
Human The Anatomy Respiratory & Physiology...
15
1 Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Human Anatomy & Physiology SEVENTH EDITION Elaine N. Marieb Katja Hoehn C H A P T E R 22 The Respiratory System P A R T B Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Carbon Dioxide Transport Carbon dioxide is transported in the blood in three forms Dissolved in plasma – 7 to 10% Chemically bound to hemoglobin – 20% is carried in RBCs as carbaminohemoglobin Bicarbonate ion in plasma – 70% is transported as bicarbonate (HCO 3 – )
Transcript of Human The Anatomy Respiratory & Physiology...

1
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Human Anatomy & PhysiologySEVENTH EDITION
Elaine N. MariebKatja Hoehn
PowerPoint® Lecture Slidesprepared by Vince Austin,Bluegrass Technicaland Community College
C H
A P
T E
R22TheRespiratorySystem
P A R T B
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Carbon Dioxide Transport
Carbon dioxide is transported in the blood in threeforms
Dissolved in plasma – 7 to 10%
Chemically bound to hemoglobin – 20% is carriedin RBCs as carbaminohemoglobin
Bicarbonate ion in plasma – 70% is transported asbicarbonate (HCO3
–)
2
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Bicarbonateion
HCO3–
Hydrogenion
H+↔+ H2O
Water
↔
Carbonicacid
Carbondioxide
+H2CO3CO2
Transport and Exchange of Carbon Dioxide
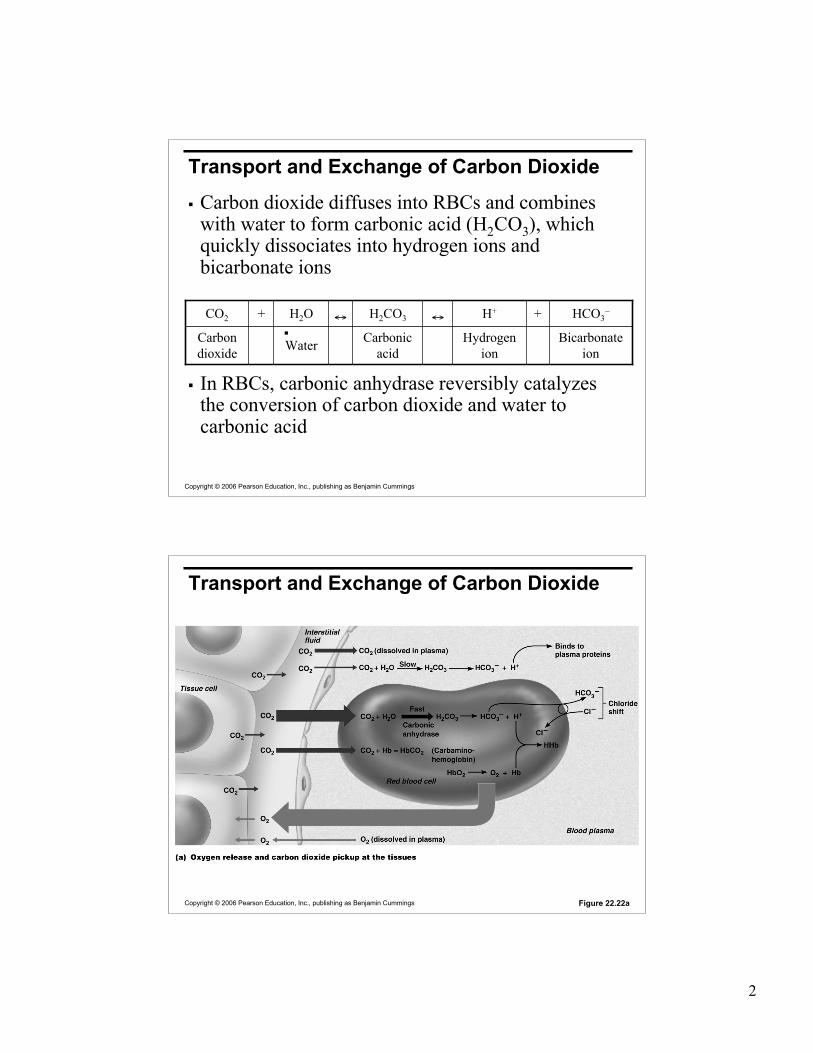
Carbon dioxide diffuses into RBCs and combineswith water to form carbonic acid (H2CO3), whichquickly dissociates into hydrogen ions andbicarbonate ions
In RBCs, carbonic anhydrase reversibly catalyzesthe conversion of carbon dioxide and water tocarbonic acid
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Transport and Exchange of Carbon Dioxide
Figure 22.22a

3
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Transport and Exchange of Carbon Dioxide
At the tissues:
Bicarbonate quickly diffuses from RBCs into theplasma
The chloride shift – to counterbalance the outrushof negative bicarbonate ions from the RBCs,chloride ions (Cl–) move from the plasma into theerythrocytes
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Transport and Exchange of Carbon Dioxide
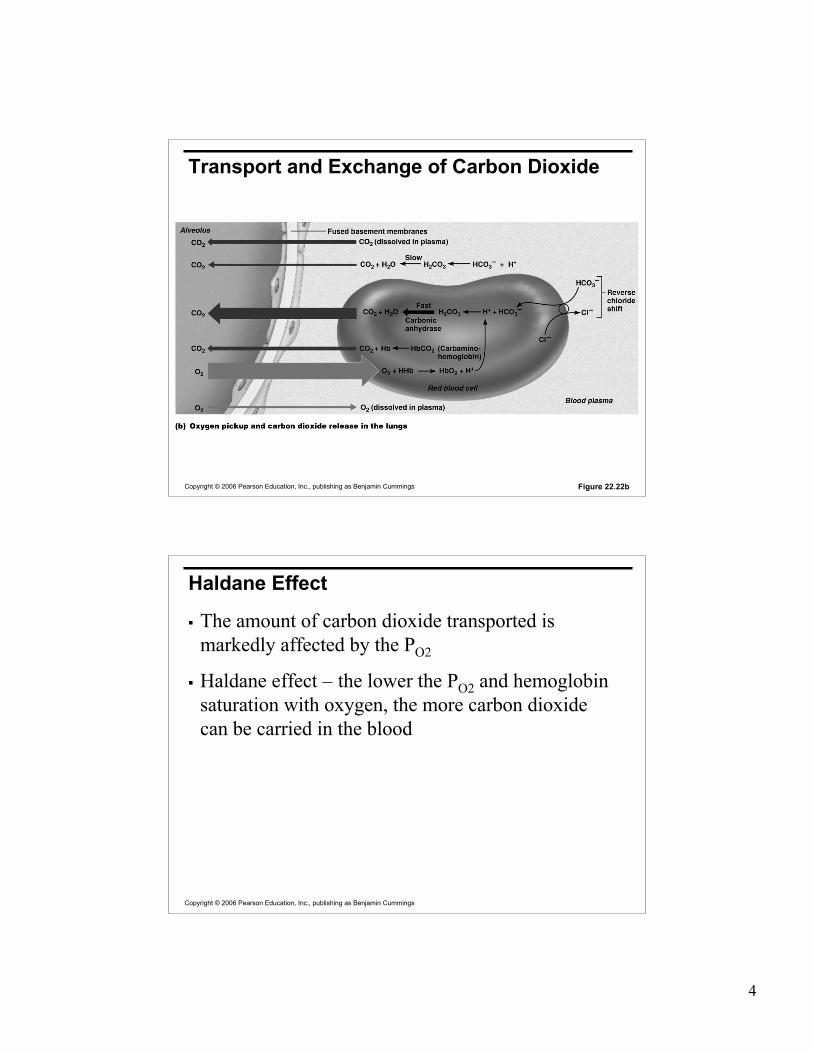
At the lungs, these processes are reversed
Bicarbonate ions move into the RBCs and bindwith hydrogen ions to form carbonic acid
Carbonic acid is then split by carbonic anhydraseto release carbon dioxide and water
Carbon dioxide then diffuses from the blood intothe alveoli
4
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Transport and Exchange of Carbon Dioxide
Figure 22.22b
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Haldane Effect
The amount of carbon dioxide transported ismarkedly affected by the PO2
Haldane effect – the lower the PO2 and hemoglobinsaturation with oxygen, the more carbon dioxidecan be carried in the blood

5
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Haldane Effect
At the tissues, as more carbon dioxide enters theblood:
More oxygen dissociates from hemoglobin (Bohreffect)
More carbon dioxide combines with hemoglobin,and more bicarbonate ions are formed
This situation is reversed in pulmonary circulation
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Haldane Effect
Figure 22.23
6
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Influence of Carbon Dioxide on Blood pH The carbonic acid–bicarbonate buffer system resists blood
pH changes
If hydrogen ion concentrations in blood begin to rise,excess H+ is removed by combining with HCO3
–
If hydrogen ion concentrations begin to drop, carbonic aciddissociates, releasing H+
Changes in respiratory rate can also: Alter blood pH
Provide a fast-acting system to adjust pH when it isdisturbed by metabolic factors
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Control of Respiration:Medullary Respiratory Centers Inspiration is mostly done by movement of the diaphragm
Diaphragm is controlled by the phrenic nerve
Basic respiratory cycle is controlled by the PaceMakwerNeurons (PN)in the medulla oblongata
The PN communicates with the dorsal respiratory group(DRG), or inspiratory center:
Is located near the root of nerve IX
Excites the inspiratory muscles (via phrenic nerve andintercostal nerves) and sets eupnea (12-15 breaths/minute)

7
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Control of Respiration:Medullary Respiratory Centers The dorsal respiratory group (DRG), also sends signals to
the ventral respiratory group (VRG) :
Appears to be the involved in expiration
Sends signals to the solitary nuclei in medulla
They in turn send inhibitory signals to the DRG. This thusturns off the stimulation of the phrenic nerve and starts theexhalation process.
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Control of Respiration:Medullary Respiratory Centers
PN
DRGDRG
DRG Phrenic Nerves
stimulationinhibition

8
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pons Respiratory Centers
Pons centers:
Influence and modify activity ofthe medullary centers
Smooth out inspiration andexpiration transitions and viceversa
The pontine respiratory group(PRG)
Pneumotaxic center
Apneustic center
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pons Respiratory CentersPneumotaxic center (PC)
Provides inhibition to the DRG,resulting in shorter periods ofinspiration
Apneustic Center
Provides stimulation of the DRGand could result in deeperinspiration or even breath-holdingat end of inspiration
Main function of PC is to providesmooth transition betweeninspiration and expiration. It tends toinhibit the apneustic center as well.
9
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
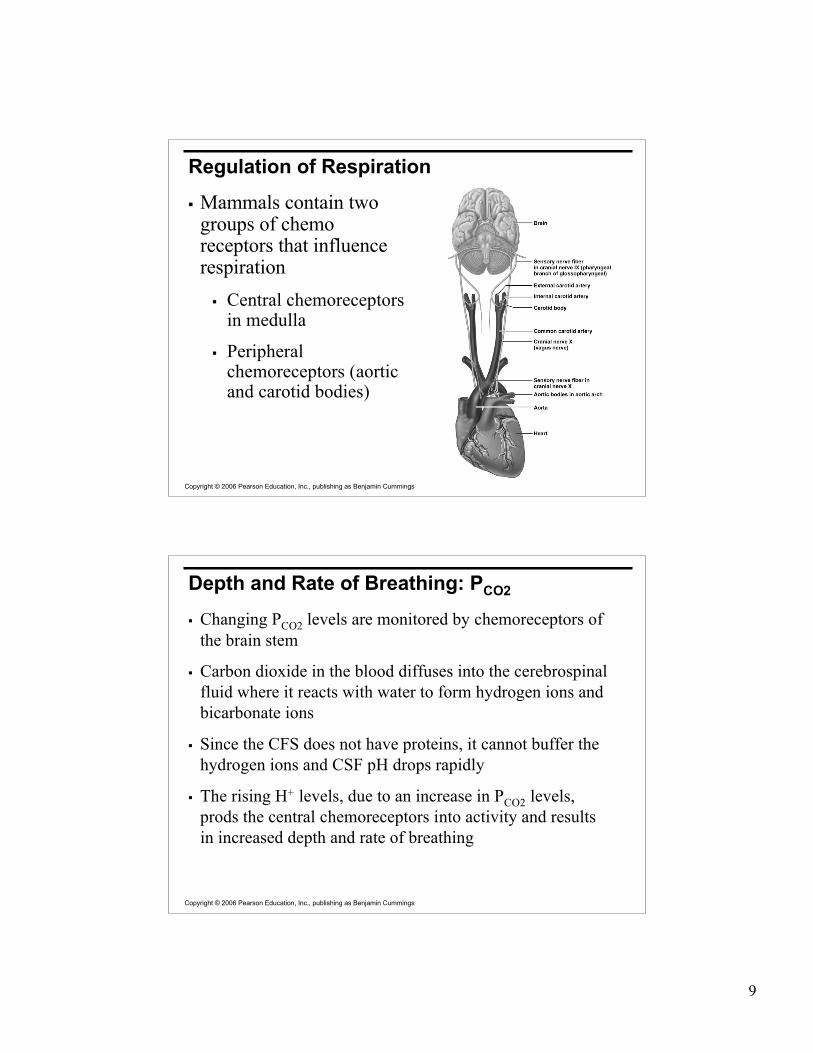
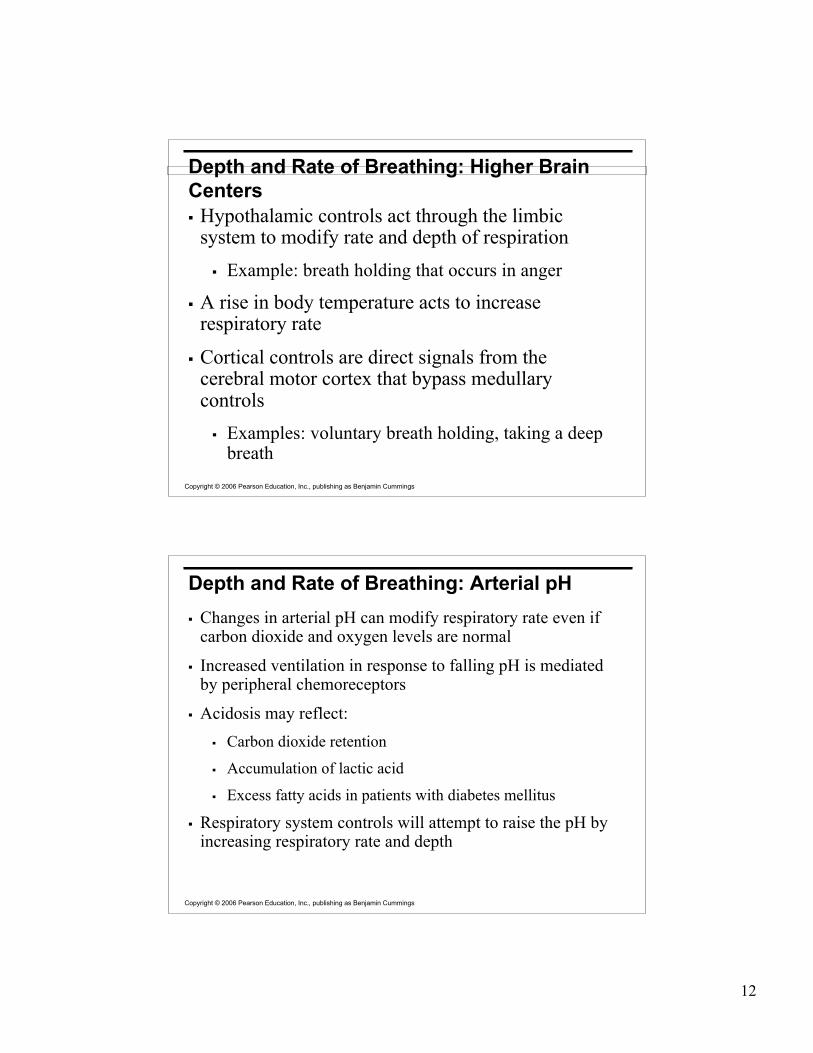
Regulation of Respiration
Mammals contain twogroups of chemoreceptors that influencerespiration
Central chemoreceptorsin medulla
Peripheralchemoreceptors (aorticand carotid bodies)
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
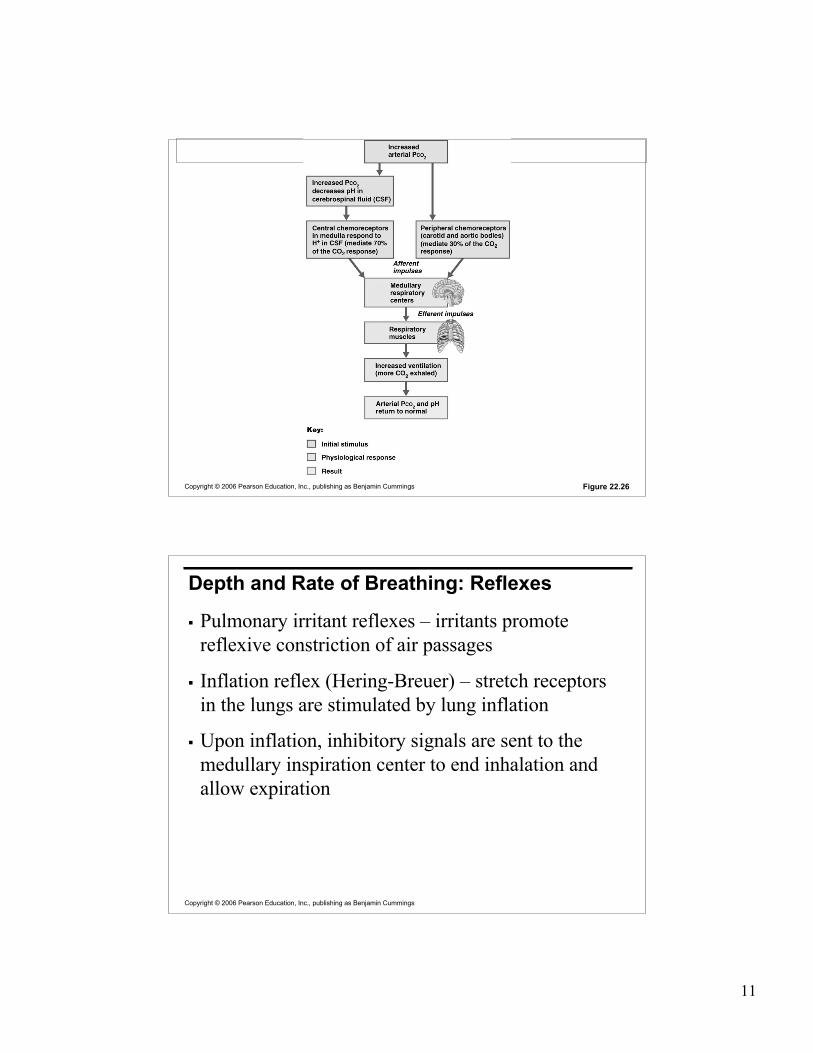
Depth and Rate of Breathing: PCO2
Changing PCO2 levels are monitored by chemoreceptors ofthe brain stem
Carbon dioxide in the blood diffuses into the cerebrospinalfluid where it reacts with water to form hydrogen ions andbicarbonate ions
Since the CFS does not have proteins, it cannot buffer thehydrogen ions and CSF pH drops rapidly
The rising H+ levels, due to an increase in PCO2 levels,prods the central chemoreceptors into activity and resultsin increased depth and rate of breathing

10
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Depth and Rate of Breathing: PCO2
Hyperventilation – increased depth and rate ofbreathing that:
Quickly flushes carbon dioxide from the blood
Occurs in response to hypercapnia
Hypoventilation – slow and shallow breathing dueto abnormally low PCO2 levels
Apnea (breathing cessation) may occur until PCO2levels rise
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Arterial oxygen levels are monitored by the aorticand carotid bodies
Substantial drops in arterial PO2 (to 60 mm Hg) areneeded before oxygen levels become a majorstimulus for increased ventilation
If carbon dioxide is not removed (e.g., as inemphysema and chronic bronchitis),chemoreceptors become unresponsive to PCO2chemical stimuli
In such cases, PO2 levels become the principalrespiratory stimulus (hypoxic drive)
Depth and Rate of Breathing: PO2
11
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 22.26
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Depth and Rate of Breathing: Reflexes
Pulmonary irritant reflexes – irritants promotereflexive constriction of air passages
Inflation reflex (Hering-Breuer) – stretch receptorsin the lungs are stimulated by lung inflation
Upon inflation, inhibitory signals are sent to themedullary inspiration center to end inhalation andallow expiration
12
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Depth and Rate of Breathing: Higher BrainCenters Hypothalamic controls act through the limbic
system to modify rate and depth of respiration Example: breath holding that occurs in anger
A rise in body temperature acts to increaserespiratory rate
Cortical controls are direct signals from thecerebral motor cortex that bypass medullarycontrols
Examples: voluntary breath holding, taking a deepbreath
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Depth and Rate of Breathing: Arterial pH Changes in arterial pH can modify respiratory rate even if
carbon dioxide and oxygen levels are normal
Increased ventilation in response to falling pH is mediatedby peripheral chemoreceptors
Acidosis may reflect: Carbon dioxide retention
Accumulation of lactic acid
Excess fatty acids in patients with diabetes mellitus
Respiratory system controls will attempt to raise the pH byincreasing respiratory rate and depth
13
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Medullary Respiratory Centers
Figure 22.25
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Chronic Obstructive Pulmonary Disease(COPD) Exemplified by chronic bronchitis and obstructive
emphysema
Patients have a history of: Smoking
Dyspnea, where labored breathing occurs and getsprogressively worse
Coughing and frequent pulmonary infections
COPD victims develop respiratory failureaccompanied by hypoxemia, carbon dioxideretention, and respiratory acidosis

14
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pathogenesis of COPD
Figure 22.28
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Asthma
Characterized by dyspnea, wheezing, and chesttightness
Active inflammation of the airways precedesbronchospasms
Airway inflammation is an immune responsecaused by release of IL-4 and IL-5, whichstimulate IgE and recruit inflammatory cells
Airways thickened with inflammatory exudatesmagnify the effect of bronchospasms

15
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Tuberculosis
Infectious disease caused by the bacteriumMycobacterium tuberculosis
Symptoms include fever, night sweats, weight loss,a racking cough, and splitting headache
Treatment entails a 12-month course of antibiotics
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Accounts for 1/3 of all cancer deaths in the U.S.
90% of all patients with lung cancer were smokers
The three most common types are: Squamous cell carcinoma (20-40% of cases) arises
in bronchial epithelium
Adenocarcinoma (25-35% of cases) originates inperipheral lung area
Small cell carcinoma (20-25% of cases) containslymphocyte-like cells that originate in the primarybronchi and subsequently metastasize
Lung Cancer


















