
HyperandrogenismHyperandrogenism Dr. Mona Shroff SOGOG CME 2007.
44
Hyperandrogenism Hyperandrogenism Dr. Mona Shroff Dr. Mona Shroff SOGOG CME 2007 SOGOG CME 2007
-
Upload
alexander-george -
Category
Documents
-
view
216 -
download
1
Transcript of HyperandrogenismHyperandrogenism Dr. Mona Shroff SOGOG CME 2007.

HyperandrogenismHyperandrogenismHyperandrogenismHyperandrogenismDr. Mona ShroffDr. Mona Shroff
SOGOG CME 2007SOGOG CME 2007
Case A
14 y/o female (menarche 1 yr back)• Menses q 3--4 months• Mild facial acne• FG Score of 5 (1 lip, 1 chin, 2 lower abd, 1 back)• BMI 29 kg/m2• No galactorrhoea

• What are the various causes of hyperandrogenism?
• In this adolescent girl what probable cause do you suspect?
Aetiology of hyperandrogenism
• FOH of puberty• PCOS• HAIR-AN syndrome• Hyperprolactinemia• Hypothyroidism• NCAH• TUMORS-Ovarian / Adrenal• Cushings disease• Drugs
• What particular aspects of history & clinical features would you like to look for?
Clinical assessment
History The following items are important::
• Family History of HA/Obesity/temporal balding/infertility• Hx of Precocious adrenarche• More than 2 years of oligomenorrhea

Clinical assessment..
Physical examination
• Degree of hirsutism, acne• Obesity ,increased W/H ratio Acanthosis nigricans- r/o PCOS,HAIR-AN• Rapidly growing hirsutism or Virilizing symptoms – r/o TUMOR• Symptoms of hypercorticism –r/o CUSHING• Galactorrhea – r/o HYPERPROLACTINEMIA

What is this C/F?


•Would you like to investigate this patient at this juncture?

• Would you like to start treatment at this time?
• In which particular patients would you evaluate & treat at an early age?
J Pediatr. 2004 Jan;144(1):23-9.
Insulin sensitization early after menarche prevents progression from precocious pubarche to polycystic ovary syndrome in a high-risk group of formerly LBW girls.

LIFESTYLE MODIFICATIONS

Adult v/s Adolescent HA
•FOH or Organic cause???•USG not reliable-ovaries may
be N.•Premature adrenarche –strong
predictor.•Lifestyle changes – biggest
impact-Prevention of PCOD !!!
J Pediatr Endocrinol Metab. 2000;13 Suppl 5:1285-9
• Same patient comes to you after 2 yrs (age 16 yrs) - still having same clinical picture but worsened
delayed periods mod. acne & hirsutism BMI 32

• Would you like to evaluate this patient now?
• What initial screening investigations would you like to go for & why?

INITIAL LAB SCREENING
• TESTOSTERONE• PROACTIN• TSH• Evaluation for
HYPERINSULINEMIA• 17 OH PROGESTERONE

INITIAL LAB SCREENING• Testosterone total – may be N in hirsute woman if T> 200 screen for tumor
free T?? Should we ask for? – no clinical need to check - if HA effect seen then free T must be raised - does not help in D/D or
treatment

• TSH - esp if alopecia• PROLACTIN - DHEAS ,free T (SHBG )• HYPERINSULINEMIA Fasting glucose : Insulin <
4.5 Fasting insulin > 20 2 hr GTT > 140

• 17 OH P - for NCAH , follicular ph/morning -routine screen in HA indicated (esp if sev hirsutism at younger age ,short stature)
* <200 ng/dl : N * 200 – 800 : ACTH stimulation test * > 800 : diagnostic
• Screen for Cushings if clinical suspicion
late eve. plasma cortisol single dose overnight DST
• Imaging of adrenals & ovaries (USG/CT/MRI)
* if rapid virilization * T > 200 micgm/ dl
Audience question• Would you like to
include S.DHEAS in her list of investigations?
If YES - WHY? If NO – WHY NOT?
DHEAS ???
• Moderate elevation common in anovulatory females
• > 700 micgm/dl – v.rare• if T> 200 – screen for tumor must• Mod. elevated DHEAS does not
necessitate or prove the need & benefit of treatment with dexamethasone
• No further benefit by testing,not cost effective
Gordon,Speroff 2002

Lab resultsof this patient
TSH, Prolactin, 17OH P : normal Total T : 70 ng/mL [<72 ng/mL] Fasting Insulin : 22 mIU/mL [<20 mIU/mL] Fasting Glucose 92 mg/dL

• What are the options available for treating HA?
COCPs
ANTIANDROGENSSPIRONOLACTONE
FUTAMIDEFINASTERIDE
CYPROTERONEDEXAMETHASONEKETOCONAZOLE
CIMETEDINEGnRH AGONISTS
INSULIN SENSITIZERSMECHANICAL AGENTS(hirsutism)
ANTIBIOTICS (acne)

• Considering our diagnosis of PCOS in this girl what are your aims of treatment
• What treatment would you like to start in this patient?
• How long should you continue with this treatment?
Management of excess ovarian androgen production :
Standard therapy is :combined E+P OCs
• It reduces ovarian androgen production
• It increases SHBG• It induces competition at the
cellular level for binding to the androgen receptor
METFORMIN• In addition to the expected improvements in insulin sensitivity and glucose metabolism• Ameliorates hyperandrogenism and menstrual
irregularity.• Reduces total cholesterol, LDL and triglycerides of
PCOS adolescents while increasing HDL cholesterol .• Decrease C-reactive protein and a normalization of
the neutrophil/lymphocyte ratio , which are predictive of cardiovascular disease.
Benefits both obese & non obese Hum Reprod. 2005 Sep;20(9):2457-62.
Hum Reprod. 2002 Jul;17(7):1729-37.
ANTIANDROGENS
•According to currenty available evidence no antiandrogen is superior to other in terms of clinical efficacy, so choice depends upon S/E & cost.Further studies needed.
Chocrane reviews, Issue 1, 2006 Fertil Steril. 1999Mar;71(3):445-51.
–
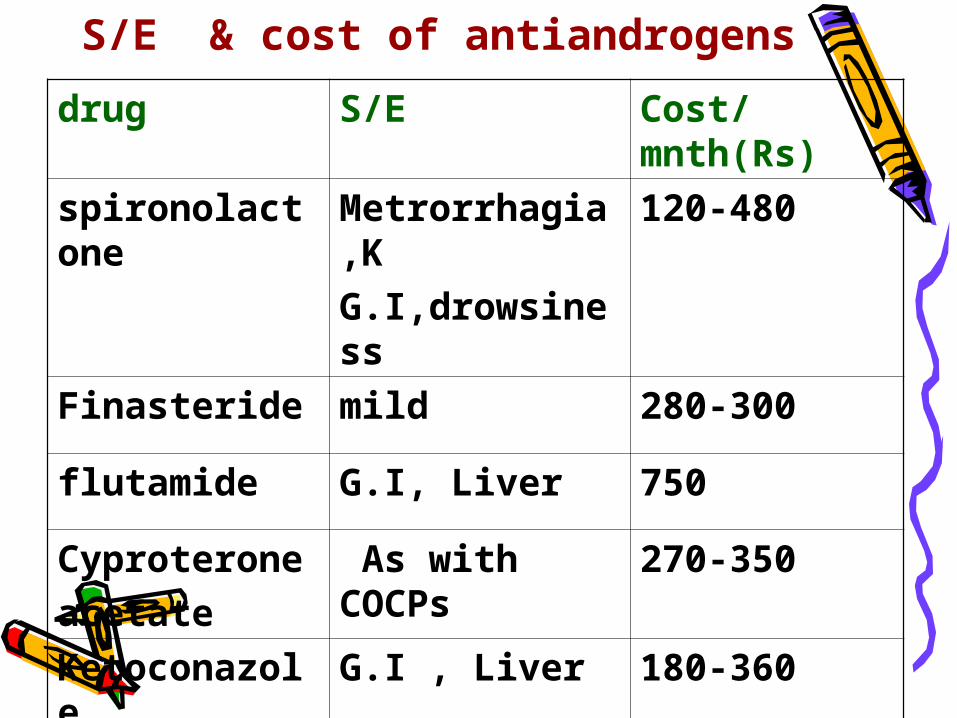
S/E & cost of antiandrogens
drug S/E Cost/mnth(Rs)
spironolactone
Metrorrhagia,KG.I,drowsiness
120-480
Finasteride mild 280-300
flutamide G.I, Liver 750
Cyproteroneacetate
As with COCPs
270-350
Ketoconazole
G.I , Liver 180-360

• Would you like to add a steroid (dexona) to your therapy in this patient?

AUDIENCE QUESTION
WHICH PILL WOULD YOU CHOOSE FOR ADOLESCENT PCOS with HA & WHY?
• LNG containing (mala-D,ovral-L,Loette)• DESOGESTREL containing (novelon,femilon)• CYPROTERONE containing (Ginette,krimson35, diane35)• DROSPIRINONE containing (yasmin)
COCs LNG vs Desogestrel vs
CPA
• DSG & CPA pills comparable efficacy, better than LNG.(CPA slightly better for acne)
• DSG & CPA pills comparable side effects ( VENOUS THROMBOEMBOLISM & LIVER )
Acta Obstet Gynecol Scand Suppl. 1986;134:29-32. Int J Fertil Menopausal Stud. 1996 Jul-Aug;41(4):423-9. Fertil Steril. 2002 May;77(5):919-27. Eur J Contracept Reprod Health Care. 2001 Mar;6(1):46-53. J Obstet Gynaecol Can. 2003 Dec;25(12):1011-8. Pharmacoepidemiol Drug Saf. 2004 Jul;13(7):427-36. Pharmacoepidemiol Drug Saf. 2003 Oct-Nov;12(7):541-50.

Case B
16 y/o female • Menses q 3-4 months• Moderate facial acne• FG Score of 5 (1 lip, 1 chin, 2 lower abd, 1 back)• Tanner Stage breast 4, pubic hair 4• BMI 26..3 kg/m2• No galactorrhoea
INITIAL SCREENING ??
Lab results
• TSH,, Prolactin normal• 17OH P : 2.5 ng/mL [<2 ng/mL]• Total T : 70 ng/mL [<72 ng/mL]• Fasting Insulin 14 mIU/mL [<17 mIU/mL]• Fasting Glucose 92 mg/dL
What would you do next?

ACTH Stimulation Test
Baseline 17 OH P 2..5 ng/dL 60 min 17 OH P 18 ng/dL
What is your inference? How would you treat this patient?
•Treat hyperandrogenism with dexamethasone or CPA or spironolactone or flutamide• Treat irregular menses with combined oral contraceptive pills• Treat infertility when patient desires pregnancy• Consider adding dexamethasone to ovulation induction
NCAHJ Clin Endocrinol Metab. 1990 Mar;70(3):642-6.
Cyproterone acetate versus hydrocortisone treatment in late-onset adrenal hyperplasia.
• Peripheral antiandrogen therapy may be more appropriate in late-onset adrenal hyperplasia patients than conventional adrenal inhibition using cortisone therapy.


CONCLUSIONS
• HA is a common adolescent probem• Our main aim is early PCOS diagnosis
& ruling out tumor/NCAH.• Watch for premature pubarche.• Initial screen –T, TSH, Prolactin,
fasting glucose:insulin, 17 OH P• Imaging for tumor if T>200 or rapid
virilisation
CONCLUSIONS (contd.)• Lifestye modification & weight
reduction plays a key role.• Integrated approach –
combination of drugs with best outcome & min. S/E. (COCs + IS +/- Antiandrogen).
• PCOS - Candidates for long term therapy.

THANK YOU


















