
Hypertension and Peripheral Vascular...
72
Hypertension and Hypertension and Peripheral Vascular Disease Peripheral Vascular Disease Week 39 Week 39
Transcript of Hypertension and Peripheral Vascular...

Hypertension and Hypertension and Peripheral Vascular DiseasePeripheral Vascular Disease
Week 39Week 39
HypertensionHypertension
Resting BP consistently >140 Resting BP consistently >140 systolic or >90 diastolicsystolic or >90 diastolic

EpidemiologyEpidemiology 74.5 million people over age 2074.5 million people over age 20 One in three adultsOne in three adults 30% do not know they are hypertensive30% do not know they are hypertensive Twice as frequent in blacks than in whitesTwice as frequent in blacks than in whites In 2006 the death rates per 100,000 population In 2006 the death rates per 100,000 population
from high blood pressure were 15.6 for white from high blood pressure were 15.6 for white males, 51.1 for black males, 14.3 for white males, 51.1 for black males, 14.3 for white females and 37.7 for black females. females and 37.7 for black females.

TypesTypes
Primary (essential) hypertensionPrimary (essential) hypertensionSecondary hypertensionSecondary hypertension

Primary HypertensionPrimary Hypertension 85 - 90% of hypertensives85 - 90% of hypertensives IdiopathicIdiopathic More common in blacks or with positive More common in blacks or with positive
family historyfamily history Worsened by increased sodium intake, Worsened by increased sodium intake,
stress, obesity, oral contraceptive use, or stress, obesity, oral contraceptive use, or tobacco usetobacco use
Cannot be curedCannot be cured

Risk FactorsRisk Factors ModifiableModifiable
• SmokingSmoking• ObesityObesity• StressStress• DyslipidemiaDyslipidemia• AtherosclerosisAtherosclerosis• Sedentary life styleSedentary life style
Non-ModifiableNon-Modifiable• AgeAge• Family HistoryFamily History• DiabetesDiabetes

Signs/SymptomsSigns/Symptoms Primary hypertension is Primary hypertension is asymptomaticasymptomatic
until complications developuntil complications develop Signs/Symptoms are Signs/Symptoms are non-specificnon-specific• Result from target organ involvementResult from target organ involvement
Dizziness, flushed face, headache, fatigue, Dizziness, flushed face, headache, fatigue, epistaxis, nervousness are epistaxis, nervousness are notnot caused by caused by uncomplicated hypertension.uncomplicated hypertension.

Secondary HypertensionSecondary Hypertension 10 - 15% of hypertensives10 - 15% of hypertensives Increased BP secondary to another disease Increased BP secondary to another disease
processprocess Causes:Causes:• Renal vascular or parenchymal diseaseRenal vascular or parenchymal disease• Adrenal gland diseaseAdrenal gland disease• Thyroid gland diseaseThyroid gland disease• Aortic coarctationAortic coarctation• Neurological disordersNeurological disorders
Small number curable with surgerySmall number curable with surgery

Hypertension PathologyHypertension Pathology
Increased BP Increased BP →→ inflammation, sclerosis of inflammation, sclerosis of arteriolar walls arteriolar walls →→ narrowing of vessels narrowing of vessels →→ decreased blood flow to major organsdecreased blood flow to major organs
Left ventricular overwork Left ventricular overwork →→ hypertrophy, CHFhypertrophy, CHF
Nephrosclerosis Nephrosclerosis →→ renal insufficiency, renal insufficiency, failurefailure

Hypertension PathologyHypertension Pathology
Coronary atherosclerosis Coronary atherosclerosis →→ AMI AMI Cerebral atherosclerosis Cerebral atherosclerosis →→ CVA CVA Aortic atherosclerosis Aortic atherosclerosis →→ Aortic Aortic
aneurysmaneurysm Retinal hemorrhage Retinal hemorrhage →→ Blindness Blindness

DiagnosisDiagnosis
Repeat findings of BP< 140/90Repeat findings of BP< 140/90Patient historyPatient history• Lifestyle and risk factorsLifestyle and risk factors• Physical effects of HTN Physical effects of HTN • EKGEKG• Blood studiesBlood studies• CXRCXR

HTN Medical ManagementHTN Medical Management
Life style modificationLife style modification• Weight lossWeight loss• Increased aerobic activityIncreased aerobic activity• Reduced sodium intakeReduced sodium intake• Stop smokingStop smoking• Limit alcohol intakeLimit alcohol intake• Relaxation, stress reductionRelaxation, stress reduction

HTN Medical ManagementHTN Medical Management
MedicationsMedications• DiureticsDiuretics• Beta blockersBeta blockers• Calcium antagonistsCalcium antagonists• Angiotensin converting enzyme Angiotensin converting enzyme
inhibitorsinhibitors• Angiotensin Receptor antagonistsAngiotensin Receptor antagonists

Other Antihypertensive AgentsOther Antihypertensive Agents
Central Adrenergic BlockersCentral Adrenergic BlockersAlpha adrenergic Receptor blockersAlpha adrenergic Receptor blockersDirect vasodilatorsDirect vasodilators

HTN Medical ManagementHTN Medical Management
Medical management prevents or Medical management prevents or forestalls all complicationsforestalls all complications
Patients Patients mustmust remain on drug remain on drug therapy to control BPtherapy to control BP

Categories of HypertensionCategories of Hypertension Hypertensive Emergency (Crisis)Hypertensive Emergency (Crisis)• acute acute BP with sx/sx of end-organ injury BP with sx/sx of end-organ injury
Hypertensive UrgencyHypertensive Urgency• sustained DBP > 115 mm Hg w/o evidence of end-sustained DBP > 115 mm Hg w/o evidence of end-
organ injuryorgan injury Mild HypertensionMild Hypertension• DBP > 90 but < 115 mm Hg w/o symptomsDBP > 90 but < 115 mm Hg w/o symptoms
Transient HypertensionTransient Hypertension• elevated due to an unrelated underlying conditionelevated due to an unrelated underlying condition
Hypertensive CrisisHypertensive Crisis
Acute life-threatening increase Acute life-threatening increase in BPin BP
Usually exceeds 200/130Usually exceeds 200/130

CausesCauses Sudden withdrawal of anti-hypertensivesSudden withdrawal of anti-hypertensives Increased salt intakeIncreased salt intake Abnormal renal functionAbnormal renal function Increase in sympathetic toneIncrease in sympathetic tone• StressStress• DrugsDrugs
Drug interactionsDrug interactions• Monoamine oxidase inhibitorsMonoamine oxidase inhibitors
Toxemia of pregnancyToxemia of pregnancy

Signs/SymptomsSigns/Symptoms
Restlessness, Restlessness, confusion, AMSconfusion, AMS
Vision disturbancesVision disturbances Severe headacheSevere headache Nausea, vomitingNausea, vomiting
SeizuresSeizures Focal neurologic Focal neurologic
deficitsdeficits Chest painChest pain DyspneaDyspnea Pulmonary edemaPulmonary edema

Hypertensive Crisis Can CauseHypertensive Crisis Can Cause
CVACVA CHFCHF Pulmonary edemaPulmonary edema Angina pectorisAngina pectoris AMIAMI Aortic dissectionAortic dissection

Hypertensive Crisis ManagementHypertensive Crisis Management
Avoid crashing BP to hypotensive Avoid crashing BP to hypotensive or normotensive levels!or normotensive levels!
Ischemia of vital organs may Ischemia of vital organs may result!result!

DASH dietDASH diet Dietary approaches to Stop HypertensionDietary approaches to Stop Hypertension High intake of:High intake of:
• Fruits and vegetablesFruits and vegetables• Low fat dairy productsLow fat dairy products• Whole grainsWhole grains• NutsNuts• Poultry and fishPoultry and fish• Potassium, magnesium, calciumPotassium, magnesium, calcium• Protein and fiberProtein and fiber
Restrict intake of:Restrict intake of:• Saturated fat, total fat, cholesterolSaturated fat, total fat, cholesterol• Red meatRed meat• Sugared drinksSugared drinks• Salt and sodiumSalt and sodium

SyncopeSyncope
Sudden, temporary loss of Sudden, temporary loss of consciousness caused by consciousness caused by
inadequate cerebral perfusioninadequate cerebral perfusion
Vasovagal SyncopeVasovagal Syncope Simple fainting occurring when uprightSimple fainting occurring when upright Increased vagal tone leads to peripheral Increased vagal tone leads to peripheral
vasodilation, bradycardia which lead to: vasodilation, bradycardia which lead to: • Decreased cardiac outputDecreased cardiac output• Decreased cerebral perfusionDecreased cerebral perfusion
CausesCauses• Fright, trauma, painFright, trauma, pain• Pressure on carotid sinus (tight collar, Pressure on carotid sinus (tight collar,
shaving)shaving)

Cardiogenic SyncopeCardiogenic Syncope
Paroxysmal Tachyarrhythmias (atrial or Paroxysmal Tachyarrhythmias (atrial or ventricular)ventricular)
BradyarrhythmiasBradyarrhythmias• Stokes-Adams attackStokes-Adams attack
Valvular diseaseValvular disease• especially aortic stenosisespecially aortic stenosis
Can occur in any positionCan occur in any position

Postural SyncopePostural Syncope
Due to decreased BP on Due to decreased BP on standing or sitting upstanding or sitting up
Orthostatic hypotensionOrthostatic hypotension

Postural SyncopePostural Syncope Drugs - usually antihypertensivesDrugs - usually antihypertensives• DiureticsDiuretics• VasodilatorsVasodilators• Beta-blockersBeta-blockers
Volume depletionVolume depletion• Acute hemorrhageAcute hemorrhage• Vomiting or diarrheaVomiting or diarrhea• Excessive diuretic useExcessive diuretic use• Protracted sweatingProtracted sweating
Neuropathic diseases - diabetesNeuropathic diseases - diabetes

Syncope HistorySyncope History What were you doing when you fainted?What were you doing when you fainted? Did you have any warning symptoms?Did you have any warning symptoms? Have you fainted before? Have you fainted before? Under what circumstances?Under what circumstances? Any history of cardiac disease?Any history of cardiac disease? Any medications?Any medications? Any other past medical history?Any other past medical history?

Syncope ManagementSyncope Management Supine position - possibly elevate lower Supine position - possibly elevate lower
extremitiesextremities• Do not sit up or move to semi-sitting Do not sit up or move to semi-sitting
position quicklyposition quickly Airway Airway Loosen tight clothingLoosen tight clothing

Syncope ManagementSyncope Management
Vital signs, Focused Hx & Physical examVital signs, Focused Hx & Physical exam• Assess for injuries sustained in fallAssess for injuries sustained in fall• Attempt to identify causeAttempt to identify cause
Based on history/physicalBased on history/physical• ECG MonitorECG Monitor• Blood glucose checkBlood glucose check• Vascular accessVascular access
Peripheral Vascular DiseasePeripheral Vascular Disease
Peripheral Atherosclerotic DiseasePeripheral Atherosclerotic DiseaseDeep Vein ThrombophlebitisDeep Vein Thrombophlebitis
Varicose VeinsVaricose Veins

Peripheral Vascular DisordersPeripheral Vascular Disorders Ischemia-lack of Ischemia-lack of
blood supply to meet blood supply to meet the needs of the the needs of the tissue.tissue.
Causes of IschemiaCauses of Ischemia• vasoconstrictionvasoconstriction• occlusion of lumen occlusion of lumen
of the artery due to:of the artery due to:
Atherosclerosis (fatty Atherosclerosis (fatty deposits) deposits)
Thrombosis/blood Thrombosis/blood clot/embolismclot/embolism• s/s = coldness, s/s = coldness,
pallor, or rubor pallor, or rubor (redness), (redness), cyanosis cyanosis (blueness)(blueness)
• pain, changes in pain, changes in skin or nailsskin or nails

Age Related changesAge Related changes
ArteriosclerosisArteriosclerosisSlowed heart rateSlowed heart rate Increased arrhythmiasIncreased arrhythmiasDecreased stroke volumeDecreased stroke volumeLowered ability to adapt to changesLowered ability to adapt to changes

Peripheral Arterial Occlusive Peripheral Arterial Occlusive DiseaseDisease
AKA: atherosclerosis obliterans, arterial AKA: atherosclerosis obliterans, arterial insufficiency, peripheral vascular diseaseinsufficiency, peripheral vascular disease
Characterized by pathologic changes in Characterized by pathologic changes in the arteriesthe arteries
Common sites for occlusion: distal Common sites for occlusion: distal superficial femoral and popliteal arteriessuperficial femoral and popliteal arteries
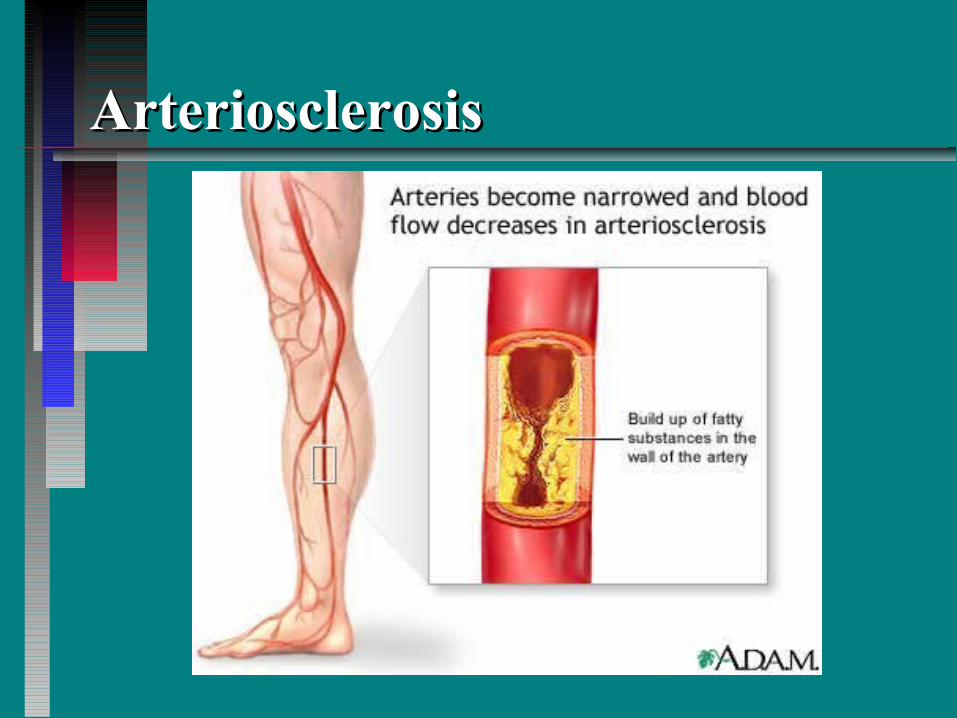
ArteriosclerosisArteriosclerosis

Peripheral AtherosclerosisPeripheral Atherosclerosis
Gradual, progressive diseaseGradual, progressive disease Common in diabeticsCommon in diabetics Thin, shiny skinThin, shiny skin Loss of hair on extremitiesLoss of hair on extremities Ulcers, gangrene may developUlcers, gangrene may develop
Peripheral AtherosclerosisPeripheral Atherosclerosis
Intermittent ClaudicationIntermittent Claudication• Deficient blood supply in exercising Deficient blood supply in exercising
musclemuscle• Pain, aching, cramps, weaknessPain, aching, cramps, weakness• Occurs in calf, thigh, hip, buttocks on Occurs in calf, thigh, hip, buttocks on
walkingwalking• Relieved by rest (2 - 5 minutes)Relieved by rest (2 - 5 minutes)

Peripheral AtherosclerosisPeripheral Atherosclerosis Acute Arterial OcclusionAcute Arterial Occlusion• Sudden blockage by embolism, plaque, Sudden blockage by embolism, plaque,
thrombusthrombus• Can result from vessel traumaCan result from vessel trauma• The 5 Ps of acute occlusionThe 5 Ps of acute occlusion
– PPain, worsening over several hoursain, worsening over several hours– PPallor, poikilothermy (cool to touch)allor, poikilothermy (cool to touch)– PPulselessnessulselessness– PParesthesias, loss of sensationaresthesias, loss of sensation– PParalysisaralysis

Physical Assessment of PVDPhysical Assessment of PVD
Arterial disease:Arterial disease:• acute acute
pain,intermittent pain,intermittent claudication (pain claudication (pain increases with increases with exercise, relieved exercise, relieved with rest), hair loss with rest), hair loss distant with distant with occlusion, thick occlusion, thick brittle nailsbrittle nails
• Paresthesia, pallor Paresthesia, pallor when limb elevated, when limb elevated, rubor when limb rubor when limb dependent(down), dependent(down), skin temp cold, skin temp cold, diminished/weak/or diminished/weak/or absent pulses, no absent pulses, no edema, but ulcers edema, but ulcers in distal areas, foot, in distal areas, foot, toes, ankles, calvestoes, ankles, calves

Deep Vein ThrombophlebitisDeep Vein Thrombophlebitis Inflammation of lower extremities, pelvic Inflammation of lower extremities, pelvic
veins with clot formationveins with clot formation Usually begins with calf veinsUsually begins with calf veins Precipitating factorsPrecipitating factors• Injury to venous endotheliumInjury to venous endothelium• HypercoagulabilityHypercoagulability• Reduced blood flow (venous stasis)Reduced blood flow (venous stasis)

DVT: Risk factorsDVT: Risk factors Bed restBed rest Surgery under anesthesia if >40Surgery under anesthesia if >40 Leg trauma resulting in immobilization Leg trauma resulting in immobilization
or castsor casts Previous venous insufficiencyPrevious venous insufficiency ObesityObesity Use of oral contraceptivesUse of oral contraceptives malignancymalignancy

Deep Vein ThrombophlebitisDeep Vein Thrombophlebitis Signs/SymptomsSigns/Symptoms• May be asymptomaticMay be asymptomatic• Pain, tendernessPain, tenderness• Fever, chills, malaiseFever, chills, malaise• Edema, warmth, bluish-red colorEdema, warmth, bluish-red color• Pain on ankle dorsiflexion during straight Pain on ankle dorsiflexion during straight
leg lifting (Homan’s sign)leg lifting (Homan’s sign)• Palpable “cord” in calfPalpable “cord” in calf
– clotted veinsclotted veins

Deep Vein ThrombophlebitisDeep Vein Thrombophlebitis
May progress to pulmonary May progress to pulmonary embolism!!!embolism!!!
Thromboangiitis obliteransThromboangiitis obliterans AKA Buerger’s diseaseAKA Buerger’s disease An inflammatory thrombotic disorder of An inflammatory thrombotic disorder of
arteries and veinsarteries and veins Not an atherosclerotic processNot an atherosclerotic process Unknown etiologyUnknown etiology Occurs only in smokersOccurs only in smokers Signs and symptoms: intermittent claudication, Signs and symptoms: intermittent claudication,
rest pain, changes in skin color or temperature, rest pain, changes in skin color or temperature, cold sensitivity, ulceration, gangrenecold sensitivity, ulceration, gangrene

TX-management of Buerger’s TX-management of Buerger’s DiseaseDisease
No tobacco , avoid factors cause vasoconstrictionNo tobacco , avoid factors cause vasoconstriction
Avoid becoming chilled, wear warm socks, boots, gloves, Avoid becoming chilled, wear warm socks, boots, gloves, warm water baths warm water baths
Avoid prolonged standing- job changes? Nursing?Avoid prolonged standing- job changes? Nursing?
Avoid injury/infectionAvoid injury/infection
exercising to stimulate circulation, however, as long as it doesn’t cause painexercising to stimulate circulation, however, as long as it doesn’t cause pain
Buerger-Allen exercises-Buerger-Allen exercises-
Do not keep legs elevated-ischemiaDo not keep legs elevated-ischemia
vasodilators/anti-vasodilators/anti-
coagulants may helpcoagulants may help

Buerger-Allen exercisesBuerger-Allen exercises
Elevate feet/legs till feet blanch(whitish), then lowering them till turn red, then resting legs/feet in a horizontal position.Elevate feet/legs till feet blanch(whitish), then lowering them till turn red, then resting legs/feet in a horizontal position.
Client performs exercises lying in bed or on sofa.Client performs exercises lying in bed or on sofa.
Dr. tells client how often to perform themDr. tells client how often to perform them
The patient is instructed to watch the changes in The patient is instructed to watch the changes in color blanching indicates inadequate blood color blanching indicates inadequate blood supply-maintaining this position could harm supply-maintaining this position could harm tissues (death)tissues (death)
May instead walk, foot exercises help tooMay instead walk, foot exercises help too

Raynaud's DiseaseRaynaud's Disease
Intermittent constriction of Intermittent constriction of arteriolesarterioles
Coldness, pain, pallorColdness, pain, pallorEtiology unknownEtiology unknownUsually women 16- 40Usually women 16- 40Aggravated by stressAggravated by stress

Varicose VeinsVaricose Veins
Dilated, elongated, tortuous Dilated, elongated, tortuous superficial veins usually in superficial veins usually in
lower extremitieslower extremities
Varicose VeinsVaricose Veins CausesCauses• Congenital weakness/absence of Congenital weakness/absence of
venous valvesvenous valves• Congenital weakness of venous wallsCongenital weakness of venous walls• Diseases of venous system (Deep Diseases of venous system (Deep
thrombophlebitis)thrombophlebitis)• Prolonged venostasis (pregnancy, Prolonged venostasis (pregnancy,
standing)standing)

Varicose VeinsVaricose Veins
Signs/SymptomsSigns/Symptoms• May be asymptomaticMay be asymptomatic• Feeling of fatigue, heavinessFeeling of fatigue, heaviness• Cramps at nightCramps at night• Orthostatic edemaOrthostatic edema• Ulcer formationUlcer formation
Varicose VeinsVaricose Veins
Rupture may cause severe Rupture may cause severe bleeding bleeding
Control with elevation and Control with elevation and direct pressuredirect pressure

Pulmonary Embolism
Pathophysiology• Pulmonary artery blocked• Blood:
– Does not pass alveoli– Does not exchange gases

Causes
Blood clots = most common causeVirchow’s Triad
• Venous stasis – bed rest, immobility, casts, CHF
• Thrombophlebitis – vessel wall damage• Hypercoagulability – Birth control pills,
especially with smoking

Causes
AirAmniotic fluidFat particles
• Long bone fracture – more quickly splinted, less chance of fat emboli
Particulates from substance abuse

Signs/Symptoms
Small Emboli• Dyspnea• Tachycardia• Tachypnea

Signs/Symptoms
Larger Emboli• Respiratory difficulty• Pleuritic pain• Pleural rub• Coughing• Hemoptysis• Localized Wheezing

Signs/Symptoms
Very Large Emboli• Respiratory distress• Central chest pain• Distended neck veins• Acute right heart failure• Shock• Cardiac arrest

Signs/Symptoms
There are NO findings specific to pulmonary embolism
Nursing AssessmentNursing Assessment
Chief complaint and history of Chief complaint and history of illnessillness
Past medical historyPast medical historyFamily historyFamily history

Physical ExaminationPhysical Examination
InspectionInspectionCapillary refillCapillary refillPalpatePalpateAuscultateAuscultate

Grading EdemaGrading Edema 1: trace, 2mm- slight indent, normal contour1: trace, 2mm- slight indent, normal contour
+2: moderate, 4mm- lasts longer than +1, fairly normal +2: moderate, 4mm- lasts longer than +1, fairly normal contourcontour
+3: deep, 6mm- remains several seconds after pressing, +3: deep, 6mm- remains several seconds after pressing, obvious swellingobvious swelling
+4: very deep, 8mm+- remains for prolonged period +4: very deep, 8mm+- remains for prolonged period (possibly minutes), gross swelling(possibly minutes), gross swelling
* There is also Brawny edema in which fluid can no * There is also Brawny edema in which fluid can no longer be displaced, hence, no pitting. longer be displaced, hence, no pitting.

Diagnostic Tests and ProceduresDiagnostic Tests and Procedures
UltrasonographyUltrasonographyPressure measurementsPressure measurementsTreadmill testTreadmill testAngiographyAngiography

Therapeutic measuresTherapeutic measures ExerciseExercise Stress managementStress management Pain managementPain management Smoking cessationSmoking cessation Anti-embolism stockingsAnti-embolism stockings SCDsSCDs PositioningPositioning ThermographyThermography

Invasive therapeuticsInvasive therapeutics
EmbolectomyEmbolectomyPCTAPCTAEndarterectomyEndarterectomySypmathectomySypmathectomyVein ligation and strippingVein ligation and strippingSclerotherapySclerotherapy

AneurysmsAneurysms
An aneurysm is an abnormal An aneurysm is an abnormal widening or ballooning of a portion widening or ballooning of a portion of an artery due to weakness in the of an artery due to weakness in the wall of the blood vesselwall of the blood vessel


Signs and symptoms vary with Signs and symptoms vary with locationlocation
May be detected during routine May be detected during routine physical exam or x-rayphysical exam or x-ray
ComplicationsComplicationsDiagnosisDiagnosis

Venous InsufficiencyVenous Insufficiency
Long standing Long standing pressure damages pressure damages veins and valveveins and valve
Venous pressure Venous pressure causes edemacauses edema
RBCs leak into RBCs leak into issue causing issue causing brown color brown color

LymphangitisLymphangitis
Inflammation of lymphatic channelsInflammation of lymphatic channelsPrimary characteristic is Primary characteristic is
enlargement of lymph nodes with enlargement of lymph nodes with tendernesstenderness
Treatment: antibioticsTreatment: antibiotics

Case StudyCase Study
Mr. Sparks is a 62 year old white Mr. Sparks is a 62 year old white male. He comes into your ED male. He comes into your ED complaining of chest pain he says is complaining of chest pain he says is probably just “something he ate.”probably just “something he ate.”
What do you do? What assessments What do you do? What assessments do you make?do you make?


Case StudyCase Study
Mr. Dingleberry is admitted to the Mr. Dingleberry is admitted to the hospital with fever, headache and joint hospital with fever, headache and joint pain. During your physical assessment pain. During your physical assessment you note petechiae on his mouth and legs. you note petechiae on his mouth and legs.
Reading his medical history you note that Reading his medical history you note that he had rheumatic fever as a child, as well he had rheumatic fever as a child, as well as orthopedic surgery five years ago. as orthopedic surgery five years ago.


















