Hypertension: New Trials – Best Treatments Karen Moncher, MD Assistant Professor University of...
67
Hypertension: New Trials – Best Treatments Karen Moncher, MD Assistant Professor University of Wisconsin School of Medicine and Public Health
-
Upload
bernice-mclaughlin -
Category
Documents
-
view
218 -
download
2
Transcript of Hypertension: New Trials – Best Treatments Karen Moncher, MD Assistant Professor University of...

Hypertension:New Trials – Best Treatments
Karen Moncher, MD
Assistant Professor
University of Wisconsin School of Medicine and Public Health

Overview
• Epidemiology • Clinical Trials and Trends
– “All things old become new again”
• Management Guidelines– Compelling reasons for treatment– Management based on patient problems and pharmacology
• Patient Adherence

Top 10 HTN RX Problems
10. Lack of Public Awareness 68%
9. Lack of Provider Awareness - Systolic BP
8. Lack of Treatment 54%
7. Lack of Provider Awareness Lifestyle RX
6. Providers / Patients - office BP is higher
5. Thought that BP rise with age is not a risk

Top 10 HTN RX Problems
4. Lack of use of combination therapy, especially with inexpensive thiazide diuretic (concept that thiazide is synergistic with all)
3. Inappropriate choice of antihypertensive agent based on patient
2. Providers and patients underestimate the benefits of RX, assume less Quality of Life
1. Adherence - Adherence - Adherence

-70
-60
-50
-40
-30
-20
-10
0
1970 1974 1978 1982 1986 1990 1994
Year
Per
cen
t d
ecli
ne
White men
White women
Black men
Black women
The decline in age-adjusted mortality for stroke in the total population is 59.0%. *Age-adjusted to the 1940 U.S. census population.
Percent Decline in Age-Adjusted* Mortality Rates for Stroke by Sex and
Race: United States, 1972-94

-60
-50
-40
-30
-20
-10
0
1970 1974 1978 1982 1986 1990 1994Year
Per
cen
t d
ecli
ne
White men
White women
Black men
Black women
The decline in age-adjusted mortality for CHD in the total population is 53.2%.*Age-adjusted to the 1940 U.S. census population.
Percent Decline in Age-Adjusted* Mortality Rates for CHD by Sex and
Race: United States, 1972-94

Incidence of Reported End-Stage Renal Disease Therapy, 1982-1995
50
100
150
200
250
1983 1985 1987 1989 1991 1993 1995
Year
Ra
te p
er
Mill
ion
Po
pu
lati
on
253*
*Provisional data.Adjusted for age, race, and sex.

Demographic Trends
Elderly US population will double “baby boomer” generation
Projected Elderly Population Age 65+ (millions)
0
25
50
75
1990 2000 2010 2020 2030
31 million
12.6% total US population
65 million
21.8% total US population

HypertensionHypertension DyslipidemiaDyslipidemia DiabetesDiabetes
Liao. Liao. Clin Chem.Clin Chem. 1998;44:1799-1808; Spieker et al. 1998;44:1799-1808; Spieker et al. J Hum Hypertens.J Hum Hypertens. 2000;14:617-630; 2000;14:617-630; Belton et al. Belton et al. Circulation.Circulation. 2000;102:840-845; Ross. 2000;102:840-845; Ross. N Engl J MedN Engl J Med. 1999;340:115-126.. 1999;340:115-126.
Risk Factors, Including Hypertension and Dyslipidemia, Promote CVD by Contributing
to Endothelial Dysfunction
Endothelial dysfunctionEndothelial dysfunction
CVDCVD
InflammationInflammation
Leukocyte adhesionLeukocyte adhesion
Endothelial permeabilityEndothelial permeability
Foam cell formationFoam cell formation
T-cell activationT-cell activation
AtherosclerosisAtherosclerosis
Thromboxane AThromboxane A22
Prostaglandin HProstaglandin H22
ProstacyclinProstacyclin
COX-1 ActivityCOX-1 ActivityNO SynthesisNO Synthesis
VasoconstrictionVasoconstriction
ThrombosisThrombosis
SuperoxideSuperoxide
EndothelinEndothelin
VasoconstrictionVasoconstriction
Calcium mobilizationCalcium mobilization
SmokingSmoking

Overview
• Epidemiology • Clinical Trials and Trends
– “All things old become new again”
• Management Guidelines– Compelling reasons for treatment– Management based on patient problems and pharmacology
• Patient Adherence

U.S. Department of Health and Human
Services
National Institutes of Health
National Heart, Lung, and Blood Institute
Major Outcomes in High Risk Hypertensive Patients Randomized to
Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)
The ALLHAT Collaborative Research Group
Sponsored by the National Heart, Lung, and Blood Institute (NHLBI)
ALLHAT
JAMA. 2002;288:2981-2997 Dec. 18, 2002

ALLHAT Trial Design
Randomized, double-blind, multi-center clinical trial
Determine whether occurrence of fatal CHD or nonfatal MI is lower for high-risk hypertensive patients treated with newer agents (CCB, ACE-I, alpha-blocker) compared with a diuretic
Known ASCVD, DM, smoker, LVH, low HDL
42,418 high-risk hypertensive patients ≥ 55 years

ALLHATJAMA 2002 Dec. 18
• 33357 men and women - diverse races• HTN and at least one other CHD risk factor• Compared: Thiazide, Lisinopril, Amlodipine, and
previously stopped doxazosin arm• Primary outcome Fatal CHD or non-fatal MI• Secondary outcomes:
– Total Mortality - CVA– Combined CHD - CHF

ALLHAT Step 1Treatment Protocol
Step 1 Agent Initial Dose* Dose 1* Dose 2* Dose 3*
Chlorthalidone 12.5 12.5 12.5 25
Amlodipine 2.5 2.5 5 10
Lisinopril 10 10 20 40
Doxazosin 1 2 4 8
* mg/day

BP Results by Treatment Group
Compared to chlorthalidone:
SBP significantly higher in the amlodipine group (~1 mm Hg) and the lisinopril group (~2 mm Hg).
Compared to chlorthalidone:
DBP significantly lower in the amlodipine group (~1 mm Hg).

Cumulative Mortality Rate
Years to Death0 1 2 3 4 5 6 7
0
.05
.1
.15
.2
.25
.3
Number at risk: Chlor 15,255 14,933 14,564 14,077 12,480 7.185 3,523 4288 Amlo 9,048 8,847 8,654 8,391 7,442 4,312 2,101 217 Lisin 9,054 8,853 8,612 8,318 7,382 4,304 2,121 144
Cumulative Event Rates for All-Cause Mortality by ALLHAT Treatment Group
HR (95% CI) p value
A/C 0.96 (0.89-1.02) 0.20
L/C 1.00 (0.94-1.08) 0.90
ChlorthalidoneAmlodipineLisinopril

Cumulative Combined CVD Event Rate
Years to Combined CVD Event0 1 2 3 4 5 6 7
0
.1
.2
.3
.4
.5
Number at risk: Chlor 15,255 13,752 12,594 11,517 9,643 5,167 2,362 288 Amlo 9,048 8,118 7,451 6,837 5,724 3,049 1,411 153 Lisin 9,054 7,962 7,259 6,631 5,560 3,011 1,375 139
Cumulative Event Rates for Combined CVD by ALLHAT Treatment Group
RR (95% CI) p value
A/C 1.04 (0.99-1.09) 0.12
L/C 1.10 (1.05-1.16) <0.001
ChlorthalidoneAmlodipineLisinopril

Cumulative CHF Rate
Years to HF0 1 2 3 4 5 6 7
0
.03
.06
.09
.12
.15
Cumulative Event Rates for Heart Failure by ALLHAT Treatment Group
HR (95% CI) p value
A/C 1.38 (1.25-1.52) <.001
L/C 1.19 (1.07-1.31) <.001
ChlorthalidoneAmlodipineLisinopril
Number at risk: Chlor 15,255 14,528 13,898 13,224 11,511 6,369 3,016 384 Amlo 9,048 8,535 8,185 7,801 6,785 3,775 1,780 210 Lisin 9,054 8,496 8,096 7,689 6,698 3,789 1,837 313

Biochemical ResultsChlorthalidone Amlodipine Lisinopril
Serum cholesterol- mg/dL
Baseline 216.1 (43.8) 216.5 (44.1) 215.6 (42.4)
4 Years 197.2 (42.1) 195.6 (41.0)* 195.0 (40.6)*
Serum potassium – mmol/L
Baseline 4.3 (0.7) 4.3 (0.7) 4.4 (0.7)*
4 Years 4.1 (0.7) 4.4 (0.7)* 4.5 (0.7)*
Estimated GFR† – mL/min/1.73m2
Baseline 77.6 (19.7) 78.0 (19.7) 77.7 (19.9)
4 Years 70.0 (19.7) 75.1 (20.7)* 70.7 (20.1)*
* p<.05 compared to chlorthalidone† Ann Intern Med. 1999;130:461-470

ALLHAT Conclusions
Amlodipine (representing CCB), lisinopril (representing ACE-I) and chlorthalidone (representing thiazide-type diuretics) were comparable in preventing major coronary events or increasing overall survival.
Although chlorthalidone did not differ from amlodipine in overall CVD event prevention, it was superior to amlodipine in preventing heart failure.

ALLHAT Conclusions
Chlorthalidone was superior to lisinopril in preventing aggregate CV events, principally stroke, HF, angina, and coronary revascularization
Chlorthalidone was superior to doxazosin (representing alpha-blockers) in preventing CV events, including both HF and other CVD.

Overall Conclusions
ALLHAT
Because of the effectiveness of thiazide-type diuretics in preventing one or more major forms of CVD and their lower cost, they should be the drugs of choice for first-step antihypertensive drug therapy, unless there are other compelling indications.

Isolated Systolic Hypertension
Systolic Pressure 140 mmHg
&
Diastolic < 90 mmHg
JNC VI Report, NIH, JNC VI Report, NIH, NHLBINHLBI

SHEP Study
• Treatment of elderly patients with ISH
• Thiazide diuretic plus atenolol if needed
• Stroke, total mortality, CVD events
• 63% patients had BP controlled with diuretic alone
• CVA reduced 36% (3/100) and CVD events reduced 6 per 100 in 4.5 years
JAMA 1991;265;3255-3264



HTN in the Elderly Trial*
ACE (enalapril) vs. HCTZ • 6083 adults with HTN aged 65 - 84 years• Australia Family Practice clinics• Open-label study in multiple practices• BP reduction was the same: 26/12 mm Hg• All CVD events or death reduced for men (17%
or approximately 4 / 100)• No difference in events for women
NEJM 2003;348:583-592

BP-Lowering Treatment Trialists’ Meta-analysis:Comparisons of Active Treatments and Control
FavorsFavorsActiveActive
FavorsFavorsControlControl
0.5 1.0 2.0
Relative Risk RR (95% CI)RR (95% CI)
StrokeStroke
Coronary heart diseaseCoronary heart disease
Heart failureHeart failure
BP Difference From PlaceboBP Difference From Placebo(SBP/DBP mm Hg)(SBP/DBP mm Hg)
Blood Pressure Lowering Treatment Trialists’ Collaboration. Blood Pressure Lowering Treatment Trialists’ Collaboration. LancetLancet. 2003;362:1527-1535.. 2003;362:1527-1535.
Major CV eventsMajor CV events
CV mortalityCV mortality
Total mortalityTotal mortality
-5/-2-5/-2
-5/-2-5/-2
-5/-2-5/-2
-5/-2-5/-2
0.72 (0.64, 0.81)0.72 (0.64, 0.81) ACEI vs placeboACEI vs placebo -5/-2-5/-2
0.80 (0.73, 0.88)0.80 (0.73, 0.88)-5/-2-5/-2 ACEI vs placeboACEI vs placebo
0.82 (0.69, 0.98)0.82 (0.69, 0.98) ACEI vs placeboACEI vs placebo
ACEI vs placeboACEI vs placebo 0.88 (0.81, 0.96)0.88 (0.81, 0.96)
ACEI vs placeboACEI vs placebo 0.78 (0.73, 0.83)0.78 (0.73, 0.83)
ACEI vs placeboACEI vs placebo 0.80 (0.71, 0.89)0.80 (0.71, 0.89)
0.62 (0.47, 0.82)0.62 (0.47, 0.82) CA vs placebo CA vs placebo -8/-4-8/-4
0.78 (0.62, 0.99)0.78 (0.62, 0.99)-8/-4-8/-4 CA vs placeboCA vs placebo
CA vs placeboCA vs placebo 0.82 (0.71, 0.95)0.82 (0.71, 0.95)-8/-4-8/-4
1.21 (0.93, 1.58)1.21 (0.93, 1.58) CA vs placeboCA vs placebo -8/-4-8/-4
CA vs placeboCA vs placebo 0.78 (0.61, 1.00)0.78 (0.61, 1.00)-8/-4-8/-4
CA vs placeboCA vs placebo 0.89 (0.75, 1.05)0.89 (0.75, 1.05)-8/-4-8/-4

0.5 1.0 2.0
BP-Lowering Treatment Trialists’ Meta-analysis: Comparisons of Different Active Treatments
Relative Risk RR (95% CI)RR (95% CI)BP Difference Between RxBP Difference Between Rx
(SBP/DBP mm Hg)(SBP/DBP mm Hg)
FavorsFavorsFirst ListedFirst Listed
FavorsFavorsSecond ListedSecond Listed
Major CV eventsMajor CV events
CV mortalityCV mortality
Total mortalityTotal mortality
1.02 (0.98, 1.07)1.02 (0.98, 1.07)2/02/0 ACEI vs D/BBACEI vs D/BB
1.03 (0.95, 1.11)1.03 (0.95, 1.11)2/02/0 ACEI vs D/BBACEI vs D/BB
1.00 (0.95, 1.05)1.00 (0.95, 1.05)2/02/0 ACEI vs D/BBACEI vs D/BB
1.04 (1.00, 1.09)1.04 (1.00, 1.09)1/01/0 CA vs D/BBCA vs D/BB
1.05 (0.97, 1.13)1.05 (0.97, 1.13)1/01/0 CA vs D/BBCA vs D/BB
0.99 (0.95, 1.04)0.99 (0.95, 1.04)1/01/0 CA vs D/BBCA vs D/BB
0.97 (0.92, 1.03)0.97 (0.92, 1.03)1/11/1 ACEI vs CAACEI vs CA
1.03 (0.94, 1.13)1.03 (0.94, 1.13)1/11/1 ACEI vs CAACEI vs CA
1.04 (0.98, 1.10)1.04 (0.98, 1.10)1/11/1 ACEI vs CAACEI vs CA
D=diuretic; BB=D=diuretic; BB=-blocker.-blocker.Blood Pressure Lowering Treatment Trialists’ Collaboration. Blood Pressure Lowering Treatment Trialists’ Collaboration. LancetLancet. 2003;362:1527-1535.. 2003;362:1527-1535.

FavorsFavorsFirst ListedFirst Listed
FavorsFavorsSecond ListedSecond Listed
0.5 1.0 2.0
BP-Lowering Treatment Trialists’ Meta-analysis: Comparisons of Different Active Treatments
Relative Risk RR (95% CI)RR (95% CI)BP Difference Between RxBP Difference Between Rx
(SBP/DBP mm Hg)(SBP/DBP mm Hg)
CA vs D/BBCA vs D/BB 1.33 (1.21, 1.47)1.33 (1.21, 1.47)1/01/0
0.93 (0.86, 1.00)0.93 (0.86, 1.00) CA vs D/BBCA vs D/BB 1/01/0
1.01 (0.94, 1.08)1.01 (0.94, 1.08) CA vs D/BBCA vs D/BB 1/01/0
ACEI vs CAACEI vs CA 0.82 (0.73, 0.92)0.82 (0.73, 0.92)1/11/1
1.12 (1.01, 1.25)1.12 (1.01, 1.25) ACEI vs CAACEI vs CA 1/11/1
0.96 (0.88, 1.04)0.96 (0.88, 1.04) ACEI vs CAACEI vs CA 1/11/1
StrokeStroke
Coronary heart diseaseCoronary heart disease
Heart failureHeart failure
1.09 (1.00, 1.18)1.09 (1.00, 1.18) ACEI vs D/BBACEI vs D/BB 2/02/0
0.98 (0.91, 1.05)0.98 (0.91, 1.05) ACEI vs D/BBACEI vs D/BB 2/02/0
1.07 (0.96, 1.19)1.07 (0.96, 1.19) ACEI vs D/BBACEI vs D/BB 2/02/0
Blood Pressure Lowering Treatment Trialists’ Collaboration. Blood Pressure Lowering Treatment Trialists’ Collaboration. LancetLancet. 2003;362:1527-1535.. 2003;362:1527-1535.

Overview
• Epidemiology • Clinical Trials and Trends
– “All things old become new again”
• Management Guidelines– Compelling reasons for treatment– Management based on patient problems and pharmacology
• Patient Adherence

National Guidelines Recognize the Relationship Between Hypertension and Dyslipidemia
JNC 7 recommends assessing a patient’s lipid profiles when setting appropriate BP treatment goals
NCEP ATP III recognizes hypertension as a major risk factor that modifies lipid goals
When hypertension or dyslipidemia is diagnosed,When hypertension or dyslipidemia is diagnosed,test for the other condition.test for the other condition.
Chobanian et al. Chobanian et al. JAMAJAMA. 2003;289:2560-2572.. 2003;289:2560-2572.Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMAJAMA. . 2001;285:2486-2497.2001;285:2486-2497.

JNC 7: Classification and Management of BP for Adults
BP Classification SBP*
mm Hg DBP*
mm Hg Lifestyle
Modification
Initial Drug Therapy
Without Compelling Indications
With Compelling Indications
Normal <120 and <80 Encourage
Prehypertension 120-139
or 80-89 Yes No antihypertensive drug indicated.
Drug(s) for compelling indications.†
Stage 1 Hypertension
140-159
or 90-99 Yes
Thiazide-type diuretics for most. May consider ACEI, ARB, -blocker, CCB, or combination.
Drug(s) for compelling indications.†
Stage 2 Hypertension
160 or 100 Yes
Two-drug combination for most‡ (usually thiazide-type diuretic and ACEI or ARB or -blocker or CCB).
Other antihypertensive drugs (diuretics, ACEI, ARB, -blocker or CCB) as needed.*Treatment determined by highest BP category.*Treatment determined by highest BP category.
††Treat patients with chronic kidney disease or diabetes to BP goal of <130/80 mm Hg. Treat patients with chronic kidney disease or diabetes to BP goal of <130/80 mm Hg. ‡‡Initial combined therapy should be used cautiously in those at risk for orthostatic hypotension.Initial combined therapy should be used cautiously in those at risk for orthostatic hypotension.ARB=angiotensin-II receptor blocker; CCB=calcium-channel blocker.ARB=angiotensin-II receptor blocker; CCB=calcium-channel blocker.Chobanian et al. Chobanian et al. JAMAJAMA. 2003;289:2560-2572.. 2003;289:2560-2572.

Not at Goal Blood Pressure (<140/90 mm Hg) Not at Goal Blood Pressure (<140/90 mm Hg) (<130/80 mm Hg for those with diabetes or chronic kidney disease)(<130/80 mm Hg for those with diabetes or chronic kidney disease)
Initial Drug Choices
Drug(s) for the compelling indications
Other antihypertensive drugs (diuretic, ACEI, ARB, BB, CCB)
as needed
With Compelling Indications
Lifestyle Modifications
Not at Goal Blood Pressure
Optimize dosages or add additional drugs until goal blood pressure is achieved
Consider consultation with hypertension specialist
Stage 2 Hypertension (SBP 160 or DBP 100 mm Hg)
2-drug combination for most (usually thiazide-type diuretic and ACEI, ARB, BB, or CCB)
Stage 1 Hypertension(SBP 140-159 or DBP 90-99 mm Hg)
Thiazide-type diuretics for most May consider ACEI, ARB, BB, CCB,
or combination
Without Compelling Indications
JNC 7 Algorithm for Treatment of Hypertension
Chobanian et al. Chobanian et al. JAMAJAMA. 2003;289:2560-2572.. 2003;289:2560-2572.

Not at Goal Blood Pressure
Algorithm for Treatment of Hypertension
Begin or Continue Lifestyle Modifications
• Lose weight• Limit alcohol• Increase physical
activity• Reduce Sodium
• Maintain potassium, calcium, magnesium
• Stop smoking• Reduce saturated fat,
cholesterol

Laboratory Tests Recommended Before Initiating Therapy
• Urinalysis
• Complete blood count
• Blood chemistry (potassium, sodium, creatinine, and fasting glucose)
• Lipid profile
• 12-lead electrocardiogram

Physical Examination
• Blood pressure readings (2 or more)
• Height, weight, and waist circumference
• Funduscopic examination
• Examination of the neck, heart, lungs, abdomen, and extremities
• S4 IMPORTANT!
• Neurological assessment

Examples of IdentifiableCauses of Hypertension
• Renovascular disease
• Renal parenchymal disease
• Polycystic kidneys
• Aortic coarctation
• Pheochromocytoma
• Primary aldosteronism
• Cushing syndrome
• Hyperparathyroidism
• Exogenous causes

Blood Pressure & Lifestyle
Blood Pressure is highly sensitive to weight loss: 5 - 10# weight loss will often control BP
Dietary Approaches: DASH (SBP 11 DBP 8)6 servings of fruits / vegetableslow sodium (no added salt) low to no alcoholhigh calcium, low fat
NEJM 2001;344:3-9 www.nhlbi.nih.gov/health/public/heart/hbp/dash

Sodium Recommendations
No Added Salt (2400 mg/day)Hypertension, impaired liver function, cardiovascular disease, cardiac failure, and acute and chronic renal failure.
1000 mg* (45 mEq)Cirrhosis of the liver, pulmonary edema, moderate to severe cardiac failure, acute and chronic liver failure.
*For short term use only due to decreased palatability and adherence.

Pharmacologic Treatment
• Decreases cardiovascular morbidity and mortality based on randomized controlled trials.
• Protects against stroke, coronary events, heart failure, progression of renal disease, progression to more severe hypertension, and all-cause mortality.

Initial Drug Choices*Uncomplicated• Diuretics• -blockersWhen other compelling reasons
(or others are contraindicated):• ACE or Calcium Blocker
Algorithm for Treatment ofHypertension
*Based on randomized controlled trials.

Initial Drug Choices*
Algorithm for Treatment of Hypertension (continued)
Compelling Indications • Heart failure
– ACE inhibitors– Diuretics
• Myocardial infarction -blockers (non-ISA)– ACE inhibitors (with systolic dysfunction)
• Diabetes mellitus (type 1) with proteinuria– ACE inhibitors
• Isolated systolic hypertension (older persons) – Diuretics preferred– Long-acting dihydropyridine calcium antagonists
*Based on randomized controlled trials.

Initial Drug Choices
Specific indications for the following drugs:
Algorithm for Treatment ofHypertension (continued)
• ACE inhibitors
• Angiotensin II receptor
blockers
• -blockers
• --blockers
• -blockers
• Calcium antagonists
• Diuretics

Specific Drug Indications
• Angina
– -blockers
– Calcium blockers
• Atrial tachycardia and fibrillation
– -blockers
– Non-dihydropyridine calcium antagonists
Some antihypertensive drugs may have favorable effects on co-morbid conditions:
•Heart failure
–Carvedilol
–Losartan
•Myocardial infarction
–Diltiazem
–Verapamil

Specific Indications (continued)
• Cyclosporine-induced hypertension– Calcium blockers
• Diabetes mellitus (1 and 2) with proteinuria– ACE inhibitors (preferred)– Calcium blockers
• Diabetes mellitus (type 2)– Low-dose diuretics
•Dyslipidemia-blockers
•Prostatism (benign prostatic hyperplasia)
-blockers•Renal insufficiency (caution in renovascular hypertension and creatinine 3 mg/dL
- ACE inhibitors
Some antihypertensive drugs may have favorable effects on comorbid conditions:

Patients Undergoing Surgery
• Those not on prior drug therapy may be best treated with cardio-selective-blockers before and after surgery.
• Those with controlled blood pressure should continue medication until surgery and begin as soon after surgery as possible.

Using Thiazide Diuretics
• Can use either HCTZ or chlorthalidone• Use only 12.5 - 25 mg. Daily• Higher doses no more effective, and have more
side effects and electrolyte problems• Do not affect lipids or glucose significantly• Do result in LVH regression• Synergistic with all other classes of medications
– reduce plasma volume

Gout
• Diuretics can increase serum uric acid levels.
• Diuretics should be avoided in patients with gout.
• Diuretic-induced hyperuricemia does not require treatment in the absence of gout or urate stones.

Using ACE Inhibitors
• Patients with:– Diabetes Mellitus– Nephropathy / Albuminuria– Post- MI– Congestive Heart Failure
• Once daily (except captopril)• Use ARB if cough develops• Use with care if hyperkalemia / CRF

Angiotensin Receptor Blocker and Hypertension
LIFE Trial:• Losartan vs. Atenolol (w / HCTZ if needed) for
9193 patients: Hypertension aged 55-80 years• BP decrease 28/9 mmHg both groups• CVD mortality*: 8.7 vs 16.9 (46% reduction)• Stroke*: 10.6 vs 18.9 (40% reduction)• New DM*: 12.6 vs 20.1 (38% reduction)• Total Mortality*: 21.2 vs 30.2 (54% reduction)
* per 1000 patient-yrs JAMA 2002;288:1491

Uses of Calcium Blockers
• Isolated Systolic HTN / Elderly
• African Americans w/better response
• CHD – Angina
• HTN – resistant – especially with a diuretic
• Exercise induced HTN
• Peripheral arterial disease
• Migraine + HTN

Calcium Blockers
A calcium blocker is not a calcium blocker:• AV node inhibitors / modest vasodilators:
– Verapamil– Diltiazem
• Vasodilators: Dihydropyridines– Amlodipine (Norvasc)– Felodipine (Plendil)*Nifedipine: also negative iontrope / adrenergic

Not at Goal Blood Pressure (< 140/90 mm Hg)
No response or troublesome side effects
Inadequate response but well tolerated
Substitute another drug from different class
Add second agent from different class (diuretic
if not already used)
Initial Drug Choices
Algorithm for Treatment ofHypertension

Causes for InadequateResponse to Drug Therapy
• Nonadherence to therapy / lifestyle
• Alcohol use
• Volume overload
• ***Failure to add a diuretic***
• Drug-related causes
• Non-steroidal anti-inflammatories
• Identifiable causes of hypertension

Overview
• Epidemiology • Clinical Trials and Trends
– “All things old become new again”
• Management Guidelines– Compelling reasons for treatment– Management based on patient problems and pharmacology
• Patient Adherence

Guidelines for ImprovingAdherence to Therapy
• Close follow-up 4 – 6 weeks
• Prescribe long-acting / once daily medications
• Adjust therapy to minimize adverse affects
• Use synergistic medications
• Utilize other health professionals
• Consider using nurse case management
• Involve the patient in self-care

Advantages of Self-Measurement
• Identifies “white-coat hypertension”
• Assesses response to medication
• Improves adherence to treatment
• Potentially reduces costs
• May confirm HTN to patient and may provide lower readings than those recorded in clinic

Thank you!
Questions?

Additional Slides

A population-wide strategy to
reduce overall blood pressure by
only a few mm Hg could affect
overall cardiovascular morbidity
and mortality as much as or more
than treatment alone.
A Population-Wide Strategy

Lifestyle Modifications
For Prevention and Management
• Lose weight if overweight.
• Limit alcohol intake.
• Increase aerobic physical activity.
• Reduce sodium intake.
• DASH diet*
For Overall and Cardiovascular Health
• Maintain adequate intake of calcium and magnesium.
• Stop smoking.
• Reduce dietary saturated fat and cholesterol.
• Increase fruits/vegetables/fiber and healthy oils

Children and Adolescents
• Blood pressure at 95th or higher percentile is considered elevated.
• Lifestyle modifications should be recommended.
• Drug therapy should be prescribed for higher levels of blood pressure.
• Attempts should be made to determine other causes of high blood pressure and other cardiovascular risk factors.

95th Percentile of Blood Pressure by Selected Ages and Height in Girls
SBP/DBP (mm Hg)
Age 50th Percentile forHeight
75th Percentile forHeight
1 104/58 105/59
6 111/73 112/73
12 123/80 124/81
17 129/84 130/85

95th Percentile of Blood Pressure by Selected Ages and Height in Boys
SBP/DBP (mm Hg)
Age 50th Percentile forHeight
75th Percentile forHeight
1 102/57 104/58
6 114/74 115/75
12 123/81 125/82
17 136/87 138/88

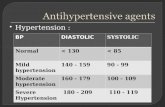
Classification of Blood Pressure for Adults
CategorySBP
(mm Hg)DBP
(mm Hg)
Optimal < 120 and < 80
Normal < 130 and < 85
High-normal 130-139 or 85-89
Hypertension Stage 1 Stage 2 Stage 3
140-159160-179 180
ororor
90-99100-109 110
When SBP and DBP fall into different categories, use the higher category.