
Hysterectomy: An analysis of early trends from Ayushman ...
20
Working Paper - 001 Patterns of utilization for Hysterectomy: An analysis of early trends from Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (PM-JAY) Authors: Sukhvinder Kaur, Dr. Nishant Jain, Dr. Sapna Desai
Transcript of Hysterectomy: An analysis of early trends from Ayushman ...

Working Paper - 001 Patterns of utilization for
Hysterectomy: An analysis of
early trends from Ayushman
Bharat Pradhan Mantri Jan
Arogya Yojana (PM-JAY)
Authors:
Sukhvinder Kaur, Dr. Nishant Jain, Dr. Sapna Desai

2 | P a g e
Disclaimer: The main objective of the working paper series of the National Health Authority (NHA) is to help staff, consultants, advisors
and partners to speedily share their research findings based on PM-JAY experience with professional colleagues and test
their research findings at the pre-publication stage. The opinion(s), view(s) and conclusion(s) expressed in the working paper
are those of the authors and do not reflect the view of any author’s employer, official policy or position of any agency of the
NHA. The PM-JAY data used in the analysis should not be utilized/quoted without prior permission of NHA. The papers do
not themselves represent policy advice.
Acknowledgements: We acknowledge with gratitude the contribution and technical support provided by all NHA colleagues, especially the Analytics
team (Chirag Sadana and Lakshya Arora) for helping in getting the required package related data from PM-JAY data
warehouse; M&E team (Abbas Hassan and Chetan Kumar) in supporting PM-JAY data analysis; and Ankita Shukla from
Population council for NFHS-4 insights. We also acknowledge support of GIZ and Population Council of India for this working
paper. Special thanks to CEO and Deputy CEO at NHA for their overall strategic guidance and facilitating the necessary
approvals.

3 | P a g e
Executive Summary
Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (PM-JAY) is India's government-funded
health insurance scheme that covers more than 10.74 crore poor and vulnerable families.
Since the launch of the scheme in September 2018 till May 2019, PM-JAY had issued more
than 3.63 crore e-cards and 22 lakhs claims for hospitalizations through public and private
empaneled hospitals across India. There is no cap on family size and age under the scheme
to ensure that nobody is left out (especially women, children and the elderly). A total of 1,393
treatment packages for 25 specialties are available for beneficiaries under the scheme.
This working paper presents highlights of broad patterns of the hysterectomy package utilized
for the first nine months under the scheme. Hysterectomy has emerged as a particular area of
interest regarding health insurance utilization in India, especially in light of the potential for
misuse. The paper describes patterns from dynamic data available for 24 States/UTs from the
PM-JAY dashboard from September 2018 to April 2019 and compares trends with
hysterectomy data collected in the National Family Health Survey-4 (NFHS-4) in 2015-16
amongst women in age group 15-49 years.
Hysterectomy comprised two percent of claims submitted for women and one percent of all
claims submitted till date across 24 States/UTs. Six states (Chhattisgarh, Uttar Pradesh,
Jharkhand, Gujarat, Maharashtra and Karnataka), which had overall high number of claims
under PM-JAY, also generated three-quarters of all hysterectomy claims. Chhattisgarh in
particular generated a high proportion of all claims, as well as specifically for hysterectomy.
The median age of claims submitted for women for hysterectomy under PM-JAY was 44 years.
The primary type of hysterectomy included hysterectomy with salpingo-oopherectomy,
indicating that almost half of claimants underwent removal of the ovaries. In Chhattisgarh and
Jharkhand, the majority of claims were submitted by private sector hospitals, while the claims
are more evenly distributed between public and private hospitals in other states.
The paper reviews implications of these trends for women's health and health systems, given
that removal of the uterus and ovaries induces premature menopause and other side effects.
We also identify issues for closer monitoring, such as review of the medical necessity of claims,
public-private sector utilization patterns and improvements in data collection and analysis.
Even though the overall percentage of hysterectomy cases are low in the scheme, the
recommended next steps are: in-depth review of claims at the state level, particularly Uttar
Pradesh, Haryana, & Arunachal Pradesh; data improvements; and further analysis of claims
for gynecological morbidity as a whole and from a health systems perspective.

4 | P a g e
1. Background PM-JAY was launched by the Government of India in September 2018 as a core component
of India’s initiatives towards Universal Health Coverage (UHC). Aligned with the National
Health Policy, PM-JAY aims to provide financial protection to 10.74 crore poor and vulnerable
families to reduce catastrophic health expenditure. The scheme offers a benefit cover of Rs.
5,00,000 (USD 7,350) per family per year for secondary and tertiary care on a family floater
basis (means one or more members of family case use the cover collectively). PM-JAY
subsumes the previous Rashtriya Swasthya Bima Yojana (RSBY) that provided health
insurance cover of Rs. 30,000 (USD 442) to families that were below poverty line.
Benefits under PM-JAY, provided on a cashless basis up to a family’s annual coverage limit,
include:
(i) Hospitalization expenses
(ii) Day care treatment (as applicable)
(iii) Pre and post-hospitalization expenses
(iv) Follow-up care
(v) Newborn child/children benefit
The scheme includes a total of 1,393 packages across 25 specialties that include medical
treatment, surgical procedures and day care treatments (if applicable). Focusing on
reproductive and maternal health, there are 73 packages for obstetric care and treatment of
gynecological morbidities (of which 41 packages mandated for pre-authorization from
Insurer/State Government). States had the option to reserve packages (such as c-section, high
risk delivery and hysterectomy) for government facilities or, based on the local situation limit
these procedures to private hospitals upon referral by government hospitals/doctors. As of
April 2019, data is analyzed for twenty-four states and union territories implementing PM-JAY.
Some of these states, such as Tamil Nadu, Gujarat, Maharashtra and Chhattisgarh, have a
previous history of implementing health insurance programs, while other states (such as Bihar,
Uttar Pradesh, Haryana and Madhya Pradesh) have not implemented health insurance
programs in recent years.

5 | P a g e
In India, a small but growing body of research has examined hysterectomy patterns over the
past decade [2-5]. Specific to health insurance, findings from Gujarat indicated that
hysterectomy was the leading claim in a community-based health insurance scheme, at a
mean age of 36 years [2]. Facility-based media and fact-finding reports from Chhattisgarh,
Rajasthan and Bihar highlighted medically unindicated use of the procedure, leading to
additional checks on hysterectomy claims submitted under RSBY. Most recently, the National
Family Health Survey (NFHS-4) in 2015-16 provided estimates of hysterectomy prevalence
amongst women aged 15-49 years.
2. Objectives This working paper focuses on insurance claims patterns for hysterectomy under the PM-JAY
scheme. The aim of this initial review of the scheme is to examine broad patterns and to identify
further areas for monitoring and analysis. This paper utilizes scheme data to:
(1) Examine claim utilization patterns for hysterectomy under PM-JAY
(2) Compare insurance claim trends to population-based data from the NFHS-4
(3) Identify areas for further review, analysis and improved monitoring
This working paper is not aimed to analyze the performance of the scheme but only provides
insights specific to hysterectomy based on the scheme data and suggests recommendations
for the future.
Hysterectomy,
Hysterectomy, the surgical removal of the uterus, has emerged as a particular area of
interest regarding health insurance utilization in India. Globally, hysterectomy is a leading
reason for hospitalization amongst adult women, with wide variation in rates by setting
and population group [1]. Available data from high-income countries suggests that
incidence is highest amongst women over 45 years. The surgery is most commonly
performed for benign causes such as abnormal uterine bleeding or fibroids and may be
accompanied by oophorectomy (which can induce premature menopause).

6 | P a g e
3. Methods The analysis draws from PM-JAY’s analytics dashboard, compiled at the state and national
level by the National Health Authority (NHA), to conduct descriptive analyses of pre-
authorizations and claims submissions from September 2018 to April 2019 in 24 states, by
state and implementation category (states with earlier schemes and new states). Data
analyzed at the state level were: pre-authorization and claim submissions for specific
packages, age of claimant and type of hospital utilized (private/public). Unless noted where
pre-authorizations are also presented, we utilized data for claims submission throughout the
analysis. This analysis focuses on broad claims patterns in the first nine months of the
scheme; further analysis after longer implementation periods will be amenable to analysis at
the state level and inclusion of disbursal amounts.
Descriptive analyses of NFHS-4 data on hysterectomy patterns provide estimates of
prevalence, medical indications and sector of procedure in all states and union territories
amongst women aged 15-49 years in 2015-16. Using publicly available data, findings
presented in this paper also draw from previous analyses conducted by the Population Council
India [6].
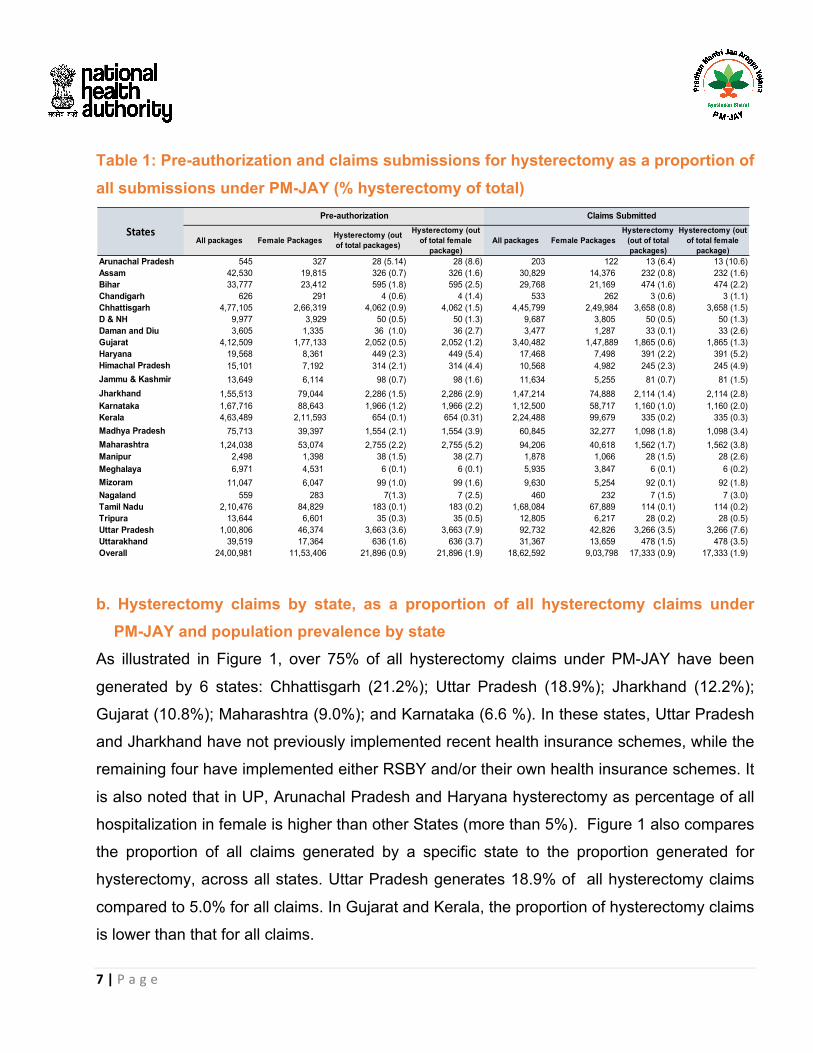
4. Findings a. Hysterectomy as a proportion of all claims, by state From September 2018 to April 2019, 24,00,981 pre-authorizations were raised for all packages
under PM-JAY. Of these, 21,896 (0.9%) were for hysterectomy. There was a total of 17,333
claims submitted for hysterectomy, comprising 0.9 percent of claims for all packages (Table
1). Amongst pre-authorizations and claims submitted for women by empaneled hospitals,
hysterectomy comprised 1.9 percent.
7 | P a g e
Table 1: Pre-authorization and claims submissions for hysterectomy as a proportion of all submissions under PM-JAY (% hysterectomy of total)
b. Hysterectomy claims by state, as a proportion of all hysterectomy claims under PM-JAY and population prevalence by state
As illustrated in Figure 1, over 75% of all hysterectomy claims under PM-JAY have been
generated by 6 states: Chhattisgarh (21.2%); Uttar Pradesh (18.9%); Jharkhand (12.2%);
Gujarat (10.8%); Maharashtra (9.0%); and Karnataka (6.6 %). In these states, Uttar Pradesh
and Jharkhand have not previously implemented recent health insurance schemes, while the
remaining four have implemented either RSBY and/or their own health insurance schemes. It
is also noted that in UP, Arunachal Pradesh and Haryana hysterectomy as percentage of all
hospitalization in female is higher than other States (more than 5%). Figure 1 also compares
the proportion of all claims generated by a specific state to the proportion generated for
hysterectomy, across all states. Uttar Pradesh generates 18.9% of all hysterectomy claims
compared to 5.0% for all claims. In Gujarat and Kerala, the proportion of hysterectomy claims
is lower than that for all claims.
All packages Female Packages Hysterectomy (out of total packages)
Hysterectomy (out of total female
package)All packages Female Packages
Hysterectomy (out of total packages)
Hysterectomy (out of total female
package)Arunachal Pradesh 545 327 28 (5.14) 28 (8.6) 203 122 13 (6.4) 13 (10.6)Assam 42,530 19,815 326 (0.7) 326 (1.6) 30,829 14,376 232 (0.8) 232 (1.6)Bihar 33,777 23,412 595 (1.8) 595 (2.5) 29,768 21,169 474 (1.6) 474 (2.2)Chandigarh 626 291 4 (0.6) 4 (1.4) 533 262 3 (0.6) 3 (1.1)Chhattisgarh 4,77,105 2,66,319 4,062 (0.9) 4,062 (1.5) 4,45,799 2,49,984 3,658 (0.8) 3,658 (1.5)D & NH 9,977 3,929 50 (0.5) 50 (1.3) 9,687 3,805 50 (0.5) 50 (1.3)Daman and Diu 3,605 1,335 36 (1.0) 36 (2.7) 3,477 1,287 33 (0.1) 33 (2.6)Gujarat 4,12,509 1,77,133 2,052 (0.5) 2,052 (1.2) 3,40,482 1,47,889 1,865 (0.6) 1,865 (1.3)Haryana 19,568 8,361 449 (2.3) 449 (5.4) 17,468 7,498 391 (2.2) 391 (5.2)Himachal Pradesh 15,101 7,192 314 (2.1) 314 (4.4) 10,568 4,982 245 (2.3) 245 (4.9)Jammu & Kashmir 13,649 6,114 98 (0.7) 98 (1.6) 11,634 5,255 81 (0.7) 81 (1.5)Jharkhand 1,55,513 79,044 2,286 (1.5) 2,286 (2.9) 1,47,214 74,888 2,114 (1.4) 2,114 (2.8)Karnataka 1,67,716 88,643 1,966 (1.2) 1,966 (2.2) 1,12,500 58,717 1,160 (1.0) 1,160 (2.0)Kerala 4,63,489 2,11,593 654 (0.1) 654 (0.31) 2,24,488 99,679 335 (0.2) 335 (0.3)Madhya Pradesh 75,713 39,397 1,554 (2.1) 1,554 (3.9) 60,845 32,277 1,098 (1.8) 1,098 (3.4)Maharashtra 1,24,038 53,074 2,755 (2.2) 2,755 (5.2) 94,206 40,618 1,562 (1.7) 1,562 (3.8)Manipur 2,498 1,398 38 (1.5) 38 (2.7) 1,878 1,066 28 (1.5) 28 (2.6)Meghalaya 6,971 4,531 6 (0.1) 6 (0.1) 5,935 3,847 6 (0.1) 6 (0.2)Mizoram 11,047 6,047 99 (1.0) 99 (1.6) 9,630 5,254 92 (0.1) 92 (1.8)Nagaland 559 283 7(1.3) 7 (2.5) 460 232 7 (1.5) 7 (3.0)Tamil Nadu 2,10,476 84,829 183 (0.1) 183 (0.2) 1,68,084 67,889 114 (0.1) 114 (0.2)Tripura 13,644 6,601 35 (0.3) 35 (0.5) 12,805 6,217 28 (0.2) 28 (0.5)Uttar Pradesh 1,00,806 46,374 3,663 (3.6) 3,663 (7.9) 92,732 42,826 3,266 (3.5) 3,266 (7.6)Uttarakhand 39,519 17,364 636 (1.6) 636 (3.7) 31,367 13,659 478 (1.5) 478 (3.5)Overall 24,00,981 11,53,406 21,896 (0.9) 21,896 (1.9) 18,62,592 9,03,798 17,333 (0.9) 17,333 (1.9)
Pre-authorization Claims Submitted
States

8 | P a g e
Figure 1: State-wise distribution of all packages and hysterectomy (% claims in specific state/total claims across all states)
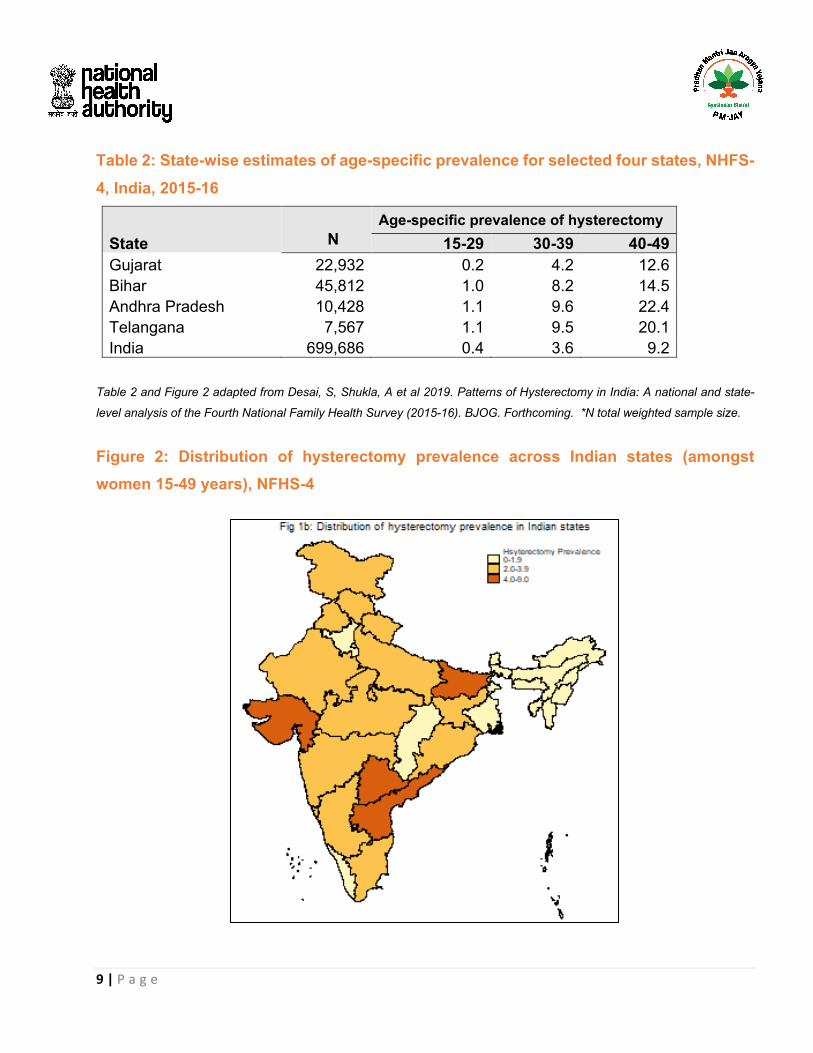
The NFHS-4 provides estimates of hysterectomy prevalence amongst women in ages 15-49
across all states and union territories. Prevalence estimates vary widely by state, as illustrated
in Figure 2. Prevalence was highest in Andhra Pradesh, Telangana, Gujarat and Bihar (Table
2). The majority of claims for hysterectomy reported in NHFS-4 were for benign conditions:
approximately one-half of women who underwent hysterectomy reported excessive menstrual
bleeding as an indication, followed by fibroid/cysts and uterine rupture. The majority of
hysterectomies were reported by women in the 40-49 age group at the time of the survey,
amongst whom the median age was 37 years. We note that this median age is not exactly
comparable to PM-JAY (44 years), as NFHS-4 only surveyed women 40-49 years while PM-
JAY covers all women.
9 | P a g e
Table 2: State-wise estimates of age-specific prevalence for selected four states, NHFS-4, India, 2015-16
State
N Age-specific prevalence of hysterectomy
15-29 30-39 40-49 Gujarat 22,932 0.2 4.2 12.6
Bihar 45,812 1.0 8.2 14.5
Andhra Pradesh 10,428 1.1 9.6 22.4
Telangana 7,567 1.1 9.5 20.1
India 699,686 0.4 3.6 9.2 Table 2 and Figure 2 adapted from Desai, S, Shukla, A et al 2019. Patterns of Hysterectomy in India: A national and state-
level analysis of the Fourth National Family Health Survey (2015-16). BJOG. Forthcoming. *N total weighted sample size.
Figure 2: Distribution of hysterectomy prevalence across Indian states (amongst women 15-49 years), NFHS-4

10 | P a g e
Figure 3: Median age of claims submitted under PM-JAY
Figure 3 indicates that the mean age of women for whom claims submitted were 46, with a
median age of 44 years. The data include major outliers, which may be due to issues with
appropriateness of claims, data errors or other issues which require further analysis and
improvement.

11 | P a g e
Table 3: Age distribution of claims and median age under PM-JAY, by state
b. Type of hysterectomy Figure 4 presents type of hysterectomy package utilization. Hysterectomy with salpingo-
oopherectomy is the most commonly used package, with some variation by state and sector
(Table in Annex 1). There are clear differences across sectors and by state for types of
packages, which requires more detailed review at the state level. (Annex provides details on
how procedures were categorized and claim amounts.
<15 15-29 30-39 40-49 50-59 60+Arunachal Pradesh 0.0 0.0 38.5 53.8 7.7 0.0 44Assam 0.0 6.9 26.3 42.7 15.9 8.2 44Bihar 0.0 4.2 27.4 35.2 17.5 15.6 45Chandigarh 0.0 0.0 66.7 33.3 0.0 0.0 42Chhattisgarh 0.0 2.2 21.1 52.7 17.3 6.6 44Dadra & Nagar Haveli 0.0 2.0 32.0 52.0 10.0 4.0 42Daman And Diu 0.0 0.0 15.2 42.4 21.2 21.2 46Gujarat 0.1 2.0 23.3 52.5 15.7 6.3 44Haryana 0.0 1.0 21.7 50.6 17.9 8.7 45Himachal Pradesh 0.0 0.0 10.6 58.0 15.5 15.9 46Jammu And Kashmir 0.0 1.2 23.5 48.1 21.0 6.2 44Jharkhand 0.0 6.7 34.2 38.8 12.7 7.6 41Karnataka 8.7 2.6 22.5 40.8 14.7 10.8 44Kerala 0.0 0.3 7.5 57.0 22.4 12.8 48Madhya Pradesh 0.0 6.2 24.5 43.6 16.6 9.1 44Maharashtra 0.0 0.4 12.3 40.4 22.2 24.7 44Manipur 0.0 3.6 25.0 50.0 10.7 10.7 43Meghalaya 0.0 0.0 0.0 20.8 75.0 4.2 44Mizoram 0.0 2.7 25.7 63.5 0.0 8.1 44Nagaland 0.0 0.0 42.9 57.1 0.0 0.0 41Tamil Nadu 0.0 0.0 13.2 46.5 28.9 11.4 44Tripura 0.0 7.1 10.7 42.9 25.0 14.3 44Uttar Pradesh 0.0 3.4 25.7 38.7 18.0 14.2 45Uttarakhand 0.0 2.7 25.5 46.7 14.2 10.9 45Overall 0.4 2.3 24.0 46.2 17.5 9.6 44
States Age-group (%) Age
(median)

12 | P a g e
Figure 4: Type of hysterectomy conducted, claims under PM-JAY
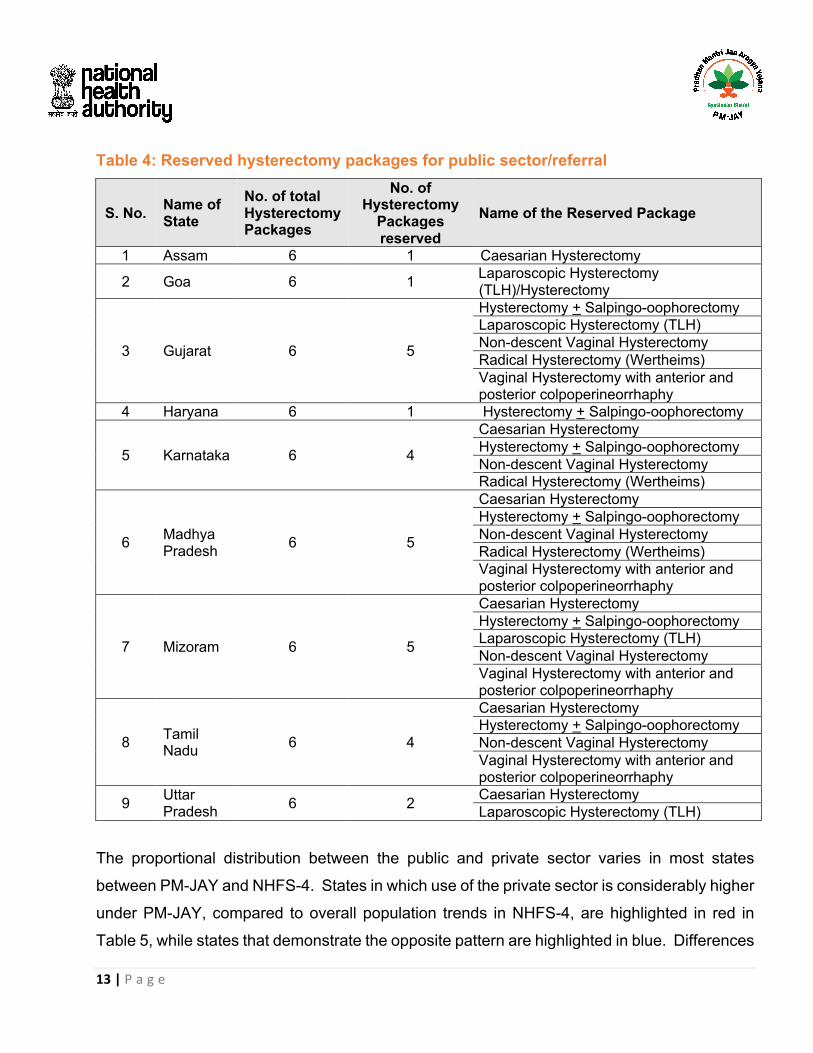
c. Public-private utilization under PM-JAY and in NFHS-4 Overall, slightly more than two-thirds (68.7%) of all claims submitted for hysterectomy were in
the private sector under PM-JAY. This overall proportion is similar to that indicated by the
NFHS-4 amongst women 15-49, across all states. However, under PM-JAY some states have
chosen to reserve hysterectomy packages at public hospitals, such as Assam, Goa, Gujarat,
Haryana, Karnataka, Madhya Pradesh, Mizoram, Tamil Nadu and Uttar Pradesh as described
in Table 4 below (Goa is not included in this analysis).
3.1
42.2
1.8 0.0
14.98.4
4.1
25.5
Caes
aria
n hy
ster
ecto
my
Hyst
erec
tom
y ±
Salp
ingo
-oop
hore
ctom
y
Hyst
erec
tom
y -ab
dom
inal
or va
gina
l + Sa
lpin
go-
ooph
orec
tom
y
Hyst
erec
tom
y as p
art o
fVV
F/ut
erov
agin
al fi
stul
are
pair
(top-
up)
Lapa
rosc
opic
hyst
erec
tom
y
Non
desc
ent v
agin
alhy
ster
ecto
my
Radi
cal H
yste
rect
omy
Vagi
nal h
yste
rect
omy
13 | P a g e
Table 4: Reserved hysterectomy packages for public sector/referral
S. No. Name of State
No. of total Hysterectomy Packages
No. of Hysterectomy
Packages reserved
Name of the Reserved Package
1 Assam 6 1 Caesarian Hysterectomy
2 Goa 6 1 Laparoscopic Hysterectomy (TLH)/Hysterectomy
3 Gujarat 6 5
Hysterectomy + Salpingo-oophorectomy Laparoscopic Hysterectomy (TLH) Non-descent Vaginal Hysterectomy Radical Hysterectomy (Wertheims) Vaginal Hysterectomy with anterior and posterior colpoperineorrhaphy
4 Haryana 6 1 Hysterectomy + Salpingo-oophorectomy
5 Karnataka 6 4
Caesarian Hysterectomy Hysterectomy + Salpingo-oophorectomy Non-descent Vaginal Hysterectomy Radical Hysterectomy (Wertheims)
6 Madhya Pradesh
6 5
Caesarian Hysterectomy Hysterectomy + Salpingo-oophorectomy Non-descent Vaginal Hysterectomy Radical Hysterectomy (Wertheims) Vaginal Hysterectomy with anterior and posterior colpoperineorrhaphy
7 Mizoram 6 5
Caesarian Hysterectomy Hysterectomy + Salpingo-oophorectomy Laparoscopic Hysterectomy (TLH) Non-descent Vaginal Hysterectomy Vaginal Hysterectomy with anterior and posterior colpoperineorrhaphy
8 Tamil Nadu
6 4
Caesarian Hysterectomy Hysterectomy + Salpingo-oophorectomy Non-descent Vaginal Hysterectomy Vaginal Hysterectomy with anterior and posterior colpoperineorrhaphy
9 Uttar Pradesh
6 2 Caesarian Hysterectomy Laparoscopic Hysterectomy (TLH)
The proportional distribution between the public and private sector varies in most states
between PM-JAY and NHFS-4. States in which use of the private sector is considerably higher
under PM-JAY, compared to overall population trends in NHFS-4, are highlighted in red in
Table 5, while states that demonstrate the opposite pattern are highlighted in blue. Differences

14 | P a g e
may reflect: (i) overuse in the private sector and/or reservations of specific packages for public
hospitals in some states; (ii) differences in data sources and time of data collection, given that
NFHS reports on ever having had a hysterectomy and PM-JAY reflects more recent trends;
(iii) differentials in cost, quality and type of treatment available across the private and public
sectors.
Table 5: Public-private utilization, PM-JAY and NFHS-4 States/UTs Claims submitted for hysterectomy- PMJAY
all women; (Sept 2018-April 2019) Reported use in NFHS-4
(ever hysterectomy, women 15-49 years, 2015-16)
Overall (n) Public Private Public Private Arunachal Pradesh 13 100.0 0.0 70.4 29.6
Assam 228 50.3 49.6 66.0 34.0
Bihar 473 52.1 48.1 17.2 82.9
Chandigarh 3 66.6 33.3 54.3 45.7
Chhattisgarh 3,648 5.4 94.5 35.0 65.1
Dadra & Nagar Havel 50 74.0 26.0 61.0 39.0
Daman and Diu 33 84.8 15.1 25.6 74.4
Gujarat 1,855 5.3 94.8 30.6 69.4
Haryana 389 40.4 59.6 41.3 58.7
Himachal Pradesh 245 82.7 17.3 46.0 54.0
Jammu And Kashmir 81 25.8 74.2 62.5 37.5
Jharkhand 2,103 3.4 96.7 27.1 73.0
Karnataka 1,146 90.7 9.3 52.8 47.2
Kerala 335 73.2 26.7 41.6 58.4
Madhya Pradesh 1,086 59.0 40.8 44.3 55.7
Maharashtra 1,548 78.2 21.8 30.8 69.2
Manipur 28 82.1 17.9 52.3 47.8
Meghalaya 6 100.0 0.0 71.4 28.6
Mizoram 92 100.0 0.0 62.9 37.1
Nagaland 7 57.1 42.9 49.0 51.0
Tamil Nadu 110 54.5 45.6 52.6 47.4
Tripura 28 100.0 0.0 41.5 58.6
Uttar Pradesh 3,252 13.7 86.3 23.0 77.0
Uttarakhand 477 44.7 55.6 38.8 61.2
Overall 17,236 31.0 69.0 32.4 67.7

15 | P a g e
4. Summary of main findings In summary, this initial analysis of PM-JAY claims suggests that:
• Hysterectomy comprised only 1 percent of all claims and 2 percent of claims submitted
for women till date.
• Six states generated three-quarters of all hysterectomy claims, which also had overall
higher claims
• The median age of women for claims submitted by hospitals was 44 years.
• The majority (two-thirds) of claims were submitted by private sector hospitals, with
considerable variation by state.
• The primary type of hysterectomy included salpingo-oopherectomy, indicating that
almost half of claimants underwent removal of the ovaries.
5. Implications for PMJAY This initial analysis raises implications for women’s health, data monitoring and health systems
responsiveness a. Women’s health The median age of claims submitted for hysterectomy and use of oophorectomy should be
monitored closely. Without data on the medical indications for claims under PM-JAY, it is
difficult to assess medical necessity for procedures. The NFHS suggests that hysterectomy is
widely performed for benign conditions, raising questions on the need for the wide use of
oophorectomy in claims. These trends suggest that women who undergo hysterectomy in their
early forties may enter menopause ten years before the global average of 51 years—which
renders women to a range of health conditions such as osteoporosis and cardiovascular
disease. Ensuring the appropriate use of hysterectomy, use of alternate procedures and
primary health services for gynaecological morbidity remains critical. It is also noted that
hysterectomy procedure usage is also a public health issue also and not only related to
insurance schemes.
16 | P a g e
b. Data improvement We identify three key areas for improved monitoring and data analysis:
(i) Improved categorization of existing packages to facilitate analysis and tracking. At
present, there are sixteen categories, many of which may overlap.
(ii) Quality checks: data included a few male hysterectomy cases as well as a few amongst
women under 15 years and more than 90 years of age, indicating most probably issues
in SECC data quality and also the need for improved monitoring of both data and claims
usage.
(iii) Include additional variables, particularly the medical indications for hysterectomy and
demographic data of claimants, such that medical necessity of claims and patterns can
be reviewed under PM-JAY. Medical indications will provide insight into whether
hysterectomy could have been replaced with a less invasive procedure, such as cyst
removal or medical management as well as allow for review of providers’ treatment
patterns of gynaecological morbidity in the public and private sectors.
c. Health systems Differential use of hysterectomy across states and sectors suggests differences in the
treatment for gynecological morbidity, potentially differential impacts of PM-JAY and the critical
need to monitor hysterectomy claims over time, across states. While data were not sufficient
to draw conclusions on medical necessity of claims or whether alternative treatment was
offered, the distribution of hysterectomy cases across states, as well as across sectors,
requires more in-depth examination at the individual state level and comparison with
population-based trends. PM-JAY dashboard administrative data provides insight into age of
claimants and hospital sector; state level reviews with population and insurance data are
critical to understand use of hysterectomy and overall treatment for gynecological morbidity.
Additionally, while some states have reserved hysterectomy packages in the public sector,
implementation till date does not suggest major differences in use of the private sector in the
larger states. This issue requires further review after longer implementation periods.

17 | P a g e
6. Next steps We recommend the following steps:
Claims review
• Conduct more detailed reviews at the state level for Uttar Pradesh, Haryana and
Arunachal Pradesh hospitals, which generated more than 5% of hysterectomy cases
out of all cases for women in this time period to age and demographic patterns,
proportion of claims amounts and payments generated by hysterectomy
• Review the use of oophorectomy and medical necessity of the procedure
• Identify and review medical indications for younger women in high incidence states
through in-depth examination of a sub-set of claims with hospitals and women
• Examine use of the public and private sector at the state level and compare across
states who have reserved hysterectomy in the public sector, package types, comparison
of pre-authorizations and claims submitted and disbursals
• Expand this analysis to review claims for other treatments for gynecological morbidity
and claims amounts
Data improvements
• Review categorization of packages with an expert group
• Address and identify issues in data quality so as to pinpoint the causes of outliers, such
as claims data for males and high proportion of claims raised for young women in some
states
• Include additional tracking of medical indications for hysterectomy claims

18 | P a g e
Annex Table 1: State-wise type of Hysterectomy package utilized by type of facilities
Cesarean
hysterectomy
Hysterectomy ± Salpingo-
oophorectomy
Hysterectomy -abdominal or
vaginal + Salpingo-
oophorectomy
Hysterectomy as part of
VVF/uterovaginal fistula repair (top-
up)
Laparoscopic hysterectomy
Non-descent vaginal
hysterectomy
Radical hysterectomy
Vaginal hysterectomy
States Pvt. Pub. Pvt. Pub. Pvt. Pub. Pvt. Pub. Pvt. Pub. Pvt. Pub. Pvt. Pub. Pvt. Pub. Arun. Pr 0.0 0.0 0.0 92.3 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 7.7
Assam 0.9 0.4 28 36.6 0.0 0.0 0.0 0.0 11.6 0.4 6.5 1.3 0.9 3.4 1.7 8.2
Bihar 1.6 2.5 23.3 18.4 0.0 0.0 0.0 0.0 1.6 0.7 0.9 0.9 2.5 1.1 18.2 28.5
Chandigarh 0.0 0.0 33.3 33.3 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 33.3
Chhattisgarh 6.2 0.8 49.1 2.4 0.0 0.0 0.0 0.0 21.4 0.4 1.6 0.1 1.9 0.4 14.3 1.3
D&NH 0.0 0.0 2.0 26 0.0 0.0 0.0 0.0 14 30.0 0.0 10.0 6.0 0.0 4.0 8.0
Daman & Diu 0.0 0.0 0.0 57.6 0.0 0.0 0.0 0.0 9.1 0.0 0.0 21.2 3.0 3.0 3.0 3.0
Gujarat 0.0 0.0 47.1 3.2 0.0 0.0 0.0 0.0 28.0 1.2 3.9 0.2 0.6 0.1 15.2 0.6
Haryana 0.0 1.9 0.0 24.4 0.0 0.0 0.0 0.0 59.6 2.5 0.0 1.9 0.0 0.3 0.0 9.4
HP 0.0 0.4 14.4 56.8 0.0 0.0 0.0 0.0 2.5 0.8 0.0 4.1 0.0 0.4 0.4 20.2
J&K 1.5 1.5 59.1 7.6 0.0 0.0 0.0 0.0 10.6 1.5 1.5 0.0 0.0 6.1 1.5 9.1
Jharkhand 5.1 0.4 72.3 1.5 0.0 0.0 0.0 0.0 1.8 0.2 0.2 0.2 1.2 0.1 16.1 1.0
Kerala 0.6 3.4 0.0 0.0 23.3 65.5 0.0 0.0 0.3 0.6 0.0 0.0 0.0 0.3 2.5 3.4
Karnataka 0.0 1.5 0.0 64.2 0.0 0.0 0.0 0.0 2.7 1.6 0.0 5.4 2.8 3 3.8 15.0
MP 0.0 5.5 0.0 36.6 0.0 0.0 0.0 0.0 38 0 0.0 0.5 2.8 0.4 0.0 16.0
Maharashtra 0.0 0.0 4.4 1.0 0.0 0.0 0.2 0.2 0.0 18 4.8 39.7 11.7 0.7 0.7 18.6
Manipur 0 0 14.3 57.1 0 0 0 0 3.6 3.6 0 0 0 7.1 0 14.3
Meghalaya 0.0 0.0 0.0 66.7 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 16.7 0.0 16.7
Mizoram 0.0 2.2 0.0 15.6 0.0 0.0 0.0 0.0 0.0 2.2 0.0 0.0 0.0 80.0 0.0 0.0
Nagaland 0.0 0.0 14.3 57.1 0.0 0.0 0.0 0.0 28.6 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Tamil Nadu 0.0 0.0 0.0 50.0 0.0 0.0 0.0 0.0 2.6 2.6 0.0 0.0 43.0 0.9 0.0 0.9
Tripura 0.0 0.0 0.0 60.7 0.0 0.0 0.0 0.0 0.0 0.0 0.0 3.6 0.0 0.0 0.0 35.7
UP 0.5 1.0 12.1 7.4 0.0 0.0 0.0 0.0 1.1 0.3 11.5 0.6 4.0 0.2 57.1 4.2
Uttarakhand 1.4 0.5 31.9 18.9 0 0 0 0 13.1 8.2 0.5 5.4 1.2 0.5 7.5 11.2
Overall 2.0 1.0 28.9 13.2 0.5 1.3 0.0 0.0 12.3 2.6 3.5 4.8 3.3 0.8 18.4 7.1
19 | P a g e
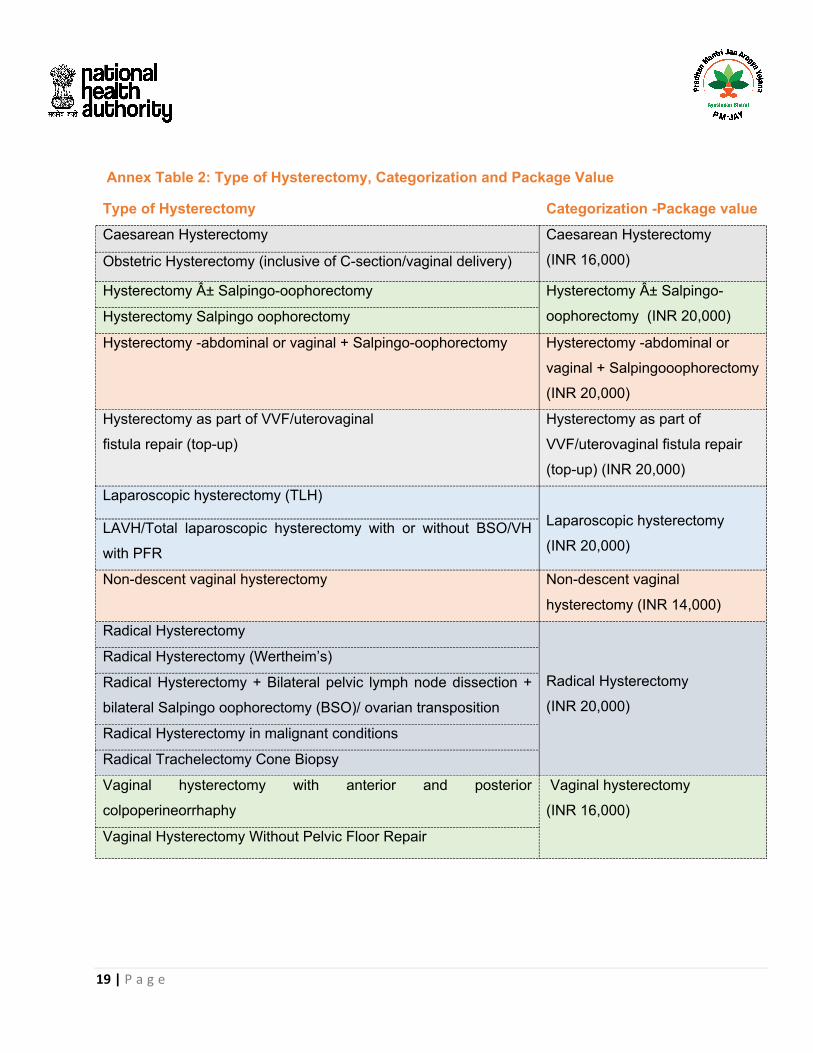
Type of Hysterectomy
Categorization -Package value
Caesarean Hysterectomy Caesarean Hysterectomy
(INR 16,000) Obstetric Hysterectomy (inclusive of C-section/vaginal delivery)
Hysterectomy ± Salpingo-oophorectomy Hysterectomy ± Salpingo-
oophorectomy (INR 20,000) Hysterectomy Salpingo oophorectomy
Hysterectomy -abdominal or vaginal + Salpingo-oophorectomy Hysterectomy -abdominal or
vaginal + Salpingooophorectomy
(INR 20,000)
Hysterectomy as part of VVF/uterovaginal
fistula repair (top-up)
Hysterectomy as part of
VVF/uterovaginal fistula repair
(top-up) (INR 20,000)
Laparoscopic hysterectomy (TLH)
Laparoscopic hysterectomy
(INR 20,000) LAVH/Total laparoscopic hysterectomy with or without BSO/VH
with PFR
Non-descent vaginal hysterectomy Non-descent vaginal
hysterectomy (INR 14,000)
Radical Hysterectomy
Radical Hysterectomy
(INR 20,000)
Radical Hysterectomy (Wertheim’s)
Radical Hysterectomy + Bilateral pelvic lymph node dissection +
bilateral Salpingo oophorectomy (BSO)/ ovarian transposition
Radical Hysterectomy in malignant conditions
Radical Trachelectomy Cone Biopsy
Vaginal hysterectomy with anterior and posterior
colpoperineorrhaphy
Vaginal hysterectomy
(INR 16,000)
Vaginal Hysterectomy Without Pelvic Floor Repair
Annex Table 2: Type of Hysterectomy, Categorization and Package Value
20 | P a g e
References 1. Hammer, A., et al., Global epidemiology of hysterectomy: possible impact on gynecological cancer rates.
American journal of obstetrics and gynecology, 2015. 213(1): p. 23-29.
2. Desai, S., et al., Incidence and determinants of hysterectomy in a low-income setting in Gujarat, India.
Health policy and planning, 2016. 32(1): p. 68-78.
3. Prusty, R.K., C. Choithani, and S.D. Gupta, Predictors of hysterectomy among married women 15–49
years in India. Reproductive health, 2018. 15(1): p. 3.
4. Singh, A. and A.K. Arora, Why hysterectomy rate are lower in India. Indian journal of community
medicine: official publication of Indian Association of Preventive & Social Medicine, 2008. 33(3): p. 196.
5. Sardeshpande, N., Why do young women accept hysterectomy? Findings from a study in Maharashtra,
India. International Journal of Innovation and Applied Studies, 2014. 8(2): p. 579.
6. Desai, S, A. Shukla, D. Nambiar and R. Ved. Patterns of hysterectomy in India: A national and state-level
analysis of the Fourth National Family Health Survey (2015-16)". BJOG, Forthcoming.


















