![Hypoglycemia and Diabetes · hypoglycemia, including severe hypoglycemia, occur in people with type 2 diabetes.[25] There is no doubt that hypoglycemia can be fatal.[26] In addition](https://static.fdocuments.us/doc/165x107/5f0518c07e708231d4113f09/hypoglycemia-and-hypoglycemia-including-severe-hypoglycemia-occur-in-people-with.jpg)
Hypoglycemia in Pregnancy

of 6
-
Upload
renzo-cruz-caldas -
Category
Documents
-
view
218 -
download
0
Transcript of Hypoglycemia in Pregnancy
-
8/12/2019 Hypoglycemia in Pregnancy
1/6
I nt . J. Gynaecol. Obstet, 1986, 24: 263-268International Federation of Gynaecolog y & Obstetrics
263
SEVERE HYPOGLYCEMIA DURING PREGNANCY ITS FREQUENCY ANDPREDISPOSING FACTORS IN DIABETIC WOMEN
W. RAYBURNa, E. PIEHLa, S. JACOBERb, A. SCHORKCand L. PLOUGHMAN aDi vi sion of M aternal Fetal M edicine, Department of Obstetri cs and Gynecology, bDw w on of Endocrinol ogy, Departmentof Int ernal M edicine, Uni versity of M ichigan M edical School and Department of Biostati stics. School of Public Healt h, Uni versit?of M ichigan, MI (USA)(Received October 28th. 1985)(Accepted March 26th, 1986)
AbstractRayburn W , Pi ehl E, Jacober S, Schork A,Ploughmann I . (Divi sion of Maternal Fet alM edicine, Department of Obst et ri cs andGynecology, Division of Endocrinology,Department of I n ernal M edicine, Uni versit yof M i chigan M edical School and Departmentof Bi ost at i st i cs, School of Publi c Heal t h,Uni versit y of M ichigan, M I , USA). Severehypoglycemia duri ng pregnancy: I t s fr e-quency and predi sposi ng factors in di abet i cw omen.
I nt J Gynaecol O bstet 24: 263-268, 1986Severe hypoglycemi c epi sodes, as defi ned
as al t ered consciousness t o t he ext ent t hatsel f t reatment i s impossi ble, w ere soughtprospecti vely i n pregnant di abet i c w omen.One or more episodes w ere found i n noneof 21 gestational onset, insulin-requiringw omen duri ng t hei r 28 pregnanci es butw ere present in 19 (33%) of t he 5 7 al readyinsul i n dependent (Type 1) w omen duri ng26 (36%) of t hei r 72 pregnanci es, The mostcommon predi sposi ng fact ors i ncluded st ri ctglucose contr ol , anorexia, earl y morni nghour s (1200-09001, l ack of an adrenergi cresponse and t ime short l y before t he nextanticipated meal.
Keywords Hypoglycemia; Diabetes; Preg-nancy; Insulin.0020-7292/86/ 03.50o 198 6 International Federation of Gynaecology & ObstetricsPublished and Printed in Ireland
IntroductionAs more diabetic wom en become pregnant,a greater emp hasis is being placed on optimal
perinatal outcomes. The trend towardsimproved fetal surviva l is largely attributedto stricter metabo lic control before andduring gestation, since most comp licationsare conditioned by maternal glucose levels[ 1 I. Furthermore, a considerable body ofclinical and scientific data has supported thecontention that meticulous m anagem entmay delay or prevent complications in thediabetic woman [ 9 I.Avoidance of hyperglycemia, rather thanhypoglycemia, is generally stressed a s thefirst priority durin g pregna ncy. In strivingfor strict metabolic control, it is expectedthat pregnan t diabetic wom en are at in-creased risk for hypoglycemia. Blood glucoselevels at these times are lower than thelowest limit of normal physiologic fluctu-ations, which in many adults is between40 60 mg [51. The release of glucagonand catecholamines (primarily epinephrine)act as overlapping glucoregulatory systemsto prevent or correct hypoglycemia [ lo].
Once low glucose levels are reached.maternal symptom s or signs become ap parenteither from an adrenergic defense responseor from cellular malnu trition at the neuronallevel [ 5 I. Adrenergic symptom s predominatein reproductive age persons without long
Int J G,anaccol Q bstet -74
-
8/12/2019 Hypoglycemia in Pregnancy
2/6
264 Rayburn et al.
standing diabetes [ 5,101. These symptomsinclude shakiness, palpitations, tachycardia,irritability, sweating, hunger and perioralparesthesias. Therapy to reverse these symp-toms includes the self-administration oforange juice, commercial glucose concen-trates, honey, sugar, candy, cola drinksand milk.
When this warning is absent, symptomsfrom neuronal cellular malnutrition maydevelop. Short-term central nervous systemdysfunction may lead to headache, loss ofconcentration, confusion, visual disturbance,stupor and unconsciousness. Convulsions,coma and even death may supervene withoutprompt treatment [ 5 I.
A search of the obstetric literature hasnot disclosed descriptions of severe maternalhypoglycemia. The purpose of this studywas to determine the frequency of severehypoglycemia during pregnancy and tobetter understand the predisposing condi-tions. In doing so, preventative medical careor prompt medical treatment may be offered.
aterials and methods
Women eligible for this investigationincluded those who were already insulin-dependent (Type 1) before conceptionand those who required insulin for the firsttime during gestation. Each person attended aweekly high risk obstetric clinic during the 3?&year period between July, 1981 and Dec-ember, 1984. Pregnancies aborting before the12th week were excluded. Care of these wo-men was overseen by both obstetric and endo-crine staff members. Attempts were madeto attain strict glucose control as determinedfrom daily capillary blood glucose deter-minations and standardized for our clinic161, Control was classified as strict if pre-prandial glucose values averaged to be 100mg/dl or less, fair if 101-149 mg/dl, andpoor if 150 mg/dl or more [61.
Data about hypoglycemic episodes weregathered prospectively. Monitoring of bloodglucoses by the patient was undertaken
using reflectance photometers or visually-readblood glucose oxidase strips. A standardform was used by the mothers to recordthe insulin dose and capillary blood glucosevalues obtained four times daily. Each personwas asked to record the time of day andevents surrounding any symptomatic hypo-glycemic episodes in the space provided onthe data sheet. Therapy to relieve thesesymptoms was also recorded. Additionalfindings were ascertained with each weeklyor bi-weekly clinic visit and recorded on theantepartum chart.
Hypoglycemic reactions were classified asmild or severe. Mild reactions were definedas hypoglycemic episodes that could beself treated. These episodes consisted ofadrenergic signs and symptoms as describedpreviously. Severe reactions were definedas hypoglycemia leading to such an alteredconsciousness (loss of concentration, con-fusion, stupor, unconsciousness) that anotherperson was required to administer glucoseor glucagon [ 71 These severe hypoglycemicepisodes were often preceded by a lack ofwarning adrenergic symptoms. Conditionsknown to predispose to severe hypoglycemiain the non-pregnant person were soughtby the investigators and recalled easily bythe patient, close friend or family member[2,3,5,7,9,101.Comparisons between women categorizedas having severe hypoglycemia or not weremade using the chi-square and Studentst-tests and the analysis of variance. A P-valueless than 0.05 was considered to be statistic-ally significant.Results
Seventy-eight diabetic women sought ourcare for 100 pregnancies during the 3?z-yearperiod. Fifty-seven (73 ) of these patientswith 72 pregnancies were already insulindependent, having received therapy beforeconception for 11 -+ 5 years (mean -+ 1 S.D.).These insulin-dependent women were follow-ed for 24 * 4 weeks gestation and delivered
Int J Gynaecol Obstet 24
-
8/12/2019 Hypoglycemia in Pregnancy
3/6
Severe hypo l ycemia duri ng pregnancy 265
at 37 + 1 weeks. The other 21 (27 ) womenwith 28 pregnancies had gestational onsetdiabetes and required insulin for 14 + 3weeks. They were followed for 22 + 3 weeksand delivered at 39 * 1 weeks. Severe hypo-glycemic episodes did not occur duringpregnancy for any of these gestational-onsetdiabetics.
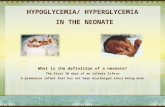
Compared with before conception, preg-nancy was found to predispose to severehypoglycemia in insulin-dependent diabetics.Thirty-five severe hypoglycemic episodes werereported. These occurred in 19 (33 ) of the5 7 already insulin-dependent women during26 (36 ) of the 72 pregnancies. The numberof severe hypoglycemic reactions per patientmonth is shown in Fig. 1. Severe hypogly-cemia occurred with much less frequency(0.08 episode/month) than symptomaticmild hypoglycemia (5 .O episodes/month).A recurrence of severe hypoglycemia duringpregnancy was found in eight of these 19women. Conditions associated with theserecurrences included the desire for strictmetabolic control, a lack of a prior adren-ergic response, and a missed meal.
Conditions predisposing to severe hypo-glycemia were similar to those associatedwith mlde hypoglycemia. These factors
M - Ef 23456769Pa.d or turnGESTATIONAL AGE imor*hr
Fig. 1. Severe hypoglycemic episodes per patient mo nthfor insulin-dependent diabetic women during pregnancy.(Num ber in parentheses represents number of pregnancies).
Table 1. C onditions predisposing to severe hypoglycemiaon 35 occasions during pregnancy. (These conditions wereoften not found to be mutua lly exclusive of each other).Condition No. ( )Strict glucose controlAnorexiaEarly morning hours (1200-0800)Lack of a prior adrenergic responseTwo hours before an anticipated mealPoor glucose controlMissed mealExcess activityInsulin overdoseRecent severe hypoglycemiaRecent hospitalization
21 (60)15 (43)14 (40)14 (40)13 (38)8 (23)6 (17)5 (14)5 (14)4 (14)4 (14)
included strict glucose control, anorexia,early morning hours (1200-0800), lackof an adrenergic response, and 2 h before thenext anticipated meal (Table I). All of thesefactors were not mutually exclusive of eachother. Pregnancy profiles of the alreadyinsulin-dependent women are compared be-tween those in which severe hypoglycemiawas present or absent (Table II). The maternalage, race, parity, prepregnancy insulin dose,Table 11. Profiles of insulin-dependent diabetic wom enaccording to the presence or absence of severe hypoglycemiaduring pregnancy.
Severe hypoglycemiaaPresent(N = 26)
Absent(N = 46)
Maternal age (years)Race (no. Caucasian)Parity (no, primiparous)Dura tion of diabetes (years)Prepregnancy insulin dose
(total units per day)Gestational ageInitial prenatal visit weeks)Delivery (weeks)
Glucose control before deliveryStrictFairPoor
24 &5 262424 (92 ) 41 (89 )15 (58 ) 34 (74;)12 25 11+746 215 41 t 17
Ilk4 12 +436+12 37_+111 (42 ) 24 (52 )10 (39 ) 13 (28 )
5 (19 ) 9 (20 )aDifference in all comparisons were not found to be statistic-
ally different (P > 0.05).
Int .J Gvnaecol Obstet 24
-
8/12/2019 Hypoglycemia in Pregnancy
4/6
266 Rayburn et al.
duration of diabetes, duration of prenatalcare, and extent of metabolic control latein gestation were not statistically differentbetween the two groups.
Therapy for any unconscious motherconsisted of either the intramuscular admini-stration of 1 ml of glucagon by a familymember or the infusion of glucose using25-50 ml of a 50 glucose solution in anemergency room. A return to conscious-ness was apparent with prompt treatment.Adverse maternal effects were found inthe two cases described below when therapywas begun after prolonged severe hypo-glycemia.Case 1
A 24-year-old Gz PO woman with class Rdiabetes and a prior history of poor glucosecontrol was evaluated initially at 11 weeksgestation. She continued to have early morn-ing nausea following the initial hospitaliz-ation, in which her glucose control becomefair (capillary glucose levels averaging be-tween 101-150 mg/dl. On the day of heremergency hospitalization at 12 weeksgestation, she had taken her usual morninginsulin dose (36 units NPH, 8 units regularinsulin) but did not eat breakfast or a latemorning snack. Her fiance last spoke withher at noon. She was found unconsciouswith vomitus in her mouth at about 1700.Her serum glucose level in the emergencyroom was 33 mg/dl, and she became moreconscious following the infusion of 25 of50 dextrose in water. Her initial testsrevealed an arterial PO, of 35 mmHg anddiffuse bilateral pulmonary infiltrates onchest X-ray. Therapy was undertaken forapparent adult respiratory distress fromaspiration of vomitus. She became increas-ingly difficult to oxygenate despite intu-bation, positive-end expiratory pressureswith high concentrations of oxygen, anti-biotics, and supportive measures. She abortedspontaneously, underwent repeated severehypoxic episodes, and subsequently diedwithin 11 days of admission.
Case 2A 22-year-old G3 PO SAbz woman sus-
tained hypoglycemia induced grand ma1seizures. Eight months before gestationher first and only seizurs occurred afterdeveloping a low blood glucose level. Aneurologic evaluation was unremarkable. Herdiabetes had been present for 13 years, andshe was seen initially at 9 weeks gestation.The 47 units of insulin were administereddaily by continuous subcutaneous infusionand intermittent subcutaneous injection. Herglucose control was excellent with a hemo-globin ArC of 6.6 and strict control (averagedglucose values below 100 mg/dl during theinitial hospitalization. During the 12thweek, she sustained a grand ma1 seizure at0900 following her usual insulin therapy anda small serving of cereal. A capillary glucosedetermination of 27 mg was similar to thatrecorded earlier in the week without anyapparent warning symptoms. The nauseaand vomiting of pregnancy were the onlyother predisposing factors. An infusionof glucose at the nearby emergency roomcaused the tonic-clonic seizure activity tosubside.
The perinatal outcomes of the insulin-dependent women sustaining severe hypo-glycemia were similar to those without
Table III. Perinatal outcomes of insulin-dependent womenaccording to the presence or absence of severe hypoglycemicepisodes during pregnancy.
Severe hypoglycemiaaPresent Absent(N = 26) (N = 46)
Gestational age~31 weeksBirth weight (g)
Large for gestational agel-mm Apgar scoreS-mm Apgar scoreMajor anomalies
15 (58 ) 30 (65 )2992 t 453 3245 C 6468 (31 ) 22 (48 )7f2 7+18+1 8211 (4 ) 2 (4 )
Differences in all comparisons were not found to be statis-tically significant (P > 0.05).
Int J Gynaecol Obstet 24
-
8/12/2019 Hypoglycemia in Pregnancy
5/6
Severe hypo l ycemia duri ng pregnancy 267
such episodes. The gestational age at delivery,route of delivery, birth weight, l- and 5-minute Apgar scores, and percent of anoma-lous infants were not significantly different(Table III). The only stillborn infant in allthe diabetic women was delivered at 3 1 weeksgestation before fetal monitoring was under-taken. This 20-year-old primigravid motherwith class C diabetes had poor glucose controlin early gestation and sustained two severehypoglycemic episodes at 13 and 15 weeksgestation. Later in pregnancy, her metaboliccontrol was much improved with dailyglucose monitoring. An autopsy of thenormal-appearing infant was unremarkable,and histologic examination of the placentarevealed chronic vascular changes.Discussion
A diabetic woman undergoing pregnancymust be educated in attempting to achievea fine balance between strict glucose controland mild hypoglycemic episodes. Most ofthese persons had never attempted such closemonitoring of their blood glucose levels.Pregnancy was found to be associated withmore frequent episodes of severe hypogly-cemia in women who were already insulin-dependent. A recent review of five centersby Santiago et al. [ 71 in non-pregnant dia-betics revealed the frequencies of severehypoglycemia to be 0.005-o. 103/patientmonth. This is similar to the O.O8/patientmonth during pregnancy in the presentstudy.
Because of improvements in screeningfor diabetes and treatment during pregnancy,more women are being treated with insulinand for longer periods during pregnancy.None of the gestational onset, insulin-requir-ing diabetic women in this study encounteredany severe hypoglycemia. Symptoms fromadrenergic responses were sufficient forhypoglycemia to be detected before it becamesevere. Once these persons became awareof these warning symptoms, relief withself-administration of oral glucose supple-
ments was all that was necessary. Many ofthese gestational diabetics required largedaily doses of insulin, and an insulin over-dose remains a theoretic concern.
Defective recovery from insulin-inducedhypoglycemia was found to occur in one-third of the already insulin-dependent womenduring pregnancy. This finding is higher thanthe 4 reported by Goldstein et al. [2] andthe 26 by Goldwicht et al. [3] in childrenand young adults. Those investigators alsofound that bouts of frequent or severe symp-tomatic hypoglycemia may be more commonwhen diabetes is well-controlled duringintensive therapy. The previously insulin-dependent diabetic women in this studywere generally very conscientious abouttheir diabetes self-care and maintained fairor strict glucose control. Difficulties witheating or missing a meal would be explainedby early gestation nausea, a lack of desireto increase caloric intake and viral gastro-enteritis.
Perinatal outcomes for insulin-dependentwomen in this study were similar regardlessof the presence or absence of severe hypo-glycemia. This reassurance is limited by thesmall number of pregnancies and the evalu-ation of infants in the newborn period only.Animal studies by Kalter and Warkanyhave revealed no increased long-term struc-tural defects in offspring following hypo-glycemic shock during an insulin overdose[4]. This contrasts with a report by Sobelin 1960 in which two children were reportedto have multiple defects following the treat-ment of 17 mothers with insulin shock forpsychiatric illness [ 81.
The authors conclude that pregnancyin already insulin-dependent diabetic womenpredisposes to a greater risk of severe hypo-glycemia. It is difficult to predict this beforegestation, but conditions in which there isinadequate caloric intake or a lack of analarming adrenergic response should beconsidered. Prompt reversal of any alteredcentral nervous function with glucose orglucagon therapy and subsequent modi-
Int J G_vnaecol Obstet 24
-
8/12/2019 Hypoglycemia in Pregnancy
6/6
268 Rayburn et alfication of therapeutic goals (permittingmild fasting hyperglycemia, more frequentglucose monitoring, patient reeducation,insulin infusion screening tests) are necessaryto avoid future catastrophic consequences.References
Gabbe S: Diabetes m ellitus in pregnancy. In Fetal andMatern al M edicine (E Quilligan, N Kretchmer eds),pp 587. 608. Wiley Medical Publication, 1980.Goldstein D, England V, Hess R et al.: A prospectivestudy of symptomatic hypoglycemia in young diabeticpatients. Diab Care 4: 601, 1 981.Goldwicht C, Stama G, Papoe L, et al.: Hypog lycemiareactions in 172 type I (insulin-dependent) diabeticpatients. Diabetologia 24: 95, 1985.Kalter H, Wa rkany J: Experimentation production ofcongenital malformations in mamm als by metabolicprocedure. Physiol Rev 39: 69, 1959.Lefebyre PJ and Luyckx AS: Hypoglycem ia. In DiabetesMellitus, Theory and Practice. (M Ellenberg, H R Ritkin
67
8
910
eds), 3rd edn, pp 987-100 4. Medical ExaminationPublishing Co., New York, 1983.Raybu rn W, Piehl E, Lewis E et al.: Changes in insulintherapy during pregnancy. Am J Perinatol 2: 271, 1985.Santiago V, White N , Skor D et al.: Defective glucosecounter-regulation limits intensive therapy of diabetesmellitus. Am J Physio1246: E 215, 1984 .Sobel DE: Fetal damage due to ECT, insulin coma,chlorpromazine or reserpine. A MA Arch Gen Psycho12: 606, 1960.Unger RH: Meticulous control of diabetes: Benefits,risks, and precautions. Diabetes 31: 479, 1 982.Unger RH: Insulin-glucagon relationships in the defenseagainst hypoglycemia. Diabetes 32: 575, 1983.
Address for reprints:
Williim Rayburn, M.D.Department of Obstetrics GynecologyUniversity of Nebraska Medical Center42nd Dewey AvenueOmaha, NE 68105, USA
Znt J Gynaecol O bstet 2 4