Hypoxia-Induced Autophagy Promotes Tumor Cell Survival ... · nant cancers like glioblastomas....
12
Molecular and Cellular Pathobiology Hypoxia-Induced Autophagy Promotes Tumor Cell Survival and Adaptation to Antiangiogenic Treatment in Glioblastoma Yu-Long Hu, Michael DeLay, Arman Jahangiri, Annette M. Molinaro, Samuel D. Rose, W. Shawn Carbonell, and Manish K. Aghi Abstract Antiangiogenic therapy leads to devascularization that limits tumor growth. However, the benefits of angiogenesis inhibitors are typically transient and resistance often develops. In this study, we explored the hypothesis that hypoxia caused by antiangiogenic therapy induces tumor cell autophagy as a cytoprotective adaptive response, thereby promoting treatment resistance. Hypoxia-induced autophagy was dependent on signaling through the hypoxia-inducible factor-1a (HIF-1a)/AMPK pathway, and treatment of hypoxic cells with autophagy inhibitors caused a shift from autophagic to apoptotic cell death in vitro. In glioblastomas, clinically resistant to the VEGF-neutralizing antibody bevacizumab, increased regions of hypoxia and higher levels of autophagy-mediating BNIP3 were found when compared with pretreatment specimens from the same patients. When treated with bevacizumab alone, human glioblastoma xenografts showed increased BNIP3 expression and hypoxia-associated growth, which could be prevented by addition of the autophagy inhibitor chloroquine. In vivo targeting of the essential autophagy gene ATG7 also disrupted tumor growth when combined with bevacizumab treatment. Together, our findings elucidate a novel mechanism of resistance to antiangiogenic therapy in which hypoxia-mediated autophagy promotes tumor cell survival. One strong implication of our findings is that autophagy inhibitors may help prevent resistance to antiangiogenic therapy used in the clinic. Cancer Res; 72(7); 1773–83. Ó2012 AACR. Introduction The hypothesis that tumor progression can be curbed by antiangiogenic agents targeting abnormal tumor vessels has been confirmed by preclinical evidence and clinical trials (1). However, these initial successes were tempered by the failure of angiogenesis inhibitors to produce enduring clinical responses. For example, in clinical trials of VEGF-neutralizing antibody bevacizumab in glioblastoma, 40% to 60% of tumors progressed after initially successful treatment (2), consistent with the development of resistance to antiangiogenic therapy, a state exhibiting a poor prognosis and poor response to available treatments (3). The molecular basis of acquired resistance to antiangiogenic treatments causing this lack of sustained responses remains undefined. We hypothesized that the devascularization caused by antiangiogenic therapy increases tumor hypoxia and that this hypoxia mediates resistance to antiangiogenic therapy. Recent reports suggest that hypoxia activates autophagy, a lysosomal degradation pathway which may promote tumor cell survival (4). The mechanisms by which hypoxia induces autophagy need clarification, but the finding that BNIP3, a hypoxia-inducible factor-1a (HIF-1a) downstream target gene, is essential to hypoxia-induced autophagy suggests one pos- sible mechanism (5). During autophagy, a crescent-shaped structure, the isolation membrane, forms in the cytoplasm and closes around com- ponents targeted for destruction, leading to formation of the autophagosome, which fuses with the lysosome to become an autolysosome, leading to enzymatic degradation of autopha- gosome contents (6). While autophagosomes were initially identified in dying cells, a phenomenon that led to the term "autophagic cell death" to describe a cell death mode distinct from apoptosis, subsequent studies have shown that autop- hagy can allow cells to cope with stressors by destroying damaged proteins and organelles as a survival-promoting mechanism (7–9). During autophagosome formation, the ATG7 protein is essential for autophagosome membrane expansion (10). While autophagosomes sequester cytosolic material non- specifically in a process called nonselective autophagy, addi- tional evidence shows that a process of selective autophagy also occurs in which autophagic degradation of specific pro- tein aggregates or organelles targeted for destruction occurs. Selective autophagy degrading–specific proteins is asso- ciated with degradation of p62 (11), a protein complex that binds ubiquitinated protein aggregates to target them for Authors' Affiliation: University of California at San Francisco (UCSF) Neurosurgery, San Francisco, California Note: Supplementary data for this article are available at Cancer Research Online (http://cancerres.aacrjournals.org/). M. DeLay and A. Jahangiri contributed equally to the work. Corresponding Author: Manish K. Aghi, UCSF Neurosurgery, Diller Can- cer Research Building, 1450 Third Street, San Francisco, CA 94158. Phone: 415-353-1172; Fax: 415-353-3907; E-mail: [email protected] doi: 10.1158/0008-5472.CAN-11-3831 Ó2012 American Association for Cancer Research. Cancer Research www.aacrjournals.org 1773 on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831
Transcript of Hypoxia-Induced Autophagy Promotes Tumor Cell Survival ... · nant cancers like glioblastomas....

Molecular and Cellular Pathobiology
Hypoxia-Induced Autophagy Promotes Tumor Cell Survivaland Adaptation to Antiangiogenic Treatment in Glioblastoma
Yu-Long Hu, Michael DeLay, Arman Jahangiri, Annette M. Molinaro, Samuel D. Rose,W. Shawn Carbonell, and Manish K. Aghi
AbstractAntiangiogenic therapy leads to devascularization that limits tumor growth. However, the benefits of
angiogenesis inhibitors are typically transient and resistance often develops. In this study, we explored thehypothesis that hypoxia caused by antiangiogenic therapy induces tumor cell autophagy as a cytoprotectiveadaptive response, thereby promoting treatment resistance. Hypoxia-induced autophagy was dependent onsignaling through the hypoxia-inducible factor-1a (HIF-1a)/AMPK pathway, and treatment of hypoxic cells withautophagy inhibitors caused a shift from autophagic to apoptotic cell death in vitro. In glioblastomas, clinicallyresistant to the VEGF-neutralizing antibody bevacizumab, increased regions of hypoxia and higher levels ofautophagy-mediating BNIP3 were found when compared with pretreatment specimens from the same patients.When treated with bevacizumab alone, human glioblastoma xenografts showed increased BNIP3 expression andhypoxia-associated growth, which could be prevented by addition of the autophagy inhibitor chloroquine. In vivotargeting of the essential autophagy gene ATG7 also disrupted tumor growth when combined with bevacizumabtreatment. Together, our findings elucidate a novel mechanism of resistance to antiangiogenic therapy in whichhypoxia-mediated autophagy promotes tumor cell survival. One strong implication of our findings is thatautophagy inhibitors may help prevent resistance to antiangiogenic therapy used in the clinic. Cancer Res; 72(7);1773–83. �2012 AACR.
IntroductionThe hypothesis that tumor progression can be curbed by
antiangiogenic agents targeting abnormal tumor vessels hasbeen confirmed by preclinical evidence and clinical trials (1).However, these initial successes were tempered by the failureof angiogenesis inhibitors to produce enduring clinicalresponses. For example, in clinical trials of VEGF-neutralizingantibody bevacizumab in glioblastoma, 40% to 60% of tumorsprogressed after initially successful treatment (2), consistentwith the development of resistance to antiangiogenic therapy,a state exhibiting a poor prognosis and poor response toavailable treatments (3). The molecular basis of acquiredresistance to antiangiogenic treatments causing this lack ofsustained responses remains undefined. We hypothesized thatthe devascularization caused by antiangiogenic therapyincreases tumor hypoxia and that this hypoxia mediatesresistance to antiangiogenic therapy.
Recent reports suggest that hypoxia activates autophagy, alysosomal degradation pathway which may promote tumorcell survival (4). The mechanisms by which hypoxia inducesautophagy need clarification, but the finding that BNIP3, ahypoxia-inducible factor-1a (HIF-1a) downstream target gene,is essential to hypoxia-induced autophagy suggests one pos-sible mechanism (5).
During autophagy, a crescent-shaped structure, the isolationmembrane, forms in the cytoplasm and closes around com-ponents targeted for destruction, leading to formation of theautophagosome, which fuses with the lysosome to become anautolysosome, leading to enzymatic degradation of autopha-gosome contents (6). While autophagosomes were initiallyidentified in dying cells, a phenomenon that led to the term"autophagic cell death" to describe a cell death mode distinctfrom apoptosis, subsequent studies have shown that autop-hagy can allow cells to cope with stressors by destroyingdamaged proteins and organelles as a survival-promotingmechanism (7–9). During autophagosome formation, theATG7 protein is essential for autophagosome membraneexpansion (10).
While autophagosomes sequester cytosolic material non-specifically in a process called nonselective autophagy, addi-tional evidence shows that a process of selective autophagyalso occurs in which autophagic degradation of specific pro-tein aggregates or organelles targeted for destruction occurs.Selective autophagy degrading–specific proteins is asso-ciated with degradation of p62 (11), a protein complex thatbinds ubiquitinated protein aggregates to target them for
Authors' Affiliation: University of California at San Francisco (UCSF)Neurosurgery, San Francisco, California
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
M. DeLay and A. Jahangiri contributed equally to the work.
Corresponding Author:Manish K. Aghi, UCSF Neurosurgery, Diller Can-cerResearchBuilding, 1450ThirdStreet, SanFrancisco,CA94158. Phone:415-353-1172; Fax: 415-353-3907; E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-11-3831
�2012 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org 1773
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

degradation, or BNIP3, a marker of autophagic destruction ofmitochondria. Nonselective autophagy can involve microtu-bule-associated protein light chain 3 (LC3), a protein that, afterconversion from its cytosolic form LC3-I to its autophagosomemembrane–associated form LC3-II, is ultimately degraded bylysosomal enzymes in autolysosomes during nonselectiveautophagy, causing the total amount of LC3 (LC3-I plusLC3-II) to drop (6).
We report here that increasing tumor hypoxia occurs duringantiangiogenic therapy and increases tumor cell autophagy asa cell survival mechanism, a novel resistance mechanism toantiangiogenic therapy. We then investigated the role of hyp-oxia-upregulated pathways in promoting autophagy. Weshowed the translational impact of this novel mechanism ofresistance to antiangiogenic therapy by showing in animalmodels that pharmacologic or genetic autophagy disruptionprevented hypoxia-associated resistance to antiangiogenictherapy. On the basis of the targetable novel mechanism ofresistance to antiangiogenic therapy described here, combin-ing antiangiogenic therapy with autophagy inhibition is atherapeutic strategy warranting further investigation in malig-nant cancers like glioblastomas.
Materials and MethodsCells and reagents
Cell lines and protocols for primary tumor cell isolation aredescribed in Supplementary Methods. A total of 300,000 cellsper well were plated in 12-well plates overnight in Dulbecco'sModified Eagle's Medium with 10% FBS, then cultured undernormoxia (5% CO2, 20%O2, 74%N2) or hypoxia (5% CO2, 1% O2,94% N2) in a humidified O2 control incubator (Sanyo) neveropened during incubation. Cells were incubated for 3, 6, 16, and24 hours in dimethyl sulfoxide (DMSO; control), bafilomycinA1(BafA1, 1 nmol/L), 3-methyladenine (3-MA, 1 mmol/L), chlo-roquine (10 mmol/L), or YC-1 (10 mmol/L; Sigma). To quantifyGFP-LC3 punctate in U373/GFP cells, 5 random 40� fieldswere photographed and the average percentage of cells perfield containing more than 10 intracellular GFP-LC3 punctatedots was calculated.
Real-time reverse transcriptase PCRReal-time reverse transcriptase PCR is described in Supple-
mentary Methods.
siRNA transfectionA total of 300,000 cells per well in 12-well plates were
transfected overnight using METAFECTENE transfectionreagent (Biontex Laboratories) with 20 nmol/L of negativecontrol, HIF-1a, or AMPKa siGENOME SMARTpool siRNAs(Dharmacon, Inc.), which combine 4 siRNAs into a single pool.After culture with fresh medium for 24 hours, knockdown wasconfirmed by Western blotting.
Short hairpin RNA–mediated ATG7 knockdownU87MG and SF8557 cells were infected with SMARTvector2.0
shRNA lentiviral particles (Thermo Scientific) expressingnontargeting negative control (S-005000-01) or 3 human ATG7short hairpin RNAs (shRNA; SH-020112-01, SH020112-02, and
SH020112-03) in the presence of 4 mg/mL polybrene. After 48hours, subcultured cells were selected in 1mg/mLpuromycin for1 week. Lysates from stably selected cells were assessed forATG7 expression by Western blotting.
Western blottingWestern blotting was carried out as described in the Sup-
plementary Methods.
Cell proliferation and apoptosis assaysA total of 5,000 cells per well in 96-well plates in triplicate
were plated overnight, then treated with DMSO, 3-MA (1mmol/L), or BafA1 (5 nmol/L) under normoxia or hypoxia for48 hours. For extended treatment (72 hours), cells were treatedwith DMSO, BafA1 (1, 2.5 nmol/L), or chloroquine (10 or 25mmol/L). Relative cell numbers were measured by CellTiter 96Aqueous One Solution Cell Proliferation Assay (Promega). Forapoptosis assays, onemillion cells perwell were plated in 6-wellplates overnight, then treatedwithDMSO, 1mmol/L 3-MA, or 1nmol/L BafA1 for 24 hours. Apoptotic and necrotic cells weremeasured by FITC-Annexin V Apoptosis Detection Kits (BDPharmingen), with FACS carried out with a BD FACSCalibur IImachine with FlowJo software (Tree Star, Inc.).
XenograftsProcedures are described in Supplementary Methods. After
tumors were established (mean subcutaneous volume ¼ 32mm3 or 7 days postintracranial implantation), 5 (subcutaneoustumors) or 10 (intracranial tumors) mice per group wererandomly allocated to treatment groups (SupplementaryMethods). Tumors were measured with calipers twice weekly.Tumor volume was (width)2 � length/2, and fold-growth wasrelative to treatment day one. Treatment continued until micereached IACUC euthanasia criteria (2.1 cmmaximal dimensionor tumor symptoms). To measure tumor oxygenation, somemice received 60 mg/kg pimonidazole (Hypoxyprobe, Inc.)intraperitoneally 1 hour before euthanasia.
Human tissue and xenograft immunohistochemistryParaffin-embedded sections and xenografts were processed
as described in Supplementary Methods. Photographs weretaken with a Zeiss Axioskop 2 and a Zeiss Axiocam color CCD.Staining quantification is described in SupplementaryMethods.
StatisticsTwo group comparisons of nonnormal values were carried
out using the Wilcoxon signed rank (paired samples, e.g., pre-and posttreatment) or Wilcoxon rank-sum (unpaired) tests.For subcutaneous tumor volumes, initial comparison of 3 ormore groups used the Kruskal–Wallis test (nonparametricalternative to ANOVA), followed by subsequent post hoctesting using the Wilcoxon rank-sum test for 2 group analyses.Kaplan–Meier analysis was used to compare survival betweengroups. P < 0.05 was considered significant, except for the posthoc Wilcoxon rank-sum testing, for which a Bonferroni cor-rection for multiple testing required usingak < 0.01 (i.e., 0.01¼0.05/k, where k ¼ 5) to define significance. Error bars are SDs,
Hu et al.
Cancer Res; 72(7) April 1, 2012 Cancer Research1774
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

except for tumor volumes, whose error bars are standarderrors. Experiments were repeated in triplicate with similarresults each time, with figures containing representativeexperiments.
ResultsPatient tumors resistant to antiangiogenic therapyexhibit increased hypoxia compared with beforetreatmentReview of an institutional database of 234 bevacizumab-
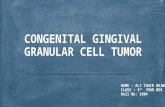
treated glioblastomas from 2006 to 2010 revealed 6 casesmeeting the following criteria: (i) after initial radiographicresponse to bevacizumab asmonotherapy (n¼ 2) or combinedwith topoisomerase inhibitor irinotecan (n ¼ 4), these casesexhibited the nonenhancing FLAIR bright growth onMRI seenin bevacizumab-treated glioblastomas (12, 13); (ii) surgicalresection of the bevacizumab-resistant tumor occurred within28 days of last bevacizumab dose; and (iii) archived paired pre-and posttreatment tissue was available. Tumor vessel density,assessed by CD31 immunostaining, decreased nearly 60% afterbevacizumab resistance compared with pretreatment speci-mens from these patients (P < 0.001), meanwhile hypoxia-inducible genes HIF-1a and carbonic anhydrase 9 (CA9; ref. 14)immunostaining increased nearly 70% (Fig. 1, P< 0.05) and 80%(Fig. 1, P < 0.05), respectively. These trends persisted whenseparating cases into those growing during bevacizumabmonotherapy (70% decreased vessel density, 72% increased
HIF-1a immunostaining, and 40% increased CA9 immunos-taining) versus those growing during bevacizumab plus irino-tecan, (50% decreased vessel density, 67% increased HIF-1aimmunostaining, and double the CA9 immunostaining), sug-gesting that, while irinotecan inhibition of HIF-1a expression(15) was more than offset by bevacizumab-induced devascu-larization and hypoxia-inducible gene expression.
Hypoxia induces autophagy in human glioblastoma celllines
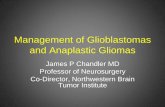
Briefly culturing U87MG and T98G glioma cell lines inhypoxia caused at least 2 autophagy-associated changes thatprogressively accumulated at 3, 6, 16, and 24 hours: degrada-tion of total LC3 (LC3-I plus LC3-II) and p62 were seen inU87MG and T98G cells (Fig. 2A–C). Of note, LC3-II expressionincreased over time in normoxia, consistent with basal autop-hagy due to metabolite accumulation (16), but this autophagywas clearly increased by hypoxia. Minimal contribution oftranscriptional changes to hypoxia-induced autophagy wassuggested by the finding that hypoxia-associated alterationsin levels of LC3A, LC3B, and p62 transcripts were insignificant(P¼ 0.1–0.9, Supplementary Fig S1) and did not correlate withhypoxia duration, consistent with prior reports (17, 18). Similarresults were observed in U251, U138MG, A172, and G55 glio-blastoma cell lines (Figs. 2D, Supplementary Fig. S2A). LC3-I toLC3-II conversion, a third autophagy-associated change (19),was seen in hypoxic T98G (Fig. 2B), U251 (Fig. 2D), and G55(Supplementary Fig. S2A) cells. We further confirmed hypoxia-
Figure 1. Glioblastoma (GBM)progressing during antiangiogenictherapy exhibit decreased vesseldensity, increased hypoxia, andincreased BNIP3 staining comparedwith pretreatment glioblastomasfrom the same patients. A,representative immunostaining forendothelial marker CD31 (top row),hypoxia markers HIF-1a (secondrow; blue, Hoescht nuclear staining;green, HIF-1a), and CA9 (third row)and autophagy-mediating BNIP3(bottom row; blue, Hoescht nuclearstaining; green, BNIP3) in thisglioblastoma resistant tobevacizumab (right) compared withpaired specimens from the samepatient before treatment (left). CA9and BNIP3 stainings are fromadjacent sections. B, vessel densitydecreased (P < 0.001), hypoxiamarker HIF-1a staining increased(P < 0.05), hypoxia marker CA9staining increased (P < 0.05), andBNIP3 immunostaining increased(P < 0.001) in 6 glioblastomas afterbevacizumab resistance comparedwith paired pretreatment specimens.Magnification, �40; scale bar,200 mm. hpf, high-power field.
Autophagy Mediates Resistance to Antiangiogenic Therapy
www.aacrjournals.org Cancer Res; 72(7) April 1, 2012 1775
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

induced autophagy when we identified that hypoxia upregu-lated BNIP3 expression in all human glioblastoma cell linesexamined (Fig. 2E).
Hypoxia upregulates autophagy in primaryglioblastoma cells
Because primary cells might respond differently to hypoxiathan cell lines, we studied the ability of hypoxia to induceautophagy-associated protein changes in primary glioblasto-ma cells from freshly resected human glioblastomas. Hypoxiainduced the same autophagy-associated changes found in celllines, degradation of p62 and total LC3, in the primary humanglioblastoma cells SF8244, SF8167, SF8106, and SF7796, with 2of these primary human glioblastoma cells also exhibitinghypoxia-induced LC3-I to LC3-II conversion (Figs. 2F, Supple-mentary Fig. S2A). Because the ATG4 protease modifies LC3(20), we investigated ATG4 expression in cells exhibiting(T98G, SF8167, and SF7796) or not exhibiting (SF8106) hypox-ia-induced LC3-I to LC3-II conversion. ATG4A and ATG4Bhomologues were not detectable in these cells (data notshown), whereas ATG4C expression decreased slightly withhypoxia in T98G and the 3 primary glioma cells (Supplemen-tary Fig. S3), suggesting that ATG4C did not contribute to the
hypoxia-induced LC3-I to LC3-II conversion occurring inmanyglioma cells.
Increased expression of autophagy mediators in humanglioblastomas after bevacizumab resistance
We used immunohistochemistry to identify hypoxic areasand areas that stained positive for autophagy mediatorBNIP3 in 6 bevacizumab-resistant glioblastomas and thepaired pretreatment glioblastomas from these samepatients. The increased hypoxia of these specimens afterbevacizumab resistance compared with before was quanti-fied earlier. While the core of hypoxic areas in these bev-acizumab-resistant glioblastomas was often necrotic, thehypoxic periphery of these necrotic areas stained positivefor autophagy-mediating factor BNIP3 (Fig. 1A). Tumorsexhibited increased BNIP3 immunoreactivity after bevaci-zumab failure in a manner reflecting the greater hypoxiaseen after resistance to antiangiogenic therapy (Fig. 1A),with image analysis revealing 55% more BNIP3 immunos-taining in the 6 glioblastomas after bevacizumab resistancethan in tumors from the same patients before bevacizumabtreatment (Fig. 1B, P < 0.001). These trends persisted whenseparating cases into those treated with bevacizumab
Figure 2. Hypoxia causesautophagy-associated proteinchanges in glioblastoma cells.Culturing U87MG (A) and T98G (B)glioblastoma cells in hypoxia for upto 24 hours increased, relative tonormoxia degradation of p62 andtotal LC3 (C), with T98G cells alsoshowing increased conversion ofLC3-I to LC3-II in hypoxia (B).Similar findings in 3 other gliomacell lines (U251, U138, A172, andG55) are shown at 24 hours (D). Allcell lines also showed hypoxia-induced increased expression ofautophagy-mediating BNIP3 (E).F, culturing primary glioma cellsSF8167, SF8106, SF7796, andSF8244 led to the same hypoxia-induced autophagy-associatedchanges (p62 degradation, LC3-Ito LC3-II conversion, anddegradation of total LC3) after 24hours. GAPDH, glyceraldehyde-3-phosphate dehydrogenase.
Hu et al.
Cancer Res; 72(7) April 1, 2012 Cancer Research1776
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

monotherapy (53% increased BNIP3 immunostaining) ver-sus bevacizumab plus irinotecan (57% increased BNIP3immunostaining).
Autophagy inhibitors disrupt hypoxia-inducedglioblastoma autophagyEarly autophagy inhibitor 3-MAand late autophagy inhibitor
BafA1 both blocked hypoxia-induced p62 degradation (Fig.4A). 3-MA inhibited LC3-I to LC3-II conversion, whereas lateautophagy inhibitor BafA1 increased LC3-I to LC3-II conver-sion (Fig. 3A), reflecting the fact that these inhibitors disruptautophagy either before (3-MA) or after (BafA1) LC3-I to LC3-IIconversion. Similar effects were seen in U373 cells transducedto express a GFP-LC3 fusion protein, with hypoxia increasingautophagy, as assessed by the number of cells with punctategreen staining, amarker reduced by early autophagy inhibitors,and Western blotting for free GFP released by autophagicdegradation, a marker reduced by early and late autophagyinhibitors (16). Early autophagy inhibitor 3-MA lowered thenumber of cells with punctate green staining in hypoxia, andlate autophagy inhibitor BafA1 maintained the high number ofcells with punctate green staining seen in hypoxia (Figs. 3B andC, P < 0.01). Similarly, hypoxia increased free GFP identifiedbyWestern blotting over 3-fold, with free GFP lowered by early
(3-MA) or late (BafA1) autophagy inhibitors, particularly thelatter (Supplementary Fig. S4),
Inhibiting hypoxia-induced autophagy increases celldeath
Next we measured cell survival under hypoxic culturingconditions in the presence of either 3-MA or BafA1. BafA1significantly decreased the number of viable U87MG andT98G cells in hypoxia (Fig. 4A, P < 0.05), with 3-MA havingslightly less inhibitory effects on cell viability (Fig. 4A, P¼ 0.06).Having shown a survival-promoting effect of hypoxia-inducedautophagy, we characterized the type of cell death occurring inhypoxia when autophagy was inhibited. We conducted flowcytometry after using Annexin V (AnnV) and propidium iodine(PI) to label hypoxic U87MGcells that hadbeen treatedwith andwithout autophagy inhibitors. In the presence of 3-MA or BafA1,hypoxia significantly increased the number of cells that wereAnnVþPIþ (late-stage apoptosis; BafA1, P< 0.01; 3-MA, P< 0.05),whereas the number of AnnVþPI� cells in early apoptosis didnot change (Fig. 4B, P > 0.05). The percentage of total PARP thatwas active or cleaved, an apoptosismarker, increased in hypoxiccells treated with autophagy inhibitors, with lesser effects seenin normoxia (Fig. 4C), suggesting that the cell death promotedwhen autophagy was inhibited was apoptotic.
Figure 3. Autophagy inhibitors block the hypoxia-induced expression of autophagy mediators in glioma cells. A, after 24 hours, 3-MA (1 mmol/L) and BafA1(1 nmol/L) blocked hypoxia-induced p62 degradation in cultured U87MG cells. 3-MA inhibited conversion of LC3-I to LC3-II, whereas BafA1 increased LC3-Ito LC3-II conversion. B, after 24 hours of hypoxia, U373/GFP-LC3 cells exhibitedmore punctate green fluorescent staining, consistent with autophagy, whichdecreased after 3-MA treatment, but remained high after BafA1 treatment. Magnification, �40; scale bar, 200 mm. C, 3-MA reduced the percentage of cellswith more than 10 punctate green fluorescent dots (P ¼ 0.01). GAPDH, glyceraldehyde-3-phosphate dehydrogenase.
Autophagy Mediates Resistance to Antiangiogenic Therapy
www.aacrjournals.org Cancer Res; 72(7) April 1, 2012 1777
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

Dependence of various aspects of hypoxia-inducedautophagy on HIF-1a or AMPK
Pathways activated by hypoxia in tumor cells that cancontribute to autophagy include those mediated by HIF-1a,activated during physiologic hypoxia (O2, 0.1%–3%), or by HIF-1a–independent 50 AMP–activated protein kinase (AMPK),activated during anoxia (�0.01% O2; ref. 4). At 1% O2, bothHIF-1a and AMPK were activated in U87MG and T98G cells,withHIF-1a activation occurring earlier than AMPKactivation(Fig. 5A). Furthermore, siRNA-mediated knockdown of AMPKor HIF-1a blocked hypoxia-mediated LC3-I to LC3-II conver-sion and total LC3 degradation but neither siRNA affectedhypoxia-mediated p62 degradation (Fig. 5B). Similarly, HIF-1ainhibitor YC-1 (21) blocked hypoxia-mediated total LC3 deg-radation and LC3-I to LC3-II conversion but did not affecthypoxia-mediated p62 degradation (Fig. 5C). We then inves-tigated the role of HIF-1a or AMPK in the hypoxia-mediatedBNIP3 expression identified earlier. Hypoxia-induced BNIP3expression was reduced with HIF-1a inhibition achievedthrough HIF-1a siRNA (Fig. 5B) or YC-1 (Fig. 5D). In contrast,AMPK inhibition achieved through AMPK siRNA failed to alterhypoxic induction of BNIP3 (Fig. 5B). Therefore, hypoxia-mediated LC3-I to LC3-II conversion depended on HIF-1a andAMPK, hypoxia-mediate BNIP3 expression depended on HIF-1a not AMPK, and hypoxia-mediated p62 degradationoccurred independent of these pathways.
Combined inhibition of autophagy and angiogenesisexerts a potent antitumor effect in vivo
3-MAandBafA1 are typically used as autophagy inhibitors invitro (22), but chloroquine or hydroxyl-chloroquine, late autop-hagy inhibitors like BafA1, are used to inhibit autophagy in vivo(23), partly because they are the only U.S. Food and Drug
Administration (FDA)-approved autophagy inhibitors. LikeBafA1, chloroquine blocked hypoxia-induced p62 degradation,but by blocking autophagy after LC3-I to LC3-II conversion,caused more LC3-I to LC3-II conversion to occur in culturedU87MG, GBM39, and G55 glioma cells (Supplementary Figs.S2B and S5A), and decreased the viability of U87MG (P < 0.05,Supplementary Fig. S5B) and G55 (P < 0.05, Supplementary Fig.S2C) in hypoxia compared with normoxia. We also examinedthe effect of chloroquine onBNIP3 expression in 5 cell lines andxenograft-derived cells and found that, whereas hypoxiaincreased BNIP3 expression in all cells, chloroquine minimallyaffected BNIP3 expression under normoxia or hypoxia (Sup-plementary Fig. S5C), consistent with prior in vitro reports (24),and suggesting that late autophagy inhibitor chloroquineexerted its effects downstream of BNIP3 upregulation.
We then investigatedwhether chloroquine counteracted thesurvival-promoting effects of hypoxia-induced autophagycaused by antiangiogenic treatment by treating subcutaneoustumors derived from GBM39 primary glioma cells with autop-hagy inhibitor chloroquine and/or antiangiogenic agent bev-acizumab. After 4weeks, tumor volumes differed between the 4treatment groups (P < 0.05) and, compared with PBS, neitherchloroquine nor bevacizumab inhibited tumor growth (P ¼0.3–0.8). Combined therapy (bevacizumab þ chloroquine)inhibited tumor growth in a prolonged and significant mannerversus either agent alone (P < 0.01, bevacizumab vs. bevaci-zumabþ chloroquine; P < 0.005, chloroquine vs. bevacizumabþ chloroquine; Fig. 6A). Bevacizumab-treated tumors, with orwithout combined chloroquine, exhibited 4- to 6-fold reducedvessel density (P< 0.01) and over double increased hypoxic area(P < 0.05), compared with PBS-treated tumors or tumorstreated with chloroquine monotherapy (Fig. 6B), confirmingthat antiangiogenic therapy induced devascularization and
Figure 4. Inhibiting hypoxia-induced autophagy increases cell death. A, U87MG and T98G cells in hypoxia for 48 hours exhibited decreased cell numbers, asassessed by absorbance at 490 nm (reflecting number of cells) minus background measured in the MTS assay, when treated with 3-MA (1 mmol/L) orbafilomycin A1 (BafA1, 1 nmol/L; P < 0.05). B, U87MG cells in hypoxia for 24 hours exhibited an increased percentage of AnnexinVþPIþ cells (permeabilizednear death cells, left bars) in the presence of 3-MA (P<0.05) or BafA1 (P <0.01) relative to the presenceof these inhibitors in normoxia, whereas these inhibitorsdid not change the percentage of AnnexinVþPI� cells (early apoptosis, right bars) in hypoxia (P > 0.05). C, Western blotting revealed increased cleavage ofPARP, indicating apoptosis, in hypoxic cells treated with 3-MA or BafA1 for 24 hours, suggesting that autophagy inhibitors were promoting apoptosis.GAPDH, glyceraldehyde-3-phosphate dehydrogenase.
Hu et al.
Cancer Res; 72(7) April 1, 2012 Cancer Research1778
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

hypoxia. While bevacizumab monotherapy increased BNIP3expression nearly 2-fold over than PBS or chloroquine treat-ment (P < 0.05), adding chloroquine to bevacizumab reducedBNIP3 expression to levels comparable with PBS- or chloro-quine-treated tumors (Fig. 6B, P < 0.05). Cell death in thesexenografts was characterized using terminal deoxynucleotidyltransferase–mediated dUTP nick end labeling (TUNEL) stain-ing to detect cells in late apoptosis, and staining increased over2-fold in chloroquine-treated xenografts compared with PBS-treated xenografts (P < 0.01) and nearly 4-fold in bevacizumabplus chloroquine–treated xenografts compared with bevaci-zumab-treated xenografts (Fig. 6B, P < 0.05).Similar sustained tumor growth inhibition in combined
treated tumors versus eventual accelerated growth in bevaci-zumab-treated tumors was noted in subcutaneous U87MGtumors (P < 0.005 for 4 group comparison; P < 0.01, bevacizu-mab vs. bevacizumabþ chloroquine; Supplementary Fig. S6A)
and G55 (P < 0.001 for 4 group comparison; P < 0.01, bevaci-zumab vs. bevacizumab þ chloroquine after 8 and 11 treat-ment days; Supplementary Fig. S7A) human glioma cell lines.For U87MG-derived xenografts, prolonged treatment of thebevacizumab monotherapy and bevacizumab plus chloro-quine groups for 2 additional weeks increased the separationbetween the 2 groups, with bevacizumab-treated tumors exhi-biting an increased growth rate, and the combined treatmenttumors exhibiting sustained growth suppression (P < 0.01,Supplementary Fig. S6B). Immunohistochemistry of treatedU87MG xenografts revealed similar findings as seen withGBM39–decreased vessel density and increased hypoxia inbevacizumab-treated xenografts, increased BNIP3 expressionin bevacizumab-treated xenografts, and increased TUNELstaining in chloroquine-treated xenografts (SupplementaryFig. S6C). Western blotting of protein from subcutaneousU87MG tumors revealed increased LC3-I to LC3-II conversion
Figure 5. Hypoxia upregulatesHIF-1a expression and AMPKphosphorylation, which contribute tosome aspects of hypoxia-inducedautophagy. A, U87MG and T98Gcells cultured in hypoxia exhibitedtime-dependent activation of HIF-1aand AMPK (with AMPK activationassessed by detectingphosphorylated AMPK in the firstrow), with HIF-1a activationoccurring before AMPKactivation. B,siRNA-mediated knockdown ofAMPK and HIF-1a in hypoxicU87MGcells exhibited reduced LC3-I to LC3-II conversion and reducedtotal LC3 degradation but neithersiRNA affected hypoxia-mediatedp62 degradation, whereas only HIF-1a siRNA reduced hypoxia-inducedBNIP3 expression. C, similarly, YC-1(a HIF-1a inhibitor) blocked hypoxia-mediated LC3-I to LC3-II conversionand total LC3 degradation withoutaffecting hypoxia-mediated p62degradation in T98G cells. D, inU87MG cells cultured for 24 hours inhypoxia, YC-1 blocked hypoxia-mediated BNIP3 upregulation.
Autophagy Mediates Resistance to Antiangiogenic Therapy
www.aacrjournals.org Cancer Res; 72(7) April 1, 2012 1779
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

Hu et al.
Cancer Res; 72(7) April 1, 2012 Cancer Research1780
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

after bevacizumab treatment, consistent with autophagy, andafter chloroquine treatment, consistent with our in vitro datareflecting the fact that chloroquine is a late autophagy inhibitor(Supplementary Fig. S6D).Another patient specimen–derived subcutaneous xenograft,
SF8244, exhibited similar sustained lack of growth in combinedtreated tumors versus eventual accelerated growth in bevaci-zumab-treated tumors (P < 0.01 for 4 group comparison,Supplementary Fig. S7B). Delayed chloroquine addition tobevacizumab-treated SF8244 tumors that had reachedvolumes averaging 400 mm3 reduced tumor volume whereasbevacizumab-treated tumors continued exponential growth(P < 0.001, Supplementary Fig. S7B), suggesting that inhibitingautophagy upon initiation of resistant growth could stillsuppress antiangiogenic therapy resistance. Chloroquine alonedid not affect tumor growth compared with PBS in anyxenografts (P ¼ 0.4–0.7).
Knockdown of essential autophagy gene ATG7 promotesbevacizumab responsiveness in vivoBecause chloroquine could exert nonspecific effects, tomore
precisely define the contribution of autophagy to antiangio-genic therapy resistance, we engineered U87MG and SF8557glioma cells to stably express 3 different shRNAs targetingautophagy-mediating gene ATG7 (Supplementary Fig. S8A).Cells expressing the shRNA causing greatest ATG7 knockdownexhibited inhibition of 2 hypoxia-mediated autophagy-associ-ated protein changes, p62 degradation, and LC3-I to LC3-IIconversion (Supplementary Fig. S8B). We treated subcutane-ous tumors derived from U87MG/shControl and U87MG/shATG7 cells and intracranial tumors derived from SF8557/shControl and SF8557/shATG7 cells with PBS or bevacizumab.Whereas subcutaneous U87MG/shControl (Fig. 6C) and intra-cranial SF8557/shControl (Fig. 6D) tumors exhibited noresponse to bevacizumab (P ¼ 0.3–0.8), all subcutaneousU87MG/shATG7 tumors regressed to cure (Fig. 6C, P <0.001) and intracranial SF8557/shATG7 tumors exhibited90% long-term survival (Fig. 6D) with bevacizumab treatment(P ¼ 0.003). Immunostaining subcutaneous and intracranialshRNA–transduced tumors except for bevacizumab-treatedsubcutaneous U87MG/shATG7 tumors, which were cured,revealed that bevacizumab decreased vascularity andincreased hypoxia in shControl- and shATG7-transducedectopic and orthotopic tumors (P < 0.05, Supplementary Fig.
S9), consistent with our in vivo results with other bevacizumab-treated tumors. BNIP3 expression increasedwith bevacizumabtreatment of shControl- and shATG7-transduced tumors (P <0.05, Supplementary Fig. S9), with the former consistent withour other in vivo results and the latter consistent with a priorreport (25).
DiscussionCells exposed to various stressors undergo a process of self-
digestion known as autophagy, during which cytoplasmiccargo sequestered inside double-membrane vesicles are deliv-ered to the lysosome for degradation. Several in vitro studiessuggest that, while autophagy initially prevents cancer cellsurvival, once a tumor develops, autophagic self-catabolizationof damaged organelles promotes cell survival by allowingtumor cells to survive the hypoxia and the nutrient and growthfactor deprivation (7–9) found in the tumor microenviron-ment. Suggestion that autophagy promotes tumor cell survivalin vivo comes from the correlation of immunostaining forautophagy-promoting BNIP3 with poor cancer survival (26,27). Several cancer therapies induce autophagy (28–30), andthe autophagic response to some treatments is cytoprotective(31).
Because of the failures of conventional DNA-damagingchemotherapy, antiangiogenic therapy has been investigated,with efficacy showed in several cancer clinical trials. However,this efficacy is often transient with acquired resistance toantiangiogenic therapy common (32). While antiangiogenictherapy can transiently normalize structural and functionalabnormalities in tumor vessels (33), the long-term effect ofantiangiogenic therapy is tumor devascularization, which ulti-mately worsens tumor hypoxia.
We hypothesized that hypoxia, as occurs after antiangio-genic therapy (34), would promote autophagy as a cytopro-tective adaptive mechanism. Others have shown that hypoxiaupregulates autophagy-associated factors, like BNIP3 (35), afinding supported by the identification of BNIP3 expression inperinecrotic regions of patient tumor specimens (36), butwhether the response is cytoprotective and which pathwaysare involved remain undetermined.
The cytoprotective nature of autophagy during hypoxiainduced by antiangiogenic therapy was verified by ourin vitro data showing decreased survival of cells treated
Figure 6. Autophagy inhibitor chloroquine (Chloro) combined with bevacizumab (Bev) inhibits GBM39 tumor growth in vivo. A, subcutaneous tumors inathymic mice were treated with PBS, chloroquine, bevacizumab, and chloroquine plus bevacizumab. After 4 weeks, there were significantly differenttumor volumes amongst groups (P < 0.05). Compared with PBS (black), neither chloroquine (pink) nor bevacizumab (blue) inhibited tumor growth(P ¼ 0.3–0.8). Combined therapy with bevacizumab and chloroquine (red) inhibited tumor growth in a prolonged and statistically significant mannerrelative to either agent alone (P < 0.01, bevacizumab vs. bevacizumab þ chloroquine; P < 0.005, chloroquine vs. bevacizumab þ chloroquine). B, vesseldensity (CD31 staining, red) decreased in bevacizumab-treated tumors (P < 0.01). Hypoxia (CA9 staining, green) increased in bevacizumab-treated tumors(P < 0.05). BNIP3 expression (green) increased with bevacizumab treatment (P < 0.05), an increase eliminated by adding chloroquine to bevacizumab(P < 0.05). TUNEL staining (red) increased in chloroquine-treated tumors (P < 0.05). 40, 6-Diamidino-2-phenylindole (DAPI) nuclear counterstaining is blue.Bevacizumab plus chloroquine–treated tumors were small enough that the entire tumor fit one field of view. Magnification, �20; scale bar, 200 mm. C, whensubcutaneous U87MG/shControl and U87MG/shATG7 xenografts were treated with PBS or bevacizumab, U87MG/shATG7 tumors completely regressedwith bevacizumab treatment (P < 0.001), whereas U87MG/shControl xenografts were minimally responsive (P ¼ 0.8). D, intracranial SF8557/shATG7xenografts exhibited 90% long-term survival with bevacizumab treatment, whereas PBS treatment of intracranial SF8557/shATG7 xenografts led to 18-daymedian survival (P¼ 0.003). Intracranial SF8557/shControl xenografts exhibited 15-daymedian survival with PBS, similar to their 18-daymedian survival withbevacizumab (P ¼ 0.3).
Autophagy Mediates Resistance to Antiangiogenic Therapy
www.aacrjournals.org Cancer Res; 72(7) April 1, 2012 1781
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

with autophagy inhibitors in hypoxic conditions, particularlywith late autophagy inhibitors, and more so at 72 hours(Supplementary Fig. S5B) than 48 hours (Fig. 4A) and ourin vivo data showing increased TUNEL staining in chloro-quine plus bevacizumab–treated xenografts compared withbevacizumab-treated xenografts (Fig. 6B, SupplementaryFig. S6C), suggesting an increased number of apoptotic cellsduring combined treatment. Of note, while chloroquineconsistently exerted antitumor effects in hypoxic conditionsin vitro and when combined with antiangiogenic therapyin vivo, it promoted tumor growth, albeit in a manner notquite statistically significant, in normoxic U87MG cells(Supplementary Fig. S5B) and as monotherapy comparedwith PBS in G55 xenografts (Supplementary Fig. S7A). Sim-ilarly, in addition to potentiating the response to antiangio-genic therapy, ATG7 knockdown caused faster in vivo growthof PBS-treated tumors than wild-type tumors. These findingsillustrate the dual functions of autophagy—a tumoricidaleffect under normoxic unstressed conditions, such thatautophagy inhibition under those conditions can actuallypromote tumor growth, versus a tumor-protective effectupon exposure to stressors like the hypoxia caused byantiangiogenic therapy. These dual functions of autophagysuggest that inhibiting autophagy may be of limited clinicalvalue alone but, when used with antiangiogenic therapy,could provide a therapeutic benefit. These findings alsosuggest that the effect we observed in vivo was not theadditive effect of combining 2 antitumor agents but insteadreflected the ability of one therapeutic modality, antiangio-genic treatment, to turn another modality, autophagy inhi-bition, with mild tumor-promoting effects into a true anti-tumor strategy.
The tumor response to hypoxia activates several factors,including HIF-1a-, felt to activate at moderate hypoxia(0.1%), and HIF-1a–independent AMPK, felt to activate atanoxia (0.01%; ref. 4). We found that at 1% oxygen, aconcentration more typical of glioblastomas than 0.1% or0.01% (37), both HIF-1a and AMPK were activated, with HIF-1a activated earlier than AMPK, suggesting that, differentdurations of hypoxia, not just different hypoxia levels, maydifferentially activate these pathways. Both HIF-1a andAMPK could contribute to autophagy, with mTOR inhibitiona possible mechanism (38–41). We found that hypoxia-mediated LC3-I to LC3-II conversion and overall LC3 deg-radation depended on both HIF-1a and AMPK, hypoxia-mediated BNIP3 expression depended on HIF-1a not AMPK,and hypoxia-mediated p62 degradation was independent ofHIF-1a and AMPK. While LC3 contributes to nonselectiveautophagy (degradation of bulk cytoplasmic contentsincluding organelles), p62 degradation and BNIP3 expres-sion are more involved in selective autophagy destroyingubiquitinated proteins and mitochondria, respectively.Future studies will need to clarify mediators of hypoxia-induced p62 degradation.
Interestingly, chloroquine minimally affected BNIP3expression in our cultured cells, consistent with priorreports using cultured colon carcinoma cells treated withBafA1, another late autophagy inhibitor (42), and suggesting
that chloroquine inhibited autophagy downstream of BNIP3expression. In contrast, chloroquine lowered BNIP3 expres-sion in bevacizumab-treated xenografts. The differencesbetween these in vitro and in vivo results could reflect asyet uncharacterized factors in the microenvironment absentin cultured cells, or could reflect the longer treatmentduration tumors were exposed to in vivo than in culture,potentially increasing cell death and reducing in vivo BNIP3expression. Tumors derived from cells transduced to expressshRNA targeting essential autophagy gene ATG7 exhibitedslightly increased BNIP3 expression, consistent with a priorreport in which genetic disruption of ATG7 eliminatedautophagy but led to a slight increase in BNIP3 expressionthat could not trigger autophagy in the setting of ATG7 loss(25).
Our findings are significant because we show that targetingautophagy through pharmacologic or genetic means disruptsantiangiogenic therapy resistance in vivo. While some of theseobservations were made in ectopic subcutaneous tumors,because of our findings of the importance of hypoxia inresistance to antiangiogenic therapy and reports that ortho-topic murine intracranial tumors exhibit less hypoxia thanectopic subcutaneous tumors and that the hypoxia of the lattermore closely resembles human glioblastoma (43, 44), ourfindings in subcutaneous tumors should be pertinent toglioblastoma.
Chloroquine, a clinically approved antimalaria drug, hasbeen studied in a randomized glioblastoma trial combiningchloroquine with conventional treatment with a benefit notquite significant (45). Currently more than 20 phase I/IIcancer clinical trials involving chloroquine or hydroxylchlor-oquine are open nationwide (24). Furthermore, while chlo-roquine plus antiangiogenic therapy in our xenografts wasnot curative, chloroquine exerts numerous nonspecificeffects, incompletely disrupts autophagy, and achieves max-imal plasma concentration (46) 10-fold lower than the con-centrations inhibiting hypoxia-induced autophagy in vitro.Thus, our finding that genetic disruption of essential autop-hagy gene ATG7 dramatically increased response to anti-angiogenic therapy from no response to curative, suggeststhat long-term evaluation of autophagy inhibitors in treatingantiangiogenic therapy resistance will require more specificand potent autophagy inhibitors currently being developed(24).
Disclosure of Potential Conflicts of InterestA. Jahangiri is a Howard Hughes Medical Institute Fellow. No potential
conflicts of interest were disclosed by the other authors.
Grant SupportThe work was supported by funding toMKA from the American Brain Tumor
Association, the James S. McDonnell Foundation, the NIH (5K02NS64167-2), andthe UCSFBrain Tumor SPORE. A. Jahangiri is aHowardHughesMedical InstituteResearch Fellow.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicate thisfact.
Received November 22, 2011; revised January 25, 2012; accepted February 14,2012; published OnlineFirst March 23, 2012.
Hu et al.
Cancer Res; 72(7) April 1, 2012 Cancer Research1782
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

References1. Jain RK. Lessons from multidisciplinary translational trials on anti-
angiogenic therapy of cancer. Nat Rev Cancer 2008;8:309–16.2. Vredenburgh JJ, Desjardins A, Herndon JE II, Dowell JM, Reardon DA,
Quinn JA, et al. Phase II trial of bevacizumab and irinotecan in recurrentmalignant glioma. Clin Cancer Res 2007;13:1253–9.
3. Clark AJ, Lamborn KR, Butowski NA, Chang SM, Prados MD, ClarkeJL, et al. Neurosurgical management and prognosis of patients withglioblastoma that progress during bevacizumab treatment. Neurosur-gery 2012;70:361–70.
4. Mazure NM, Pouyssegur J. Hypoxia-induced autophagy: cell death orcell survival? Curr Opin Cell Biol 2010;22:177–80.
5. TracyK, Dibling BC, Spike BT, Knabb JR, Schumacker P,Macleod KF.BNIP3 is an RB/E2F target gene required for hypoxia-induced autop-hagy. Mol Cell Biol 2007;27:6229–42.
6. Xie Z, Klionsky DJ. Autophagosome formation: core machinery andadaptations. Nat Cell Biol 2007;9:1102–9.
7. Boya P, Gonzalez-Polo RA, Casares N, Perfettini JL, Dessen P,Larochette N, et al. Inhibition of macroautophagy triggers apoptosis.Mol Cell Biol 2005;25:1025–40.
8. Lum JJ, Bauer DE, Kong M, Harris MH, Li C, Lindsten T, et al. Growthfactor regulation of autophagy and cell survival in the absence ofapoptosis. Cell 2005;120:237–48.
9. Sato K, Tsuchihara K, Fujii S, Sugiyama M, Goya T, Atomi Y, et al.Autophagy is activated in colorectal cancer cells and contributes to thetolerance to nutrient deprivation. Cancer Res 2007;67:9677–84.
10. Geng J, Klionsky DJ. The Atg8 and Atg12 ubiquitin-like conjugationsystems inmacroautophagy. 'Protein modifications: beyond the usualsuspects' review series. EMBO Rep 2008;9:859–64.
11. Kirkin V, McEwan DG, Novak I, Dikic I. A role for ubiquitin in selectiveautophagy. Mol Cell 2009;34:259–69.
12. Norden AD, YoungGS, Setayesh K, Muzikansky A, Klufas R, Ross GL,et al. Bevacizumab for recurrent malignant gliomas: efficacy, toxicity,and patterns of recurrence. Neurology 2008;70:779–87.
13. Paez-RibesM,Allen E,Hudock J, Takeda T,OkuyamaH, Vinals F, et al.Antiangiogenic therapy elicits malignant progression of tumors toincreased local invasion and distant metastasis. Cancer Cell 2009;15:220–31.
14. Wykoff CC, Beasley NJ, Watson PH, Turner KJ, Pastorek J, Sibtain A,et al. Hypoxia-inducible expression of tumor-associated carbonicanhydrases. Cancer Res 2000;60:7075–83.
15. Kamiyama H, Takano S, Tsuboi K, Matsumura A. Anti-angiogeniceffects of SN38 (active metabolite of irinotecan): inhibition of hypox-ia-inducible factor 1 alpha (HIF-1alpha)/vascular endothelial growthfactor (VEGF) expression of glioma and growth of endothelial cells.J Cancer Res Clin Oncol 2005;131:205–13.
16. Eng CH, Yu K, Lucas J, White E, Abraham RT. Ammonia derived fromglutaminolysis is a diffusible regulator of autophagy. Sci Signal 2010;3:ra31.
17. Rzymski T, Milani M, Pike L, Buffa F, Mellor HR, Winchester L, et al.Regulation of autophagy by ATF4 in response to severe hypoxia.Oncogene; 29:4424–35.
18. Pursiheimo JP, Rantanen K, Heikkinen PT, Johansen T, Jaakkola PM.Hypoxia-activated autophagy accelerates degradation of SQSTM1/p62. Oncogene 2009;28:334–44.
19. Mizushima N, Yoshimori T. How to interpret LC3 immunoblotting.Autophagy 2007;3:542–5.
20. Satoo K, Noda NN, Kumeta H, Fujioka Y, Mizushima N, Ohsumi Y, et al.The structure of Atg4B-LC3 complex reveals themechanismof LC3 pro-cessing and delipidation during autophagy. EMBO J 2009;28:1341–50.
21. Yeo EJ, Chun YS, Cho YS, Kim J, Lee JC, Kim MS, et al. YC-1: apotential anticancer drug targeting hypoxia-inducible factor 1. J NatlCancer Inst 2003;95:516–25.
22. Mizushima N, Yoshimori T, Levine B. Methods in mammalian autop-hagy research. Cell 2010;140:313–26.
23. Yang S,Wang X, Contino G, LiesaM, Sahin E, Ying H, et al. Pancreaticcancers require autophagy for tumor growth. Genes Dev 2011;25:717–29.
24. Amaravadi RK, Lippincott-Schwartz J, Yin XM, Weiss WA, TakebeN, Timmer W, et al. Principles and current strategies for
targeting autophagy for cancer treatment. Clin Cancer Res 2011;17:654–66.
25. Masiero E, Agatea L, Mammucari C, Blaauw B, Loro E, Komatsu M,et al. Autophagy is required to maintain muscle mass. Cell Metab2009;10:507–15.
26. Giatromanolaki A, Koukourakis MI, Sowter HM, Sivridis E, Gibson S,Gatter KC, et al. BNIP3 expression is linked with hypoxia-regulatedprotein expression and with poor prognosis in non-small cell lungcancer. Clin Cancer Res 2004;10:5566–71.
27. GiatromanolakiA,KoukourakisMI,GatterKC,HarrisAL,SivridisE.BNIP3expression in endometrial cancer relates to active hypoxia induciblefactor 1alpha pathway and prognosis. J Clin Pathol 2008;61:217–20.
28. Kanzawa T, Germano IM, Komata T, Ito H, Kondo Y, Kondo S. Role ofautophagy in temozolomide-induced cytotoxicity formalignant gliomacells. Cell Death Differ 2004;11:448–57.
29. Apel A,Herr I, SchwarzH,RodemannHP,Mayer A.Blocked autophagysensitizes resistant carcinoma cells to radiation therapy. Cancer Res2008;68:1485–94.
30. Amaravadi RK, ThompsonCB. The roles of therapy-induced autophagyand necrosis in cancer treatment. Clin Cancer Res 2007;13:7271–9.
31. Carew JS, Nawrocki ST, Kahue CN, Zhang H, Yang C, Chung L, et al.Targeting autophagy augments the anticancer activity of the histonedeacetylase inhibitor SAHA to overcomeBcr-Abl-mediateddrug resis-tance. Blood 2007;110:313–22.
32. Bergers G, Hanahan D. Modes of resistance to anti-angiogenic ther-apy. Nat Rev Cancer 2008;8:592–603.
33. Winkler F, Kozin SV, Tong RT, Chae SS, Booth MF, Garkavtsev I, et al.Kinetics of vascular normalization by VEGFR2 blockade governs braintumor response to radiation: role of oxygenation, angiopoietin-1, andmatrix metalloproteinases. Cancer Cell 2004;6:553–63.
34. Keunen O, Johansson M, Oudin A, Sanzey M, Abdul Rahim SA, Fack F,etal.Anti-VEGFtreatment reducesbloodsupplyand increases tumorcellinvasion in glioblastoma. Proc Natl Acad Sci U S A 2011;108:3749–54.
35. Pouyssegur J, Dayan F, Mazure NM. Hypoxia signalling in cancer andapproaches to enforce tumour regression. Nature 2006;441:437–43.
36. Sowter HM, Ratcliffe PJ, Watson P, Greenberg AH, Harris AL. HIF-1-dependent regulation of hypoxic induction of the cell death factorsBNIP3 and NIX in human tumors. Cancer Res 2001;61:6669–73.
37. Brown JM,WilsonWR. Exploiting tumour hypoxia in cancer treatment.Nat Rev Cancer 2004;4:437–47.
38. Li Y, Wang Y, Kim E, Beemiller P, Wang CY, Swanson J, et al. Bnip3mediates the hypoxia-induced inhibition on mammalian target ofrapamycin by interacting with Rheb. J Biol Chem 2007;282:35803–13.
39. Bernardi R,Guernah I, JinD,Grisendi S, Alimonti A, Teruya-Feldstein J,et al. PML inhibits HIF-1alpha translation and neoangiogenesisthrough repression of mTOR. Nature 2006;442:779–85.
40. GwinnDM,ShackelfordDB,EganDF,MihaylovaMM,MeryA,VasquezDS, et al. AMPK phosphorylation of raptor mediates a metaboliccheckpoint. Mol Cell 2008;30:214–26.
41. Jung CH, Jun CB, Ro SH, Kim YM, Otto NM, Cao J, et al. ULK-Atg13-FIP200 complexesmediatemTOR signaling to the autophagymachin-ery. Mol Biol Cell 2009;20:1992–2003.
42. Bellot G, Garcia-Medina R, Gounon P, Chiche J, Roux D, PouyssegurJ, et al. Hypoxia-induced autophagy is mediated through hypoxia-inducible factor induction of BNIP3 andBNIP3L via their BH3domains.Mol Cell Biol 2009;29:2570–81.
43. AghiM,CohenKS, KleinRJ, ScaddenDT,Chiocca EA. Tumor stromal-derived factor-1 recruits vascular progenitors to mitotic neovascula-ture, where microenvironment influences their differentiated pheno-types. Cancer Res 2006;66:9054–64.
44. Blouw B, Song H, Tihan T, Bosze J, Ferrara N, Gerber HP, et al. Thehypoxic response of tumors is dependent on their microenvironment.Cancer Cell 2003;4:133–46.
45. Sotelo J, Briceno E, Lopez-Gonzalez MA. Adding chloroquine to con-ventional treatment for glioblastomamultiforme: a randomized, double-blind, placebo-controlled trial. Ann Intern Med 2006;144:337–43.
46. Augustijns P, Geusens P, Verbeke N. Chloroquine levels in bloodduring chronic treatment of patients with rheumatoid arthritis. Eur JClin Pharmacol 1992;42:429–33.
Autophagy Mediates Resistance to Antiangiogenic Therapy
www.aacrjournals.org Cancer Res; 72(7) April 1, 2012 1783
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831

2012;72:1773-1783. Published OnlineFirst March 23, 2012.Cancer Res Yu-Long Hu, Michael DeLay, Arman Jahangiri, et al. Adaptation to Antiangiogenic Treatment in GlioblastomaHypoxia-Induced Autophagy Promotes Tumor Cell Survival and
Updated version
10.1158/0008-5472.CAN-11-3831doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2012/02/21/0008-5472.CAN-11-3831.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/72/7/1773.full#ref-list-1
This article cites 45 articles, 20 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/72/7/1773.full#related-urls
This article has been cited by 33 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/72/7/1773To request permission to re-use all or part of this article, use this link
on March 16, 2021. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 23, 2012; DOI: 10.1158/0008-5472.CAN-11-3831