
Hyperfractionated whole abdominal irradiation for stage III ovarian cancer: Salvage radiation...
2
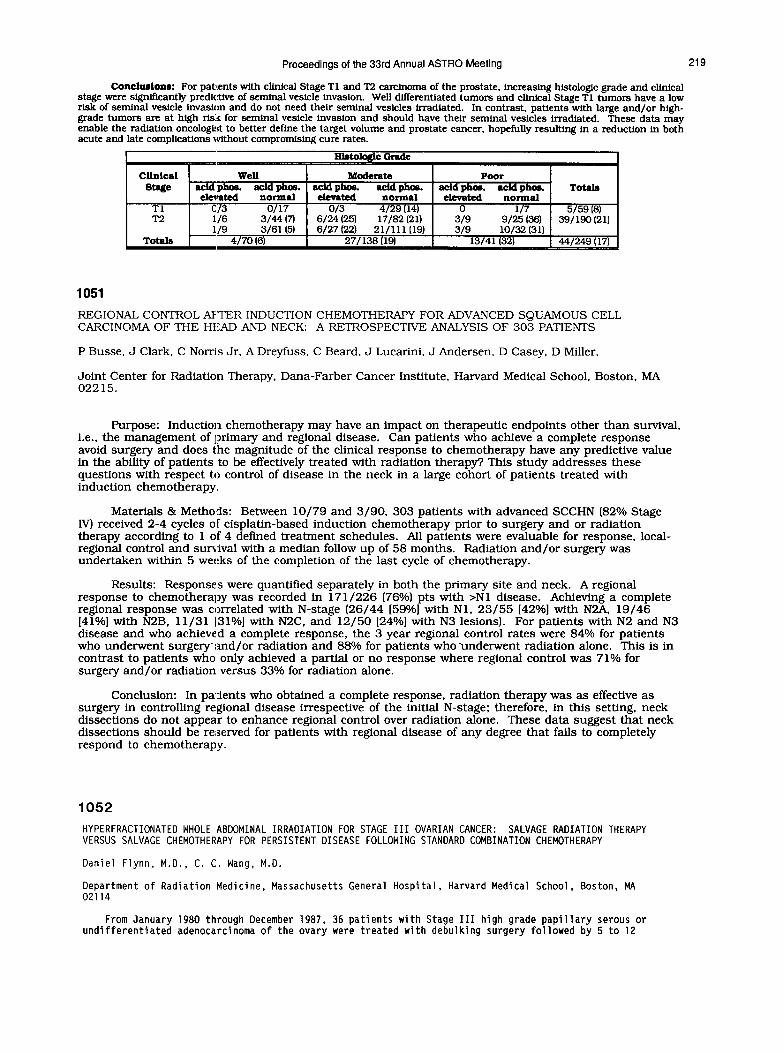
Proceedings of the 3rd Annual ASTRO Meeting 219 Conclartonr: For patients with clinical Stage Tl and T2 carcinoma of the prostate, increasing histologic grade and clinical stage were significantly predictive of seminal vesicle invasion. Well differentiated tumors and clinical Stage Tl tumors have a low risk of semtnal vesicle invasion and do not need their seminal vesicles irradiated. In contrast, patients with large and/or high- grade tumors are at high rlelz for seminal vesicle invasion and should have their seminal vesicles irradiated. These data may enable the radiation oncologist to better define the target volume and prostate cancer, hopefully resulting in a reduction in both acute and late complications without compromising cure rates. 1051 REGIONAL CONTROL AFTER INDUCTION CHEMOTHERAPY FOR ADVANCED SQUAMOUS CELL CARCINOMA OF THE HEAD AND NECK: A RETROSPECTIVE ANALYSIS OF 303 PATIENTS P Busse. J Clark, C Norris Jr, A Dreyfuss, C Beard. J Lucarini. J Andersen, D Casey, D Miller, Joint Center for Radiation Therapy, Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA 02215. Purpose: Induction chemotherapy may have an impact on therapeutic endpoints other than survival, i.e., the management of primary and regional disease. Can patients who achieve a complete response avoid surgery and does the magnitude of the clinical response to chemotherapy have any predictive value in the ability of patients to be effectively treated with radiation therapy? This study addresses these questions with respect to control of disease in the neck in a large cohort of patients treated with induction chemotherapy. Materials & Methods: Between lo/79 and 3/90, 303 patients with advanced SCCHN (82% Stage N) received 2-4 cycles of cisplatin-based induction chemotherapy prior to surgery and or radiation therapy according to 1 of 4 defined treatment schedules. All patients were evaluable for response, local- regional control and sunWal with a median follow up of 58 months. Radiation and/or surgery was undertaken within 5 weeks of the completion of the last cycle of chemotherapy. Results: Responses were quantified separately in both the primary site and neck. A regional response to chemotherapy was recorded in 171/226 (76%) pts with >Nl disease. Achieving a complete regional response was correlated with N-stage (26/44 [59O/6] with Nl, 23/55 [42%] with N2A. 19/46 [410/o] with N2B, 11/31 ]31%] with N2C. and 12/50 [24%] with N3 lesions). For patients with N2 and N3 disease and who achieved a complete response, the 3 year regional control rates were 84% for patients who underwent surgery’and/or radiation and 88% for patients who underwent radiation alone. This is in contrast to patients who only achieved a partial or no response where regional control was 71% for surgery and/or radiation versus 33O/6 for radiation alone. Conclusion: In patients who obtained a complete response, radiation therapy was as effective as surgery in controlling regional disease irrespective of the initial N-stage: therefore, in this setting, neck dissections do not appear to enhance regional control over radiation alone. These data suggest that neck dissections should be reserved for patients with regional disease of any degree that fails to completely respond to chemotherapy. 1052 HYPERFRACTIONATED WHOLE ABDOMINAL IRRADIATION FOR STAGE III OVARIAN CANCER: SALVAGE RADIATION THERAPY VERSUS SALVAGE CHEMOTHERAPY FOR PERSISTENT DISEASE FOLLOWING STANDARD COMBINATION CHEMOTHERAPY Daniel Flynn, M.D., C. C. Wang, M.D. Department of Radiation Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114 From January 1980 through December 1987, 36 patients with Stage III high grade papillary serous or undifferentiated adenocarcinoma of the ovary were treated with debulking surgery followed by 5 to 12
-
Upload
daniel-flynn -
Category
Documents
-
view
213 -
download
1
Transcript of Hyperfractionated whole abdominal irradiation for stage III ovarian cancer: Salvage radiation...
Proceedings of the 3rd Annual ASTRO Meeting 219
Conclartonr: For patients with clinical Stage Tl and T2 carcinoma of the prostate, increasing histologic grade and clinical stage were significantly predictive of seminal vesicle invasion. Well differentiated tumors and clinical Stage Tl tumors have a low risk of semtnal vesicle invasion and do not need their seminal vesicles irradiated. In contrast, patients with large and/or high- grade tumors are at high rlelz for seminal vesicle invasion and should have their seminal vesicles irradiated. These data may enable the radiation oncologist to better define the target volume and prostate cancer, hopefully resulting in a reduction in both acute and late complications without compromising cure rates.
1051 REGIONAL CONTROL AFTER INDUCTION CHEMOTHERAPY FOR ADVANCED SQUAMOUS CELL CARCINOMA OF THE HEAD AND NECK: A RETROSPECTIVE ANALYSIS OF 303 PATIENTS
P Busse. J Clark, C Norris Jr, A Dreyfuss, C Beard. J Lucarini. J Andersen, D Casey, D Miller,
Joint Center for Radiation Therapy, Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA 02215.
Purpose: Induction chemotherapy may have an impact on therapeutic endpoints other than survival, i.e., the management of primary and regional disease. Can patients who achieve a complete response avoid surgery and does the magnitude of the clinical response to chemotherapy have any predictive value in the ability of patients to be effectively treated with radiation therapy? This study addresses these questions with respect to control of disease in the neck in a large cohort of patients treated with induction chemotherapy.
Materials & Methods: Between lo/79 and 3/90, 303 patients with advanced SCCHN (82% Stage N) received 2-4 cycles of cisplatin-based induction chemotherapy prior to surgery and or radiation therapy according to 1 of 4 defined treatment schedules. All patients were evaluable for response, local- regional control and sunWal with a median follow up of 58 months. Radiation and/or surgery was undertaken within 5 weeks of the completion of the last cycle of chemotherapy.
Results: Responses were quantified separately in both the primary site and neck. A regional response to chemotherapy was recorded in 171/226 (76%) pts with >Nl disease. Achieving a complete regional response was correlated with N-stage (26/44 [59O/6] with Nl, 23/55 [42%] with N2A. 19/46 [410/o] with N2B, 11/31 ]31%] with N2C. and 12/50 [24%] with N3 lesions). For patients with N2 and N3 disease and who achieved a complete response, the 3 year regional control rates were 84% for patients who underwent surgery’and/or radiation and 88% for patients who underwent radiation alone. This is in contrast to patients who only achieved a partial or no response where regional control was 71% for surgery and/or radiation versus 33O/6 for radiation alone.
Conclusion: In patients who obtained a complete response, radiation therapy was as effective as surgery in controlling regional disease irrespective of the initial N-stage: therefore, in this setting, neck dissections do not appear to enhance regional control over radiation alone. These data suggest that neck dissections should be reserved for patients with regional disease of any degree that fails to completely respond to chemotherapy.
1052 HYPERFRACTIONATED WHOLE ABDOMINAL IRRADIATION FOR STAGE III OVARIAN CANCER: SALVAGE RADIATION THERAPY VERSUS SALVAGE CHEMOTHERAPY FOR PERSISTENT DISEASE FOLLOWING STANDARD COMBINATION CHEMOTHERAPY
Daniel Flynn, M.D., C. C. Wang, M.D.
Department of Radiation Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114
From January 1980 through December 1987, 36 patients with Stage III high grade papillary serous or undifferentiated adenocarcinoma of the ovary were treated with debulking surgery followed by 5 to 12
220 Radiation Oncology, Biology, Physics Volume 21, Supplement I
cycles of CAP or CHAP chemotherapy. All patients were clinically free of disease following chemotherapy however all had unsuspected persistent disease at second-look laparotomy. Eleven patients were treated for salvage with hyperfractionated whole abdominal irradiation (HWAI). Irradiation was given with 100 cGy bid fractions to 3000 cGy with no liver block and with a PA kidney block for half of the PA treatments. Twenty five patients were treated for salvage with various second line chemotherapy (CTX) modalities. Both the irradiation and chemotherapy groups were matched for stage, histology, grade, primary treatment, initial response, and for second look laparotomy results.
Treatment breaks from irradiation were given due to significant nausea and vomiting (two patients), severe diarrhea (one patient), neutropenia (one patient) with only one patient failing to complete treatment. asymptomatic neutropenia and thrombocytopenia occurred to some degree in all eleven patients with nadirs generally occurred one to two weeks after completing treatment. The mean doses to the kidneys and liver were 2330 cGy and 2970 cGy respectively. Three patients exhibited mild increased creatinine after 6-12 months and three patients exhibited mild increase in liver enzymes but no patient became svmotomatic. In the irradiation arouo there was one subseauent small bowel obstruction (SBO) attributed to the radiation and four patient; were subsequent SBO'associated with massive recurrent tumor. The overall occurrence of SBO following HWAI was no different than that following salvage CTX.
Minimum follow-up was three years. The medial survival following positive second look laparotomy (SLL) based on maximum residual disease after SLL debulking was as follows:
HWAI microscopic: 17.4 months (4 pts) macroscopic: 11.5 months (7 pts)
CTX microscopic: 18.0 months (8 pts) macroscopic: 13.3 months (17 pts)
The two year absolute survival was 27% in the HWAI group (114 micro, 217 macro) and 28% in the second line CTX group (3/B micro, 4117 macro). The overall survival at three years was 14% (5/36) but only one patient is alive without disease at five Years. A durable response to the treatment of high grade stage III tumors that recur is uncommon regardless of the method of salvage treatment.
POSTER NUMBER 1053 HAS BEEN WITHDRAWN
1054
RADIOTHERAPYISSUCCESSFULTREATMENTFORORBITALLYMPHOMA
Melanie Smith, M.D. and Sarah Donaldson, M.D.
Depatimentof Radiation Oncology, Stanford University, Stanford, California, 94305
Purpose: To describe the clinical presentation, treatment technique, outcome and complications in a large single institutional experience using radiotherapy for treatment of orbital lymphoma.
Materials & Methods: Twenty-four patients with lymphoma of the orbii were treated with orbital radiotherapy between 1977 and 1990. Biopsy was obtained in all cases. Patients were staged using the Ann Arbor criteria with chest x-ray, chest and abdominal CT, lymphangiogram, bone marrow biopsy, and orbital CT. Patients with disease localized to the orbiis as well as those with disseminated disease and symptomatic orbiial lesions were treated. Thirty involved eyes were treated. Mean radiotherapy dose was 35.60 Gy, range 28 Gy lo 48 Gy. One patient, prior 10 1978, was treated with orthovoltage. The remainder were treated with complex megavoltage techniques tailored to the disease distribution as visualized by clinical exam and CT scan. Two patients alSo received chemotherapy as part of therr rntlral treatment. Followup ranged from 10 months to 13 years, mean 4 years.
Results: The mean age was 52 years, range 26-71 years. The femalemale ratio 1.51. Sites of involvement were: conjunctiva, 15 patients (5 with bilateral involvement); retroorbii, 4 patients (1 bilateral); conjunctiva and retroorbii, 3 patients; and nasolacrimal region, 2 patients. One patient had a monoclonal atypical infiltrate, while the remainder had a histologic diagnosis of malignant lymphoma: diise small lymphocylic, 12; diffuse small cleaved, 3; diffuse large cell, 2; folliilar mixed, 3; folliiular small cleaved, folliilar and diffuse small cleaved, and undlferentiated. 1 each. Four patients had disease outside the orbii and were staged: IleA. ; IlleA, I; IVA, I‘; IV& 1. Only two local relapses occurred: one distant relapse occurred in the contralateral eye. Al five years, the actuarial freedom from local relapse was 89%, freedom from distant relapse was 74%, freedom from any relapse was 88%, and overall survival was 93%. No relapse occurred beyond five years. Acute complications of treatment were mild and included conjunctival irritation, skin eryihema, and temporary dry eye. Long-term complications included transient cystoid macular edema (I), subcapsular and medical sector cataract formation (2), radiation retinopathy (I), cosmetically signifiini eyelid retraction (2), and dry eye with secondary conjunctivitis (1). Corrected visual acuity was 2OI25 or better in these patients.
Conclusion: Carefully planned radiotherapy with lens shielding is an effective and safe modality in the treatment of orbital lymphoma. The recommended dose for bw grade lesions is 30-35 Gy, and for intermediate or high grade lesions is 36-40 Gy. Although there is a 25% incidence of initial bilateral involvement and the wntralateral eye may be at increased risk of relapse, we dc not recommend chemotherapy in the initial treatment of disease confined to the orbits.


















