HYDROCEPHALUS THERAPYbritpics.co.uk/becky/LIT-11032_Hydro.pdfAnatomy and Physiology delicate balance...
15
HYDROCEPHALUS THERAPY Living with Hydrocephalus
Transcript of HYDROCEPHALUS THERAPYbritpics.co.uk/becky/LIT-11032_Hydro.pdfAnatomy and Physiology delicate balance...

HYDROCEPHALUS THERAPY
Living with Hydrocephalus

T he purpose of this booklet is to helppatients and their families gain an under-standing of hydrocephalus and its treatment.
Although an ideal treatment is not yet available,numerous advances have contributed to moreeffective treatment within the past few decades.
Contents
What is Hydrocephalus? .................................................................................... 4Types of Hydrocephalus ...................................................................................... 4
Anatomy and Physiology ................................................................................... 6
Diagnosis ...................................................................................................................................... 8Diagnostic Studies ...................................................................................................... 9
Treatment ................................................................................................................................. 10Shunt Components .................................................................................................. 12Valve Types ........................................................................................................................13Surgery and Hospitalization ........................................................................ 16Participating in Your Care ............................................................................. 17
Complications .................................................................................................................... 18Obstruction ....................................................................................................................... 18Infection ................................................................................................................................ 19Overdrainage ................................................................................................................. 20Precautions ....................................................................................................................... 20
Emotional Support ....................................................................................................22
Glossary ....................................................................................................................................... 24
Contributing Editors:
Delia R Nickolaus, MSN, RNLeanne Lintula

44444 55555
What Is Hydrocephalus?
Obstructive or non-communi-cating hydrocephalus occurswhen CSF flow is blockedwithin the ventricular system.
Non-obstructive, or communi-cating, , , , , hydrocephalus occurswhen the CSF leaving the fourthventricle is restricted in its flowover the surface of the brain, orif the sites of absorption are notfunctioning adequately. Hydro-cephalus may also be due tooverproduction of CSF by a raretumor known as a choroidplexus papilloma.
Obstructive or non-obstructivehydrocephalus can be a con-genital or an acquired condi-tion. Congenital hydrocephalus
Types of Hydrocephalus
simply means that the conditionexisted before birth, such asaqueductal stenosis or spinabifida. Acquired hydrocephalusdevelops after birth, for a vari-ety of reasons, such as trauma, abrain tumor, scar tissue forma-tion, or meningitis.
Normal Pressure Hydroceph-alus (NPH) is an increase in theamount of CSF in the ventricleswith little or no increase in thepressure inside the head. It ismost often seen in adults over60 years of age. There are threeclassic symptoms associatedwith NPH: difficulty walking,mild dementia, and impairedbladder control.
The term hydrocephalusis derived from twoGreek words: hydro for
water and kephale for head.Hydrocephalus implies anexcessive amount of cerebro-spinal fluid (CSF), within thecavities of the brain known asventricles. This excessiveamount of CSF can result froma blockage in the brain’s ventri-cular system which preventsthe normal flow of the CSF, oras the result of a problem withCSF absorption.
In most instances, hydroceph-alus is a lifelong condition sincethe patient is treated ratherthan “cured.” Treatment, byshunting (sending) the CSF toanother area of the bodythrough a small tube, generallyallows people with hydroceph-alus to lead full and active lives.
People with hydrocephalus andtheir families, however, shouldbe aware of the potentialcomplications and their signsand symptoms so that medicalcare can be sought in a timelymanner when necessary. Thisbooklet is intended to helpprovide that information.
Hydrocephalus can be treated,allowing people to lead full andproductive lives.
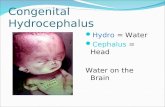
Fig 1. Normal Ventricles Fig 2. Hydrocephalic Ventricles

66666 77777
The illustration below shows aview of the center of the brainwith the ventricles and sur-rounding structures. The solidarrows show the major pathwayof CSF flow. The broken arrowsshow additional pathways.Tobetter understand hydroceph-alus, a basic knowledge of theanatomy of the skull and brain,and the formation and absorp-tion of CSF is helpful.
one pint) per day. The fluid isin continuous circulation andcontains many substancesessential for nourishment andnormal function of the nervoussystem. CSF also provides aprotective cushion within andaround the brain.
CSF flows through the ven-tricular system, and out threesmall openings in the fourthventricle before entering thesubarachnoid space surround-ing the brain and spinal cord.The fluid then flows over thesurfaces of the brain and spinalcord, and is eventually absorbedinto the blood stream throughvalve-like structures calledpacchionian granulations.Thus, CSF is in a continuousprocess of production, circula-tion, and absorption. Undernormal conditions, there is a
Anatomy and Physiology delicate balance associated withthis process in order to keep theamount of CSF at a constantlevel.
Hydrocephalus develops whenCSF cannot flow through theventricular system, or whenabsorption into the bloodstream is not the same as theamount of CSF produced.
The brain occupies most of thespace inside the skull and issurrounded by a cushioninglayer of CSF. This fluid is pri-marily produced and circulatedwithin the four interconnectingventricles of the brain.
The ventricles contain delicatetufted structures known aschoroid plexus. These struc-tures produce most of the CSF,approximately 500 ml (about
Fig 3. Cerebrospinal Fluid (CSF) Circulatory Pathway
Lateral ventricles
Choroid plexus Subarachnoid space
Arachnoid space
Aqueductof Sylvius
Sagittal sinus
Third ventricle
Fourth ventricle
Skull
Brain

88888 99999
There are several diagnostic teststhat can help in diagnosing hydro-cephalus. These same studies canalso help evaluate the shuntsystem in case of malfunction orinfection.
Ultrasound Ultrasound Ultrasound Ultrasound Ultrasound is a sophisticatedmethod of outlining structureswithin the head using high fre-quency sound waves. This proce-dure can be used only in infantswhose fontanels are open, since theskull otherwise blocks soundwaves.
Computerized Tomography (CTComputerized Tomography (CTComputerized Tomography (CTComputerized Tomography (CTComputerized Tomography (CTScan)Scan)Scan)Scan)Scan) is a technique in which tinybeams of x-ray outline the skull,brain, ventricles, and subarachnoidspace. In addition to visualizingthe size and shape of the ventricles,abnormalities such as tumors,cysts, and other pathology can alsobe seen.
Magnetic ResonanceMagnetic ResonanceMagnetic ResonanceMagnetic ResonanceMagnetic ResonanceImaging (MRI)Imaging (MRI)Imaging (MRI)Imaging (MRI)Imaging (MRI) is a non-invasivediagnostic tool that uses radiosignals and a magnet to formcomputer images of the brain, itsventricular system and coverings,and pathological lesions.
Cisternography Cisternography Cisternography Cisternography Cisternography is a test requiringinjection of a small amount of radio-active material into the CSF. Thistest differentiates communicating
Diagnostic Studiesfrom obstructive hydrocephalus,and determines CSF flow.
Air StudiesAir StudiesAir StudiesAir StudiesAir Studies are done much lessfrequently today than in the past.Injection of air into the ventricles,either by direct puncture orthrough a spinal needle, may benecessary in certain instances.
Angiography Angiography Angiography Angiography Angiography is a specializedtechnique in which contrastmaterial is injected into thearteries supplying the brain.Abnormal blood vessel problemsor pathological lesions can bedetected with this technique.
Neuropsychological TestsNeuropsychological TestsNeuropsychological TestsNeuropsychological TestsNeuropsychological Tests are aseries of questions and answersused to determine if there isdecrease in brain functioning dueto hydrocephalus.
Lumbar Infusion TestLumbar Infusion TestLumbar Infusion TestLumbar Infusion TestLumbar Infusion Test is a special-ized technique in which fluid is in-jected into the lumbar subarach-noid space. This procedure is usedin NPH patients to determine theirCSF absorptive capacity.
Controlled Lumbar DrainageControlled Lumbar DrainageControlled Lumbar DrainageControlled Lumbar DrainageControlled Lumbar Drainage is atechnique used to externally drainCSF. The test is used to determineif a patient with NPH will improvewith shunt placement
Diagnosis
In infants and toddlers, thebones of the skull are notyet closed and hydroceph-
alus may be obvious. The child’shead will enlarge, and thefontanel (soft spot) may betense and/or bulging. The skinmay appear thin and shiny, andthe veins of the scalp mayappear full or engorged. Symp-toms may include vomiting,poor feeding, listlessness,irritability, constant downwardgaze of the eyes, and at times,seizures.
In older children and adults, thebones of the skull have closed.These patients have symptomsof increased intracranial pres-sure due to ventricular enlarge-ment (from the extra CSF)which causes compression ofthe brain tissue. Symptomsmay include, but are not lim-ited to, headache, nausea,vomiting, visual disturbances,poor coordination, personalitychanges, lack of concentration,and lethargy.
The signs and symptoms ofincreasing intracranial pres-sure are likely to change overtime, as the cranial sutures (thejoints between the bones of theskull) begin to close in theinfant and toddler and are fullyclosed in the school age child.
Signs and symptoms of in-creased intracranial pressureare useful in the initial diagno-sis of hydrocephalus and alsowhen there is a shunt malfunc-tion or infection as will bediscussed later.
In adults with normal pressurehydrocephalus, the symptomsare usually difficulty in walk-ing, mild dementia, and urinaryincontinence.

1010101010 1111111111
Regular visits to your neurosurgeonwill be necessary.
A t this time, the standardtreatment for hydro-cephalus is surgery.
There is no long term medicaltreatment. The surgical proce-dure usually involves diverting(sending) CSF to either theabdominal cavity (a ventri-culo-peritoneal or VP shunt), orto a chamber of the heart calledthe right atrium (a ventriculo-atrial or VA shunt). Occasion-ally, the CSF is shunted (sent)into the pleural cavity (ventri-culo-pleural shunt) or from thelumbar spine (lower back) tothe abdominal cavity (lumbo-peritoneal or LP shunt).
In order to divert the CSF, thesurgeon will insert a shuntsystem made from silicone andpolypropylene plastic. Allcomponents of the system areplaced under the skin. Thereare no parts on the outside ofthe body.
Treatment
Fig 4. Ventriculo-peritoneal (VP) Shunt
Fig 6. Ventriculo-pleural Shunt Fig 7. Lumbo-peritoneal (LP) Shunt
DistalCatheter
VentricularCatheter
Valve
Fig 5. Ventriculo-atrial (VA) ShuntFig 8. Shunt Components

1212121212 1313131313
The components of a shuntsystem usually include twocatheters and a one-way valve.The catheter placed in theventricle of the brain is calledthe proximal catheter becauseit is closest to the ventricles.The catheter placed in eitherthe peritoneal cavity (abdomen)or, occasionally, in the rightatrium of the heart, is called thedistal catheter because it is thecatheter farthest way from theventricles. Both catheters areattached to a one-way valveused to regulate the amount,direction, and pressure of CSFflow out of the ventricles. Thereare several different kinds CSFvalves. Each valve is designed tooperate at a different pressure/flow range or performancelevel. The surgeon’s choice ofvalve is based on an evaluationof the type of hydrocephalusand the individual needs of thepatient.
In some shunt systems areservoir is included in thedesign. A reservoir can be usedfor a variety of reasons. Byflushing the reservoir, shuntfunction can be tested. Also,samples of CSF for lab studiescan be obtained through areservoir. Patients and theirfamilies are discouraged frompressing the reservoir in anattempt to “test” the shunt.This maneuver can be danger-ous unless done under explicitinstructions from a physician.
Patients with obstructivehydrocephalus must have onecatheter inserted into theventricle. Patients with com-municating hydrocephalus,however, may have the CSFdrained from the subarachnoidspace of the lumbar spine toanother cavity of the body,usually the peritoneal cavity.This is known as a lumbo-peritoneal shunt (LP shunt)
Fig 9. Valve Pumping
Shunt Components
Small Needle
and is usually reserved for, butnot entirely limited to, the adultpopulation.
The type of shunt and theplacement of the shunt is basedon what the neurosurgeondetermines is best for thepatient based on the type ofhydrocephalus and any othermedical conditions the patientmay have.
Fig 10. CSF Sampling
Some of the shunt types avail-able include fixed pressurevalves, valves with overdrainageprotection (Delta® valves), orvalves that can be adjusted todifferent pressure settings aftersurgery (Strata® valves).
The fixed pressure valves in-clude a single valve mechanismthat regulates the shunt flowrate. The valves are typicallyavailable in three pressureranges: low, medium or high.
The Delta valves include anoverdrainage device at the valveoutlet. The purpose of theoverdrainage device is to mini-mize excessive drainage due togravity causing more fluid todrain when the patient is in theupright position.
Valve Types
The adjustable Strata valveincludes a mechanism that canbe non-invasively adjustedmagnetically. This gives thedoctor the ability to change thevalve pressure setting in hisoffice without using a surgicalprocedure. Since the valveincludes a magnet, special pre-cautions must be observed whenbeing around strong magneticsources such as retail securityscanners, metal detectors, andsome audio headphones. Com-mon everyday household equip-ment such as microwave ovens,telephones, and computers arenot strong enough to affect thevalve. For patients that areundergoing an MRI procedure, itwill be necessary for the doctorto check the valve pressuresetting afterwards and readjustit if necessary.

1414141414 1515151515
Integral InletConnector
Proximal OccluderSilicone Dome
Reservoir
RadiopaquePerformance/Flow Direction Indicators
DeltaChamber
Distal Occluder
Integral OutletConnector
RadiopaqueMarker Firm Polypropylene
Plastic Base
Silicone MembraneValve
DistalOccluder
RadiopaqueFlow DirectionIndicator
Reservoir
SiliconeDome
ProximalOccluderIntegral
Inlet Connector
RadiopaqueMarker
RadiopaquePressure Dots
SiliconeMembrane
Valve
Firm Polypropylene
Plastic Base OutletPorts
IntegralOutlet Connector
Fig 14. Cutaway of a Fixed Pressure Valve
Fig 15. Cutaway of a Delta Valve
Integral InletConnector
Proximal OccluderSilicone Dome
Radiopaque FlowDirection Indicator
Reservoir
Delta ChamberIntegral OutletConnector
Radiopaque Valveto Catheter Indicator
Adjustable ValveMechanism
Firm Plastic BaseRadiopaque Valveto Catheter
Indicator
Distal Occluder
Fig 16. Cutaway of a Strata Valve
Fig 12. Delta® Valves with Siphon Control
Fig 11. Fixed Pressure Valves
Fig 13. Adjustable Strata® Valves

1616161616 1717171717
Surgery and Hospitalization
The surgical procedure iscarried out under sterileconditions in the operat-
ing room. Although the opera-tion is relatively short, carefulpreparation for the surgeryadds extra time. In order tohelp prevent infection, some ofthe hair on the head may needto be shaved. The head andbody are washed with specialsoap. Sterile linen is used tocover the patient and to main-tain the sterile environmentthroughout the surgery.
A small incision (cut) is madein the scalp (the skin coveringthe head). A small hole is thenmade in the skull. A tinyopening is made in the dura, aprotective covering of the brain.These openings are made toaccommodate the ventricularcatheter (proximal catheter)being placed into the lateralventricle. The neurosurgeonthen makes two or three smallincisions in order to place theshunt valve (usually above orbehind the ear). The peritonealor atrial catheter (distal cath-eter) is tunneled under the skinto the abdominal or neckincision. Finally, the end of the
Participating in Follow-Up Care
catheter is carefully placedeither in the peritoneal cavityor in a vein of the neck leadingto the atrium of the heart.Following the operation, smallsterile bandages are applied toeach incision.
Immediately after surgery, thepatient will go to the post-anesthesia care unit. Thepatient will remain there forclose observation for about anhour and then go to his/herroom. The length of hospital-ization varies from patient topatient. Most patients leave thehospital within two to sevendays, depending on theirclinical progress.
Although this is the usualprocedure when a shunt isplaced, each patient may have aslightly different experiencebased upon their neurosur-geon, hospital, and the need toindividualize the care for thepatient.
Most patients withhydrocephalus haveevery right to look
forward to a normal future.However, because this condi-tion is “on-going,” patients dorequire long-term, follow-upcare by a neurosurgeon. Havingmedical check-ups at intervals
recommended by the neurosur-geon is sensible. The patient, orhis/her family, must assume ashare of the responsibility forfollow-up care. The neurosur-geon will also keep a watchfuleye on the patient and pick upsubtle changes that may indi-cate a shunt malfunction.

1818181818 1919191919
Obstruction
Complications
Children and adultswho have shunts inplace will normally
require surgical shunt revisionsto replace a part of the shuntthat is no longer working.Children can physically out-grow a shunt; any patient mayeventually need a differentpressure valve. CT or MRIscanning provides the physicianwith the tools necessary tomake an early and noninvasiveevaluation of the shunt’s per-formance. In addition to regu-lar follow-up visits to theneurosurgeon, family membersshould watch for symptoms ofshunt complications. Immedi-ate and accurate reporting ofhealth related problems is veryimportant. Flu symptoms, forexample, mimic those of shuntobstruction. The early detectionof complications allows revi-sions to be scheduled, prevent-ing emergency situations.
Patients and their families mustbe alert for the signs and symp-
toms resulting from shuntcomplications. The majorcomplications of shunting areobstruction, infection andoverdrainage.
tumor cells. The shunt mayalso become obstructed if thecomponents become separated,or if the position of the shuntchanges with the growth of theinfant or child, either in theproximal or the distal end.
Obstruction of the shunt willproduce signs and symptomsof increased pressure in thehead. These will vary depend-ing upon the degree of obstruc-tion and age of the patient.Partial, or intermittent, ob-struction may result in peri-odic headache, nausea andvomiting, along with drowsi-ness, listlessness, and decreasedmental function. Poor perfor-mance in school or at work iscommon under these condi-tions.
If complete obstruction occurs,there will be a rapid develop-ment of the signs and symp-toms — headache, nausea,vomiting, blurring of vision,loss of coordination, and deter-ioration of consciousness. The
patient may become stuporousor comatose. Should this occur,emergency hospitalization forobservation and treatment isrequired. The neurosurgeon willrun tests to determine thelocation and degree of shuntobstruction. Removal andreplacement of the obstructedpart of the shunt system maybe necessary.
The most common complica-tion of shunting is obstructionof the system. Obstruction mayoccur at any point along theshunt system. The openings ofthe ventricular catheter maybecome plugged with brain orchoroid plexus tissue. Theymay become plugged due to anexcessive reduction in size ofthe ventricular cavity (slitventricle) due to overdrainageof CSF. The peritoneal end maybecome surrounded by loops ofbowel, other structures, or byscar tissue. Shunts in the rightatrium of the heart may beobstructed by the clotting ofblood around the end of thetube. Shunt tubing may be-come plugged with bloodelements, brain fragments, or
InfectionThe second most commoncomplication of CSF shunting isinfection. This hazard ispresent in all surgical opera-tions — particularly when aforeign body such as a shuntsystem is implanted. Infectionshould be suspected if there isunusual redness or swelling ofthe wounds or along the lengthof the shunt system (the shunttrack). These changes should becalled to the attention of theneurosurgeon. If not treated,infection can lead to the wound

2020202020 2121212121
opening up or, more seriously,to systemic infection withchills and high fever. Infectionusually requires removal of theshunt system. In some cases,the infection can be controlledwith intensive antibiotictherapy, without removing theshunt.
Since the shunt system is a“foreign body,” a patient maydevelop an allergic or inflam-matory reaction to it at anytime. Inflammation or opensores over any part of theimplanted system should bebrought to the attention of theneurosurgeon immediately.
Check with yourhealth care teamabout specificphysical activitiesyou would like todo after receivingyour shunt implant.
The following table summar-izes many of the signs andsymptoms of a shunt malfunc-tion based on the patient’s age.Each patient is an individual.Therefore, not everyone willhave all of these symptoms, andsome patients may have othersymptoms not listed here.
Symptoms of Shunt Malfunction or InfectionSymptoms of Shunt Malfunction or InfectionSymptoms of Shunt Malfunction or InfectionSymptoms of Shunt Malfunction or InfectionSymptoms of Shunt Malfunction or Infection
InfantsInfantsInfantsInfantsInfants ToddlersToddlersToddlersToddlersToddlers Children and AdultsChildren and AdultsChildren and AdultsChildren and AdultsChildren and Adults
Enlargement of baby’s head
Fontanel full and tense wheninfant is upright and quiet
Prominent scalp veins
Swelling along shunt tract
Vomiting
Irritiability
Sleepiness
Downward deviation of eyes
Poor feeding
Fever*
Redness along shunt tract*
Head enlargement
Vomiting
Headache
Irritability and/or sleepiness
Swelling along shunt tract
Loss of previous abilities(sensory or motor function)
Fever*
Redness along shunt tract*
Vomiting
Headache
Vision problems
Irritability and/or tiredness
Personality change
Loss of coordination or balance
Swelling along shunt tract
Difficulty in waking up orstaying awake
Decline in academic performance
Fever*
Redness along shunt tract*
*Fever and redness along the shunt tract both indicate infection.
The information in this table is courtesy of the Hydrocephalus Association,www. hydroassoc.org. This list of symptoms is for your reference only andis not a diagnostic aid. If you are in doubt about your child’s medical condi-tion, consult your neurosurgeon immediately.
It is important to rememberthat many other commonillnesses may have these samesymptoms. But since thesesymptoms could also be a shuntmalfunction, it is very impor-tant that the patient be evalu-ated immediately by a neuro-surgeon.
changes in vision, particularlydouble vision. Overdrainageshould be suspected in schoolage children if their perform-ance in school is declining.
Overdrainage is generallycaused when gravity drains toomuch fluid while the patient isupright. Overdrainage of CSFmay produce a variety of signsand symptoms. Patients gener-ally experience a headache thatis worse when standing andreduced by lying down. Addi-tional symptoms are nausea,vomiting, drowsiness and
Overdrainage
In addition to recognizing thesigns and symptoms of shunt-ing complications, commonsense precautions shouldalways be taken. Since a shuntsystem is implanted in theattempt to regulate CSF flowand intracranial pressure,participation in activities thatmight upset the delicate bal-ance should be limited. Inparticular, rough contact sportsand diving should be discussedin advance with the neurosur-geon.
Precautions

2222222222 2323232323
The physical aspect ofhydrocephalus is onlyone part of dealing with
this condition. Emotionalfactors must also be considered,for the patient as well as thefamily.
Although the surgical proce-dure is likely to control thehydrocephalus, those involvedmay be upset, fearful, de-pressed, angry or frustrated. Ifthe patient is a child, keep inmind that children have feel-ings similar to adults, and maybe suspicious that there is aserious problem.
Since the child may not feelwell, may have had some un-usual tests, and is visiting thedoctor more than usual, thissuspicion is understandable.Rather than allowing the child’sfright to escalate, and theimagination to create unrealis-tic, unnecessary fears, the
child’s anxiety may be relievedwith an explanation. Knowingwhat to expect increases thecooperation of the child. Chil-dren, like adults, generally don’tlike surprises.
Explain hydrocephalus to thechild in terms the child canunderstand. A quiet, calmatmosphere with a loving,supportive family, and as fewdistractions as possible, is thebest environment for such adiscussion.
Young children, up to about 3years of age, are unlikely tounderstand. They will mostlybe concerned with the here andnow, especially separation fromparents. In this age group,crying is quite typical as ameans of attempting to gaincontrol.
Older children, up to about 10years of age, are usually satis-
Emotional Support fied with simple explanationsand honesty. Acknowledge thechild’s feelings and allow thechild to express them. Reassurethe child that when the needleshurt, it’s okay to cry and becomforted. Although going tothe hospital may not be anexperience a child looks for-ward to, telling the child thetruth will help to establish andmaintain trust.
Children over the age of 10 areusually able to understandmore complex concepts. Theycan associate a variety of signsand symptoms with theircondition, and can better acceptlimitations placed upon them.
Children of all ages are curious,and eventually ask questions.Since parents know their chil-dren and have their trust, thosequestions will probably bedirected at Mom and Dad.Honesty is the best policy, inorder to maintain the estab-lished trust. Most children’shospitals have a child lifespecialist on staff that can helpexplain about hydrocephalusand the surgery on the child’sdevelopmental level. Also, thereare numerous children’s booksavailable to help children better
understand their visits to thehospital.
Expressing feelings to thedoctor will help him/her withprofessional guidance. Manypeople can handle their emo-tions with the help of relativesand friends, but for others,professional help is necessary.Health professionals caring forthe patient are interested in atotal well-being. Their goal is todo what is best for the patientand his/her family.
As a patient, or as the parent ofa patient, take control over thedialogue with the doctor. Be anactive participant in the com-munication process, so that thecaregivers understand whatkind of help is needed.

2424242424 2525252525
Hydrocephalus, Non-Communicat-Hydrocephalus, Non-Communicat-Hydrocephalus, Non-Communicat-Hydrocephalus, Non-Communicat-Hydrocephalus, Non-Communicat-ing or Obstructiveing or Obstructiveing or Obstructiveing or Obstructiveing or Obstructive: Hydrocephalusin which there is obstruction of CSFflow between ventricles
IsotopeIsotopeIsotopeIsotopeIsotope: A radioactive material usedfor determining spinal fluid flowand shunt function
Lumbar SpineLumbar SpineLumbar SpineLumbar SpineLumbar Spine: The area of the spinein the small of the back
MeningesMeningesMeningesMeningesMeninges: The coverings of thebrain and spinal cord
MeningitisMeningitisMeningitisMeningitisMeningitis: Inflammation or infec-tion of the meninges
MRIMRIMRIMRIMRI: Abbreviation for MagneticResonance Imaging. By means ofmagnetic energy, images are taken,showing the ventricles and otherstructures within the brain
PeritoneumPeritoneumPeritoneumPeritoneumPeritoneum: Lining of the abdomi-nal cavity
PleuraPleuraPleuraPleuraPleura: Lining covering the lungs inthe chest cavity
Pleural SpacePleural SpacePleural SpacePleural SpacePleural Space: The space betweenthe pleura and the chest wall whichcontains a small amount of fluid
PneumoencephalogramPneumoencephalogramPneumoencephalogramPneumoencephalogramPneumoencephalogram: X-raydone after filling the ventricles orsubarachnoid space with air, or an-other gas, injected through a spinalneedle
PolypropylenePolypropylenePolypropylenePolypropylenePolypropylene: Plastic used in themanufacture of shunt systems
Proximal CatheterProximal CatheterProximal CatheterProximal CatheterProximal Catheter: Shunt catheterthat is in the ventricle
Shunt (noun)Shunt (noun)Shunt (noun)Shunt (noun)Shunt (noun): A system of tubingused to drain CSF from the ven-tricles or subarachnoid space intoanother area of the body
Shunt (verb)Shunt (verb)Shunt (verb)Shunt (verb)Shunt (verb): Surgical procedureduring which a shunt system is im-planted
SiliconeSiliconeSiliconeSiliconeSilicone: A polymer characterizedby inertness in the body tissues andused in the manufacture of shuntsystems and other medical devices
Slit VentricleSlit VentricleSlit VentricleSlit VentricleSlit Ventricle: Excessive narrowingof the lateral ventricle due tooverdrainage of CSF
Spinal CordSpinal CordSpinal CordSpinal CordSpinal Cord: The elongated struc-ture of the nervous system lyingwithin the spine
StuporousStuporousStuporousStuporousStuporous: A semi-conscious con-dition, in which the patient is verysleepy
Subdural HematomaSubdural HematomaSubdural HematomaSubdural HematomaSubdural Hematoma: A collectionof blood between the skull and thebrain
UltrasoundUltrasoundUltrasoundUltrasoundUltrasound: Sound waves of highfrequency used to outline structureswithin the brain
VentriclesVentriclesVentriclesVentriclesVentricles: The four cavities (twolateral, one third, and one fourth) ly-ing within the brain
VentriculogramVentriculogramVentriculogramVentriculogramVentriculogram: An x-ray tech-nique to visualize the ventricles byfilling them with air or another gas
Abdominal CavityAbdominal CavityAbdominal CavityAbdominal CavityAbdominal Cavity: The area of thebody between the chest and pelviscontaining the liver, intestines, kid-neys and other organs
AngiographyAngiographyAngiographyAngiographyAngiography: X-ray examination ofblood vessels using a contrast dyematerial (giving the vessels visibil-ity)
AntibioticAntibioticAntibioticAntibioticAntibiotic: Any substance (such asPenicillin) which destroys or inhib-its the growth of bacteria
AtriumAtriumAtriumAtriumAtrium: One of the two upperchambers of the heart
CSFCSFCSFCSFCSF: The cerebrospinal fluid
Cerebrospinal FluidCerebrospinal FluidCerebrospinal FluidCerebrospinal FluidCerebrospinal Fluid: The fluid fill-ing the ventricles of the brain andsurrounding the brain and spinalcord
CAT or CT ScanCAT or CT ScanCAT or CT ScanCAT or CT ScanCAT or CT Scan: Abbreviation forcomputerized axial tomography, aspecial x-ray technique which out-lines the ventricles and other struc-tures of the brain in cross section
Choroid PlexusChoroid PlexusChoroid PlexusChoroid PlexusChoroid Plexus: Delicate structuresin the ventricles of the brain thatproduce CSF
CisternographyCisternographyCisternographyCisternographyCisternography: Special x-ray tech-nique using a small amount of ra-dioactive material for seeing theventricles and CSF filled spaces atthe base of the brain
ComatoseComatoseComatoseComatoseComatose: A state in which the pa-tient does not respond to stimula-tion
CongenitalCongenitalCongenitalCongenitalCongenital: A condition presentsince birth
DiagnosisDiagnosisDiagnosisDiagnosisDiagnosis: Determination of apatient’s problem
Distal CatheterDistal CatheterDistal CatheterDistal CatheterDistal Catheter: Shunt catheter thatis farthest from the ventricles, usu-ally in the peritoneum or atrium
DuraDuraDuraDuraDura: The fibrous membrane thatsurrounds the brain and spinal cord(also dura mater)
FistulaFistulaFistulaFistulaFistula: An abnormal passage be-tween two structures or organs
FontanelsFontanelsFontanelsFontanelsFontanels: The spaces between thegrowing bones of the skull of the in-fant, commonly called the soft spot
Foreign BodyForeign BodyForeign BodyForeign BodyForeign Body: An object, such as animplant, introduced into a livingbody from the outside
HydrocephalusHydrocephalusHydrocephalusHydrocephalusHydrocephalus: Excessive build-upof CSF in the ventricles of the brain,causing head enlargement andbrain compression
Hydrocephalus, AcquiredHydrocephalus, AcquiredHydrocephalus, AcquiredHydrocephalus, AcquiredHydrocephalus, Acquired: Hydro-cephalus developed after birth
Hydrocephalus, CommunicatingHydrocephalus, CommunicatingHydrocephalus, CommunicatingHydrocephalus, CommunicatingHydrocephalus, Communicating:Hydrocephalus in which there is noobstruction between ventricles andsubarachnoid space
Hydrocephalus, CongenitalHydrocephalus, CongenitalHydrocephalus, CongenitalHydrocephalus, CongenitalHydrocephalus, Congenital: Hy-drocephalus existing before or atbirth
Glossary

Hydrocephalus Association1-888-598-3789www.hydroassoc.org
Medtronicwww.medtronic.com
Spina Bifida Association of America1-800-621-3141www.sbaa.org
Hydrocephalus: A Guide for Patients, Families & FriendsChuck Toporek and Kelli Robinson
Resources

Medtronic Neurosurgery125 Cremona Drive • Goleta, California 93117-5500 USA(800) 468-9710 USA/Canada(901) 344-0645 International(800) 468-9713 FAX(901) 396-2698 FAX International
LIT11032-1B©Medtronic, Inc. 2003
All Rights ReservedPrinted in USA
Caution: Federal (USA) law restricts these devices to sale by or on the order of a physician.Refer to product package insert for instructions, warnings, precautions and complications.




![Low-pressure hydrocephalus: A case report · 2015-06-22 · Hydrocephalus is a pathological increase in the CSF volume, regardless of hydrostatic or barometric pressure [1]. Normal](https://static.fdocuments.us/doc/165x107/5f932f5774b0c262f97f04f4/low-pressure-hydrocephalus-a-case-report-2015-06-22-hydrocephalus-is-a-pathological.jpg)

![Management of subdural effusion and hydrocephalus ......hydrocephalus in patients with DC for TBI is 10 to 40% [10, 12, 13, 19]. SDE is defined as cerebrospinal fluid (CSF) accumula-tion](https://static.fdocuments.us/doc/165x107/60f77946a97a3c60fd2cc41f/management-of-subdural-effusion-and-hydrocephalus-hydrocephalus-in-patients.jpg)