Chairperson: Dr. Satya Ranjan Sutradhar FCPS (Medicine), MD (Endocrinology)

Hypothyroidism
Ally P. H. PrebtaniProfessor of Medicine
Internal Medicine, Endocrinology & MetabolismMcMaster University

Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
by any means – graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of
Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s statements, materials, acts or omissions.
2

Case
• 55yo woman
• Feeling well, otherwise healthy
• Mother with Grave’s disease
• No meds
• Exam normal except irregular thyroid gland
• TSH 11, Free T4 normal
• 6 months later TSH 20, Free T4 8

One year later
• More tired, cold, constipated, weight gain
• On l-thyroxine 250mcg daily
• On exam
– Looks tired, BP 140/92 P 62
– Thyroid irregular
– Periorbital puffiness
– DTR delayed
• TSH 35, Free T4 6

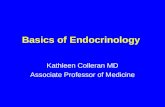
Thyroid Axis
UpToDate 2006
T3 > potency vs T4
•80% from gland
•20% from 5’ DI enzyme conversion


Definition
• Subclinical– TSH above the upper limit normal
– Normal T4
– 0.45-4.12mIU/L• ? 0.5-2.5mIU/L
– Few or no Sx
• Overt– High TSH
– Low T4

DDx High TSH
• Recovery from illness– Sick Euthyroid
• Central Hyperthyroidism– Free T4 high
• Thyroiditis recovery– Transient
• rhTSH (Thyrogen)• Assay variability• 10 Adrenal Insufficiency
– Untreated• Heterophilic/interfering antibodies
– Murine, RF, anti-TSH • Thyroid hormone resistance

Epidemiology
• 4.0-8.5% U.S.A. Subclinical• 0.3% Overt• Higher Risk
– Age– Women 60yo– Thyroid disease Hx– DM-1/Other Autoimmune– Turner’s/Kleinfelter’s Syndromes– Family History– XRT H&N– On l-thyroxine– + TPO Ab

Prevalence
J Clin Endocrinol Metab 2001 Oct;86(10):4585-90


Delayed DTRs

Zimmermann et al. Lancet Vol 372 Oct 4, 2008

Zimmermann et al. Lancet Vol 372 Oct 4, 2008


Dx & Screening• TSH is best screening test for primary
– Outpatient, stable
– Not central, NO recent hyperT4 Tx
– Use uln of reference laboratory
• Free T4
– if abnormal TSH
– Suspect central hypothyroidism (TSH useless!!)• 99.97% protein bound
• Esp TBG
– Affected by drugs, diseases, pregnancy
• Free T4 inaccurate in pregnancy
– Low
– Thus use Total T4
• Collect T4 before l-T4 dosing
• T3 quite useless in hypothyroid assessment

Garber et al. Endocrine Practice Vol 18 No. 6


TPO Ab
• Subclinical hypothyroidism
• Nodular thyroid disease
• Recurrent miscarriage/infertility

Screening
N Engl J Med 2001 Jul 26;345(4):260-5

Screening
• Controversial– High risk
• Symptoms
• ? > 60yo
• Goitre/nodules
• ? All pregnant
• Hx thyroid disease
• DM-1/Autoimmune Disease
• FH 1st degree relative
• XRT H&N, surgery
• On l-thyroxine, amio, Li, others…

Treatment
• TSH > 10• TSH 4.5-10 more controversial
– Trial for Sx if • ? Placebo effect
– Pregnant or planning (? TSH > 2.5)• Fetus needs in T-1• Neurocognitive effects
– Infertility– Goitre/nodules– ? TPO Ab
• Overt Hypothyroidism– Aim TSH low-normal

Goals of Tx• Improve Sx
– Not all Sx improvement with normal TSH
• ? Genetics dec T4 -> T3
• ? T4 transporter defect
– Acknowledge
– r/o other causes
– ? Psych
• Minimize complications– Lipids, CVD…
• Normalize TSH
– Consider Sx, comorbidities
– Higher targets for elderly
• Avoid over Tx (esp older, post-menopause, TSH < 0.1)– A.fib, osteoporosis

Symptoms
J Clin Endocrinol Metab 2001 Oct;86(10):4585-90

How to Tx
• L-thyroxine (Synthroid/Eltroxin)
– Standard, efficacy, safety, long term experience, cheap
– Once daily po
• Once weekly if adherance issue (since t ½ 7 days)
– 1.6mcg/kg od if young, healthy
– No dose issues with CKD or CLD
– higher doses Nephrotic syndrome
– 25-50mcg od to start– Older/CVD
– Subclinical

• Same preparation/brand if possible on repeats
• Empty stomach
– 60min ac breakfast or 4hrs pc
– 70-80% bioavailability on fasting
• Consistent timing, avoid drug interactions
• Adjust q4-6weeks & aim normal TSH
– Dose/brand change, drug interaction, pregnant, wt change…
– then q6-12mos
• NOT Dessicated, Extracts, T3/Cytomel, Nutracetical, Diet supps
• If suspect Adrenal Insufficiency (AI)– r/o 1st and treat 1st before l-thyroxine!!!

Allergic/Intolerant to l-T4
• Decrease dose
• Change product
• Change to compounded preparation
– No evidence improves bioavailablity
– Only if allergic to excipient
• Gelatin capsules

Pregnancy• Risks
– Maternal
• Abruptio/PPH
• Miscarriage
• HTN/Preeclampsia
– Fetal
• Preterm delivery
• LBW
• No fetal production of T4 till 2nd trimester– IQ/Brain development
– Motor
– Neuro-psych

Pregnancy
– > doses in pregnancy by 25-50% (increased TBG)
– 2 extra doses per week– At onset of pregnancy
– TSH– Check q4weeks 1st half of preg; then qtrimester
– T1 0.1-2.5
– T2 0.2-3.0
– T3 0.3-3.0
– 6 weeks after dose change
– Back to pre-pregnancy dose post-partum– TSH in 4-6 weeks

Refractory Hypothyroidismesp if > 2.5mcg/kg/d l-thyroxine
Ramadhan et al. CMAJ, February 7, 2012, 184(2)

Garber et al. Endocrine Practice Vol 18 No. 6

Interfering Substances
Ramadhan et al. CMAJ, February 7, 2012, 184(2)
• sertraline

Approach to Tx Resistant Hypothyroidism
Ramadhan et al. CMAJ, February 7, 2012, 184(2)

Therapeutic Endpoints
• Clinical
• TSH most important– Target controversial
– 0.45-4.12 if no reference range for lab
– ? < 2.5
– Pregnancy trimester specific
– FT4– Central hypothyroidism
– Avoiding over-Tx

Special Situations
• Infertility– Even normal TSH
– + TPO• L-T4 Tx
• Obese– No Tx if TSH normal
• Sx but n TSH (“Wilson’s Syndrome”)– No Tx
– Much overlap


Natural History of Subclinical
• 2-5%/year progress to Overt Hypothyroidism (decreased Free T4)
• > if antibodies– TPO
– Thyroglobulin
• > if TSH higher– > 10mIU/L
• 5% return to normal in 1 year


What if Subclinical untreated?
• Controversial– Cardiac
– Lipids
– Symptoms
– Neuropsych
– Overt Hypothyroidism
• > if higher TSH
• But does Tx make a difference ??

Subclinical Evaluation
• Repeat in 3 months
• Assess Risk factors
– For overt hypothyroidism
• TPO Antibody testing
• Monitor q6-12 months

Pros of TreatmentSubclinical
1. May relieve symptoms
2. May decrease cardiac disease, lipids
3. May decrease neuro-psych Sx
4. Prevent overt hypothyroidism

Cons of TreatmentSubclinical
Thyrotoxicosis
– 14-21% subclinical
• A. Fib
• Osteoporosis
• Neuro-psych Sx

ApproachSubclinical
Elevated TSH
Repeat TSH Elevated
n Free T4
Pregnant Goitre/Nodules
Symptoms Already on l-Thyroxine
Ovulatory Dysfunction
? Antibodies ? Lipids
Yes No
l-Thyroxine Monitor q6-12 months

When to refer to Endo?
• Children & infants
• Refractory to Tx
• Woman planning conception
• Cardiac disease
• Abnormal thyroid gland
• Adrenal/pituitary disease
• Confusing thyroid tests
• Medications affecting thyroid status

Question # 1
What are some indications to treat subclinical Hypothyroidism which is persistent?
1. All with TSH 5-10
2. If pregnant and TSH > 10
3. Especially in elderly with TSH 5-10
4. Dyslipidemia

Question # 2
What is not a cause of a persistently elevated TSH?
1.Non adherence
2.Inadequate dosing
3.1º hyperthyroidism
4.Central hyperthyroidism

Case
• 55yo woman
• Feeling well, otherwise healthy
• Mother with Grave’s disease
• No meds
• Physical Exam normal except irregular thyroid gland
• TSH 11, Free T4 normal
• 6 months later TSH 20, Free T4 8

One year later
• More tired, cold, constipated, weight gain
• On l-thyroxine 250mcg daily
• On exam
– Looks tired, BP 140/92 P 62
– Thyroid irregular
– Periorbital puffiness
– DTR delayed
• TSH 35, Free T4 6

Summary
• Common
• Screening controversial
• Risk factors
• TSH best screening test
• Evidence not great for subclinical state
• Treatment best with levothyroxine
• Target to reference range TSH
• For pregnancy trimester specific