Hypoxic Hepatopathy: Pathophysiology and Prognosis
8
1063 □ ORIGINAL ARTICLE □ Hypoxic Hepatopathy: Pathophysiology and Prognosis Richard Birrer 1 , Yasuharu Takuda 2 and Tsuyoshi Takara 3 Abstract Background Dramatic transient elevation in serum concentrations of hepatic enzymes occurs in some pa- tients following a hypo-perfusion state. This entity is variously termed “shock liver” or “ischemic hepatitis”, since the pathogenesis is considered to be ischemia. However, hypotension or shock is not always present. Methods We analyzed the medical records of 293 patients (322 episodes) who had a hypoxic state and were admitted to the critical care units of two general hospitals over a 13-year period. Results Hepatic injury was identified in about 1% of patients in critical care admissions. In addition to hy- potension, the causes for hepatic injury were a low flow state secondary to congestive heart failure and hy- poxia from sepsis or respiratory failure and hypoxemia from a variety of etiologies. These values were mostly normalized within several days when the hypoxic etiology was corrected and a serious co-morbid state did not intervene. Conclusion Marked elevation of hepatic enzymes can be identified not only in patients with hypotension, but also in normotensive patients in hypoxic state. Thus, the condition is appropriately termed hypoxic hepa- topathy. Key words: ischemic hepatitis, hypoxic hepatitis, shock liver (DOI: 10.2169/internalmedicine.46.0059) Introduction Though clinically significant, impairment of hepatic func- tion is unusual in shock, a transient (5-25 days), and often marked (10-300 times the upper limit of normal) change in serum enzyme levels in association with centrilobular he- patic necrosis has been described (1-9). Historically referred to as “shock liver”, clinical and experimental reports over the last five decades have confirmed that the liver is a target organ during certain hypotensive states (10-12). More recent reports have focused on hepatic dysfunction resulting from passive congestion (e.g., heart failure), termed ischemic hepatitis, or hypoxic insult (e.g., respiratory failure), termed hypoxic hepatitis (3, 13-16). Although the pathogenesis is multifactorial, the final common pathway is hepatocellular dysfunction secondary to critically low levels of oxygen for metabolic processes. We conducted a 13-year retrospective review of the pattern of serum enzyme changes in 293 criti- cally ill patients involving 322 episodes to describe the char- acteristics of hypoxic hepatopathy. Materials and Methods Study patients We reviewed the medical records of 293 patients admitted to the medical and surgical intensive care units at the 792- bed St. Joseph’s University Medical Center in Paterson, NJ and the 523-bed Chubu Hospital in Okinawa, Japan from March 1, 1990 to January 1, 2003. We enrolled patients with diagnoses of non-viral or unspecified hepatitis, hepatic infarct or hepatic congestion, severe acute or chronic heart failure (New York Heart Association Class IV), massive pul- monary embolus, hyperthermia, intoxications, ischemic heart disease, primary valvular heart disease, status-post cardio- pulmonary resuscitation (CPR), arrhythmia, respiratory fail- ure, or circulatory shock secondary to hypovolemia (e.g., hemorrhage, dehydration, excessive dialysis) or sepsis. Ex- clusion criteria were inadequate data, death within 72 hours, immediately preceding hepatic or cardiac surgery, other acute or chronic hepatobiliary disease, such as known causes 1 Medicine, St. Joseph’s University Medical Center, U.S.A, 2 Clinical Practice Evaluation and Research Center, St. Luke’s Life Science Institute, Tokyo and 3 Emergency Medicine, Chubu Hospital, Okinawa Received for publication January 29, 2007; Accepted for publication March 18, 2007 Correspondence to Dr. Richard Birrer, [email protected]
Transcript of Hypoxic Hepatopathy: Pathophysiology and Prognosis

1063
□ ORIGINAL ARTICLE □
Hypoxic Hepatopathy: Pathophysiology and Prognosis
Richard Birrer 1, Yasuharu Takuda 2 and Tsuyoshi Takara 3
Abstract
Background Dramatic transient elevation in serum concentrations of hepatic enzymes occurs in some pa-tients following a hypo-perfusion state. This entity is variously termed “shock liver” or “ischemic hepatitis”,since the pathogenesis is considered to be ischemia. However, hypotension or shock is not always present.Methods We analyzed the medical records of 293 patients (322 episodes) who had a hypoxic state andwere admitted to the critical care units of two general hospitals over a 13-year period.Results Hepatic injury was identified in about 1% of patients in critical care admissions. In addition to hy-potension, the causes for hepatic injury were a low flow state secondary to congestive heart failure and hy-poxia from sepsis or respiratory failure and hypoxemia from a variety of etiologies. These values weremostly normalized within several days when the hypoxic etiology was corrected and a serious co-morbidstate did not intervene.Conclusion Marked elevation of hepatic enzymes can be identified not only in patients with hypotension,but also in normotensive patients in hypoxic state. Thus, the condition is appropriately termed hypoxic hepa-topathy.
Key words: ischemic hepatitis, hypoxic hepatitis, shock liver
(DOI: 10.2169/internalmedicine.46.0059)
Introduction
Though clinically significant, impairment of hepatic func-tion is unusual in shock, a transient (5-25 days), and oftenmarked (10-300 times the upper limit of normal) change inserum enzyme levels in association with centrilobular he-patic necrosis has been described (1-9). Historically referredto as “shock liver”, clinical and experimental reports overthe last five decades have confirmed that the liver is a targetorgan during certain hypotensive states (10-12). More recentreports have focused on hepatic dysfunction resulting frompassive congestion (e.g., heart failure), termed ischemichepatitis, or hypoxic insult (e.g., respiratory failure), termedhypoxic hepatitis (3, 13-16). Although the pathogenesis ismultifactorial, the final common pathway is hepatocellulardysfunction secondary to critically low levels of oxygen formetabolic processes. We conducted a 13-year retrospectivereview of the pattern of serum enzyme changes in 293 criti-cally ill patients involving 322 episodes to describe the char-acteristics of hypoxic hepatopathy.
Materials and Methods
Study patients
We reviewed the medical records of 293 patients admittedto the medical and surgical intensive care units at the 792-bed St. Joseph’s University Medical Center in Paterson, NJand the 523-bed Chubu Hospital in Okinawa, Japan fromMarch 1, 1990 to January 1, 2003. We enrolled patientswith diagnoses of non-viral or unspecified hepatitis, hepaticinfarct or hepatic congestion, severe acute or chronic heartfailure (New York Heart Association Class IV), massive pul-monary embolus, hyperthermia, intoxications, ischemic heartdisease, primary valvular heart disease, status-post cardio-pulmonary resuscitation (CPR), arrhythmia, respiratory fail-ure, or circulatory shock secondary to hypovolemia (e.g.,hemorrhage, dehydration, excessive dialysis) or sepsis. Ex-clusion criteria were inadequate data, death within 72 hours,immediately preceding hepatic or cardiac surgery, otheracute or chronic hepatobiliary disease, such as known causes
1Medicine, St. Joseph’s University Medical Center, U.S.A, 2Clinical Practice Evaluation and Research Center, St. Luke’s Life Science Institute,Tokyo and 3Emergency Medicine, Chubu Hospital, OkinawaReceived for publication January 29, 2007; Accepted for publication March 18, 2007Correspondence to Dr. Richard Birrer, [email protected]

DOI: 10.2169/internalmedicine.46.0059
1064
of hepatitis from chemical, toxin, drug or infectious etiolo-gies, multiple organ dysfunction, myonecrosis, rhabdomy-olysis, hemolysis or refusal to participate. The diagnosis ofthese entities was made from clinical (history and physicalfindings), noninvasive or invasive tests (arterial blood gasanalysis and hemodynamic evaluation), or autopsy evidenceand then grouped by primary pathophysiology: decreasedoxygen uptake [1] (e.g., respiratory failure), decreased oxy-gen delivery [2] (e.g., hypotension), decreased oxygen avail-ability [3] (e.g., sepsis) and increased oxygen consumption[4] (e.g., hyperthermia).
Data collection
Hypotension was defined as, 1) a sustained mean arterialblood pressure (MAP) of less than 80 mmHg for at least fif-teen minutes, with one of the followings; tachycardia, cool,clammy skin, oliguria or anuria, and depressed or alteredmental states, or 2) a low cardiac output in association withthe use of massive volume resuscitation, inotropic agents,pericardiocentesis or intra-aortic balloon counterpulsation.Arterial blood pressures were recorded by cuff or from acannula in the femoral or radial artery. Central venous pres-sure was derived from the internal jugular or pulmonary ar-tery (Swan-Ganz) catheters.We defined hypoxic hepatopathy as a sudden, transient
ten-fold or greater rise above the patients’ baseline levelwithin 48 hours of the insult event in two or more of thefollowing hepatic enzymes: lactate dehydrogenase (lactatedehydrogenase) [reference level=98-200 IU/L] serum alanineaminotransaminase (alanine aminotransferase) [referencelevel=17-63 IU/L] and serum aspartate aminotransaminase(aspartate aminotransferase) [reference level=12-54 IU/L].Serum bilirubin, prothrombin time, partial thromboplastin
time, creatinine and alkaline phosphatase were also mea-sured. All biochemical determinations were made on a dailybasis beginning at the time of admission by SMA-C multi-panel method (Technicon Instruments Corp., Elmhurst, IL).Hemodynamic data included mean arterial blood pressure([2 × diastolic pressure + systolic pressure]/3), central ve-nous pressure (reference level=1-12cmH2O), arterial bloodgas analysis (reference level=80-98 mmHg), oxygen satura-tion (reference level�95% with PaO2 >80 mmHg), bloodlactate (reference level=0.5-2.2 mEq/L), pulmonary capillarywedge pressure (reference level=0-12 mmHg), cardiac out-put (CO), and hepatic blood flow (reference level=1,950-2,480 mL/min/m2). The hepatic blood flow was measured bythe technique of galactose clearance at the time of hypoxichepatopathy or within 6 hours following admission to an in-tensive care setting for hemodynamic instability (15). Calcu-lations were derived for the cardiac index (cardiac output/body surface area; reference level=2.7-3.6 L/min/m2), oxy-gen delivery (CI × 13.8 × Hemoglobin × oxygen saturation;reference level=530-730 mL/min/m2) and systemic vascularresistance ({mean arterial pressure-central venous pressure}/cardiac index ×80; reference level=1,750-2,600 dyn-S/cm5/m2]). Apache II scores were calculated and recorded for
each patient (17).Discrete data between 2 groups were compared by chi-square test. We calculated means, standard deviations, stan-dard error of the means and 95% confidence intervals. TheMann-Whitney U test was used to compare the non-normally distributed numerical variables for 2 groups. Themean of all pairs of the groups were compared by theScheffe test. A one-way ANOVA and the Kruskal-Wallis Htest were utilized for more than 2 groups where appropriate.Spearman rank order correlation coefficient was determinedfor blood pressure data. We considered 2-tailed p<0.05 asstatistically significant. All analyses were performed usingthe SAS version 9.0 and JMP version 5.0 (SAS InstituteInc., Gary, NC).
Results
The 322 episodes of hypoxic hepatopathy, involving 293patients, represented 1.1% of the total admissions (32,209)to the intensive care units during the study period. The aver-age age was 70.3 years. The male-to-female ratio was 2.4.Eleven patients had multiple episodes; six patients had 2episodes; three had 3 episodes and two had 4 episodes. Theprevalence of hypoxic hepatopathy was higher in the coro-nary care unit (1.4%) than in the medical (0.8%) and surgi-cal (0.5%) intensive care settings. The pathophysiologicgrouping and respective hemodynamic data are shown in Ta-ble 1. The distinguishing features of each group were: hy-poxemia in Group 1 (n=51), decreased hepatic blood flow inGroup 2 (n=198), severe hypotension in Group 3 (n=68) andincrease oxygen consumption in Group 4 (n=5). None ofGroup 1 patients had left-sided heart failure, but 3 patientswith respiratory failure had clinical and hemodynamic evi-dence of right ventricular failure.The final clinical diagnoses of patients are listed in Ta-ble 2. An acute event (e.g. myocardial infarction, pulmonaryembolus, and arrhythmia) was associated with congestiveheart failure and hypoxic hepatopathy in 86% of cases. Hy-povolemic causes of shock were trauma, dehydration, hem-orrhage and excessive dialysis. Trauma (2.7%) included gun-shot wound, motor vehicle accident, major assault or acci-dent (e.g., fall). Respiratory failure included interstitial lungdisease, pleural fibrosis, and chronic obstructive pulmonarydisease. Toxigenic etiologies were carbon monoxide, cyanidepoisoning and methemoglobinemia. The miscellaneous cate-gory included such diagnoses as sleep apnea, massive he-patic metastasis, myasthenia gravis, Guillian-Barre andamyotrophic lateral sclerosis.One hundred and forty-five (45%) patients of the enrolledpatients died during admission. Autopsies were performed in23 patients. Deaths in these patients occurred at least 6 dayspost-hypoxic event and were due to sudden cardio-respiratory collapse. Hepatic centrilobular necrosis, disinte-gration of hepatocyte nuclei, white cell infiltration, and hem-orrhage were identified. The mean length of stay was 16days for the series with no significant difference between

DOI: 10.2169/internalmedicine.46.0059
1065
Table 1. Data (Means and 95% Confidence Intervals) by Pathophysiologic Grouping
those that survived and those that died. The survival rate atthe time of discharge was 55% and at one year was 24%,based on 78 of 102 patients whose long term follow-up wasavailable. There was no difference of mortality rates amongthe groups.Of 293 patients who met hypoxic hepatopathy criteria,
164 (51%) experienced a hypotensive episode of 87 (51-78)mmHg of mean arterial pressure which lasted an average 18minutes with range of 0-7.4 hours (Table 3). All Group 3
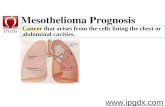
patients experienced hypotension, whereas only 45% ofGroup 2 patients developed hypotension. In 19 patients ofGroup 2 and the diagnosis of hypovolemia (e.g., hemor-rhage, dehydration, and excessive dialysis), there was a sig-nificant positive correlation (r=0.94; p<0.005) between theduration (hours) of hypotension and the onset and degree ofelevation of liver function abnormality (Fig. 1). The changewas most notable after 4.5 hours of sustained hypotension.Hypoxic hepatopathy was significantly (p<0.01) more com-

DOI: 10.2169/internalmedicine.46.0059
1066
Table 2 Final Clinical Diagnoses
mon in males as was hypotension from trauma. Significantlygreater lengths of stay and higher Apache scores were ob-served in Groups 1 and 3.The lactate dehydrogenase rose from a mean admission
baseline of 637 IU/L on day 0 to a peak of 3,045 IU/L onday 2, alanine aminotransferase rose from a mean admissionlevel of 284 IU/L to a peak of 1,803 IU/L on day 2, and as-partate aminotransferase rose from a mean admission base-line of 341 IU/L to a peak of 2,388 IU/L on day 2 (Ta-ble 3). There were no significant differences in the data be-tween hypotensive and non-hypotensive patients in the se-ries. Enzyme elevations were consistently lowest in Group 2and highest in Group 3. Prothrombin and partial throm-boplastin activity fell under fifty percent in 84% and 63% ofcases and below twenty-five percent in 16% and 12% re-spectively. Thirty-one percent of patients exhibited hypergly-cemia (>180 mg/dL); 2.8% developed hypoglycemia (<60mg/dL). Bilirubin, alkaline phosphatase, prothrombin timeand partial thromboplastin time were mildly elevated inmost patients with no significant differences between the hy-potensive and non-hypotensive subgroups. Overt jaundicewas uncommon (11% of cases). The serum creatinine waselevated in 69% of the study groups, 77% of whom hadacute renal failure.
Discussion
Jolliffe first reported the association of abnormal liverfunction tests and cardiovascular disease in conjunction withcongestive heart failure causing passive congestion of theliver in 1930 (18), but most subsequent work has been per-formed in animal models of shock (10, 11, 19, 20). Humanstudies have, until recently, not made any distinction be-tween the relative contributions of passive congestion, circu-latory failure and hypoxia and the patterns of abnormal en-zymes observed in these patients (21, 22, 42). The reportedetiologies include: primary heart disease (78%), congestive
heart failure (65%), acute myocardial infarction (17%),chronic respiratory failure (12%), circulatory shock and/orsepsis (15%). Severe hypotension or shock was reported in61% of patients (range 31-100%) (4, 6, 9, 12, 16, 21-23).The mean in-hospital mortality was 52.2%. Richman andcoworkers (24) further detailed abnormalities of liver func-tion tests in cases of chronic congestive heart failure and re-ported a fall in albumin and elevations of globulin,prothrombin time, bilirubin, alkaline phosphatase, alanineaminotransferase, and aspartate aminotransferase.Additionally, there were a number of reports of fulminant“hepatitis” or hepatic failure in the presence of acute con-gestive heart failure (1, 4, 25, 26). However, the absence ofshock, passive congestion, or acute myocardial infarction isassured in only one report (4). Yet, several studies concludedfrom their investigations that ischemic liver damage was raresecondary to acute congestive heart failure and that pro-found and prolonged shock was usually necessary for thedevelopment of “shock liver” (9, 27, 28). An inconsistentpattern of liver function test abnormalities in acute disease,thus, emerged in these early studies.The retrospective review by Champeon and co-workers(29) and the prospective study by Grimaud and colleagues(30) found that there was an initial insult phase, an interme-diate functional impairment state, and a final recoveryphase. The intermediate dysfunctional state immediately fol-lowed the shock phase and was proportional to the degree ofshock. Biological and histological findings often did not cor-relate in the studies. Gibson and Dudley’s study of 17 pa-tients described the clinical, pathological and enzymaticchanges associated with ischemic hepatitis (21). Twenty-ninepercent of patients had an episode of severe hypotension/shock, but all had a significant fall in cardiac output fromeither right (n=4) or left (n=14) heart failure.Histologically, central hepatic vein congestion with centri-lobular hepatic necrosis, fragmentation of liver bulks, poly-morphonuclear cell infiltration, abnormal hepatocyte com-

DOI: 10.2169/internalmedicine.46.0059
1067
Table 3 Demographic, Clinical and Laboratory Data
plexes and pyknosis and disintegration of hepatocyte nucleihave been observed. The reticulum network is preserved.Hyperplasia, inflammation and regeneration, characteristic ofmany forms of hepatitis, are absent. Post-mortem examina-tion of liver tissue obtained from 23 patients in the currentstudy who died shortly after initial recovery showed thecharacteristic changes of the red net pattern. The etiology ofenzyme rise is presumed to be hypoxic injury to the hepato-cyte mitochondria and endoplasmic reticulum, especially tothe centrilobular region. Experimental injury to the liver,whether due to arterial hypoxemia, hypo-perfusion factors,or endotoxin has produced similar pathologic results (31-36).The present results allow several conclusions. There is
sufficient clinicopathologic data to support the finding thathepatocellular dysfunction is common in certain populationsin the intensive care setting. Hypoxic hepatopathy is not rare
in the critical care setting with a prevalence of 0.6-1.5%(16, 22, 23). Over 50% of hospital laboratory identifiedtransient and dramatic elevations of serum aminotransferaseelevations have been attributed to hypoxic hepatopathy (37).The profound transient serum enzyme elevation in conjunc-tion with abnormal renal function and abnormalities in PTand PTT activity distinguish hypoxic hepatopathy from vi-ral, drug-induced or alcoholic hepatitis. A variety of etiolo-gies can produce this entity: arrest with prompt resuscita-tion, hypovolemia with prolonged, severe hypotension, andlow cardiac output states, especially right-sided heart failure,respiratory failure, severe anemia, sepsis, certain toxins andheat stroke. Severe hypotension/shock per se is unnecessaryfor the development of hypoxic hepatopathy, being presentin this series in 51% of cases.Acute circulatory failure in children has been noted tocause transient hepatic dysfunction probably as a conse-

DOI: 10.2169/internalmedicine.46.0059
1068
Figure 1. Liver enzyme elevation and hours of hypotension in 19 hypovolemic patients.
quence of hypoperfusion (38). Laparoscopic colectomy andlaparoscopic cholecystectomy have been associated withsubclinical hepatocyte dysfunction, presumably due to in-creased intra-abdominal pressure, patient positioning and theneurohumoral response to surgical stress (39). Profound he-patic hypoperfusion (66% reduction of portal flow duringischemia and 80% reduction in hepatic artery flow duringreperfusion) producing temporary acute hepatic dysfunctionhas been found to follow intestinal ischemia-reperfusion in-jury in the rat (40). In the pig model the reduction of aorticblood flow by cardiac tamponade can exhaust the hepatic ar-terial buffer response resulting in hepatic dysfunction with-out signs of cellular damage (41).The original work of Dunn et al identified 3 hypothetical
mechanisms for hypoxic injury to the liver in the setting ofCHF: venous congestion secondary to RVF, ischemia due todecreased hepatic blood flow, and hypoxemia due to de-creased oxygen in the hepatic artery (42). The results of thisstudy and those of others (16, 22) support these mecha-nisms. However, the evaluation of detailed hemodynamicdata provides further insight into additional mechanisms ofinjury.Severe respiratory failure, anemia, sleep apnea (Group 1)
are characterized by marked hypoxemia, depressed oxygendelivery, low SVR and HBF and elevated lactate, CI andMAP. In contradistinction, the oxygen delivery, CI and HBFare significantly depressed in Group 2 patients while thePCWP and CVP are elevated. Thus, hypoperfusion from de-creased HBF is the primary pathogenetic mechanism leadingto hypoxic hepatopathy from cardiac failure with passivecongestion being a secondary cause. We found no biochemi-cal differences that could distinguish the hypotensive from
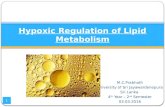
the non-hypotensive non-hypovolemic patients in Group 2who developed hypoxic hepatopathy. Indeed, we found alow cardiac output syndrome without hypotension to be fre-quently associated (47.2%) with hypoxic hepatopathy. Wefound that hypotension (decreased MAP), as noted by Hen-rion and colleagues, appears to be a more critical factor inthe setting of acute cardiac failure (massive pulmonary em-boli, acute myocardial infarction) (16).Sepsis alone does not cause hepatic enzyme elevation.Septic shock (Group 3), which is characteristically accompa-nied by increased flow (i.e., increased CI, HBF), produceshypoxic hepatic injury by inhibiting oxygen extraction at thehepatocyte level, despite reasonably preserved oxygen satu-ration and PaO2 levels. Circulating endotoxins and inflamma-tory cytokines in the presence of good hepatic perfusionprobably cause hypoxic hepatopathy in this selected popula-tion (32). Certain toxins (e.g. carbon monoxide) and similarconditions (e.g., methemoglobinemia) cause hypoxic hepato-pathy by a similar pathogenetic mechanism (i.e., main-tainance of perfusion, oxygen saturation and Pa02 withoutoxygen release at the hepatocyte). Despite the small sample,hyperthermia (Group 4) likely leads to hypoxic hepatopathythrough increased oxygen consumption as evidenced byslightly decreased oxygen saturation and PaO2 levels and ele-vated serum lactate, DO2 and HBF. The duration of hypoten-sion, as reflected by decreased MAP and CVP was of shortduration (range 16-33 minutes) and, therefore, is consideredto be non-contributory to the hepatic enzyme elevation. Fig-ure 2 summarizes the possible pathogenetic mechanismsleading to hypoxic hepatopathy.No prospective studies have been performed to determinethe incidence rate of hypoxic hepatopathy in various set-tings. It has been recognized in 26% of all patients diag-nosed having had significant hypo-perfusion, and indeed, in24% of patients not having shock, but having markedly lowflow states (22). The series of Henrion et al found a 0.9%prevalence rate for all critical care units (16). Certainly, hy-poxic hepatopathy appears to be more common than hasbeen previously recognized and occurs frequently withouthypotension due to forward (i.e., ischemia) and backward(i.e., passive congestion) flow abnormalities producing hy-poxic injury through the common pathway of hypoperfu-sion, especially in the setting of passive congestion (16), hy-poxia, increased oxygen consumption and decreased oxygenavailability. The diagnosis can be made on clinical and bio-chemical criteria without procedural intervention (i.e., bi-opsy). Risk factors for hypoxic hepatopathy include acuteand chronic heart failure, respiratory failure, sepsis, pro-longed hypotension, certain toxins and heat stroke. The term“shock liver” is clearly a misnomer, since the entity is morefrequent in non-hypotensive hypo-perfusion states than inshock, and it is better described as a hypoxic liver injury.The prognosis of a patient with ischemic liver damage de-pends on the prognosis of the underlying disease (37). Noneof the patients in the reported series developed fulminant he-patic failure. Liver biopsy is not necessary for diagnosis and

DOI: 10.2169/internalmedicine.46.0059
1069
Figure 2. Proposed pathogenesis of hypoxic hepatopathy.
prognosis is largely independent of the subclinical illness.However, the occurrence of hypoxic hepatopathy is a har-binger of a potentially poor prognosis since the mortalityrate varies from 25-73% (6, 16, 22).
Conclusion
Hypoxic injury to the liver is a reversible subclinical con-dition occurring in at least 1% of critically ill patients andaccounting for over 50% of dramatic serum aminotrans-ferase activity (24-48 hours following the hypoxic insult)
identified in hospital admissions. Hypotension, especiallyshock, appears to be important but not a sine qua non forthe condition. Hepatic injury occurring from a low flowstate secondary to congestive heart failure and hypoxia fromsepsis or respiratory failure and hypoxemia from a variety ofetiologies are also important pathogenetic mechanisms forthe development of hypoxic hepatopathy, the prognosis ofwhich is related to the presence of underlying comorbidstates, particularly ventricular failure. From a pathogeneticperspective, the term hypoxic hepatopathy should, therefore,be used in preference to “shock liver” or ischemic hepatitis.
References
1. Kaymakcalan H, Dourdourekas D, Szant PB, Steigmann F. Con-gestive heart failure as a cause of fulminant hepatic failure. Am J
Med 65: 384, 1978.2. Gadeholt H. Centrilobular hepatic necrosis in cardiac failure. Acta

DOI: 10.2169/internalmedicine.46.0059
1070
Med Scand 176: 525-528, 1964.3. Bynum TE, Boitnott JK, Maddrey WC. Ischemic hepatitis. DigDis Sci 24: 129-135, 1979.
4. Nouel O, Henrion J, Bernau J, DeGott C, Rueff B, Benhamou JP.Fulminant hepatic failure due to transient circulatory failure in pa-tients with chronic heart disease. Dig Dis Sci 25: 49, 1980.
5. Ellenberg M, Osserman E. The role of shock in the production ofcentral liver cell necrosis. Am J Med 11: 170-177, 1951.
6. Killip T, Payne AM. High serum transaminase activity in heartdisease. Circulatory failure and hepatic necrosis. Circulation 21:646-660, 1960.
7. Rawson JS, Achord JL. Shock liver. South Med J 78: 1421-1425,1985.
8. Bang N. Serum glutamic-oxaloacetic transaminase activity as anindex of centrilobular liver cell necrosis in cardiac and circulatoryfailure. Acta Med Scand 164: 385-389, 1959.
9. Birgens HS, Henriksen J, Matzen P, Paulsen H. The Shock liver.Acta Med Scand 204: 417, 1978.
10. Holden WD, de Palma RG, Drucker WR, McKalen A. Ultrastruc-tural changes in hemorrhagic shock. Electron microscopic study ofliver, kidney and striated muscle cells in rats. Ann Surg 162: 517,1965.
11. Borokov SA, Volkova MI. Changes in the activity of certain en-zymes in acute disorders of liver blood flow. Pathol Fiziol EkspTher 1: 57, 1974.
12. Arcidi IM Jr, Moore GW, Hutchins GM. Hepatic morphology incardiac dysfunction: a clinicopathologic study of 100 subjects atautopsy. Am J Pathol 104: 159-166, 1981.
13. Gitlin N, Serio KM. Ischemic hepatitis: widening horizons. Am JGastroenterol 87: 831-836, 1992.
14. Henrion J, Schapira M, Heller FR. Ischemic hepatitis: the need forprecise criteria. J Clin Gastroenterol 23: 305, 1996.
15. Henrion J, Descamps O, Luwaert R, Schapira M, Parfonry A,Heller F. Hypoxic hepatitis in patients with cardiac failure: inci-dence in a coronary care unit and measurement of hepatic bloodflow. J Hepatol 21: 696-703, 1994.
16. Henrion J, Schapira M, Luwaert R, Cohn L, Delannoy A, HellerFR. Hypoxic hepatitis: Clinical and hemodynamic study in 142consecutive cases. Medicine 82 (6): 392-406, 2003.
17. Knaus WA, Draper EA, Wagner DP, Zimmerman J. Apache II: aseverity of disease classification system. Crit Care Med 13: 818-829, 1985.
18. Jolliffe N. Liver function in congestive heart failure. J Clin Invest8: 419, 1930.
19. Hajomanova B, Konikova Z, Musil J, Moserova J. Changes inbiochemical indices in rat liver tissue after intraperitoneal applica-tion of endotoxin. Acta Chir Plast 21: 182, 1979.
20. Davidson CS, Lewis JH, Tagnon W, Burton V, Bishop T. Medicalshock: Abnormal changes in patients with severe acute medical ill-nesses, with and without peripheral vascular failure. N Engl J Med234: 279, 1946.
21. Gibson PR, Dudley FJ. Ischemic hepatitis: clinical features, diag-nosis and prognosis. Aust N Z J Med 14: 822-825, 1984.
22. Seeto RK, Fenn B, Rockey DC. Ischemic hepatitis: clinical pres-entation and pathogenesis. Am J Med 109 (2): 109-113, 2001.
23. Fuchs S, Bogomolski-Yahalom V, Paltiel O, Ackerman Z.Ischemic hepatitis. Clinical and laboratory observation of 34 pa-tients. J Clin Gastroenterol 26: 183-186, 1984.
24. Richman SM, Delman AJ, Grob D. Alteration of indices of liverfunction in congestive heart failure with particular reference to se-rum enzymes. Am J Med 30: 211, 1962.
25. Raute-Ereinsen N, Squarr HN, Houx P. Blood, chemical and ultra-structural changes in human liver, following different forms ofshock. Verhandlungen der Deutschen Gesellschaft fur Pathologie62: 275, 1978.
26. Cohen JA, Kaplan NM. Left-sided heart failure presenting ashepatitis. Gastroenterology 74: 583, 1978.
27. Irie H, Mori W. Fatal hepatic necrosis after shock. Acta Pathol Jpn36: 363-374, 1986.
28. Henrion J, Colin L, Schmitz A, Schapira M, Heller FR. Ischemichepatitis in cirrhosis. Rare but lethal. J Clin Gastroenterol 16: 35-39, 1993.
29. Champeon HR, Jones RT, Trump BF, et al. A clinicopathologicstudy of hepatic dysfunction following shock. Surg Gyn Obst 142:657, 1976.
30. Grimaud D, Philip F, Livrelli N, LeForge D. Etude biologique dufoie de choc chez l. homme. Ann Anesth Franc 20: 79, 1979.
31. Wallach HF, Popper H. Central necrosis of the liver. Arch Path 49:33, 1950.
32. Lefer AM, Lalvin MJ. Comparison of the cytotoxic actions of hy-poxia and endotoxin in the perfused cat liver. Circ Shock 5: 14,1978.
33. Janson PMC, Kuhn SH, Geldenhuys JJ. Lysosomal disruption dur-ing the development of endotoxic shock in the baboon. S Afr MedJ 49: 1041, 1975.
34. Sayeed MM. Alterations in hepatic Na+-K+ transport during endo-toxemia in rats. Am J Phys 247 (3) [Pt.2] : R465-474, 1984.
35. Lens K, Logan J, Cohem JA. Shock liver. Leber Magen Darm(Engl. Abstr.) 12 (5): 198-202, 1982.
36. Cameron DE, Edhag O, Lanfrance A. Hepatocellular dysfunctionin early sepsis despite increased hepatic blood flow. Adv ShockRes 6: 65-74, 1981.
37. van Riel JM, Kerremans AL. Ischemic hepatitis. Ned TijdschrGeneeskd 136 (42): 2078-2081, 1992.
38. Jacquemin E, Saliba E, Blond MH, Bertrand C, Vaillet W. Liverdysfunction and acute cardiocirculatory failure in children. Eur JPediatr 151 (10): 731-734, 1992.
39. Kotake Y, Takeda J, Matsumoto M, Wasabe H, Iwata F. Subclini-cal hepatic dysfunction in laproscopic cholecystectomy and lapar-scopic colectomy. Br J Anaesth 87 (5): 774-777, 2001.
40. Turnage RH, Kadesky KM, Myers SI, Takala J, Wagner GR. He-patic hypoperfusion after intestinal reperfusion. Surgery 119 (2):151-160, 1996.
41. Jakob SM, Tenhunen JJ, Laitinen S, Clavian PA. Effects of sys-temic arterial hypoperusion on splanchnic hemodynamics and he-patic arterial buffer response in pigs. Am J Physiol GastrointestLiver Physiol 280 (5): G819-827, 2001.
42. Dunn GD, Hayes P, Breen KJ, Schenker S. The liver in congestiveheart failure: A review. Am J Med Sci 265: 174-189, 1973.
Ⓒ 2007 The Japanese Society of Internal Medicinehttp://www.naika.or.jp/imindex.html