
Hypokalemia and Potassium Deficit (1) Concept (2) Causes and mechanism (3) Effect on the body (4)...
53
Hypokalemia and Potassium Deficit (1) Concept (2) Causes and mechanism (3) Effect on the body (4) Principle of treatment
-
Upload
sabrina-suzanna-manning -
Category
Documents
-
view
221 -
download
0
Transcript of Hypokalemia and Potassium Deficit (1) Concept (2) Causes and mechanism (3) Effect on the body (4)...
Hypokalemia and Potassium Deficit
(1) Concept (2) Causes and mechanism (3) Effect on the body (4) Principle of treatment
(1) Concept
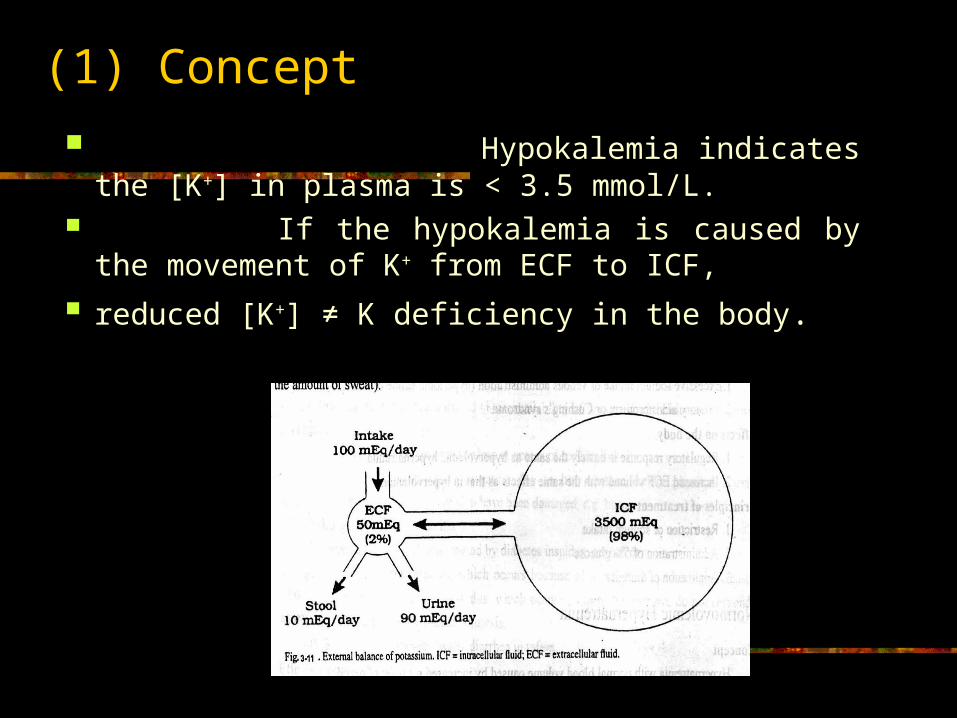
Hypokalemia indicates the [K+] in plasma is < 3.5 mmol/L.
If the hypokalemia is caused by the movement of K+ from ECF to ICF,
reduced [K+] ≠ K deficiency in the body.
(2) Causes and mechanism
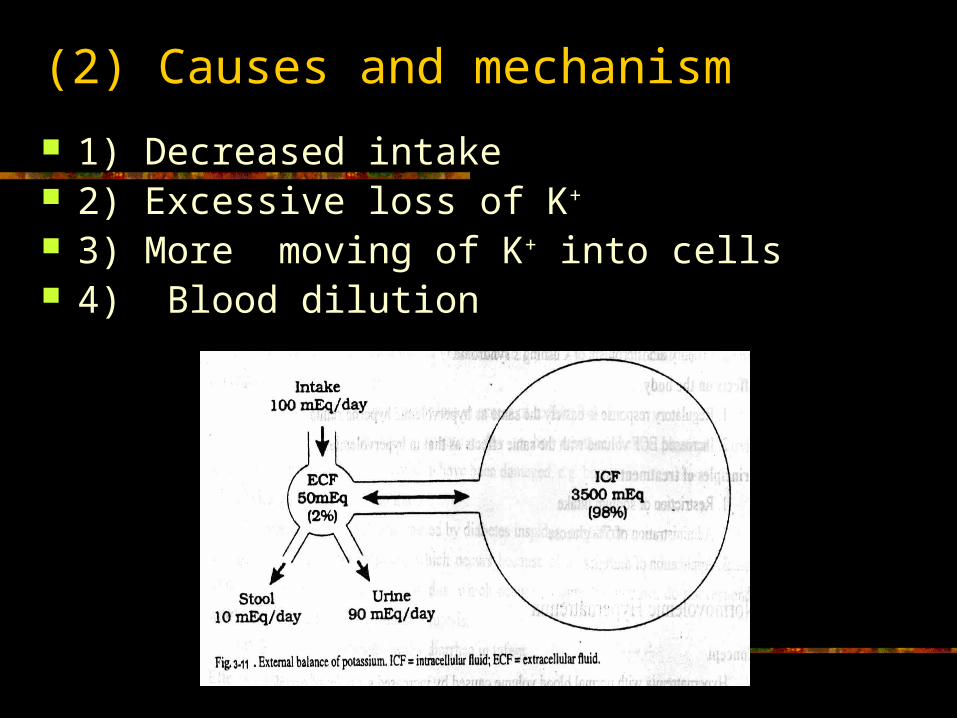
1) Decreased intake 2) Excessive loss of K+
3) More moving of K+ into cells 4) Blood dilution

1)Decreased intake Since food is the main source of potassium
in the body, fast, anorexia or inability to eat may cause hypokalemia.
At the same time, there is still loss of potassium from kidneys (5~10 mmol/ day at least).

Renal excretion of potassium continuously ----------------------------------------------------- amount of K+ excretion -----------------------------------------------------Normal 38~150 mmol/dayNo K intake 1~3 day 50 mmol/ day 4~7 day 20 mmol/ day 10 day 5~10 mml/ day------------------------------------------------------
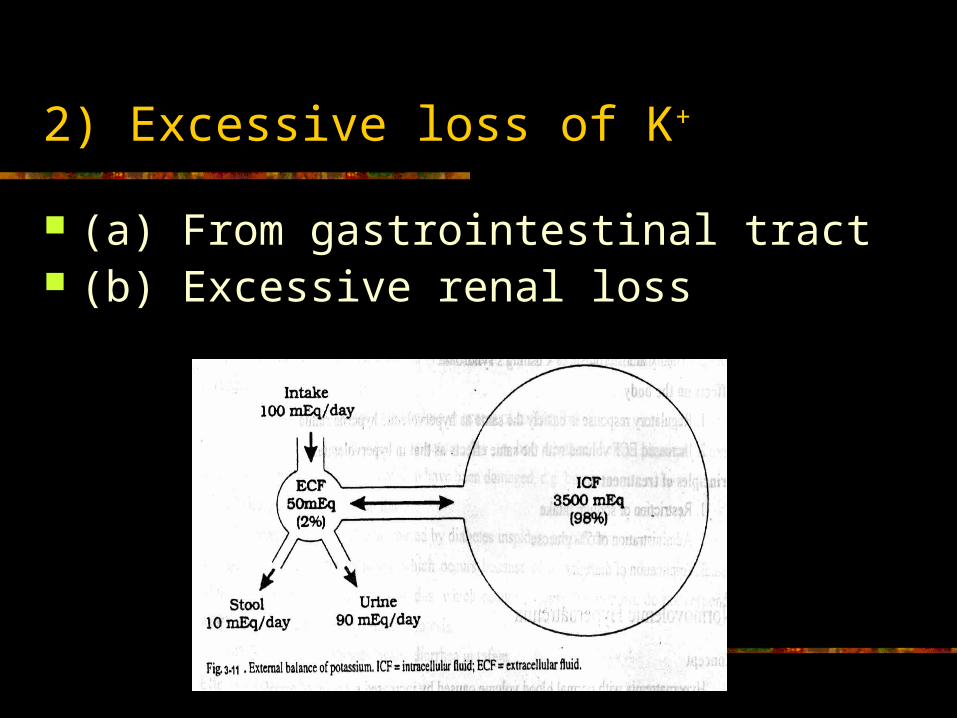
2) Excessive loss of K+
(a) From gastrointestinal tract (b) Excessive renal loss
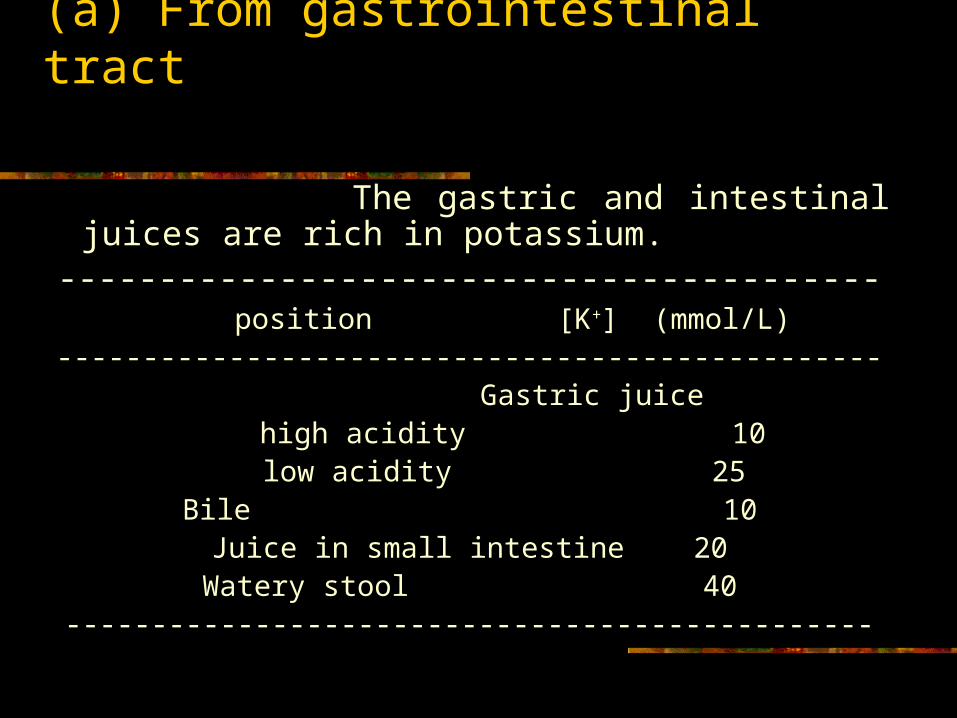
(a) From gastrointestinal tract
The gastric and intestinal juices are rich in potassium.
----------------------------------------- position [K+] (mmol/L)
------------------------------------------------ Gastric juice
high acidity 10 low acidity 25Bile 10
Juice in small intestine 20Watery stool 40
-----------------------------------------------

Persistent vomiting, diarrhea, gastric suction and fistula are the common ways to lose potassium directly.
At the same time hypovolemia may lead to increased secretion of aldosterone. Increased aldosterone (caused by hypovolemia) will enhance the loss of potassium from gastrointestinal tract like the renal tubules.
At the same time, loss of gastric juice may lead to metabolic alkalosis.
(b) Excessive renal loss
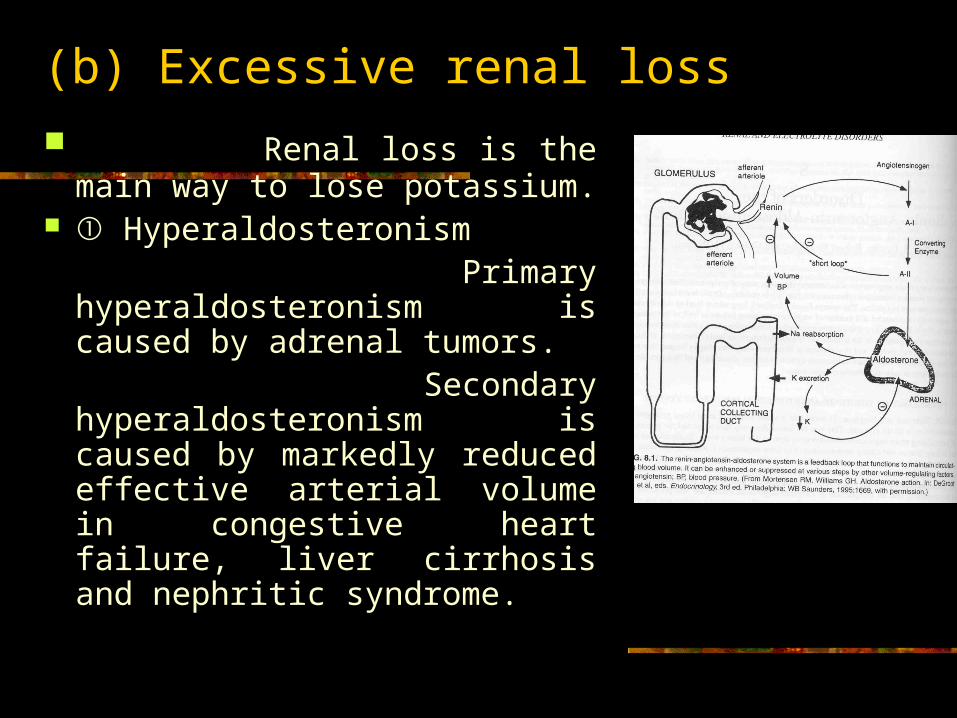
Renal loss is the main way to lose potassium.
① Hyperaldosteronism Primary hyperaldosteronism
is caused by adrenal tumors. Secondary hyperaldosteronism
is caused by markedly reduced effective arterial volume in congestive heart failure, liver cirrhosis and nephritic syndrome.
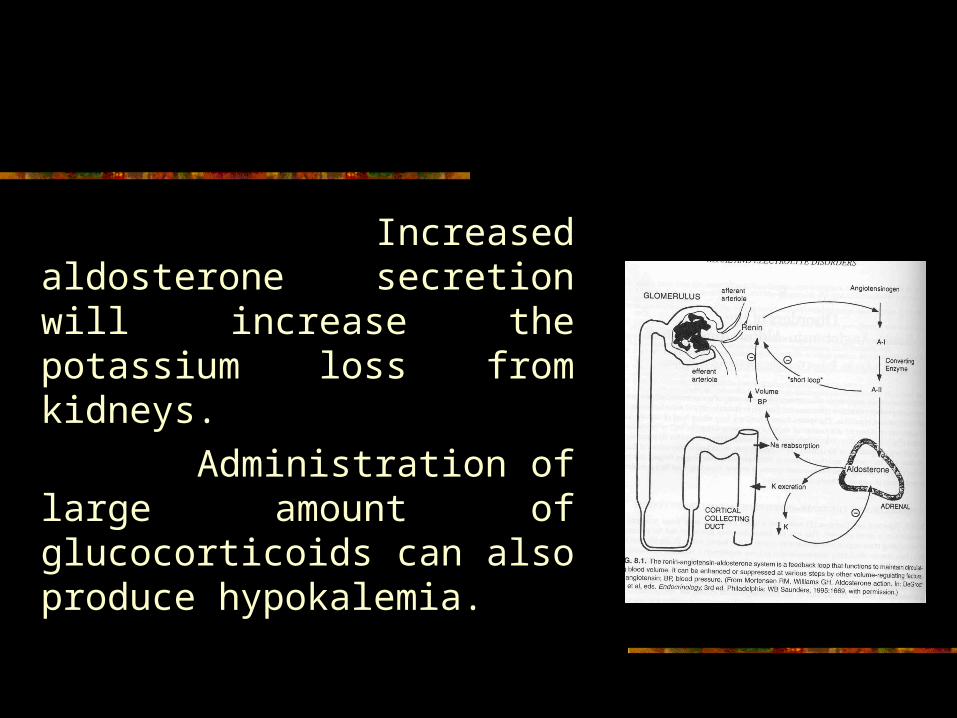
Increased aldosterone secretion will increase the potassium loss from kidneys.
Administration of large amount of glucocorticoids can also produce hypokalemia.

② Diuretics
The most common diuretics losing potassium are thiazines 噻嗪类 , furosemide 速尿 and ethacrynic acid 利尿酸 , which block the reabsorption of Na+ and Cl- in proximal tubule and Henle’s loop, then deliver more Na+ and Cl- to the distal tubules.
More K+ are exchanged with Na+ and the loss of potassium will increase.

Acetazolamide 乙酰唑胺 inhabits the activaty of CA in proximal tubule, H+-Na+ exchange decreases, More Na+ arrive at distal tubules, K+-Na+ exchange increases, K excretion increases.
All diuretics including increase osmotic diuretics mannitol 甘露醇 ,can increase the urine volume.
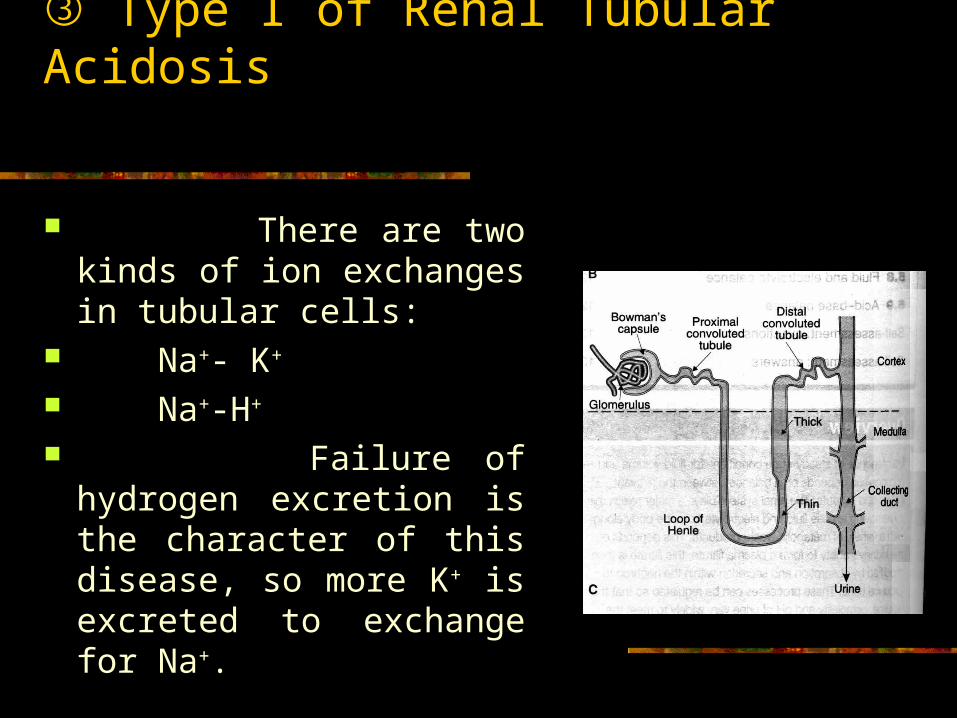
③ Type I of Renal Tubular Acidosis
There are two kinds of ion exchanges in tubular cells:
Na+- K+ Na+-H+
Failure of hydrogen excretion is the character of this disease, so more K+ is excreted to exchange for Na+.
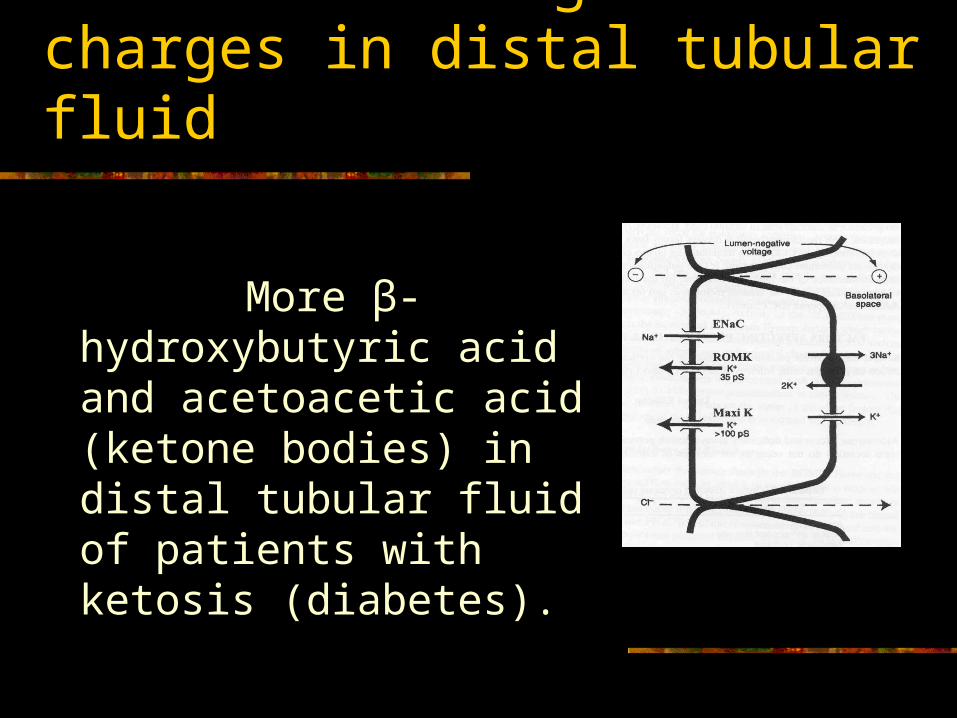
④ Increased negative charges in distal tubular fluid
More β-hydroxybutyric acid and acetoacetic acid (ketone bodies) in distal tubular fluid of patients with ketosis (diabetes).

3) More K+ moves into cell
(a) In alkalosis, H+ moves out of the cells, at the same time, K+ moves into the cells.
For each 0.1 unit increase of pH in ECF, the [K+] of serum decreases 0.7 mmol/L.
(b) Insulin stimulates glycogen synthesis in the liver and skeletal muscle cells, at the same time, K+ moves into cells.
Insulin stimulates Na+-K+ ATPase.

(c) Familiar hypokalemia periodic paralysis is a rare disease, there is a acute shift of K+ from ECF to ICF, the [K+]e will reduce, which causes paralysis of the limb and trunk.
(d) Hyperthyroidism 甲 亢 : Over-dose thyroxin stimulates Na+-K+ ATPase.
(e) Barium poisoning 钡中毒 : Brium ion is a K+ channel block in cell membrane.
(e) Barium poisoning 钡中毒 : Brium ion is a K+ channel block in cell membrane.
据 2006 年 6 月 26 日中央电视台《每周质量报告》节目报道, 5 月 31 日江西省上饶市发生多起咸蛋中毒事件,铅山县鹅湖镇罗溪村一黑窝点用工业盐下脚料,用来加工生产咸蛋生产出的咸蛋钡超标达 30 ~ 80 倍。 2 人死亡 . 东瓦窑村 69 岁的吴贤水,在午饭吃过咸蛋后 3 小时发病,先是呕吐、腹泻,后气管切开,上了呼吸机,最后死亡。

4) Blood dilution
The concentration of potassium in plasma will reduce in dilute blood.
Multiple factors in diabetes with ketosis and coma.
(3) Effect on the body
1) Effect on neuromuscular irritability 2) Effect on heart 3) Effect on the acid-base balance 4) Effect on the kidney

1) Effect on neuromuscular irritability
Neuromuscular irritability (excitability) indicates the degree of difficulty or easy to start AP. High excitability means easy to start AP.
Excitability is determined by the distance between the RMP and TMP. The less distance (difference) , the higher of excitability.
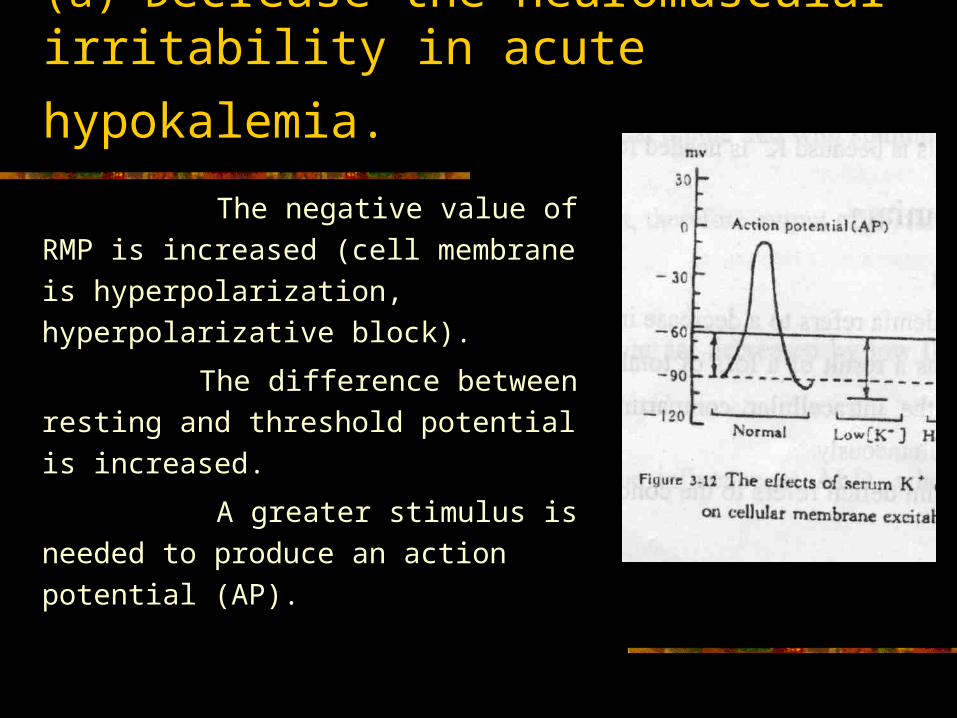
(a) Decrease the neuromuscular irritability
in acute hypokalemia. The negative value of RMP is
increased (cell membrane is
hyperpolarization, hyperpolarizative
block).
The difference between resting
and threshold potential is increased.
A greater stimulus is needed to
produce an action potential (AP).

(b) manifestations
① Effect on skeletal muscles The effects of hypokalemia depend on partly
the decrease speed of serum [k+]. The rapidly decreased serum [k+] leads to
skeletal muscle weakness, flabbiness (soft), and flaccid (soft) paralysis.
The most severe problem of muscular paralysis is ??
In chronic potassium depletion, the k+ in ICF
moves to ECF, both intracellular and extracellular
[k+] are decreased, the ratio of [k+]i to [k+]e is not
obviously changed, the resting potential is not
changed.
Chronic potassium depletion may lead to the
muscle atrophy (thin and weakness of the muscle)
, which is mainly caused by disturbance of protein
metabolism. Chronic K deficiency decreases the
ATP production and ATPase activity.

In severe K deficiency (<2.5mmol/L),
during strenuous exercises the cells cannot release enough K to dilate the vessels, which can lead to ischemia and necrosis of muscle cells with energy metabolism disturbance (exertional rhabdomyolysis).

② Effect on SMC gastrointestinal tract,
Decreased neuromuscular irritability causes: decreased intestinal motility, abdominal distension, anorexia, nausea constipation. bowel sound 肠鸣音 disappear, paralytic ileus 麻痹性肠梗阻 .

③ Effect on vascular SMC
Decreased muscular excitability leads to postural hypotension.

④ If there are some other electrolytes disturbances at the same time, the manifestations will change.
Low [k+] leads to more negative of RMP; High [Ca2+] leads to the elevation of TMP. (Ca2+ inhabits the Na+ into the cells) Low [k+] + High [Ca2+] will increase the distance
between the RMP and TMP and cause very low neuromuscular excitability.

Low [k+] + low [Ca2+] will restore the normal distance between the RMP and TMP and cause the normal neuromuscular excitability.
Low [k+] leads to more negative of RMP;
Low [Ca2+] leads to the decrease of TMP.

Ca2+ ←————→ combining calcium
H+ OH-
2) Effect on heart (a)Effects on myocardiac cells
a) Arrhythmia
b) Abnormal contractibility c) Abnormal electrocardiogram (ECG)
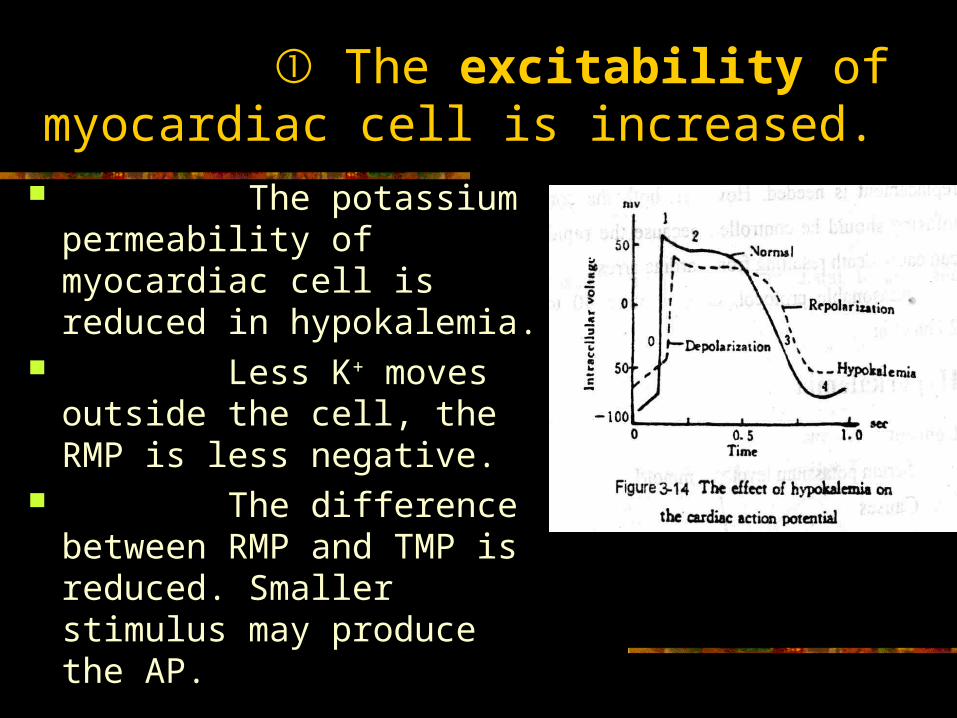
① The excitability of myocardiac cell is increased.
The potassium permeability of myocardiac cell is reduced in hypokalemia.
Less K+ moves outside the cell, the RMP is less negative.
The difference between RMP and TMP is reduced. Smaller stimulus may produce the AP.

Prolonged exaltation phase 超常期 caused by decreased K permeability and rate of phase 3 (repolarization)
Short absolute refractory period caused by short phase 2.
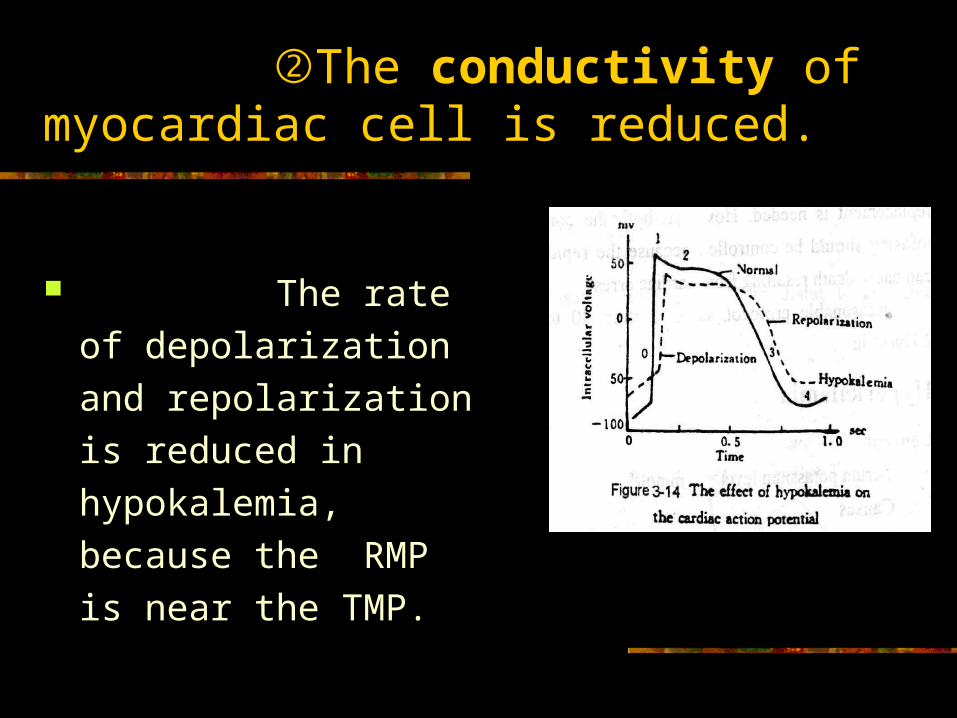
②The conductivity of myocardiac cell is reduced.
The rate of
depolarization and
repolarization is reduced
in hypokalemia, because
the RMP is near the
TMP.

③ The autorhythmicity is increased.
In phase 4, the potassium permeability in hypokalemia is reduced, the outward potassium current is decreased and inward sodium current is relatively increased.The speed of spontaneous depolarization is increased. (Slope rise steeply)

Summary of the effect of hypokalemia on the myocardiac cells
The excitability is increased.Prolonged exaltation phase 超常期延长 :Short absolute refractory period 有效不应期
短 :The conductivity is reduced. The autorhythmcity is increased.
All the alters make it easy to produce arrhythmia (increased heart rate, ectopic beats from Purkinje fiber and ventricular muscle). (Ectopic pacemaker) (nodus sinuatrialis)
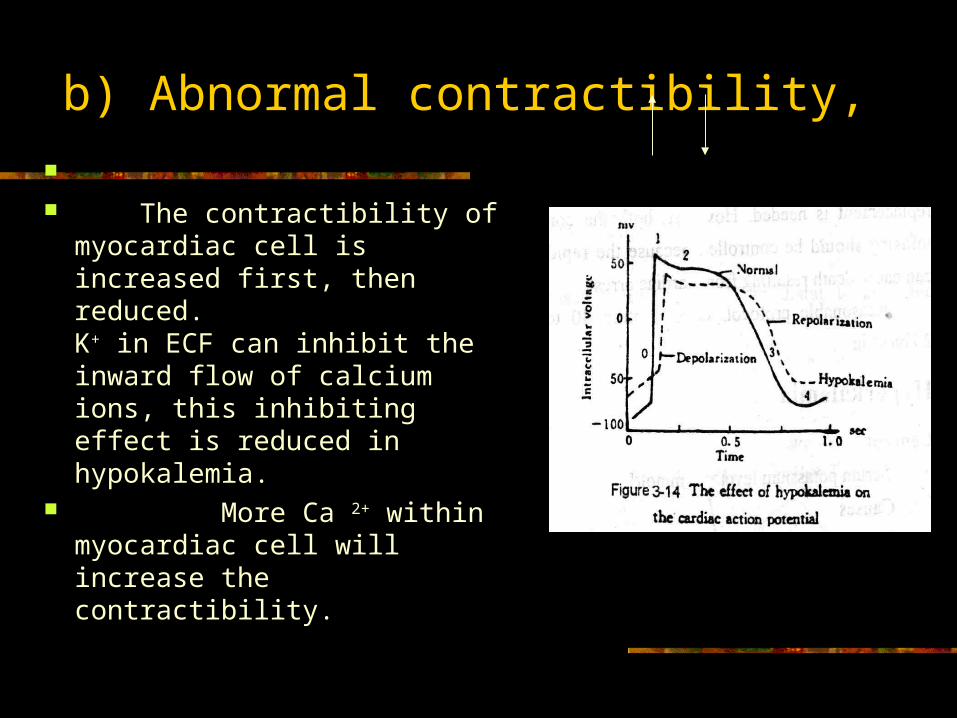
b) Abnormal contractibility,
The contractibility of
myocardiac cell is increased first, then reduced. K+ in ECF can inhibit the inward flow of calcium ions, this inhibiting effect is reduced in hypokalemia.
More Ca 2+ within myocardiac cell will increase the contractibility.

In severe hypokalemia , ATP production and ATPase activity are reduced which causes low myocardial contractibility.

Electrocardiogram (ECG)The P wave reflects depolarization of atrial muscle and represents the original impulse passes through the atrium.
The QRS complex represents depolarization of the ventricular muscle mass, and reflects the speed of conduction throughout the ventricle.
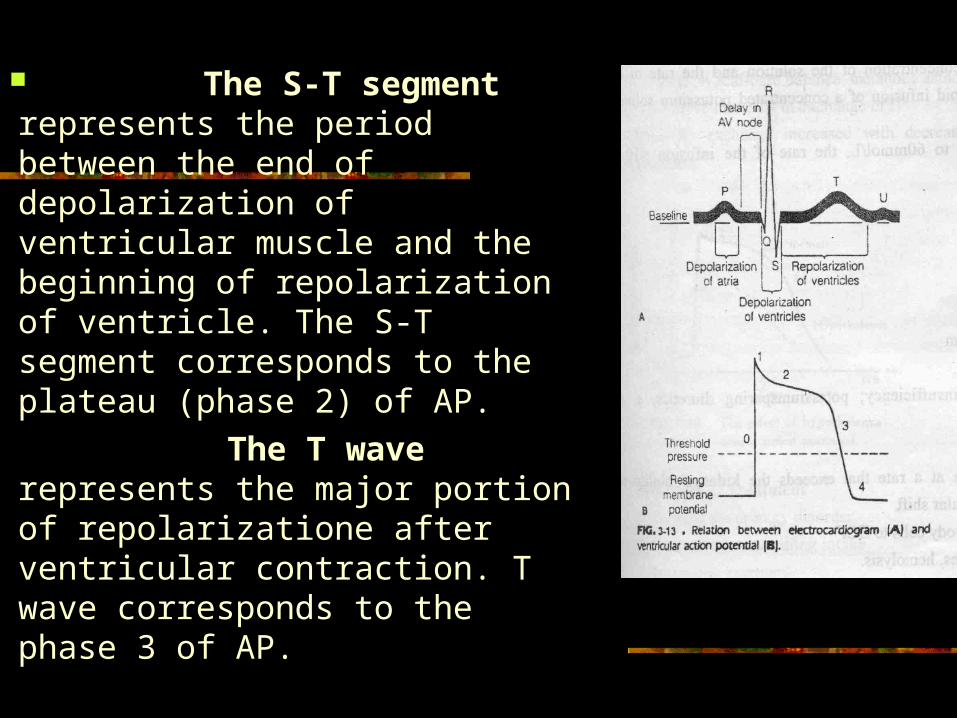
The S-T segment represents the period between the end of depolarization of ventricular muscle and the beginning of repolarization of ventricle. The S-T segment corresponds to the plateau (phase 2) of AP.
The T wave represents the major portion of repolarizatione after ventricular contraction. T wave corresponds to the phase 3 of AP.

C) Abnormal ECG

Broad and flat T wave appears because the potassium permeability in hypokalemia is reduced, the rate of repolarization is reduced. The phase 3 is prolonged.
Prolonged QRS complex are caused by reduced conductivity.

Suppressive S-T segment is related to the short phase 2 due to accelerated inward flow of calcium.
Prominent U wave can be often seen in hypokalemia, but it is hard to explain the mechanism.

3) Effect on the acid-base balance
Hypokalemia leads to metabolic alkalosis.
When [K+]e of ECF reduce, the K+ of ICF moves out of the cells, at the same time, H+ moves into the cells for electric neutrality.
Then the [H+] in ECF will be reduced, which is called metabolic alkalosis. (Depending on the primary disease)
There are two kinds of ion exchange in renal tubules:
K+ -- Na+ H+ -- Na+ ,. In hypokalemia, the K+-Na+ exchange is
reduced, the H+--Na+ exchange will increase, so the excretion of H+ from kidneys is increased, which leads to acidic urine.

Usually in alkalosis, the elimination of H+ is reduced from kidneys, and the urine should be alkaline.
But in the alkalosis caused by hypokalemia, the urine is acidic, it is unusual, so it is called unusual aciduria.

4) Effect on the kidney
Pathologic study found the swelling, proliferation, vacuolation in proximal tubular cells, the renal tubular cells can not produce sufficient cAMP, which is necessary for ADH to work, so the tubules lose the concentrating ability to urine.
The volume of urine is increased and the specific gravity will reduce.
Thirst may occur in patients with hypokalemia.

4. Principle of treatment 1) Etiological treatment is to correct the
underlying diseases. 2) The major problem of replacement of
potassium is to produce the hyperkalemia Replacement of potassium salts slowly
after urination (no oliguria). 见尿补钾 Oral potassium chloride is better than
intravenous administration. We must pay attention to the rate of
intravenous administration and the potassium concentration of potassium chloride solution.

(a) When K deficiency and oliguria, the [K+]e may not be severely reduced because of dehydration and acidosis at the same time.
(b) It will take 1~2 days to get the balance of [K+]I and [K+]e. (10~15 days)

Replenish KCl may correct both hypokalemia and metabolic alkalosis.
Replenish KHCO3 may correct both hypokalemia and metabolic acidosis. .

Case Discussion No.1 1. A 36-year-old man was hospitalized with a
3-day history of fever and watery diarrhea. His blood pressure was 90/60 mmHg, the pulse was 112/min, temperature is 38.0 . The ℃abdomen was distended with low skin elasticity.
The laboratory results were: Arterial blood: pH=7.21, PaCO2=26 mmHg PaO2= 108 mmHg. [Na+]=135 mmol/L [K+] =3.0 mmol/L [HCO3-] = 16 mmol/L Urine: pH=5.0, Specific gravity= 1.028

The patient’s problems were: (1)isotonic dehydration (2)metabolic acidosis (3)hypokalemia.

病例分析 1 .患婴, 3 个月,入院前 1 天开始发热。
呕吐,水样便每日 20 余次。伴烦躁、烦渴。查体: 39.8 , ℃ 嗜睡,醒后烦躁,皮肤干热,明显腹胀。治疗:抗菌素,输入生理盐水 1200ml 。次日病情加重,极烦渴,呼吸深,惊厥,昏迷,并发肠麻痹死亡。







![Disorders of Potassium Metabolismanemia is associated with potassium uptake by newly formed cells, which is occasionally of sufficient magnitude to cause hypokalemia [13]. FIGURE 3-8](https://static.fdocuments.us/doc/165x107/5e5313ac9e88f738f0525316/disorders-of-potassium-metabolism-anemia-is-associated-with-potassium-uptake-by.jpg)



![Simple Algorithm of Arterial Blood Gas Analysis to Ensure ... · a. acidosis→ hyperkalemia b. alkalosis→ hypokalemia Base excess & base deficit [9,10] In human physiology base](https://static.fdocuments.us/doc/165x107/5e68d1f9a3c8150f0033b9c4/simple-algorithm-of-arterial-blood-gas-analysis-to-ensure-a-acidosisa-hyperkalemia.jpg)





