Hypersensitivity
38
HYPERSENSITIVITY HYPERSENSITIVITY Injurious consequences in the sensitised host Injurious consequences in the sensitised host following contact with the specific antigens following contact with the specific antigens due to exaggerated response to them, leads to due to exaggerated response to them, leads to tissue damage, disease or death tissue damage, disease or death Antigens are of no concern, Host is concerned Antigens are of no concern, Host is concerned Allergy & Atopy Allergy & Atopy Sensitising or priming dose & shocking dose Sensitising or priming dose & shocking dose Classification Classification : Based on time required : Based on time required - - Immediate Hypersensitivity Immediate Hypersensitivity :- Appears :- Appears and recedes rapidly, Induced by Ags by any and recedes rapidly, Induced by Ags by any route, Ab mediated, Passively transferred with route, Ab mediated, Passively transferred with serum, desensitisation easy and short lived serum, desensitisation easy and short lived - - Delayed Hypersensitivity Delayed Hypersensitivity :- Appears :- Appears slowly, lasts longer, Ag or haptens slowly, lasts longer, Ag or haptens intradermally or with adjuvants or skin intradermally or with adjuvants or skin contact, Cell mediated response, Transferred contact, Cell mediated response, Transferred with T cells or TF, Desensitisation difficult with T cells or TF, Desensitisation difficult
-
Upload
shafayet5hossain -
Category
Education
-
view
15 -
download
6
description
Transcript of Hypersensitivity

HYPERSENSITIVITYHYPERSENSITIVITY Injurious consequences in the sensitised host Injurious consequences in the sensitised host following contact with the specific antigens due to following contact with the specific antigens due to exaggerated response to them, leads to tissue damage, exaggerated response to them, leads to tissue damage, disease or deathdisease or death Antigens are of no concern, Host is concernedAntigens are of no concern, Host is concerned Allergy & AtopyAllergy & Atopy Sensitising or priming dose & shocking doseSensitising or priming dose & shocking dose ClassificationClassification : Based on time required : Based on time required
- - Immediate HypersensitivityImmediate Hypersensitivity :- Appears and :- Appears and recedes rapidly, Induced by Ags by any route, Ab recedes rapidly, Induced by Ags by any route, Ab mediated, Passively transferred with serum, mediated, Passively transferred with serum, desensitisation easy and short liveddesensitisation easy and short lived
- - Delayed HypersensitivityDelayed Hypersensitivity :- Appears slowly, :- Appears slowly, lasts longer, Ag or haptens intradermally or with lasts longer, Ag or haptens intradermally or with adjuvants or skin contact, Cell mediated response, adjuvants or skin contact, Cell mediated response, Transferred with T cells or TF, Desensitisation difficult Transferred with T cells or TF, Desensitisation difficult but long lastingbut long lasting

Coombs & GellCoombs & Gell (1963)- Based on mechanism & (1963)- Based on mechanism & pathogenesispathogenesis
1. 1. Type IType I : : IgEIgE mediatedmediated - Anaphylaxis- Anaphylaxis- Atopy- Atopy
2. 2. Type IIType II : : Cytotoxic /Cytotoxic / - Haemolytic Anaemia- Haemolytic AnaemiaCytolyticCytolytic - Agranulocytosis- Agranulocytosis- Thrombocytopenia- Thrombocytopenia
3. 3. Type IIIType III : : Immune complexImmune complex - Arthus reaction- Arthus reaction- Serum sickness- Serum sickness
4. 4. Type IVType IV : : Delayed HSDelayed HS - Tuberculin- Tuberculin- Contact dermatitis- Contact dermatitis
5. 5. Type VType V : : Varient of Type IIVarient of Type II, Cells in combination , Cells in combination with Ab cause stimulation instead of damage with Ab cause stimulation instead of damage Eg : long acting thyroid stimulator (LATS)Eg : long acting thyroid stimulator (LATS)

TYPE - ITYPE - I- - AnaphylaxisAnaphylaxis :- Acute, potentially fatal, systemic form :- Acute, potentially fatal, systemic form- - AtopyAtopy :- Chronic, nonfatal, localised form :- Chronic, nonfatal, localised form
ANAPHYLAXISANAPHYLAXIS(ana = without, phylaxis = protection), Richet (1902)(ana = without, phylaxis = protection), Richet (1902)
Experiment on dog with toxic extract of sea anemonesExperiment on dog with toxic extract of sea anemones Theoblad- Smith phenomenonTheoblad- Smith phenomenon Factors effectingFactors effecting :- Route of stimulation, Interval :- Route of stimulation, Interval
between sensitisng and shocking dose, species variation between sensitisng and shocking dose, species variation and susceptibility to anaphylaxis, shock organsand susceptibility to anaphylaxis, shock organs
Anaphylaxis in humanAnaphylaxis in human :- Very rare, Symptoms begin :- Very rare, Symptoms begin with itching of scalp and tongue, flushing of skin over the with itching of scalp and tongue, flushing of skin over the body, bronchial spasm, nausa, vomitting, abdominal pain body, bronchial spasm, nausa, vomitting, abdominal pain and diarrhoea, Acute hypotension, loss of consciousness and diarrhoea, Acute hypotension, loss of consciousness & death& death
Common with injections of antibiotics, drugs & Insect Common with injections of antibiotics, drugs & Insect stings, Treated with Adrelanile :0.5 ml 1 in 1000 soln, S/C stings, Treated with Adrelanile :0.5 ml 1 in 1000 soln, S/C or I/M, dose can be repeated till 2 ml over 15 minor I/M, dose can be repeated till 2 ml over 15 min

CUTANEOUS ANAPHYLAXISCUTANEOUS ANAPHYLAXIS :- :- Very small shocking dose of Ag intradermally cause Very small shocking dose of Ag intradermally cause
local wheal –and-flare response (local anaphylaxis)local wheal –and-flare response (local anaphylaxis) Useful in testing for hypersensitivity and identifying Useful in testing for hypersensitivity and identifying
the allergen responsible in atopic diseasesthe allergen responsible in atopic diseases
PASSIVE CUTANEOUS ANAPHYLAXISPASSIVE CUTANEOUS ANAPHYLAXIS Ovary (1952), extremely sensitive in-vivo method for Ovary (1952), extremely sensitive in-vivo method for
detection of antibodiesdetection of antibodies A small volume of Ab injected Id into a normal animal, A small volume of Ab injected Id into a normal animal,
if Ag along with a dye, Evans blue is injected IV 4- 24 if Ag along with a dye, Evans blue is injected IV 4- 24 hours after, blueing at the site of ID takes place due hours after, blueing at the site of ID takes place due to vasodlataion and increased capillary permeabilityto vasodlataion and increased capillary permeability
ANAPHYLAXIS IN VITROANAPHYLAXIS IN VITRO Isolated tissues from sensitised guinea pigs, uterus Isolated tissues from sensitised guinea pigs, uterus
muscle strips held in water bath of ringer’s soln will muscle strips held in water bath of ringer’s soln will contract vigorously on addition of specific Ag- Schultz contract vigorously on addition of specific Ag- Schultz - Dale phenomenon- Dale phenomenon

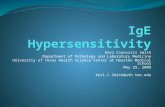
Skin testing by intradermal injection of allergens into the forearm. In this individual, a weal and flare response developed within a few minutes at the site where grass was injected, indicatingthat the individual is allergic to grass.

MECHANISM OF ANAPHYLAXISMECHANISM OF ANAPHYLAXIS Cytotropic IgE bound to surface receptors ( FcER ) on Cytotropic IgE bound to surface receptors ( FcER ) on
Mast cells and Basophils by Fc end, Following Mast cells and Basophils by Fc end, Following exposure to shocking dose, Ag combine with the cell exposure to shocking dose, Ag combine with the cell bound IgE, bridging gap between adjacent Ab, this bound IgE, bridging gap between adjacent Ab, this cross linking increases he permeability of the cells to cross linking increases he permeability of the cells to Ca ions and leads to degranulation with release of Ca ions and leads to degranulation with release of biologically active substances in granulesbiologically active substances in granules
Anaphylactic manifestations are de to Anaphylactic manifestations are de to pharmacological mediators :- pharmacological mediators :-
1. 1. Primary mediatorsPrimary mediators :- Histamine, Seratonin, :- Histamine, Seratonin, Eosnophil & Neutrophil chemotactic factors, Heparin Eosnophil & Neutrophil chemotactic factors, Heparin & Enzyme mediators (Proteases & Hydrolases)& Enzyme mediators (Proteases & Hydrolases)
2. 2. Secondary mediatorsSecondary mediators :- Prostaglandins, :- Prostaglandins, leukotrenes, Platelet activating factors & other leukotrenes, Platelet activating factors & other cytokines , IL- 3,4,5,6 & GM-CSFcytokines , IL- 3,4,5,6 & GM-CSF


TYPE – I HYPER SENSITIVITY



ATOPYATOPY Atopy = Out of place or strangeness – Coca (1923)Atopy = Out of place or strangeness – Coca (1923) Atopens : Inhalants, Ingestants, contact allergensAtopens : Inhalants, Ingestants, contact allergens Occur as natural familial hypersensitivities in humanOccur as natural familial hypersensitivities in human Mediated by IgE, reagin Abs, develops spontaneously, Mediated by IgE, reagin Abs, develops spontaneously,
cannot induce artificiallycannot induce artificially Predisposition is genetically determined – To produce Predisposition is genetically determined – To produce
IgE in unusually large quantitiesIgE in unusually large quantities Characteristics of IgE antibodiesCharacteristics of IgE antibodies Prausnitz- Kustner (PK) reactionPrausnitz- Kustner (PK) reaction Deficiency of IgA predispose to atopyDeficiency of IgA predispose to atopy Symptoms due to release of phamacologically active Symptoms due to release of phamacologically active
substances following combination of Ag with cell fixed substances following combination of Ag with cell fixed IgEIgE
Conjunctivitis, Rhinitis, GI symptoms, dermatitis & Conjunctivitis, Rhinitis, GI symptoms, dermatitis & UrticariaUrticaria


ALLERGIC RHINITIS
The most common atopic disorder, affecting 10% of the population, is allergic rhinitis, commonly known as hay fever.
This results from the reaction of airborne allergens with sensitized mast cells in the conjunctivae and nasal mucosa to induce the release of pharmacologically active mediators from mast cells; these mediators then cause localized vasodilation and increased capillary permeability.
The symptoms include watery exudation of the conjunctivae, nasal mucosa, and upper respiratory tract, as well as sneezing and coughing.

ASTHMA Airborne or blood-borne allergens, such as pollens, dust,
fumes, insect products, or viral antigens, trigger an asthmatic attack (allergic asthma); in other cases, an asthmatic attack can be induced by exercise or cold, apparently independently of allergen stimulation (intrinsic asthma).
Like hay fever, asthma is triggered by degranulation of mast cells with release of mediators, but instead of occurring in the nasal mucosa, the reaction develops in the lower respiratory tract. The resulting contraction of the bronchial smooth muscles leads to bronchoconstriction. Airway edema, mucus secretion, and inflammation contribute to the bronchial constriction and to airway obstruction.
Asthmatic patients may have abnormal levels of receptors for neuropeptides. For example, asthmatic patients have been reported to have increased expression of receptors for substance P, a peptide that contracts smooth muscles, and decreased expression of receptors for vasoactive intestinal peptide, which relaxes smooth muscles.

The asthmatic response can be divided into early and late responses. The early response occurs within minutes of allergen exposure and primarily involves histamine, leukotrienes (LTC4), and prostaglandin (PGD2). The effects of these mediators lead to bronchoconstriction, vasodilation, and some buildup of mucus.
The late response occurs hours later and involves additional mediators, including IL-4, IL-5, IL-16,TNF-, eosinophil chemotactic factor (ECF), and platelet-activating factor (PAF). The effects of these mediators is to increase endothelial cell adhesion as well as to recruit inflammatory cells, including eosinophils &neutrophils, into the bronchial tissue. The neutrophils &eosinophils cause significant tissue injury by releasing toxic enzymes, oxygen radicals, and cytokines.
These events lead to occlusion of the bronchial lumen with mucus, proteins, and cellular debris; sloughing of the epithelium; thickening of the basement membrane; edema; and hypertrophy of the bronchial smooth muscles. A mucus plug adheres to the bronchial wall and plug contains clusters of detached epithelial-cell fragments, eosinophils, some neutrophils, and spirals of bronchial tissue known as Curschmann’s spirals.

FOOD ALLERGIESFOOD ALLERGIES Various foods also can induce localized anaphylaxis in Various foods also can induce localized anaphylaxis in
allergic individuals. Allergen crosslinking of IgE on mast allergic individuals. Allergen crosslinking of IgE on mast cells along the upper or lower gastrointestinal tract can cells along the upper or lower gastrointestinal tract can induce localized smooth-muscle contraction and induce localized smooth-muscle contraction and vasodilation and symptoms as vomiting or diarrhea. vasodilation and symptoms as vomiting or diarrhea.
Mast-cell degranulation along the gut increases the Mast-cell degranulation along the gut increases the permeability of mucous membranes, so that the allergen permeability of mucous membranes, so that the allergen enters the bloodstream. Various symptoms can ensue, enters the bloodstream. Various symptoms can ensue, depending on where the allergen is deposited. depending on where the allergen is deposited.
Some individuals develop asthmatic attacks after Some individuals develop asthmatic attacks after ingesting certain foods. Others develop atopic urticaria, ingesting certain foods. Others develop atopic urticaria, commonly known as hives, when a food allergen is commonly known as hives, when a food allergen is carried to sensitized mast cells in the skin, causing carried to sensitized mast cells in the skin, causing swollen (edematous) red (erythematous) eruptions; this swollen (edematous) red (erythematous) eruptions; this is the wheal and flare response, or P-K reaction is the wheal and flare response, or P-K reaction

ATOPIC DERMATITISATOPIC DERMATITIS
Atopic dermatitis (allergic eczema) is an Atopic dermatitis (allergic eczema) is an inflammatory disease of skin that is inflammatory disease of skin that is frequently associated with a family history frequently associated with a family history of atopy. The disease is observed most of atopy. The disease is observed most frequently in young children, often frequently in young children, often developing during infancy. developing during infancy.
Serum IgE levels are often elevated. The Serum IgE levels are often elevated. The allergic individual develops skin eruptions allergic individual develops skin eruptions that are erythematous and filled with pus. that are erythematous and filled with pus. Unlike a delayed-type hypersensitive Unlike a delayed-type hypersensitive reaction, which involves TH1 cells, the skin reaction, which involves TH1 cells, the skin lesions in atopic dermatitis have TH2 cells lesions in atopic dermatitis have TH2 cells and an increased number of eosinophils and an increased number of eosinophils

TYPE - IITYPE - II Cytolytic or cytotoxic IgG or IgM Abs with antigenic Cytolytic or cytotoxic IgG or IgM Abs with antigenic
determinants on cell surface determinants on cell surface Lysis of RBC’s : Haemolytic anaemia & Haemolytic Lysis of RBC’s : Haemolytic anaemia & Haemolytic
diseasedisease Complement mediated lysis of RBC’s, Leucocytes & Complement mediated lysis of RBC’s, Leucocytes &
PlateletsPlatelets Hemolytic anaemia, Agranulocytosis & Hemolytic anaemia, Agranulocytosis &
Thrombocytopenic purpuraThrombocytopenic purpura In some reactions antibody combines with cell surface In some reactions antibody combines with cell surface
receptors and disrupts normal function like receptors and disrupts normal function like uncontrolled activation (eg: Long acting thyroid uncontrolled activation (eg: Long acting thyroid stimulator in Graves’ disease ), or by blocking stimulator in Graves’ disease ), or by blocking (Myasthenia gravis) (Myasthenia gravis)

Transfusion Reactions Are Type II Transfusion Reactions Are Type II ReactionsReactions A large number of proteins and glycoproteins on the membrane A large number of proteins and glycoproteins on the membrane
of RBC’s are encoded by different genes, each has a number of of RBC’s are encoded by different genes, each has a number of alternative alleles. An individual possessing one allelic form of a alternative alleles. An individual possessing one allelic form of a blood-group antigen can recognize other allelic forms on blood-group antigen can recognize other allelic forms on transfused blood as foreign and mount an antibody response. transfused blood as foreign and mount an antibody response.
In some cases, the antibodies have already been induced by In some cases, the antibodies have already been induced by natural exposure to similar antigenic determinants on a variety natural exposure to similar antigenic determinants on a variety of microorganisms (PAMP’s) present in the normal flora of the of microorganisms (PAMP’s) present in the normal flora of the gut. gut.
Antibodies to the A, B, and O antigens, isohemagglutinins, are of Antibodies to the A, B, and O antigens, isohemagglutinins, are of the IgM class. An individual with blood type A, recognizes B-like the IgM class. An individual with blood type A, recognizes B-like epitopes on intestinal microorganisms and produces epitopes on intestinal microorganisms and produces isohemagglutinins to the B-like epitopes. This same individual isohemagglutinins to the B-like epitopes. This same individual does not respond to A-like epitopes on the same intestinal does not respond to A-like epitopes on the same intestinal microorganisms because these A-like epitopes are too similar to microorganisms because these A-like epitopes are too similar to self Ags. If a type A individual is transfused with blood containing self Ags. If a type A individual is transfused with blood containing type B cells, a type B cells, a transfusion reactiontransfusion reaction occurs in which the anti-B occurs in which the anti-B isohemagglutinins bind to the B blood cells and mediate their isohemagglutinins bind to the B blood cells and mediate their destruction by means of complement-mediated lysis. destruction by means of complement-mediated lysis.
Antibodies to other blood-group antigens may result from Antibodies to other blood-group antigens may result from repeated blood transfusions because minor allelic differences in repeated blood transfusions because minor allelic differences in these antigens can stimulate antibody production. These these antigens can stimulate antibody production. These antibodies are usually of the IgG class. antibodies are usually of the IgG class.

The clinical manifestations of The clinical manifestations of
transfusion reactionstransfusion reactions Massive intravascular hemolysisMassive intravascular hemolysis of the transfused of the transfused
red blood cells by antibody plus complement. These red blood cells by antibody plus complement. These manifestations may be either immediate or delayed. manifestations may be either immediate or delayed.
Reactions that begin immediately are associated Reactions that begin immediately are associated with with ABO blood-group incompatibilitiesABO blood-group incompatibilities, which lead , which lead to complement mediated lysis triggered by the IgM to complement mediated lysis triggered by the IgM isohemagglutinins. Within hours, free hemoglobin isohemagglutinins. Within hours, free hemoglobin can be detected in the plasma; it is filtered through can be detected in the plasma; it is filtered through the kidneys, resulting in the kidneys, resulting in hemoglobinuriahemoglobinuria. Some of . Some of the hemoglobin gets converted to the hemoglobin gets converted to bilirubinbilirubin, which at , which at high levels is toxic. Typical symptoms include fever, high levels is toxic. Typical symptoms include fever, chills, nausea, clotting within blood vessels, pain in chills, nausea, clotting within blood vessels, pain in the lower back, and hemoglobin in the urinethe lower back, and hemoglobin in the urine
TreatmentTreatment involves prompt involves prompt termination of the termination of the transfusiontransfusion and and maintenance of urine flowmaintenance of urine flow with a with a diureticdiuretic, because the accumulation of hemoglobin in , because the accumulation of hemoglobin in the kidney can cause acute tubular necrosis. the kidney can cause acute tubular necrosis.

Delayed hemolytic transfusion reactionsDelayed hemolytic transfusion reactions generally generally occur in individuals who have received occur in individuals who have received repeated repeated transfusionstransfusions of ABO-compatible blood that is of ABO-compatible blood that is incompatible for other blood group antigens. The incompatible for other blood group antigens. The reactions develop between 2 and 6 days after reactions develop between 2 and 6 days after transfusion, reflecting the secondary nature of these transfusion, reflecting the secondary nature of these reactions. reactions.
The transfused blood induces clonal selection and The transfused blood induces clonal selection and production of production of IgGIgG against a variety of blood-group against a variety of blood-group membrane antigens, most commonly membrane antigens, most commonly Rh, Kidd, Kell, Rh, Kidd, Kell, and Duffyand Duffy. The predominant isotype involved in these . The predominant isotype involved in these reactions is IgG, which is less effective than IgM in reactions is IgG, which is less effective than IgM in activating complement. activating complement.
For this reason, For this reason, complement-mediated lysiscomplement-mediated lysis of the of the transfused red blood cells is transfused red blood cells is incompleteincomplete, and many of , and many of the transfused cells are destroyed at extravascular the transfused cells are destroyed at extravascular sites by agglutination, opsonization, and subsequent sites by agglutination, opsonization, and subsequent phagocytosis by macrophages. phagocytosis by macrophages. SymptomsSymptoms include include fever, low hemoglobin, increased bilirubin, mild fever, low hemoglobin, increased bilirubin, mild jaundice, and anemia. Free hemoglobin is usually not jaundice, and anemia. Free hemoglobin is usually not detected in the plasma or urine in these reactions detected in the plasma or urine in these reactions because RBC destruction occurs in extravascular sites.because RBC destruction occurs in extravascular sites.

Hemolytic Disease of the Newborn Is Hemolytic Disease of the Newborn Is Caused by Type II ReactionsCaused by Type II Reactions Hemolytic disease of the newborn develops when Hemolytic disease of the newborn develops when
maternal IgG antibodies specific for fetal blood-group maternal IgG antibodies specific for fetal blood-group antigens cross the placenta and destroy fetal RBC’s. The antigens cross the placenta and destroy fetal RBC’s. The consequences of such transfer can be minor, serious, or consequences of such transfer can be minor, serious, or lethal. Severe hemolytic disease of the newborn, called lethal. Severe hemolytic disease of the newborn, called erythroblastosis fetaliserythroblastosis fetalis, , most commonly develops most commonly develops when an Rh+ fetus expresses an when an Rh+ fetus expresses an Rh antigenRh antigen on its on its blood cells that the Rh– mother does not express blood cells that the Rh– mother does not express
During her first pregnancy with an Rh+ fetus, an Rh– During her first pregnancy with an Rh+ fetus, an Rh– woman is usually not exposed to enough fetal red blood woman is usually not exposed to enough fetal red blood cells to activate her Rh-specific B cells. At the time of cells to activate her Rh-specific B cells. At the time of delivery, however, separation of the placenta from the delivery, however, separation of the placenta from the uterine wall allows larger amounts of fetal umbilical-cord uterine wall allows larger amounts of fetal umbilical-cord blood to enter the mother’s circulation. These fetal RBC’s blood to enter the mother’s circulation. These fetal RBC’s activate Rh-specific B cells, resulting in production of activate Rh-specific B cells, resulting in production of Rh-Rh-specific plasma cellsspecific plasma cells and and memory B cellsmemory B cells in the mother. in the mother. The The secreted IgM antibodysecreted IgM antibody clears the Rh+ fetal red cells clears the Rh+ fetal red cells from the mother’s circulation, but the from the mother’s circulation, but the memory cells memory cells remainremain, a threat to any subsequent pregnancy with an , a threat to any subsequent pregnancy with an Rh+ fetus. Rh+ fetus.

Activation of these memory cells in a Activation of these memory cells in a subsequent subsequent pregnancypregnancy results in the formation of IgG anti-Rh results in the formation of IgG anti-Rh antibodies, which antibodies, which cross the placentacross the placenta and and damage the damage the fetal RBC’sfetal RBC’s. Mild to severe anemia can develop in the . Mild to severe anemia can develop in the fetus, sometimes with fatal consequences. In addition, fetus, sometimes with fatal consequences. In addition, conversion of hemoglobinconversion of hemoglobin to to bilirubinbilirubin cause threat to cause threat to the newborn because the lipid-soluble bilirubin may the newborn because the lipid-soluble bilirubin may accumulate in the brain and cause accumulate in the brain and cause brain damagebrain damage..
Hemolytic disease of the newborn caused by Rh Hemolytic disease of the newborn caused by Rh incompatibility in a subsequent pregnancy can be incompatibility in a subsequent pregnancy can be almost entirely prevented by administering antibodies almost entirely prevented by administering antibodies called called RhogamRhogam against the Rh antigen to the mother against the Rh antigen to the mother within 24–48 h after the first delivery. They bind to any within 24–48 h after the first delivery. They bind to any fetal RBC’s that enter the mother’s circulation at the fetal RBC’s that enter the mother’s circulation at the time of delivery and facilitate their clearance time of delivery and facilitate their clearance before B-before B-cell activationcell activation and production of memory-cells. and production of memory-cells.
In a subsequent pregnancy with an Rh+ fetus, a In a subsequent pregnancy with an Rh+ fetus, a mother who has been treated with Rhogam is unlikely mother who has been treated with Rhogam is unlikely to produce IgG anti-Rh antibodies; thus, the fetus is to produce IgG anti-Rh antibodies; thus, the fetus is protected from the damage that would occur when protected from the damage that would occur when these antibodies crossed the placenta.these antibodies crossed the placenta.

Diagnosis & Treatment of Diagnosis & Treatment of
erythroblastosis fetaliserythroblastosis fetalis Testing maternal serum at intervals during pregnancy Testing maternal serum at intervals during pregnancy
for antibodies to the Rh antigen. for antibodies to the Rh antigen. A rise in the titerA rise in the titer of of these antibodies as pregnancy progresses indicates these antibodies as pregnancy progresses indicates that the mother has been exposed to Rh antigens and that the mother has been exposed to Rh antigens and is producing increasing amounts of antibody. The is producing increasing amounts of antibody. The presence of maternal IgG on the surface of fetal red presence of maternal IgG on the surface of fetal red blood cells can be detected by a blood cells can be detected by a Coombs testCoombs test. .
For a severe reaction, the fetus can be given an For a severe reaction, the fetus can be given an intrauterine blood-exchange transfusionintrauterine blood-exchange transfusion to replace to replace fetal Rh+ red blood cells with Rh– cells. These fetal Rh+ red blood cells with Rh– cells. These transfusions are given every 10–21 days until delivery. transfusions are given every 10–21 days until delivery. Primarily to Primarily to removeremove bilirubinbilirubin; the infant is also ; the infant is also exposed to low levels of UV lightexposed to low levels of UV light to break down the to break down the bilirubin and prevent cerebral damage bilirubin and prevent cerebral damage
The mother can also be treated during the pregnancy The mother can also be treated during the pregnancy by by plasmapheresisplasmapheresis

The majority of cases (65%) of hemolytic disease of the The majority of cases (65%) of hemolytic disease of the newborn have minor consequences and are caused by newborn have minor consequences and are caused by ABO blood-group incompatibility between the mother ABO blood-group incompatibility between the mother and fetus. Type A or B fetuses carried by and fetus. Type A or B fetuses carried by type O type O mothersmothers most commonly develop these reactions. most commonly develop these reactions.
A type O mother is most likely to develop A type O mother is most likely to develop IgG antibodyIgG antibody to the to the A or B blood-group antigensA or B blood-group antigens either through either through natural exposure or through exposure to fetal blood-natural exposure or through exposure to fetal blood-group A or B antigens in successive pregnancies.group A or B antigens in successive pregnancies.
Usually the fetal anemia resulting from this Usually the fetal anemia resulting from this incompatibility is incompatibility is mildmild; the major clinical manifestation ; the major clinical manifestation is a is a slight elevation of bilirubinslight elevation of bilirubin, with jaundice. , with jaundice. Depending on the severity of the anemia and jaundice, Depending on the severity of the anemia and jaundice, a blood-exchange transfusion may be required in these a blood-exchange transfusion may be required in these infants. In general the reaction is mild, however, and infants. In general the reaction is mild, however, and exposure of the infant to exposure of the infant to low levels of UV lightlow levels of UV light is is enough to break down the bilirubin and avoid cerebral enough to break down the bilirubin and avoid cerebral damage. damage.
Hemolytic disease of new born due Hemolytic disease of new born due to ABO blood-group incompatibilityto ABO blood-group incompatibility


Drug-Induced Hemolytic Anemia Is a Type II Response
Certain antibiotics (e.g., penicillin, cephalosporin, and streptomycin) can adsorb nonspecifically to proteins on RBC membranes, forming a complex similar to a hapten-carrier complex.
In some patients, such drug-protein complexes induce formation of antibodies, which then bind to the adsorbed drug on red blood cells, inducing complement mediated lysis and thus progressive anemia.
When the drug is withdrawn, the hemolytic anemia disappears. Penicillin is notable in that it can induce all four types of hypersensitivity with various clinical manifestations


TYPE - IIITYPE - III Arthus reactionArthus reaction : : Arthus (1903), Local manifestation of Arthus (1903), Local manifestation of
generalised HSgeneralised HS In rabbits injected repeatedly with s/c normal horse serum- In rabbits injected repeatedly with s/c normal horse serum-
No local effects initially, but intense local reaction with No local effects initially, but intense local reaction with edema, induration and hemorrhagic necrosis subsequentlyedema, induration and hemorrhagic necrosis subsequently
Tissue damage due to Ag-Ab ppt causing C activation and Tissue damage due to Ag-Ab ppt causing C activation and release of inflammatory molecules – Leads to increased release of inflammatory molecules – Leads to increased vascular permeability and neutrophil infiltration- Leucocyte-vascular permeability and neutrophil infiltration- Leucocyte-platelet thrombi reduce blood supply leads to tissue platelet thrombi reduce blood supply leads to tissue necrosisnecrosis
Farmer’s lung, Hypersensitivity pneumonitisFarmer’s lung, Hypersensitivity pneumonitis
Serum sicknessSerum sickness :- :- Systemic form, Pirquet & Schick (1905)Systemic form, Pirquet & Schick (1905) 7 to 12 days following single injection of diphtheria 7 to 12 days following single injection of diphtheria
antitoxin antitoxin Leads to fever, lymphadenopathy, splenomegaly, arthritis, Leads to fever, lymphadenopathy, splenomegaly, arthritis,
glomerulonephritis, endocarditis, vasculitis, urticarial glomerulonephritis, endocarditis, vasculitis, urticarial rashes, abdominal pain, nausea & vomitingrashes, abdominal pain, nausea & vomiting
Immune complexes deposited on endothelial lining of Immune complexes deposited on endothelial lining of various partsvarious parts

Development of a localized Arthus reaction (type III
hypersensitive reaction). Complement activation initiated by immune complexes (classical pathway) produces complement intermediates that
(1) mediate mast-cell degranulation,
(2) chemotactically attract neutrophils,
(3) stimulate release of lytic enzymes from neutrophils trying to phagocytose C3b-coated immune complexes.

Type III Reactions Can Be Localized Injection of an antigen intradermally or subcutaneously into
an animal that has high levels of circulating antibody specific for that antigen leads to formation of localized immune complexes, which mediate an acute Arthus reaction in 4–8 h.
Microscopic examination of the tissue reveals neutrophils adhering to the vascular endothelium and then migrating into the tissues at the site of immunecomplex deposition. As the reaction develops, localized tissue and vascular damage results in an accumulation of fluid (edema) and red blood cells (erythema) at the site. The severity of the reaction can vary from mild swelling and redness to tissue necrosis.
After an insect bite, a sensitive individual may have a rapid, localized type I reaction at the site. Often, some 4–8 h later, a typical Arthus reaction also develops at the site, with pronounced erythema and edema. Intrapulmonary Arthus-type reactions induced by bacterial spores, fungi, or dried fecal proteins can also cause pneumonitis or alveolitis. They are known by a variety of common names reflecting the source of the antigen. “farmer’s lung” develops after inhalation of thermophilic actinomycetes from moldy hay, and “pigeon fancier’s disease” results from inhalation of a serum protein in dust derived from dried pigeon feces.

Type III Reactions Can Also Be Generalized When large amounts of antigen enter the bloodstream and
bind to antibody, circulating immune complexes can form. If antigen is in excess, small complexes form; because these are not easily cleared by the phagocytic cells, they can cause tissue- damaging type III reactions at various sites.
Within days or weeks after exposure to foreign serum antigens, an individual begins to manifest a combination of symptoms that are called serum sickness. These symptoms include fever, weakness, generalized vasculitis (rashes) with edema and erythema, lymphadenopathy, arthritis, and sometimes glomerulonephritis.
The precise manifestations of serum sickness depend on the quantity of immune complexes formed as well as the overall size of the complexes, which determine the site of their deposition.

The sites of deposition vary but, complexes accumulate in tissues where filtration of plasma occurs. This explains the high incidence of glomerulonephritis (complex deposition in kidney) and vasculitis (in arteries) and arthritis (in synovial joints) caused by serum sickness.
Complexes of antibody with various bacterial, viral & parasitic antigens have been shown to induce a variety of type III hypersensitive reactions, including skin rashes, arthritic symptoms, and glomerulonephritis.
Poststreptococcal glomerulonephritis, develops when circulating complexes of antibody and streptococcal antigens are deposited in the kidney and damage the glomeruli.
A number of autoimmune diseases stem from circulating complexes of antibody with self-proteins, with glycoproteins, or even with DNA. In systemic lupus erythematosus, complexes of DNA and anti-DNA antibodies accumulate in synovial membranes, causing arthritic symptoms, or accumulate on the basement membrane of the kidney, causing progressive kidney damage.

TYPE - IVTYPE - IV Delayed HS, Stimulated by intra cellular microbial infections, Delayed HS, Stimulated by intra cellular microbial infections,
haptens like chemicals applied on skin consist of mixed haptens like chemicals applied on skin consist of mixed cellular reaction involving lymphocytes and macrophagescellular reaction involving lymphocytes and macrophages
Induced by sensitised T cellsInduced by sensitised T cells TUBERCULIN TYPETUBERCULIN TYPE :- Tuberculin test in Tuberculosis :- Tuberculin test in Tuberculosis Injection of tuberculoprotein ID in sensitised individualsInjection of tuberculoprotein ID in sensitised individuals Indurated inflammatory reaction in 48-72 hoursIndurated inflammatory reaction in 48-72 hours CONTACT DERMATITISCONTACT DERMATITIS :- Skin contact with chemicals – :- Skin contact with chemicals –
Metals such as nickel, chromium, Dyes – Picryl chloride, Metals such as nickel, chromium, Dyes – Picryl chloride, Dinitrochlorobenzene, Drugs – Penicillin, toiletriesDinitrochlorobenzene, Drugs – Penicillin, toiletries
More sensitisation if applied over inflamed area or in oily baseMore sensitisation if applied over inflamed area or in oily base Mechanism: Langerhans’ cell capture & present the haptens Mechanism: Langerhans’ cell capture & present the haptens
with tissue proteins and present to T cells- release IFN –g & IL-with tissue proteins and present to T cells- release IFN –g & IL-2 activate macrophages and lymphocytes, IL-4,5 & GM-CSF 2 activate macrophages and lymphocytes, IL-4,5 & GM-CSF leads to tissue damageleads to tissue damage
Patch test : Itching in 4-5 hours, local reaction after 24-48 hrsPatch test : Itching in 4-5 hours, local reaction after 24-48 hrs


Overview of the DTH response. (a) In the sensitization phase after initial contact with antigen (e.g., peptides derived from intracellular bacteria), TH cells proliferate and differentiate into TH1 cells. Cytokines secreted by these T cells are indicated by the dark blue balls.

(b) In the effector phase after subsequent exposure of sensitized TH1 cells to antigen, the TH1 cells secrete a variety of cytokines and chemokines. These factors attract and activate macrophages and other nonspecific inflammatory cells. Activated macrophages are more effective in presenting antigen, thus perpetuating the DTH response, and function as the primary effector cells in this reaction.

A prolonged DTH response can lead to formation ofa granuloma, a nodule-like mass. Lytic enzymes released from activated macrophages in a granuloma can cause extensive tissue damage.