
Bushnell,)Bynum.)JAAOS)2007(Watson)and)Castle)JHS)1988)
Sliding'Osteotomy Trapezoidal'Osteotomy
26#yo Male#s/p#Fall#20#Feet
• Injury 6#weeks ago• Gross#deformityleft distal#radius• Unable to flex thethumb IP#joint
6"Weeks"Post*Op
• Opening wedgecorrective osteotomy• Bone allograft chips• FPL"reconstruction w/"free tendon graft
8/18/19
10
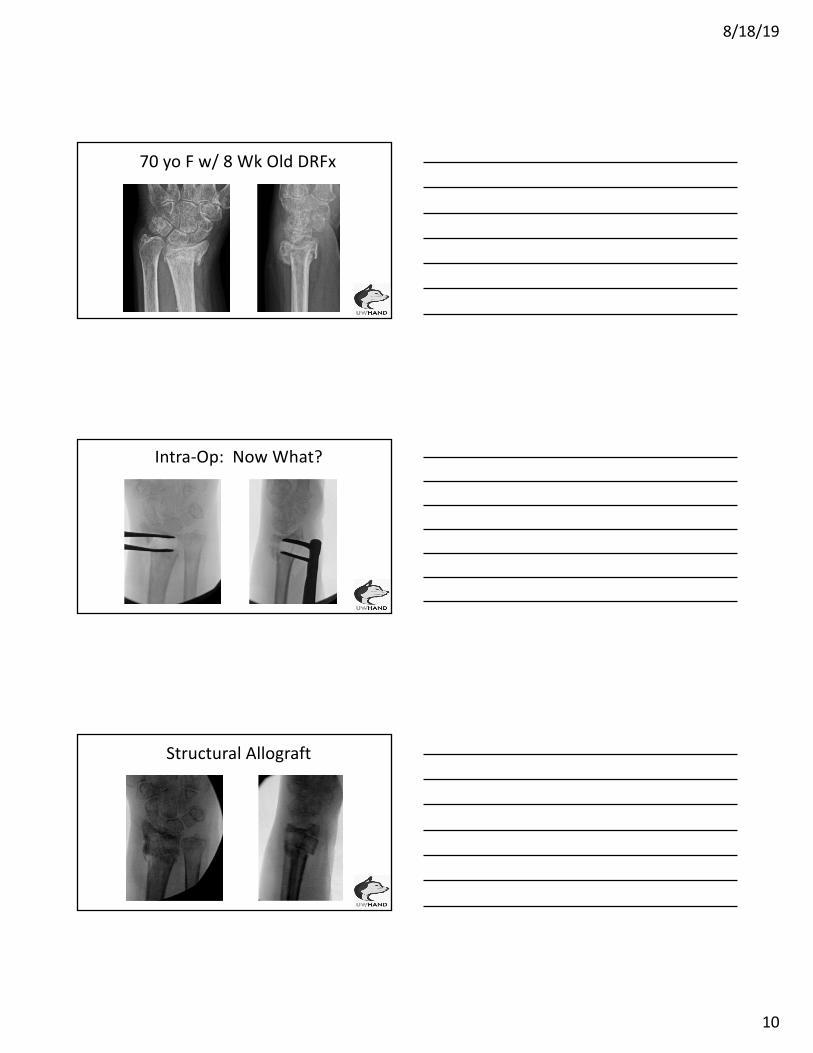
70#yo F#w/#8#Wk Old#DRFx
Intra&Op:**Now*What?
Structural(Allograft

8/18/19
11
3"Months"Post*Op*Good"to"be"Lucky
• Avg 5.6(mm• Fast,(Reliable• Short(recovery

8/18/19
12
Corrective)OsteotomyRadial
MeasurementsRadioulnarLength
Shortening>45mm
DRUJ4Arthrosis Surgery4Indicated
Unacceptable Unacceptable No No Opening)Wedge)Osteotomy
Acceptable Unacceptable Yes No Ulnar)ShorteningOsteotomy
Unacceptable Unacceptable Yes No Closing)Wedge)+)Ulnar Shortening
Unacceptable Unacceptable Yes/No Yes Opening)Wedge+)DRUJ)Salvage
• Nascent (mean 8.2-weeks)-vs.-Mature (mean 39.9-weeks)• Similar outcome• Early:-technically easier correction• Early-intervention if disability
• Treat&the&Patient&Not&the&X.ray• Indications: radial&shortening&>&5&mm&and&dorsal&angulation&30°rees• DRUJ pain and loss of supination• Early&corrective&osteotomy• Bone&allograft&or&no&graft
Summary

74th Annual meeting of the ASSH September 7, 2019; 6:45-7:45a ICL: Distal radius gone wrong - management of the malunion Dorsal spanning wrist plate for distal radius malunion Alexander Lauder, MD Disclosures: none Learning Objectives
• Indications
• Plating options: second vs third metacarpal
• Anatomic considerations
• Surgical technique
• Pearls

Indications
• Distal radius correctional osteotomy is indicated for patients with a malunion who have: pain with motion or activity, weakness, instability, pain with forearm motion, decreased grip strength, decreased range of motion.
• Contraindications include: advanced arthritic changes (radiocarpal or intercarpal), fixed carpal malalignment, serious medical illness/comorbidity
• Dorsal spanning bridge plate fixation has been described for treatment of unstable comminuted distal radial fractures, bilateral wrist fractures with metaphyseal bone loss or diaphyseal extension, complex injuries requiring extensive soft-tissue and osseous reconstruction, injuries necessitating early weight-bearing and transfer, dorsal shear fractures, clinically unstable patients, osteoporotic fragility fractures, and as a salvage option for the treatment of distal radial nonunion.1-4
• The plate is temporarily fixed to the second or third metacarpal under the extensor compartment to the radial shaft, bridging the wrist joint for approximately 12 weeks. The plate utilizes and supplements ligamentotaxis with indirect reduction, provides a dorsal buttress to prevent fracture displacement after reduction, and is removed after fracture-healing has been achieved.1,3,5,6
• While not specifically described previously for distal radius malunion, the principles of malunion correction and fixation have been well described to include anatomic reduction, stable construct fixation for the duration of healing, and a treatment plan that allows for the restoration of functional wrist kinematics.7,8 The published literature supports the use of bridge plating demonstrating functional outcomes and complication rates similar to those associated with other methods for the treatment of distal radial fractures.9,10
• Specific indications for malunion correctional osteotomy with use of a bridge plate include: very distal extra-articular malunions where adequate fixation is difficult, poor soft tissue environment on the volar wrist, osteoporosis, patients who necessitate early weight bearing and transfer, and as a bail out option when other planned fixation fails or is not adequate.
Plating options: second vs third metacarpal
• Cadaveric biomechanical studies have compared (1) second metacarpal dorsal spanning wrist plating (DSWP) to external fixation with regard to flexion-extension bending moment,2 (2) volar locking plate fixation to second metacarpal DSWP fixation in an axial loading, crutch weight bearing simulating construct,11 and (3) second metacarpal compared to third metacarpal DSWP fixation with assessment of flexion-extension bending strength.12
• Recent studies support that the third metacarpal provides a stiffer construct, but that both provide enough stability to allow clinical healing.12
• Second metacarpal plating advantages: Plating to the second metacarpal may provide potentially greater grip strength as the hand is placed in slight ulnar deviation, less tendon excursion over the plate, and has the potential for improved restitution of radial length, radial inclination, and volar tilt of the radial column1,2,13

• Third metacarpal plating advantages: Plating to the third metacarpal may be advantageous in situations which direct visualization of the osteotomy is needed for reduction, bone-grafting is used to fill a defect, or a subchondral buttress screw is needed.5,6
Surgical technique
• Osteotomy. Distal radius malunion is typically associated with dorsal or volar angulation, radial shortening, and possible loss of radial inclination. A variety of approaches have been described (volar, dorsal, radial, combination). Adequate exposure should allow osteotomy at the center of rotation and angulation (CORA), while protecting vital anatomical structures. Typically, bridge plating is used for opening wedge osteotomies as distraction is easily achieved with the plate.
• Second or third metacarpal bridge plate fixation. The surgical technique allows the surgeon to choose either the third metacarpal or the second metacarpal for distal fixation based on malunion characteristics, surgeon preference, surgical approach, and supplemental fixation.1,5,6,10 The patient is anesthetized and placed supine with the extremity placed on a radiolucent hand table. Sterile finger traps (index and middle finger) can be used to provide approximately 4.5 kg (10 lbs) of longitudinal traction.
• After osteotomy, reduction is attempted with the use of indirect capsular ligamentotaxis using longitudinal traction combined with correction of the angular deformity. If
Study Comparison Model Size Loading Principal Conclusions
Wolf et al. J Hand Surg Am. 20062
External fixator versus dosrsal wrist spanning plate
Cadaveric Extra-articular distal radius fracture
5 pairs Flexion, Extension
Fracture fixation was more stable with dorsal wrist spanning plate than external fixator in both flexion and extension
Huang et al. Hand (N Y). 201711
Dorsal wrist spanning plate to second metacarpal versus volar locking plate
Cadaveric Extra-articular distal radius fracture
5 matched pairs
Axial load simulating crutch weight-bearing
Fracture fixation with a volar locking plate was more stable than dorsal wrist spanning plate to the second metacarpal
Alluri et al. J Hand Surg Am. 201712
Dorsal wrist spanning plate fixation to second versus third metacarpal
Cadaveric Extra-articular distal radius fracture
10 matched pairs
Flexion, extension
Fixation to the third metacarpal resulted in greater stiffness in flexion compared to second metacarpal. No significant difference in stiffness in extension or maximum displacement in flexion or extension.
Guerrero et al. 2019. Unpublished data, under review
Dorsal wrist spanning plate fixation to second versus third metacarpal, versus third metacarpal with an intrafragmentary screw
Cadaveric Intra-articular distal radius fracture
14 matched pairs
Axial load Fixation to the third metacarpal more effectively resisted fracture displacement than fixation to the second. Lunate facet screw fixation further stiffened the construct at loads of 150 N or greater.

reduction is successful, the plate application then proceeds. If acceptable reduction is not possible, provisional fixation (i.e., temporary plate fixation, Kirschner wire fixation, lamina spreader) may be required.10
• The plate is positioned over the skin, with use of image intensification (from the radial shaft to either the second or third metacarpal), to guide the placement of each incision.
• Second metacarpal fixation (two incisions). A 4 to 5-cm incision is made over the metacarpal base and the insertions of the extensor carpi radialis longus (ECRL) on the second metacarpal base and the extensor carpi radialis brevis (ECRB) on the third metacarpal base are identified. A second incision is then made over the radial shaft at the level of the planned plate placement, commonly just proximal to the outcropping muscle bellies of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB), which are retracted to identify the interval between the ECRL and the ECRB in the proximal incision.
• Third metacarpal fixation (three incisions). A 4 to 5-cm incision is made at the base of the third metacarpal. A second incision is positioned just ulnar to the Lister tubercle, and the third compartment is opened to allow extensor pollicis longus (EPL) tendon transposition radial to the tubercle. The extensor tendons in the fourth compartment are then elevated ulnarly to allow plate placement on the floor of this compartment, and a 2-cm segment of the posterior interosseous nerve may be excised to prevent neuroma. A third incision is made on the dorsoradial aspect of the radius as decribed above.
• In both techniques, an elevator is used to clear a track from the proximal incision to the distal incision in order to allow for unobstructed passage of the plate. The plate can either be advanced distally starting within the proximal incision, or vice versa, with care being taken to avoid extensor tendon impingement 14,24. Plate fixation is carried out with a combination of cortical locking and non-locking screws.1,6,10

Anatomic considerations
From JBJS Rev. 2017 Feb 14;5(2).10
• Second metacarpal fixation places the radial sensory nerve at risk.14
• Third metacarpal fixation risks tendon entrapment (EPL, APL, APB) unless an additional incision is made over the radiocarpal joint.14,15
Pearls
• Osteotomy. Typically opening wedge with bone grafting.
• Longitudinal traction via finger traps (index and middle finger), 4.5kg (10lbs). Adjust amount of traction as needed.
• Reduction. Placement of towel bumps under the wrist to help correct deformity. Lamina spreader may be used to help open the malunion site. Provisional fixation with k-wires or temporary plates may be used.
• Plate fixation distally to the metacarpal allows deformity correction with the use of the plate prior to fixing the plate to the radial shaft
• Bone graft. Opening wedge defects with one cortex in contact can be grafted with cancellous bone graft. If both the volar and dorsal cortex are distracted out of contact with each other, structural (corticocancellous) graft is typically used.
• Subchondral screw placement enhances fixation at the osteotomy site
• The bridge plate is removed after the osteotomy is healed at around 12 weeks.

References 1. Hanel DP, Lu TS, Weil WM. Bridge plating of distal radius fractures: the Harborview
method. Clin Orthop Relat Res. Apr 2006;445:91-99. 2. Wolf JC, Weil WM, Hanel DP, Trumble TE. A biomechanic comparison of an internal
radiocarpal-spanning 2.4-mm locking plate and external fixation in a model of distal radius fractures. J Hand Surg Am. Dec 2006;31(10):1578-1586.
3. Richard MJ, Katolik LI, Hanel DP, Wartinbee DA, Ruch DS. Distraction plating for the treatment of highly comminuted distal radius fractures in elderly patients. J Hand Surg Am. May 2012;37(5):948-956.
4. Mithani SK, Srinivasan RC, Kamal R, Richard MJ, Leversedge FJ, Ruch DS. Salvage of distal radius nonunion with a dorsal spanning distraction plate. J Hand Surg Am. May 2014;39(5):981-984.
5. Ruch DS, Ginn TA, Yang CC, Smith BP, Rushing J, Hanel DP. Use of a distraction plate for distal radial fractures with metaphyseal and diaphyseal comminution. J Bone Joint Surg Am. May 2005;87(5):945-954.
6. Ginn TA, Ruch DS, Yang CC, Hanel DP. Use of a distraction plate for distal radial fractures with metaphyseal and diaphyseal comminution. Surgical technique. J Bone Joint Surg Am. Mar 2006;88 Suppl 1 Pt 1:29-36.
7. Lafontaine M, Hardy D, Delince P. Stability assessment of distal radius fractures. Injury. Jul 1989;20(4):208-210.
8. Handoll HH, Madhok R. Surgical interventions for treating distal radial fractures in adults. Cochrane Database Syst Rev. 2003(3):CD003209.
9. Lauder A, Agnew S, Bakri K, Allan CH, Hanel DP, Huang JI. Functional Outcomes Following Bridge Plate Fixation for Distal Radius Fractures. J Hand Surg Am. Aug 2015;40(8):1554-1562.
10. Lauder A, Hanel DP. Spanning Bridge Plate Fixation of Distal Radial Fractures. JBJS Rev. Feb 14 2017;5(2).
11. Huang JI, Peterson B, Bellevue K, Lee N, Smith S, Herfat S. Biomechanical Assessment of the Dorsal Spanning Bridge Plate in Distal Radius Fracture Fixation: Implications for Immediate Weight-Bearing. Hand (N Y). Apr 01 2017:1558944717701235.
12. Alluri RK, Bougioukli S, Stevanovic M, Ghiassi A. A Biomechanical Comparison of Distal Fixation for Bridge Plating in a Distal Radius Fracture Model. J Hand Surg Am. Sep 2017;42(9):748 e741-748 e748.
13. Pryce JC. The wrist position between neutral and ulnar deviation that facilitates the maximum power grip strength. J Biomech. 1980;13(6):505-511.
14. Dahl J, Lee DJ, Elfar JC. Anatomic relationships in distal radius bridge plating: a cadaveric study. Hand (N Y). Dec 2015;10(4):657-662.
15. Lewis S, Mostofi A, Stevanovic M, Ghiassi A. Risk of tendon entrapment under a dorsal bridge plate in a distal radius fracture model. J Hand Surg Am. Mar 2015;40(3):500-504.

Carpal and DRUJ Malalignment ICL 56
Robert Medoff, MD

Carpal and DRUJ Malalignment ICL 56 Robert Medoff, MD

Carpal and DRUJ Malalignment ICL 56 Robert Medoff, MD

Carpal and DRUJ Malalignment ICL 56 Robert Medoff, MD

Carpal and DRUJ Malalignment ICL 56 Robert Medoff, MD
Carpal and DRUJ Malalignment ICL 56 Robert Medoff, MD

Carpal and DRUJ Malalignment ICL 56 Robert Medoff, MD

Carpal and DRUJ Malalignment ICL 56 Robert Medoff, MD
Carpal and DRUJ Malalignment ICL 56 Robert Medoff, MD

Carpal and DRUJ Malalignment ICL 56 Robert Medoff, MD

Carpal and DRUJ Malalignment ICL 56 Robert Medoff, MD
Notes:

Klinik für
Handchirurgie
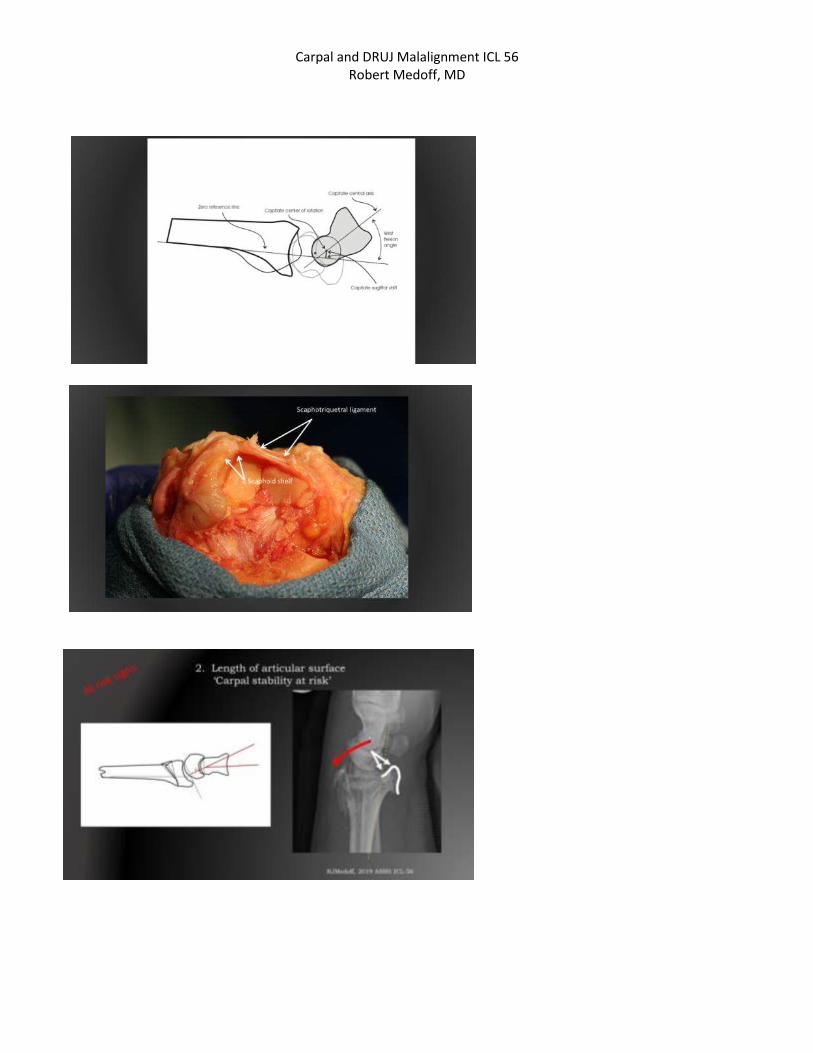
Corrective Osteotomy for Inta-articular Malunion
of the Distal Radius
Karl-Josef Prommersberger


Baratz et al: J Hand Surg 1996;21A:183-188
Pressure distribution in
intraarticulare malunion

• intra-articular malunion
– step-off
– gap
– radiocarpal joint
– distal radioulnar joint
Deformity

Techniques
• „classic“
• dorsal: capsulotomy,
visual control
• volar: fluoroscopic
control
• computer-assisted virtual
planning with patient-
specific guides
• arthroscopic
F. del Pinal

preoperative work-up
Ring D, Prommersberger KJ, Jupiter JB: JBJS 2005;87-A:1503-1509
Prommersberger KJ, Ring D, Jupiter JB: JBJS 2006;88-A Suppl 1 Pt 2:202-211

preoperative work-up
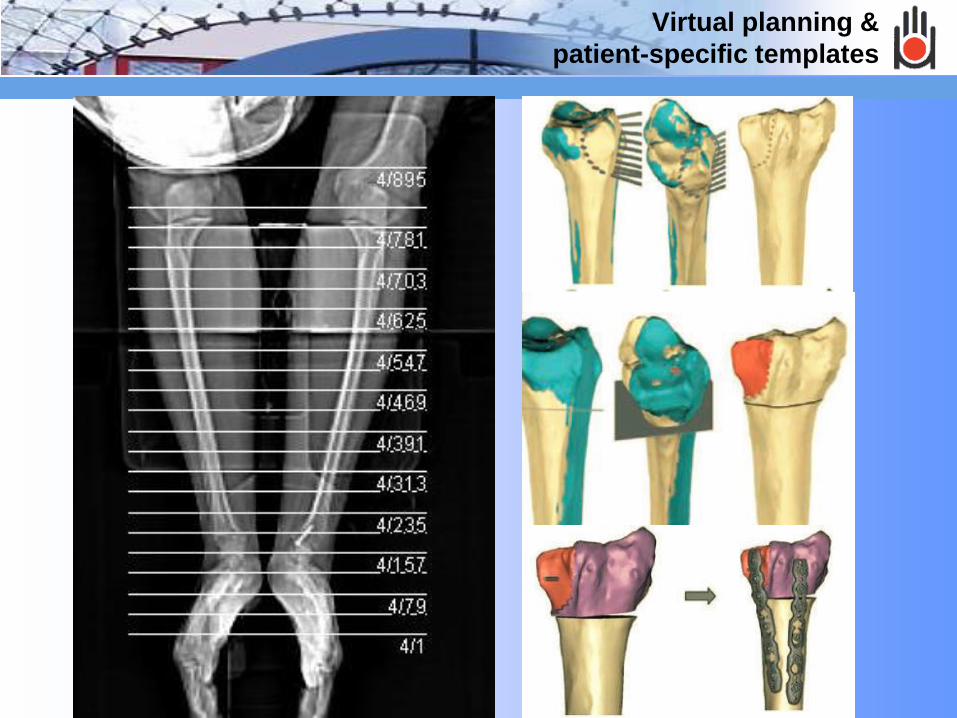
Virtual planning &
patient-specific templates

future
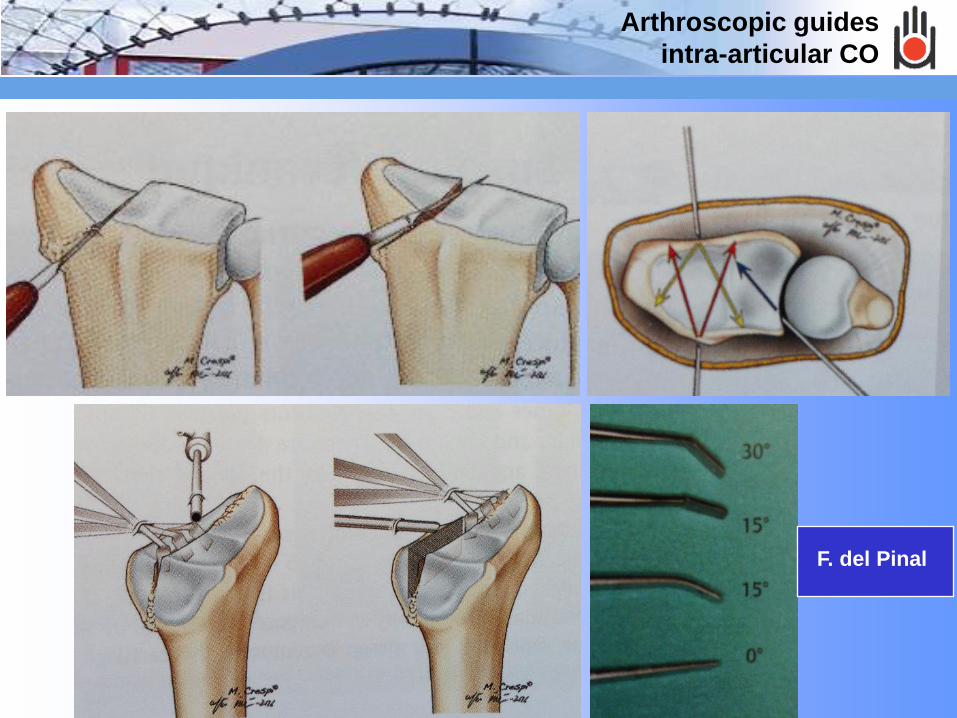
Arthroscopic guides
intra-articular CO
F. del Pinal
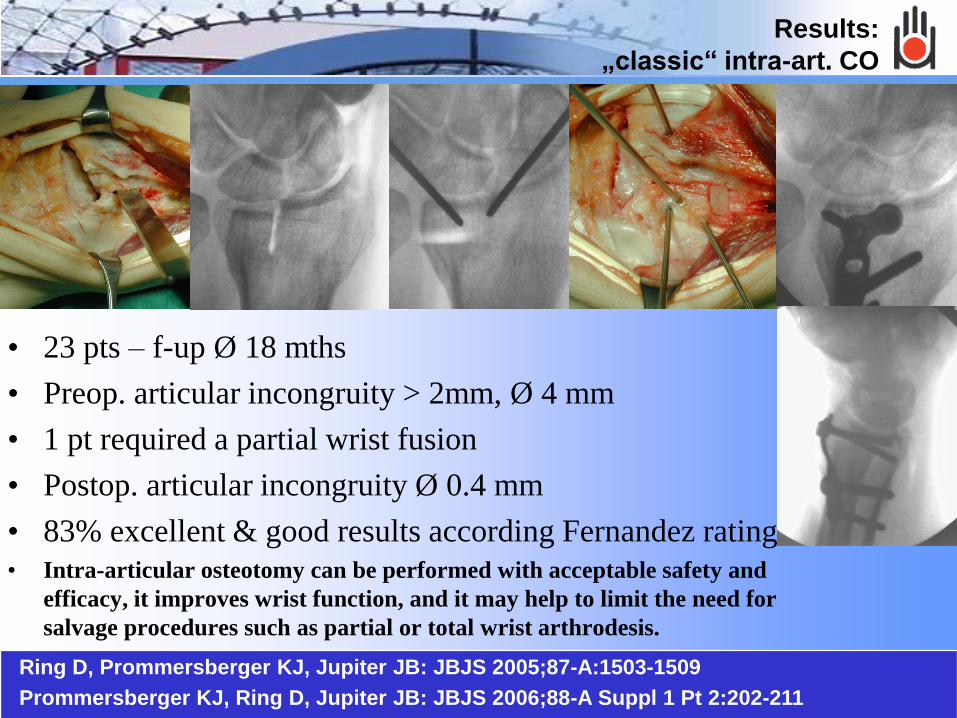
Results:
„classic“ intra-art. CO
Ring D, Prommersberger KJ, Jupiter JB: JBJS 2005;87-A:1503-1509
Prommersberger KJ, Ring D, Jupiter JB: JBJS 2006;88-A Suppl 1 Pt 2:202-211
• 23 pts – f-up Ø 18 mths
• Preop. articular incongruity > 2mm, Ø 4 mm
• 1 pt required a partial wrist fusion
• Postop. articular incongruity Ø 0.4 mm
• 83% excellent & good results according Fernandez rating
• Intra-articular osteotomy can be performed with acceptable safety and
efficacy, it improves wrist function, and it may help to limit the need for
salvage procedures such as partial or total wrist arthrodesis.
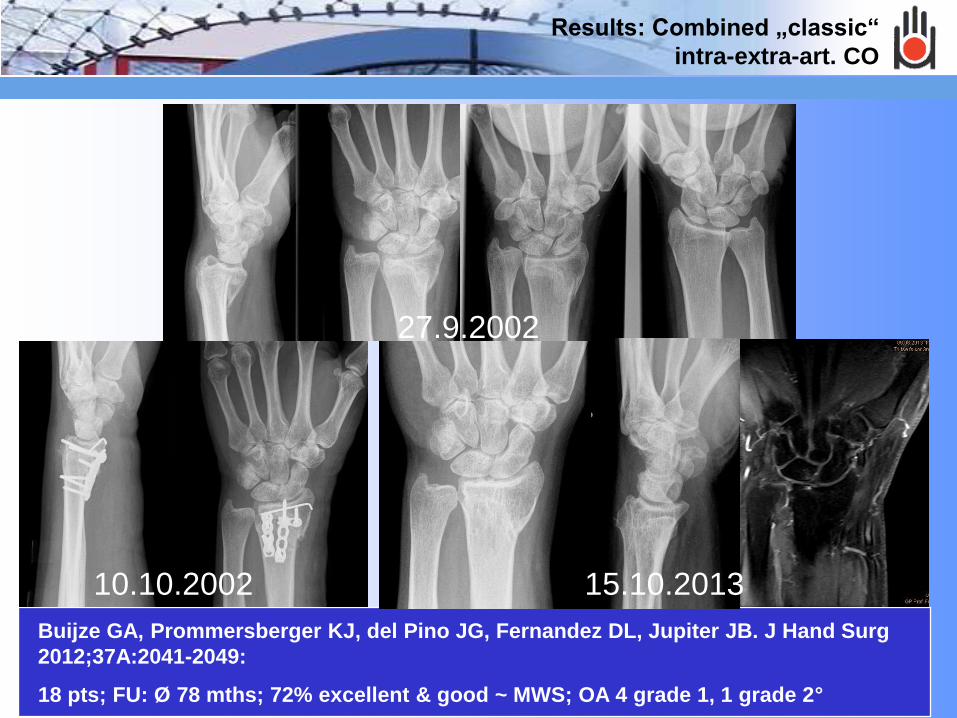
Results: Combined „classic“
intra-extra-art. CO
Buijze GA, Prommersberger KJ, del Pino JG, Fernandez DL, Jupiter JB. J Hand Surg
2012;37A:2041-2049:
18 pts; FU: Ø 78 mths; 72% excellent & good ~ MWS; OA 4 grade 1, 1 grade 2°
27.9.2002
10.10.2002 15.10.2013
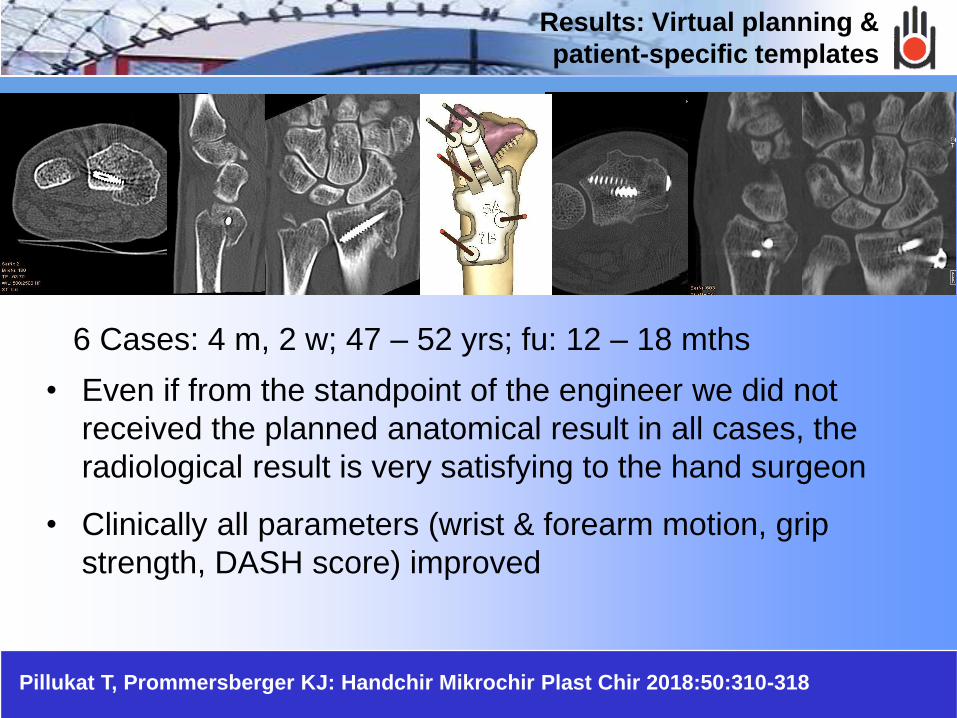
• Even if from the standpoint of the engineer we did not
received the planned anatomical result in all cases, the
radiological result is very satisfying to the hand surgeon
• Clinically all parameters (wrist & forearm motion, grip
strength, DASH score) improved
6 Cases: 4 m, 2 w; 47 – 52 yrs; fu: 12 – 18 mths
Results: Virtual planning &
patient-specific templates
Pillukat T, Prommersberger KJ: Handchir Mikrochir Plast Chir 2018:50:310-318

Results: Virtual planning &
patient-specific templates
• Makes the surgery easier
• Needs a more extensiv approach
• Needs less time for surgery
31 pts. with a „classic“ CO ./. 25 with a computer-assisted CO
• Operating time shorter in the CA group
• After 12 weeks sig. more CA CO had healed as with
„classic“ CO
• 2 pts. with CA CO required revision for non-union
• Otherwise clinical results were similar among both groups.

Results: arthroscopic
guided intra-art. CO
10 pts; 17 -68 yrs
Stepoffs 2 – 6 mm
FU: Ø 28 mths
average extension improved from 24° to 54°, average grip
strength improved from 47% to 89% of the contralateral wrist,
average DASH score improved from 74 to 18, and average
PRWE score improved from 79 to 15.

• CO of intra-art. Distal radial malunion is save
• It lead to a more anatomical conguity of the
articular surface of the distal radius, but not to
a normal one.
• From the 3 different techniques – „classic“ –
computer-assisted – arthroscopic guided –
none is superior to the others.
Summary

Thank you


















