Hyponatremia booklet slides · • Discuss the clinical consequences of undertreatment of...
14
A Patient-Centric, Process of Care Guide Empowering Pharmacists to Improve Management of Hyponatremia Learning Objectives • Discuss the clinical consequences of undertreatment of hyponatremia, including clinical manifestation, related comorbidities and clinical and resource burden • Describe the pathophysiology of hyponatremia, including euvolemic hyponatremia in SIADH and hypervolemic hyponatremia in heart failure • Classify patients with hyponatremia based on clinical presentation and comorbidities and recommend appropriate correction therapy • Outline current recommendations and guidelines for the treatment of hyponatremia • Summarize the pathophysiology of disease and related mechanisms- of-action, efficacy and safety/tolerability evidence for hyponatremia pharmacotherapies • Identify and commit to three or more practice improvements pharmacists can make to improve the process of care for hyponatremia Renal Losses Diuretic excess Mineral corticoid deficiency Salt-losing deficiency Bicarbonaturia with renal tubal acidosis and metabolic alkalosis Ketonuria Osmotic diuresis Extrarenal Losses Vomiting Diarrhea Third spacing of fluids Burns Pancreatitis Trauma Glucocorticoid deficiency Hypothyroidism SIADH secretion Drug-induced stress Acute or chronic renal failure Nephrotic syndrome Cirrhosis Cardiac failure Diagnostic Algorithm for Hyponatremia SIADH = syndrome of inappropriate antidiuretic hormone. Adapted from Kumar S, Beri T. Diseases of water metabolism. In: Berl T, Bonventre JV, eds. Atlas of Diseases of the Kidney. Vol. 1. Philadelphia, PA: Current Medicine, Inc; 1999:1.1-1.22. Legend: ↑ increase; ↑ ↑ greater increase; ↓ decrease; ↓ ↓ greater decrease; ↔ no change Assessment of volume status Hypovolemia Total body water ↓ Total body Na+ ↓ ↓ Euvolemia (no edema) Total body water ↑ Total body Na+ ↔ Hypervolemia Total body water ↑ ↑ Total body Na+ ↑ U[Na+] >20 mEq/L U[Na+] <20 mEq/L U[Na+] >20 mEq/L U[Na+] >20 mEq/L U[Na+] <20 mEq/L
-
Upload
vuongkhanh -
Category
Documents
-
view
219 -
download
1
Transcript of Hyponatremia booklet slides · • Discuss the clinical consequences of undertreatment of...

A Patient-Centric, Process of Care Guide
Empowering Pharmacists toImprove Management of
Hyponatremia
Learning Objectives
• Discuss the clinical consequences of undertreatment of hyponatremia, including clinical manifestation, related comorbidities and clinical and resource burden
• Describe the pathophysiology of hyponatremia, including euvolemichyponatremia in SIADH and hypervolemic hyponatremia in heart failure
• Classify patients with hyponatremia based on clinical presentation and comorbidities and recommend appropriate correction therapy
• Outline current recommendations and guidelines for the treatment of hyponatremia
• Summarize the pathophysiology of disease and related mechanisms-of-action, efficacy and safety/tolerability evidence for hyponatremia pharmacotherapies
• Identify and commit to three or more practice improvements pharmacists can make to improve the process of care for hyponatremia
Renal Losses
Diuretic excess
Mineral corticoid deficiency
Salt-losing deficiency
Bicarbonaturia with renal tubal acidosis
and metabolic alkalosis
Ketonuria
Osmotic diuresis
Extrarenal Losses
Vomiting
Diarrhea
Third spacing of fluids
Burns
Pancreatitis
Trauma
Glucocorticoid deficiency
Hypothyroidism
SIADH secretion
Drug-induced stress
Acute or chronicrenal failure
Nephrotic syndrome
Cirrhosis
Cardiac failure
Diagnostic Algorithm for Hyponatremia
SIADH = syndrome of inappropriate antidiuretic hormone. Adapted from Kumar S, Beri T. Diseases of water metabolism. In: Berl T, Bonventre JV, eds. Atlas of Diseases
of the Kidney. Vol. 1. Philadelphia, PA: Current Medicine, Inc; 1999:1.1-1.22.
Legend: ↑ increase; ↑ ↑ greater increase; ↓ decrease; ↓ ↓ greater decrease; ↔ no change
Assessment of volume status
Hypovolemia
Total body water ↓
Total body Na+ ↓ ↓
Euvolemia (no edema)
Total body water ↑
Total body Na+ ↔
Hypervolemia
Total body water ↑ ↑
Total body Na+ ↑
U[Na+] >20 mEq/L U[Na+] <20 mEq/L U[Na+] >20 mEq/L U[Na+] >20 mEq/L U[Na+] <20 mEq/L
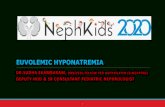
AVP Release and Sites of Action
Anxiety and stress (V1)
Myocyte hypertrophy (V1)
Blood:Platelet aggregation (V1)
Von Willebrand factor (V2)
Body fluid:Water retention (V2)
Vascular tone:Vasoconstriction (V1)
Vasodilation (V2)
Glycogenolysis (V1)
Posterior pituitaryAVP release
AVP = arginine vasopressin.Adapted from Ferguson JW, et al. Clin Sci (Lond). 2003;105(1):1-8.
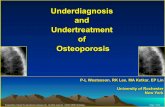
AVP Regulation of Water Reabsorption from Renal Tubular Cells
AQP = aquaporin; GTP = guanine nucleotide binding protein; ATP = adenosine triphosphate; cAMP = cyclic adenosine monophosphate; PKA = protein kinase A.Mayinger B, et al. Exp Clin Endocrinol Diabetes. 1999;107(3):157-165.
Co
llecting
du
ctAVPAVP V2
receptor
Basolateral membrane
Luminal membrane
H2O
H2OAQP2
Exocytic insertioncAMP
ATP
PKA
Recyclingvesicle
AQP2
Endocytic retrieval
GTP(Gs)
Vas
a re
cta Collecting Duct CellAQP3
AQP4
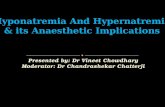
Risk Stratification
• First Decision: Presentation Acute vs. Chronic?
– How aggressive?
– How fast?
• Second Decision: Duration of hyponatremia
– Acute = less than 48 hours in duration
• Concerned about neurologic sequellae
– Osmotic differential between brain and blood
– Brain swelling
– Chronic = greater than 48 hours in duration
• Symptoms may be more modest
– Brain has time to adapt

LEVEL 1 - NO OR MINIMAL SYMPTOMS: headache, irritability, inability to concentrate, altered mood, depression
LEVEL 2 - MODERATE SYMPTOMS: nausea, confusion, disorientation, altered mental status
LEVEL 3 - SEVERE SYMPTOMS:vomiting, seizures, obtundation,respiratory distress, coma
Hyponatremia Treatment Options
Fluid restrictionConsider vasopressin antagonist or hypertonic saline if…•Unable to tolerate fluid restriction or failure of fluid restriction
•Need for rapid correction of Na+
Vasopressin Antagonist or Hypertonic Saline***
Hypertonic Saline
***Vasopressin antagonists may be preferred if volume overloaded
Traditional Pharmacological Treatment Strategies
• Text
Footnotes and references. This refuses to adhere to a template. Copy and paste this text box into whatever slides need it, and replace the text.
Traditional Pharmacological Treatment Strategies

Hyponatremia: Practical Approach on the Use of Hypertonic Saline
Comparison of Sodium Chloride Injection
Drug Facts and Comparisons 2013. St. Louis, MO: Wolters Kluwer Health; 2011.
Rate of Sodium Correction
• Initial rate of sodium correction not to exceed 1-2 mEq/L/hr
• High risk of Osmotic Demyelination Syndrome (ODS) do not exceed 8 mEq/L in 24 hours
– Hypokalemia, alcoholism, malnutrition,advanced liver disease or serum sodium < 105mEq/L
• Normal risk of ODS rate of sodium correction should be limited to < 12 mEq / L /24 hr or 18 mEq/L in 1st 48 hr
Verbalis JG et al. Amer J Med 2013;126, S1-S42. Laureno R et al. Ann Intern Med 1997;126:57- 62. Cawley MJ. Ann Pharmacotherapy 2007;41:840 - 50

Calculation of Sodium Requirement:
Adrogué-Madias EquationChange in serum sodium = infusate Na – serum Na
TBW + 1
Infusate Na = sodium concentration of infusate
0.9% (154mEq/L); 3% (513mEq/L)
Serum Na = patient’s serum sodium concentration
TBW = total body water = weight x correction factor
(Correction factor of 0.6 L/kg men, 0.45 L/kg women)
1 = 1 liter of solution
Adrogue HJ et al. N Engl J Med 2000;342:1581-9
Calculation Example
70-kg unresponsive male, serum sodium 110 mEq/L
•If 1 L of 3% sodium chloride injection is administered how much of a change in serum sodium will occur?
– Infusate Na (3%) = 513 mEq/L– Patient’s serum Na = 110mEq/L– TBW = 0.6 L/kg x 70 kg
Change in serum sodium = infusate Na – serum NaTBW + 1
Change in serum sodium = 9.4 mEq/L
Calculation Continued
Estimated effect of 1 liter of 3% sodium chloride would be 9.4 mEq/L or 0.94 mEq per 100 mL
How do you administer the infusate?
•Calculate total volume to administer in 24 hr, given 12 mEq/L is max increase in serum Na in 24 hr
100 mL x 12 mEq/L = 1,277mL
0.94 mEq/L
•Calculate recommended rate of infusion
100 mL x 1.5 mEq/L/hr* = 160 mL/hr 1st 4 hr
0.94 mEq/L ~32 mL/hr for 20 hr
* Recommended rate of sodium correction for severe symptoms at normal risk for ODS
Calculation Continued
• Calculation of infusion rate
– Multiply body weight in kg by desired rate of increase in sodium in mEq/L/hr • (ex., 70kg patient, a 3% NaCl infusion at 70 ml/hr will
increase sodium ~1 mEq/L/hr, while infusing 35ml/hr will increase serum sodium ~0.5 mEq/L/hr)
– Monitor sodium levels frequently (q 4-6 hr)
Rate of Sodium Correction is more important thanthe infusion rate………..
Verbalis JG et al. The Amer J Med 2013;126:S1-S42. Ellison DH et al. N Engl J Med 2007;356:2064-2072
Hyponatremia Patient Case Study
Heart Failure
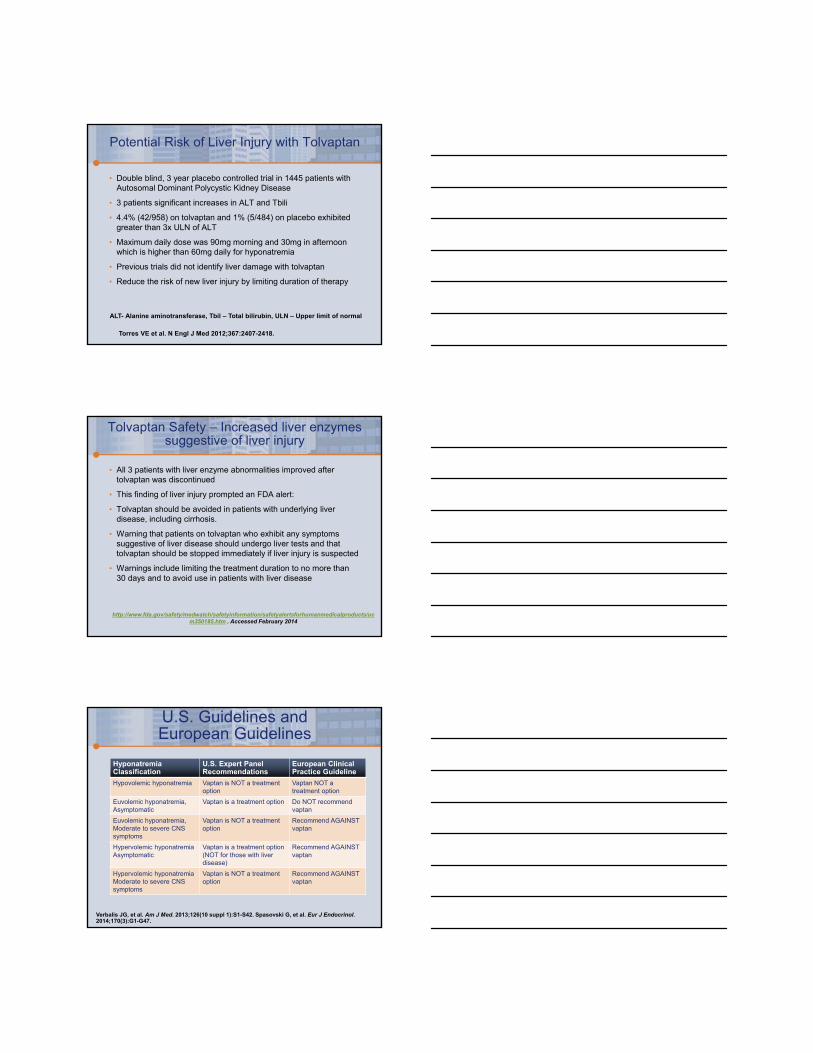
1. Gheorghiade et al. Eur Heart J. 2007;28:980-988. 2. Gheorghiade et al. Arch Intern Med. 2007;167:1998-2005. 3. Gheorghiade et al. JAMA. 2004;291(16):1963-1971. 4. Klein et al. Circulation. 2005;111:2451-2460.
P < .0001
P < .0001
In-Hospital Mortality (%)
Post-Discharge Mortality (%)
Death or RehospitalizationSince Discharge (%)
Admission Serum Sodium
[Na+] < 135 mEq/L
[Na+] ≥ 135 mEq/L
45
40
35
30
25
20
15
10
5
0
P < .0001
6.4 5.5
LOS (days)
P < .0001
6.03.2
7.1
12.4
34.8
42.5
Hyponatremia in Heart Failure
0.5 -
0.4 -
0.3 -
0.2 -
0.1 -
|0
|200
|400
|600
|800
|1000
|1200
|1400
|1600
|1800
Time (days)
Cu
mu
lati
ve P
rob
abili
tyo
f D
eath
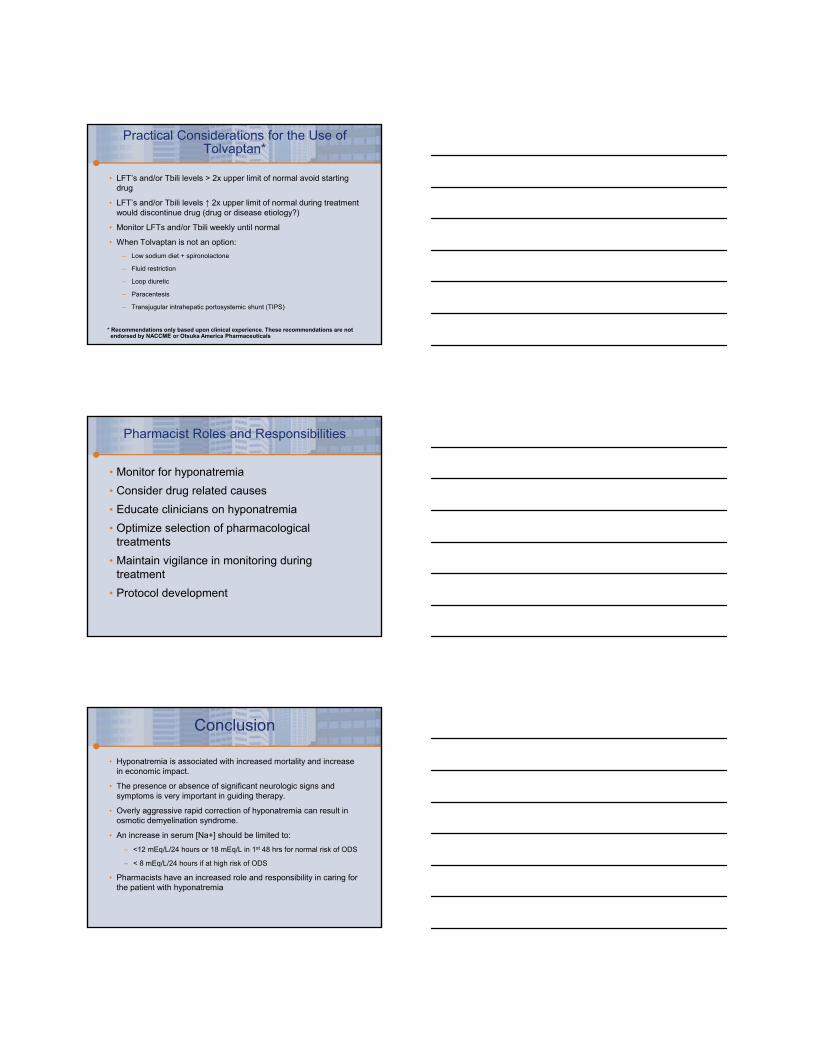
Sodium Level <136 mEq/L
Sodium Level ≥136 mEq/L
Log-rank P<.001
Number at RiskSodium Level 870 835 749 626 524 387 273 169 91 33
<136 mEq/LSodium Level 107 91 81 70 65 60 47 37 21 4
≥136 mEq/L
Survival in HF Decreased with Concomitant Hyponatremia*
*Survival rates were significantly reduced if patients with acute ST-elevation myocardial infarction had concomitant hyponatremia ([Na+] <135 mEq/L) on
admission (P<.0001). Adapted from Goldberg A, et al. Arch Intern Med. 2006;166(7):781-786.
Patient Chart Overview
• John is a 78-year-old, 75 kg hispanic male admitted to the CCU in acute decompensated heart failure. He has been extremely fatigued with SOB for several weeks prior to admission. After 6 days of treatment the patient is now receiving intravenous diuretics and vasodilator therapy and is now moved to a step down unit for medication stabilization prior to discharge.
• Medical history
– Ischemic cardiomyopathy (LVEF 23%)
– s/p AMI x 2 in 2007 and 2010
– HTN x 35 years
– Hyperlipidemia x 32 years
– Osteoporosis x 20 years
CCU = coronary care unit; LVEF = left ventricular ejection fraction
Patient Chart Overview
• Family history
– Unremarkable
• Social history
– Smokes 1.5 packs per day x 29 years (D/C 5 years)
– No alcohol use
• Physical assessment
– Vital signs: HR: 92 bpm, BP: 116/82 mm Hg, RR: 14 bpm, Temp: 38.9°C
– Weight: 81 kg (dry weight 77 Kg), Height: 157 cm
– Chest: Crackles bilateral bases
– Abdomen: Distended
– Skin: + 2 pitting edema in both arms and legs
– Neurologic
• Cranial nerves II-VIII grossly intact
• A&O x 3
HR = heart rate; BP = blood pressure; RR = respiratory rate; bpm = breaths per minute; A&O = alert and oriented.

Patient Chart Overview
• Laboratory (day 7 of admission)
– Serum sodium: 125 mEq/L
– Serum osmolality: 264 mOsm/kg
– Urine sodium: 18 mEq/L
– Urine osmolality: 255 mOsm/kg
– Serum creatinine: 1.2 mg/dL
• Intake/output (total over 7 days)
– 5360 mL/3200 mL (+ 2160 mL)
• Current medications
– Furosemide 40 mg IV every 8 hours
– Lisinopril 5 mg qday
– Carvedilol 6.25 mg BID
– Spironolactone 12.5 mg by mouth daily
Optimal Treatment Strategies
AGENT LIMITATIONS
Fluid restriction • Slow to correct over days (1-2 mEq/L/day)
• Poorly tolerated due to thirst
• Should not be used with high AVP level and urine osmolality
Diuretics • Allows relaxation of fluid restriction
• Potential for ototoxicity, volume depletion, and K+ and Mg+
depletion
Demeclocycline • Not FDA approved for hyponatremia
• Slow to correct over days
• Nephrotoxic in cirrhosis and heart failure
Oral Sodium Chloride
• Nausea and vomiting
• Rarely can give large enough dose to be effective
• No data
Optimal Treatment Strategies
AGENT LIMITATIONS
Isotonic saline • Ineffective in dilutional hyponatremia
• Should not be used in setting of edema
• No safety data
• Complex calculations
Hypertonic saline • No consensus regarding appropriate infusion rates
• Overcorrection can cause osmotic demyelination syndrome
• Should not be used in setting of edema
• No safety data
• Complex calculations

Optimal Treatment Strategies
AGENT OPTIONS
Standard Heart Failure Treatment Measures
• Consider Increase in ACEi dose
• Consider increase in Carvedilol dose
Vaptan Clinical Considerations
• Tolvaptan
– Indicated for clinically significant hypervolemic and euvolemic hyponatremia (serum sodium <125 mEq/L or less marked hyponatremia that is symptomatic and has resisted correction with fluid restriction), including patients with HF, cirrhosis, and SIADH
– Available in 15-mg and 30-mg tablets
– Dosing: 15 mg orally once daily. Dosing may be increased at intervals ≥24 hours to 30 mg once daily to a maximum of 60 mg once daily
– Should only be initiated and re-initiated in a hospital setting. Healthcare providers must review the FDA-approved medication guide with every patient
– Coadministration with potent CYP3A4 enzyme inhibitors (ketoconazole, itraconazole, indinavir) is contraindicated
Tolvaptan [package insert]. Rockville, MD: Otsuka America Pharmaceutical, Inc; 2009.
Vaptan Clinical Considerations
• Conivaptan
– Indicated for euvolemic/hypervolemic hyponatremia in hospitalized patients
– Administer IV via large veins due to infusion-site reactions (63% to 73%)
• Change infusion site every 24 h
– Hypervolemic hyponatremia associated with heart failure: Data are limited. Use other treatment options
– Dosing: 20 mg IV LD @ 30min followed by 20 mg as a continuous infusion @ 24 h
– Duration of infusion limited to 4 days
– Limited data on drug-drug compatibility
– Contraindicated with potent CYP3A4 enzyme inhibitors (ketoconazole, itraconazole, indinavir)
Conivaptan [package insert]. Northbrook, IL: Astellas Pharma US, Inc; 2010.

LEVEL 1 - NO OR MINIMAL SYMPTOMS: headache, irritability, inability to concentrate, altered mood, depression
LEVEL 2 - MODERATE SYMPTOMS: nausea, confusion, disorientation, altered mental status
LEVEL 3 - SEVERE SYMPTOMS:vomiting, seizures, obtundation,respiratory distress, coma
Hyponatremia Treatment Options
Fluid restrictionConsider vasopressin antagonist or hypertonic saline if…•Unable to tolerate fluid restriction or failure of fluid restriction
•Need for rapid correction of Na+
Vasopressin Antagonist or Hypertonic Saline***
Hypertonic Saline
***Vasopressin antagonists may be preferred if volume overloaded
Hyponatremia Patient Case Study
Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
Causes of Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
Upadhyay A et al. Sem Nephrol 2009;29:227-338

Recognition of SIADH
• Hyponatremia with low serum osmolality
• Excessive renal excretion of sodium
– (> 20mEq/L)
• Limited clinical evidence of volume depletion or overload
– Normal skin turgor and blood pressure (euvolemia)
• Normal renal, adrenal and thyroid function
Bartter FC, et al. Am J Med 1967;42:790-806
Patient Case
• Rebecca is a 67 year-old female who presents to the ED with her husband who states “ my wife has become more confused and forgetful over the past 12-24 hours”
• Medical History
– HTN x 16 years
– COPD x 10 years
– Osteoporosis x 11 years
– Depression diagnosed 4 weeks ago
Patient Case
• Family history– Unknown
• Social history(-) alcohol, (-) tobacco, (-) IVDA
• Physical assessment– Vital signs: HR: 84bpm, BP 128/82mmHg, RR: 12BPM, Temp: 98.6F – Weight: 61kg (admission weight), Height: 167cm– General
• Confused– Chest
• Clear A & P– Abdomen
• Unremarkable– Skin
• Unremarkable– Neurologic
• Cranial nerves II-VIII grossly intact• A & O x 1 (person)
HR= heart rate; BP = blood pressure; RR = respiratory rate; bpm = breaths per minute; A7O = alert and oriented

Patient Case
• Laboratory (admission)
– Serum sodium 112 mEq/L
– Serum osmolality 265 mOsm/kg
– Urine sodium 25 mEq/L
– Serum creatinine 1.1 mg/dL
• Current medications
– Tiotropium bromide 18 mcg capsule
• 2 inhalation of one capsule, once daily with HandiHaler device
– Cardizem 240mg by mouth daily x 8 yrs
– HCTZ 25 mg by mouth daily x 5 years
– Oscal 600mg by mouth twice daily x 10 years
– Venlafaxine 100mg by mouth daily x 30 days
Drug-Induced Hyponatremia (SIADH)
• Risk factors for the development of hyponatremia with SSRI’s:
– Older age
– Female gender
– Concomitant use of diuretics
– Lower body weight
– Lower baseline serum sodium level
• Hyponatremia develops within weeks of treatment and resolves after two weeks after therapy discontinued
• Treatment for severe hyponatremia includes hypertonic saline +/- loop diuretic
Jacob S, et al. Annals of Pharmacotherapy 2006;40:1618-1622.
Drug-Induced Hyponatremia (SIADH)
• Retrospective controlled study
• 199 elderly psychiatric inpatients (mean age 74.2 years)
• 74 prescribed SSRI or venlafaxine
• 10 of 14 patients on venlafaxine developed hyponatremia
• 39% of patients on an SSRI or venlafaxine had hyponatremia vs 10% of controls
• Elderly patients on SSRI or venlafaxine should have
• serum sodium levels checked before and after
• commencement of antidepressant therapy
Kirby D et al. Int Geriatr Psychiatry 2002;17:231-7.
Potential Risk of Liver Injury with Tolvaptan
• Double blind, 3 year placebo controlled trial in 1445 patients with Autosomal Dominant Polycystic Kidney Disease
• 3 patients significant increases in ALT and Tbili
• 4.4% (42/958) on tolvaptan and 1% (5/484) on placebo exhibited greater than 3x ULN of ALT
• Maximum daily dose was 90mg morning and 30mg in afternoon which is higher than 60mg daily for hyponatremia
• Previous trials did not identify liver damage with tolvaptan
• Reduce the risk of new liver injury by limiting duration of therapy
ALT- Alanine aminotransferase, Tbil – Total bilirubin, ULN – Upper limit of normal
Torres VE et al. N Engl J Med 2012;367:2407-2418.
Tolvaptan Safety – Increased liver enzymes suggestive of liver injury
• All 3 patients with liver enzyme abnormalities improved after tolvaptan was discontinued
• This finding of liver injury prompted an FDA alert:
• Tolvaptan should be avoided in patients with underlying liver disease, including cirrhosis.
• Warning that patients on tolvaptan who exhibit any symptoms suggestive of liver disease should undergo liver tests and that tolvaptan should be stopped immediately if liver injury is suspected
• Warnings include limiting the treatment duration to no more than 30 days and to avoid use in patients with liver disease
http://www.fda.gov/safety/medwatch/safetyinformation/safetyalertsforhumanmedicalproducts/ucm350185.htm . Accessed February 2014
U.S. Guidelines andEuropean Guidelines
Hyponatremia Classification
U.S. Expert Panel Recommendations
European Clinical Practice Guideline
Hypovolemic hyponatremia Vaptan is NOT a treatmentoption
Vaptan NOT a treatment option
Euvolemic hyponatremia,Asymptomatic
Vaptan is a treatment option Do NOT recommend vaptan
Euvolemic hyponatremia,Moderate to severe CNS symptoms
Vaptan is NOT a treatment option
Recommend AGAINST vaptan
Hypervolemic hyponatremiaAsymptomatic
Vaptan is a treatment option(NOT for those with liver disease)
Recommend AGAINST vaptan
Hypervolemic hyponatremiaModerate to severe CNS symptoms
Vaptan is NOT a treatment option
Recommend AGAINST vaptan
Verbalis JG, et al. Am J Med. 2013;126(10 suppl 1):S1-S42. Spasovski G, et al. Eur J Endocrinol. 2014;170(3):G1-G47.
Practical Considerations for the Use of Tolvaptan*
• LFT’s and/or Tbili levels > 2x upper limit of normal avoid starting drug
• LFT’s and/or Tbili levels ↑ 2x upper limit of normal during treatment would discontinue drug (drug or disease etiology?)
• Monitor LFTs and/or Tbili weekly until normal
• When Tolvaptan is not an option:
– Low sodium diet + spironolactone
– Fluid restriction
– Loop diuretic
– Paracentesis
– Transjugular intrahepatic portosystemic shunt (TIPS)
* Recommendations only based upon clinical experience. These recommendations are not endorsed by NACCME or Otsuka America Pharmaceuticals
Pharmacist Roles and Responsibilities
• Monitor for hyponatremia
• Consider drug related causes
• Educate clinicians on hyponatremia
• Optimize selection of pharmacological treatments
• Maintain vigilance in monitoring during treatment
• Protocol development
Conclusion
• Hyponatremia is associated with increased mortality and increase in economic impact.
• The presence or absence of significant neurologic signs and symptoms is very important in guiding therapy.
• Overly aggressive rapid correction of hyponatremia can result in osmotic demyelination syndrome.
• An increase in serum [Na+] should be limited to:
– <12 mEq/L/24 hours or 18 mEq/L in 1st 48 hrs for normal risk of ODS
– < 8 mEq/L/24 hours if at high risk of ODS
• Pharmacists have an increased role and responsibility in caring for the patient with hyponatremia