Hyperbilirubinemia, Phototherapy, and Childhood Asthma · hyperbilirubinemia and/or phototherapy...
11
ARTICLE Hyperbilirubinemia, Phototherapy, and Childhood Asthma Michael W. Kuzniewicz, MD, MPH, a,b Hamid Niki, MS, a Eileen M. Walsh, RN, MPH, a Charles E. McCulloch, PhD, c Thomas B. Newman, MD, MPH b,c OBJECTIVES: Our aim was to quantify the associations of both hyperbilirubinemia and phototherapy with childhood asthma using a population-based cohort with total serum bilirubin (TSB) levels. METHODS: Retrospective cohort study of infants born at ≥35 weeks’ gestation in the Kaiser Permanente Northern California health system ( n = 109 212) from 2010 to 2014. Cox models were used to estimate hazard ratios (HRs) for a diagnosis of asthma. RESULTS: In the study, 16.7% of infants had a maximum TSB level of ≥ 15 mg/dL, 4.5% of infants had a maximum TSB level of ≥ 18 mg/dL, and 11.5% of infants received phototherapy. Compared with children with a maximum TSB level of 3 to 5.9 mg/L, children with a TSB level of 9 to 11.9 mg/dL, 12 to 14.9 mg/dL, and 15 to 17.9 mg/dL were at an increased risk for asthma (HR: 1.22 [95% confidence interval (CI): 1.11–1.3], HR: 1.18 [95% CI: 1.08–1.29], and HR: 1.30 [95% CI: 1.18–1.43], respectively). Children with a TSB level of ≥ 18 mg/dL were not at an increased risk for asthma (HR: 1.04; 95% CI: 0.90–1.20). In propensity-adjusted analyses, phototherapy was not associated with asthma (HR: 1.07; 95% CI: 0.96 –1.20). CONCLUSIONS: Modest levels of hyperbilirubinemia were associated with an increased risk of asthma, but an association was not seen at higher levels. No dose-response relationship was seen. Using phototherapy to prevent infants from reaching these modest TSB levels is unlikely to be protective against asthma. abstract a Division of Research, Kaiser Permanente, Oakland, California; and Departments of b Pediatrics and c Epidemiology and Biostatistics, University of California, San Francisco, San Francisco, California Dr Kuzniewicz assisted with obtaining funding, supervised data management and the creation of Kaiser Permanente Northern California data sets, analyzed data, and drafted the initial manuscript and revisions; Dr Newman conceptualized, designed, and led efforts to obtain funding for the study and reviewed the manuscript; Mr Niki helped design data analyses, assisted with the interpretation of results, and reviewed and revised multiple drafts of the manuscript; Ms Walsh assisted with data analyses and reviewed and revised the manuscript; Dr McCulloch provided statistical and design consultation, assisted with obtaining funding, and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. DOI: https://doi.org/10.1542/peds.2018-0662 Accepted for publication Jul 11, 2018 Address correspondence to Michael W. Kuzniewicz, MD, MPH, Division of Research, Kaiser Permanente, Office 022R09, 2000 Broadway, Oakland, CA 94612. E-mail: michael.w.kuzniewicz@ kp.org PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2018 by the American Academy of Pediatrics PEDIATRICS Volume 142, number 4, October 2018:e20180662 WHAT’S KNOWN ON THIS SUBJECT: Observational studies have revealed an association between hyperbilirubinemia and/or phototherapy and childhood asthma. In many studies, researchers have only used codes for hyperbilirubinemia or jaundice and have lacked the ability to distinguish between the effects of hyperbilirubinemia and its treatment. WHAT THIS STUDY ADDS: By using actual bilirubin levels, modest levels of hyperbilirubinemia were associated with a slightly increased risk of asthma in a large modern cohort, but an association was not seen at higher levels. Phototherapy did not alter the risk of asthma. To cite: Kuzniewicz MW, Niki H, Walsh EM, et al. Hyperbil- irubinemia, Phototherapy, and Childhood Asthma. Pediatrics. 2018;142(4):e20180662 by guest on March 28, 2020 www.aappublications.org/news Downloaded from
Transcript of Hyperbilirubinemia, Phototherapy, and Childhood Asthma · hyperbilirubinemia and/or phototherapy...

ARTICLE
Hyperbilirubinemia, Phototherapy, and Childhood AsthmaMichael W. Kuzniewicz, MD, MPH, a, b Hamid Niki, MS, a Eileen M. Walsh, RN, MPH, a Charles E. McCulloch, PhD, c Thomas B. Newman, MD, MPHb, c
OBJECTIVES: Our aim was to quantify the associations of both hyperbilirubinemia and phototherapy with childhood asthma using a population-based cohort with total serum bilirubin (TSB) levels.METHODS: Retrospective cohort study of infants born at ≥35 weeks’ gestation in the Kaiser Permanente Northern California health system (n = 109 212) from 2010 to 2014. Cox models were used to estimate hazard ratios (HRs) for a diagnosis of asthma.RESULTS: In the study, 16.7% of infants had a maximum TSB level of ≥15 mg/dL, 4.5% of infants had a maximum TSB level of ≥18 mg/dL, and 11.5% of infants received phototherapy. Compared with children with a maximum TSB level of 3 to 5.9 mg/L, children with a TSB level of 9 to 11.9 mg/dL, 12 to 14.9 mg/dL, and 15 to 17.9 mg/dL were at an increased risk for asthma (HR: 1.22 [95% confidence interval (CI): 1.11–1.3], HR: 1.18 [95% CI: 1.08–1.29], and HR: 1.30 [95% CI: 1.18–1.43], respectively). Children with a TSB level of ≥18 mg/dL were not at an increased risk for asthma (HR: 1.04; 95% CI: 0.90–1.20). In propensity-adjusted analyses, phototherapy was not associated with asthma (HR: 1.07; 95% CI: 0.96–1.20).CONCLUSIONS: Modest levels of hyperbilirubinemia were associated with an increased risk of asthma, but an association was not seen at higher levels. No dose-response relationship was seen. Using phototherapy to prevent infants from reaching these modest TSB levels is unlikely to be protective against asthma.
abstract
aDivision of Research, Kaiser Permanente, Oakland, California; and Departments of bPediatrics and cEpidemiology and Biostatistics, University of California, San Francisco, San Francisco, California
Dr Kuzniewicz assisted with obtaining funding, supervised data management and the creation of Kaiser Permanente Northern California data sets, analyzed data, and drafted the initial manuscript and revisions; Dr Newman conceptualized, designed, and led efforts to obtain funding for the study and reviewed the manuscript; Mr Niki helped design data analyses, assisted with the interpretation of results, and reviewed and revised multiple drafts of the manuscript; Ms Walsh assisted with data analyses and reviewed and revised the manuscript; Dr McCulloch provided statistical and design consultation, assisted with obtaining funding, and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
DOI: https:// doi. org/ 10. 1542/ peds. 2018- 0662
Accepted for publication Jul 11, 2018
Address correspondence to Michael W. Kuzniewicz, MD, MPH, Division of Research, Kaiser Permanente, Office 022R09, 2000 Broadway, Oakland, CA 94612. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2018 by the American Academy of Pediatrics
PEDIATRICS Volume 142, number 4, October 2018:e20180662
WHAT’S KNOWN ON THIS SUBJECT: Observational studies have revealed an association between hyperbilirubinemia and/or phototherapy and childhood asthma. In many studies, researchers have only used codes for hyperbilirubinemia or jaundice and have lacked the ability to distinguish between the effects of hyperbilirubinemia and its treatment.
WHAT THIS STUDY ADDS: By using actual bilirubin levels, modest levels of hyperbilirubinemia were associated with a slightly increased risk of asthma in a large modern cohort, but an association was not seen at higher levels. Phototherapy did not alter the risk of asthma.
To cite: Kuzniewicz MW, Niki H, Walsh EM, et al. Hyperbil-irubinemia, Phototherapy, and Childhood Asthma. Pediatrics. 2018;142(4):e20180662
by guest on March 28, 2020www.aappublications.org/newsDownloaded from

The prevalence of childhood asthma has been increasing worldwide, and asthma is one of the most common childhood diseases, yet much remains to be elucidated concerning its etiology.1 There is clearly a genetic predisposition, and the interaction between the environmental pollutants and/or allergens, inflammatory mediators, and cellular response play a crucial role in its pathogenesis.2 – 6 Reactive oxygen species that are generated by both cellular metabolism and environmental pollutants result in oxidant injury and contribute to the severity and symptom exacerbation of asthma.3, 7, 8
Observational studies have revealed an association between hyperbilirubinemia and/or phototherapy and childhood asthma.9 – 14 Using the Swedish birth registry, Aspberg et al10 first reported an association between a diagnosis of icterus or history of phototherapy and hospitalizations for asthma after 2 years of age (adjusted odds ratio [aOR]: 1.27; 95% confidence interval [CI]: 1.08–1.50). The group confirmed their findings using an outcome of asthma, which was defined by receiving medications for asthma.11 Similarly, a Chinese9 (aOR: 1.64; 95% CI: 1.36–1.98) and Taiwanese study12 (adjusted hazard ratio [HR]: 1.21; 95% CI: 1.15–1.27) revealed an association between a diagnosis of neonatal jaundice and an inpatient or outpatient diagnosis of asthma later in childhood.
None of the authors of these studies analyzed actual bilirubin levels; all relied only on a diagnosis of jaundice.
Because phototherapy is a primary treatment of neonatal jaundice, it is hard to distinguish the effects of phototherapy from those of jaundice. The only study in which actual bilirubin levels were included was an examination of data from the US Collaborative Perinatal Project; subjects were enrolled in 1959–1965, before the use of phototherapy.13
Total serum bilirubin (TSB) levels were obtained on all infants at 36 to 60 hours after birth and repeated 24 hours later if the TSB level was >10 mg/dL. Compared with infants with a maximum TSB level of ≤3 mg/dL, infants with a maximum TSB level as low as 6.1 to 9 mg/dL were more likely to be diagnosed with asthma before age 7 years. Infants with a maximum TSB level of ≥15 mg/dL had the highest increased risk of asthma (aOR: 1.61; 95% CI: 1.04–2.08).
Our objective was to quantify the associations of both hyperbilirubinemia and phototherapy with childhood asthma, controlling for confounding using a large, modern, and population-based cohort and actual TSB levels.
METHODS
Study Design
We performed a retrospective cohort study as an extension of the Late Impact of Getting Hyperbilirubinemia or Phototherapy study.15 – 20 The Institutional Review Boards at Kaiser Permanente Northern California (KPNC) and the University of California, San Francisco, approved the study.
Population
The cohort included infants born at ≥35 weeks’ gestation at KPNC hospitals between January 1, 2010, and December 31, 2014. Only the 11 facilities that were employing universal bilirubin screening with TSB levels before discharge were included. To ensure full ascertainment of bilirubin levels, infants had to remain in the KPNC system during their entire birth hospitalization (n = 126 376). To assess asthma outcomes, we excluded children who did not remain in the health plan for at least 25 months after birth (n = 17 496). We excluded 332 children with no TSB levels.
The final study cohort consisted of 109 212 children.
Predictors
Bilirubin Measurement
From existing KPNC laboratory databases, we obtained all TSB levels from an infant’s first month after birth using previously described methods.21 We excluded any TSB measurements for which a corresponding conjugated or direct bilirubin measurement constituted ≥50% of the TSB level. These infants represent a small and different population of infants and are also excluded from the American Academy of Pediatrics (AAP) guideline.22 TSB levels were obtained before discharge or if clinically indicated. Subsequent TSB testing was done at the discretion of the treating physicians. A bilirubin measurement was performed by using the Vitros BuBc Neonatal Bilirubin assay (Ortho Clinical Diagnostics, Raritan, NJ).23, 24 In May 2012, Ortho Clinical Diagnostics adjusted the calibrator values for Vitros BuBc Slides, 25 so we included an indicator variable for whether the TSB level was obtained before or after recalibration in analyses.
Phototherapy
We classified infants as having received inpatient phototherapy if they had either a phototherapy nursing flow sheet or both a procedure code and an order for phototherapy. Home phototherapy was determined from the KPNC durable medical equipment database.
Additional Covariables
From the KPNC electronic data sources, we abstracted covariates, including maternal age, maternal race and/or ethnicity, infant sex, gestational age, birth weight, 5-minute Apgar score, year, and hospital of birth, and the results of a direct antiglobulin test and glucose-6-phosphate dehydrogenase
KUZNIEWICZ et al2 by guest on March 28, 2020www.aappublications.org/newsDownloaded from

activity, if performed. A maternal history of asthma was defined as 2 asthma diagnoses (International Classification of Diseases, Ninth Revision diagnosis code 493.×) in the mother from any outpatient or inpatient encounter, separated by at least 30 days, occurring within 10 years before the birth of the infant (obtained from the KPNC Virtual Data Warehouse).26 We classified feeding during the birth hospitalization as exclusively breastfed, received 1 formula feeding, or received >1 formula feeding.
Outcomes
An occurrence of asthma was defined as a child having both (1) at least 2 asthma diagnoses from any outpatient or inpatient encounter, separated by at least 30 days, occurring after 2 years of age and (2) at least 2 asthma medication prescriptions in a 12-month period, separated by at least 30 days, prescribed after 2 years of age. Medications that were considered asthma medications were short- or long-acting β-agonists, inhaled corticosteroids, a combination inhaled corticosteroid and long-acting β-agonist, or a montelukast.
Follow-up Time
Length of follow-up varied in this study because some subjects left the KPNC health care system and follow-up began at birth (2010–2014) but ended in 2017 for all subjects. For purposes of quantifying incidence rates and using proportional hazards models, follow-up for each member of the cohort began at either age 2 years and ended at death, at the date when the individual met all criteria for asthma (2 asthma diagnoses and 2 medication prescriptions), or at the last follow-up date, which was defined as the last day of the last calendar month of coverage by the KPNC health plan or the last
encounter date through April 30, 2017, whichever came later.
Statistical Analysis
We calculated crude incidence rates by dividing asthma cases by person years of follow-up, and we calculated CIs for comparing incidence rate ratios (IRRs) using exact binomial calculations. We used Cox proportional hazards models to evaluate the independent associations between hyperbilirubinemia and asthma and phototherapy and asthma, adjusting for potential confounders. We investigated which variables were independently associated with asthma in models that included maximum TSB levels and phototherapy. Covariables with a significance value of P < .05 were included in the final model.
In addition to traditional models, we used a phototherapy propensity score among infants who had a TSB level within 3 mg/dL of the AAP phototherapy threshold, as previously described.16 We categorized propensity scores for phototherapy by decile. In propensity-adjusted analyses we controlled for measured confounding variables by creating a model for the probability of exposure (in this case, phototherapy) and then controlled for that probability. This allowed us to adjust for TSB levels before but not after phototherapy, thus allowing us to investigate whether phototherapy might reduce the risk of asthma by preventing hyperbilirubinemia. We performed all analyses using Stata version 15 (Stata Corp, College Station, TX).
RESULTS
Characteristics of the study cohort by asthma status are shown in Table 1. As expected, African American children, children of mothers with a history of asthma, and infants of lower gestational
age were overrepresented in the asthma group. Infants who were exclusively breastfed during the birth hospitalization were underrepresented in the asthma group. Infants who received phototherapy were overrepresented in the asthma group.
Of the 109 212 children in the cohort, 16.7% (18 205) had a maximum TSB level of ≥15 mg/dL, and 4.7% (4865) had a maximum TSB level of ≥18 mg/dL. Phototherapy was administered to 11.5% (12 533) of the children. The majority of children who were treated received inpatient phototherapy (8.9%), whereas a minority (2.5%) received only home phototherapy. Children were managed for a total of 263 967 person years after age 2 years. The mean age at the last follow-up was 4.4 (SD: 1.5) years. In the study, 4854 (4.4%) children met the criteria for asthma (incidence rate: 18.4 per 1000 person years). The mean age to achieving criteria for an asthma diagnosis was 3.6 (SD: 1.1) years old.
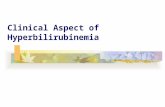
Asthma cases, the cumulative incidence of asthma, the incidence rate, and IRRs by maximum TSB level category are shown in Table 2. Although incidence rates for asthma increased significantly for maximum TSB levels between 9 and 17.9 mg/dL compared with maximum TSB levels between 3 and 5.9 mg/dL, there was not a significant increase in incidence rates for asthma in children with maximum TSB levels of ≥18 mg/dL. Figure 1 includes the asthma incidence rate by maximum TSB level. No clear relationship is present.
For the Cox proportional hazards models, sex, maternal history of asthma, cesarean delivery, birth hospitalization length of stay >7 days, recalibration, race, maternal age, gestational age, birth facility, birth year, and feeding type during the birth hospitalization were included in the final model. In the final model, phototherapy was not associated with asthma (HR: 1.01; 95%
PEDIATRICS Volume 142, number 4, October 2018 3 by guest on March 28, 2020www.aappublications.org/newsDownloaded from

CI: 0.92–1.11; Table 3). Maximum TSB levels between 9 and 17.9 mg/dL were associated with an elevated HR for asthma; however, there was no association between a TSB level of ≥18 mg/dL and asthma. In our cohort, 88% of those who met criteria for an asthma diagnosis, met criteria before 5 years of age. Limiting the
analysis to individuals with at least 5 years of follow-up yielded similar associations with TSB levels. In additional analyses, we separated home phototherapy and inpatient phototherapy. Neither was associated with asthma (HR: 0.98 [95% CI: 0.86–1.16] for inpatient phototherapy; HR: 1.01 [95% CI: 0.85–1.19]
for home phototherapy). Lastly, restricting the model to infants with a positive Coombs test revealed higher TSB levels to be protective.
In the subset of infants with a TSB level within 3 mg/dL of the AAP phototherapy threshold before any treatment with phototherapy (n = 28 290), phototherapy was not associated with childhood asthma (HR: 1.07; 95% CI: 0.96–1.20; controlling for the propensity to receive phototherapy).
DISCUSSION
In a large modern cohort, with TSB levels for all subjects, we found that infants with moderately elevated maximum TSB levels (9–17.9 mg/dL) were more likely to develop asthma later in childhood. This association did not persist for infants with maximum TSB levels of ≥18 mg/dL. We found no association between phototherapy and asthma when adjusting for the maximum TSB level or in analyses when adjusting for a propensity to receive phototherapy.
Although we have confirmed an association between moderately elevated bilirubin levels at birth and the development of asthma later in childhood, the question is if the association is causal. There is undoubtedly consistency because this association has now been seen in diverse populations in Sweden, 10, 11 Taiwan, 12 China, 9 and now in a historic13 and modern cohort in the United States. The strength of the association in the aforementioned studies ranged from aORs of 1.37 to 1.64. The strength of the association in our study was attenuated, which may be secondary to our controlling for other important predicators, such as a history of maternal asthma and the more specific definition of asthma that we used.
Is there any biological plausibility for why hyperbilirubinemia or phototherapy may result in asthma?
KUZNIEWICZ et al4
TABLE 1 Characteristics of the Cohort by Asthma Status
Variable Nonasthma, n (%) Asthma, n (%)
Total 104 358 (100) 4854 (100)Male sex 52 632 (50.4) 3031 (62.4)Race Asian American 22 319 (21.4) 1008 (20.8) African American 6469 (6.2) 552 (11.4) Hispanic 21 197 (20.3) 1117 (23.0) Non-Hispanic white 44 202 (42.4) 1747 (36.0) Other 10 171 (9.7) 430 (8.9)Maternal age, y <20 2803 (2.7) 196 (4.0) 20–29 39 345 (37.3) 1802 (37.1) 30–39 57 174 (54.8) 2626 (54.1) ≥40 5036 (4.8) 230 (4.7)Maternal history of asthma 8548 (8.2) 822 (16.9)Parity 0 30 159 (28.9) 1333 (27.5) 1 38 639 (37.0) 1811 (37.3) ≥1 35 201 (33.7) 1688 (34.8) Unknown 359 (0.3) 22 (0.5)Cesarean delivery 7488 (7.2) 1387 (28.6)SGA (<10th percentile) 4983 (4.8) 261 (5.4)LGA (>90th percentile) 8447 (8.1) 429 (8.8)Gestational age, wk 35 1961 (1.9) 135 (2.8) 36 3633 (3.5) 255 (5.3) 37 8451 (8.1) 447 (9.2) 38 18 082 (17.3) 866 (17.8) 39 35 422 (33.9) 1585 (32.7) 40 25 364 (24.3) 1105 (22.8) ≥41 11 445 (11.0) 461 (9.5)Positive DAT 3461 (3.3) 181 (3.7)Birth hospitalization length of stay ≥7 d 1550 (1.5) 140 (2.9)Birth hospitalization feeding Exclusive breast milk 64 795 (62.1) 2539 (52.3) 1 formula feed 4935 (4.7) 286 (5.9) >1 formula feed 34 249 (32.8) 1999 (41.2) No data 379 (0.4) 30 (0.6)Birth hospitalization phototherapy 6692 (6.4) 423 (8.7)Readmission phototherapy 2859 (2.7) 174 (3.6)Home phototherapy 3673 (3.5) 166 (3.4)Any phototherapy 11 831 (11.3) 702 (14.5)Maximum TSB level, mg/dL <3 5020 (4.8) 205 (4.2) 3–5.9 26 166 (25.0) 1004 (20.7) 6–8.9 24 677 (23.5) 1059 (21.8) 9–11.9 14 867 (14.2) 757 (15.6) 12–14.9 16 403 (15.6) 849 (17.5) 15–17.9 12 588 (12.0) 752 (15.5) ≥18 4637 (4.4) 228 (4.7)
DAT, direct antiglobulin test; LGA, large for gestational age; SGA, small for gestational age.
by guest on March 28, 2020www.aappublications.org/newsDownloaded from

In vivo, bilirubin plays an important role as an antioxidant; however, at higher levels (>20 mg/dL) bilirubin fails to provide protection.27 – 30 Perhaps a resultant oxidant–antioxidant imbalance may result in airway inflammation, with the development of asthma later in life.3 Our results do not support this mechanism because it would predict the risk to be greatest in children with the highest maximum TSB level. This rationale also requires that a brief exposure early in life would result in enough injury that would predispose an individual to asthma many years later, which seems unlikely.
Others have suggested that bilirubin may influence the immune
system.31 – 33 Unconjugated bilirubin may shift the T helper (Th) cell balance of T helper 1 to T helper 2 (Th2) toward the Th2 phenotype through an inhibition of interleukin-2 production.34 A Th2 predominance had been associated with the development of allergy and asthma.35, 36 Interleukin-2 is essential for the development and maintenance of T regulatory cells, which play an important role in regulating immunologic processes in peripheral tolerance to allergens.37, 38 The exposure is brief, but perhaps an alteration in cytokine production with hyperbilirubinemia could favor intolerance at a critical time in immune system development.
However, our data did not reveal a biological gradient or dose response of maximum bilirubin level and the risk of asthma. In fact, as maximum TSB levels increased, we saw a fall in the incidence of asthma after a maximum TSB level of 16 mg/dL. In comparison, the Collaborative Perinatal Project revealed a trend of an increasing risk of asthma with higher TSB levels at 48 hours and maximum TSB levels, 13 with the highest risk in children with a TSB level of >15 mg/dL. However, we were able to look at more gradations >15 mg/dL rather than group all the individuals together. Although the Collaborative Perinatal Project had 901 infants with a TSB level of >15 mg/dL, we had 13 340 infants with a maximum TSB level of 15 to 17.9 mg/dL and another 4865 infants with a maximum TSB level of 18 to 20.9 mg/dL.
If hyperbilirubinemia is implicated in the development of asthma, could the effect be ameliorated or prevented by treatment? No differences in the risk of asthma were seen between infants who were and were not treated with phototherapy. This may not fully answer the question, however, because the increased risk was seen at maximum TSB levels as low as 9 mg/dL. Many infants may have already reached TSB levels that are associated with an increased risk of asthma but are well below AAP recommended thresholds for phototherapy. Because there was no dose-response relationship between maximum TSB levels and asthma risk, preventing higher levels through phototherapy may not have any effect on asthma risk unless started at much lower thresholds.
The most likely alternative explanation for this association is a confounder, such as a genetic predisposition to both moderate hyperbilirubinemia and asthma. A potential example is polymorphisms in the glutathione S-transferase (GST) gene. Mutations have been linked to
PEDIATRICS Volume 142, number 4, October 2018 5
TABLE 2 Cumulative Incidence, Incidence Rate, and IRRs of Asthma by Maximum TSB Level Category
TSB, mg/dL
No. Infants
Asthma Cases
Cumulative Incidence of Asthma,
%
Incidence Per 1000 Person Years
IRR (95% CI) P
<3 5225 205 3.9 16.69 1.01 (0.87–1.18) .93–5.9 27 170 1004 3.7 16.46 Reference —6–8.9 25 736 1059 4.1 17.42 1.06 (0.97–1.15) .29–11.9 15 624 757 4.8 20.02 1.22 (1.11–1.34) <.00112–14.9 17 252 849 4.9 19.45 1.18 (1.08–1.29) <.00115–17.9 13 340 752 5.6 21.41 1.30 (1.18–1.43) <.001≥18 4865 228 4.7 17.15 1.04 (0.90–1.20) .9
—, not applicable.
FIGURE 1Maximum TSB levels and asthma incidence rates. TSB levels are categorized by 1 mg/dL intervals (eg, 3–3.9 mg/dL = 3 mg/dL level group).
by guest on March 28, 2020www.aappublications.org/newsDownloaded from

both neonatal hyperbilirubinemia39, 40 and asthma.41 – 47 GSTs can function both as enzymes and as intracellular binding proteins for nonsubstrate ligands, such as bilirubin and bilirubin conjugates, decreasing reflux from the hepatocytes back into plasma.48 Neonates with the GSTM1-null genotype have higher TSB levels compared with those with the wild phenotype.39, 40 GST is also involved in cytoprotection from byproducts of oxidative stress.49 GST is widely expressed in human airways and may play a role in modifying the risk of allergic response to environmental pollutants.50– 52 Multiple meta-analyses of the
association between GST genes and asthma have had conflicting results and have been hampered by study heterogeneity.42 –45 The polymorphism is not rare, which adds to the plausibility; the frequency of the GSTM1-null genotype is ∼50% in white individuals and ∼20% in African Americans.53
A possible explanation to why an association was seen between moderate hyperbilirubinemia and asthma and not a more severe hyperbilirubinemia may relate to the etiology of hyperbilirubinemia. Moderate hyperbilirubinemia may be associated with polymorphisms in the GST gene, whereas a more severe
hyperbilirubinemia may be seen more commonly with etiologies, such as ABO incompatibility, glucose-6-phosphate dehydrogenase deficiency, or sepsis. As a result, a common gene polymorphism that leads to moderate hyperbilirubinemia may be the etiology of hyperbilirubinemia in a greater percentage of infants with moderate hyperbilirubinemia, whereas in infants with severe hyperbilirubinemia, other etiologies are more common. Another possibility may be that there are 2 conflicting mechanisms. Bilirubin is both causal and protective at different levels, and at a level of >18 mg/dL, the protective mechanism overcomes the causal one.
Further lessening the case for causality, in both this study and past studies, TSB levels of <10 mg/dL were associated with asthma. The low bilirubin levels make it more plausible that it is not the bilirubin itself that is increasing the risk of asthma but rather a confounder.
A finding in our results that deserves further examination was that any formula feeding, even a single formula feeding during the birth hospitalization, was associated with an increased risk for developing childhood asthma. The extent to which formula feeding during the birth hospitalization serves as simply an indication of formula feeding in the subsequent months is unknown.
A major strength of our study is the large, modern, and diverse cohort. Homogenous populations were used in many of the previous studies, whereas in our cohort, there was representation of many races and ethnicities, increasing its generalizability. For our main predictors, we had actual bilirubin levels rather than codes for jaundice, and we used both orders and flow sheets for phototherapy rather than administrative codes. Additionally, our outcome variable was specific; multiple encounters were used with diagnostic codes in conjunction with
KUZNIEWICZ et al6
TABLE 3 Cox Proportional Hazards Model
Variable Adjusted HRa (95% CI) P
Maximum TSB level, mg/dL <3 1.00 (0.86–1.16) 0.98 3–5.9 Reference — 6–8.9 1.04 (0.96–1.14) .3 9–11.9 1.14 (1.04–1.26) .007 12–14.9 1.12 (1.02–1.24) .02 15–17.9 1.22 (1.10–1.36) <.001 ≥18 0.99 (0.84–1.16) .9Any phototherapy 1.01 (0.92–1.11) .8Male sex 1.61 (1.52–1.71) <.001Maternal history of asthma 2.34 (2.17–2.52) <.001Cesarean delivery 1.01 (0.94–1.08) .839Birth hospitalization length of stay >7 d 1.51 (1.26–1.17) <.001Recalibration 1.03 (0.91–1.17) .622Race Asian American 1.13 (1.04–1.23) .003 African American 1.95 (1.76–2.16) <.001 Hispanic 1.25 (1.16–1.36) <.001 White Reference — Other 1.11 (0.99–1.24) .080Maternal age, y <20 1.17 (1.01–1.36) .038 20–29 Reference — 30–39 1.04 (0.97–1.10) .253 ≥40 0.93 (0.81–1.07) .291Gestational age, wk 35 1.13 (0.93–1.37) .202 36 1.28 (1.11–1.48) .001 37 1.10 (0.98–1.23) .095 38 1.05 (0.96–1.15) .276 39 1.00 (0.93–1.08) .931 40 Reference — ≥41 0.94 (0.84–1.04) .240Birth hospitalization feeding Exclusive breast milk Reference — 1 formula feed 1.25 (1.10–1.41) <.001 >1 formula feed 1.17 (1.10–1.25) <.001
—, not applicable.a Adjusted for facility and birth year.
by guest on March 28, 2020www.aappublications.org/newsDownloaded from

pharmacy data that indicated the use of asthma medications. We were able to control for a large number of possible confounding variables, including infant feeding type (breast milk versus formula) during the birth hospitalization, maternal history of asthma, and gestational age. Using a modern cohort, we were limited by differential follow-up, although this was accounted for in our analyses by using Cox models.There is a possible underdiagnosis of asthma in those infants who were born in the later birth years because of a more limited follow-up. However, when we limited the analysis to those with at least 5 years of follow-up, the same associations persisted.Lastly, all bilirubin measurements were obtained as clinically indicated. Especially for infants with lower
maximum TSB levels, an infant’s true maximum TSB level may have been higher but unmeasured because repeat testing may not have been clinically indicated if there was a low likelihood of reaching phototherapy treatment levels. However, this misclassification would have made it more difficult to detect an association in the study.
CONCLUSIONS
An association between modest levels of hyperbilirubinemia and asthma exists. The association is unlikely to be causal because no dose-response relationship was seen, with the highest levels of hyperbilirubinemia not being associated with asthma. A confounder, such as a genetic polymorphism, is more likely associated with both asthma and
modestly decreased bilirubin conjugation. Phototherapy did not alter the risk of asthma. Using phototherapy to prevent infants from reaching these modest TSB levels is unlikely to be useful and would require phototherapy use in ∼50% of the birth population.
ABBREVIATIONS
AAP: American Academy of Pediatrics
aOR: adjusted odds ratioCI: confidence intervalHR: hazard ratioIRR: incidence rate ratioKPNC: Kaiser Permanente
Northern CaliforniaTh: T helperTh2: T helper 2TSB: total serum bilirubin
REFERENCES
1. Eder W, Ege MJ, von Mutius E. The asthma epidemic. N Engl J Med. 2006;355(21):2226–2235
2. Subbarao P, Mandhane PJ, Sears MR. Asthma: epidemiology, etiology and risk factors. CMAJ. 2009;181(9):E181–E190
3. Nadeem A, Masood A, Siddiqui N. Oxidant–antioxidant imbalance in asthma: scientific evidence, epidemiological data and possible therapeutic options. Ther Adv Respir Dis. 2008;2(4): 215–235
4. Wills-Karp M, Luyimbazi J, Xu X, et al. Interleukin-13: central mediator of allergic asthma. Science. 1998;282(5397): 2258–2261
5. Holt PG, Macaubas C, Stumbles PA, Sly PD. The role of allergy in the development of asthma. Nature. 1999;402(suppl 6760):B12–B17
6. Marguet C, Jouen-Boedes F, Dean TP, Warner JO. Bronchoalveolar cell profiles in children with asthma, infantile wheeze, chronic cough, or cystic fibrosis. Am J Respir Crit Care Med. 1999;159(5, pt 1):1533–1540
7. Henricks PA, Nijkamp FP. Reactive oxygen species as mediators in asthma. Pulm Pharmacol Ther. 2001;14(6):409–420
8. Sugiura H, Ichinose M. Oxidative and nitrative stress in bronchial asthma. Antioxid Redox Signal. 2008;10(4):785–797
9. Wei CC, Lin CL, Shen TC, Kao CH. Neonatal jaundice and risks of childhood allergic diseases: a population-based cohort study. Pediatr Res. 2015;78(2):223–230
10. Aspberg S, Dahlquist G, Kahan T, Källén B. Is neonatal phototherapy associated with an increased risk for hospitalized childhood bronchial
asthma? Pediatr Allergy Immunol. 2007;18(4):313–319
11. Aspberg S, Dahlquist G, Kahan T, Källén B. Confirmed association between neonatal phototherapy or neonatal icterus and risk of childhood asthma. Pediatr Allergy Immunol. 2010; 21(4, pt 2):e733–e739
12. Ku MS, Sun HL, Sheu JN, Lee HS, Yang SF, Lue KH. Neonatal jaundice is a risk factor for childhood asthma: a retrospective cohort study. Pediatr Allergy Immunol. 2012;23(7):623–628
13. Huang L, Bao Y, Xu Z, et al. Neonatal bilirubin levels and childhood asthma in the US Collaborative Perinatal Project, 1959-1965. Am J Epidemiol. 2013;178(12):1691–1697
14. Das RR, Naik SS. Neonatal hyperbilirubinemia and childhood allergic diseases: a systematic review. Pediatr Allergy Immunol. 2015;26(1):2–11
PEDIATRICS Volume 142, number 4, October 2018 7
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported by grant R01HS020618 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality. The funder played no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
by guest on March 28, 2020www.aappublications.org/newsDownloaded from

15. Kuzniewicz MW, Wickremasinghe AC, Wu YW, et al. Incidence, etiology, and outcomes of hazardous hyperbilirubinemia in newborns. Pediatrics. 2014;134(3):504–509
16. Newman TB, Wickremasinghe AC, Walsh EM, Grimes BA, McCulloch CE, Kuzniewicz MW. Retrospective cohort study of phototherapy and childhood cancer in Northern California. Pediatrics. 2016;137(6):e20151354
17. Newman TB, Wickremasinghe AC, Walsh EM, Grimes BA, McCulloch CE, Kuzniewicz MW. Phototherapy and risk of type 1 diabetes. Pediatrics. 2016;138(5):e20160687
18. Wickremasinghe AC, Risley RJ, Kuzniewicz MW, et al. Risk of sensorineural hearing loss and bilirubin exchange transfusion thresholds. Pediatrics. 2015;136(3):505–512
19. Wu YW, Kuzniewicz MW, Croen L, Walsh EM, McCulloch CE, Newman TB. Risk of autism associated with hyperbilirubinemia and phototherapy. Pediatrics. 2016;138(4):e20161813
20. Wu YW, Kuzniewicz MW, Wickremasinghe AC, et al. Risk for cerebral palsy in infants with total serum bilirubin levels at or above the exchange transfusion threshold: a population-based study. JAMA Pediatr. 2015;169(3):239–246
21. Kuzniewicz MW, Escobar GJ, Newman TB. Impact of universal bilirubin screening on severe hyperbilirubinemia and phototherapy use. Pediatrics. 2009;124(4):1031–1039
22. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation [published correction appears in Pediatrics. 2004;114(4):1138]. Pediatrics. 2004;114(1):297–316
23. Kazmierczak SC, Robertson AF, Catrou PG, Briley KP, Kreamer BL, Gourley GR. Direct spectrophotometric method for measurement of bilirubin in newborns: comparison with HPLC and an automated diazo method. Clin Chem. 2002;48(7):1096–1097
24. Wu TW, Dappen GM, Powers DM, Lo DH, Rand RN, Spayd RW. The Kodak Ektachem clinical chemistry slide for measurement of bilirubin in newborns:
principles and performance. Clin Chem. 1982;28(12):2366–2372
25. Kuzniewicz MW, Greene DN, Walsh EM, McCulloch CE, Newman TB. Association between laboratory calibration of a serum bilirubin assay, neonatal bilirubin levels, and phototherapy use. JAMA Pediatr. 2016;170(6):557–561
26. Chimmula S, Dhuru R, Folck B, et al. PS2-44: VDW data sources: Kaiser Permanente Northern California. Clin Med Res. 2012;10(3):193
27. Shekeeb Shahab M, Kumar P, Sharma N, Narang A, Prasad R. Evaluation of oxidant and antioxidant status in term neonates: a plausible protective role of bilirubin. Mol Cell Biochem. 2008;317(1–2):51–59
28. Dani C, Masini E, Bertini G, et al. Role of heme oxygenase and bilirubin in oxidative stress in preterm infants. Pediatr Res. 2004;56(6):873–877
29. Sedlak TW, Snyder SH. Bilirubin benefits: cellular protection by a biliverdin reductase antioxidant cycle. Pediatrics. 2004;113(6):1776–1782
30. Stocker R, Yamamoto Y, McDonagh AF, Glazer AN, Ames BN. Bilirubin is an antioxidant of possible physiological importance. Science. 1987;235(4792):1043–1046
31. Nejedlá Z. The development of immunological factors in infants with hyperbilirubinemia. Pediatrics. 1970;45(1):102–104
32. Ollinger R, Wang H, Yamashita K, et al. Therapeutic applications of bilirubin and biliverdin in transplantation. Antioxid Redox Signal. 2007;9(12):2175–2185
33. Rocuts F, Zhang X, Yan J, et al. Bilirubin promotes de novo generation of T regulatory cells. Cell Transplant. 2010;19(4):443–451
34. Haga Y, Tempero MA, Kay D, Zetterman RK. Intracellular accumulation of unconjugated bilirubin inhibits phytohemagglutin-induced proliferation and interleukin-2 production of human lymphocytes. Dig Dis Sci. 1996;41(7):1468–1474
35. Romagnani S. The Th1/Th2 paradigm and allergic disorders. Allergy. 1998;53(suppl 46):12–15
36. Romagnani S. The role of lymphocytes in allergic disease. J Allergy Clin Immunol. 2000;105(3):399–408
37. Liao W, Lin JX, Leonard WJ. Interleukin-2 at the crossroads of effector responses, tolerance, and immunotherapy. Immunity. 2013;38(1):13–25
38. Akdis M, Blaser K, Akdis CA. T regulatory cells in allergy: novel concepts in the pathogenesis, prevention, and treatment of allergic diseases. J Allergy Clin Immunol. 2005;116(5):961–968; quiz 969
39. Abdel Ghany EA, Hussain NF, Botros SK. Glutathione S-transferase gene polymorphisms in neonatal hyperbilirubinemia. J Investig Med. 2012;60(1):18–22
40. Muslu N, Dogruer ZN, Eskandari G, Atici A, Kul S, Atik U. Are glutathione S-transferase gene polymorphisms linked to neonatal jaundice? Eur J Pediatr. 2008;167(1):57–61
41. Hoskins A, Wu P, Reiss S, Dworski R. Glutathione S-transferase P1 Ile105Val polymorphism modulates allergen-induced airway inflammation in human atopic asthmatics in vivo. Clin Exp Allergy. 2013;43(5):527–534
42. Piacentini S, Polimanti R, Simonelli I, et al. Glutathione S-transferase polymorphisms, asthma susceptibility and confounding variables: a meta-analysis. Mol Biol Rep. 2013;40(4):3299–3313
43. Minelli C, Granell R, Newson R, et al. Glutathione-S-transferase genes and asthma phenotypes: a Human Genome Epidemiology (HuGE) systematic review and meta-analysis including unpublished data.Int J Epidemiol. 2010;39(2):539–562
44. Saadat M, Ansari-Lari M. Genetic polymorphism of glutathione S-transferase T1, M1 and asthma, a meta-analysis of the literature. Pak J Biol Sci. 2007;10(23):4183–4189
45. Li F, Li S, Chang H, et al. Quantitative assessment of the association between the GSTM1-null genotype and the risk of childhood asthma. Genet Test Mol Biomarkers. 2013;17(9):656–661
46. Karam RA, Pasha HF, El-Shal AS, Rahman HM, Gad DM. Impact of glutathione-S-transferase gene polymorphisms on enzyme activity, lung function and bronchial asthma susceptibility in Egyptian children. Gene. 2012;497(2):314–319
KUZNIEWICZ et al8 by guest on March 28, 2020www.aappublications.org/newsDownloaded from

47. Islam T, Berhane K, McConnell R, et al. Glutathione-S-transferase (GST) P1, GSTM1, exercise, ozone and asthma incidence in school children. Thorax. 2009;64(3):197–202
48. Sherlock S, Dooley J. Diseases of the Liver and Biliary System. 11th ed. Milan, Italy: Blackwell Science; 2002
49. Hayes JD, Flanagan JU, Jowsey IR. Glutathione transferases. Annu Rev Pharmacol Toxicol. 2005;45:51–88
50. Gilliland FD, Li YF, Saxon A, Diaz-Sanchez D. Effect of glutathione-S-transferase M1 and P1 genotypes on xenobiotic enhancement of allergic responses: randomised, placebo-controlled crossover study. Lancet. 2004;363(9403):119–125
51. Rahman I, Biswas SK, Kode A. Oxidant and antioxidant balance in the airways and airway diseases. Eur J Pharmacol. 2006;533(1–3):222–239
52. Strange RC, Spiteri MA, Ramachandran S, Fryer AA. Glutathione-S-transferase family of enzymes. Mutat Res. 2001;482(1–2):21–26
53. Ginsberg G, Smolenski S, Hattis D, Guyton KZ, Johns DO, Sonawane B. Genetic polymorphism in glutathione transferases (GST): population distribution of GSTM1, T1, and P1 conjugating activity. J Toxicol Environ Health B Crit Rev. 2009;12(5–6):389–439
PEDIATRICS Volume 142, number 4, October 2018 9 by guest on March 28, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-0662 originally published online September 12, 2018; 2018;142;Pediatrics
Thomas B. NewmanMichael W. Kuzniewicz, Hamid Niki, Eileen M. Walsh, Charles E. McCulloch and
Hyperbilirubinemia, Phototherapy, and Childhood Asthma
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/142/4/e20180662including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/142/4/e20180662#BIBLThis article cites 52 articles, 16 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/asthma_subAsthmaubhttp://www.aappublications.org/cgi/collection/allergy:immunology_sAllergy/Immunologybhttp://www.aappublications.org/cgi/collection/hyperbilirubinemia_suHyperbilirubinemiasubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on March 28, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-0662 originally published online September 12, 2018; 2018;142;Pediatrics
Thomas B. NewmanMichael W. Kuzniewicz, Hamid Niki, Eileen M. Walsh, Charles E. McCulloch and
Hyperbilirubinemia, Phototherapy, and Childhood Asthma
http://pediatrics.aappublications.org/content/142/4/e20180662located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2018 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on March 28, 2020www.aappublications.org/newsDownloaded from